Back to Journals » Orthopedic Research and Reviews » Volume 17
Challenges for the Female Surgeon in Orthopedic Surgery – A Scoping Review
Authors Alrumaidhi Y, Alenizi N, Almulla N, Almousa Z, Alenezi D, Lari A ![]()
Received 13 March 2025
Accepted for publication 21 August 2025
Published 6 September 2025 Volume 2025:17 Pages 451—464
DOI https://doi.org/10.2147/ORR.S524482
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Clark Hung
Yasmen Alrumaidhi, Norah Alenizi, Nawar Almulla, Zainab Almousa, Danah Alenezi, Ali Lari
Department of Orthopedic Surgery, AlRazi National Orthopedic Hospital, Kuwait City, Kuwait
Correspondence: Yasmen Alrumaidhi, Email [email protected]
Background: The number of female doctors graduating from medical schools worldwide is increasing; however, orthopedic surgery remains one of the least gender-diverse surgical fields.
Objective: This scoping review aims to map the literature on the challenges faced by female orthopedic surgeons, categorize them into key domains, and identify essential gaps to guide future research and institutional reform.
Methods: A scoping review study design was employed, utilizing the Arksey and O’Malley framework. PubMed, Scopus, and Web of Science were searched for articles published between January 2000 and 2024. Papers that addressed challenges faced by female orthopedic residents and surgeons were included; of the studies screened, 92 met the inclusion criteria.
Results: Challenges were discussed in three main domains: female representation, the health and occupational risks, and the emotional environment. Approximately 23 challenges were identified. While the increase in female representation in orthopedic surgery more than doubled between 2000 and 2020, gender disparity persists. Musculoskeletal injuries were identified as the most common occupational health concern. Microaggressions were described in several forms: verbal comments, assumptions about skills, traditional role stereotypes, sexist language, and exclusion from informal networks.
Limitations: The study’s limitations include unexplored multiple challenges due to the limited availability of data, such as unequal pay, patient preferences, and military orthopedic care. Most of the included studies were cross-sectional surveys, which limits generalizability and causal inference.
Conclusion: This review highlights the persistent gender-related challenges in the field of orthopedic surgery. Initiatives for mentorship and representation are in place and appear promising. Nonetheless, challenges related to occupational safety, well-being support, and leadership roles remain inadequately addressed. Future efforts must prioritize mentorship, ergonomic equipment design, strategies to address microaggressions, and institutional commitment to support female orthopedic surgeons.
Keywords: female orthopedic surgeon, gender disparity, orthopedic residency, barriers, women in surgery
Introduction
Gender disparities persist across surgical specialties. Currently, only one-third of surgeons worldwide are women.1 Despite progress in female representation within surgical fields, they are still underrepresented in many domains, orthopedic surgery in particular.2 This raises concerns, especially given that women currently make up more than 50% of medical school graduates worldwide.3 These statistics highlight a gender imbalance that persists in medical education, particularly within surgical fields.
Orthopedic surgery is considered one of the least diverse fields of surgery.4 Historically, orthopedic surgery has been associated with physical strength and masculine identity, and progress in dismantling these stereotypes has been slow.5 The practicing female orthopedic surgeons account for only 16% in Canada, 6.9% in the United Kingdom, 6.5% in the United States, and only 1% in India.6–8 Some individuals may wonder about the reasons these figures are alarming. Numerous studies regarding group performance demonstrate that workforces characterized by diversity in aspects such as gender, race, and ethnicity yield enhanced decision-making processes and superior outcomes.5
While the literature has explored challenges faced by female orthopedic surgeons, such as mentorship, physical demands, pregnancy-related concerns, and more, the evidence remains fragmented and lacks a comprehensive synthesis.9–11 There is limited research exploring the perspectives of female orthopedic surgeons on these challenges and their related outcomes. Furthermore, the lack of research on the long-term impact of these challenges on female surgeons’ careers, patient care, and training environment is another noteworthy gap in the literature.
To address these gaps, this scoping review was designed. While systematic reviews typically focus on evaluating the quality or effectiveness of interventions, a scoping review is more appropriate for this topic. This is because the aim is to map a broad, complex field where the evidence is emerging. Given the heterogeneity in the study types, ranging from qualitative to national surveys, a scoping review was chosen to collect and categorize the existing evidence on the obstacles faced by female orthopedic surgeons.
Understanding these challenges not only promotes gender equality but also has direct implications for patient care, workforce diversity, and the sustainability of the orthopedic profession.5,12 Gender-related barriers can directly influence career satisfaction and surgical performance, ultimately affecting clinical outcomes.
This paper aims to systematically map the professional, cultural, and structural challenges reported in the literature and to identify gaps in knowledge, highlight areas for future research, and interventions. The challenges will be analysed by subcategorization into three main domains: female representation, the health and occupational concerns and the emotional environment.
Methodology
For this topic, it was found that there was wide variation in the evidence and research design in the literature. Therefore, a scoping review study design was chosen, utilizing the Arksey and O’Malley framework.13
Search Strategy
A scoping review was conducted using Covidence software.14 The following databases were used in the search: PubMed, Scopus, and Web of Science. This search included studies published between January 2000 and December 2024.
Keywords used included: female orthopedic surgeon, gender disparity, orthopedic residency, barriers, women in surgery.
Eligibility Criteria
Studies that met the following criteria were included: 1) Studies mentioned one or more of the challenges faced by female orthopedic surgery residents. 2) Statistics or records mentioning the female representation in orthopedic surgery.
Excluded studies: 1) Personal commentaries or opinion articles, 2) Challenges in orthopedic surgery fellowships, 3) Studies that included medical student perspectives only and did not include residents or qualified orthopedic surgeons in the population, 4) Symposium study design.
Study Screening
Covidence was also used for screening the articles. With the use of Covidence and our team, two reviewers independently screened both titles and abstracts, voted to include or exclude each paper, and a third member voted only if there was any conflict.
Data Extraction and Collection
The data were extracted from the papers using Microsoft Excel (Microsoft, Redmond, Washington, USA). Extracted data included: title, country, study type, population, methods, challenges included in the paper facing female orthopedic surgeons, and the conclusions reached. A total of 92 studies were included in the main Excel sheet (Appendix 1). A further subdivision of the data was performed to facilitate data analysis. Three domain-specific tables were created, covering female representation, emotional environment, and health concerns, each with three columns: author name, study design, and challenges included. For the female representation domain, 50 studies were isolated from the primary data that discussed the female representation in orthopedic surgery, mentorship, and leadership challenges (See Appendix 2). The emotional environment, which is the second domain, was also isolated from the primary dataset and included 23 papers (See Appendix 3). The third domain, health challenges, on the other hand, comprised 20 papers (See Appendix 4).
Results
Firstly, as described in Figure 1, the PRISMA framework for scoping reviews is presented.14 Screening was conducted using Covidence software, and the initial number of studies identified was 4785. After duplication was removed, the total number was 4516. The second step of the literature search was screening, which ended with a total of 1016. Furthermore, the studies were assessed for eligibility through a full-text review, applying the eligibility criteria outlined in the methods section. Finally, 92 studies were included in this paper (see Appendix 1).
 |
Figure 1 Literature search and method for the scoping review. Notes: PRISMA figure adapted from Tricco AC, Lillie E, Zarin W, et al. Prisma extension for scoping reviews (PRISMA-SCR): checklist and explanation. Ann Internal Med. 2018;169(7):467–473. Creative Commons.14 |
There were around 23 challenges mentioned in the papers that were included in this scoping review. These challenges include representation, mentorship, academic/ research opportunities, work-life balance, leadership roles, bias, fertility/parenthood issues, mental health impacts, career advancement opportunities, recruitment effort, microaggression, unequal pay, radiation/cancer, occupational injuries, inappropriate interview questions, difficulty networking, technical difficulties, patients’ preference, military orthopedics, conflicts, and fellowship choice. The most commonly discussed challenge in the literature was the underrepresentation of women in orthopedic surgery (Figure 2). Lower-frequency but still significant challenges included unequal pay, patients’ preferences for female or male orthopedic surgeons, and military orthopedics.
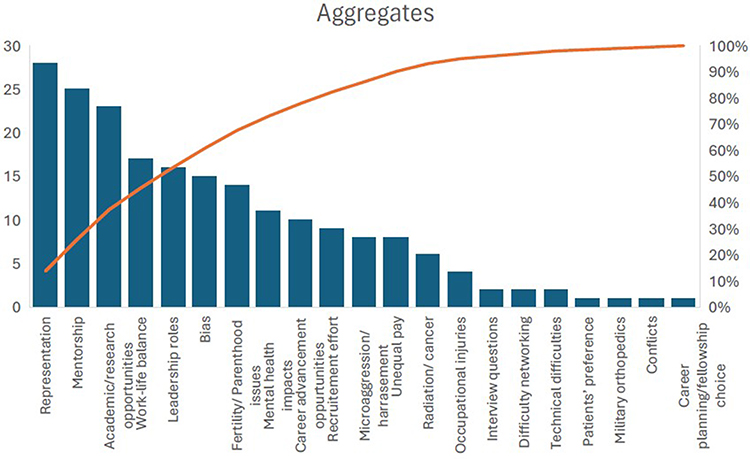 |
Figure 2 Pareto graph aggregates of the challenges for female orthopedic surgeons in residency mentioned in the literature. |
(Figure 3) highlights the trends in female representation in orthopedic surgery from 2000 to 2020. There was an increase from 6% in 2000 to more than double in 2020 (15%). Over the past 20 years, the trend has shown a consistent and linear increase from 2000 to 2010, followed by a sharper increase in the subsequent five years (2010–2015).
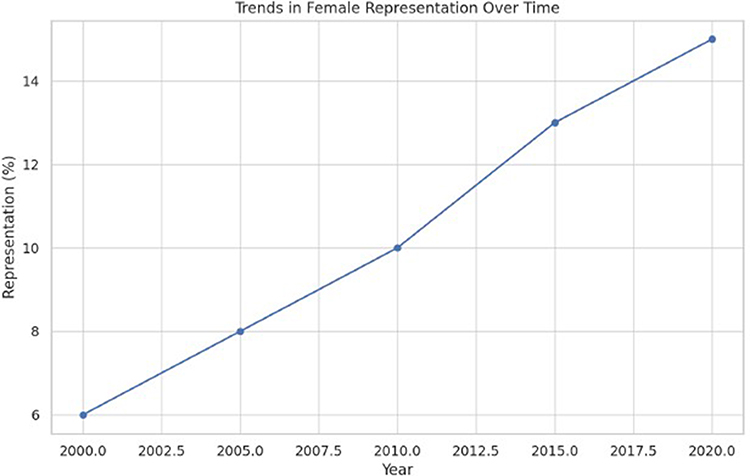 |
Figure 3 Trends in Female Representation in Orthopedic Surgery (2000–2020). |
Figure 4 summarizes the reported health challenges for female orthopedic surgeons. These challenges include breast cancer risk, radiation exposure concerns, ergonomic mismatch, musculoskeletal injuries, and pregnancy complications. Musculoskeletal injuries were the most frequently reported health challenge. Radiation exposure concerns and ergonomic mismatch were equally reported across the included papers. Breast cancer risk and pregnancy complications were identified as notable health concerns.
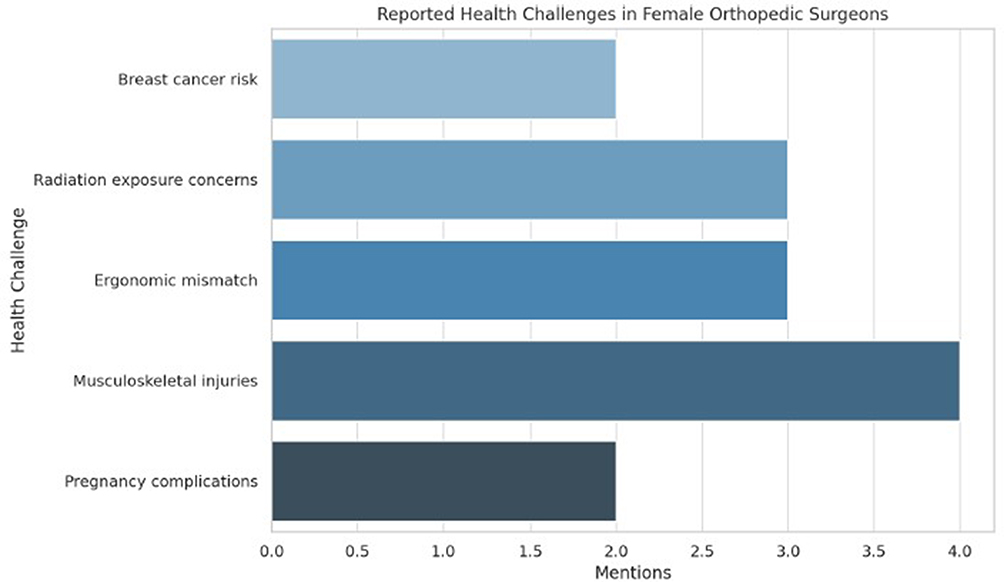 |
Figure 4 Reported Health Challenges in Female Orthopedic Surgeons. |
Papers discussing microaggressions describe them in the following forms: verbal comments, assumptions about skills, traditional role stereotypes, sexist language, and exclusion from informal networks (Figure 5). Verbal comments were the most commonly reported form of microaggression cited in 17 studies. Assumptions about skill were reported in 13 studies by female respondents. Male reports of microaggressions were minimal in the literature. There were no male reports of microaggressions related to traditional roles, stereotypes, and sexist language in orthopedic surgery.
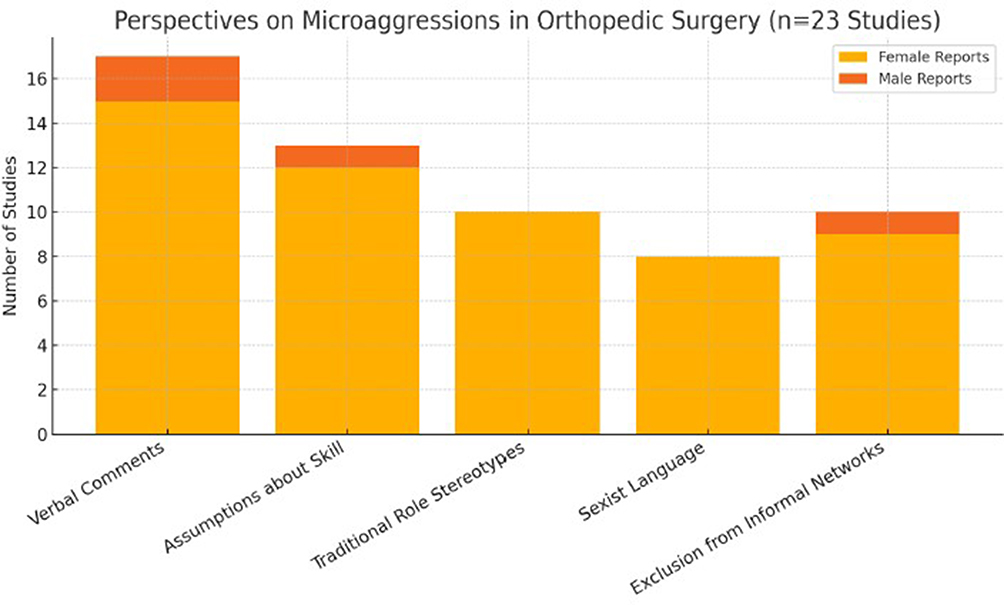 |
Figure 5 Perspectives on Microaggressions in Orthopedic Surgery. |
Discussion
Representation, Mentorship, and Leadership
Representation, mentorship, and leadership opportunities are interconnected pillars that influence the visibility, recruitment, and retention of women in orthopedic surgery. These challenges were widely discussed in the literature, primarily through observational studies, survey-based articles, and institutional reports. Each has been cited both as a standalone barrier and as part of a broader cultural gap in orthopedic training and practice.
Representation, defined in this paper as the presence of female residents and faculty in orthopedic programs, remains significantly lower compared to male counterparts. Bowe et al (2021) highlighted the ongoing lack of a clear understanding regarding the root causes of underrepresentation.15 Between 2009 and 2014, nearly 50% of US orthopedic surgery programs trained fewer than 10% of their residents as females. More recent data from Julian et al (2023) show an increase to 19.2%, which is encouraging, but still far from equitable, especially when compared to international trends in other surgical specialties.16
Projections about the timeline to gender equity are inconsistent. Acuña et al (2021) estimated it would take over 200 years to reach gender parity, while Pinpin et al (2023) predicted it could be achieved by 2038.17,18 These contrasting projections highlight the uncertainty and complexity of progress in this area. Speculations of the more ambitious projection may be attributed to the interventions implemented by Initiatives such as the Ruth Jackson Orthopedic Society, the Perry Initiative, and the AAOS Diversity Advisory Board, which have aimed to promote orthopedic surgery to women.19–21 While it was suggested that increasing the number of female graduating doctors would naturally increase their presence in the surgical fields, current trends indicate that a passive demographic shift is insufficient without systemic and cultural reform.
Surveys consistently identify a lack of representation as one of the top three perceived barriers to women entering orthopedic surgery.22 Multiple studies observed that programs with female residents or faculty had higher rates of female applicants, suggesting a positive effect on recruitment. In certain studies, it was mentioned that being the “only woman” led to feelings of isolation or increased pressure to act as a role model without adequate support.9 These observations underscore the need to examine whether visibility alone is sufficient or whether broader institutional and cultural changes are also necessary.
In response, numerous national and institutional organizations have led efforts to improve representation. Initiatives like the Ruth Jackson Orthopedic Society, the Perry Initiative, and the AAOS Diversity Advisory Board aim to promote orthopedic surgery to women through early exposure, workshops, and networking.19–21 Programs also introduced outreach to medical students, updated website content to reflect diversity, and launched women-in-orthopedics groups.19–21 These initiatives are promising and have received positive feedback from participants; however, these efforts currently lack a long-term assessment of their effectiveness.
Mentorship in surgical specialties is one of the most critical determinants of success. Its absence in this context was cited as one of the main challenges in the reviewed literature.23–26 It directly affects career progression, limits research output, reduces confidence in surgical performance, and hinders access to leadership positions.27 Conversely, effective mentorship was linked to better retention, research productivity, and overall satisfaction with training.
Several structured efforts have been developed to improve mentorship for female orthopedic surgeons. The Ruth Jackson Orthopedic Society established formal mentorship programs pairing female residents and students with experienced female surgeons across the United States.20 Additionally, residency programs have initiated their internal mentorship pairings, while national conferences now also include mentorship and workshops.28,29 Other forms of support were also available on digital platforms, such as Women in Orthopedics Worldwide, which provided webinars and peer support forums.4 Despite these significant efforts, the reach remains limited due to the small number of senior female faculty and the reliance on voluntary participation. There is growing advocacy for mentorship to be formally integrated into the academic workload, rather than being treated as informal or optional.
Gender disparity in leadership positions persists in the field of orthopedic surgery. Women occupy only 9% of leadership roles in orthopedic surgery, a figure that has remained substantially unchanged over the past decade.30 Data from surveys indicates that many female surgeons reported being overlooked for promotions or leadership positions because of their gender.31–33 Nevertheless, it is believed that promotion may also be influenced by factors such as research productivity, time off during training, and differing professional priorities.
Some studies found that institutions with more women in leadership positions have a positive correlation with recruitment.34,35 This suggests that visibility at senior levels may help rectify the underrepresentation of women. To ensure the long-term sustainability of this positive trend, the structures need to be reformed, such as implementing transparent promotion criteria and bias mitigation strategies.
Additionally, several leadership-focused efforts have emerged, including the AAOS Leadership Institute and internal leadership development programs at some centers.21 They aim to equip female surgeons with skills, visibility, and support for their career advancement. However, these programs have not been formally evaluated for their long-term effectiveness.
Health Impacts and Occupational Injuries in Orthopedic Surgery
Occupational and health challenges in orthopedic surgery are extensive and affect both male and female surgeons. However, women face unique risks related to radiation exposure, musculoskeletal injuries, and ergonomic mismatch, many of which are underrecognized or insufficiently addressed by current institutional policies and equipment design companies (Figure 4).
Radiation Exposure and Breast Cancer Risk in Women
Radiation exposure is an occupational hazard faced by both male and female orthopedic surgeons, especially during fluoroscopy-heavy procedures such as trauma and minimally invasive spine surgeries. 86 While both male and female surgeons are exposed to radiation, multiple studies suggest that female surgeons may face increased health consequences, particularly concerning breast cancer risk.
A 2010 study reported a 2.9-fold increased prevalence of breast cancer in female orthopedic surgeons compared to the general population.36 A follow-up study found the risk had increased further to a 3.97-fold elevation relative to age-matched controls in 2023.36 It is hypothesized that the contributing factors include inadequate radiation shielding due to poorly fitting lead aprons, apron gapping near breast tissue, and positioning of the surgeon during surgery that may increase chest exposure to radiation.37
Concerns about radiation exposure, fertility, and pregnancy have led some female residents to implement precautionary strategies to limit exposure.38 These strategies include avoiding high-radiation subspecialties and altering their caseload.39 Despite these challenges, radiation safety protocols remain generalized for males and females in orthopedic surgery and are not tailored to gender-specific risks. Proposed strategies to limit the radiation occupational hazards for female orthopedic surgeons include better-fitting protective equipment designed for female anatomy, consistent access to thyroid and ovarian shields, and more precise radiation exposure tracking during pregnancy.
Current Radiation Exposure Guidelines for Females
The International Commission on Radiological Protection (ICRP) recommends a dose limit for radiation exposure for pregnant workers of less than 1 mSv for the remainder of the pregnancy. The National Council on Radiation Protection and Measurement (NCRP) provides guidelines on radiation protection for the abdomen and thyroid, as well as badge monitoring for pregnant workers.40 Additionally, the American College of Radiology and the American College of Obstetrics and Gynecology emphasize the importance of fitted shields for females.41,42 Gender-specific fit of aprons and ergonomic adjustment to avoid breast and ovarian cancer remains a gap in the literature. Transparent and standardized guidelines are needed to evaluate their effectiveness.
Musculoskeletal Injuries and Ergonomic Challenges
Female orthopedic surgeons report higher rates of musculoskeletal injuries compared to their male colleagues. The areas commonly affected include the hands, shoulders, neck, and lower back. In a 2022 national survey, around 68% of female orthopedic surgeons reported at least one occupational injury.43
Ergonomic mismatch between commonly used orthopedic tools and the physical characteristics of female users has been described as one of the main contributors. The design of surgical instruments is based on average male grip strength and hand size, making them more difficult for many females to use efficiently and safely.44 Additionally, shorter stature may lead to poor posture and increased overextension during procedures, further increasing the risk of injury.45
Some argue that women have a lower threshold for reporting such injuries.46 However, qualitative data confirm that many women actively modify their techniques to compensate for shortcomings in equipment design.47 Such practice adaptations lead to repetitive strain and long-term musculoskeletal damage.47 Future research is needed to answer the question of whether frequent reporting is due to injury or a lower threshold for reporting among females.
Proposed solutions to musculoskeletal injuries for female surgeons are limited.48 While some academic centers have begun offering ergonomic assessments and advocating for gender-inclusive instrument design, these initiatives remain underreported and insufficiently evaluated in the literature for their effectiveness.48 There is a lack of prospective data evaluating whether these strategies reduce injury rates or improve career longevity for female surgeons.
Comparative Health Impacts Among Male Orthopedic Surgeons
Male orthopedic surgeons’ radiation exposure risk has also been documented in the literature. One study implied an association between radiation exposure and a low male-to-female sex ratio among offspring.49 Another paper measuring radiation doses in invasive spinal surgery reported higher exposure on the genitals and hands of the surgeons, emphasizing the need for comprehensive protective measures.50
While female orthopedic surgeons face unique risks, male orthopedic surgeons are not immune to musculoskeletal injuries. Studies have shown elevated rates of low back pain, neck strain, and hand injuries among male surgeons as well, though at a lower rate compared to female surgeons.32
Emotional Environment
The emotional environment in orthopedic surgery significantly shapes the learning experience, professional growth, and the mental well-being of residents and practicing surgeons. Mental health impacts, gender bias, and microaggressions are the three most reported challenges in this context. While the literature presents strong evidence of their presence and impact, interpretations of such challenges can vary, and institutional responses are still evolving.
Mental Health Impacts
Many female surgeons have reported through several survey studies the mental health impacts that this career has had on them. In a survey study of 373 female orthopedic surgeons, around 11% reported depression, 19% anxiety, and 23% experienced burnout.51 A survey-based research conducted in the United States also highlighted the burnout, anxiety, and depression among both male and female orthopedic surgeons.52 In comparison, burnout rates for female surgeons in other surgical disciplines, such as general surgery and obstetrics and gynecology, were also significantly high (42% and 100%, respectively).53 Moreover, higher rates of psychological distress and burnout were reported in female compared to male orthopedic surgeons.54 Factors contributing to higher psychological issues among females were suggested in literature to be due to: lack of mentorship, females often work more hours and internalize negative stereotypes about women’s capabilities. Another mental health impact reported was social isolation among female orthopedic surgeons.9,54,55 These reports are concerning, especially with the potential negative impact on patients’ safety, academic productivity, surgical performance, and personal life implications. There remains a significant gap in the current institutional response to the mental well-being of female orthopedic residents. For instance, many residency programs still lack formal, structured wellness programs.
Gender Bias
Gender bias in orthopedic surgery is one of the most commonly described issues faced by female orthopedic surgeons, affecting various aspects of the training environment. Many women describe experiencing a male-dominated culture in the operating room, where exclusionary behaviors, stereotypes, and dismissive attitudes are not uncommon.51,56 Many women have reported feeling as though they must prove their competence repeatedly to gain the same recognition as their male peers. Implicit bias has also been linked to often manifesting as assumptions about physical capability, particularly regarding height, grip strength, and the ability to handle equipment.44
Bias in career advancement is another significant barrier for female orthopedic surgeons. Women in orthopedics have reported bias in access to leadership positions compared to their male colleagues, which has harmed their job satisfaction.9 A survey conducted in the United States and Canada reported gender bias in speaking opportunities at technical conferences and representation on editorial boards,9,22,57 Bias related to pregnancy and parenthood has also been documented, with some women feeling penalized for taking maternity leave or being viewed as less committed to the specialty.44,58
However, not all women have these experiences in orthopedic surgery. Reports of positive, supportive environments where they feel valued and encouraged in some initiatives.9 Some theories suggest that bias has decreased over the past decade due to growing awareness and cultural change within the field.59 Male surgeons also expressed support for initiatives promoting gender equity. Some express concerns about reverse bias or the potential for overcorrection in recruitment and promotion practices.60 These varying perspectives suggest that bias, while real and impactful, may manifest differently depending on the institutional culture and the individuals involved.
Strategies to address gender bias include implementing implicit bias training, using standardized interview scoring rubrics, adopting transparent promotion criteria, and employing inclusive communication strategies. Organizations like the AAOS and Ruth Jackson Orthopaedic Society (RJOS) have developed structured initiatives to increase female representation, support professional development, and promote leadership opportunities for women.20,21 Despite these efforts, the same issue remains where long-term follow-up on the effectiveness of these interventions is limited, and more data are needed to assess whether these interventions result in measurable cultural change.
Microaggressions
The Cleveland Clinic defines microaggression as a verbal or nonverbal slight that impacts an individual who might identify as being from a marginalized or non-mainstream community.61 Studies discussing microaggressions expressed them in the following forms: verbal comments, assumptions about skills, traditional role stereotypes, sexist language, and exclusion from informal networks (Figure 3). In the context of orthopedic surgery, female residents and surgeons have reported various experiences, including being mistaken for non-physician staff, being told they are “too small” for orthopedics, or facing skepticism about their technical skills.33,62,63 A scoping review of surgical training environments highlighted encounters related to traditional gender roles, condescending jokes, or being interrupted or ignored during discussions.64
These incidents, though perceived as minor, can accumulate and contribute to emotional fatigue, self-doubt, and burnout. Female trainees report facing the emotional burden of having to either tolerate these slights or confront them, often without institutional support.65 The female residents can constantly manage these dynamics while maintaining professional composure, which can impact confidence, engagement, and satisfaction during training.65
The perception of microaggressions can be subjective and differs significantly between individuals.59 Not all women report experiencing microaggressions, and some describe their environment as respectful and inclusive.66 Some male surgeons admit to acknowledging a lack of awareness of comments or behaviors that might be perceived as offensive.59 Others report being unsure how to help or respond when witnessing microaggressions or feeling excluded in initiatives that focus on gender-based networking.66
In response, several institutions have begun implementing education programs on respectful communication, bystander intervention training, and anti-harassment policies that address both explicit and subtle misconduct.67,68 Additionally, structured mentorship programs and peer support initiatives have also been introduced to provide safe spaces where concerns can be expressed and validated. Although these efforts are still in early phases, they represent a shift toward more inclusive surgical environments.
Microaggressions for the Male Orthopedic Surgeon
There is limited reporting of microaggressions for the male orthopedic surgeon.59 The gap in literature is thought to be related to the perception that such experiences are less impactful for males. Assumptions of physical strength or emotional tolerance are reported to be faced by males as a type of microaggression.59
Limitations
Despite the wide range of themes identified in this scoping review regarding challenges faced by female orthopedic surgeons, critical analysis of some domains remains limited due to the scarcity of available evidence. Challenges of this kind include residency interview experiences, workplace conflicts, technical difficulties, unequal pay, networking barriers, patients’ preferences, military orthopedics, fellowship choice, and work-life balance.
For instance, inappropriate interview questions, although historically reported, recent data are sparse, possibly due to institutional regulations currently in place to mitigate these, making prevalence difficult to evaluate.31 Similarly, conflict in the workplace attributed to gender was mentioned in multiple studies; nevertheless, there was no clear operational definition, frequency of data, or outcomes-based analysis to evaluate.10,33 Female orthopedic surgeons have reported technical difficulties related to the design of instruments.44 No evidence-based study assessed the impact of technical challenges on surgical performance in female orthopedic surgeons. Neither does it serve as a proper tool to evaluate technical difficulties.
In the domain of unequal pay, it was cited by multiple studies that female orthopedic surgeons are underpaid compared to their male counterparts.69–72 Yet studies often fail to account for confounding factors such as subspeciality, workload, or institutional reimbursement models, which might render the claims of underpayment untrue. Networking difficulties are also anecdotally described, but fewer studies quantify the foundational barriers or include both male and female perspectives on the matter.9
Patient preference is another critical challenge that is also underrepresented in the literature. Primarily, this challenge is assessed through localized perception studies that may be generalized to other populations.73,74 Military orthopedics and fellowship choice are particularly understudied, with only one study found to be limiting the ability to draw meaningful conclusions.75,76
Work-life balance, a challenge that is often described as a deterrent to entering the orthopedic specialty, was also underexamined in the literature.57 Papers that discussed this challenge relied on self-reported experiences without examination of regulations implemented by institutions such as childcare, flexible scheduling, or wellness programming.76–78 The topics of research opportunities and career advancement were addressed to some extent concerning bias. Further research is necessary for these two challenges, as they form the foundational elements of a surgeon’s career.
While helpful in documenting lived experiences, the majority of studies on the challenges faced by women in orthopedic surgery are survey-based. These study designs often lack generalizability and are insufficient for establishing concrete correlations. As a result, critical appraisal of these challenges is constrained by the studies’ methodological limitations and the subjective nature of the data. Nevertheless, it serves as a stepping stone in understanding the difficulties reported by female orthopedic surgeons. A smaller sample size, such as in Bowe et al and Julian et al, is another notable limitation. The lack of uniform definitions for microaggressions and career satisfaction further complicates comparison. For future research, this helped identify the main challenges, and it is recommended to prioritize diverse, methodologically rigorous, and longitudinal studies to define these barriers better. This next step will generate actionable, evidence-based strategies to help better support the female orthopedic surgeons.
Conclusion
In conclusion, this scoping review identifies key challenges faced by female orthopedic surgeons. These challenges include underrepresentation, health risk, and impacts on mental well-being. While progress has been made in the representation of women in orthopedic surgery, mentorship programs, and exposure initiatives (RJOS and AAOS), persistent gaps remain across leadership roles, burnout, bias, and occupational health. Ergonomic strain and radiation exposure are reported more frequently among female surgeons, with few inclusive, tailored institutional solutions in place. Despite efforts to eliminate bias in the workplace, such issues are still being reported, particularly in career advancement opportunities.
Limitations of this study include the scarcity of evidence for several challenges, which limits the ability to analyze and draw conclusions critically. These under-examined challenges include residency interview experiences, workplace conflicts, technical difficulties, unequal pay, networking barriers, patients’ preferences, military orthopedics, fellowship choice, and work-life balance. Most evidence is based on cross-sectional surveys, which is another significant limitation, limiting generalizability and causal inference.
Future research should prioritize longitudinal and more methodologically robust studies. Institutional reforms must focus on inclusive mentorship, equipment designed for both genders, and equitable promotion regulations. Programs such as RJOS and AAOS need to be followed up and evaluated for their effectiveness. Awareness and regulations regarding microaggressions are vital for the well-being of both male and female residents. Achieving meaningful change will require serious research, as well as a cultural and institutional commitment to gender equity in orthopedic surgery.
Acknowledgments
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no financial, commercial, or personal competing interests in this work.
References
1. Surprising Medical School statistics [Internet]. [cited 2025 Jun 13]. Available from: https://www.inspiraadvantage.com/blog/surprising-medical-school-statistics.
2. Statistics [Internet]. [cited 2025 Jun 13]. Available from: https://www.rcseng.ac.uk/careers-in-surgery/women-in-surgery/statistics/.
3. Khamisy-Farah R, Biras E, Shehadeh R, et al. Gender and sexuality awareness in medical education and practice: mixed methods study. JMIR Med Educ. 2024;10:e59009. doi:10.2196/59009
4. British Orthopaedic Association. Wow: women in orthopaedics worldwide introduces and celebrates Pioneer Women in Orthopaedics [Internet]. [cited 2025 Jun 13]. Available from: https://www.boa.ac.uk/resource/wow-women-in-orthopaedics-worldwide-introduces-and-celebrates-pioneer-women-in-orthopaedics.html.
5. DeMaio M. Making the case (again) for gender equity [Internet]. [cited 2025 Jun 13]. Available from: https://www.aaos.org/AAOSNow/2019/Jun/YourAAOS/youraaos05/.
6. Diversity in orthopaedics and traumatology: a global perspective. EFORT Open Rev. 2020;5(10):743–752. doi:10.1302/2058-5241.5.200022
7. Ahmed M, Hamilton LC. Current challenges for women in orthopaedics. Bone Joint Open. 2021;2(10):893–899. doi:10.1302/2633-1462.210.bjo-2021-0089.r1
8. Paul D, Ghoshdastidar S, Halder S, Sarkar DK. Are women finally joining Orthopedics in India? A study of the causes limiting the number of women in Orthopedics in India with steps for furthering progress. Indian J Orthopaedics. 2023;57(4):586–595. doi:10.1007/s43465-023-00834-5
9. Van Heest AE, Agel J. The uneven distribution of women in orthopaedic surgery resident training programs in the United States. J Bone Joint Surg Am. 2012;94(2). doi:10.2106/jbjs.j.01583
10. Phillips EA, Nimeh T, Braga J, Lerner LB. Does a surgical career affect a woman’s childbearing and fertility? A report on pregnancy and fertility trends among female surgeons. J Am College Surgeons. 2014;219(5):944–950. doi:10.1016/j.jamcollsurg.2014.07.936
11. Bucknall V, Pynsent PB. Sex and the Orthopaedic Surgeon: a survey of patient, medical student and male orthopaedic surgeon attitudes towards female orthopaedic surgeons. Surgeon. 2009;7(2):89–95. doi:10.1016/s1479-666x(09)80023-1
12. Myers SP, Dasari M, Brown JB, et al. Effects of gender bias and stereotypes in surgical training. JAMA Surg. 2020;155(7):552. doi:10.1001/jamasurg.2020.1127
13. Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32. doi:10.1080/1364557032000119616
14. Tricco AC, Lillie E, Zarin W, et al. Prisma extension for scoping reviews (PRISMA-SCR): checklist and explanation. Ann Internal Med. 2018;169(7):467–473. doi:10.7326/m18-0850
15. Bowe SN, Wang X, Whipple ME, Bly RA. Evidence of specialty-specific gender disparities in resident recruitment and selection. J Graduate Med Edu. 2021;13(6):841–847. doi:10.4300/jgme-d-21-00337.1
16. Julian KR, Anand M, Sobel AD, Mulcahey MK, Wong SE. A 5-year update and comparison of factors related to the sex diversity of orthopaedic residency programs in the United States. JBJS Open Access. 2023;8(1). doi:10.2106/jbjs.oa.22.00116
17. Acuña AJ, Sato EH, Jella TK, et al. How long will it take to reach gender parity in orthopaedic surgery in the United States? an analysis of the National Provider Identifier Registry. Clin Orthopaedics Related Res. 2021;479(6):1179–1189. doi:10.1097/corr.0000000000001724
18. Pinpin C, White PB, Nellans KW, Bitterman AD, Mulcahey MK, Cohn RM. Exponential growth in female residency applicants in orthopaedic surgery over the past 15 years. JBJS Open Access. 2023;8(2). doi:10.2106/jbjs.oa.23.00004
19. Ruth Jackson Orthopaedic Society[Internet]. [cited 2025 Jun 13]. Available from: https://www.rjos.org/about/about-rjos.
20. American Academy of Orthopaedic Surgeons. Diversity Advisory Board aaos [Internet]. [cited 2025 Jun 13]. Available from: https://www.aaos.org/about/meet-aaos/leadership-governance/aaos-governance/committee-charges/7738/.
21. Xu AL, Humbyrd CJ, De Mattos CB, LaPorte D. The importance of perceived barriers to women entering and advancing in orthopaedic surgery in the US and beyond. World J Surg. 2023;47(12):3051–3059. doi:10.1007/s00268-023-07165-4
22. Hiemstra LA, Kerslake S, Clark M, Temple-Oberle C, Boynton E. Experiences of Canadian female orthopaedic surgeons in the Workplace. J Bone Joint Surg. 2022;104(16):1455–1461. doi:10.2106/jbjs.21.01462
23. Hill JF, Yule A, Zurakowski D, Day CS. Residents’ perceptions of sex diversity in orthopaedic surgery. J Bone Joint Surg. 2013;95(19):e144. doi:10.2106/jbjs.l.00666
24. Hoof MA, Sommi C, Meyer LE, Bird ML, Brown SM, Mulcahey MK. Gender-related differences in research productivity, position, and advancement among academic orthopaedic faculty within the United States. J Am Acad Orthopaedic Surg. 2020;28(21):893–899. doi:10.5435/jaaos-d-19-00408
25. Sutherland M, Sanchez C, Baroutjian A, Ali A, McKenney M, Elkbuli A. Gender, race, age, allopathic degree, board score, and research experience among applicants matching to General and Orthopedic Surgery Residencies, 2015-2019. Am SurgeonTM. 2021;88(6):1207–1216. doi:10.1177/0003134821991982
26. Yin C, McAuliffe PB, Liao CD, et al. Has the increase of women in surgical training programs led to a concomitant increase in female leadership positions? A 10-year analysis. Annals Plastic Surg. 2023;90(4):376–379. doi:10.1097/sap.0000000000002807
27. Oladeji LO, Ponce BA, Worley JR, Keeney JA. Mentorship in orthopedics: a national survey of orthopedic surgery residents. J Surg Educ. 2018;75(6):1606–1614. doi:10.1016/j.jsurg.2018.04.007
28. Joe MB, Cusano A, Leckie J, et al. Mentorship programs in residency: a scoping review [Internet]. U.S. National Library of Medicine; 2023 [cited 2025 Jun 13]. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10150829/.
29. Elkadi SH, Donaldson S, Krisanda E, Kessler MW. Trends in medical training and leadership at Academic Orthopedic Programs. Cureus. 2022. doi:10.7759/cureus.29100
30. Levy KH, Gupta A, Murdock CJ, et al. Effect of faculty diversity on minority student populations matching into orthopaedic surgery residency programs. JBJS Open Access. 2023;8(1). doi:10.2106/jbjs.oa.22.00117
31. Sobel AD, Lavorgna TR, Ames SE, Templeton KJ, Mulcahey MK. Interpersonal interactions and biases in orthopaedic surgery residency: do experiences differ based on gender? Clin Orthopaedics Related Res. 2022;481(2):369–378. doi:10.1097/corr.0000000000002457
32. Rodarte P, Kammire MS, Cannada LK, Poon S, Israel H. The “other side” of conflict: examining the challenges of female orthopaedic surgeons in the workplace. J Orthopaedic Exp Innov. 2022;3(2). doi:10.60118/001c.36644
33. Saxena S, Cannada LK, Weiss JM. Does the proportion of women in orthopaedic leadership roles reflect the gender composition of specialty societies? Clin Orthopaedics Related Res. 2019;478(7):1572–1579. doi:10.1097/corr.0000000000000823
34. Ramos MB, Criscuoli de Farias FA, Einsfeld Britz JP, et al. Representation of women on Editorial Boards of MEDLINE-indexed spine, neurosurgery, and orthopedic journals. Int J Spine Surg. 2022;16(2):404–411. doi:10.14444/8223
35. Chou LB, Kha ST, Shapiro LM. Health considerations for female orthopaedic surgeons. J Am Acad Orthopaedic Surg. 2023;32(3):e125–e133. doi:10.5435/jaaos-d-23-00221
36. Valone LC, Chambers M, Lattanza L, James MA. Breast radiation exposure in female orthopaedic surgeons. J Bone Joint Surg. 2016;98(21):1808–1813. doi:10.2106/jbjs.15.01167
37. Cheon BK, Kim CL, Kim KR, et al. Radiation safety: a focus on lead aprons and thyroid shields in Interventional Pain Management. Korean J Pain. 2018;31(4):244–252. doi:10.3344/kjp.2018.31.4.244
38. The 2007 recommendations of the International Commission on Radiological Protection [Internet]. [cited 2025 Jun 13]. Available from: https://www.icrp.org/publication.asp?id=ICRP+Publication+103.
39. Laura. Report no. 174 – preconception and prenatal radiation exposure: health effects and protective guidance (2013). NCRP: Bethesda, MD [Internet]. 2025
40. Guidelines for diagnostic imaging during pregnancy and lactation [Internet]. [cited 2025 Jun 13]. Available from: https://www.acog.org/clinical/clinical-guidance/committee-opinion/articles/2017/10/guidelines-for-diagnostic-imaging-during-pregnancy-and-lactation.
41. American Academy of Orthopaedic Surgeons. Radiation Safety for Orthopaedic Surgeons: position Statement. AAOS; 2015. https://www.aaos.org/globalassets/about/bylaws-library/information-statements/1050-radiationsafety.pdf.
42. Cohen-Rosenblum AR, Varady NH, Leonovicz O, Chen AF. Repetitive musculoskeletal injuries: a survey of female adult reconstruction surgeons. J Arthroplasty. 2022;37(8):1474–1477.e6. doi:10.1016/j.arth.2022.01.001
43. Fram B, Bishop ME, Beredjiklian P, Seigerman D. Female sex is associated with increased reported injury rates and difficulties with use of orthopedic surgical instruments. Cureus. 2021. doi:10.7759/cureus.14952
44. Lurie B, Albanese J, Allenback G, Elliott I, Nelson K. Small glove size and female gender are associated with greater reported difficulty using orthopaedic instruments among residents. JBJS Open Access. 2024;9(2). doi:10.2106/jbjs.oa.23.00151
45. Kletzer LG, Koch WL. International Experience with Job Training: Lessons for the United States. Job Training Policy in the United States. 2004.Oct.26. 245–288. doi:10.17848/9781417549993.ch8
46. Sedani AB, Yakkanti RR, Syros A, et al. An overview of occupational injuries among female orthopaedic surgeons. J Orthopaedics. 2024;47:94–99. doi:10.1016/j.jor.2023.10.037
47. Balch B, Writer S. 22 A. Oversized and overlooked: women surgeons struggle to find equipment that fits [Internet]. 2022 [cited 2025 Jun 13]. Available from: https://www.aamc.org/news/oversized-and-overlooked-women-surgeons-struggle-find-equipment-fits?utm_source=chatgpt.com.
48. Yoshinaga S, Mabuchi K, Sigurdson AJ, Doody MM, Ron E. Cancer risks among Radiologists and Radiologic Technologists: review of Epidemiologic Studies. Radiology. 2004;233(2):313–321. doi:10.1148/radiol.2332031119
49. Mehlman CT, DiPasquale TG. Radiation exposure to the orthopaedic surgical team during fluoroscopy: “how far away is far enough? J Orthop Trauma. 1997;11(6):392–398. doi:10.1097/00005131-199708000-00002
50. Davis WT, Sathiyakumar V, Jahangir AA, Obremskey WT, Sethi MK. Occupational injury among orthopaedic surgeons. J Bone Joint Surg Am Volume. 2013;95(15). doi:10.2106/jbjs.l.01427
51. Ponzio DY, Bell C, Stavrakis A, et al. Discrepancies in work-family integration between female and male orthopaedic surgeons. J Bone Joint Surg. 2021;104(5):465–472. doi:10.2106/jbjs.21.00345
52. Gosselin MM, Alolabi B, Dickens JF, et al. Cross-sectional survey results on mental health among orthopedic surgery residents across North America. J Surg Educ. 2019;76(6):1484–1491. doi:10.1016/j.jsurg.2019.06.003
53. Becker JL, Milad MP, Klock SC. Burnout, depression, and career satisfaction: cross-sectional study of obstetrics and gynecology residents. Am J Clin Exp Obstet Gynecol. 2006;195(5):1444–1449. doi:10.1016/j.ajog.2006.06.075
54. Tosi LL, Mankin HJ. Ensuring the success of women in Academic Orthopaedics. Clin Orthopaedics Related Res. 1998;356:254–263. doi:10.1097/00003086-199811000-00034
55. Kerluku J, Wessel L, Ling D, et al. Assessing gender differences in technical skills and confidence in orthopaedic surgery residency applicants. J Am Acad Orthop Surg Glob Res Rev. 2023;7(7). doi:10.5435/jaaosglobal-d-22-00265
56. Ortega G, Benson E, Pierrie SN, McLaurin TM, Tejwani NC. Diversity in orthopaedic trauma: where we are and where we need to be. OTA Int. 2021;4(2). doi:10.1097/oi9.0000000000000102
57. Mulcahey MK, Nemeth C, Trojan JD, O’Connor MI. The perception of pregnancy and parenthood among female orthopaedic surgery residents. J Am Acad Orthopaedic Surg. 2019;27(14):527–532. doi:10.5435/jaaos-d-18-00216
58. Poon SC. The effect of implicit bias and current culture in orthopaedic surgery. J Pediatric Orthopaedic Soc North Am. 2023;5:606. doi:10.55275/jposna-2023-606
59. Lim WH, Wong C, Jain SR, et al. The unspoken reality of gender bias in surgery: a qualitative systematic review. PLoS One. 2021;16(2). doi:10.1371/journal.pone.0246420
60. Cleveland Clinic. What are microaggressions? Cleveland Clinic. Updated November 17, 2022. https://my.clevelandclinic.org/health/articles/22053-microaggressions.
61. Carino Mason MR, Pandya S, Joshi P, Cai N, Murdock CJ, Hui-Chou HG. Perceptions of racial and gender microaggressions in an academic orthopaedic department. JBJS Open Access. 2023;8(3). doi:10.2106/jbjs.oa.22.00150
62. Haruno LS, Chen X, Metzger M, et al. Racial and sex disparities in resident attrition in orthopaedic surgery. JBJS Open Access. 2023;8(2). doi:10.2106/jbjs.oa.22.00148
63. Sprow HN, Hansen NF, Loeb HE, et al. Gender‐based microaggressions in surgery: a scoping review of the global literature. World J Surg. 2021;45(5):1409–1422. doi:10.1007/s00268-021-05974-z
64. Thiart M, O’Connor M, Müller J, Holland N, Bantjies J. Operating in the margins: women’s lived experience of training and working in Orthopaedic Surgery in South Africa. Qualitative Res Med Healthcare. 2023;7(1):10902. doi:10.4081/qrmh.2023.10902
65. Samora JB, Denning J, Haralabatos S, Luong M, Poon S. Do women experience microaggressions in orthopaedic surgery? current State and future directions from a survey of women orthopaedists. Current Orthopaedic Pract. 2020;31(5):503–507. doi:10.1097/bco.0000000000000909
66. Salles A, Mueller CM, Cohen GL. Exploring the relationship between stereotype perception and residents’ well-being. J Am College Surgeons. 2016;222(1):52–58. doi:10.1016/j.jamcollsurg.2015.10.004
67. Association of American Medical colleges. Understanding and addressing sexual harassment in academic medicine [Internet]. Washington (DC): AAMX; 2022 July. [Cited 2025 June 15]. Available from: https://ophd.ucsf.edu/sites/g/files/tkssra9441/f/aamc-understanding-addressing-sexual-harassment-academic-medicine-july-2022.pdf?utm_source=chatgpt.com.
68. Bohl DD, Iantorno SE, Kogan M. Inappropriate questions asked of female orthopaedic surgery applicants from 1971 to 2015: a cross-sectional study. J Am Acad Orthopaedic Surg. 2019;27(14):519–526. doi:10.5435/jaaos-d-17-00868
69. Avila A, Sato EH, Acuña AJ, Vasavada K, Kamath AF. Gender differences in reimbursement among orthopaedic surgeons: a cross-sectional analysis of Medicare claims. J Am Acad Orthopaedic Surg. 2023;31(15):e570–e578. doi:10.5435/jaaos-d-22-00823
70. Chapman TR, Zmistowski B, Purtill JJ, Chen AF. Profiles of practicing female orthopaedists caring for Medicare patients in the United States. J Bone Joint Surg. 2018;100(10):e69. doi:10.2106/jbjs.17.00505
71. Dossa F, Simpson AN, Sutradhar R, et al. Sex-based disparities in the hourly earnings of Surgeons in the fee-for-service system in Ontario, Canada. JAMA Surg. 2019;154(12):1134. doi:10.1001/jamasurg.2019.3769
72. Dineen HA, Patterson JMM, Eskildsen SM, et al. Gender preferences of patients when selecting orthopaedic providers. Iowa Orthop J. 2019;39:203. PMID: 31413695.
73. AlSamhori JF, Rayyan R, Hammouri M, et al. Factors influencing gender preference towards surgeons among Jordanian adults: an investigation of healthcare bias. Sci Rep. 2023;13(1). doi:10.1038/s41598-023-38734-1
74. Hoyt BW, Anderson AB, Dingle ME, et al. Racial and gender diversity of physicians accepted to American military orthopaedic and surgical residencies. JBJS Open Access. 2023;8(1). doi:10.2106/jbjs.oa.22.00091
75. Higgins MJ, Kale NN, Brown SM, Mulcahey MK. Taking family call: understanding how orthopaedic surgeons manage home, family, and life responsibilities. J Am Acad Orthopaedic Surg. 2021;29(1):e31–e40. doi:10.5435/jaaos-d-20-00182
76. Balch CM, Oreskovich MR, Dyrbye LN, et al. Personal consequences of malpractice lawsuits on American surgeons. J Am College Surgeons. 2011;213(5):657–667. doi:10.1016/j.jamcollsurg.2011.08.005
77. Summers MA, Matar RN, Denning JR, et al. Closing the gender gap: barriers to success for recruitment and retention of the female orthopedic surgery. JBJS Rev. 2020;8(5):e0211–e0211. doi:10.2106/jbjs.rvw.19.00211
78. Hariri S, York SC, O’Connor MI, Parsley BS, McCarthy JC. Career plans of current orthopaedic residents with a focus on sex-based and generational differences. J Bone Joint Surg. 2011;93(5):e16. doi:10.2106/jbjs.j.00489
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Women as Urologists in Saudi Arabia: Career Choice and Practice Challenges: A Comparative Cross-Sectional Study
Alzahrani MA, Almhmd A, Khan MA, Badriq F, Salman B, Aljaziri ZY, Alotaibi N, Alkhamees M, Almutairi S, Ahmad MS, Alkhateeb S
Research and Reports in Urology 2023, 15:273-289
Published Date: 27 June 2023