Back to Journals » The Application of Clinical Genetics » Volume 16
Challenges and Pragmatic Solutions in Pre-Test and Post-Test Genetic Counseling for Prenatal Exome Sequencing
Authors Diderich KEM ![]() , Klapwijk JE
, Klapwijk JE ![]() , van der Schoot V, Brüggenwirth HT, Joosten M, Srebniak MI
, van der Schoot V, Brüggenwirth HT, Joosten M, Srebniak MI ![]()
Received 5 March 2023
Accepted for publication 19 April 2023
Published 15 May 2023 Volume 2023:16 Pages 89—97
DOI https://doi.org/10.2147/TACG.S411185
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Martin Maurer
Karin EM Diderich, Jasmijn E Klapwijk, Vyne van der Schoot, Hennie T Brüggenwirth, Marieke Joosten, Malgorzata I Srebniak
Department of Clinical Genetics, Erasmus MC, Rotterdam, the Netherlands
Correspondence: Karin EM Diderich, Department of Clinical Genetics, Erasmus MC, Wytemaweg 50, Rotterdam, the Netherlands, Tel +31 10 70 43214, Email [email protected]
Abstract: The yield of genetic prenatal diagnosis has been notably improved by introducing whole genome chromosomal microarray (CMA) and prenatal exome sequencing (pES). However, together with increased numbers of diagnoses made, the need to manage challenging findings such as variants of unknown significance (VUS) and incidental findings (IF) also increased. We have summarized the current guidelines and recommendations and we have shown current solutions used in our tertiary center in the Netherlands. We discuss four of the most common clinical situations: fetus with normal pES results, fetus with a pathogenic finding explaining the fetal phenotype, fetus with a variant of uncertain clinical significance fitting the phenotype and fetus with a variant leading to an incidental diagnosis. Additionally, we reflect on solutions in order to facilitate genetic counseling in an NGS-era.
Keywords: exome sequencing, genetic counseling, prenatal diagnosis, incidental findings, variants of unknown significance, VUS, IF
Introduction
The yield of genetic prenatal diagnosis has been notably improved by introducing whole genome chromosomal microarray (CMA) analysis, which is now recommended in all cases with structural anomalies,1 allowing an additional diagnostic yield as compared to karyotyping of up to 10%.2,3 Moreover, recent data suggest that the expected diagnostic yield of prenatal exome sequencing (pES; for the detection of single nucleotide variants [SNVs]) would be 8.5% in an unselected cohort and up to ~15% in fetuses with multisystem anomalies.4 Therefore, one may anticipate that soon pES may also be recommended as a standard diagnostic tool in all cases of fetal structural anomalies. The diagnostic yield is highest in fetal cases with multiple congenital anomalies (MCA), and therefore MCA is already an unquestionable indication for pES recognized by many professionals.5 It is well known that many syndromes have postnatal features that cannot be detected prenatally on routine or expert ultrasound scans, e.g., intellectual disability or hypotonia.6,7 In cases of a treatable anomaly, the association with or absence of intellectual disability is the most important information for the parents in their decision to terminate or continue the pregnancy.8 In these cases, the detection of a genetic cause of fetal anomalies may be of special value as a molecular diagnosis may have more impact on decision-making during pregnancy than the anomalies seen on the fetal scan.6,9 Several studies show a large clinical impact of pES in ongoing pregnancies on either decision-making potentially resulting in a termination of pregnancy or on pre- or perinatal management.10,11
Offering pES to an increasing number of prospective parents asks for a critical reflection on prenatal counseling practices. The aim of this study was to reflect on challenges in counseling prenatal genetic testing using pES. We formulate pragmatic solutions for prenatal genetic counseling when an ultrasound anomaly is found.
Major Challenges in pES Results
While aiming at uncovering (likely) pathogenic findings (class 4 and 5) that fit the phenotype, there is a probability of uncovering variants of unknown significance (VUS) and variants not explaining the phenotype when performing whole genome diagnostics.
VUS present a major challenge when using genome wide techniques in fetuses with incomplete phenotypes.12 When comparing pES to CMA, pES presents more variants, which cannot be evaluated manually. Automatic filters in diagnostic pipelines and analyses of restricted gene panels limit VUS detection.13 Nevertheless, it is not possible to avoid all VUS. When encountered, some will raise the question to report or not to report. Guidelines that specifically describe the prenatal settings recommend reporting (likely) pathogenic variants and only some VUS that may have contributed to the abnormal fetal phenotype.5,14 How to decide on VUS disclosure is often not evident and depends on local practice.15–17 Discussing selected VUS in a multidisciplinary team setting to ensure a supported and well-grounded disclosure of uncertain results has been recommended.18
Another important difficulty in pES diagnostics is the probability to encounter (likely) pathogenic variants not explaining the phenotype. Throughout the years various terms (i.e., incidental findings [IF], unexpected findings) have been used to describe these variants.
For the classification of array findings, we have proposed the term unexpected diagnoses (UDs) for pathogenic findings not explaining the phenotype or not matching the indication for genetic testing.19 Examples are Angelman syndrome in a fetus with a heart abnormality or a deletion in the DMD gene in a male fetus in a pregnancy that was tested because of abnormal first trimester screening.8 Van El et al propose the term unsolicited findings and recommend reporting those that are indicative of serious health problems and (clinically) actionable.20 Some authors use it not only to describe a relation with indication for testing, but also to describe the inactionability of such a finding. Berg et al differentiate IF that may have no direct clinical actionability from IF that may be unwelcome to many individuals.21
Klapwijk et al defined IF as pathogenic variant(s) not related to indication of testing and identified inadvertently (unexpected result).22 Secondary findings are defined as pathogenic variant(s) not related to indication of testing, but intentionally searched for as an additional analysis (next to the standard test). There are several guidelines and recommendation papers which advise on the management of such findings.13–15,17,20,23–25 In the Netherlands there is, unlike in the United States, no policy to screen for secondary findings.26,27
For the purpose of this article, we will use the term IF for actionable CNVs/SNVs unrelated to the fetal phenotype.
Recommendations for the Pre -Test Counseling According to Currently Available Guidelines
Guidelines on both prenatal microarray testing28–34 and prenatal whole exome sequencing5,14 underline the value of (pre-test) genetic counseling for genomic testing in pregnancy. Although there are some publications on pre-test counseling for CMA,35–41 there is limited literature on pre-test counseling for pES.42,43 In pre-test counseling, it is not only important to share the knowledge on the possible outcomes and limitations of the genomic test to enable deliberative decision-making, but it is advised5,14,15,17,23,25,28–30,32,33,44,45 to obtain informed consent including patients’ preferences on the possible outcomes that are going to be reported. With regard to IF, it has been recommended to offer an “opt-in” to have non-actionable diseases disclosed and/or an “opt-out” to abstain from disclosure of late onset actionable conditions that do not match the indication.13,23,46,47 Offering these options holds the premise of increasing patients’ autonomy.48,49 The autonomy of the future child and the option of termination of pregnancy based on IF disclosure ask for specific recommendations on IF disclosure in the prenatal setting. So far, there is no consensus about disclosure of IF in the prenatal situation. Also, it is challenging to provide enough information to allow informed choices, but at the same time to avoid information overload as the complexity of this issue potentially restricts patients’ autonomy.49,50
Pre-test counselling for pES needs to be comprehensive for patients from all educational, religious and cultural backgrounds. This is best performed by trained genetic professionals who have expertise with prenatal testing.51–53 Creating realistic expectations about the likelihood of a diagnosis and the time-frame in which a result can be obtained should be part of the pre-test counseling.14 It should be communicated which outcomes are to be expected, which type of results can be expected, how likely they are, and which of these results will be reported.17 Specifically, limitations of the test should be addressed.25 pES (and CMA) do not completely cover all genes, especially if gene panels are used, and both can uncover variants that may not be interpretable yet. It should be explained that a normal result of pES in case of a mild prenatal phenotype might be reassuring for prospective parents, but does not fully exclude an underlying syndrome.5,7 Additionally, prospective parents should be informed about the probability of detecting an IF in order to “make unexpected results expected.”8 Expectations that are set in the pre-test counseling are not only crucial for the pregnant couples, but also helpful for the clinicians who are to convey an IF.50
Regarding uncertainty in the prenatal setting Hammond et al recommended to take time, explain everything in an understandable manner (in a language the couple speaks and to a level they can understand), show empathy and be available for additional questions during this diagnostic process as well as after diagnosis.54
These aspects have been previously identified as being important to counseling prenatal CMA.28–34 This makes it possible to provide one pre-test counseling for both CMA and pES. The classification with illustrative examples of results can be adapted from CMA counseling.19 In Table 1 we have summarized the types of CMA/ES findings and recommendations to report or not to report.
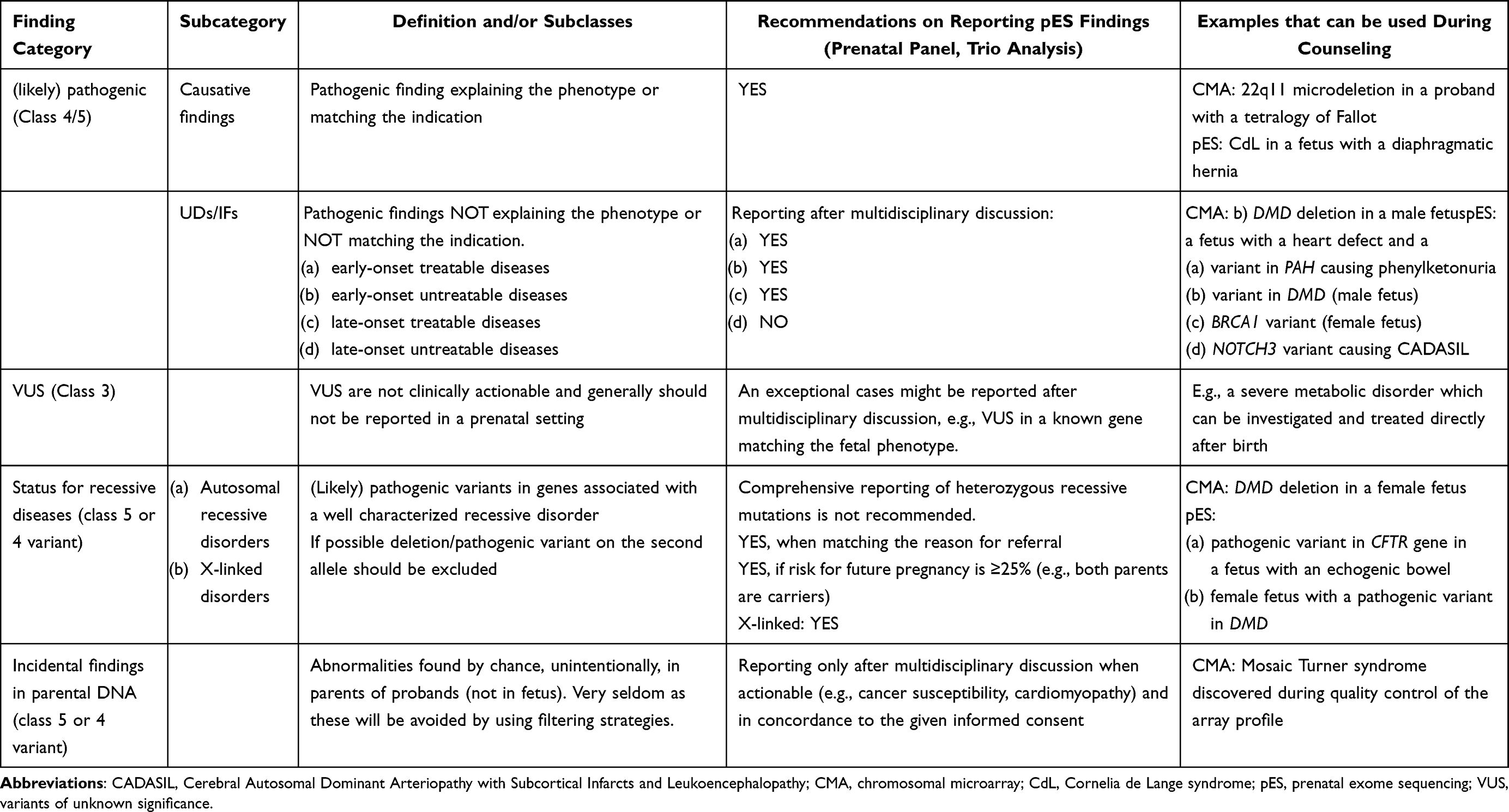 |
Table 1 Types of pES Findings, Recommendations for Reporting and Simple Examples Used in Pre-Test Counseling |
Pre-Test Counseling for Genomic Test in Our Practice
The most important issues that are covered by pre-test counseling are summarized in Table 2. After ultrasound imaging (and before or after chorion villus biopsy/ amniocentesis) in a tertiary care hospital, prospective parents with fetal ultrasound abnormalities are referred to a clinical geneticist specialized in prenatal genetics. Generally, the fetal medicine specialist/gynecologist performed simplified pre-test counseling for CMA. From 2019 onwards, based on the guidelines of the ISPD 2018,14 the department of Clinical Genetics in Rotterdam offers pES in the majority of prenatal ultrasound anomalies in addition to CMA analysis.55 A standard gene panel containing about 3400 genes associated with congenital abnormalities and/or intellectual disability is offered in all cases.7 pES pre-test counseling performed by a clinical geneticist, consists of discussing the differential diagnosis, explaining the basics of genetics and discussing the possibilities of genetic testing. During pre-test counseling, possible outcomes are discussed: no genetic abnormalities, a (likely) disease-causing variant in a gene that fits the phenotype, VUS and IF, which does not match the phenotype seen on ultrasound. VUS are not reported prenatally unless the multidisciplinary team deems the variant of potential relevance for pregnancy management or when a functional test is available (Diderich et al, manuscript under review). VUS might be reclassified to (likely) pathogenic findings based on additional information or increased insights over time, allowing a genetic diagnosis after birth.56 Re-classification of VUS to (likely) pathogenic variants after birth may cause distress in healthcare professionals and/or patients. This urges to address this issue sufficiently during pre or post-test counseling.
 |
Table 2 Comprehensive List of Items That are Discussed During Pre-Test Counseling for pES |
In practice, national recommendations regarding the disclosure of IF in the postnatal setting are being followed. These guide towards disclosure of variants associated with early onset and/or treatable disorders, while variants associated with an untreatable late-onset disorders are not disclosed (https://www.vkgn.org/vakinformatie/richtlijnen-en-protocollen/uitgebreid-dna-onderzoek-en-nevenbevindingen/). Carrier status of a recessive disease allele is revealed almost only when a couple has at least 25% risk of affected offspring. Patients’ preferences other than this default are discussed during pre-test counselling and noted on the consent form.
When discussing possible outcomes we use examples that couples can easily understand. Examples of IF that are disclosed by default could be a predisposition to (breast) cancer or a cardiomyopathy. Adult-onset dementia (e.g., adult-onset monogenic neurodegenerative disorder as CADASIL) is frequently used as an example of a non-actionable late onset disease which is not disclosed by default (see Table 1). Oral (and written) information is provided, before the prospective parent(s) give their consent.
Recently due to the COVID-19 pandemic, we have learnt that pre-test counseling by web consultation or telephone is feasible, brings logistic benefits and is less time consuming for both professionals and couples. Pictures of chromosomes and DNA were sent by mail to facilitate counseling by telephone. Therefore, consultations that do not require physical examination might be planned digitally.
Post-Test Counseling in Our Practice
The results of pES are always communicated to the patient by a clinical geneticist (after discussion in a multidisciplinary team if relevant). When an incidental finding or VUS has been found, a multidisciplinary team reflects on the finding, considering patients’ preferences. The genetic variant and the related phenotype are discussed with the pregnant couple. When available, data on prenatal cohorts of the specific condition is discussed as the phenotypic diversity of chromosomal abnormalities and monogenic syndromes is larger than previously thought.
If relevant, the possibilities to continue or terminate the pregnancy are discussed again. Depending on the situation, the procedure of termination of pregnancy and the perceived emotional burden of terminating are explained. In addition, the recurrence risk and reproductive options for a next pregnancy are mentioned (briefly in anticipation of a follow up appointment). Unexpected bad news is not communicated to patients on Friday afternoon, unless further action is needed over the weekend (e.g., due to the legal limit of pregnancy termination) to avoid a stressful weekend prior to appropriate counseling.
In case of a normal result, it is explained to prospective parents that a genetic cause or syndrome is not completely excluded. Depending on the situation, it can be explained that after the child is born, new phenotypic information may become available urging for re-evaluation of the pES data, which may, together with new literature data, reveal a pathogenic finding.
Examples of Most Common Clinical Situations
- No (likely) pathogenic pES/CMA finding explaining the fetal phenotype is found:
- there is no additional phenotypic information after birth, and re-classification does not lead to new information – end of the diagnostic procedure or revision in several years
- there are additional phenotypic findings after birth that bring possibilities for additional diagnostic testing (e.g., methylation study) and/or re-analysis which could reveal a genetic cause of abnormal phenotype of the child
- (Likely) pathogenic pES/CMA finding explaining the phenotype, prenatal genetic diagnosis in a future pregnancy is possible
[e.g., in a fetus with growth restriction we found a pathogenic variant in PLAG1 associated with Silver-Russell syndrome 4 (OMIM 618907). After careful consideration, the couple decided to continue the pregnancy.]
[e.g., In a fetus with a growth restriction we found a maternal, pathogenic variant in ATP2C1 associated with a mild variant of Hailey-Hailey disease (OMIM 169600).57 After disclosure of this result, the pregnant woman told us that she and other family members had a skin condition of which they did not know the cause. She was glad to find the cause and to be able to inform her family members about this and the possible treatment.]
Future Perspectives
We anticipate that, similar to CMA, pES will soon be offered in all cases (with ultrasound anomalies) in which invasive sampling is performed. Due to the complexity of the techniques used in prenatal genetic testing, awareness of test limitations and possible outcomes has become more important than before. Extensive pre-test counseling aiming at informed consent and understanding of the diagnostic complexity and potential (unexpected) results is highly appreciated by couples,54 but very time consuming. Currently, pre-test counseling for pES in the Netherlands is performed by a clinical geneticist. When pES is offered to all prospective parents with anomalies on fetal ultrasound, this might not be feasible. We reflect on several solutions, which all include specialist education on pre-test counseling and providing educational materials for patients:
- One pre-test counseling could be given for both CMA and pES.
- When the far majority of VUS is not reported, pre-test counseling is mainly important because of the possibility of IF. We have experienced that IFs are not common. The probability of uncovering an incidental finding is about 0.5% after CMA58 and about 1% after WES offered in postnatal settings when analyzing broad gene panels.59 The low probability of uncovering such finding might direct towards simplification of the pre-test counseling.
- Pre-test counseling by web consult or telephone as done in times of COVID-19 might be a first step in making pre-test counseling more efficient (for counselor and patient).
- The moment of providing information could be shifted. One could provide all patients who consider having an invasive procedure (because of ultrasound abnormalities) with a video to explain the procedure, the tests and possible outcomes to prepare for the pre-test counseling and informed consent.
- If all the necessary information is given through video or fetal medicine specialist, clinical geneticists could focus on post-test counseling. To be able to serve more patients, extensive post-test counseling by a clinical geneticist could be reserved for the cases in which genetic abnormalities are found as in the mentioned examples 2, 3b and 4. In the remaining cases (1, 3a and 4) genetic re-evaluation can be done after birth or after autopsy if the pregnancy was terminated (when additional information [about the development, for example] is available).
In addition, as the costs of sequencing decrease, bioinformatics and analytic capabilities improve and rapid sequencing becomes available, it could be considered to switch from pES/CMA approaches towards whole genome sequencing (WGS).51 Because of the improved ability to detect a wider range of genomic abnormalities, e.g., non-coding variants, this will further improve the diagnostic capabilities.51 WGS is more suitable for CNV analysis than ES, so it is likely that in the near future the request for CMA and pES test will be replaced by a request for prenatal genome sequencing, which will include both CNV and SNV analysis. Employing one test (WGS) will facilitate reducing pre- and post-test counseling time to one session when both CNV and SNV results are given in one final report.
Limitations
The presented practice of pre- and post-test counseling is the practice in our tertiary center in the Netherlands and thus not necessarily applicable to all healthcare systems and cultural contexts.
Conclusions
While pES increases the diagnostic yield in cases of fetal ultrasound abnormalities, it also increases the chance of uncovering VUS and variants not explaining the phenotype. Addressing these issues in pre-test counseling is highly recommended. Available guidelines and our practice are presented to enable pre- and post-test counseling. We recommend performing post-test counseling in all cases and discussing the residual genetic risk and the possibility of future reclassifications, when new literature and phenotypic data become available.
Acknowledgments
The authors would like to thank all members of the prenatal multidisciplinary team of Erasmus MC for sharing expertise, (un)certainties, responsibility and for creating a safe team environment for everyone.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. American College of O, Gynecologists. Practice bulletin no. 162: prenatal diagnostic testing for genetic disorders. Obstet Gynecol. 2016;127(5):e108–e122. doi:10.1097/AOG.0000000000001405
2. Srebniak MI, Boter M, Oudesluijs GO, et al. Genomic SNP array as a gold standard for prenatal diagnosis of foetal ultrasound abnormalities. Mol Cytogenet. 2012;5(1):14. doi:10.1186/1755-8166-5-14
3. Robson SC, Chitty LS, Morris S, et al. Evaluation of array comparative genomic hybridisation in prenatal diagnosis of fetal anomalies: a multicentre cohort study with cost analysis and assessment of patient, health professional and commissioner preferences for array comparative genomic hybridisation. Effic Mechan Eval. 2017;4(1):1–04. doi:10.3310/eme04010
4. Lord J, McMullan DJ, Eberhardt RY, et al. Prenatal exome sequencing analysis in fetal structural anomalies detected by ultrasonography (PAGE): a cohort study. Lancet. 2019;393(10173):747–757. doi:10.1016/S0140-6736(18)31940-8
5. Monaghan KG, Leach NT, Pekarek D, et al. The use of fetal exome sequencing in prenatal diagnosis: a points to consider document of the American College of Medical Genetics and Genomics (ACMG). Genet Med. 2020;22(4):675–680. doi:10.1038/s41436-019-0731-7
6. Diderich K, Joosten M, Govaerts L, et al. Is it feasible to select fetuses for prenatal WES based on the prenatal phenotype?. Prenat Diagn. 2019;39(11):1039–1040.
7. Diderich KEM, Romijn K, Joosten M, et al. The potential diagnostic yield of whole exome sequencing in pregnancies complicated by fetal ultrasound anomalies. Acta Obstet Gynecol Scand. 2020;2020:1.
8. Joosten M, Diderich KE, Van Opstal D, et al. Clinical experience of unexpected findings in prenatal array testing. Biomark Med. 2016;10(8):831–840. doi:10.2217/bmm-2016-0054
9. de Koning MA, Haak MC, Adama van Scheltema PN, et al. From diagnostic yield to clinical impact: a pilot study on the implementation of prenatal exome sequencing in routine care. Genet Med. 2019;21(10):2303–2310. doi:10.1038/s41436-019-0499-9
10. Deden C, Neveling K, Zafeiropopoulou D, et al. Rapid whole exome sequencing in pregnancies to identify the underlying genetic cause in fetuses with congenital anomalies detected by ultrasound imaging. Prenat Diagn. 2020;40(8):972–983. doi:10.1002/pd.5717
11. Corsten-Janssen N, Bouman K, Diphoorn JCD, et al. A prospective study on rapid exome sequencing as a diagnostic test for multiple congenital anomalies on fetal ultrasound. Prenat Diagn. 2020;40:1300–1309. doi:10.1002/pd.5781
12. Mellis R, Chandler N, Chitty LS. Next-generation sequencing and the impact on prenatal diagnosis. Expert Rev Mol Diagn. 2018;18(8):689–699. doi:10.1080/14737159.2018.1493924
13. Boycott K, Hartley T, Adam S, et al. The clinical application of genome-wide sequencing for monogenic diseases in Canada: position statement of the Canadian College of Medical Geneticists. J Med Genet. 2015;52(7):431–437. doi:10.1136/jmedgenet-2015-103144
14. International Society for Prenatal Diagnosis, Society for Maternal Fetal Medicine, Perinatal Quality Foundation. Joint Position Statement from the International Society for Prenatal Diagnosis (ISPD), the Society for Maternal Fetal Medicine (SMFM), and the Perinatal Quality Foundation (PQF) on the use of genome‐wide sequencing for fetal diagnosis. Prenat Diagn. 2018;38(1):6–9. doi:10.1002/pd.5195
15. Matthijs G, Souche E, Alders M, et al. Guidelines for diagnostic next-generation sequencing. Euro J Human Genet. 2016;24(1):2–5. doi:10.1038/ejhg.2015.226
16. Wallis Y, Payne S, McAnulty C, et al. Practice guidelines for the evaluation of pathogenicity and the reporting of sequence variants in clinical molecular genetics. Assoc Clin Genet Sci Dutch Soc Clin Genet Labor Spec. 2013;2013:1.
17. Acmg_Board_of_Directors. Points to consider in the clinical application of genomic sequencing. Genet Med. 2012;14(8):759. doi:10.1038/gim.2012.74
18. Cornthwaite M, Turner K, Armstrong L, et al. Impact of variation in practice in the prenatal reporting of variants of uncertain significance by commercial laboratories: need for greater adherence to published guidelines. Prenat Diagn. 2022;42(12):1514–1524. doi:10.1002/pd.6232
19. Srebniak MI, Diderich KE, Govaerts LC, et al. Types of array findings detectable in cytogenetic diagnosis: a proposal for a generic classification. Eur J Hum Genet. 2014;22(7):856–858. doi:10.1038/ejhg.2013.254
20. Van El CG, Cornel MC, Borry P, et al. Whole-genome sequencing in health care. Euro J Human Genet. 2013;21(6):580–584. doi:10.1038/ejhg.2013.46
21. Berg JS, Khoury MJ, Evans JP. Deploying whole genome sequencing in clinical practice and public health: meeting the challenge one bin at a time. Genet Med. 2011;13(6):499–504. doi:10.1097/GIM.0b013e318220aaba
22. Klapwijk JE, Srebniak MI, Go A, et al. How to deal with uncertainty in prenatal genomics: a systematic review of guidelines and policies. Clin Genet. 2021;100(6):647–658. doi:10.1111/cge.14010
23. Vears DF, Senecal K, Clarke AJ, et al. Points to consider for laboratories reporting results from diagnostic genomic sequencing. Eur J Hum Genet. 2018;26(1):36–43. doi:10.1038/s41431-017-0043-9
24. Kalia SS, Adelman K, Bale SJ, et al. Recommendations for reporting of secondary findings in clinical exome and genome sequencing, 2016 update (ACMG SF v2. 0): a policy statement of the American College of Medical Genetics and Genomics. Genet Med. 2017;19(2):249–255. doi:10.1038/gim.2016.190
25. Hegde M, Bale S, Bayrak-Toydemir P, et al. Reporting incidental findings in genomic scale clinical sequencing—a clinical laboratory perspective: a report of the association for molecular pathology. J Mol Diag. 2015;17(2):107–117. doi:10.1016/j.jmoldx.2014.10.004
26. Miller DT, Lee K, Chung WK, et al. Correction to: ACMG SF v3.0 list for reporting of secondary findings in clinical exome and genome sequencing: a policy statement of the American College of Medical Genetics and Genomics (ACMG). Genet Med. 2021;23(8):1582–1584. doi:10.1038/s41436-021-01278-8
27. Hufnagel SB, Antommaria AH. Laboratory policies on reporting secondary findings in clinical whole exome sequencing: initial uptake of the ACMG’s recommendations. Am J Med Genet A. 2014;164A(5):1328–1331. doi:10.1002/ajmg.a.36398
28. Armour CM, Dougan SD, Brock J-A, et al. Practice guideline: joint CCMG-SOGC recommendations for the use of chromosomal microarray analysis for prenatal diagnosis and assessment of fetal loss in Canada. J Med Genet. 2018;55(4):215–221. doi:10.1136/jmedgenet-2017-105013
29. Skirton H, Goldsmith L, Jackson L, Lewis C, Chitty L. Offering prenatal diagnostic tests: European guidelines for clinical practice [corrected]. Eur J Hum Genet. 2014;22(5):580–586. doi:10.1038/ejhg.2013.205
30. Vetro A, Bouman K, Hastings R, et al. The introduction of arrays in prenatal diagnosis: a special challenge. Hum Mutat. 2012;33(6):923–929. doi:10.1002/humu.22050
31. Gardiner C, Wellesley D, Kilby MD, Kerr B. Joint Committee on Genomics in M. Recommendations for the use of chromosome microarray in pregnancy. London. 2015;2015:290615.
32. Vanakker O, Vilain C, Janssens K, et al. Implementation of genomic arrays in prenatal diagnosis: the Belgian approach to meet the challenges. Eur J Med Genet. 2014;57(4):151–156. doi:10.1016/j.ejmg.2014.02.002
33. Suela J, López-Expósito I, Querejeta ME, et al. Recommendations for the use of microarrays in prenatal diagnosis. Med Clín. 2017;148(7):328.e1–328. e8. doi:10.1016/j.medcle.2016.12.065
34. Dugoff L, Norton ME, Kuller JA. The use of chromosomal microarray for prenatal diagnosis. Am J Obstet Gynecol. 2016;215(4):B2–B9. doi:10.1016/j.ajog.2016.07.016
35. van der Steen SL, Bunnik EM, Polak MG, et al. Choosing between higher and lower resolution microarrays: do pregnant women have sufficient knowledge to make informed choices consistent with their attitude? J Genet Couns. 2018;27(1):85–94. doi:10.1007/s10897-017-0124-5
36. Levy B, Wapner R. Prenatal diagnosis by chromosomal microarray analysis. Fertil Steril. 2018;109(2):201–212. doi:10.1016/j.fertnstert.2018.01.005
37. Darilek S, Ward P, Pursley A, et al. Pre- and postnatal genetic testing by array-comparative genomic hybridization: genetic counseling perspectives. Genet Med. 2008;10(1):13–18. doi:10.1097/GIM.0b013e31815f1ddb
38. Srebniak M, Boter M, Oudesluijs G, et al. Application of SNP array for rapid prenatal diagnosis: implementation, genetic counselling and diagnostic flow. Eur J Hum Genet. 2011;19(12):1230–1237. doi:10.1038/ejhg.2011.119
39. McGillivray G, Rosenfeld JA, McKinlay Gardner RJ, Gillam LH. Genetic counselling and ethical issues with chromosome microarray analysis in prenatal testing. Prenat Diagn. 2012;32(4):389–395. doi:10.1002/pd.3849
40. Klugman S, Suskin B, Spencer BL, et al. Clinical utility of chromosomal microarray analysis in prenatal diagnosis: report of first 6 months in clinical practice. J Matern Fetal Neonatal Med. 2013;27:1333–1338. doi:10.3109/14767058.2013.858243
41. Riedijk S, Diderich KEM, van der Steen SL, et al. The psychological challenges of replacing conventional karyotyping with genomic SNP array analysis in prenatal testing. J Clin Med. 2014;3(3):713–723. doi:10.3390/jcm3030713
42. Vora NL, Gilmore K, Brandt A, et al. An approach to integrating exome sequencing for fetal structural anomalies into clinical practice. Genet Med. 2020;22(5):954–961. doi:10.1038/s41436-020-0750-4
43. Westerfield LE, Stover SR, Mathur VS, et al. Reproductive genetic counseling challenges associated with diagnostic exome sequencing in a large academic private reproductive genetic counseling practice. Prenat Diagn. 2015;35(10):1022–1029. doi:10.1002/pd.4674
44. Claustres M, Kožich V, Dequeker E, et al. Recommendations for reporting results of diagnostic genetic testing (biochemical, cytogenetic and molecular genetic). Euro J Human Genet. 2014;22(2):160–170. doi:10.1038/ejhg.2013.125
45. Silva M, De Leeuw N, Mann K, et al. European guidelines for constitutional cytogenomic analysis. Euro J Human Genet. 2019;27(1):1–16. doi:10.1038/s41431-018-0244-x
46. Lazier J, Hartley T, Brock JA, et al. Clinical application of fetal genome-wide sequencing during pregnancy: position statement of the Canadian College of Medical Geneticists. J Med Genet. 2021;59:931–937. doi:10.1136/jmedgenet-2021-107897
47. Directors AB. ACMG policy statement: updated recommendations regarding analysis and reporting of secondary findings in clinical genome-scale sequencing. Genet Med. 2015;17(1):68–69. doi:10.1038/gim.2014.151
48. Christenhusz GM, Devriendt K, Dierickx K. To tell or not to tell? A systematic review of ethical reflections on incidental findings arising in genetics contexts. Eur J Hum Genet. 2013;21(3):248–255. doi:10.1038/ejhg.2012.130
49. Saelaert M, Mertes H, Moerenhout T, De Baere E, Devisch I. Criteria for reporting incidental findings in clinical exome sequencing - a focus group study on professional practices and perspectives in Belgian genetic centres. BMC Med Genom. 2019;12(1):123. doi:10.1186/s12920-019-0561-0
50. van der Schoot V, Damste C, Yntema HG, Brunner HG, Oerlemans AJM. Clinical geneticists’ views on and experiences with unsolicited findings in next-generation sequencing: “A great technology creating new dilemmas”. J Genet Couns. 2022;32:387–396. doi:10.1002/jgc4.1647
51. Best S, Wou K, Vora N, Van der Veyver IB, Wapner R, Chitty LS. Promises, pitfalls and practicalities of prenatal whole exome sequencing. Prenat Diagn. 2018;38(1):10–19. doi:10.1002/pd.5102
52. Horn R, Parker M. Opening Pandora’s box?: ethical issues in prenatal whole genome and exome sequencing. Prenat Diagn. 2018;38(1):20–25. doi:10.1002/pd.5114
53. Kilby MD, Mackie FL, Cox P. The role of Next Generation Sequencing in the investigation of ultrasound identified fetal structural anomalies. BJOG. 2020;127:1507–1515. doi:10.1111/1471-0528.16533
54. Hammond J, Klapwijk JE, Hill M, et al. Parental experiences of uncertainty following an abnormal fetal anomaly scan: insights using Han’s taxonomy of uncertainty. J Genet Couns. 2020;30:198–210. doi:10.1002/jgc4.1311
55. Srebniak MI, Van Opstal D, Joosten M, et al. Whole-genome array as a first-line cytogenetic test in prenatal diagnosis. Ultrasound Obstet Gynecol. 2015;45(4):363–372. doi:10.1002/uog.14745
56. Liu P, Meng L, Normand EA, et al. Reanalysis of clinical exome sequencing data. New England J Med. 2019;380(25):2478–2480. doi:10.1056/NEJMc1812033
57. Kono M, Niizawa M, Takeichi T, Muro Y, Akiyama M. Hailey-Hailey disease due to ATP2C1 splice site mutation, successfully treated with minocycline hydrochloride. J Eur Acad Dermatol Venereol. 2018;32(1):e19–e20. doi:10.1111/jdv.14439
58. Srebniak MI, Diderich KE, Joosten M, et al. Prenatal SNP array testing in 1000 fetuses with ultrasound anomalies: causative, unexpected and susceptibility CNVs. Eur J Hum Genet. 2016;24(5):645–651. doi:10.1038/ejhg.2015.193
59. van der Schoot V, Haer-Wigman L, Feenstra I, et al. Lessons learned from unsolicited findings in clinical exome sequencing of 16,482 individuals. Eur J Hum Genet. 2022;30(2):170–177. doi:10.1038/s41431-021-00964-0
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.