Back to Journals » Infection and Drug Resistance » Volume 16
Cerebral Abscess Infected by Nocardia gipuzkoensis
Authors Li X, Feng Y, Li D, Chen L, Shen M, Li H, Li S, Wu X, Lu L
Received 30 June 2023
Accepted for publication 31 October 2023
Published 15 November 2023 Volume 2023:16 Pages 7247—7253
DOI https://doi.org/10.2147/IDR.S428415
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Xiaosi Li,1 Yan Feng,2 Dan Li,3 Liyang Chen,1 Mengli Shen,1 Hongsheng Li,1 Shuo Li,3 Xiaoyan Wu,1 Lingling Lu3
1Department of Clinical Laboratory, The Second Affiliated Hospital of Jiaxing University, Jiaxing, People’s Republic of China; 2Department of Clinical Laboratory, Jiaxing Maternity and Child Health Care Hospital Affiliated to Jiaxing University, Jiaxing, People’s Republic of China; 3Key laboratory of Digital Technology in Medical Diagnostics of Zhejiang Province, Dian Diagnostics Group Co, Ltd, Hangzhou, People’s Republic of China
Correspondence: Lingling Lu, Key laboratory of Digital Technology in Medical Diagnostics of Zhejiang Province, Dian Diagnostics Group Co, Ltd, No. 329, Jinpeng Street, Sandun Town, West Lake District, Hangzhou, Zhejiang Province, 310000, People’s Republic of China, Tel +86-13587528187, Email [email protected] Xiaoyan Wu, Department of Clinical Laboratory, the Second Affiliated Hospital of Jiaxing University, No. 1518, North Huancheng Road, Nanhu District, Jiaxing, Zhejiang Province, 314000, People’s Republic of China, Tel +86-13586330218, Email [email protected]
Purpose: Nocardia gipuzkoensis is a novel species that solely identified in patients with pulmonary infections by far. Growing evidence showed the excellent performance of metagenomics next-generation sequencing (mNGS) on pathogenic identification, especially for new species. Here, we described the first case of an elderly female patient suddenly suffering from neurological disorders owing to N. gipuzkoensis infection. And linezolid could effectively treat N. gipuzkoensis infection.
Patients and Methods: The results of imaging, laboratory cultures, and mNGS, as well as therapeutic process are shared.
Results: An elderly female patient suddenly suffered from neurological disorders with dysphasia and right limb trembles under no obvious causes. Subsequently, she was diagnosed as intracranial space-occupying lesions by magnetic resonance imaging (MRI). The isolate from brain secretion was further identified as N. gipuzkoensis through mNGS. The targeted therapy with linezolid according to the antimicrobial susceptibility was used to treat cerebral abscess induced by N. gipuzkoensis. During the follow-up, no relapse was observed for the patient after surgery for 104 days.
Conclusion: Cerebral abscess induced by N. gipuzkoensis is rare disorder with high mortality. mNGS has been identified as a promising tool in pathogen diagnosis for timely therapy. Linezolid as one of the antimicrobial drugs could effectively treat N. gipuzkoensis infection and prevent adverse outcomes.
Keywords: Nocardia gipuzkoensis, cerebral abscess, metagenomics next-generation sequencing, linezolid, mNGS
Introduction
The genus of Nocardia is aerobic, Gram-positive, weakly acid-fast, and branching bacilli bacteria that widely distributed in soil, water, and degraded organic material.1,2 Over recent years, an increasing number of species have been recognized as pathogens causing pulmonary and cutaneous infections through respiratory inhalation and wound, respectively.3,4 In addition, cerebral abscess caused by Nocardia is infrequent with a worldwide estimated incidence ranging from 0.3 to 1.3 per 100,000 persons per year.5 While nocardial cerebral abscess represents more than three times mortality compared with other pathogens,6,7 and a recent systematic review highlighted 22.8% mortality in all cases with CNS nocardiosis.2 Significantly, it is a novel Nocardia species that was identified in a patient with cerebral abscess through metagenomics next-generation sequencing (mNGS). As we all know, the cases infected by N. gipuzkoensis has solely been reported in patients with bronchiectasis.8,9 We now described a rare case of cerebral abscess infected by N. gipuzkoensis in an elderly female patient. And the process of treatment was also shared (Figure 1).
 |
Figure 1 Imaging changes documented the alleviation of brain lesions during the timeline of treatment (a) The initial image of brain MRI at external healthcare center, and the section that indicated by red arrow represented intracranial space-occupying lesions. (b) The image of brain MRI before surgery in our hospital, the region that indicated by red arrows suggested further exacerbation of brain lesion. (c) The image of brain MRI in early postoperative, the region that indicated by red arrow documented the removal of cerebral abscess and existence of perilesional edema. (d) The brain CT scan of day 25 after surgery, documented recovered well of brain lesions without a relapse. |
Case Description
A 71-year-old female patient was admitted to our hospital. Twenty-five days before the admission, she suddenly presented with neurological symptoms such as dysphasia and right limb trembling with no obvious causes. She was diagnosed as intracranial space-occupying lesions at Pinghu hospital of traditional Chinese medicine through magnetic resonance imaging (MRI) scanning (Figure 1a). Then the patient was discharged and admitted into the first hospital of Jiaxing. The further extending of brain lesions was reflected by the images of brain MRI showing a space-occupying rounded lesion in left parietal and abnormal signal in the right frontal lobe (Figure 1b). Finally, the patient was admitted to our hospital for treatment owing to the unsolved cerebral lesions.
On admission, the patient had no obvious traumas or liquid secretions on brain, ear, or nose. Physical detection showed that normal consciousness state, sensitive to light reflex, soft neck, normal limb muscle strength, and negative for brain nerve system. Meanwhile, the inflammatory in the upper lobe of the left lung was observed. Except it, no obvious positive signs were observed in cardiopulmonary and abdominal examinations. There were no surgical contraindications that suggested by multiple preoperative detection. The leukocyte count was 6×109/L (normal range is 3.5–9.5×109/L), and ultra-sensitive C reaction protein was 9.07 mg/L (normal range is 0–8 mg/L), the percentage of neutropenia was 52.50 (normal range is 40–75%), the concentration of hemoglobin was 124 g/L (normal range is 130–175 g/L), and the packed cell volume was measured at 38.1% (normal range is 40–50%), respectively. A cerebral lesion resection with the excision and drainage of the abscess was carried out for the patient. Then surgical specimens were sent for histopathological examination along with pathology, culture, and mNGS. After that, the injections of vancomycin (1g, q12h) and meropenem (2g, q8h) were used as empirical treatment.
Postoperatively, the decreased hypointense image in left parietal lesion and surrounding loch were observed through MRI that indicating the removal of lesions and the existence of perilesional edema (Figure 1c). Three-days after surgery, the isolate from cerebral abscess exhibited characteristic of Nocardia genus with the appearance of white, rough, dry colonies on Columbia blood agar medium. mNGS further identified it as N. gipuzkoensis with the 99% similarity according to the Sequence Read Archive (SRA) database (Table 1). And the bacteria with branching rods showed weakly acid-fast (Figure 2). In addition, the isolate of Nocardia genus was not detected in the sputum sample from the patient. And the lesions in lung without obvious changes was observed through lung CT. These findings suggested that the cerebral abscess was affected by N. gipuzkoensis, which is independent of lung infection.
 |
Table 1 Identification of Nocardia Genus in Cerebral Abscess Using mNGS |
 |
Figure 2 Microbiology detection of N. gipuzkoensis. (a) The traditional culture of cerebral abscess with the pale yellow, rough, and dry colonies on Columbia Blood Agar medium. (b) The characteristic of weakly acid-fast was identified by acid-fast staining. |
Antimicrobial drug susceptibility testing showed that the isolate was susceptible to several antibiotics, including amikacin, linezolid, sulfamethoxazole-trimethoprim (SMZ-TMP) and ceftriaxone (Table 2). According to above, the patient originally received meropenem (2.0g q8h) injection for one time, then orally received linezolid (0.6g, q12h) for continual 3 days. The patient decided to discharge home 12 days after surgery, because she recovered well from the treatment and was no longer suffered from neurological symptoms. Then brain computed tomography (CT) 25 days after surgery documented the complete removal of lesions (Figure 1d). Subsequently, linezolid and sodium valproate sustained-release tablets were continually used for 28 days. Neurological disorders and side effects were not observed in the course of her treatment.
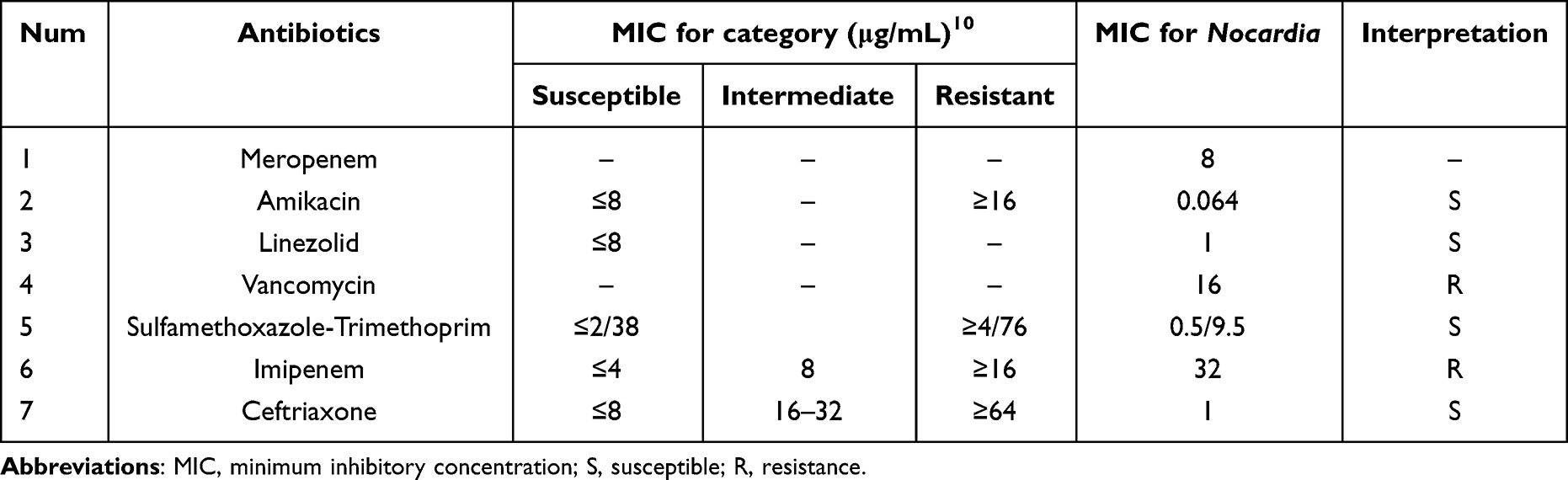 |
Table 2 Antimicrobial Drug Susceptibility Testing of Nocardia Gipuzkoensis |
Discussion
Nocardia genus contains a great number of rare opportunistic bacteria that mainly causing pulmonary infections.3,8,11,12 For extra-pulmonary infections, the central nervous system (CNS) is the most frequent site that exhibits headache, seizures, mental status change, aphasia, and hemiparesis in patients.13 Nocardial cerebral abscesses account for about 1–2% of all brain abscesses. Reports involved in N. gipuzkoensis infections were solely detected in patients with bronchiectasis, the brain abscesses were all caused by other than N. gipuzkoensis, including N. farcinica, N. asteroides, N. cyriacigeorgica, N. asiatica, and N. beijingensis (Table 3). Herein, as a novel strain, the first case of cerebral abscess infected by N. gipuzkoensis was described in an elderly female who suddenly suffered from neurological disorders without obvious causes.
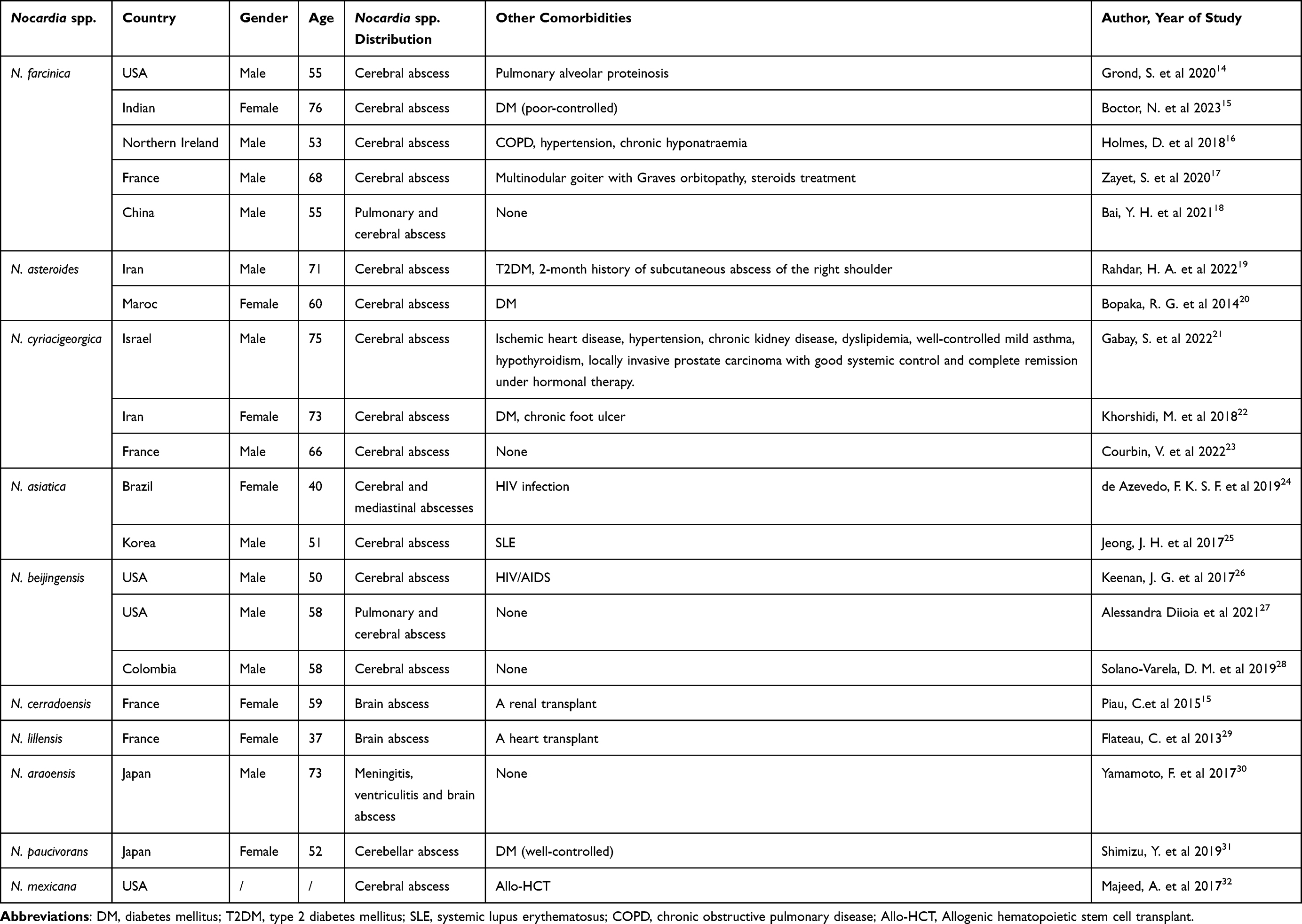 |
Table 3 Summarizes Some Data from the Case Literature of Cerebral Abscess Infected by Nocardia spp. in Patients |
Nocardial cerebral abscess is generally related to immunodeficiency. While infectious cases of Nocardia spp. in immunocompetent individuals have also been observed. A higher risk of nocardial cerebral abscess challenged individuals with immunosuppression owing to diabetes mellitus, malignancy, solid organ transformation, corticosteroid treatment, HIV/AIDS, and autoimmune disease.5,14–16,20–22,24–26,28–34 No obvious immunosuppression was seen in the patient we described, the chronic inflammatory owing to aging within patient might partly explain the occurrence of nocardiosis, leading to the immunocompromised status.6
In general, the clinical diagnosis of nocardiosis is extremely challenged due to nonspecific and insidious characteristics compared with other bacterial infections. Up to now, culture is still the gold standard for aetiology, it usually takes about 2 to 7 days for the cultures of Nocardia species to be positive. Compared with traditional culture, mNGS was more sensitive and efficient in detecting Nocardia species, showing tremendous application in rapid diagnosis.35 In our case, mNGS identified the pathogen of brain secretion as N. gipuzkoensis to assist targeted treatment in clinical. We believe that mNGS would be a promising tool in clinical practice.
Vancomycin, as the first-line antibiotic, has been suggested as a good therapeutic option for infections.36,37 Here, the empirical treatment postoperatively with the combination of vancomycin and meropenem was inaccurate according to the antibiotic susceptibility of the strain. In our study, N.gipuzkonesis was susceptible to sulfamethoxazole-trimethoprim (SMX-TMP) and linezolid. Reviewing the literature, more than 98% of Nocardia genus was sensitive to SMX-TMP treatment, then SMX-TMP has become the primary agent for primary skin nocardiosis and nonsevere lung infection.38 Compared with SMX-TMP, a wider antimicrobial spectrum of linezolid was observed in many studies.38 Linezolid showed bacteriostatic activity against almost all G-positive bacteria, especially for Nocardia spp (100%). Besides, the concentrations of cerebrospinal fluid (CSF) in neurosurgical patients who were treated with recommended dose of linezolid were largely exceeded the minimum inhibitory concentration of the isolates, indicating the excellent penetration of linezolid in the CSF.39,40 It is to keep linezolid for severe cases or brain infection due to its large CNS penetration, it would be an alternative therapy with rare and mild side effects. In our case, we switched to orally linezolid without relapse of neurological symptoms during 104-day follow-up, indicating linezolid could be potential used for empiric treatment of nocardiosis in China.
Limitation
We have reported a case of an elderly female suffering from intracranial lesions that infected by N. gipuzkoensis. However, the mechanisms and contributes of the strain on brain lesions were needed to be further explored in animal studies.
Conclusion
In conclusion, this report described a CNS infection by a new Nocardia species (N. gipuzkoensis) identified by mNGS. Owing to the limited treatment of vancomycin, linezolid could be promising therapy for the treat of N. gipuzkoensis infection.
Data Sharing Statement
The original data of Nocardia gipuzkoensis sequencing has been submitted in GenBank. The names of the repository/repositories and accession number(s) can be found below: https://www.ncbi.nlm.nih.gov/, PRJNA981362.
Ethics and Consent
Written informed consent was provided by the patient to have the case details and any accompanying images published. Our report was approved by the Medical Ethics Committee of the Second Affiliated Hospital of Jiaxing University in accordance with the principles stated in the Declaration of Helsinki to publish the case details (Approval NO., 2023-CA-22).
Disclosure
The author declare that the study was conducted in the absence of any commercial or financial relationships that could be considered as potential conflict of interest.
References
1. Fatahi-Bafghi M. Nocardiosis from 1888 to 2017. Microb Pathog. 2018;114:369–384. doi:10.1016/j.micpath.2017.11.012
2. Meena DS, Kumar D, Bohra GK, Midha N, Garg MK. Clinical characteristics and treatment outcome of central nervous system nocardiosis: a systematic review of reported cases. Med Principl Pract. 2022;31(4):333–341. doi:10.1159/000525509
3. Abe S, Tanabe Y, Ota T, Fujimori F, Youkou A, Makino M. Case report: pulmonary nocardiosis caused by Nocardia exalbida in an immunocompetent patient. BMC Infect Dis. 2021;21(1):776. doi:10.1186/s12879-021-06416-w
4. Alavi Darazam I, Shamaei M, Mobarhan M, et al. Nocardiosis: risk factors, clinical characteristics and outcome. Iran Red Crescent Med J. 2013;15(5):436–439. doi:10.5812/ircmj.2384
5. Matthijs CB, Jonathan MC, Diederik van de B. Clinical characteristics and outcome of brain abscess. Neurology. 2014;82(9):806. doi:10.1212/WNL.0000000000000172
6. Corsini Campioli C, Castillo Almeida NE, O’Horo JC, et al. Clinical presentation, management, and outcomes of patients with brain abscess due to nocardia species. Open Forum Infect Dis. 2021;8(4):ofab067. doi:10.1093/ofid/ofab067
7. Brouwer MC, Coutinho JM, van de Beek D. Clinical characteristics and outcome of brain abscess: systematic review and meta-analysis. Neurology. 2014;82(9):806–813. doi:10.1212/WNL.0000000000000172
8. Liu C, Yang J, Huang H, Zhan S, Xia X. Case report: nocardia gipuzkoensis infection in an immunocompetent patient diagnosed by metagenomic next-generation sequencing and whole genome sequencing. Front Immunol. 2022;13:1053914. doi:10.3389/fimmu.2022.1053914
9. Nouioui I, Cortes-Albayay C, Neumann-Schaal M, et al. Genomic virulence features of two novel species nocardia barduliensis sp. nov. and nocardia gipuzkoensis sp. nov., isolated from patients with chronic pulmonary diseases. Microorganisms. 2020;8(10):1517. doi:10.3390/microorganisms8101517
10. Woods GL, Brown-Elliott BA, Conville PS, et al. Susceptibility testing of mycobacteria, nocardiae, and other aerobic actinomycetes. CLSI Standards: Guidelines for Health Care Excellence; 2011.
11. Li J, Cao J, Wu Y, Wan N, Pan L, Chen Y. A case of an immunocompetent young man obtaining community-acquired disseminated Nocardia brasiliensis. Heart Lung. 2014;43(2):164–167. doi:10.1016/j.hrtlng.2013.12.002
12. Mamelak AN, Obana WG, Flaherty JF, Rosenblum ML. Nocardial brain abscess: treatment strategies and factors influencing outcome. Neurosurgery. 1994;35(4):622–631. doi:10.1227/00006123-199410000-00007
13. Martinez-Barricarte R. Isolated nocardiosis, an unrecognized primary immunodeficiency? Front Immunol. 2020;11:590239. doi:10.3389/fimmu.2020.590239
14. Grond SE, Schaller A, Kalinowski A, Tyler KA, Jha P. Nocardia farcinica brain abscess in an immunocompetent host with pulmonary alveolar proteinosis: a case report and review of the literature. Cureus J Med Sci. 2020;12(11):e11494. doi:10.7759/cureus.11494
15. Boctor N, Aronowitz P. brain abscess in a patient with diabetes: a case report. J Med Case Rep. 2023;17(1):336. doi:10.1186/s13256-023-04071-0
16. Holmes DN, Armstrong L, Bennett J, Simms HN. Neurosurgical management of multiple intracranial and abscesses in an immunocompetent patient. J Surg Case Rep. 2018;2018(2):rjy015. doi:10.1093/jscr/rjy015
17. Zayet S, Lang S, Ben Abdallah Y, Klopfenstein T, Gendrin V. Asymptomatic cerebral abscesses after pleuropulmonary infection. New Microb New Infec. 2020;38:100808. doi:10.1016/j.nmni.2020.100808
18. Bai YH, Liu KY, Chen YQ, et al. Disseminated infection of Nocardia farcinica in an immunocompetent adult: mistaken for tuberculosis bacilli in acid-fast staining of bronchoalveolar lavage fluid. Journal of Cytology. 2021;38(2):106–108. doi:10.4103/Joc.Joc_208_20
19. Rahdar HA, Heidari H, Karami-Zarandi M, Soori T, Asadollahi P, Kazemian H. Brain abscess caused by in a diabetic patient: a rare case report. Yale J Biol Med. 2022;95(4):407–411. doi:10.1128/cmr.19.2.259-282.2006
20. Bopaka RG, Janah H, Khattabi WE, Aichane A, Afif H. Pleurésie purulente à Nocardia asteroides. Pan Af Med J. 2014;18. doi:10.11604/pamj.2014.18.346.5132
21. Gabay S, Yakubovsky M, Ben-Ami R, Grossman R. Nocardia cyriacigeorgica brain abscess in a patient on low dose steroids: a case report and review of the literature. BMC Infect Dis. 2022;22(1):635. doi:10.1186/s12879-022-07612-y
22. Khorshidi M, Navid S, Azadi D, Shokri D, Shojaei H. A case report of brain abscess caused by Nocardia cyriacigeorgica in a diabetic patient. JMM Case Rep. 2018;5(9). doi:10.1099/jmmcr.0.005133
23. Courbin V, Riller Q, Amegnizin JL, et al. Case report: cerebral nocardiosis caused by detected by metagenomics in an apparently immunocompetent patient. Front Immunol. 2022;13:719124. doi:10.3389/fimmu.2022.719124
24. de Azevedo FKSF, Dutra V, Souto FJD. Cerebral and mediastinal abscesses caused by in an HIV-infected patient. Rev Soc Bras Med Tro. 2019;52:e20180485. doi:10.1590/0037-8682-0485-2018
25. Jeong JH, Moon SM, Park PW, et al. Multiple brain abscesses caused by in a patient with systemic lupus erythematosus: the first case report and literature review. Ann Lab Med. 2017;37(5):459–461. doi:10.3343/alm.2017.37.5.459
26. Keenan JG, Mohapatra S. Nocardia beijingensis brain abscesses in an HIV-infected individual. IDCases. 2017;9:65–69. doi:10.1016/j.idcr.2017.03.006
27. Diioia A, Kalra L, Krop LC. Stroke like presentation of disseminated CNS infection in an immunocompetent patient: case report and review of the literature. IDCases. 2021;25:e01223. doi:10.1016/j.idcr.2021.e01223
28. Solano-Varela DM, Barrios-Vidales EM, Plaza DF, et al. Immunocompetent patient with a brain abscess caused by Nocardia beijingensis in Latin America. Medicine. 2019;98(11):e14879. doi:10.1097/MD.0000000000014879
29. Flateau C, Jurado V, Lemaitre N, et al. First case of cerebral abscess due to a novel species in an immunocompromised patient. J Clin Microbiol. 2013;51(2):696–700. doi:10.1128/Jcm.00762-12
30. Yamamoto F, Yamashita S, Kawano H, et al. Meningitis and Ventriculitis due to Infection. Internal Med. 2017;56(7):853–859. doi:10.2169/internalmedicine.56.7332
31. Shimizu Y, Tsuchiya K, Fujisawa H. Nocardia paucivorans cerebellar abscess: surgical and pharmacotherapy. Surg Neurol Int. 2019;10(1). doi:10.4103/sni.sni_370_18
32. Majeed A, Mushtaq A, Zangeneh T, et al. Intractable cerebral in a GvHD patient successfully treated with linezolid. Bone Marrow Transpl. 2017;52(10):1476–1478. doi:10.1038/bmt.2017.167
33. Piau C, Kerjouan M, Le Mouel M, et al. First Case of Disseminated Infection with in a Human. J Clin Microbiol. 2015;53(3):1034–1037. doi:10.1128/Jcm.02979-14
34. Wang CH, Sun Q, Yan J, et al. The species distribution and antimicrobial resistance profiles of species in China: a systematic review and meta-analysis. PLoS Neglect Trop D. 2023;17(7):e0011432. doi:10.1371/journal.pntd.0011432
35. Weng SS, Zhang HY, Ai JW, et al. Rapid detection of nocardia by next-generation sequencing. Front Cell Infect Microbiol. 2020;10:13. doi:10.3389/fcimb.2020.00013
36. Pfausler B, Spiss H, Beer R, et al. Treatment of staphylococcal ventriculitis associated with external cerebrospinal fluid drains: a prospective randomized trial of intravenous compared with intraventricular vancomycin therapy. J Neurosurg. 2003;98(5):1040–1044. doi:10.3171/jns.2003.98.5.1040
37. Hasanpour M, Rezaee H, Samini F, Keykhosravi E. Effects of intraventricular vancomycin administration on the prevention of ventricular shunt infection. J Neurol Surg a Cent Eur Neurosurg. 2023. doi:10.1055/a-2104-1461
38. Yang J, Ren H-T, Wang J, et al. Clinical characteristics, susceptibility profiles, and treatment of nocardiosis: a multicenter retrospective study in 2015–2021. Inter J Infect Dis. 2023;130:136–143. doi:10.1016/j.ijid.2023.02.023
39. Viale P, Pagani L, Cristini F, et al. Linezolid for the treatment of central nervous system infections in neurosurgical patients. Scand J Infect Dis. 2002;34(6):456–459. doi:10.1080/00365540110080467
40. Rupprecht TA, Pfister HW. Clinical experience with linezolid for the treatment of central nervous system infections. Eur J Neurol. 2005;12(7):536–542. doi:10.1111/j.1468-1331.2005.01001.x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Sequential Therapy of Linezolid and Contezolid to Treat Hematogenous Lung Abscess Caused by Staphylococcus aureus in a Congenital Cerebral Hypoplasia Patient: A Case Report
Zhou S, Xin C, Liu W
Infection and Drug Resistance 2025, 18:253-260
Published Date: 13 January 2025