Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Challenges to Implementation of Community Health Worker-Led Chronic Obstructive Pulmonary Disease (COPD) Screening and Referral in Rural Uganda: A Qualitative Study using the Implementation Outcomes Framework
Authors Ingenhoff R ![]() , Robertson N
, Robertson N ![]() , Munana R, Bodnar BE
, Munana R, Bodnar BE ![]() , Weswa I, Sekitoleko I, Gaal J, Kirenga BJ, Kalyesubula R
, Weswa I, Sekitoleko I, Gaal J, Kirenga BJ, Kalyesubula R ![]() , Knauf F, Siddharthan T
, Knauf F, Siddharthan T
Received 25 May 2023
Accepted for publication 30 October 2023
Published 28 November 2023 Volume 2023:18 Pages 2769—2783
DOI https://doi.org/10.2147/COPD.S420137
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Rebecca Ingenhoff,1,2 Nicole Robertson,3 Richard Munana,4,5 Benjamin E Bodnar,6 Ivan Weswa,5 Isaac Sekitoleko,7,8 Julia Gaal,1 Bruce J Kirenga,9 Robert Kalyesubula,5,10,11 Felix Knauf,1,11 Trishul Siddharthan12
1Department of Nephrology and Medical Intensive Care, Charité - Universitätsmedizin Berlin, Berlin, Germany; 2Charité Center for Global Health, Charité - Universitätsmedizin Berlin, Berlin, Germany; 3University of Kentucky College of Medicine, Lexington, KY, USA; 4School of Public Health, Makerere University College of Health Sciences, Makerere University, Kampala, Uganda; 5African Community Center for Social Sustainability, Nakaseke, Uganda; 6Department of Medicine, Johns Hopkins University School of Medicine, Baltimore, MD, USA; 7MRC/UVRI and LSHTM Uganda Research Unit, Kampala, Uganda; 8London School of Hygiene and Tropical Medicine, London, UK; 9Makerere University Lung Institute, Kampala, Uganda; 10Department of Physiology, Department of Internal Medicine, Makerere University College of Health Sciences, Kampala, Uganda; 11Department of Internal Medicine, Yale School of Medicine, New Haven, CT, USA; 12Department of Pulmonary, Critical Care and Sleep Medicine, University of Miami, Coral Gables, FL, USA
Correspondence: Rebecca Ingenhoff, Email [email protected]
Background: Chronic obstructive pulmonary disease (COPD) is the third leading cause of death globally. The burden of COPD is expected to increase in low- and middle-income countries (LMICs). COPD screening and diagnostics tools are often inaccessible in rural settings of LMICs. To contribute to the growing body of evidence on the effectiveness of Community Health Worker (CHW) interventions, this study aims to understand the facilitators and barriers of implementing a CHW-led COPD screening and referral program in rural Uganda.
Methods: This qualitative study was conducted from September to October 2022 to explore Community Members, CHWs, and Healthcare Providers (HCPs) perceptions on the challenges of CHW-delivered COPD programming in Nakaseke, rural Uganda. In total, we held eight individual in-depth interviews with CHWs, ten in-depth interviews with HCPs and six focus group discussions with 34 Community Members. Research assistants audio-recorded and transcribed interviews verbatim. The implementation outcomes framework guided the thematic analysis.
Results: Implementation acceptability was constrained by a lack of COPD awareness, a lack of perceived utility in COPD screening as well as stigma around the diagnostic process. Limited spirometry adoption was also attributed to Community Member accessibility and willingness to participate in the COPD diagnostic referral process. The high patient volume and the complex, time-consuming diagnostic and referral process hindered successful implementation. To enhance program sustainability, all participants suggested increasing CHW support, medication access, decentralizing COPD care and upscaling follow-up of Community Members by CHWs.
Conclusion: CHW-led interventions remain a potentially critical tool to alleviate barriers to treatment and self-management in settings where access to care is limited. While community-based interventions can create sustainable infrastructure to improve health outcomes, formative assessments of the potential barriers prior to intervention are required. Evidence-based, localized approaches and sustained funding are imperative to achieve this.
Keywords: community health workers, task shifting, screening and referral, chronic obstructive pulmonary disease, Uganda
Introduction
Non-communicable diseases (NCDs) account for an estimated 41 million deaths annually.1 Among these NCDs, chronic obstructive pulmonary disease (COPD), a preventable condition characterized by progressive limitation of airflow, is the third leading cause of death globally.2 COPD is expected to be the leading cause of death in low- and middle-income countries (LMICs) within the next decade, causing severe economic impacts in LMICs, with nearly 90% of COPD deaths occurring in these settings.2–4 In Uganda, the reported prevalence of COPD is disproportionately higher in rural populations ranging from 6.1% to 16.8% compared to 1.5% in urban populations.5,6
In the majority of LMICs, especially in Sub-Saharan Africa, spirometry is not available particularly in the primary care healthcare settings.7,8 COPD diagnosis in LMICs settings, including Uganda, is limited due to numerous barriers including limited awareness of COPD, lack of financial means for medical care, and limited availability and accessibility of diagnostic devices and healthcare worker training.8–10
To increase accessibility of spirometry in LMICs, facility-based COPD screening has been utilized in primary care settings and tertiary care centers to screen symptomatic and at-risk patient populations.11–14 Unfortunately, various health systems and patient level barriers with facility-based COPD screening limit the accessibility and adoption of spirometry in resource-constrained settings.15 Emerging studies suggest that community health workers (CHWs) are more effective in delivering NCD prevention and control interventions compared to standard practice in LMIC settings.16–19 Community-based strategies with CHWs using inexpensive portable handheld spirometers or case-finding instruments may provide benefit for screening and early detection of COPD in rural communities in LMICs.20 A study in rural India utilizing a two-stage sequential screening strategy among community health workers (CHWs) demonstrated accurate and effective detection of COPD.21 However, most of the CHW-led COPD screening and referral interventions studies have been limited to observational studies in high-income countries rather than LMICs like Uganda.22,23
Understanding implementation of CHW-led programs may reduce COPD underdiagnoses, facilitate early-stage COPD diagnosis, and optimize strategies to implementation in LMIC communities. However, CHW-led COPD screening and referral programs have not been evaluated in terms of implementation challenges to increase their effectiveness and sustainability. The aim of this qualitative study is to understand and analyze the challenges of a community health worker-led COPD screening and referral in rural Uganda using the implementation outcomes framework.
Methods
Study Site
Nakaseke is a rural district in Central Uganda featuring a population of an estimated 202200 in nine sub-counties.24 We purposively selected the study site as the previous community census presented an organized sample of participants while implementing partners provided the necessary infrastructure and skills to conduct a population-based study.25
Study Design
Between March and August 2022, we employed a household-based, community health worker (CHW)-led COPD screening and referral program in Nakaseke district. Through proactive household visits, CHWs set out to collective data on socioeconomic characteristics COPD prevalence using peak flow meters among 3500 participants who were sampled from a previous census study.25 Participants that met the referral criteria for necessary spirometry testing were referred to Nakaseke District Hospital by CHWs. To generate an understanding of the complex healthcare environment and the challenges stakeholders experience throughout the screening program, we explored Community Members, CHW and Healthcare Provider (HCP) experiences through a qualitative post-screening intervention from September to October 2022. We conducted focus group discussions (FGDs) with Community Members and individual in-depth interviews (IDIs) with CHWs and HCPs. Participants who currently lived or worked in Nakaseke district were chosen through a purposive sampling to include certain characteristics such as disease status, adherence to referral or role in the screening program in the three selected groups (Figure 1).
 |
Figure 1 Illustration of two-step COPD screening and qualitative post-evaluation. |
Participants
A total of 52 participants grouped into Community Members, CHWs and HCPs participated in the study (Table 1). Eight CHWs and ten HCPs took part in individual IDIs. Further, we conducted six FGDs with 34 Community Members in total. A heterogeneous sample of Community Members that previously participated in the CHW-led household-based COPD screening featuring diversity in age, gender, COPD status, and adherence to referral was selected purposefully. Most of the FGD participants were referred for further spirometry testing to Nakaseke Hospital but the study included some that did not screen as high risk and were hence not referred by CHWs. In addition, we included participants that did or did not reach the referral site after receiving a referral note from CHWs (adherence to referral). Moreover, we ensured a balance in Community Members’ age while also including males and females. The local project managers identified Community Members from clinical and research records. CHWs were residents of Nakaseke district, employed by the local non-governmental organization (NGO) the African Community Center for Social Sustainability Uganda (ACCESS), and previously conducted the COPD screening using peak flow meters along with COPD case finding questionnaires as well as referral at household level. The HCPs were recruited from ACCESS or Nakaseke District Hospital and were selected clinicians (physicians and nurses) or research and administration staff that played a crucial role in screening, referral, clinical care, or operations during the COPD management program implementation. HCPs roles included screening (n = 3, 30%), clinical care (n = 3, 30%), and administration and research (n = 4, 40%).
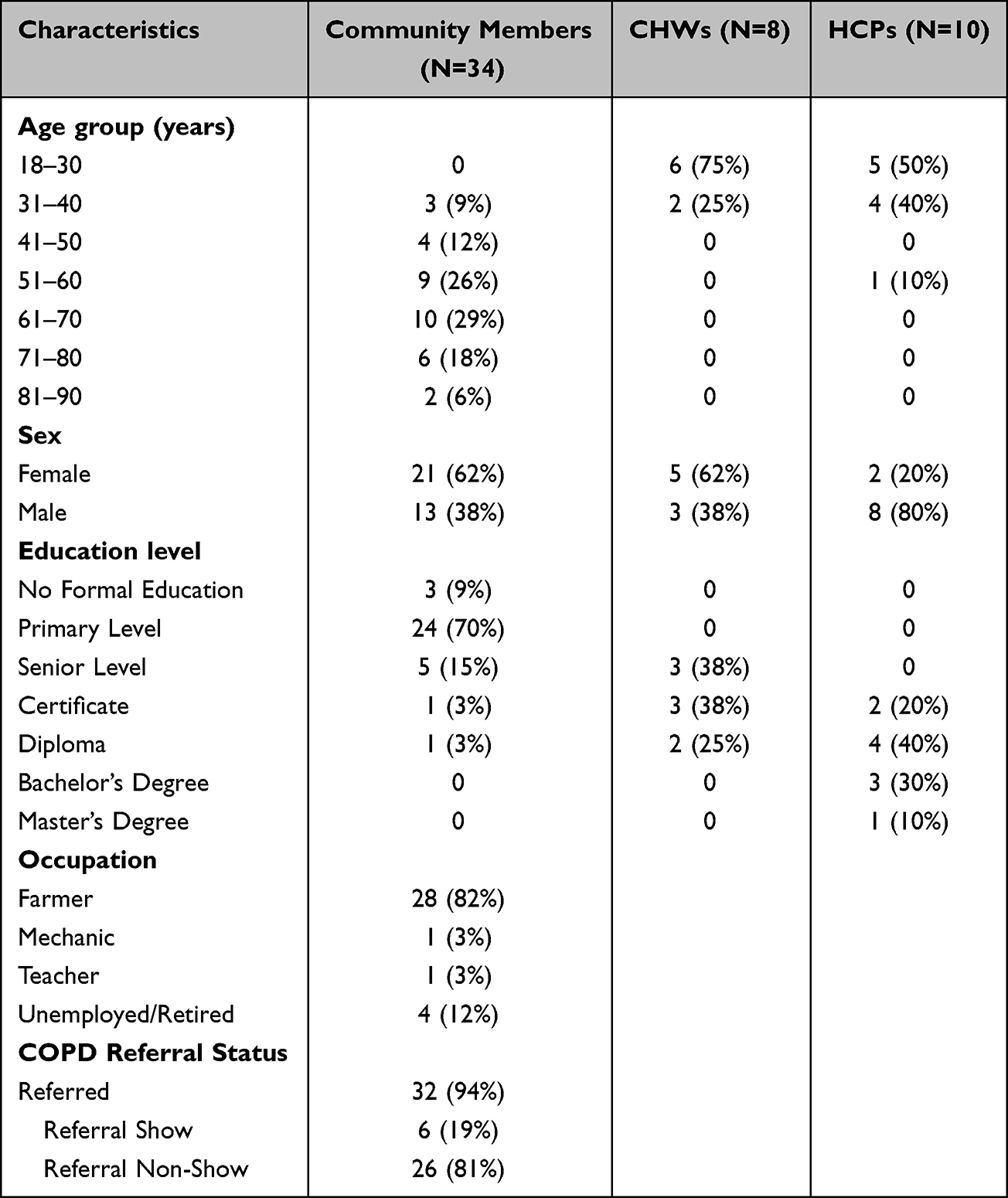 |
Table 1 Characteristics of Study Participants, Community Members, Community Health Workers (CHWs), and Healthcare Providers (HCPs) |
Data Collection
The data collection took place in Nakaseke, a rural district in Uganda between September and October 2022. To gain integrated insights on challenges encountered throughout the process, we developed three separate interview guidelines to adapt questions to each target group. Interview guide 1 was developed for the FGDs with Community Members, addressing personal experiences and challenges throughout the screening and referral process. Interview guide 2 was designed for the IDIs with CHWs, questions related to their challenges, experiences, and recommendations in performing the required tasks. Interview guide 3 was used for HCPs, focusing on professional experiences in administering the program and screening on the hospital level. The research team developed interview guides initially in English, which were translated to Luganda by professional translators at Makerere University, School of Languages, Literature and Communication. A team of research assistants trained social scientists who were fluent in both English and Luganda, a local dialect in Nakaseke district, collected the data. During a two-day training run by the local project managers from ACCESS Uganda, research assistants familiarized themselves with the study objectives and the data collection tools. The local project managers and research assistants conducted pilot interviews and pilot FGDs to ensure that the questionnaires met the needs and objectives of the study. Participants were contacted by phone or physically to recruit them for the study. FGDs were conducted in Luganda, HCP interviews and CHW interviews were conducted in English or Luganda based on the participants’ preference. Interviews in Luganda were recorded and transcribed verbatim to English by research assistants. Interviews conducted in English were recorded and transcribed in English. Most interviews were conducted on the premises of ACCESS Uganda or Nakaseke District Hospital. One HCP was facilitated via digital video software. On average IDIs ran for 45 minutes, FGDs lasted approximately an hour.
Analysis
Data was analyzed using the implementation outcomes criteria.26 The research team used an inductive approach to thematic analysis to link the data to the implementation outcomes.27,28 Having the implementation outcomes in mind, RI and NR created independent code books using line-by-line coding of arising themes via a sample of transcripts with Microsoft Word. After discussing the first set of themes, RI and NR agreed to continue with a selected set of implementation outcomes (acceptability, adoption, appropriateness, implementation cost and sustainability) that were chosen as appropriate to analyze the remaining data. These categories were selected due to applicability to the research context, thematically occurrence in the transcripts, as well as the frameworks’ recommendation for the use of qualitative data.26 In the next step, both RI and NR read and coded all remaining transcripts individually. The previously discussed themes were used while allowing new themes to emerge throughout the process. Afterwards, RI and NR compared resulting themes while agreeing on how to organize them under the implementation outcomes. At the next stage, categorization and themes were evaluated and further refined by RI, NR and TS and according to the research team’s feedback.
Ethical Approval and Consent
Ethical approval for this study was granted from the Makerere University School of Biomedical Sciences Research and Ethics Committee (SBS-REC 874) on February 21, 2021 and the Uganda National Council of Science and Technology (SS821ES) on May 7, 2021. This study complies with the Declaration of Helsinki. Participants gave written informed consent, were monetarily compensated for their time, and agreed to anonymized publication of their interview data.
Results
We summarize the key qualitative findings within the Implementation Outcomes framework themes including (1) acceptability, (2) adoption, (3) appropriateness, (4) cost, and (5) sustainability in Table 2.26
 |
Table 2 Implementation Outcomes Themes and Sub-Themes as Derived from the Qualitative Data Among Community Members, Community Health Workers (CHWs), and Healthcare Providers (HCPs) |
Acceptability
Challenges to acceptability, or community satisfaction to the intervention included lack of COPD awareness and associated health-seeking behaviors, lack of perceived utility of COPD screening, lack of community trust, and fear and stigma surrounding the diagnostic process.
Lack of Patient COPD Awareness and Health Seeking Behavior
All levels of participants recognized limited awareness of COPD in the community as a challenge, as the disease is relatively unknown compared to other NCDs. Community beliefs surrounding witchcraft often contributed to this misinformation surrounding COPD. Additionally, most Community Members (64.7%, n = 22) expressed that stepwise evaluation with peak flow meter and confirmatory spirometry testing contributed to confusion on COPD diagnosis.
People in the villages do not have the idea of going to the hospital to do checkups. Most of them actually resort to thinking they have been bewitched when they fall sick. -Community Member, Female, 74 years old
Lack of Perceived Utility of Screening
Community Members, CHWs and HCPs recognized that mild or minimal symptoms in most patient screening positive on community testing and a lack of awareness of the importance of screening compared to other NCDs, and infectious disease (ie, Human Immunodeficiency Virus) led to decreased perceived usefulness of COPD screening.
The COPD screened patients are unbothered by the diagnosis during screening and they are reluctant to go to the referred health facility for further analysis and management. Only when one feels the pain is out of control is when they turn up at the health facility (…). -Healthcare Provider, Male, 32 years old, NGO Staff
Lack of Community Trust
Community Members displayed issues of trust towards the government, the operating organization and CHWs. Personal conflicts between participants and CHWs may impact community acceptance of screening. Community Members raised concerns that CHWs were initially perceived “conmen” as they offered services free of charge. In addition, bad social behaviors of CHWs may lead to mistrust among Community Members.
Another challenge was being chased by the Community Members who did not want to take part in the screening exercise. [Land grabbing] is a very common vice in our communities and people can easily mistake community health workers for land grabbers (…). -Community Health Worker, Male, 28 years old
The second time when they came at home, I asked them who had brought them, I was a bit difficult (…) until they pulled out a register which contained our names and told me my name(…). I was not easy on them. -Community Member, Female, 77 years old
Fear and Stigma of Diagnostic Process
Community Members feared COPD screening due to the common belief of spread of COPD or infectious disease during diagnostic testing with equipment. Additionally, due to discomfort with diagnostic testing, Community Members expressed fear of lung damage from the lung “bursting”.
Some [Community Members] would not accept to use the [peak flow] machine thinking (…) it was used by the previous participant (…). Some people also refuse because of superstitions that we are instead affecting them with COVID-19. -Community Health Worker, Female, 27 years old
Due to overlap with infectious disease and lack of awareness surrounding COPD, all participant levels reported stigmatization of COPD diagnosis.
Some people hid and did not want to take part in the [COPD] screening process because of fear of stigmatization from other Community Members who assume that when one coughs (…) [they] are tuberculosis patients. COPD is not a condition they think of (…). -Healthcare Worker, Male, 27 years old, NGO Staff
Adoption
Most participants expressed challenges in implementation including administration of COPD diagnostics and equipment, accessibility, and willingness to participate in COPD diagnostic process.
Community Member Accessibility and Willingness to Participate in COPD Diagnosis
Many participants (73.1%, n = 38) reported difficulty with performing peak flow and spirometry COPD screening due to pain during screening, lack of familiarity, and duration of time. Furthermore, most CHWs (80%, n = 8) endorsed difficulty using complex diagnostic equipment and limited access to this equipment.
Screening for COPD involves so many things. If we are to check someone. You may tell them to blow into the peak flow meter and they find challenges. We require that someone blows into the peak flow meter not less than three times (…). -Community Health Worker, Male, 42 years old
Most healthcare providers (70%, n = 7) at referral sites were concerned about rumors on screening difficulty that may lead to rejection of screening participation.
The only discomfort [is] some fear to perform the test. (…). Some [Community Members] go spreading it that it’s [spirometry] not easy to perform; it stretches your lungs and so on. You therefore find that patient who was willing to perform ends up rejecting. -Healthcare Provider, Male, 30 years old, Screening Staff
Administration of COPD Diagnostics and Equipment Use
Participants at all levels voiced concern over participant confidentiality with neighbors and other family members who approach participants during screening at homes. More female compared to male participants and CHWs were concerned that there were no designated screening space and expressed concern for comfort and privacy.
Some people step into other people’s space. For example, neighbors who cross over from their households to others, which interferes with privacy and confidentiality. (…). -Community Health Worker, Female, 27 years old
Community Members felt at times comorbid conditions such as hypertension, malnutrition, and infectious disease deemed them unwilling and unable to participate due to debility.
You may notice that someone may be unable to blow into the peak flow meter due to old age and hunger…Blowing into the peak flow meter is easy but a challenge comes in if someone hasn’t eaten, they’re weak or when the [blood] pressure is high. -Community Health Worker, Female, 32 years old
Appropriateness
Challenges to intervention appropriateness assessed the perceived fit, practicality, and suitability for the LMIC community and at the HCP, CHW, and Community Member level. We found a high volume of patients with positive peak flow screening in the community, limited CHW time, and fragmented and time intensive referral process for screened Community Members.
High Patient Volume and Community Member Time
CHWs and Community Members described the time intensive screening process as an implementation challenge. CHWs struggled to locate participants in rural areas, which lengthened the already complex procedure. As daily screening targets of CHWs rose, CHWs presented a feeling of being overburdened by their workload.
At first, we were given 10 people, they [supervisors] increased it to 15 people and for the current study, they want 30 people per week. It’s very hard to find those people [Community Members] because the questionnaire has so many questions, the consent is long …you spend a lot of time on one person. -Community Health Worker, Female, 32 years old
In addition, nurses performing the spirometry at the referral site argued that the high patient volume was a challenge due to the time intensive testing procedure.
At first it was hard and still it is because imagine if we were getting many patients, we couldn’t screen all of them (…) someone looks at spending the whole day at the facility because it would take (…) like two to three hours. –Healthcare Provider, Female, 25 years old, Nurse
Fragmented and Time Intensive Referral Process
Respondents at all levels described a fragmented and time intensive referral process resulting in lack of follow up at referral center and non-adherence to COPD treatment and management. Community Members stated they were reluctant to follow up at the referral center due to fear of COPD diagnosis and lack of debilitating COPD symptoms (ie, breathlessness). A CHW argued that Community Members are prioritizing their work.
It’s the fear [of COPD] that stops them not the lack of [financial] means (…). They just don’t want to leave their work they feel like this is time wasting. -Community Health Worker, Female, 32 years old
Repeatedly, most HCPs (70%, n = 7) demonstrated that Community Members are reluctant to participate in the referral process until worsening symptoms.
Most of them [Community Members] (…) had the conditions [NCDs] but the signs [and symptoms] were not yet out so telling them to come to hospital, they could be like after all I’m not feeling any pain so I’ll go when I feel pain. (…) Some of them refused totally. -Healthcare Provider, Female, 26 years, Nurse
Many CHWs (60%, n = 6) argued that Community Members present an indifference to their referral while outlining a lack of transparency during the referral process. CHWs would like to be informed whether their referred Community Members reached the referral site to gain a better understanding of the discrepancy between referred Community Members and no-shows.
The challenge in referral is we expect the patients to reach the referred site or clinic and they don’t come, (…) Some don’t want their sickness to be cared for, they tell you happily (…) you have given me referral but I will not come (…). -Community Health Worker, Female, 28 years old
Community Members present distinct reasons such as limited time, inability to travel due to funds or loss of documents for not showing up to their referred testing. We found a disconnect between HCPs and CHWs and Community Members in availability of HCPs at referral centers. CHWs and Community Members alike reported Community Members were confused on where to attend referral appointments and when arriving had difficulty finding HCPs leading to lack of future follow up.
When we reached the hospital, we [Community Members] were told to sit somewhere at mid-day (…). We were then told to shift to another spot, (…) moving aimlessly until one doctor took pity on us and directed us to the concerned doctor (…). By the time I came back the doctor had left, so I left without returning the results to the doctor. -Community Member, Female, 74 years
Implementation Cost
Challenges to implementation cost include transportation, COPD medication, and intervention-related costs to engage the community and facilitate screening. Most participants reported transportation costs for both Community Members and CHWs as a major financial cost and challenge to implementation.
Transportation for Community Members and CHWs
Transportation costs for travelling to the referral site presented a tremendous obstacle for many Community Members (67.6%, n = 23). HCPs confirmed that Community Members who reside far from the referral center tend to not reach.
We had issues because transport is a major challenge. -Community Member, Female, 77 years old
We were receiving a little number of referrals due to the lack of transportation to the facility (…). Those who need a lot of money will not be able to come so there is a transport problem. -Healthcare Provider, Male, 32 years old, NGO Staff
Particularly older Community Members are often unable to move long distances. As fuel prices are increasing in Uganda, transport becomes even more inaccessible, as a CHW argued.
Long distance and limited funds for transport and no funds to facilitate for their eating while at [the] hospital is a challenge to them (…). -Community Health Worker, Female, 26 years old
Transport challenges further occurred for CHWs as they described that the transport or gasoline allowance as insufficient for the large catchment area, which forces them to cover expenses out of their own pocket at times.
On our side [as CHWs] (…) sometimes we fail because the villages are far apart, the distance is long and too much fuel is consumed (…) Even the [fuel] prices went up. With this, we end up spending our own money which we would have saved for other purposes. -Community Health Worker, Male, 42 years old
Some CHWs were employed far from their place of residence but received the same transport allowance as those assigned closer to their home village. Particularly female CHWs, who typically do not drive or own motorcycles in the study area, experienced transportation challenges, as they had to cover the additional cost for a driver.
The distance is long we walk, me as a lady I don’t have a motorcycle therefore I will need to board a motorcycle (…). -Community Health Worker, Female, 30 years old
Limited transportation allowance for CHWs decreases satisfaction among Community Members, whose services are delayed and among CHWs whose requests for a raise have been denied. Providing a more independent transport solution for CHWs may simplify travelling and locating participants.
You wait for a long time for them to come. They end up coming late when you are already tired (…). -Community Member, Male, 73 years old
We have been faced with the challenge of transportation, with the increase in prices for fuel, (…) in most cases CHWs come back and request for more transport facilitation, which has been a challenge in the administrative area. -Healthcare Provider, Male, 33 years old, NGO Staff
Intervention Costs
CHWs routinely contact community leaders to help CHWs in pointing out places of residence of study participants for which community leaders expect compensation, posing a financial challenge.
We were all given UGX 10,000 to give to the chairman. (…) These people don’t help for free. Sometimes they would just direct you where the people are and they tell you to go find them yourself (…) hence facing so many hardships moving from house to house. -Community Health Worker, Female, 32 years old
COPD Medication Costs
Some participants (30.8%, n = 16) reported COPD medication cost as unaffordable in comparison to Community Member daily wages when medications were available, which led participants to express greater uptake of more affordable traditional, herbal medications instead.
The drugs (…) are a bit expensive and not all these people (…), [can] afford those drugs so they end up buying like five tabs out of 30, which means (…) the patient is not taking the drugs as they are supposed to be taken. -Healthcare Provider, Female, 26 years old, Nurse
The biggest hindrance was lack of money. You could have pain but every time you went to the clinic, they needed a lot of money. (…) This really hindered us (…), we decided to resort to local herbs, but they were not effective (…). -Community Member, Male, 38 years old
Sustainability
Participants suggested programmatic elements that may contribute to intervention sustainability and long-term continuation beyond the study period. Challenges to sustainability of the intervention included the need for decentralized COPD diagnostic and referral centers, limited CHW follow up after referral, limited CHW support, and inadequate medication provision.
Medication Provision
Community Members and CHWs both suggested a potential role for CHWs in providing medication in the community. In addition, CHWs suggested that they could continue following up Community Members and confirming their medication adherence.
The other thing is that they should also train us on which medication to give to those who are sick. Because there are people who can’t come to the clinic at all simply because they are too sick (…) If I know the medications to give (…), I would be of great help (…). -Community Health Worker, Male, 42 years old
A Community Member presented medication adherence as a challenge. Participants had expectations that the referral center would provide drugs for free. These unmet expectations led to non-adherence.
The screened and referred patients complain that the referral centers do not have drugs to treat them. (…) This stops them from going to the referral centers. -Community Health Worker, Male, 28 years old
Increase CHW Supervision, Trainings, and Incentives
Due to rising costs of inflation CHWs and HCPs alike agree that an increase in financial support for CHWs in terms of salary and incentives would lead to more effective intervention delivery.
I would change the salary and increase it, change transport allowance, (…) they should give us lunch allowance (…) because we get hungry, we work in rural areas finding a shop to purchase water its hard (…) even when it shines or rains, we still work (…). -Community Health Worker, Female, 27 years old
We go out without money for eating and transport isn’t enough, (…) we don’t get any money for lunch. -Community Health Worker, Female, 27 years old
This enhanced facilitation would motivate CHWs to fulfill their roles. Most CHWs and HCPs (77.8%, n = 14) pointed out that CHWs operate in difficult environments but are crucial for the success of the screening program.
Increase on the money paid would be a motivator. -Community Health Worker, Male, 28 years old
One thing I would change is improvement on the incentives such as wages for community health workers since the program greatly lies on their shoulders (…). -Healthcare Provider, Male, 27, Clinician
All participant groups believed that greater CHW support would allow scaling up of the intervention and inclusion of a greater number of screened Community Members. Additionally, most HCPs felt that intervention sustainability could be maintained with continued COPD training and greater supervision for CHWs.
Continuous trainings or refresher trainings. (…) This would provide a better understanding of COPD and how to go about it. -Healthcare Provider, Male, 56, Clinician
Another implementation challenge was equipment shortage. CHWs recommended keeping their equipment long-term to enable them to screen Community Members for NCDs continuously.
Equipment and supplies availability should be timely and according to the schedule of the screening processes. For instance, COPD screening was planned for three months but it lasted five months (…). To get more supplies to enable the work to go on took two weeks. -Community Health Worker, Male, 28 years old
Decentralize Screening and Referral Centers
Most Community Members (61.8%, n = 21) expressed the need for a greater number and more decentralized referral centers to increase accessibility and address Community Members’ transport barriers.
The program should consider having a central point on a particular day where all the people who need to be checked / tested and treated can converge to be attended to by the CHWs other than doing the door-to-door service. -Community Member, Female, 60 years old
CHWs supported this idea, emphasizing that ongoing village outreaches are needed to increase screening accessibility while reducing Community Members’ transportation and cost challenges.
There are those cases of people who are unable to move. You may check them today and find that this one can try to move; one day later you find they are unable to move completely. So, for such a person I suggest, they find a day and do some out reaches in the villages. -Community health worker, Female, 22 years old
Program Continuity and Follow Up
Participants raised several recommendations to ensure the screening program’s continuity. CHWs laid out their interest in continuing to follow up with referred and non-referred participants. However, as with HCPs, participants acknowledged that the current amount of CHWs is insufficient for expanding services in the screening area.
The community health workers should continue coming to carry out tests in our communities but should broaden the number of people to be tested. There are so many other people who also would really benefit from this (…). -Community Member, Female, 53 years old
Furthermore, to address the loss of screened Community Members at time of referral, most participants expressed the need for more frequent CHW follow-up and continuity of COPD care.
There should be routine follow-up checkups by the community health workers on people who were tested and referred to health facilities. -Community Member, Female, 62 years old
Moreover, financing is a major challenge for the program and the continuity of medical services. CHWs questioned how the program will be able to continue beyond the current funding.
What are they going to do in order to make sure that the community in which these programs have been implemented are going to continue receiving the services whether they have money or not? -Community Health Worker, Male, 42 years old
Discussion
COPD screening and referral programs led by CHWs are promising interventions that may reduce access barriers to primary health care in rural parts of LMICs like Uganda, where diagnostic tools are inaccessible for the majority of the population. However, prior to an intervention’s rollout, stakeholders need to consider implementation challenges that may halt a program’s success. This is the first study in Sub-Saharan Africa to evaluate challenges of implementing a CHW-led COPD intervention using robust qualitative methodology. Among Community Members, CHWs, and HCPs, we found that challenges to implementation included a lack of COPD awareness in the community, a perceived lack of utility of COPD screening, and stigma surrounding the diagnostic process. Participants expressed that Community Member accessibility and willingness to participate in the COPD diagnostic process limited programmatic impact. The high patient volume and fragmented, time intensive diagnostic and referral process impeded implementation given local realities. The rising cost of transportation appeared to be the greatest barrier to effective implementation. Participants in all cadres identified avenues for improvement to promote sustainability including increasing CHW support, increasing COPD medication access, decentralizing COPD diagnosis and treatment, and strengthening program follow-up.
As our findings indicate, a community-led program may face challenges in acceptability due to the lack of COPD awareness in the community. Previous Ugandan studies indicate a low awareness or knowledge of COPD leading to barriers in accessing and accepting screening services.9,29–31 Building on this, the limited perceived utility of participating in the COPD screening process, which Community Members repeatedly expressed, further impedes community-based screening. Potential lack of trust in CHWs also plays a role in shaping Community Members’ perceptions. Interestingly, however, the lack of perceived utility of screening and lack of community trust expressed by CHWs and HCPs were discordant from Community Members, with community participants demonstrating lower frequency of concern compared to CHWs and HCPs. In addition, stigma-associated with respiratory diseases in Uganda (ie, TB, COVID-19) and the similarity of symptoms in these diseases and COPD may decrease the acceptability of Community Members’ screening participation. Similar concerns have previously been documented in a qualitative study in Malawi that describes stigma related to CHW interventions for infectious diseases or early pregnancies.32 Findings from the Malawi study indicate that through the establishment of long-term relationships with CHWs, CHW associated stigma can be mitigated while care and treatment improve. Building on this study, we argue that challenges on acceptance of CHW services due to stigma or trust can be reduced through positive interpersonal, trust-based relationships between Community Members and CHWs. By incorporating stakeholders from all levels in formative research interventions -prior to an intervention’s rollout- potential challenges related to trust and stigma can be addressed. In addition, solutions such as how to nurture trustful collaborations can be developed jointly. Moreover, we argue that continuous patient-centered health education efforts are imperative to raise patients’ awareness to COPD screening services and thus agency in self-management.33,34
Previous studies have demonstrated the feasibility of CHW-delivered education for COPD in rural Ugandan settings.31 We argue that interventions need to be accompanied by basic, yet comprehensive education packages, delivered by CHWs. These education components may strengthen Community Members’ acceptance and adoption of proposed COPD interventions while reducing perceived stigma that is often present when utilizing community-based COPD care.30 An effective COPD management intervention delivered by female community health volunteers in Nepal similarly found Community Members were responsive and viewed home-based COPD care favorably.35 Therefore, to effectively treat and manage COPD in LMICs, it is vital that Community Members with COPD gain knowledge about COPD and agency to implement these COPD self-management skills from trusted CHWs.
The cost of CHW-delivered NCD or COPD programs continues to inhibit program implementation as budget allocation for CHW programs is limited.36 As our findings present, CHW-led programs require sustainable financial support to be effectively implemented to fund integration of local government support and medication provision. We found all participants described increasing transportation costs that are inherent with a community-based screening program. This challenge aligns with a costing analysis of a CHW program in rural Nepal that identified transportation cost as a main obstacle.37 Transportation facilitation for CHWs has also been classified as a major challenge in a prior qualitative study in rural Uganda, which assessed the rollout of a cardiovascular disease prevention program.38 Our results highlight this challenge as participants at all levels recognized transportation to referral centers for further COPD diagnostics and care as unaffordable. To limit the transportation challenges of individual Community Members, participants proposed to decentralize the referral centers. We recommend that by offering more localized spirometry screening services, transportation and time challenges ofCommunity Members can be minimized while scaling up services. Moreover, intervention and medication-related costs might strain an already fragile health system underfunded in NCD prevention and CHW programs. The continuing financial dependency on donor support for CHW program financing poses a risk on the sustainability of these efforts and increases the need for policy change, prioritizing NCDs such as COPD by national governments.36
Strengths and Limitations
There were several study strengths and limitations. Data collection took place in natural settings at familiar clinical settings and workplaces providing a conducive environment for open expression of participants to share their experiences. Furthermore, local research assistants conducted these interviews in the language preferred by the participant. Through the inclusion of Community Members, CHWs and HCPs, all stakeholders that had previous training and/or experience in screening for various NCDs including COPD, we generated a holistic view on community-based COPD screening in rural Uganda. This study is part of a set of mixed-methods studies conducted within a unique rural Ugandan cohort, assessing the usefulness of CHW-led NCD screening and management interventions that allow for the longitudinal observation of disease progression and interventions effectiveness.25,39,40
One limitation of this study was that purposive sampling might have yielded HCPs, CHWs, and Community Members with greater knowledge and awareness of COPD to participate in the study. Moreover, the compensation of participants, which was a requirement imposed by the local Institutional Review Board, also poses a limitation as it is unlikely to be applicable to real life settings of COPD screening in LMICs, where healthcare funding is limited.
While the research team was mindful to avoid participants at risk of bias responses, due to the small size of the local team, some of the CHWs and HCPs held leadership positions within, which could lead to expressing experiences that are more favorable rather than intervention challenges. Another limitation is that the study is limited to a unique research site in rural Uganda, which has been running community-based programs and research studies for many years. The reputation of the research site and implementing organization may have shaped the responses of particularly Community Members and CHWs. Due to the choice of framework, the study may have focused on certain themes while others were neglected. As a qualitative study, there may be limitations in scaling these results to different contexts or LMICs.
Conclusion
Understanding the challenges of CHW-led COPD screening and referral interventions is key to addressing the growing burden of COPD in LMIC settings like Uganda. In resource-constrained settings, where the access to COPD care is limited, community-based screening and referral programs are promising tools, but we recommend these programs consider implementation barriers at all stakeholder levels and incorporate feedback from these stakeholders. By addressing these challenges, CHW-led community-based COPD programs have the potential to create sustainable infrastructure to identify and empower Community Members to access COPD care, self-manage their condition, and thus improve COPD-related outcomes. Our findings highlight the need for localized evidence-based approaches to CHW-led COPD interventions and increased sustainable access to funding to implement these interventions long term.
Acknowledgments
The content has been previously presented as a poster at the European Public Health Conference and published as a conference abstract supplement (doi: 10.1093/eurpub/ckad160.1349).
Funding
This study was funded by the Else Kröner-Fresenius-Stiftung (2019_HA178). The funding agency had no role in the design of the study or collection, analysis, interpretation of data, and in writing the manuscript.
Disclosure
The authors report no conflicts of interest for this work.
References
1. IHME IfHMaE. Global burden of disease collaborative network, global burden of disease study 2019 (gdb 2019) results. Available from: https://vizhub.healthdata.org/gbd-results/.
2. World Health Organization. Chronic obstructive pulmonary disease (COPD). 2023. Available from: https://www.who.int/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-copd.
3. Alwan A. Global Status Report on Non-Communicable Diseases. World Health Organization; 2010.
4. Quaderi SA, Hurst JR. The unmet global burden of COPD. Glob Health Epidemiol Genom. 2018;3:e4. doi:10.1017/gheg.2018.1
5. Siddharthan T, Grigsby M, Morgan B, et al. Prevalence of chronic respiratory disease in urban and rural Uganda. Bull World Health Organ. 2019;97(5):318–327. doi:10.2471/BLT.18.216523
6. van Gemert F, Kirenga B, Chavannes N, et al. Prevalence of chronic obstructive pulmonary disease and associated risk factors in Uganda (FRESH AIR Uganda): a prospective cross-sectional observational study. Lancet Glob Health. 2015;3(1):e44–51. doi:10.1016/S2214-109X(14)70337-7
7. World Health Organization. General availability of peak flow measurement spirometry at the primary health care level; 2023. Available from: https://www.who.int/data/gho/data/indicators/indicatordetails/GHO/general-availability-of-peak-flow-measurementspirometry-at-the-primary-health-care-level.
8. Rossaki FM, Hurst JR, van Gemert F, et al. Strategies for the prevention, diagnosis and treatment of COPD in low- and middle- income countries: the importance of primary care. Expert Rev Respir Med. 2021;15(12):1563–1577. doi:10.1080/17476348.2021.1985762
9. Robertson NM, Nagourney EM, Pollard SL, et al. Urban-rural disparities in chronic obstructive pulmonary disease management and access in Uganda. Chronic Obstr Pulm Dis. 2019;6(1):17–28. doi:10.15326/jcopdf.6.1.2018.0143
10. Nagourney EM, Robertson NM, Rykiel N, et al. Illness representations of chronic obstructive pulmonary disease (COPD) to inform health education strategies and research design-learning from rural Uganda. Health Educ Res. 2020;35(4):258–269. doi:10.1093/her/cyaa016
11. Ruppel GL, Carlin BW, Hart M, Doherty DE. Office spirometry in primary care for the diagnosis and management of copd: national lung health education program update. Respir Care. 2018;63(2):242–252. doi:10.4187/respcare.05710
12. Nihlen U. Detection of chronic obstructive pulmonary disease (COPD) in primary health care: role of spirometry and respiratory symptoms. Scand J Prim Health Care. 1999;17(4):232–237. doi:10.1080/028134399750002467
13. Van Schayck CP. Detecting patients at a high risk of developing chronic obstructive pulmonary disease in general practice: cross sectional case finding study. BMJ. 2002;324(7350):1370. doi:10.1136/bmj.324.7350.1370
14. Yawn BP, Enright PL, Lemanske RF Jr, et al. Spirometry can be done in family physicians’ offices and alters clinical decisions in management of asthma and COPD. Chest. 2007;132(4):1162–1168. doi:10.1378/chest.06-2722
15. Joo MJ, Sharp LK, Au DH, Lee TA, Fitzgibbon ML. Use of spirometry in the diagnosis of COPD: a qualitative study in primary care. COPD. 2013;10(4):444–449. doi:10.3109/15412555.2013.766683
16. Jeet G, Thakur JS, Prinja S, Singh M. Community health workers for non-communicable diseases prevention and control in developing countries: evidence and implications. PLoS One. 2017;12(7):e0180640. doi:10.1371/journal.pone.0180640
17. Miles A, Reeve MJ, Grills NJ. Effectiveness of community health worker-delivered interventions on non-communicable disease risk and health outcomes in India: a systematic review. Christian J Global Health. 2020;7(5):31–51. doi:10.15566/cjgh.v7i5.439
18. Lin JS, O’Connor E, Evans CV, Senger CA, Rowland MG, Groom HC. Behavioral counseling to promote a healthy lifestyle in persons with cardiovascular risk factors: a systematic review for the U.S. preventive services task force. Ann Intern Med. 2014;161(8):568–578. doi:10.7326/M14-0130
19. Joshi R, Alim M, Kengne AP, et al. Task shifting for non-communicable disease management in low and middle income countries--a systematic review. PLoS One. 2014;9(8):e103754. doi:10.1371/journal.pone.0103754
20. Siddharthan T, Pollard SL, Quaderi SA, et al. Discriminative accuracy of chronic obstructive pulmonary disease screening instruments in 3 low- and middle-income country settings. JAMA. 2022;327(2):151–160. doi:10.1001/jama.2021.23065
21. Jarhyan P, Hutchinson A, Khatkar R, et al. Diagnostic accuracy of a two-stage sequential screening strategy implemented by community health workers (CHWs) to identify individuals with copd in rural India. Int J Chron Obstruct Pulmon Dis. 2021;16:1183–1192. doi:10.2147/COPD.S293577
22. DeJong SR, Veltman RH. The effectiveness of a CNS-led community-based COPD screening and intervention program. Clin Nurse Spec. 2004;18(2):72–79. doi:10.1097/00002800-200403000-00012
23. Parekh TM, Copeland CR, Dransfield MT, Cherrington A. Application of the community health worker model in adult asthma and COPD in the U.S.: a systematic review. BMC Pulm Med. 2019;19(1):116. doi:10.1186/s12890-019-0878-7
24. Uganda Bureau of Statistics. National population and housing census. Available from: https://www.ubos.org/explore-statistics/.
25. Siddharthan T, Kalyesubula R, Morgan B, et al. The rural Uganda non-communicable disease (RUNCD) study: prevalence and risk factors of self-reported NCDs from a cross sectional survey. BMC Public Health. 2021;21(1):2036. doi:10.1186/s12889-021-12123-7
26. Proctor E, Silmere H, Raghavan R, et al. Outcomes for implementation research: conceptual distinctions, measurement challenges, and research Agenda. Adm Policy Ment Hlth. 2011;38(2):65–76. doi:10.1007/s10488-010-0319-7
27. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res. Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
28. Patton MQ. Qualitative Evaluation and Research Methods. Sage Publications; 1990.
29. Katagira W, Jones AV, Orme MW, et al. Identifying appropriate delivery of and referral to pulmonary rehabilitation in Uganda: a survey study of people living with chronic respiratory disease and health care workers. Int J Chron Obstruct Pulmon Dis. 2021;16:2291–2299. doi:10.2147/COPD.S314849
30. van Gemert F, Chavannes N, Nabadda N, et al. Impact of chronic respiratory symptoms in a rural area of sub-Saharan Africa: an in-depth qualitative study in the Masindi district of Uganda. Prim Care Respir J. 2013;22(3):300–305. doi:10.4104/pcrj.2013.00064
31. Jones R, Kireng B, Buteme S, Williams S, van Gemertzs F. A novel lung health programme addressing awareness and behaviour-change aiming to prevent chronic lung diseases in rural Uganda. Afr J Respir Med. 2019;14(2):2–9.
32. Ndambo MK, Munyaneza F, Aron M, Makungwa H, Nhlema B, Connolly E. The role of community health workers in influencing social connectedness using the household model: a qualitative case study from Malawi. Glob Health Action. 2022;15(1):2090123. doi:10.1080/16549716.2022.2090123
33. Robertson NM, Siddharthan T, Pollard SL, et al. Development and validity assessment of a chronic obstructive pulmonary disease knowledge questionnaire in low- and middle-income countries. Ann Am Thorac Soc. 2021;18(8):1298–1305. doi:10.1513/AnnalsATS.202007-884OC
34. Wang LH, Zhao Y, Chen LY, Zhang L, Zhang YM. The effect of a nurse-led self-management program on outcomes of patients with chronic obstructive pulmonary disease. Clin Respir J. 2020;14(2):148–157. doi:10.1111/crj.13112
35. Adhikari TB, Neupane D, Karki A, et al. Community-based intervention for prevention and management of chronic obstructive pulmonary disease in Nepal (COBIN-P trial): study protocol for a cluster-randomized controlled trial. Trials. 2021;22(1):474. doi:10.1186/s13063-021-05447-7
36. Masis L, Gichaga A, Zerayacob T, Lu C, Perry HB. Community health workers at the dawn of a new era: 4. programme financing. Health Res Policy Syst. 2021;19(Suppl 3). doi:10.1186/s12961-021-00751-9
37. Nepal P, Schwarz R, Citrin D, et al. Costing analysis of a pilot community health worker program in rural Nepal. Glob Health Sci Pract. 2020;8(2):239–255. doi:10.9745/GHSP-D-19-00393
38. Ndejjo R, Musinguzi G, Nuwaha F, Wanyenze RK, Bastiaens H. Acceptability of a community cardiovascular disease prevention programme in Mukono and Buikwe districts in Uganda: a qualitative study. BMC Public Health. 2020;20(1):75. doi:10.1186/s12889-020-8188-9
39. Ingenhoff R, Nandawula J, Siddharthan T, et al. Effectiveness of a community health worker-delivered care intervention for hypertension control in Uganda: study protocol for a stepped wedge, cluster randomized control trial. Trials. 2022;23(1):440. doi:10.1186/s13063-022-06403-9
40. Ingenhoff R, Munana R, Weswa I, et al. Principles for task shifting hypertension and diabetes screening and referral: a qualitative study exploring patient, community health worker and healthcare professional perceptions in rural Uganda. BMC Public Health. 2023;23(1):881. doi:10.1186/s12889-023-15704-w
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.