Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 16
Characteristics and Prevalence of Early Chronic Obstructive Pulmonary Disease in a Middle-Aged Population: Results from a Nationwide-Representative Sample
Authors Kim T ![]() , Kim J
, Kim J ![]() , Kim JH
, Kim JH
Received 7 September 2021
Accepted for publication 3 November 2021
Published 12 November 2021 Volume 2021:16 Pages 3083—3091
DOI https://doi.org/10.2147/COPD.S338118
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Richard Russell
Taeyun Kim,1 Jehun Kim,2 Jun Hyeong Kim3
1Division of Pulmonology, Department of Internal Medicine, The Armed Forces Goyang Hospital, Goyang-si, South Korea; 2Division of Pulmonology, Department of Internal Medicine, Kosin University College of Medicine, Kosin University Gospel Hospital, Busan, South Korea; 3Division of Pulmonology, Department of Internal Medicine, Busan Veterans Hospital, Busan, South Korea
Correspondence: Jehun Kim
Division of Pulmonology, Department of Internal Medicine, Kosin University College of Medicine, Kosin University Gospel Hospital, 262 Gamcheon-ro, Seo-gu, Busan, 49267, South Korea
Tel/Fax +82-51-990-5820
Email [email protected]
Jun Hyeong Kim
Division of Pulmonology, Department of Internal Medicine, Busan Veterans Hospital, 420, Baegyang-daero, Sasang-gu, Busan, 46996, South Korea
Tel +82-51-601-6988
Fax +82-51-601-6339
Email [email protected]
Introduction: Few studies have examined the prevalence and associated factors of early chronic obstructive pulmonary disease (COPD) in Asians.
Objective: To evaluate the prevalence of early COPD and its associated factors among non-institutionalized middle-aged Korean adults.
Methods: A total of 3195 participants aged 40– 49 years from the 2016– 2018 Korea National Health and Nutrition Examination Survey were included in this study. Patients (1) aged less than 50 years, (2) with a minimum of 10 pack-years of smoking, and (3) with forced expiratory volume in 1 s/forced vital capacity (FEV1/FVC) below the lower limit of normal were diagnosed with early COPD. The prevalence and odds ratio (OR) for early COPD were measured using multivariate logistic regression analysis, and the demographic data, anthropometric measurements, socioeconomic status, and lifestyle factors were considered covariates.
Results: The overall prevalence of early COPD among the middle-aged Korean population was 2.4% (4.4% in men and 0.4% in women), while that in participants with ≥ 10 pack-years was 8.2% (8.1% in men and 11.3% in women). A multivariate logistic regression model showed that male sex, urban residence, chronic sputum production, and hypertriglyceridemia were associated with increased ORs for early COPD in middle-aged, non-institutionalized Korean adults.
Conclusion: Early COPD is prevalent among middle-aged smokers in Korea. Efforts are needed to reduce the potential negative effects of early COPD on public health in Korea and other Asian countries.
Keywords: early COPD, KNHANES, prevalence
Introduction
Chronic obstructive pulmonary disease (COPD) refers to a chronic inflammatory lung disease characterized by severe airflow limitation and health-related problems, and smoking has been traditionally considered a major risk factor for the disease.1 Although smoking is the leading cause of COPD, other risk factors such as biomass exposure or air pollution have substantial effects on the development of the disease in women, especially those living in Asia and Africa.2 According to the World Health Organization, COPD is currently the third leading cause of death. Moreover, COPD remains the most common cause of chronic respiratory disease-related death worldwide,2 and its increasing disease burden is a major public health concern.3
Understanding the early origins of COPD is imperative. However, the marked heterogeneity of COPD owing to various etiologies, different pathogenic mechanisms, varying presentations, and progression impedes the identification of the full trajectory of the disease. For example, exposure to airborne contaminants, childhood asthma, smoke during adolescent, and maternal smoking could all affect the lung function in early life and could contribute to the early development of COPD.4 Given that most studies in COPD have included adults aged >60 years old and recent studies have increasingly suggested significant differences in lung function trajectory that could be detected at a much younger age, distinguishing early disease from late disease is of utmost importance.6
The concept of early COPD is emerging in both academic and clinical fields, although the universally accepted criteria for diagnosing the disease are lacking. Early COPD is defined based on operational and practical considerations, assuming that detecting the initial abnormalities may halt the development of significant COPD.7 A 10-year follow-up study revealed that adults with early COPD had a much higher risk of developing COPD compared with those without early COPD. Approximately 24% of heavy smokers with early COPD developed clinical COPD 10 years later.8 Patients with early COPD presented distinct structural abnormalities and physiologic impairment,9 frequent respiratory symptoms, and increased risks of hospitalization and death.10
Although several studies have investigated the prevalence, features, and prognosis of early COPD, there remains a paucity of data regarding the disease in Asian populations. A recent study assessed the bronchodilator response in patients with early COPD, defined as stage 1 and 2 COPD based on the Global Initiative for Chronic Obstructive Lung Disease (GOLD) classifications, rather than based on the lower limit of normal (LLN).11 However, the categorization of early COPD in a younger population (<50 years) using a fixed ratio may preclude estimating the true burden of the early changes of lung parenchyma and airway remodeling.7 Consequently, the present study aimed to evaluate the prevalence and clinical characteristics of early COPD in middle-aged adults by applying an operational definition of early COPD7 to a dataset obtained from a nationwide representative sample of the South Korean population.
Materials and Methods
Study Participants
This study analyzed the data from the 7th Korea National Health and Nutrition Examination Survey (KNHANES, 2016–2018). The KNHANES is a population-based, cross-sectional, and nationally representative study designed to evaluate the health and nutritional status of non-institutionalized Korean citizens. The Korea Center for Disease Control conducts the survey annually based on the data from the Korean Statistical Office census, and the survey includes 3800 households from 576 randomly assigned survey areas. The survey was performed in three parts and involved the collection of health-related information from each study participant: a health interview, a health examination, and a nutrition survey. The detailed protocols and data resource profiles of the KNHANES are summarized elsewhere.12
The 2016–2018 KNHANES assessed 31,689 individuals; of them, only 24,269 (76.6%) participants responded to the survey. The participants were selected using a stratified two-stage cluster sampling method through a two-step process: probability proportional to size sampling and systematic sampling. However, as only adults aged ≥40 years underwent pulmonary function tests (PFTs) and the operational definition of early COPD included those aged <50 years to more sensitively detect this condition,7 20,350 participants were excluded. Participants with missing values on variables of interest were also excluded. Although the KNANES initially evaluated 30,000 citizens, 90% of the participants were excluded, and only 3195 were included in the final analyses.
Data Measurements
Spirometry was performed using a Vyntus SPIRO (CareFusion, San Diego, CA, USA) by highly trained medical technicians at the mobile examination center. Quality control and standardization were conducted based on the standards for reporting PFT results released by the American Thoracic and European Respiratory Societies.13 The forced expiratory volume in 1 s (FEV1, liter [L]), predicted FEV1%, forced vital capacity (FVC, L), predicted FVC%, and the percentages of FEV1/FVC from the pre-bronchodilator PFT results were measured.
Early COPD was defined according to the operational definitions proposed by Martinez et al7—participants <50 years old with ≥10 pack-years of smoking history and any of the following abnormalities: 1) early airflow limitation (FEV1/FVC < LLN), 2) compatible computed tomography (CT) abnormalities, and 3) rapid decline in FEV1 (≥60 mL/years). Of these abnormalities, CT images and subsequent FEV1 levels were not available in the KNHANES. Thus, age, pack-years, and LLN were used to categorize early COPD among the study participants.
Data on self-reported respiratory symptoms (chronic cough and chronic sputum) were obtained based on the participants’ responses to the following question: “have you had sputum or cough for more than 3 months?” Quality of life was measured using the European Quality of Life-5 Dimensions index, which evaluates mobility, self-care, usual activity, pain/discomfort, and anxiety/depression, with a maximum score of 1 indicating the best health state.
Data on sociodemographic characteristics including age, sex, residence, educational level (middle school or lower, high school, and college or higher), household income (lowest, lower middle, higher middle, and highest), smoking status (never, former, and current), and alcohol consumption were obtained during face-to-face interviews. Anthropometric variables, including body mass index (BMI, kg/m2) and waist circumference (cm), were also measured. Blood pressure was calculated as the average of the second and third measurements, with hypertension defined as a systolic blood pressure of ≥140 mmHg, diastolic blood pressure of ≥90 mmHg, or use of antihypertensive medication.14 Data on the laboratory examination results, including fasting glucose (mg/dL), glycosylated hemoglobin (%), triglyceride (mg/dL), low-density lipoprotein cholesterol (mg/dL), high-density lipoprotein cholesterol (mg/dL), hematocrit (%), high sensitivity C-reactive protein (mg/dL), estimated glomerular filtration rate (mL/min/1.73 m2) calculated using the modification of diet in renal disease equation, urine cotinine level (ng/mL), and urine 4-(methylnitrosamino)-1-(3-pyridyl)-1-butanol (NNAL) (pg/mL) levels were also obtained.
Statistical Analysis
The KNAHNES followed a multi-stage clustered probability design to obtain the data of a nationally representative sample of Korean population. To address the issues related to the complex survey design, non-responders and post-stratification census data-based sample weights were determined. Therefore, all analyses used a complex survey design and sample weights. Categorical variables were compared using chi-square or Fisher’s exact tests and expressed as weighted percentages with 95% confidence intervals (CIs). Continuous variables were compared using Student’s t-tests and expressed as weighted numbers with 95% CIs. Complex sample logistic regression was used to calculate the odds ratios (OR) with the corresponding 95% CI for early COPD. The P-values for all comparative variables and those for the trends in each variable were calculated. The multivariate model considered age, sex, BMI, alcohol consumption, smoking status, educational level, household income level, and residence as covariates. All tests were two-tailed, and a P-value of <0.05 was considered significant. All statistical analyses were performed using IBM SPSS Statistics for Windows, version 24.0 (IBM Corp., Armonk, NY, USA) and R software version 4.0.3 for Windows (R Development Core Team).
Ethical Approval
The study protocol was approved by the Institutional Review Board of the Kosin University Gospel Hospital (no. 2021-08-033), and was conducted in accordance with the principles of the Declaration of Helsinki. All procedures were performed in accordance with the relevant guidelines and regulations.
Results
The prevalence rates of early COPD among the middle-aged Korean population were 2.4% (4.4% in men and 0.4% in women) and 8.2% in smokers with ≥10 pack-years (8.1% in men and 11.3% in women, Figure 1). The prevalence was higher in men than in women; however, among heavy smokers, the prevalence was higher in women than in men.
 |
Figure 1 The prevalence of early chronic obstructive pulmonary disease in a middle-aged Korean population (A) and in smokers with ≥10 pack-years (B). Data are expressed as proportions or means with 95% confidence intervals (error bars). |
Table 1 shows the general characteristics of the early COPD and control groups. Participants with early COPD presented a lower FEV1/FVC ratio, a lower predicted FEV1%, and a higher predicted FVC% compared with the control group. Although the overall mean age was not different, participants with early COPD comprised a high proportion of men, urban residents, current smokers, heavy alcohol drinkers, individuals with chronic sputum production, and individuals with hypertension. They also showed higher systolic and diastolic blood pressure, triglyceride levels, hematocrit count, and urinary tobacco metabolite levels (eg, urine cotinine and urine NNAL).
 |
 |
 |
Table 1 Characteristics of Study Participants Under 50 Years of Age According to the Presence of Early COPD |
The adjusted ORs for early COPD in terms of demographic characteristics, anthropometric measurements, socioeconomic, and lifestyle factors are presented in Table 2. Male sex and the presence of hypertension were significantly positively associated with early COPD. Urban residence, chronic sputum production, and hypertriglyceridemia were positively associated with early COPD; however, only a positive trend was observed.
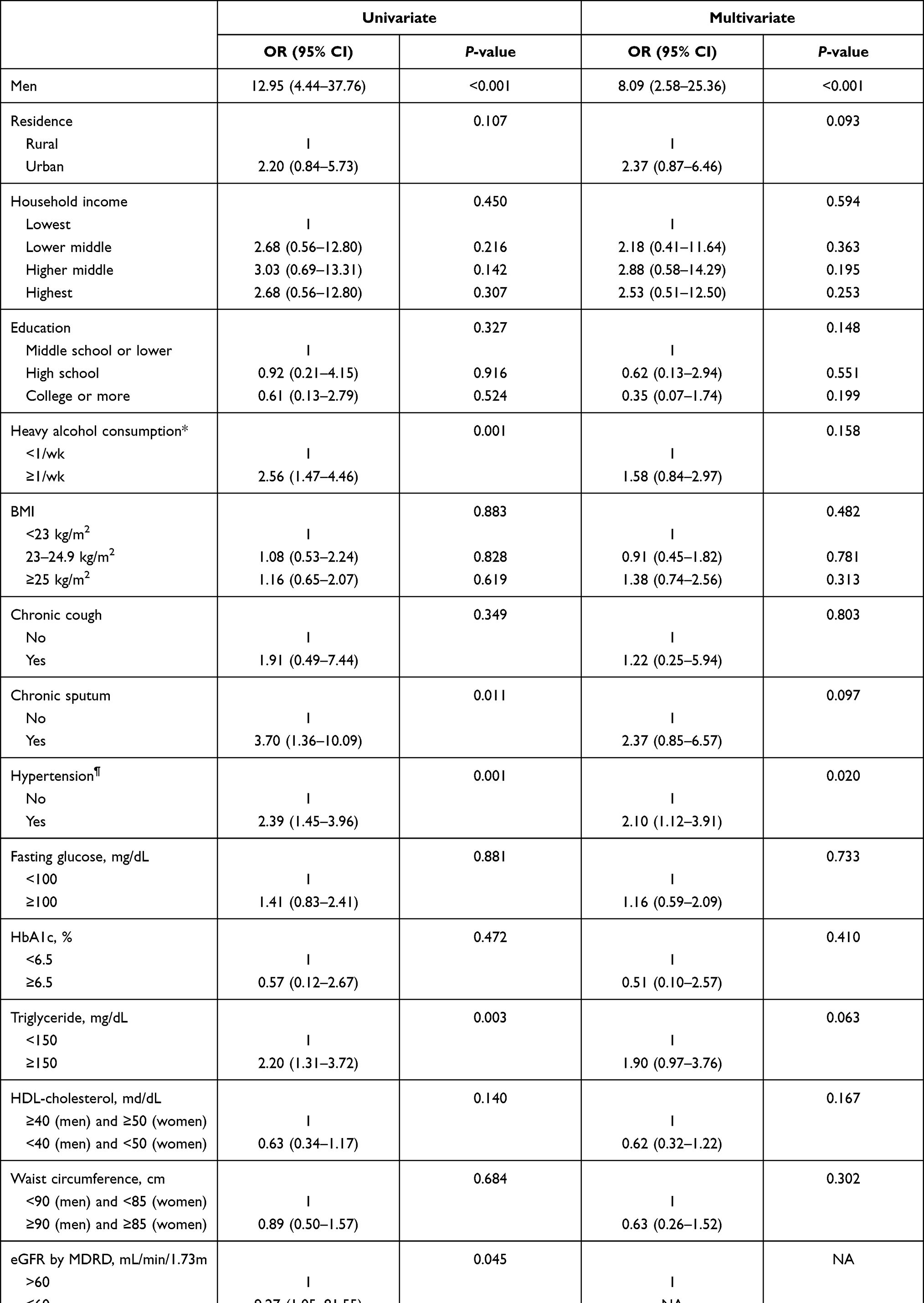 |
Table 2 Factors Affecting Early COPD Among Middle-Aged (40–49 Years) Adults |
Discussion
Although the concept of early COPD is not novel, there has been renewed interest in its importance. The present study assessed the recent prevalence and clinical characteristics of early COPD among middle-aged Korean adults in a nationwide representative sample of South Korean population. To our knowledge, this is the first study to evaluate Asian patients with early COPD based on an operational definition.7
In this study, the prevalence of early COPD in a middle-aged (40–49 years) population was 2.4% (4.4% in men and 0.4% in women), while a much higher prevalence was observed in adults with ≥10 pack-years (8.2% overall, 8.1% in men, and 11.3% in women). Although the prevalence of early COPD was higher in men than in women, the trend was reversed in participants with ≥10 pack-years. The prevalence of early COPD in heavy smokers was lower than the estimated prevalence in the Copenhagen General Population Study (CGPS).10 The CGPS included 8064 participants aged 40–49 years with ≥10 pack-years, with an estimated prevalence of early COPD of 15%. This result is partially explained by reports of a lower prevalence of COPD in the Korean population compared with that in the Danish population2 and a lower OR for COPD in Asians than in Caucasians.15
A recent cross-sectional study in South Korea reported an estimated early COPD prevalence of 10%, which is slightly higher than the estimates from other ethnic groups,16 as well as the current results. The study, which assessed a dataset similar to that in our study, included adults aged ≥50 years with a reduced fixed ratio, rather than LLN, which is a more comprehensive approach than the operational definition of early COPD. Thus, the categorization in that study might have overestimated the prevalence of early COPD.
The multivariate model in the present study revealed an association between chronic sputum production and an increased OR for early COPD in middle-aged adults. The importance of chronic sputum secretion was minimized because sputum production is weakly related to disease progression in COPD.17 However, evidence has consistently shown that symptoms are associated with rapid FEV1 decline,18 acute exacerbation, and hospitalization in COPD patients.19 Moreover, in middle-aged smokers without airflow limitation, a longitudinal cohort study reported that chronic mucus hypersecretion was an important predictor of COPD development.18
Furthermore, male sex, hypertension, urban life, and hypertriglyceridemia were positively associated with early COPD. First, in terms of sex, chronic sputum production, which represents the early development of COPD,18 is more prevalent in men than in women,20 and this may partially explain the observed finding, although complex underpinnings of the sex difference exist in COPD development. Second, considering an intricate relationship between hypertension, cardiovascular disease, and COPD, the observed positive association may be plausible, which is in line with the report of a previous study.21 Third, an urban-rural disparity for COPD has been suggested in several studies. Further understanding of the epidemiology, risk factors, and potential interventions in the urban population with COPD may be warranted, as the group has been understudied.22 Fourth, the observed association between hypertriglyceridemia and COPD seems interesting. A previous cohort study reported a positive relationship between hyperlipidemia and COPD,23 suggesting a different COPD phenotype or other factors as reasons related to this finding.
The early initiation of disease-modifying treatment has been highlighted in several clinical trials in different medical fields. The terms “preclinical,” “pre-,” “early,” and “mild” have been widely and complexly combined to understand the longitudinal course of COPD. However, preclinical COPD is defined as FEV−1/FVC of <0.70 with or without mild respiratory symptoms,24 pre-COPD or GOLD stage 0 is defined as FEV−1/FVC of >0.70 and at an increased risk for COPD development,25 and mild COPD is defined as GOLD stage 1.
The international complexity in COPD epidemiology,26 early-life exposure to smoking, and low maximum attained lung function make it difficult to identify the early disease burden of COPD.27 Additionally, smoking is not the only risk factor for COPD; the factors include genetic susceptibility,28 air pollution, infections in childhood,4 and innate/adaptive immune dysfunction,29 which can also result in early changes in the small airways and contribute to the development of COPD at an early age. Despite the importance and interest in this topic, there remains no universally accepted definition of early COPD, and only a few studies have reported on the disease course. Thus, longitudinal clinical studies on the disease course and early interventions are required.
Our study had several limitations. First, as this cross-sectional study did not consider temporality in the analysis, caution is necessary when interpreting the findings. Second, although this study assessed the data from 30,000 participants, only a few of them were classified as having early COPD, and this might have impacted the observed statistical probabilities. Additional studies involving larger populations may more accurately demonstrate the burden of early COPD in Asian populations. Moreover, a revised definition that reflects the different biological characteristics of Asian individuals may be required. Third, because the KNHANES only evaluated pre-bronchodilator PFTs, this might have resulted in misclassifications and misdiagnoses. Fourth, the KNHANES did not investigate the data on childhood asthma or childhood respiratory infections, which could be related to the early development of COPD,5 and this might have affected the observed findings.
Despite these limitations, this study was the first to evaluate the prevalence and clinical characteristics of early COPD, a condition that was classified based on practical and operational definitions. Furthermore, the results of this study are consistent with those of other studies that have emphasized the importance of chronic sputum production in COPD development. Considering the importance of COPD on public health problems, even in the early stages, little is known about early COPD. In order to draw holistic picture of this complex condition, understanding the heterogeneous nature of COPD is of utmost importance, and our results may elucidate some part of this picture.
Conclusion
Early COPD was prevalent in a middle-aged Korean population, especially among smokers with ≥10 pack-years. Male sex, urban residence, chronic sputum production, and hypertriglyceridemia were positively associated with early COPD. As only a few studies have reported on this topic in Asian populations, more studies are needed to elucidate the epidemiology of early COPD and its associated factors. Moreover, special efforts are necessary to understand the complex biological underpinnings of early COPD.
Funding
This work was supported by the National Research Foundation of the Korea grant funded by the Korean government (grant no. 2021R1G1A1009361).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Viegi G, Pistelli F, Sherrill DL, Maio S, Baldacci S, Carrozzi L. Definition, epidemiology and natural history of COPD. Eur Respir J. 2007;30(5):993–1013. doi:10.1183/09031936.00082507
2. Soriano JB, Kendrick PJ, Paulson KR. Prevalence and attributable health burden of chronic respiratory diseases, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Respir Med. 2020;8(6):585–596. doi:10.1016/S2213-2600(20)30105-3
3. Zhu B, Wang Y, Ming J, Chen W, Zhang L. Disease burden of COPD in China: a systematic review. Int J Chron Obstruct Pulmon Dis. 2018;13:1353–1364. doi:10.2147/COPD.S161555
4. Martinez FD, Drazen JM. Early-life origins of chronic obstructive pulmonary disease. N Engl J Med. 2016;375(9):871–878. doi:10.1056/NEJMra1603287
5. Lange P, Celli B, Agustí A, et al. Lung-function trajectories leading to chronic obstructive pulmonary disease. N Engl J Med. 2015;373(2):111–122. doi:10.1056/NEJMoa1411532
6. Marott JL, Ingebrigtsen TS, Çolak Y, Vestbo J, Lange P. Lung function trajectories leading to chronic obstructive pulmonary disease as predictors of exacerbations and mortality. Am J Respir Crit Care Med. 2020;202(2):210–218. doi:10.1164/rccm.201911-2115OC
7. Martinez FJ, Han MK, Allinson JP, et al. At the root: defining and halting progression of early chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2018;197(12):1540–1551. doi:10.1164/rccm.201710-2028PP
8. Çolak Y, Afzal S, Nordestgaard BG, Lange P, Vestbo J. Importance of early COPD in young adults for development of clinical COPD: findings from the Copenhagen General Population Study. Am J Respir Crit Care Med. 2021;203(10):1245–1256. doi:10.1164/rccm.202003-0532OC
9. Cosío BG, Pascual-Guardia S, Borras-Santos A, et al. Phenotypic characterisation of early COPD: a prospective case–control study. ERJ Open Res. 2020;6(4):00047–2020. doi:10.1183/23120541.00047-2020
10. Çolak Y, Afzal S, Nordestgaard BG, Vestbo J, Lange P. Prevalence, characteristics, and prognosis of early chronic obstructive pulmonary disease. The Copenhagen General Population Study. Am J Respir Crit Care Med. 2020;201(6):671–680. doi:10.1164/rccm.201908-1644OC
11. Chen C, Jian W, Gao Y, Xie Y, Song Y, Zheng J. Early COPD patients with lung hyperinflation associated with poorer lung function but better bronchodilator responsiveness. Int J Chron Obstruct Pulmon Dis. 2016;11:2519–2526. doi:10.2147/COPD.S110021
12. Kweon S, Kim Y, Jang M-J, et al. Data resource profile: the Korea National Health and Nutrition Examination Survey (KNHANES). Int J Epidemiol. 2014;43(1):69–77. doi:10.1093/ije/dyt228
13. Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirometry. Eur Respir J. 2005;26(2):319–338. doi:10.1183/09031936.05.00034805
14. James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311(5):507–520. doi:10.1001/jama.2013.284427
15. Gilkes A, Ashworth M, Schofield P, et al. Does COPD risk vary by ethnicity? A retrospective cross-sectional study. Int J Chron Obstruct Pulmon Dis. 2016;11:739–746. doi:10.2147/COPD.S96391
16. Lee J-H, Park MA, Park MJ, Jo YS. Clinical characteristics and related risk factors of depression in patients with early COPD. Int J Chron Obstruct Pulmon Dis. 2018;13:1583–1590. doi:10.2147/COPD.S157165
17. Fletcher C, Peto R. The natural history of chronic airflow obstruction. Br Med J. 1977;1(6077):1645–1648. doi:10.1136/bmj.1.6077.1645
18. Allinson JP, Hardy R, Donaldson GC, Shaheen SO, Kuh D, Wedzicha JA. The presence of chronic mucus hypersecretion across adult life in relation to chronic obstructive pulmonary disease development. Am J Respir Crit Care Med. 2016;193(6):662–672. doi:10.1164/rccm.201511-2210OC
19. Burgel PR, Nesme-Meyer P, Chanez P, et al. Cough and sputum production are associated with frequent exacerbations and hospitalizations in COPD subjects. Chest. 2009;135(4):975–982. doi:10.1378/chest.08-2062
20. Lee BR, Kim YI, Kim S, et al. Prevalence of chronic sputum and associated factors in Korean adults. J Korean Med Sci. 2014;29(6):825–830. doi:10.3346/jkms.2014.29.6.825
21. Kim S-H, Park J-H, Lee J-K, Heo EY, Kim DK, Chung HS. Chronic obstructive pulmonary disease is independently associated with hypertension in men: a survey design analysis using nationwide survey data. Medicine. 2017;96(19):e6826. doi:10.1097/MD.0000000000006826
22. Drummond MB. Obstructive airway disease in urban populations. Curr Opin Pulm Med. 2014;20(2):180–185. doi:10.1097/MCP.0000000000000025
23. Kahnert K, Lucke T, Huber RM, et al. Relationship of hyperlipidemia to comorbidities and lung function in COPD: results of the COSYCONET cohort. PLoS One. 2017;12(5):e0177501. doi:10.1371/journal.pone.0177501
24. Choi JY, Rhee CK. Diagnosis and treatment of early Chronic Obstructive Lung Disease (COPD). J Clin Med. 2020;9(11):3426. doi:10.3390/jcm9113426
25. Celli BR, Agustí A. COPD: time to improve its taxonomy? ERJ Open Res. 2018;4(1):00132–02017. doi:10.1183/23120541.00132-2017
26. Lamprecht B, Soriano JB, Studnicka M, et al. Determinants of underdiagnosis of COPD in national and international surveys. Chest. 2015;148(4):971–985. doi:10.1378/chest.14-2535
27. Soriano JB, Polverino F, Cosio BG. What is early COPD and why is it important? Eur Respir J. 2018;52(6):1801448. doi:10.1183/13993003.01448-2018
28. Morlá M, Busquets X, Pons J, Sauleda J, MacNee W, Agustí AG. Telomere shortening in smokers with and without COPD. Eur Respir J. 2006;27(3):525–528. doi:10.1183/09031936.06.00087005
29. Suzuki M, Sze MA, Campbell JD, et al. The cellular and molecular determinants of emphysematous destruction in COPD. Sci Rep. 2017;7(1):9562. doi:10.1038/s41598-017-10126-2
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.