")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 13
Changes in High-Density Lipoprotein Cholesterol Levels in Relation to Coffee Consumption Among Taiwanese Adults
Authors Chang HC, Nfor ON, Ho CC, Chen PH, Kung YY, Hsu SY, Tantoh DM, Liaw YC, Hsieh CF, Liaw YP
Received 10 August 2020
Accepted for publication 29 September 2020
Published 2 November 2020 Volume 2020:13 Pages 1427—1432
DOI https://doi.org/10.2147/JMDH.S276395
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Huan-Cheng Chang,1,2 Oswald Ndi Nfor,3 Chien-Chang Ho,4,5 Pei-Hsin Chen,3 Ya-Yu Kung,6 Shu-Yi Hsu,3 Disline Manli Tantoh,3,7 Yi-Ching Liaw,8 Chuan-Fa Hsieh,9,10 Yung-Po Liaw3,7
1Division of Family Medicine, Department of Community Medicine, Landseed International Hospital, Taoyuan City 324, Taiwan; 2Department of Health Business Management Administration, Hungkuang University, Taichung City 43302, Taiwan; 3Department of Public Health and Institute of Public Health, Chung Shan Medical University, Taichung City 40201, Taiwan; 4Department of Physical Education, Fu Jen Catholic University, New Taipei 24205, Taiwan; 5Research and Development Center for Physical Education, Health, and Information Technology, Fu Jen Catholic University, New Taipei 24205, Taiwan; 6Division of Health Management, Landseed International Hospital, Taoyuan City 324, Taiwan; 7Department of Medical Imaging, Chung Shan Medical University Hospital, Taichung City 40201, Taiwan; 8Graduate School of Frontier Sciences, University of Tokyo, Tokyo, Japan; 9Department of Medical Education, Research & Quality Management, Landseed International Hospital, Taoyuan City 324, Taiwan; 10College of Health Sciences & Technology, National Central University, Taoyuan City 32001, Taiwan
Correspondence: Yung-Po Liaw
Department of Public Health and Institute of Public Health, Chung Shan Medical University, No. 110, Sec. 1 Jianguo N. Road, Taichung City 40201, Taiwan
Tel +886-4-24730022 ext.11838
Fax +886-4-23248179
Email [email protected]
Chuan-Fa Hsieh
Department of Medical Education, Research & Quality Management, Landseed International Hospital, No. 77, Guangtai Road, Pingzhen City, Taoyuan, Taiwan
Tel +886-3-4941234 ext. 2172
Fax +886-3-20641333-4246
Email [email protected]
Purpose: High-density lipoprotein cholesterol (HDL-C) is essential for cardiometabolic health. Coffee consumption influences the body’s ability to regulate serum lipid profile. Although there is extensive information on coffee and cholesterol, not much is known whether changes in HDL-C concentrations are affected by coffee with or without flavoring substances.
Materials and Methods: Using historical data collected from 1272 participants in Li-Shin (Landseed) International Hospital in Northern Taiwan, we examined the relationship between HDL-C and consumption of plain black coffee with and without additives. Data on coffee consumption between 2006 and 2019 were collected based on self-reported questionnaires while HDL-C measurements were obtained from the electronic medical records of the hospital. t-test, chi-square test and multivariate linear regression analysis were used for analysis.
Results: In our primary analysis, we found that coffee consumption of ≥ 5 cups per week was positively associated with HDL-C (β = 1.9586, p=0.0442) compared with the lowest level (< 1 cup/week) of consumption. We found in a separate model that higher (≥ 5 cups/week) or lower (1– 4 cups/week) consumption of plain black coffee without additives was associated with higher HDL-C. The corresponding β values were 4.0674 (p = 0.0007) and 4.1253 (p = 0.0008), respectively. However, HDL-C levels were not affected by coffee with additives.
Conclusion: We found that consumption of black coffee without additives was associated with higher concentrations of HDL-C among Taiwanese adults over the age of 30. However, HDL-C levels did not change significantly among individuals who consumed black coffee with additives.
Keywords: coffee, cardiometabolic health, caffeine, lipid
Introduction
High-density lipoprotein cholesterol is one of the major components of metabolic syndrome that have been greatly associated with several conditions including cardiovascular diseases (CVD).1 Managing dyslipidemia (defined as high concentrations of triglyceride (TG) and low‐density lipoprotein cholesterol (LDL‐C), and/or low HDL‐C)2 is an important step aimed at reducing CVD risk.2,3 In recent years, lipid therapy had been seen as an appropriate means of preventing coronary heart diseases.4 Of the serum lipids, HDL-C has been widely investigated and found to be influenced by several lifestyle variables including exercise, alcohol drinking, diet, coffee consumption, and body mass index.5 However, its association with coffee consumption has remained inconsistent.6–8
Coffee consumption is increasing rapidly in many parts of the world including Taiwan. Observational studies have suggested that drinking 1–4 cups of coffee a day may help to reduce the risk of MetS.9–11 According to evidence from previous epidemiological studies, moderate coffee drinking appears to be beneficial to cardiovascular health.12–14 On the other hand, contrary findings have also emerged.15,16 Because of the variability previously observed across studies, more investigations are required to clarify these associations.
Associations between normal coffee drinking and cardiometabolic risk factors or biomarkers (such as HDL-C, total cholesterol, and LDL-C) have so far been described.17 Nonetheless, results have been conflicting. With attention directed towards HDL-C, it remains debatable whether its concentration is altered by coffee as some have suggested that possible increases may depend on the type of coffee consumed.18 So far, no study to our knowledge has attempted to describe such an association in Taiwan. To clarify this, we compared changes in HDL cholesterol levels among Taiwanese adults who consumed plain black coffee with no additives versus plain black coffee with additives.
Materials and Methods
Study Population
Data used in this study were from Li-Shin Outreach Neighborhood Screening (LIONS) project that was established in 2005 by the Landseed International Hospital in Pingzhen District, Taoyuan, Taiwan. The major objective of this project was to survey chronic disease and the potential risk factors among Taiwanese adults resident in PinZhen District.19 Eligible participants included those over 30 who had lived in the City for at least 30 years.20 These participants provided written informed consent. A self-administered questionnaire on medical history, lifestyle, and diet was completed by each participant before going through physical examinations. The LIONS project was conducted in accordance with the Declaration of Helsinki, and approval for this study was by the Institutional Review Board of Li-Shin Hospital (LSHIRB No./Protocol No 17–019).
In this study, the overall data were from 1272 participants who were recruited between 2006 and 2019.
Assessment of Coffee Consumption
Information on coffee consumption and other lifestyle variables was collected based on self-reported questionnaires. Participants responded “yes” to having a habit of drinking coffee. They reported drinking either plain black coffee alone or together with additives, and the number of cups consumed each week. Each cup had a capacity of approximately 240 mL. Alcohol drinkers were those who consumed on average 350 cc of wine, or 150 cc of beer, or 10 cc of spirit or distilled liquor (whiskey, vodka, rum, etc.) per day. Details of the other lifestyle variables in our model have been previously described.21
Assessment of Blood Lipids
Blood samples were collected from patients (n = 1272) at Li-Shin hospital. Serum concentrations of HDL-C and other lipids were measured using the Hitachi 7600/7180 automated biochemical analyzer (Hitachi, Tokyo, Japan).
Statistical Analysis
We performed statistical analysis using the SAS 9.4 (SAS Institute Inc., Cary, North Carolina, USA) version. Coffee consumption was categorized as <1, 1–4, and ≥5 cups per week. We compared categorical variables using the Chi-square test. Paired samples were compared using the Student’s t-test. Results were represented as mean ± standard deviation (SD) or as n (%). Multivariate linear regression analysis was performed to evaluate the effect of coffee on HDL-C. Independent parameters included age, sex, cigarette smoking, alcohol intake (betel nut chewing, body mass index, determined as weight (kg)/height (m2), vegetarian diet, exercise, and non-HDL cholesterol, defined as total cholesterol minus the HDL-C (<130 mg/dl representing normal values, and ≥ 130 mg/dl representing higher values). The β-coefficients and p-values were reported.
Results
Demographic characteristics of the study participants are presented in Table 1. The mean HDL-C was 57.43 mg/dL among participants who consumed black coffee with additives and 60.37 mg/dL among those who consumed only plain black coffee (p = 0.0007). Association of HDL-C with overall coffee consumption is presented in Table 2. Compared with the lowest level of coffee consumption (<1 cup/week), coffee consumption of ≥5 cups/week was associated with higher HDL-C (β = 1.9586, p=0.0442). However, coffee consumption of 1–4 cups/week was not associated with HDL-C (β = 1.5635, p=0.0919). HDL-C levels were lower (β = −2.3558, p=0.0021) in participants with higher levels of non-HDL (≥ 130 mg/dl) compared with the lower levels (≤130mg/dl). We also observed that men had lower HDL-C than women (β = −11.7347, p<0.0001). Furthermore, HDL-C levels of current smokers were lower than in never smokers (β = −2.3824, p = 0.0304). Compared with nondrinkers, alcohol drinking was significantly associated with higher HDL-C among former (β = 5.7309, p = 0.0083) and current (β = 5.7832, p<0.0001) drinkers. We also examined changes in HDL-C levels based on consumption of coffee brewed with and without additives (Table 3). When the category, <1 cup/week of black coffee with additives was used as the reference category, the corresponding β-coefficients for categories of 1–4 and ≥5 cups/week of black coffee with additives were 0.4995 (p = 0.6488) and 0.8860 (p=0.4543), respectively. Those for categories of <1, 1–4, and ≥5 cups/week of black coffee without additives were 1.9295 (p = 0.3052), 4.0674 (p = 0.0007), and 4.1253 (p = 0.0008), respectively.
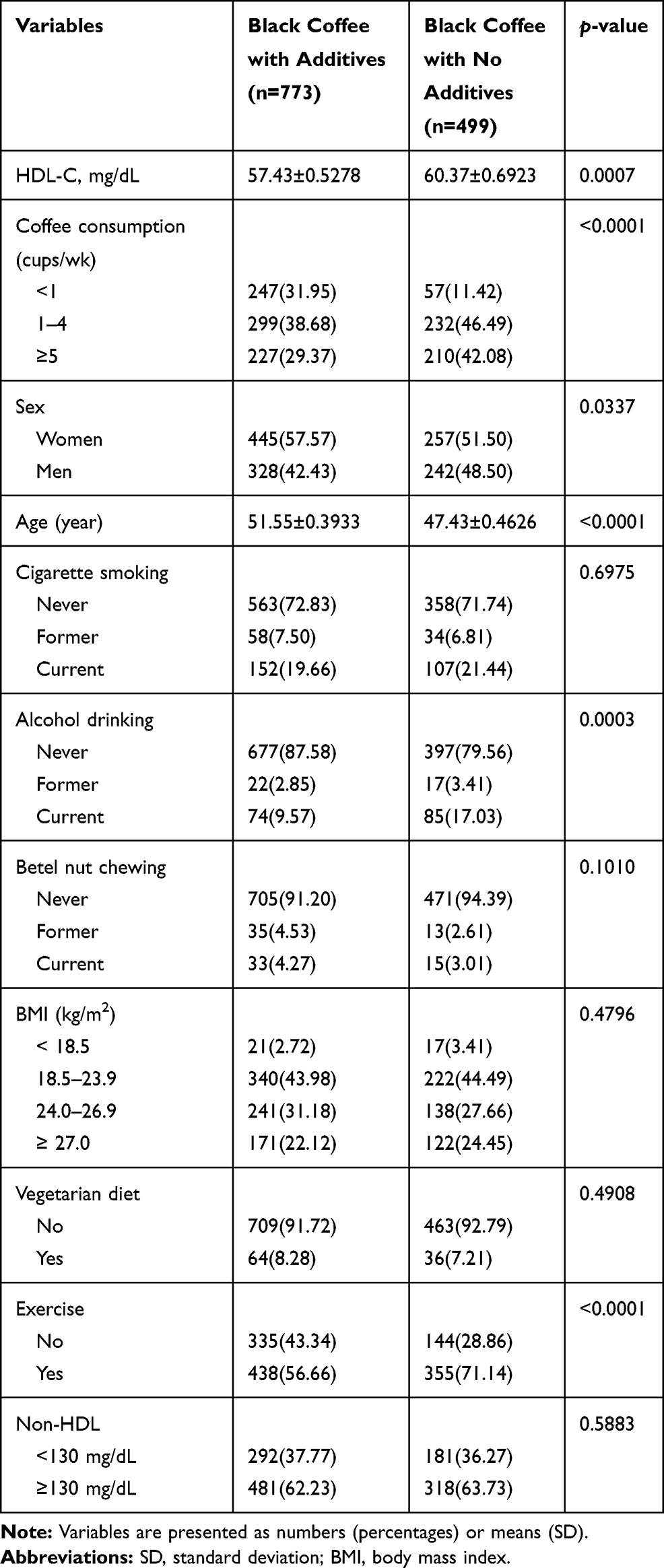 |
Table 1 Demographic Characteristics of Study Participants |
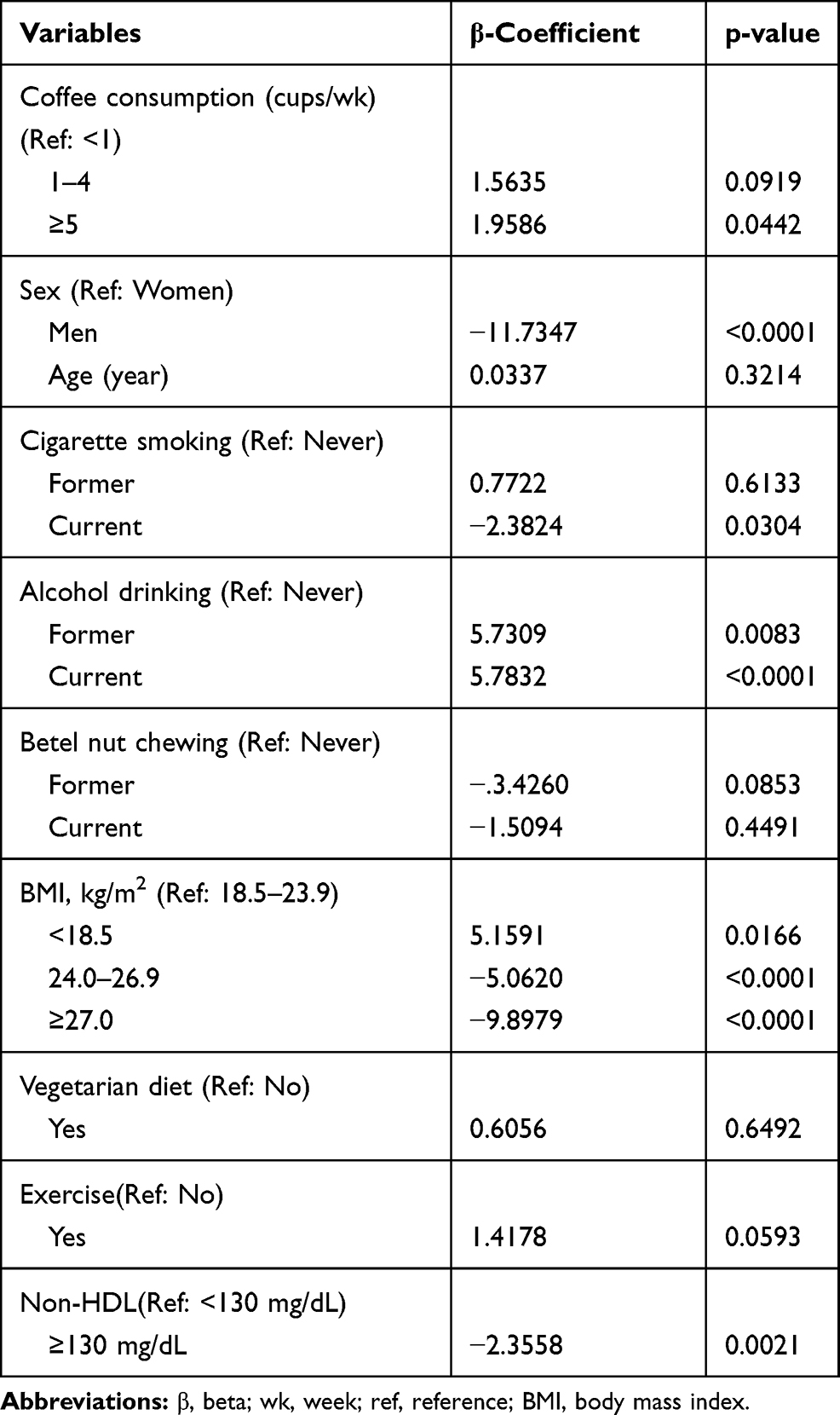 |
Table 2 Changes in HDL-C Concentrations Based on Coffee Consumption |
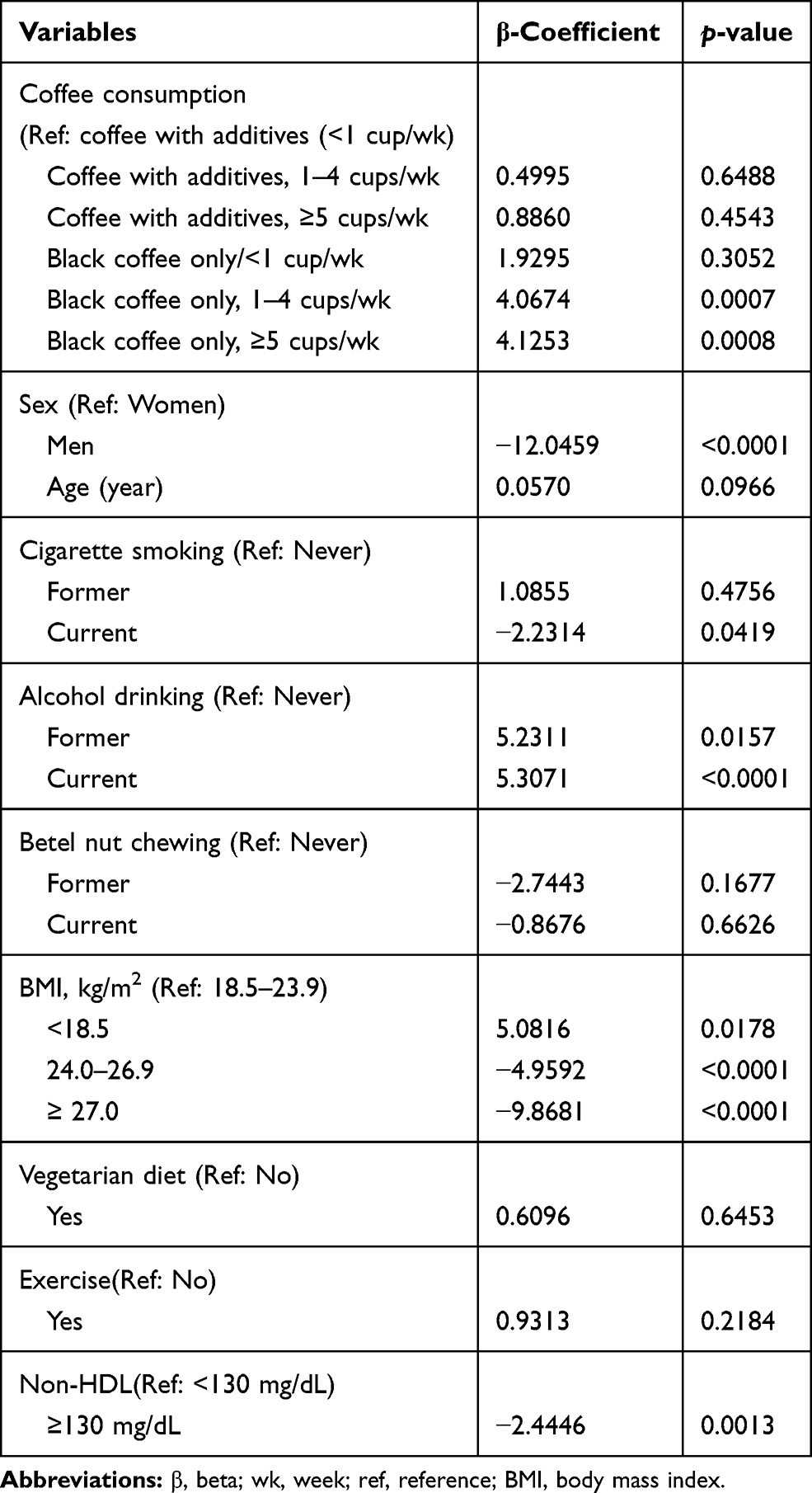 |
Table 3 Changes in HDL-C Based on Consumption of Plain Black Coffee with and without Additives |
Discussion
In this study, we observed that coffee consumption of ≥5 cups per week was greatly associated with higher levels of HDL-C among Taiwanese adults 30 years and older. However, there was no association between HDL-C and coffee consumption of 1–4 cups per week. Prior clinical studies have suggested that higher consumption of coffee may improve HDL-C.22,23 On the contrary, other studies have found no association between coffee consumption and HDL-C.17,24,25
In this study, we performed more analysis to determine whether changes in HDL-C are affected by coffee brewed with or without additives. When we used the lowest category, <1 cup/week of black coffee with additives as the reference group, we found that the association between coffee and HDL-C was stronger only among those that consumed 1–4 (β = 4.0674, p = 0.0007) and ≥5 cups (β = 4.1253, p = 0.0008) of plain black coffee without additives. Higher (≥5 cups/week) or lower (1–4 cups/week) consumption of plain black coffee with additives did not have any substantial effect on HDL-C levels. Findings from a randomized cross over study showed that HDL-C levels of patients who consumed a single 6-oz cup of black coffee with no flavoring substances significantly rose from 43.2 mg/dL to 44.8 mg/dL (p<0.001).26 However, no significant changes were observed among patients who consumed coffee with creamer and sugar. The biological mechanism by which black coffee may alter HDL-C levels is not clear. However, according to Cheung and his colleagues, such an increase may be associated with the concomitant decrease in triglycerides.26 Further investigations are required to support or clarify these findings.
In the primary analysis, we observed that HDL-C values were relatively lower in men than women. Another interesting finding was that higher concentrations of non-HDL-C (≥130 mg/dl) were greatly associated with lower HDL-C (β = −2.3558 (p = 0.0021). Higher values of non-HDL cholesterol are predictive of cardiovascular disease: Decreased levels have been associated with a lower risk of cardiovascular diseases among older adults.27 In our study, overweight and obesity also showed a strong but negative association with HDL-C. Physical exercise was weakly associated with HDL-C whereas the association did not differ by diet and betel nut chewing.
Despite these preliminary findings, it is wise stating our limitations. First, information on coffee consumption was collected based on a self-reported questionnaire. This might have introduced misclassification bias. Second, we could not determine the brew mechanism, the amount of coffee used, and the roasting time, which in part are believed to influence serum lipids. Next, data were not available on the exact ranges of cream, milk, sugar, or other flavoring substances that might have been used. Finally, data were from participants who were resident only in the Pingzhen District. Therefore, our findings may not be generalized.
Conclusions
Taken together, our findings indicated that consumption of black coffee without additives was associated with higher concentrations of HDL cholesterol among Taiwanese adults over the aged over 30 years. However, HDL-C levels were not affected by consumption of coffee with additives. We believe that these preliminary findings may be useful for future investigations on coffee drinking and cardiometabolic health.
Funding
This work was supported by funds from the collaborative projects between Chung Shan Medical University and Li-Shin International Hospital (CSMU-LSH-106-01).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Marjani AA. Review on HDL-cholesterol alterations in metabolic syndrome. J Biol Sci. 2013;13(8):679–684. doi:10.3923/jbs.2013.679.684
2. Haslam DE, Peloso GM, Herman MA, et al. Beverage consumption and longitudinal changes in lipoprotein concentrations and incident dyslipidemia in US adults: the Framingham heart study. J Am Heart Assoc. 2020;9(5):e014083. doi:10.1161/JAHA.119.014083
3. Nelson RH. Hyperlipidemia as a risk factor for cardiovascular disease. Prim Care. 2013;40(1):195–211.
4. Ventura HO, Lavie CJ, Mehra MR. HDL and heart failure regulation: still breathing but exhausted. J Am Coll Cardiol. 2019;187–189.
5. Steyn K, Fourie J, Benade A, et al. Factors associated with high density lipoprotein cholesterol in a population with high high density lipoprotein cholesterol levels. Arteriosclerosis. 1989;9(3):390–397. doi:10.1161/01.ATV.9.3.390
6. Corrêa TA, Rogero MM, Mioto BM, et al. filtered coffee increases cholesterol and inflammation biomarkers independent of roasting degree: a clinical trial. Nutrition. 2013;29(7–8):977–981. doi:10.1016/j.nut.2013.01.003
7. Zargar A, Auttapibarn C, Hong SH, Larson TJ, Hayworth KH, Ito MK. The effect of acute café latte ingestion on fasting serum lipid levels in healthy individuals. J Clin Lipidol. 2013;7(2):165–168. doi:10.1016/j.jacl.2012.11.001
8. Salonen JT, Happonen P, Salonen R, et al. Interdependence of associations of physical activity, smoking, and alcohol and coffee consumption with serum high-density lipoprotein and non-high-density lipoprotein cholesterol—a population study in eastern Finland. Prev Med. 1987;16(5):647–658. doi:10.1016/0091-7435(87)90048-X
9. Shang F, Li X, Jiang X. Coffee consumption and risk of the metabolic syndrome: a meta-analysis. Diabetes Metab. 2016;42(2):80–87. doi:10.1016/j.diabet.2015.09.001
10. Grosso G, Stepaniak U, Micek A, et al. Association of daily coffee and tea consumption and metabolic syndrome: results from the Polish arm of the HAPIEE study. Eur J Nutr. 2015;54(7):1129–1137. doi:10.1007/s00394-014-0789-6
11. Marventano S, Salomone F, Godos J, et al. Coffee and tea consumption in relation with non-alcoholic fatty liver and metabolic syndrome: a systematic review and meta-analysis of observational studies. Clin nutr. 2016;35(6):1269–1281. doi:10.1016/j.clnu.2016.03.012
12. Choi Y, Chang Y, Ryu S, et al. Coffee consumption and coronary artery calcium in young and middle-aged asymptomatic adults. Heart. 2015;101(9):686–691. doi:10.1136/heartjnl-2014-306663
13. Freedman ND, Park Y, Abnet CC, Hollenbeck AR, Sinha R. Association of coffee drinking with total and cause-specific mortality. N Engl J Med. 2012;366:1891–1904. doi:10.1056/NEJMoa1112010
14. Kokubo Y, Iso H, Saito I, et al. The impact of green tea and coffee consumption on the reduced risk of stroke incidence in Japanese population: the Japan public health center-based study cohort. Stroke. 2013;44(5):1369–1374. doi:10.1161/STROKEAHA.111.677500
15. Fung K, Biasiolli L, Hann E, et al. 9 Effect of coffee consumption on arterial stiffness from UK biobank imaging study. British Cardiac Society. 2019;A8–A10.
16. Wang Y, Tuomilehto J, Jousilahti P, et al. Coffee consumption and the risk of heart failure in Finnish men and women. Heart. 2011;97(1):44–48. doi:10.1136/hrt.2010.206045
17. Jee SH, He J, Appel LJ, Whelton PK, Suh I, Klag MJ. Coffee consumption and serum lipids: a meta-analysis of randomized controlled clinical trials. Am J Epidemiol. 2001;153(4):353–362. doi:10.1093/aje/153.4.353
18. Ricketts M-L. Does Coffee Raise Cholesterol? Taylor & Francis; 2007.
19. Chang H-C, Liang J, Hsu H-C, Lin S-K, Chang T-H, Liu S-H. Regular exercise and the trajectory of health-related quality of life among Taiwanese adults: a cohort study analysis 2006–2014. BMC Public Health. 2019;19(1):1352. doi:10.1186/s12889-019-7662-8
20. Chang H, Kung Y, Hsieh C, Hsiung L, Chang S, Chen T. Biological risk factors relevant to chronic disease in three ethnic groups in Taiwan: results from Li-Shin outreaching neighborhood screening (Lions A1). Ethn Dis. 2008;18(2):228.
21. Chang H-C, Hsieh C-F, Lin Y-C, et al. Does coffee drinking have beneficial effects on bone health of Taiwanese adults? A longitudinal study. BMC Public Health. 2018;18(1):1273.
22. Fried RE, Levine DM, Kwiterovich PO, et al. The effect of filtered-coffee consumption on plasma lipid levels: results of a randomized clinical trial. JAMA. 1992;267(6):811–815. doi:10.1001/jama.1992.03480060057030
23. Kempf K, Herder C, Erlund I, et al. Effects of coffee consumption on subclinical inflammation and other risk factors for type 2 diabetes: a clinical trial. Am J Clin Nutr. 2010;91(4):950–957. doi:10.3945/ajcn.2009.28548
24. Miyake Y, Kono S, Nishiwaki M, et al. Relationship of coffee consumption with serum lipids and lipoproteins in Japanese men. Ann Epidemiol. 1999;9(2):121–126. doi:10.1016/S1047-2797(98)00051-9
25. Cai L, Ma D, Zhang Y, Liu Z, Wang P. The effect of coffee consumption on serum lipids: a meta-analysis of randomized controlled trials. Eur J Clin Nutr. 2012;66(8):872–877. doi:10.1038/ejcn.2012.68
26. Cheung RJ, Gupta EK, Ito MK. Acute coffee ingestion does not affect LDL cholesterol level. Ann Pharmacother. 2005;39(7–8):1209–1213. doi:10.1345/aph.1G005
27. Brunner FJ, Waldeyer C, Ojeda F, et al. Application of non-HDL cholesterol for population-based cardiovascular risk stratification: results from the multinational cardiovascular risk consortium. Lancet. 2019;394(10215):2173–2183. doi:10.1016/S0140-6736(19)32519-X
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.