Back to Journals » Drug Design, Development and Therapy » Volume 19
Characteristics and Efficacy of Warfarin Sodium Tablet Subdivided by 3D Printing Technology: A Retrospective Cohort Study of Patients After Prosthetic Valve Replacement
Authors Lv J ![]() , Fu K, Xiong L, Chen B, Zhan L, Liu J, Lin Z, Yang F, Chen J
, Fu K, Xiong L, Chen B, Zhan L, Liu J, Lin Z, Yang F, Chen J ![]()
Received 27 February 2025
Accepted for publication 2 July 2025
Published 16 July 2025 Volume 2025:19 Pages 6089—6109
DOI https://doi.org/10.2147/DDDT.S525232
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Tamer Ibrahim
Jieqiong Lv,1 Kaixia Fu,2 Lingjuan Xiong,3 Bishan Chen,4 Luchuan Zhan,3 Jiang Liu,3 Zhanyi Lin,5 Fan Yang,2,4 Jisheng Chen4
1Department of Pharmacy, The Second Affiliated Hospital of Shantou University Medical College, Shantou, Guangdong, People’s Republic of China; 2Guangdong Provincial Key Laboratory of Advanced Drug Delivery Systems and Guangdong Provincial Engineering Center of Topical Precise Drug Delivery System, Teaching Laboratory Center, Guangdong Pharmaceutical University, Guangzhou, Guangdong, People’s Republic of China; 3Department of Pharmacy, Guangdong Provincial People’s Hospital (Guangdong Academy of Medical Sciences), Southern Medical University, Guangzhou, Guangdong, People’s Republic of China; 4Key Specialty of Clinical Pharmacy, The First Affiliated Hospital of Guangdong Pharmaceutical University, Guangzhou, Guangdong, People’s Republic of China; 5Guangdong Geriatric Institute, Guangdong Provincial People’s Hospital (Guangdong Academy of Medical Sciences), Southern Medical University, Guangzhou, Guangdong, People’s Republic of China
Correspondence: Fan Yang, Email [email protected] Jisheng Chen, Email [email protected]
Background: Due to the individual-level clinical variation in dosing requirements in commercially available drugs, attaining the objective of clinical individualization and precise drug administration continues to pose a global challenge. Currently, the optimal approach for preparing personalized and precise medications within the clinical setting is unknown.
Aim: This study aimed to explore the effectiveness, safety and satisfaction of three-dimensional (3D) printing technology as a novel subdivision method in providing precise warfarin sodium (WFS) subdivided tablets for patients after prosthetic valve replacement (PVR).
Methods: The optimal formulation, preparation process, parameters, and the relationship between dose and the printing volume were investigated, and the quality of the six specifications of WFS 3D-printed subdivided and pharmacist-split tablets was studied. A retrospective cohort study evaluated the effectiveness, safety, and satisfaction of patients taking WFS 3D-printed subdivided or pharmacist-split tablets.
Results: The hardness, weight variation, drug content, and content uniformity of the six specifications of WFS pharmacist-split tablets did not comply with the European Pharmacopoeia, United States Pharmacopoeia, and Chinese Pharmacopoeia. In contrast, all doses of 3D-printed subdivided tablets met the requirements. The 3D-printed subdivided group showed a significantly higher target international normalized ratio (INR) compliance rate (P< 0.05) and lower over-anticoagulation rate (P< 0.05) than the pharmacist-split group. Also, 66.67% of patients preferred taking 3D-printed subdivided tablets.
Conclusion: 3D printing technology is superior to the traditional subdivision method, as it can improve the effectiveness and safety of patients receiving WFS anticoagulation after PVR.
Keywords: 3D printing technology, warfarin sodium, subdivided tablets, clinical efficacy, a retrospective study
Graphical Abstract:

Introduction
Valvular heart disease (VHD) is a type of heart disease caused by multiple factors, resulting in valve stenosis (and/or) insufficiency, which is the leading cause of cardiovascular morbidity and mortality worldwide.1 According to a population survey, the weighted prevalence of VHD in China is 3.8%, which corresponds to approximately 25 million patients affected by VHD, and this number continues to rise.2 Surgical methods such as heart valve replacement (HVR) or valve repair are the most effective ways for treating moderate to severe VHD. Currently, hundreds of thousands of patients worldwide undergo HVR every year but face a high risk of valve thrombosis and subsequent embolism.3 Therefore, the guidelines recommend that patients undergoing biological valve replacement receive anticoagulant therapy lasting at least 3–6 months, and those undergoing mechanical valve replacement receive lifelong anticoagulant therapy.4
Warfarin is an oral anticoagulant drug characterized by remarkable effectiveness, long anticoagulant time, and low cost. It is widely used for the prevention and treatment of various thromboembolic diseases, such as VHD, atrial fibrillation (AF), deep vein thrombosis (DVT), and pulmonary embolism (PE). New oral anticoagulants (NOACs) have been found to be equal to warfarin in preventing and treating venous thrombosis. However, due to a lack of sufficient clinical evidence, they are strictly prohibited as a substitute for warfarin in patients after HVR, especially for those who have undergone mechanical valve replacement.5 Current guidelines recommend warfarin as the preferred anticoagulant for patients with rheumatic mitral stenosis and those who have undergone mechanical valve replacement.6,7 However, the application of warfarin in real-world clinical settings is associated with three significant limitations. Firstly, its therapeutic window is relatively narrow; even minor dose adjustments can lead to severe bleeding events.8 Secondly, there are significant individual differences in warfarin dosage requirements, which may be as high as 20 times.8,9 Thirdly, in China, only fixed-dose tablets (2.5 mg and 3 mg) are available. Conventional large-scale manufacturing processes do not offer a dose-flexible platform, making it challenging to meet clinical needs.10,11 Therefore, it is very important to realize the accuracy and personalization of warfarin dosage for the safety and effectiveness of patient treatment.
To date, traditional subdivision methods, such as tablet splitting, powder grinding and sub-packaging, or converting solid formulations into liquids, are often used at hospitals to address the limitations of dosage specifications for commercially available drugs.12 However, they also have some disadvantages, affecting therapeutic effects and leading to adverse reactions, including inaccurate dosage, poor stability, microbial contamination, and poor patient compliance. Some researchers have tried subdividing WFS tablets using traditional splitting tools (tablet splitters, hand, and knife); however, the weight, drug content, and content uniformity of the subdivided tablets did not meet the requirements.13,14 A study on splitting 16 commonly used drugs revealed that over one-third of the subdivided tablets did not meet the requirements set by the United States Pharmacopoeia, which increased the medication risk for patients and the workload of medical staff.15 Accordingly, it is of utmost importance to develop a novel subdivision method to achieve the personalized and precise administration of WFS among clinical patients, thus improving their anticoagulant efficacy and safety of patients.
Three-dimensional (3D) printing technology, as an novel subdivision method, possesses considerable potential for the fabrication of precise and personalized doses of WFS tablets within the context of hospital pharmacy settings.16 3D printing is an unrivaled technique that uses computer-aided design (CAD) to produce 3D objects from digital models by fusing, depositing, or solidifying various types of materials layer by layer.17 This technology has been applied in aerospace manufacturing,18 healthcare,19 food,20 and other fields.21 After the approval of 3D-printed levetiracetam orally disintegrating tablets as the first 3D-printed drug formulation by the United States Food and Drug Administration (FDA),22 this technology has become widely used in the pharmaceutical industry.23 Recently, the predominant types of 3D printing technology utilized in the pharmaceutical industry mainly include fused deposition modeling (FDM) printing, inkjet printing (IJP), and semi-solid extrusion (SSE) printing. Among these, FDM 3D printing is only suitable for thermostable active pharmaceutical ingredients and polymers, and it can material waste and low drug resolution in IJP, which limits their development. SSE-printing utilizes pneumatic pressure or piston-driven extrusion as the driving force, featuring high repeatability, room-temperature molding, simple operation, and high precision. Furthermore, it can be used to prepare drugs with complex structures using traditional pharmaceutical excipients, thus having great potential for clinical personalized administration. A previous study showed that SSE-printing technology can produce spironolactone and hydrochlorothiazide subdivided tablets with precise doses, good stability, and personalization.24 Despite the well-documented advantages of 3D printing pharmaceuticals, the clinical potential of this technology has yet to be fully realized.11 Furthermore, as an emerging technology, 3D-printed drugs currently exhibit limited public awareness and face low market acceptance. Therefore, there is a paucity of clinical evidence on the efficacy, safety and satisfaction of 3D printing technology in clinical drug subdivision.
The study aimed to explore the anticoagulation effect of WFS subdivided tablets obtained by 3D printing technology in patients after PVR, providing strong evidence for the effectiveness and safety of 3D printing technology in clinical personalized and accurate drug delivery. The optimal formulation, preparation processes and printing parameters for prepared WFS subdivided tablets were studied, as well as the relationship between dose and model volume, after which a comparison was made on the appearance, harness, weight variation, drug content, content uniformity, related substances, microbial limit, drug release, and long-term stability of six specifications of WFS 3D-printed subdivided tablets and pharmacist-split tablets. In addition, this is the first study that explored the effectiveness, safety, and patient satisfaction of WFS 3D-printed subdivided tablets based on 3D printing technology in patients after PVR.
Materials and Methods
Materials
Commercially available WFS tablets (specification 2.5mg) were purchased from Shanghai Xinyi Pharmaceutical Factory Co., Ltd. WFS reference substance (91.7% purity) was purchased from China Institute for Food and Drug Control. Hydroxypropyl methylcellulose E30 (HPMC-E30) was purchased from Anhui Shanhe Auxiliary Materials Co., Ltd. Anhydrous ethanol solution (pharmaceutical grade) was purchased from Shanghai McLean Biochemical Technology Co., Ltd. All other reagents mentioned in the study were of chromatographic or analytical grade.
Two Subdivision Methods for Pharmacist Splitting and 3D Printing
Pharmacist Splitting Method
In our hospital, the common subdivision method for WFS tablets is the pharmacist splitting method, which is done as follows: based on the patient’s dosage need, the resident pharmacist uses sterilized scissors or a splitter to split the commercially available WFS tablets into the required dosage as much as possible. Next, the subdivided tablets are placed in the drug bag and labeled.
3D Printed Subdivision Method
The preparation process of WFS 3D-printed subdivided tablets in a sterile biological safety cabinet (Suzhou Antai Air Technology Co., Ltd). was carried out, as shown in Figure 1. First, after cleaning and disinfecting the utensils and equipment, the powder of commercial WFS tablets was mixed with an adhesive to make a 3D printing paste with suitable viscosity (the paste can be extruded during 3D printing, the filament will not break when printing, and will not flow out automatically when loaded on the 3D printer).24 Second, the 3D printing paste was loaded into the disposable syringes, and the designed model was imported into printing software in the STL file format; the printing parameters were adjusted, and the SSE-based 3D printer (SHINNOVE-S1, Hangzhou Shiyin Technology Co., Ltd). was started for printing. Finally, the WFS printed tablets were placed in an oven (BGZ-30, Shanghai Boxun Industrial Co., Ltd). to dry, and the qualified 3D printed tablets were stored in brown dosing bottles with labels.
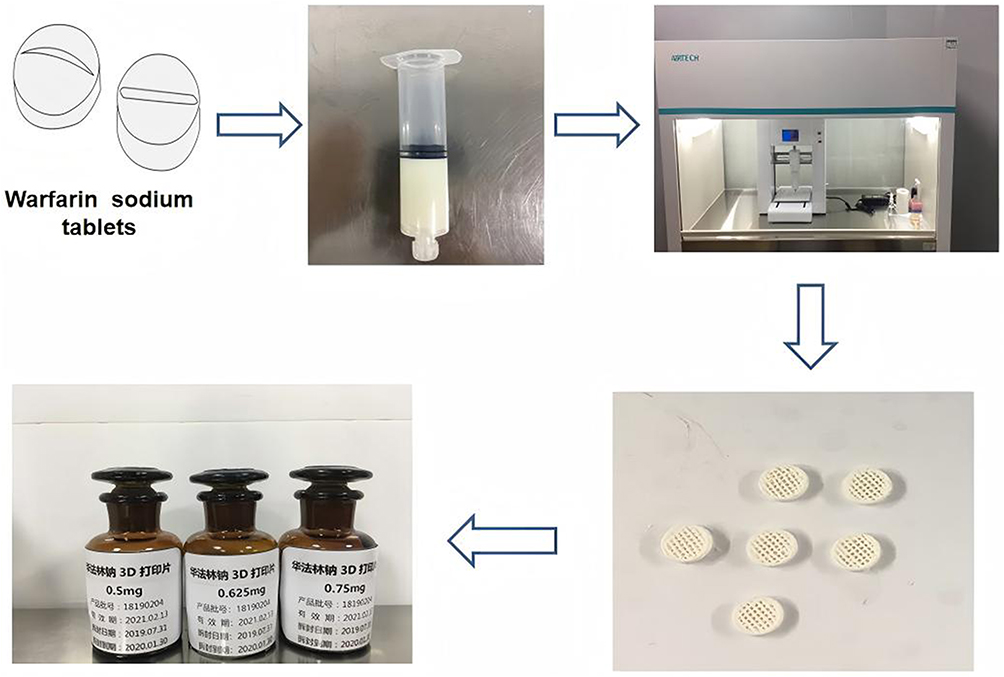 |
Figure 1 The clinical preparation process of WFS 3D-printed subdivided tablets. |
The standard operating procedure (SOP) for 3D-printed subdivided tablets was established. According to the SOP, pharmacists operated 3D printers to prepare WFS subdivided tablets, and qualified WFS 3D-printed subdivided tablets were administered to hospital patients for anticoagulant therapy.
Optimal Formulation and Preparation Process of WFS 3D-Printed Subdivided Tablets
The starting material for SSE is a semi-solid or hydrogel-like material with a specific viscosity. Therefore, several commonly used adhesives were screened to obtain 3D printing paste with appropriate viscosity, including carboxymethyl cellulose sodium (CMC-Na) aqueous solution, polyvinylpyrrolidone K30 (PVP-K30) aqueous solution, polyethylene glycol (PEG-4000) aqueous solution, HPMC-E30 hydroalcoholic gel, and HPMC-E30 powder. The preparation processes of grinding, screening, and mixing were optimized. (Supplementary Material Table 1).
Optimal Parameters of WFS 3D-Printed Subdivided Tablets
In the piston extrusion-based 3D printer, the nozzle diameter, layer height, and printing speed had an influence on the printability of the 3D-printed tablets.24 The investigation of the parameters including the nozzle diameter, layer height, and printing speed were carried out, respectively (Supplementary Material Table 2). The basic parameters were as follows: diameter and layer height of 3D-printed tablets were 3.5 cm and 0.20 mm (80% of the nozzle diameter), printing speed, nozzle diameter, and paste flow rate of the printer were 12 mm/s, 0.26 mm, and 100%, respectively.
Design of Personalized Dose and Appearance for WFS 3D Printed Tablets
Personalized Dose Design
In order to meet the clinical needs of any dose of WFS tablets, the relationship between the theoretical volume and the actual dose of 3D-printed subdivided tablets was explored. The model of 3D-printed subdivided tablets was a cylindrical grid shape. By fixing other parameters and setting the height (h) to half of the radius (r), and then changing the r of the 3D-printed subdivided tablets, a series of volumes of 15.1, 29.5, 45.2, 69.2, 108.8, 139.3, and 208.1 mm3 were obtained, respectively. Then, the weight (W2) of each 3D printed tablet was precisely weighed, and their doses were calculated by using Equation 1. Finally, a linear fitting was performed on the theoretical volume (x) and the actual dose (y) of 3D-printed subdivided tablets.
a: the drug content of commercially available WFS tablets; W1: the average weight of commercially available WFS tablets; w1: the powder weight of commercially available tablets in 3D printed prescriptions; w2: the weight of auxiliary materials in 3D printed prescription; W2: the weight of the 3D-printed subdivided tablet; y: a dose of the 3D-printed subdivided tablet.
Personalized Appearance Design
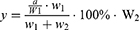
In clinical practice, traditional split tablets are similar in appearance and lack identification, making it difficult to distinguish them and usually causing drug errors by pharmacists, nurses, and patients. Accordingly, there is an urgent need for a simple and highly recognizable subdivided technology to address this issue. In this study, 3D printing technology was used to label the dosage, drug name, and other information of 3D-printed subdivided tablets by designing different model files, such as numbers and alphabetic symbols, and adding edible pigment, as shown in Figure 2.
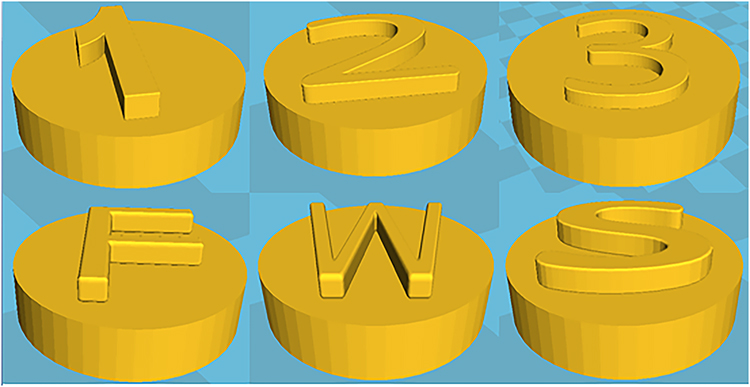 |
Figure 2 Model of 3D-printed subdivided tablets with personalized identification. |
Quality Evaluation of WFS Subdivided Tablets
Appearance
The appearance of tablets can significantly impact patients’ acceptance and medication adherence, affecting the anticoagulant efficacy of warfarin. Therefore, the appearance of pharmacist-split tablets and 3D-printed subdivided tablets of WFS at doses of 0.50, 0.625, 0.75, 1.25, 1.5, and 1.875 mg were observed.
Hardness
Tablets should have enough hardness to ensure that they are not easy to break during packaging and transportation, and ensure the accuracy of dosage. Therefore, the hardness of pharmacist-split tablets and 3D-printed subdivided tablets of WFS at dosages of 0.50, 0.625, 0.75, 1.25, 1.5, and 1.875 mg were observed by tablet hardness tester (YPD-200C, Shanghai Huanghai Drug Testing Instrument Co., Ltd).
Weight Variation
To evaluate the drug weight variation, 30 pharmacist-split tablets and 3D-printed subdivided tablets of WFS in the doses of 0.50, 0.625, 0.75, 1.25, 1.5, and 1.875 mg were randomly selected for precise weighing, and average weight and weight variation of each group was calculated and compared.
Drug Content and Content Uniformity
Based on the requirements of Chinese Pharmacopoeia (Ch. P),25 the content of 0.5, 0.625, 0.75, 1.25, 1.5, 1.875 mg WFS pharmacist-split tablets and 3D-printed subdivided tablets were determined using high-performance liquid chromatography (HPLC), and the drug content uniformity (L) was calculated according to Equation 2. If the L is ≤ 15, the requirement for drug content uniformity is met.
The drug was separated using an Agilent C18 column (5 μm, 150×4.6 mm) at a temperature of 30°C in the HPLC system (Agilent 1260; Agilent Technologies, Santa Clara, CA, USA), which included an ultraviolet (UV) detector and a quaternary pump. The mobile phase consisted of acetonitrile, water and glacial acetic acid in volume ratio of 55:45:1, with a flow rate maintained at 1.0 mL/min. The UV detection was performed at a wavelength 282 nm, and the injection volume was set to 20 μL.

 : the average relative content of the sample with a labeled quantity of 100; S: the relative content standard deviation of the sample with a labeled quantity of 100.
: the average relative content of the sample with a labeled quantity of 100; S: the relative content standard deviation of the sample with a labeled quantity of 100.
Related Substances
The detection of related substances in WFS tablets is essential for ensuring the quality and safety of the drug. According to the Ch. P,25 a HPLC method was employed to analyze the related substances of two groups of subdivided tablets. A test solution at a concentration of 1 mg/mL and an excipient solution at 6 mg/mL were prepared by dissolving WFS powder or cyclodextrin (as an excipient) in a mobile phase composed of 55% acetonitrile, 45% water, and 1% glacial acetic acid. Subsequently, 0.5 mL of the test solution was diluted by a factor of 100 to produce a control solution with a concentration of 5 μg /mL. In accordance with the chromatographic conditions outlined in “Drug Content and Uniformity”, the filtered test solution, control solution, and excipient solution were injected into the liquid chromatograph separately. The total running time for each analysis was set at 25 minutes, with all measurements repeated three times for accuracy. When the cumulative area of all impurity peaks (excluding any excipient peaks) in the chromatogram of the test solution (WFS tablet solution) does not exceed twice (1.0%) that of the main peak in the control solution, it indicates that the drug meets the requirement of the related substances limits.
Microbial Limit
Following the requirement of the plate method in Ch. P,25 the total viable aerobic count, total combined molds and yeasts count, and Escherichia coli counts were detected in two groups of subdivided tablets.
Drug Release Test
In vitro drug release studies25 of the 3D-printed subdivided tablets of WFS were conducted using a 500 mL phosphate buffer solution (pH6.8) as the dissolution medium, with a rotation speed set at 100 rpm and maintained at a temperature of 37 °C± 0.5 °C. Samples of 10 mL were withdrawn at time points of 2, 5, 15, 30, and 45 minutes, with an equal volume of dissolution medium added simultaneously to maintain constant conditions. The samples were subsequently filtered and analyzed using HPLC. All measurements repeated three times.
Accelerated Stability Study and Long-Term Stability Test
To evaluate the storage conditions and stability of WFS pharmacist-split tablets and 3D-printed subdivided tablets, an accelerated stability study alongside a long-term test were conducted at temperatures of 40°C with 75% relative humidity (RH), as well as at 25°C with 60% RH.25 Two groups of subdivided tablets were placed in high-density polyethylene bottles and stored for six months under the following conditions: 40°C ± 2°C /75% ±5% RH, and 25°C ± 2°C /60% ±10% RH, respectively. Three batches were repeated per group, and their stability was evaluated at 0, 1, 2, 3, and 6 months based on their properties and drug content.
Clinical Efficacy and Safety
Study Design and Participants
Study Design
This study was conducted at the Guangdong General Hospital and approved by the Medical Ethics Committee of the Guangdong General Hospital. (The approval number is [2019] XJS01-2). This retrospective study included patients after PVR who received WFS subdivided tablets in the cardiovascular department of a hospital in China between June 2021 and December 2022. Their demographic and clinical data were collected from electronic medical records. Depending on whether the patients received WFS 3D-printed subdivided tablets or pharmacist-split tablets for anticoagulant therapy, they were divided into two groups: the 3D-printed subdivided group and the pharmacist-split group.
Participants
Inclusion criteria were as follows: patients with a normal psychological state and > 18 years old; patients who underwent PVR during hospitalization and received anticoagulant therapy with WFS after surgery. Exclusion criteria: patients with missing basic information; patients with severe chronic diseases, such as abnormal liver and kidney function, thyroid insufficiency, malignant tumor, and mental illness; pregnant women; patients with non-heart valve disease or no PVR; patients taking other oral anticoagulants after surgery, hospitalization days < 7 days or hospitalization days > 60 days, and the dose of WFS tablets not adjusted during hospitalization for various reasons; patients with INR testing less than five times and INR more than three times in one day.
Treatment Regimens
After PVR, the patients were initially treated with low-dose WFS 3D-printed subdivided tablets or pharmacist-split tablets for anticoagulant therapy. The dose of WFS subdivided tablets for patients was adjusted by experienced cardiovascular doctors following patients’ international normalized ratio (INR) value and other clinical examination results. The study was conducted strictly with the Principles for Ethical Review of Drug Clinical Trials and the Declaration of Helsinki.
Evaluation of Anticoagulant Efficacy and Safety
Efficacy Evaluation
According to guidelines and consensuses for warfarin,6,7 the target INR range of warfarin is recommended to be 1.8–3.0 (1.8–2.5 for aortic or mitral valve replacement and 2.0–3.0 for tricuspid valve replacement). The target INR compliance rate of the two groups was calculated as the primary efficacy index. Additionally, statistical comparisons were made on the target INR compliance rate among subgroups categorized by valve replacement location, valve material, and the presence or absence of AF.
Safety Evaluation
As is well known, bleeding is one of the most serious complications of WFS treatment. When the INR of the patient is greater than 3.0, it is considered as overtreatment and the risk of bleeding events increases.26–28 Vitamin K is commonly used to reverse the anticoagulant effect of WFS.26,29 The current guidelines and literatures recommend taking vitamin K to counteract excessive anticoagulant effects in patients treated with warfarin with high INR values who are asymptomatic or have mild bleeding.29–31 Therefore, in this study, the percentage of patients who experienced drug-related bleeding events or received excessive anticoagulant therapy (INR>3) or required vitamin K1 treatment due to potential bleeding was recorded to assess safety differences between the WFS 3D-printed subdivided group and the pharmacist-split group.
Satisfaction Evaluation
Patients’ compliance was crucial to the efficacy and safety of long-term anticoagulant therapy by taking WFS tablets after discharge. Therefore, the satisfaction survey on WFS subdivided tablets was designed for patients and pharmacists to investigate their satisfaction with the use of 3D-printed subdivided tablets and pharmacist-split tablets (See Supplementary Material Figures A1 and A2).
Statistical Analyses
Statistical Product and Service Solutions (SPSS 26.0) software was used for statistical analysis. The measurement data with the normal distribution were expressed as the mean and standard deviation ( ) and compared by independent sample t-test. The count data were expressed as frequency (n) and percentage (%), and the chi-square test was used for comparison. The non-parametric test was used for data with non-normal distribution, and the Mann–Whitney U-test was used for comparison. P value <0.05 represented statistical significance.
) and compared by independent sample t-test. The count data were expressed as frequency (n) and percentage (%), and the chi-square test was used for comparison. The non-parametric test was used for data with non-normal distribution, and the Mann–Whitney U-test was used for comparison. P value <0.05 represented statistical significance.
Results
The Optimal Formulation and Preparation Process of WFS 3D-Printed Subdivided Tablets
The Optimal Formulation of 3D-Printed Subdivided Tablets
The effect of different adhesives on the appearance of 3D-printed tablets is shown in Figure 3. When employing adhesives such as PVP-K30 aqueous solution (Figure 3A), PEG-4000 aqueous solution (Figure 3B), and CMC-Na aqueous solution, the 3D printing paste exhibited a propensity for nozzle blockage and printing filament truncation. After drying, the fragmentation rate of 3D-printed tablets from CMC-Na aqueous solution exceeded 80% (Figure 3C). In contrast, when HPMC-E30 hydroalcoholic gel or a mixture of HPMC-E30 powder and 75% ethanol solution was utilized to prepare the paste, the resulting 3D-printed tablets had good formability and excellent appearance (Figure 3D and E). These findings demonstrated that they were suitable for fabricating subdivided tablets intended for use with SSE-based 3D printer. Notably, HPMC-30 hydroalcoholic gel requires prior preparation and specific storage conditions; however, HPMC-30 powder and 75% ethanol solution were readily available and easy to prepare, aligning more closely with the clinical administration requirements.
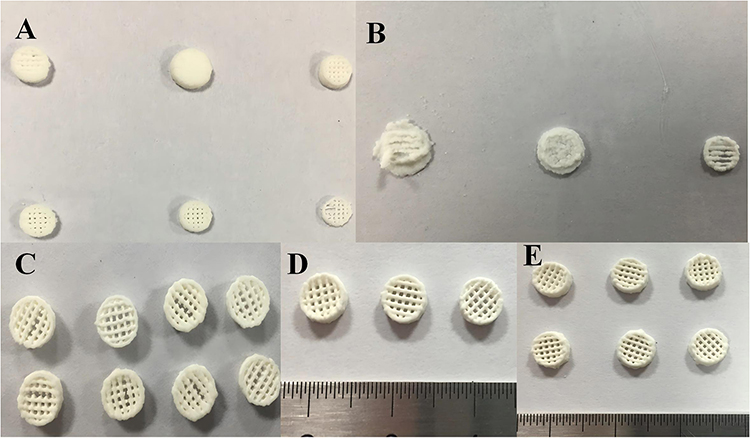 |
Figure 3 Appearance of 3D-printed tablets with different adhesives. (A) PVP-K30 aqueous solution; (B) PEG-4000 aqueous solution; (C) CMC-Na aqueous solution after drying; (D) HPMC-30 hydroalcoholic gel; (E) HPMC-30 powder. |
In short, the optimal formulation for WFS 3D-printed subdivided tablets included the powder of commercially available WFS tablets, HPMC-E30, and 75% ethanol solution.
The Optimal Preparation Process of 3D-Printed Subdivided Tablets
The comparison of various grinding methods and mixing time is presented in Table 1. Two grinding methods were evaluated to obtain powder from commercially available WFS tablets. Compared to manual grinding using a glass mortar, the automatic grinding machine had a shorter time (32.79 min vs 8.44 min) and a lower loss rate (8.13%±0.27% vs 5.23%±0.29%). Due to the small dose of the 3D-printed subdivided tablets, the precise 0.41mm or 0.26mm nozzles were required for printing. It was found that materials with particle sizes of 700μm and 250μm could block the nozzles during the printing process, so the printable particle size of 0.41mm or 0.26mm nozzles was < 120μm. It should be noted that the extrusion weight of 75μm was lighter, resulting in an optimized final particle size of 120μm (120 mesh screen). In addition, compared to the mixing time of 2 minutes, the actual drug content of 3D-printed tablets at both 5 and 10 minutes was consistent with the theoretical drug content rate of 2.95%; the RSD was also small.
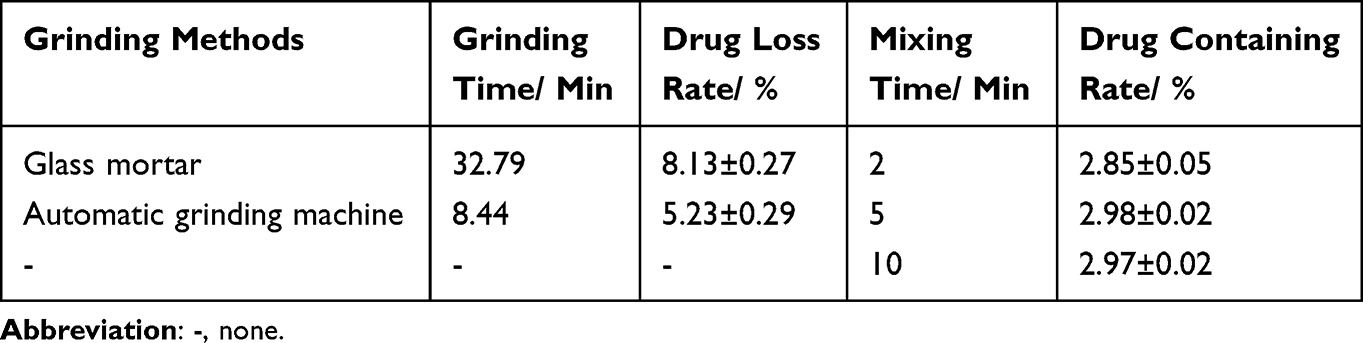 |
Table 1 Comparison of Different Grinding Methods and Mixing Time |
Optimal Parameters of 3D-Printed Subdivided Tablets
The nozzle diameter significantly influences the smoothness of the tablet surface. When the nozzle diameter was 0.60 mm, the printed tablet was relatively rough, with unclear printed lines and patterns, and may even be unable to identify the appearance of the printed products. When the nozzle diameter was 0.41 mm, the printing effect of the product was improved, but it collapsed at the bottom of the product. The best printing results with 3D printed tablets were achieved when the nozzle diameter was 0.26 mm, with smooth lines on the printed tablet and without deposit collapse and rough lines at the bottom (Supplementary Material Figure 2). In the printing process, layer height plays a decisive role in determining whether the material can be smoothly deposited on the printing platform, but also affects the final molding effect of the printed product. A layer height of 0.20 mm could obtain the best printing effect of the product, and the layers of the printed product had better fusion, and there was no sediment collapse and rough lines at the bottom. When the printing speed was 15 mm/s, the printing effect was the best, without uneven discharge and filament breaking.
Based on the results, the optimal printing parameters of 3D-printed subdivided tablets were as follows: nozzle diameter of 0.26 mm, layer height of 0.20 mm, and printing speed of 15 mm/s.
Personalized Dose and Appearance of 3D-Printed Subdivided Tablets
(1) Personalized dose: When the theoretical volume of WFS 3D-printed subdivided tablets ranged from 15.1 mm3 to 208.1 mm3, a good linear correlation was found between the theoretical volume (x) and the actual dose (y). The relationship can be expressed by the equation y=0.0135x+0.1218, with a coefficient of determination (R²) of 0.9991. According to this formula, it is possible to print any desired dose of WFS tablets by adjusting the volume of the 3D printing model.
(2) Personalized appearance: According to the individualized appearance needs of patients, the surface of 3D-printed subdivided tablets was marked with numbers, letter symbols, and colors, which improved the recognition of 3D-printed subdivided tablets and reduced the incidence of medication errors (Figure 4).
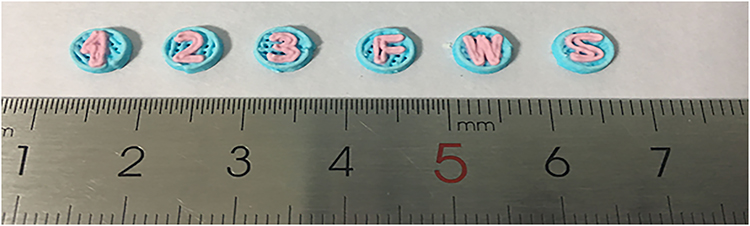 |
Figure 4 3D-printed subdivided tablets with numbers, letters, and colors. |
Quality Evaluation of WFS Subdivided Tablets
Appearance
The appearance of six specifications of WFS pharmacist-split tablets and 3D-printed subdivided tablets is shown in Figure 5. The pharmacist-split tablets had an irregular and rough texture, with instances of the drug detaching, which rendered them difficult to grip. Several doses of the subdivided tablets, such as 1.5 mg and 1.875 mg, were composed of two split parts, leading to a higher incidence of drug loss. In contrast, all dosage specifications of the WFS 3D-printed subdivided tablets had a cylindrical shape that was uniform and smooth.
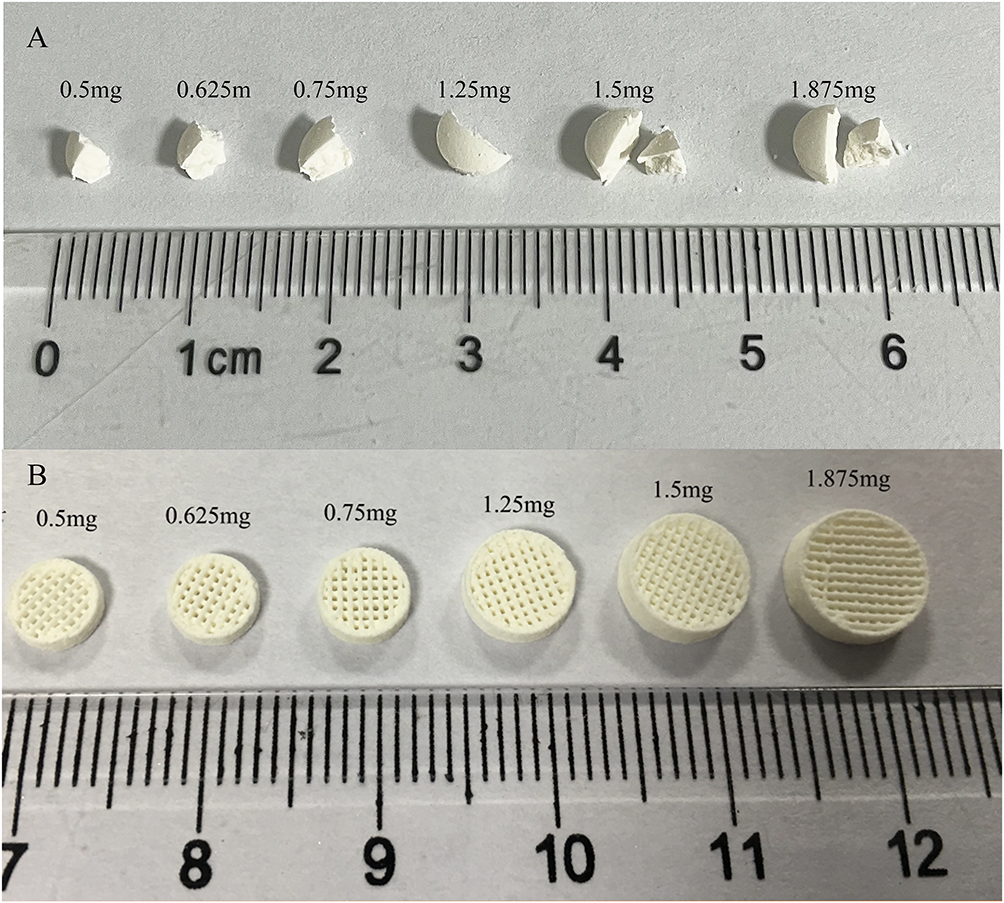 |
Figure 5 Appearance of two groups of subdivided tablets for WFS. (A) Appearance of six specifications of pharmacist-split tablets; (B) Appearance of six specifications of 3D-printed subdivided tablets. |
Hardness
The six specifications of WFS pharmacist-split tablets exhibited irregular shapes, resulting in their hardness being too low to be accurately measured. However, WFS 3D-printed subdivided tablets with dosages of 0.50, 0.625, 0.75, 1.25, 1.5 and 1.875 mg had appropriate hardness (Supplementary Material Table 3), ensuring that they are not easily broken during packaging and transportation.
Weight Variation
The weight variation of six specifications of 3D-printed subdivided tablets and pharmacist-split tablets are shown in Table 2. The weight variation for five specifications of pharmacist-split tablets, including 0.5, 0.625, 0.75, 1.25, and 1.5 mg, which had more than one individual weight, was outside the limit of 85% to 115% of the average weight and did not comply with the requirement of the European Pharmacopoeia 10.5 (Eur. P, 10.5) (European Pharmacopoeia Commission, 10.5). Additionally, the RSD of these weights was > 6%, failing to meet the requirement of the United States Pharmacopoeia (US. P) (United States Pharmacopoeia Commission). Although the weight variation of 1.875 mg pharmacists-split tablet only exceeded the limit of 85% to 115% for one individual, its RSD exceeded 6%, thus failing to comply with the US. P.
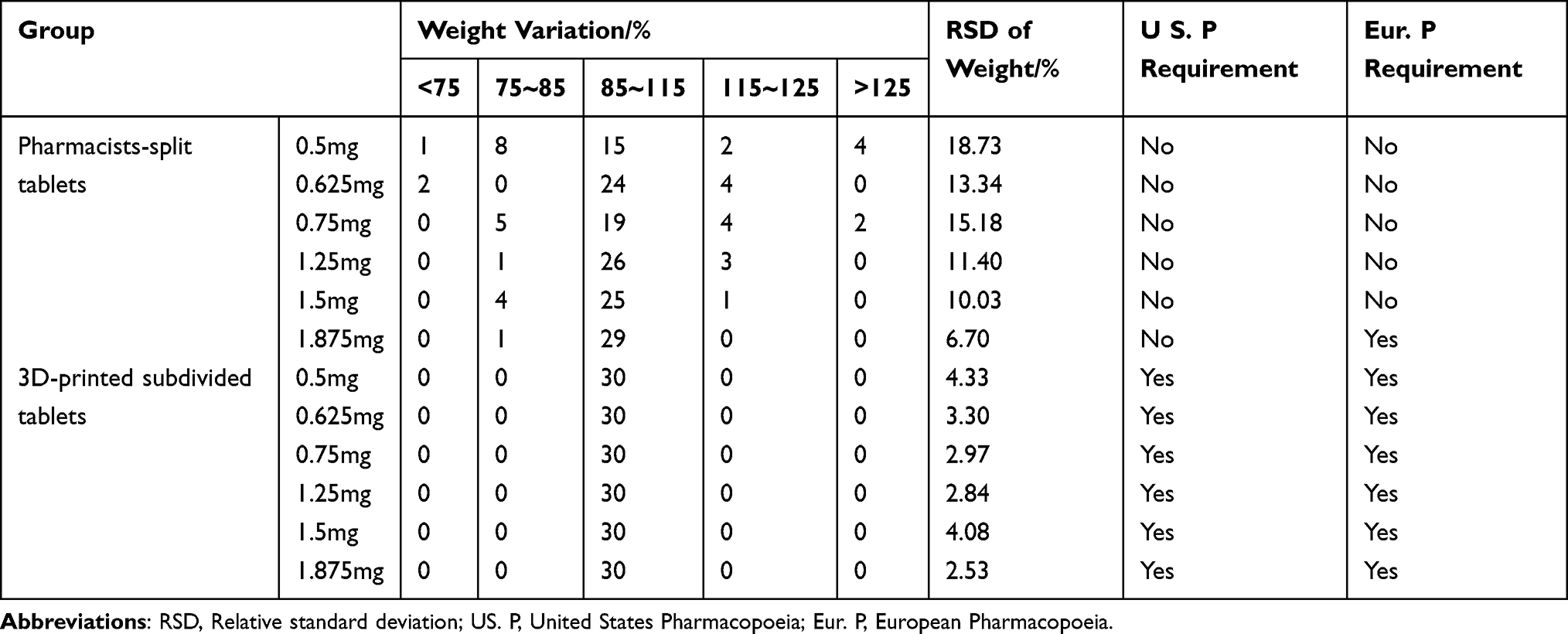 |
Table 2 Comparison of the Weight Variation Between the Two Subdivision Methods of WFS (n=30, |

As the dose of the pharmacist-split tablets decreased, a corresponding increase in RSD values was observed for their weight variation, indicating that the smaller dosages were associated with greater deviations in the weight of subdivided tablets and increased challenges in achieving accurate dosage subdivision. In contrast, six specifications of WFS 3D-printed subdivided tablets were all within±15%, and the value of RSD was < 6%, thus meeting the requirement of the Eur. P and US. P.
Drug Content and Content Uniformity
As shown in Table 3, the drug content of six specifications of 3D printed tablets with doses of 0.5, 0.625, 0.75, 1.25, 1.5, and 1.875 mg were as follows: 103.67±0.69%, 101.31±0.79%, 101.79±0.93%, 99.56±2.53%, 99.41±1.31% and 99.60±1.91%. The corresponding drug content uniformity was 8.02, 8.48, 7.96, 6.01, 4.43, and 4.60, respectively. These results met the requirements of Ch. P for tablet drug content of 97–107% and drug content uniformity < 15, indicating that the dose of 3D-printed subdivided tablets was precise. Conversely, the drug content and drug content uniformity for the six specifications of pharmacist-split tablets far exceeded the requirements of 93–107% and 15, respectively, all of which did not comply with the requirements of the Ch. P, indicating a dosage error in the manual subdivision operation of drugs.
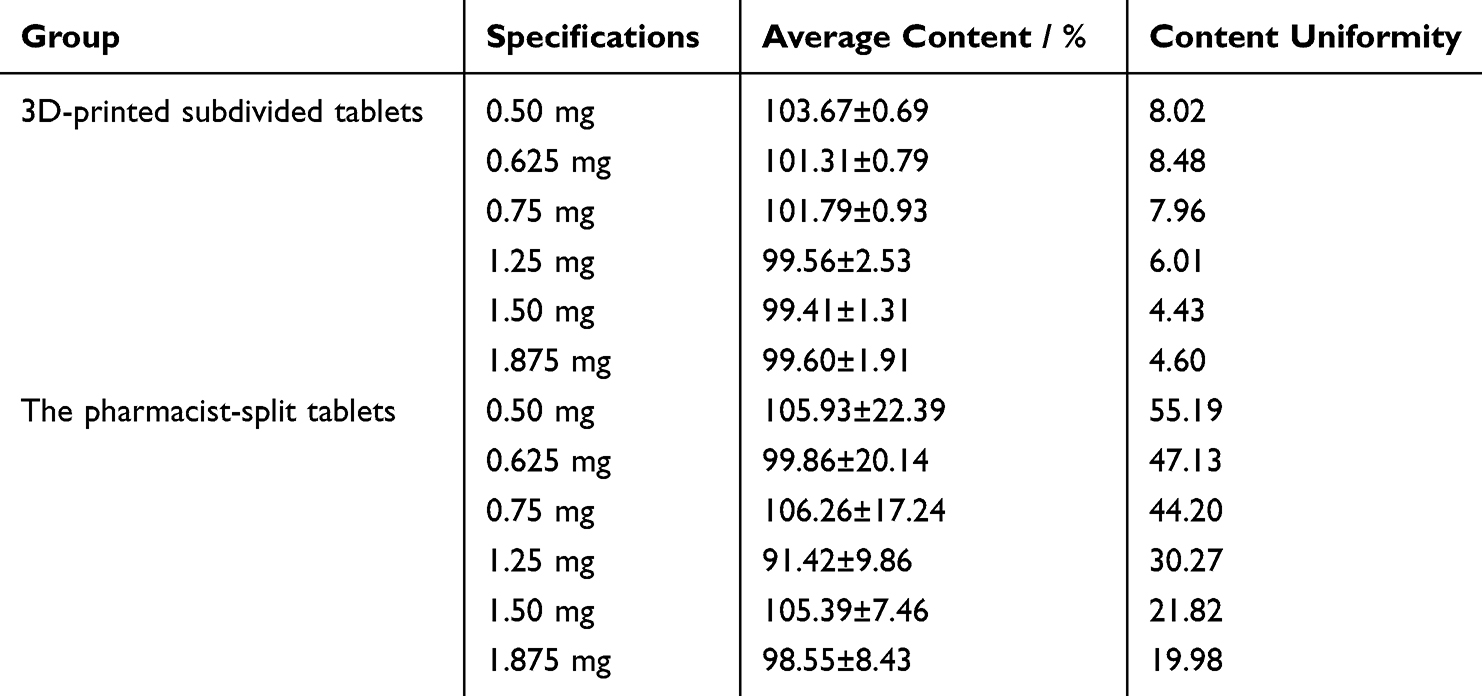 |
Table 3 Drug Content and Content Uniformity in Two Subdivision Methods of WFS (n=10, |

Related Substances
The results indicated that the related substances in six specifications of WFS 3D-printed subdivided tablets and pharmacist-split tablets were below 1.0%, thereby meeting the requirements of Ch.P (Supplementary Material Table 4).
Microbial Limit
As shown in Table 4, the detection values of various microorganisms in WFS 3D-printed subdivided tablets and pharmacist-split tablets were in line with the requirement of the Ch. P.
 |
Table 4 Comparison of Microbial Limit in Two Subdivision Methods of WFS |
Drug Release
The results showed that six specifications of WFS 3D-printed subdivided tablets could be released 101.86%±1.99%, 101.33%±5.88%, 104.18%±1.43%, 100.64%±2.61%, 104.18%±1.43%, 100.64%±2.61% and 98.53%±5.31% at 15 minutes (Supplementary Material Figure 3). Adding adhesive may delay the release of WFS, but it can still achieve the requirement of releasing more than 85% in 15 minutes.
Accelerated Stability Study and Long-Term Stability Test
The drug content and appearance of WFS 3D-printed subdivided tablets, as well as pharmacist-split tablets, remained unchanged after storage for 0, 1, 2, 3, and 6 months under both accelerated stability conditions and long-term stability conditions. All samples met the requirements of the Ch. P, indicating that the tablet properties maintained their stability when stored at 40°C/75% RH. Furthermore, the shelf life could extend up to six months. Our results suggested that the subdivided tablets produced through 3D printing technology and pharmacist splitting method were stable at room temperature, breaking the traditional notion that subdivided tablets using the pharmacist splitting method were unstable (Table 5).
 |
Table 5 Accelerated Stability Study and Long-Term Test Results of Two Subdivision Methods of WFS (n=3, |

Clinical Efficacy Comparison Results
Characteristics of the Patients
A total of 654 patients receiving WFS subdivided tablets for anticoagulant therapy were admitted to our hospital between June 2021 and December 2022. After excluding 435 patients who received anticoagulant therapy following non-PVR surgery, 219 patients who underwent PVR surgery were included. The ratio of the 3D-printed subdivided group to the pharmacist-split group was 119:100. Among them, 52 cases in the 3D-printed subdivided group and 33 cases in the pharmacist-split group were excluded as they failed to meet the standards. Ultimately, 134 patients were enrolled, including the 3D-printed subdivided group (n=67) and the pharmacist-split group (n=67).
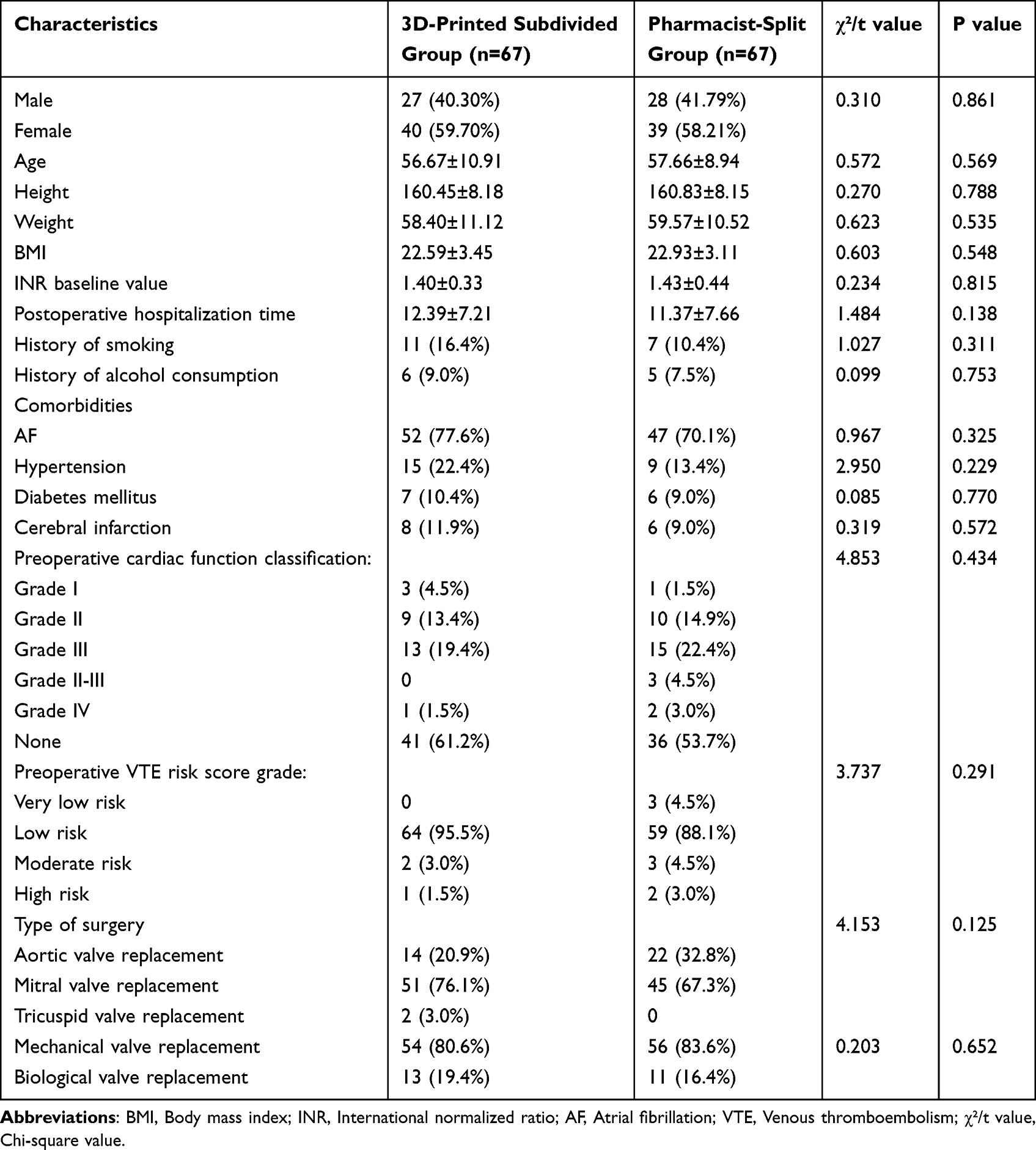
The baseline characteristics of the two groups are shown in Table 6. The average age of the 3D-printed subdivided group and pharmacist-split group was 56.67±10.91 and 57.66±8.94, respectively (P=0.569), and the percentage of male patients in the two groups was 40.30% (27/67) and 41.79% (28/67), respectively (P=0.861). There were also no significant differences in other baseline characteristics between the two groups (P>0.05), indicating that the two groups were comparable. Furthermore, in the two groups, AF and mechanical valve replacement were found in 52 (77.6%) and 47 patients (70.1%), and 54 (80.6%) and 56 patients (83.6%), respectively, indicating that a majority of valve replacement patients required lifelong anticoagulant therapy with WFS.
 |

Efficacy and Safety
Efficacy
As shown in Table 7, the target INR compliance rates of the 3D-printed subdivided and pharmacist-split groups were 33.42% and 28.29%, respectively, with statistically significant differences (P=0.034). There was no significant difference in the number of warfarin dose adjustments between the two groups (3.54±2.01 vs 3.25±2.32, P=0.197). The percentage of patients who reached the target INR for the first time in the 3D-printed subdivided group was higher than in the pharmacist-split group (88.06% vs 83.58%, P=0.458).
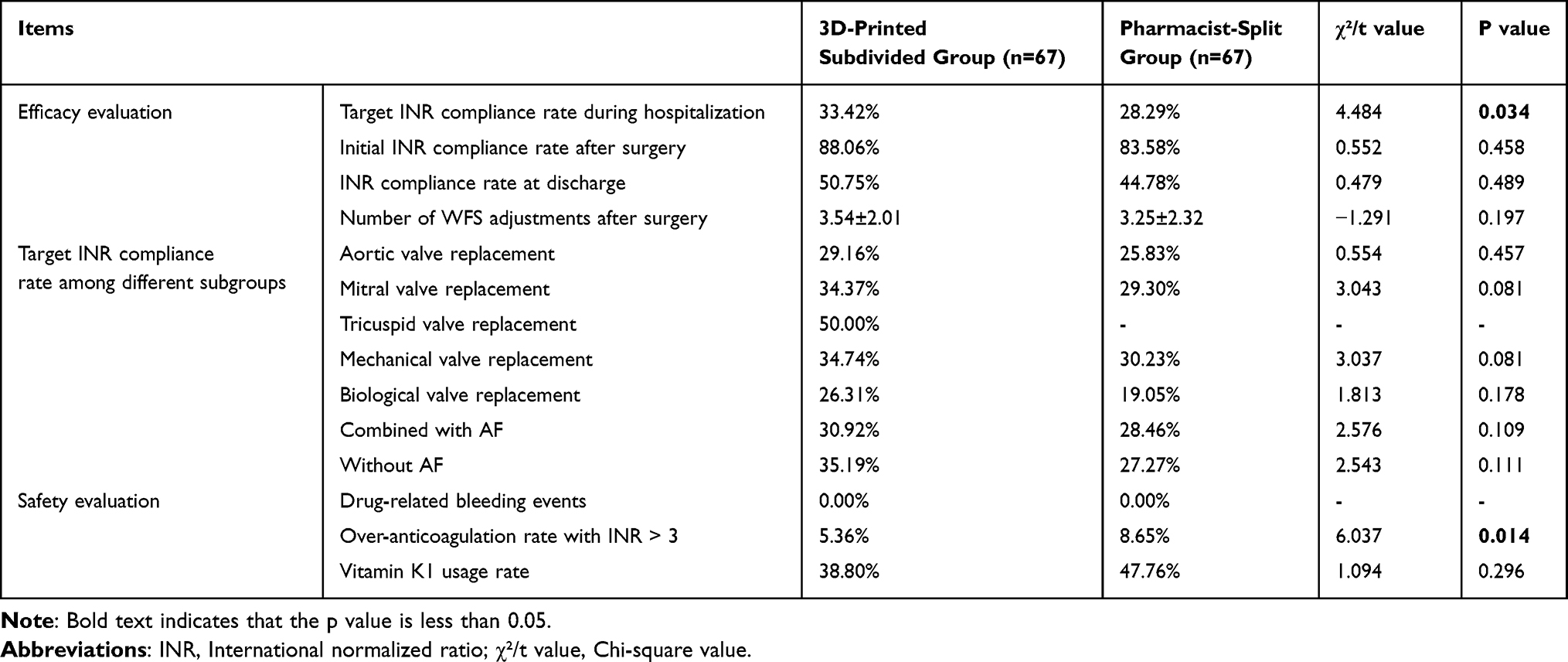 |
Table 7 Comparison of Clinical Efficacy and Safety Between Two Groups ( |

In addition, the target INR compliance rates of patients in different subgroups are shown in Table 7. In the subgroups of valve replacement and mitral valve replacement, the target INR compliance rate in the 3D-printed subdivided group was higher than in the pharmacist-split group (29.16% vs 25.83%, 34.37% vs 29.30%), with no statistically significant differences. However, the number of patients who underwent tricuspid valve replacement was too small to be compared. Moreover, among the subgroup of patients receiving mechanical valve replacement and biological valve replacement, the target INR compliance rate in the 3D-printed subdivided group was higher than in the pharmacist-split group (34.74% vs 30.23%, P=0.081; 26.31% vs 19.05%, P=0.178). Meanwhile, in patients with concomitant AF, the target INR compliance rate of the 3D-printed subdivided group was higher than that of the pharmacist-split group (30.92% vs 28.46%, P=0.109).
Therefore, the results indicated that the clinical efficacy of the WFS subdivision method based on 3D printing technology was superior to that of the pharmacist splitting method, showing better anticoagulant effects in patients after PVR.
Safety
The results showed that neither group of patients experienced drug-related bleeding events. In terms of the ratio of INR > 3, the 3D-printed subdivided group demonstrated a significantly lower incidence compared to the pharmacist-split group (5.36% vs 8.65%, P=0.014). Regarding the usage of vitamin K1, the 3D-printed subdivided group had a lower rate than the pharmacist-split group (38.80% vs 47.76%, P=0.296). In summary, the bleeding risks associated with drug were consistent between the two groups of patients, but compared with the pharmacist-split group, the subdivided group based on 3D printing technology reduced the incidence of excessive anticoagulation and potential bleeding events associated with WFS.
Satisfaction Survey
In order to understand the perceptions of patients and medical staff on the 3D printed subdivision method and traditional subdivision method, we conducted a questionnaire survey involving nine patients who performed tablet subdivision at home and five pharmacists who performed traditional splitting work in the hospital. The completion rate for the questionnaire was 100%; the results are presented in Figure 6. In the past, 57.14% and 42.86% of patients chose to use scissors or manually divide tablets (Figure 6A), respectively. Also, over 50.00% of patients believed these methods had drawbacks such as compromised efficacy of drugs, potential contamination, or difficulty swallowing (Figure 6B). Meanwhile, all pharmacists believed that the traditional splitting method led to inaccurate drug administration and difficulty in identification, and 60.00% (3/5) of pharmacists considered that this process could easily result in drug waste. Among the nine patients surveyed, 66.67% expressed a preference for 3D-printed subdivided tablets (Figure 6C). Within this group of respondents, 75.00%, 62.5%, and 50.00% stated that the dose of 3D printed tablets is easy to swallow, avoids drug waste, and is more accurate, respectively (Figure 6D). The five pharmacists considered that 3D printing technology has dramatically reduced their workload, minimized pollution risks, avoided drug waste, etc. Overall, compared to traditional splitting methods, the customizable and personalized 3D printing subdivided technology was recognized by patients and pharmacists.
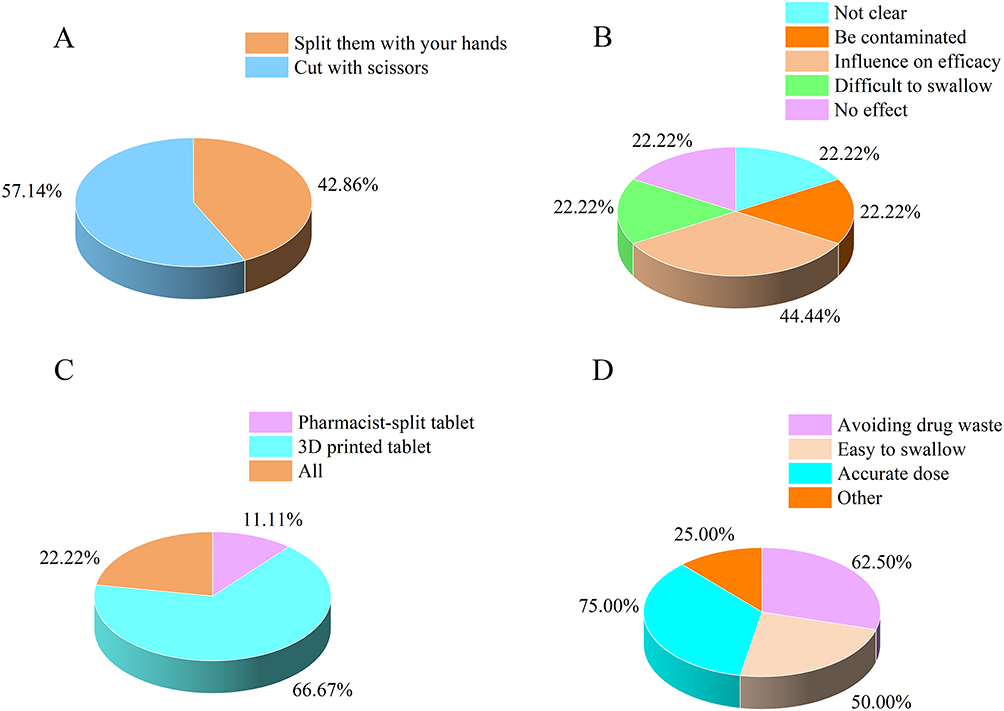 |
Figure 6 The satisfaction of two subdivision methods. (A) The selection of traditional splitting methods; (B) Patients’ satisfaction with traditional splitting methods; (C) Willingness to take two groups of subdivided tablets; (D) Opinions on 3D printed tablets. |
Discussion
Global medicine is advancing towards the era of precision medicine, characterized by providing personalized and precise drugs for every patient, thus achieving the optimal therapeutic effect and the lowest toxic side effects.32–36 However, the limited specifications of currently available drugs have raised a common issue of dose subdivision worldwide.15,37 In Swedish pharmacy, over 125,000 out of 600,000 dispensed prescriptions require a dose subdivision within a month.38 Insufficient or excessive dosage of the subdivided tablets may lead to decreased therapeutic efficacy or increased toxic effects.39 Moreover, the growing demand for subdivided tablets with varying doses poses a significant challenge to pharmacist operation and patient compliance.
Herein, we used the 2.5 mg commercially available WFS tablets as model drugs. Six specifications of 1/5, 1/4, 3/10, 1/2, 3/5, and 3/4 tablets of these model drugs were subdivided using 3D printing technology and the pharmacist-split method, and their quality was compared. The RSD for weight, drug content, and content uniformity among the six specifications of pharmacist-split tablets were 6.70–18.73, 91.42%±9.86%-105.93%±22.39%, and 14.04–55.19, respectively. These results did not meet the US. P (with an RSD requirement of < 6), the Eur. P (where the part weight must not exceed 85–115% of the average weight), and the Ch. P (requires the content uniformity to be < 15, with drug content ranging from 93.00% to 107.00%). Conversely, all six specifications of the 3D-printed subdivided tablets met the requirements. The results indicated that the dose of 3D-printed subdivided tablets was more accurate than pharmacist-split tablets. In addition, the population administered with WFS 3D-printed tablets exhibited a significantly higher target INR compliance rate and a lower incidence of INR >3 events for those treated with WFS pharmacist-split tablets (P<0.05). Our comprehensive results convincingly demonstrated the efficacy and safety of 3D printing technology in the personalized and precise administration of WFS in clinical practice.
A 3D printing technology is an innovative additive manufacturing technology characterized by high precision, efficiency, and customizability, leading to rapid pharmaceutical development.40 FDM and SSE are the most commonly used types of extrusion 3D printing technology in drug development. Among them, FDM 3D printing requires obtaining thermoplastic polymers and drug-loaded filaments of drugs and/or excipients first, then using heating nozzles to print objects through processes such as heating, melting, and extrusion of the drug-loaded filaments. However, this technology is unsuitable for thermally unstable drugs and excipients.41 In contrast, SSE 3D printing is a material extrusion technology that extrudes high-viscosity liquid or semi-solid materials (gels, pastes, etc). from disposable syringes at room temperature and stacks them layer by layer to create objects of any size and shape.42,43 The prepared WFS subdivided tablets exhibited personalized, precise dosage and digital/color identification. Previous study have reported that SSE 3D printing can produce isoleucine chewable tablets in various flavors and colors within hospital pharmacies, which were well-received by pediatric patients.44 Moreover, 3D printer are portable, small, and easy to use, which makes them ideal for usage in hospital wards, in-patient pharmacies, specialist clinics, and community pharmacies.45 Consequently, SSE 3D printing technology may be the most suitable for producing personalized drugs, demonstrating great potential for personalized and precise drug administration in clinical applications.
In traditional subdivision methods, a certain amount of excipients is usually required when the dosage is small. For SSE 3D printing technology, it is crucial to select materials with a certain viscosity of semi-solid slurry.46 HPMC, a cellulose-based polymer, is commonly used as a binder, diluent, and sustained-release agent in pharmaceuticals and food products.47 Compared to other 3D printing materials, HPMC has good solubility and low toxicity.45 When employing a mixture of HPMC-E30 and 75% ethanol as excipients, the water molecules from the ethanol solution interact with HPMC-E30 to form a wetting film on the surface of the 3D-printed slurry. This film effectively encapsulates other particles while ethanol inhibits excessive hydration of HPMC, making the 3D printing slurry smooth and achieving appropriate viscosity.24 This characteristic also explains why HPMC hydroalcoholic gels exhibit favorable rheological properties conducive to slurry extrusion.48 Lu et al49 demonstrated that a 3D printing slurry prepared from HPMC hydro-alcohol gel and levothyroxine sodium tablets obtained good printability in SSE 3D printer. Additionally, the particle size of the material directly affected the smooth extrusion of the 3D printing slurry during preparation. Our findings indicated that when using printing nozzles with diameters of 0.41 mm or 0.26 mm, the particle size of the 3D printing materials should not exceed 120 μm. Furthermore, the grinding method and mixing time affected drug uniformity and material loss. When an automatic grinder was used to grind commercially available tablets and sieve them through a 120-mesh screen (particle size 120 μ m), a 3D printing slurry with uniform and suitable particle size could be obtained.
For 3D printing technology, the parameters of 3D printed models are controlled by computers to meet the personalized dosage needs of clinical drugs. Nevertheless, blindly adjusting printed parameters every time to gain specific doses of 3D-printed subdivided tablets can substantially waste manpower and material resources. Therefore, by fixing other parameters and varying the radius of the printing models, we obtained a linear formula for the actual dose of the 3D printed tablets and the volume of the printed model, with a fitting degree of up to 0.9991, meeting the clinical need for WFS subdivided tablets in any dose. Additionally, we designed innovative printed models and incorporated edible pigments to print tablets in various shapes and colors. This customization meets patients’ individual preferences and enhances the recognizability of subdivided tablets while reducing potential dosing errors.46,50
In this study, the clinical anticoagulant efficacy and safety of patients in the 3D-printed subdivided group were superior to those in the pharmacist-split group for two reasons. First, many factors can influence the accuracy of drug subdivision when pharmacists perform splitting operations,51,52 including the characteristics of the tablets (size, shape, hardness, structure, etc), the equipment used for tablet splitting, and the physical condition of pharmacists. Our results showed that the tablets split by pharmacists did not meet the pharmacopoeia requirements, while the quality of 3D-printed subdivided tablets was higher than that of pharmacist-split tablets. Second, compared with other subdivision specifications, one-quarter and one-half doses of tablets are relatively easy to obtain by scissors or splitter in clinic, so pharmacists usually prefer to prepare the subdivided tablets of these two doses in advance in the pharmacist-split group. This prompts physicians to prescribe medications in half-dose increments, so some patients in the pharmacist-split group had a higher incidence of INR exceeding the treatment range due to receiving excessive doses. Because of the relatively narrow INR window of WFS, its anticoagulation effect is directly related to dose. An insufficient dosage of WFS can easily lead to thrombosis, while an excessive dosage may result in major bleeding events.53 Bleeding is the most significant adverse effect associated with WFS and is directly related to the level of INR.54 It has been reported that more than 65,000 patients are treated in US emergency departments annually for WFS-related bleeding.55 Vitamin K is a commonly used first-line reversal agent for WFS therapy in patients presenting with a supra therapeutic INR with or without significant bleeding.26 Therefore, in the pharmacist-split group, the incidence of excessive anticoagulation and the usage of vitamin K1 were higher than that 3D printed group due to the unprecise dosage. On the contrary, 3D printing technology allows any desired dose to be tailored to individual patient needs, enabling more personalized and precise dosing within the 3D-printed subdivided group.
This study found that patients had a higher acceptance of 3D-printed subdivided tablets than pharmacist-split tablets, which can be attributed to several advantages of 3D-printed subdivided tablets, including good appearance, ease of swallowing, elimination of the need for patient operation, and potential for personalization and customization.24 These features genuinely enable each patient to experience personalized and precise medical services. Furthermore, pharmacists strongly support using 3D-printing subdivided technology instead of pharmacist splitting method, considering that the 3D printing technology is easy to operate, highly automated and greatly reduces their workload.56
This study also has some limitations. First, the study only focused on patients who underwent artificial heart valve replacement surgery and did not include individuals receiving anticoagulant therapy following non-valve replacement surgery. Second, owing to the limited sample size, the data for some subgroups were insufficient for statistical analysis. Finally, as this was a retrospective study, further prospective, large-sample, randomized studies are necessary to validate these findings.
Currently, we have established the SOP for 3D printed subdivided tablets in hospitals, trained a group of pharmacists proficient in operating 3D printers, and constructed a 3D printed dispensing center for subdivided tablets in the hospital pharmacy. This center provides accurate and personalized 3D-printed subdivided tablets for all inpatients with subdivided drug needs, earning the favor of patients, physicians, and pharmacists. In the future, 3D printing technology, as a highly precise subdivision method, is expected to completely replace traditional technologies. Furthermore, it will trigger a huge transformation in clinical medication practice and the pharmaceutical industry, leading to the arrival of a new era of digital pharmacies.
Conclusion
The WFS subdivided tablets produced through 3D printing technology have the characteristics of accurate dosage, stable quality, high identifiability and good compliance. In addition, compared with the tablets splitting by pharmacists, they improve the effectiveness, safety and satisfaction for patients after PVR. All these prove that the subdivision method based on 3D printing technology can completely replace the traditional subdivision method, realizing accurate and personalized medication for patients in hospital. We expect that 3D printing technology will play an inestimable role in achieving global precision medicine.
Data Sharing Statement
The data supporting the study findings are available from the corresponding author (Professor Fan Yang) upon reasonable request.
Ethics Statement
This retrospective study was approved by the Medical Ethics Committee of the Guangdong General Hospital. (The approval number is [2019] XJS01-2). Given the retrospective nature of the study and the use of de-identified patient data, the requirement for informed consent was waived by the Medical Ethics Committee. The use of personal data was approved by the Medical Ethics Committee of the Guangdong General Hospital ensuring that all data was anonymized and securely stored.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas, took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Medical Service and Security Capacity Improvement Subsidy Fund of the Central Government (grant numbers Z155080000004), the Special Projects in Key Areas of Artificial Intelligence of Guangdong Provincial Department of Education (grant numbers 2019KZDZX1019), Guangzhou People’s Livelihood Science and Technology Research Program (grant numbers 201803010096) and Guangdong Province Higher Education Innovation Team (grant numbers 2024KCXTD035).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Aluru JS, Barsouk A, Saginala K, Rawla P, Barsouk A. Valvular heart disease epidemiology. Med Sci. 2022;10(2):32.
2. Yang Y, Wang Z, Chen Z, et al. Current status and etiology of valvular heart disease in China: a population-based survey. BMC Cardiovasc Disord. 2021;21. doi:10.1186/s12872-021-02154-8
3. Peters AS, Duggan JP, Trachiotis GD, Antevil JL. Epidemiology of valvular heart disease. Surg Clin North Am. 2022;102(3):517–528. doi:10.1016/j.suc.2022.01.008
4. Whitlock RP, Sun JC, Fremes SE, Rubens FD, Teoh KH. Antithrombotic and thrombolytic therapy for valvular disease: antithrombotic therapy and prevention of thrombosis, 9th ed: American college of chest physicians evidence-based clinical practice guidelines. Chest. 2012;141(2 Suppl):e576S–e600S. doi:10.1378/chest.11-2305
5. Eikelboom JW, Connolly SJ, Brueckmann M, et al. Dabigatran versus warfarin in patients with mechanical heart valves. N Engl J Med. 2013;369:1206–1214. doi:10.1056/NEJMoa1300615
6. Alec V, Friedhelm B, Fabien P, et al. 2021 ESC/EACTS guidelines for the management of valvular heart disease: developed by the task force for the management of valvular heart disease of the European Society Of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Revista espanola de cardiologia. 2022;75. doi:10.1016/j.rec.2022.05.006
7. Otto CM, Nishimura RA, Bonow RO. 2020 ACC/AHA guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Thoracic Cardiovasc Surg. 2021;162:e183–e353. doi:10.1016/j.jtcvs.2021.04.002
8. Lam MP, Cheung BM. The pharmacogenetics of the response to warfarin in Chinese. Br J Clin Pharmacol. 2012;73(3):340–347. doi:10.1111/j.1365-2125.2011.04097.x
9. Ma W, Li H, Dong L, et al. Warfarin maintenance dose prediction for Chinese after heart valve replacement by a feedforward neural network with equal stratified sampling. Sci Rep. 2021;11(1):13778. doi:10.1038/s41598-021-93317-2
10. Öblom H, Sjöholm E, Rautamo M, Sandler N. Towards printed pediatric medicines in hospital pharmacies: comparison of 2D and 3D-printed orodispersible warfarin films with conventional oral powders in unit dose sachets. Pharmaceutics. 2019;11:334. doi:10.3390/pharmaceutics11070334
11. Seoane-Viaño I, Trenfield SJ, Basit AW, Goyanes A. Translating 3D printed pharmaceuticals: from hype to real-world clinical applications. Adv Drug Deliv Rev. 2021;174:553–575. doi:10.1016/j.addr.2021.05.003
12. Lopez FL, Ernest TB, Tuleu C, Gul MO. Formulation approaches to pediatric oral drug delivery: benefits and limitations of current platforms. Expert Opin Drug Deliv. 2015;12(11):1727–1740. doi:10.1517/17425247.2015.1060218
13. Hill SW, Varker AS, Karlage K, Myrdal PB. Analysis of drug content and weight uniformity for half-tablets of 6 commonly split medications. J Manag Care Pharm. 2009;15(3):253–261. doi:10.18553/jmcp.2009.15.3.253
14. Isbera M, Abbood A, Ibrahim W. Weight and content uniformity of warfarin sodium half tablets. Res J Pharm Technol. 2016;9:215–218. doi:10.5958/0974-360X.2016.00039.1
15. Helmy SA. Tablet splitting: is it worthwhile? Analysis of drug content and weight uniformity for half tablets of 16 commonly used medications in the outpatient setting. J Managed Care Specialty Pharm. 2015;21:76–86. doi:10.18553/jmcp.2015.21.1.76
16. Sandler N, Preis M. Printed drug-delivery systems for improved patient treatment. Trends Pharmacol Sci. 2016;37(37):1070–1080. doi:10.1016/j.tips.2016.10.002
17. Ryan V, Purab S, Sahil S, et al. 3D printing in the pharmaceutical sector: Advances and evidences. Sensors Int. 2022;3:1–11.
18. Tuli NT, Khatun S, Rashid AB. Unlocking the future of precision manufacturing: a comprehensive exploration of 3D printing with fiber-reinforced composites in aerospace, automotive, medical, and consumer industries. Heliyon. 2024;10:e27328. doi:10.1016/j.heliyon.2024.e27328
19. Gu Z, Fu J, Lin H, He Y. Development of 3D bioprinting: From printing methods to biomedical applications. Asian J Pharm Sci. 2020;15(5):529–557. doi:10.1016/j.ajps.2019.11.003
20. Liu Z, Zhang M, Bhandari B, et al. 3D printing: printing precision and application in food sector. Trends Food Sci Technol. 2017;69:83–94. doi:10.1016/j.tifs.2017.08.018
21. Sovetova M, Calautit JK. Thermal and energy efficiency in 3D-printed buildings: review of geometric design, materials and printing processes. Energy Buildings. 2024;323. doi:10.1016/j.enbuild.2024.114731
22. Drugs.Com. FDA approves spritam (levetiracetam) as the first 3D printed drug product. 2015. Available from: https://www.drugs.com/newdrugs/fda-approves-spritam-levetiracetam-first-3d-printedproduct-4240.html.
23. Siyawamwaya M, du Toit LC, Kumar P, Choonara YE, Kondiah PPPD, Pillay V. 3D printed, controlled release, tritherapeutic tablet matrix for advanced anti-HIV-1 drug delivery. Eur J Pharm Biopharm. 2019;138:99–110. doi:10.1016/j.ejpb.2018.04.007
24. Zheng Z, Lv J, Yang W, et al. Preparation and application of subdivided tablets using 3D printing for precise hospital dispensing. Eur J Pharm Sci. 2020;149:105293. doi:10.1016/j.ejps.2020.105293
25. State Pharmacopoeia Commission. Pharmacopoeia of the People’S Republic of China: S. Beijing: China Medical Science and Technology Press; 2020.
26. Van Berkel MA, Crannage AJ, Murphy JA. Evaluation of education on the appropriate use of vitamin k in warfarin reversal in adult inpatients. Hosp Pharm. 2013;48(8):662–667. doi:10.1310/hpj4808-662
27. Odén A, Fahlén M. Oral anticoagulation and risk of death: a medical record linkage study. BMJ. 2002;325(7372):1073–1075. doi:10.1136/bmj.325.7372.1073
28. Acar J, Iung B, Boissel JP, et al. AREVA: multicenter randomized comparison of low-dose versus standard-dose anticoagulation in patients with mechanical prosthetic heart valves. Circulation. 1996;94(9):2107–2112. doi:10.1161/01.CIR.94.9.2107
29. Tsu LV, Dienes JE, Dager WE. Vitamin K dosing to reverse warfarin based on INR, route of administration, and home warfarin dose in the acute/critical care setting. Ann Pharmacother. 2012;46(12):1617–1626. doi:10.1345/aph.1R497
30. Kampouraki E, Avery PJ, Wynne H, et al. Assessment of the efficacy of a novel tailored vitamin K dosing regimen in lowering the International Normalised Ratio in over-anticoagulated patients: a randomised clinical trial. Br J Haematol. 2017;178(5):800–809. doi:10.1111/bjh.14777
31. Holbrook A, Schulman S, Witt DM, et al. Evidence-based management of anticoagulant therapy: American College of Chest Physicians evidence-based clinical practice guidelines (9th edition). Chest. 2012;141(2 Suppl):e152S–e184S. doi:10.1378/chest.11-2295
32. Denny JC, Collins FS. Precision medicine in 2030-seven ways to transform healthcare. Cell. 2021;184:1415–1419. doi:10.1016/j.cell.2021.01.015
33. Schaffhausen J. What Precisely Is Precision Medicine? Trends Pharmacol Sci. 2017;38:1–2. doi:10.1016/j.tips.2016.11.004
34. Sadee W, Wang D, Hartmann K, Toland AE. Pharmacogenomics: Driving personalized medicine. Pharmacol Rev. 2023;75(4):789–814. doi:10.1124/pharmrev.122.000810
35. Wahida A, Buschhorn L, Fröhling S, et al. The coming decade in precision oncology: six riddles. Nat Rev Cancer. 2023;23:43–54. doi:10.1038/s41568-022-00529-3
36. Sarhangi N, Hajjari S, Heydari SF, Ganjizadeh M, Rouhollah F, Hasanzad M. Breast cancer in the era of precision medicine. Mol Biol Rep. 2022;49(10):10023–10037. doi:10.1007/s11033-022-07571-2
37. Olgac S, Yilmaz Usta D, Incecayir T. Comparison of tablet splitting techniques for dosing accuracy of nebivolol tablets: hand splitting versus tablet cutter and knife. Saudi Pharm J. 2021;29:1486–1491. doi:10.1016/j.jsps.2021.11.005
38. Berg C, Ekedahl A. Dosages involving splitting tablets: common but unnecessary? J Pharmaceut Health Serv Res. 2010;1:137–141. doi:10.1111/j.1759-8893.2010.00020.x
39. Pirmohamed M, James S, Meakin S, et al. Adverse drug reactions as cause of admission to hospital: prospective analysis of 18 820 patients. BMJ. 2004;329:15–19. doi:10.1136/bmj.329.7456.15
40. Aguilar-de-Leyva Á, Casas M, Ferrero C, Linares V, Caraballo I. 3D printing direct powder extrusion in the production of drug delivery systems: state of the art and future perspectives. Pharmaceutics. 2024;16(4):437. doi:10.3390/pharmaceutics16040437
41. Honghe W, Kumar VS, Suresh B, et al. Preparation of core-shell controlled release tablets using direct powder extrusion 3D printing techniques. J Drug Delivery Sci Technol. 2023;88:104896.
42. Eduardo D, Lucía R, Jie OJ, et al. Integrating pressure sensor control into semi-solid extrusion 3D printing to optimize medicine manufacturing. Int J Pharmaceut. 2022;4. doi:10.1016/j.ijpx.2022.100133
43. Seoane-Viaño I, Januskaite P, Alvarez-Lorenzo C, Basit AW, Goyanes A. Semi-solid extrusion 3D printing in drug delivery and biomedicine: personalised solutions for healthcare challenges. J Control Release. 2021;332:367–389. doi:10.1016/j.jconrel.2021.02.027
44. Goyanes A, M MC, Umerji A, et al. Automated therapy preparation of isoleucine formulations using 3D printing for the treatment of MSUD: first single-centre, prospective, crossover study in patients. Int J Pharm. 2019;567:118497. doi:10.1016/j.ijpharm.2019.118497
45. Huanbutta K, Burapapadh K, Sriamornsak P, Sangnim T. Practical application of 3D printing for pharmaceuticals in hospitals and pharmacies. Pharmaceutics. 2023;15(7):1877. doi:10.3390/pharmaceutics15071877
46. Rautamo M, Kvarnström K, Sivén M, Airaksinen M, Lahdenne P, Sandler N. Benefits and prerequisites associated with the adoption of oral 3D-printed medicines for pediatric patients: a focus group study among healthcare professionals. Pharmaceutics. 2020;12(3):229. doi:10.3390/pharmaceutics12030229
47. Guarve K, Kriplani P. HPMC- A marvel polymer for pharmaceutical industry-patent review. Recent Adv Drug Deliv Formul. 2021;15:46–58. doi:10.2174/1872211314666210604120619
48. Aina M, Baillon F, Sescousse R, et al. Evaluation of the printability of agar and hydroxypropyl methylcellulose gels as gummy formulations: insights from rheological properties. Int J Pharm. 2024;654:123937. doi:10.1016/j.ijpharm.2024.123937
49. Lu L, Kaixia F, Shijie H, et al. Improving the quality and clinical efficacy of subdivided levothyroxine sodium tablets by 3D printing technology. Journal of Drug Delivery Science and Technology. 2023;89. doi:10.1016/j.jddst.2023.105000
50. Tan YJN, Yong WP, Kochhar JS, et al. On-demand fully customizable drug tablets via 3D printing technology for personalized medicine. J Control Release. 2020;322:42–52. doi:10.1016/j.jconrel.2020.02.046
51. Tahaineh LM, Gharaibeh SF. Tablet splitting and weight uniformity of half-tablets of 4 medications in pharmacy practice. J Pharm Pract. 2012;25:471–476. doi:10.1177/0897190012442716
52. Elliott I, Mayxay M, Yeuichaixong S, Lee SJ, Newton PN. The practice and clinical implications of tablet splitting in international health. Trop Med Int Health. 2014;19(7):754–760. doi:10.1111/tmi.12309
53. Yeh CH, Fredenburgh JC, Weitz JI. Oral direct factor Xa inhibitors. Circ Res. 2012;111(8):1069–1078. doi:10.1161/CIRCRESAHA.112.276741
54. Harter K, Levine M, Henderson SO. Anticoagulation drug therapy: a review. West J Emerg Med. 2015;16(1):11–17. Epub 2015 Jan 12. doi:10.5811/westjem.2014.12.22933
55. Shehab N, Sperling LS, Kegler SR, Budnitz DS. National estimates of emergency department visits for hemorrhage-related adverse events from clopidogrel plus aspirin and from warfarin. Arch Intern Med. 2010;170(21):1926–1933. doi:10.1001/archinternmed.2010.407
56. Vaz VM, Kumar L. 3D printing as a promising tool in personalized medicine. AAPS PharmSciTech. 2021;22:49. doi:10.1208/s12249-020-01905-8
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.