Back to Journals » Journal of Pain Research » Volume 15
Central Sensitization in Migraine: A Narrative Review
Authors Suzuki K ![]() , Suzuki S, Shiina T, Kobayashi S, Hirata K
, Suzuki S, Shiina T, Kobayashi S, Hirata K
Received 27 May 2022
Accepted for publication 16 August 2022
Published 7 September 2022 Volume 2022:15 Pages 2673—2682
DOI https://doi.org/10.2147/JPR.S329280
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Natalie Strand
Keisuke Suzuki, Shiho Suzuki, Tomohiko Shiina, Saro Kobayashi, Koichi Hirata
Department of Neurology, Dokkyo Medical University, Mibu, Japan
Correspondence: Keisuke Suzuki, Department of Neurology, Dokkyo Medical University, 880 Kitakobayashi, Shimotsuga, Mibu, Tochigi, 321-0293, Japan, Tel +81-282-86-1111, Fax +81-282-86-5884, Email [email protected]
Abstract: Central sensitization (CS) is an increase in the responsiveness of nociceptive neurons in the central nervous system to their normal afferent input. As a result, even minor irritation can induce severe pain, leading to the chronicity and severity of various diseases, such as neurological disorders. CS is associated with migraine, which is a major neurological disorder that inflicts a high disability in daily life. Specifically, CS is thought to be involved in the pathogenesis of cutaneous allodynia as well as chronification of migraine. In this article, we reviewed the association between CS and migraine, including pathophysiological aspects and evidence from clinical studies. We suggest that appropriate screening and management of CS in migraine could further improve the quality of life of migraine patients.
Keywords: migraine, central sensitization, cutaneous allodynia, restless legs syndrome
Introduction
Central sensitization (CS) occurs when the function of circuits in nociceptive pathways is enhanced and results in abnormal sensitivity; it is defined as “increased responsiveness of nociceptive neurons in the central nervous system to their normal or subthreshold afferent input” according to the International Association for the Study of Pain.1 An original work by Woolf2 showed that a peripheral injury-induced increase in the excitability of spinal cord neurons profoundly modifies the gain of the somatosensory system. While peripheral sensitization is an increase in the sensitivity of the local peripheral terminals of sensory fibers that innervate injured tissue, CS involves the central nervous system. Moreover, CS can occur due to tissue damage after peripheral nerve injury but also in diseases without any peripheral pathology, such as migraine, fibromyalgia, temporomandibular joint disease, and irritable bowel syndrome.3 A multicenter case–controlled study showed higher central sensitization inventory (CSI) scores in patients with various neurological, psychological, and pain disorders, including migraine, than in healthy controls. Additionally, CS-related symptoms were associated with pain severity, interference of pain with daily activities, and depressive symptoms in the patient group.4 Therefore, the management of CS-related pain and symptoms in various pain-related diseases is urgent. Migraine is a major neurological disorder that inflicts a high disability in daily life, and many patients suffer from intractable pain. Although genetic predisposition and activation of the trigeminal vasculature are considered the main pathophysiological factors for migraine,5 CS is thought to be involved in the pathogenesis of cutaneous allodynia (CA) and chronicity in migraine. In this article, we provide a narrative review of CS in people with migraine.
Methods
We performed a literature search of MEDLINE, a PUBMED database, and Web of Science to retrieve articles published in the English language between March and May 2022 using a combination of keywords such “migraine” and “central sensitization” or “central sensitization syndrome”. The important literature that was retrieved by handsearching was also included in this review.
Definition and Diagnosis of Central Sensitization
CS clinically manifests as CA (a reduction in the pain threshold of the skin), hyperalgesia (an increase and prolonged responsiveness to noxious stimuli) and secondary hyperalgesia (a spread of sensitivity outside of the region of injury into noninjured tissue).3,6 To diagnose pain due to CS, three major criteria are recommended: 1) experiencing pain disproportionate to the nature and extent of injury or pathology; 2) a diffuse pain distribution and the presence of allodynia and hyperalgesia; and 3) hypersensitivity of senses unrelated to the musculoskeletal system.7 People suffering pain due to CS show hypersensitivity to bright lights, touch, noise, pesticides, mechanical pressure, medication and temperature (low and high), and these symptoms may also be associated with fatigue, sleep disturbances, unrefreshing sleep, concentration difficulties, a feeling of swelling in the limbs, tingling and numbness.7 These characteristics are important in differentiating pain due to CS from neuropathic pain.
Screening Tools for Diagnosing Central Sensitization
The CSI is a widely used self-administered questionnaire for assessing CS-related symptoms in clinical studies.8 Part A of the CSI comprises 25 CS-related items with total scores ranging from 0 to 100. A Part A score≥40 contributes to CS diagnosis and can be used as an alternative to the aforementioned third criterion (hypersensitivity of senses unrelated to the musculoskeletal system).7 Part B of the CSI assesses whether seven CS-related diseases (fibromyalgia, chronic fatigue syndrome, temporomandibular joint disorder, irritable bowel syndrome, migraine or tension headaches, multiple chemical sensitivities and restless legs syndrome (RLS)) were previously diagnosed.9 Additionally, quantitative sensory testing (QST) is a noninvasive method for evaluating the function of the A delta and C fibers.10 By detecting mechanical hyperalgesia and mechanical allodynia, pain due to CS can be evaluated.
As later described, cutaneous allodynia (CA), a skin hypersensitivity often seen in patients with migraine, is believed to be related to the pathogenesis of CS. The Allodynia Symptom Checklist (ASC) consists of 12 questions that inquire about the frequency of various allodynia symptoms associated with headache attacks. The ASC has been validated for usefulness and validity. In a study of 88 patients with migraine, ASC was used to correctly identify 84.8% of patients classified as allodynic by QST.11 In a large survey of 16,573 headache sufferers, the ASC showed that the prevalence of severe CA (ASC score ≥9) was highest in patients with transformed migraine (28.5%) followed by those with migraine (20.4%), probable migraine (12.3%), other chronic daily headaches (6.2%), and severe episodic tension-type headache (5.1%).12 Additionally, for patients with migraine, CA is associated with female sex, headache frequency, increased body mass index, disability, and depression.
A self-rated pain sensitivity questionnaire (PSQ) has been developed to assess pain intensity in daily life as an alternative to experimental pain testing. In a validation study, the results of comprehensive experimental pain testing, including different modalities such as heat, cold, pressure and pinprick, were compared on the PSQ. PSQ scores were significantly correlated with experimental pain intensity ratings, suggesting that PSQ could be a useful, alternative tool for experimental procedures on rating pain intensity in healthy subjects.13 In addition, the validity of the PSQ has been tested in patients with chronic pain. In that study, patients with chronic pain had significantly higher PSQ scores than healthy controls, and PSQ scores were significantly correlated with both experimental pain intensity ratings and experimental pain thresholds.14 The PSQ can be used to directly measure the sensory facilitation involved in CS, whereas the CSI can be used to assess CS in a broader context and the characteristics of CS-related conditions.15
Central Sensitization-Related Diseases
Table 1 shows CS-related diseases.6,9 Patients with restless legs syndrome (RLS) showed decreased pain thresholds and enhanced temporal summation of thermal pain, indicating involvement of spinal levels and supraspinal processes.16 A study comprising 11 RLS patients showed static mechanical hyperalgesia to puncture stimuli, which was reversed by long-term dopaminergic treatment. This observation suggests that RLS is associated with CS of spinal cord neurons due to abnormal peripheral input or altered spinal cord ascending inhibitory dopaminergic control.17 The symptoms of chronic fatigue syndrome (CFS) and fibromyalgia (FM) overlap in that both cause debilitating fatigue and chronic widespread pain. In patients with FM, abnormal pain modulation has been attributed to dysregulation of thalamic activity and hypoperfusion of the caudate nucleus according to imaging studies.18 When pain is induced in FM patients, there is no observation of significant activation of the thalamus, but bilateral activation of the somatosensory cortex and right anterior cingulate is observed,19 which is characteristic of patients with allodynia. Patients with CFS have been reported to have lower pain thresholds and hyperalgesia at various sites compared to controls.20 As with FM, the absence of peripheral tissue damage together with the lack of a clear localization of pain in patients with CFS suggests that CS may be the cause of chronic widespread pain.18
 |
Widespread bilateral mechanical and thermal pain sensitivity was reported in female patients with temporomandibular disorders compared to age-matched controls,21 suggesting that CS has a role. The relationship between migraine and CS will be later discussed in detail. During headache attacks in patients with tension-type headache, muscle tenderness was increased in the temporal region and thermal pain thresholds were decreased, but were normal in the hands, indicating that a segmental central sensitization may contribute to pain in patients with frequent tension-type headache.22
Most patients with irritable bowel syndrome (IBS) show both rectal and somatic sensitivity;6 recurrent sigmoid colon stimulation in patients with IBS leads to rectal hyperalgesia and visceral somatic reactions.23 In contrast, rectal local anesthesia decreases rectal and somatic pain in patients with IBS, suggesting CS involvement in IBS patients. Multiple chemical sensitivity (MCS) is a condition in which chemical intolerance or toxicant-induced loss of tolerance is triggered by exposure to multiple chemical substances. MCS is frequently induced by olfactory stimuli. Compared to controls, patients with MCS reported greater perceived odor intensity and discomfort following exposure to odorants.24 Compared to healthy controls, patients with MCS showed significantly higher bilateral olfactory cortex metabolism at rest.25 These observations suggest that CS is involved in sensory hypersensitivity in patients with MCS.
Imaging Data for Central Sensitization
A functional magnetic resonance imaging (fMRI) study of capsaicin-induced CS in humans revealed activation of the brainstem and thalamus;26 moreover, these were the only areas where activity remained elevated in the hyperalgesic state compared with the normal state, suggesting that brainstem activity contributes to the maintenance of CS. Additionally, a study of capsaicin-induced CS observing somatosensory evoked potentials showed increased excitability in the somatosensory cortex.27 In patients with fibromyalgia, region-specific changes in the gray matter volume of the prefrontal cortex, anterior cingulate cortex, insula, thalamus, pons and left precuneus, altered functional connectivity in the descending pain-modulating system, and increased activity in the pain matrix related to CS, such as the dorsolateral prefrontal cortex, periaqueductal gray and anterior cingulate cortex, have been reported.28 In patients with chronic fatigue syndrome, the white matter volume in the midbrain29 and left inferior fronto-occipital fasciculus are decreased30 and this volume correlated with disease duration. CS also plays a role in chronic lower back pain, a common musculoskeletal disorder. In a study that utilized fMRI, after equal pressure was applied to the thumb nail, patients with chronic lower back pain showed significantly more activation in pain-associated areas, such as the primary and secondary contralateral somatosensory cortex, inferior parietal lobule, cerebellum, and ipsilateral somatosensory cortex, than healthy subjects.31
Migraine
Migraine is a disabling neurological disorder affecting over 1 billion people worldwide, with a one-year prevalence of 15%. Its prevalence peaks in those aged 35–39, and it is the leading cause of disability in people younger than 50 years old, particularly women.32 Migraine is characterized by a recurrent unilateral, pulsating headache, with moderate to severe intensity, accompanied by nausea, vomiting, and sensory hypersensitivity symptoms such as photophobia and phonophobia.33 This disorder can be classified as migraine without aura and migraine with aura. Aura, marked by transient focal neurological symptoms that last 5–60 minutes and usually precede or accompany the headache, is present in one-third of migraine patients. Chronic migraine (CM) is defined as headaches that occur 15 or more days per month for at least 3 months, while episodic migraine (EM) refers to headaches that occur 14 days or less per month. Patients with migraine develop changes in brain activity in association with concomitant symptoms before the headache attack, and these symptoms persist after the attack. Migraine involves multiple phases: the premonitory, aura, headache, postdrome, and interictal phases.34 Hypothalamic activation develops during the premonitory phase, followed by dorsal pontine activation in the headache phase.5,35 During the aura phase, changes in the visual cortex consistent with cortical spreading depression (CSD) have been observed.36 CSD, first described by Leao, is a slowly propagating (2‐5 mm/min) state of altered electrocortical activity accompanied by vasodilation and followed by prolonged inhibition; it is thought to be the neural correlate of the migraine aura.37 A neuroimaging study showed a slowly spreading area of abnormal blood flow, a CSD-like phenomenon, in the occipital lobe during the aura phase of migraine, supporting this concept.36 CSD sensitizes peripheral and central trigeminovascular neurons as shown by stimulating the cortex with pinpricks or potassium chloride (KCl) granules.38 However, whether CSD can trigger migraine headaches is debatable because approximately 70% of migraine patients do not experience an aura, and migraine patients have not usually experienced the trauma that triggers CSD, as in animal studies.
Migraine Pathophysiology is Related to Central Sensitization
Peripheral sensitization is the pain that develops when sensitized nociceptors begin to stimulate the spinal cord with increasing intensity, resulting in further pain amplification known as CS.39 Peripheral sensitization is clinically observed in migraine patients because their migraine headaches are exacerbated by physical activity. CS is associated with abnormal neuronal excitability in the trigeminal nucleus caudalis.39 An animal study showed that astrocytic activation of the trigeminal nucleus caudalis contributed to CS in CM.40 Peripheral sensitization of dural and meningeal trigeminovascular nociceptors is involved in the throbbing nature of migraine headaches. In contrast, CA is considered a manifestation of CS during migraine attacks and could be a marker of CS.39,41
Thus, although CS is thought to be more involved in pain amplification and the chronification of CM than in EM, CS is observed during and between attacks, suggesting that CS may have a role in EM and not only in CM. Plasma glutamate levels, which could be a marker for CS, were significantly higher in patients with CM and EM than those in controls, but they were not significantly different between participants with EM and CM.42 In a study in which researchers used an experimental protocol based on slowly repeated evoked pain (SREP), characteristic patterns were observed in patients with EM, but not in controls, therefore indicating CS in patients with EM.43 A dynamic evoked pain index based on the application of SREP could be used as a CS marker in patients with migraine. In a study consisting of 136 patients with migraine, compared with patients with low-frequency EM (1–8 headache days a month), patients with high-frequency EM (9–14 headache days a month) and CM (>14 headache days a month) had similar severe degrees of headache-related disability and CS-related symptoms.44 A comparison of migraine patients with 15 or more headaches per month and those with 8 to 14 or more headache days per month showed no differences in parameters such as depression, anxiety, and pain scores between the two groups.45 Becerra et al46 investigated differences in brain metabolite in the anterior cingulate cortex during the interictal phase in EM patients using magnetic resonance spectroscopy, and concluded that the brain in EM patients is hyperexcitable during the interictal state based on the findings of alterations of metabolites, such as aspartate /Cre, N-acetyl aspartate /Cre and glutamine /Cre.
The hypothalamus is a possible origin of migraine attacks as the trigeminovascular system, innervating the dura mater and of the major brain blood vessels, is activated during the headache phase.34,47 Some studies have suggested that patients with migraine exhibit subtle differences in brain structures related to pain processing or in the trigeminovascular system during the interictal phase.41 Calcitonin gene‐related peptide (CGRP), abundant in trigeminal ganglion neurons, has an important role in generating migraine headaches. This peptide is secreted in the trigeminal ganglion and may perpetuate peripheral sensitization by interacting with adjacent neurons and satellite glial cells to promote CS of second-order neurons.37 Photophobia, phonophobia and osmophobia are common sensory hypersensitivity symptoms in migraine. More severe symptoms of photophobia, phonophobia, osmophobia and nausea are associated with greater intensity of migraine headaches.48 In fact, patients with migraine exhibit atypical brain activation in response to painful, olfactory, and visual stimuli and atypical functional connectivity in the sensory-discriminative processing of pain, affective emotional processing, cognitive processing, and pain modulation.49 In migraine patients, activation of the limbic and rostral pons has been reported following exposure to odors,50 and activation of the visual cortex has been reported following visual stimulation.51
Clinical Studies on Migraine and Central Sensitization
Table 2 shows clinical studies on CS in patients with migraine. In a case–control study, the rate of CS in 186 patients with migraine was higher than that of 186 age- and sex-matched healthy controls (21.0% vs 8.6%). The determinants of CS in patients with migraine were the presence of RLS and interference of headache pain with daily activities, suggesting a potential role of comorbid migraine and RLS in CS.52 A significant association between RLS and migraine has been confirmed by many population-based and clinical studies,53 and CS may also be involved in this association. For example, in a cross-sectional study including 164 patients with migraine, CS was observed in 53 patients (32.3%).54 CS is associated with cranial parasympathetic symptoms such as lacrimation, aural fullness, nasal blockage, and rhinorrhea, suggesting that both trigeminovascular systems and the cranial parasympathetic system contribute to persistent CS in patients with migraine. MCS is reported to overlap with fibromyalgia, a disease known to be associated with CS.55 Similarly, there is a report suggesting a link between MCS and migraine. A cross-sectional study that included 95 patients with migraine found that 20% had MCS. Migraine patients with MCS had higher rates of photophobia, osmophobia, visual aura, sensory aura, and CS as well as higher migraine-related disability and Kessler Psychological Distress scores than those without MCS.56 This study showed a possible association of MCS with CS and hypersensitivity-related symptoms, such as photophobia and osmophobia, in migraine patients.
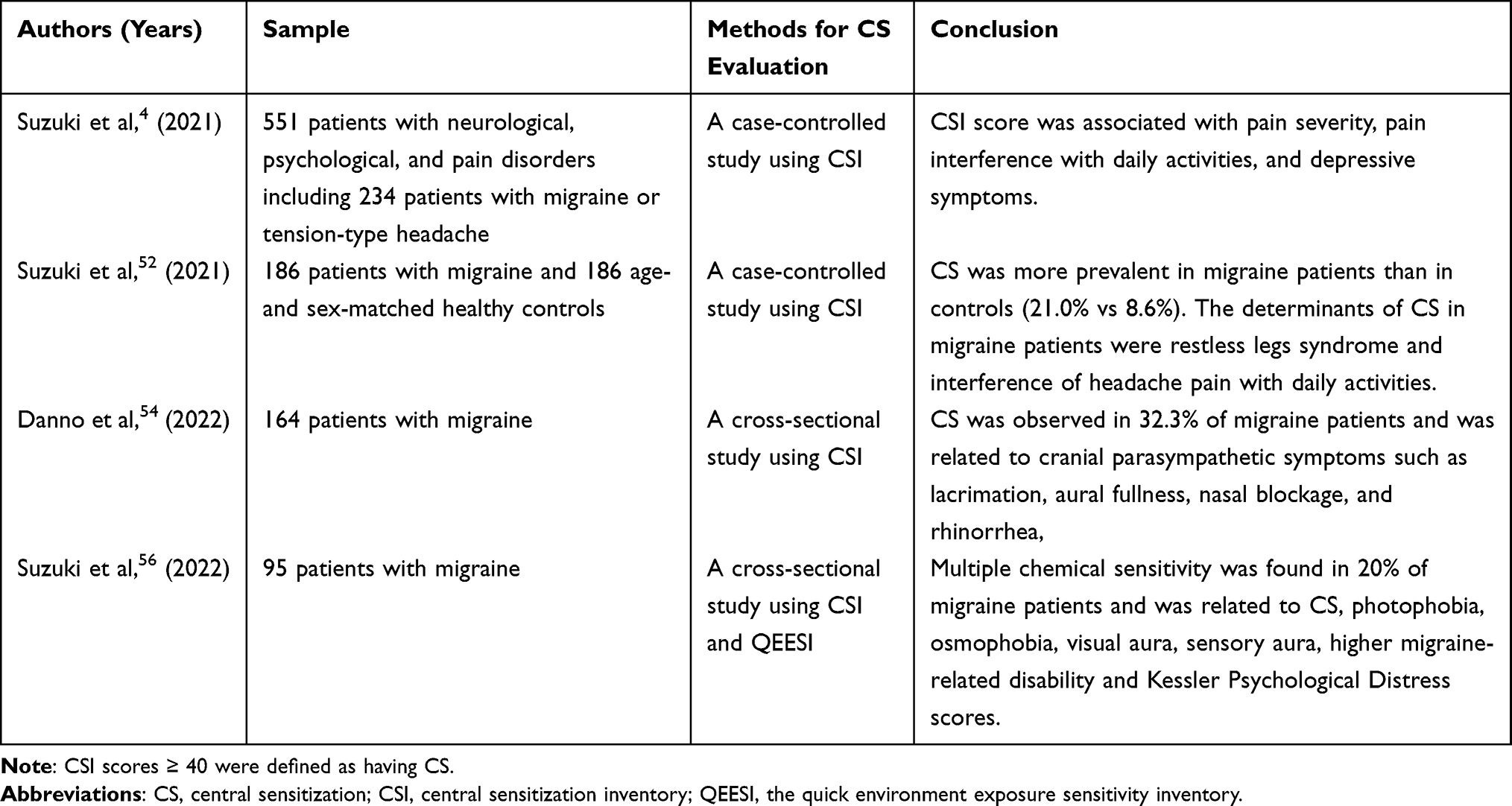 |
Table 2 Clinical Studies on Central Sensitization in Patients with Migraine |
In a cross-sectional study, photophobia, phonophobia and osmophobia were observed in 75.4%, 76.5% and 55.1% of patients with migraine, respectively; these hypersensitivities exhibited substantial overlap, as the proportions of patients with 2 and 3 coexisting sensory hypersensitivities were 33.2% and 41.7%.57 In the same study, the migraine Disability Assessment score was found to be higher in patients with 3 sensory hypersensitivities than in those with 0–2 sensory hypersensitivities. These results, which illustrate the burden of multiple hypersensitivity symptoms, may support the contribution of CS to migraine. In patients with chronic but not episodic migraine, a clear relationship between photophobia and CA was noted, suggesting that light stimulation may contribute to CS and subsequent chronicity.58
Cutaneous Allodynia and Central Sensitization
CA is a condition defined as perceptions of pain elicited by the application of nonpainful stimuli to normal skin; it has been observed in 60% of patients with migraine59 and is even more prevalent in patients with chronic migraine (up to 90%).60 The CS of trigeminovascular neurons has been implicated in the development of CA.41 CA may be evoked by thermal or dynamic/static mechanical stimulation and may be localized to the head (cephalic) or generalized (extracephalic). In particular, CA in the head and face during a migraine attack is thought to be the result of sensitization at the level of the trigeminospinal tract nucleus, which is connected to the periaqueductal gray.61 In a study consisting of a random sample of 24,000 headache sufferers, CA was more common and more severe in patients with transformed migraine and migraine than in other primary headaches.12 In patients with migraine, the presence of CA was associated with female sex, depression, disability, an increase in headache days and increased body mass index. The authors suggest that recurrent activation of trigeminovascular neurons and modulatory pain pathways involving the periaqueductal gray plays an important role in the progression of migraine. Other risk factors for CA include acute medication overuse and early age of migraine onset.59 Longitudinal data over 2 years showed that CA is an independent risk factor for migraine chronification.62 A study of resting-state functional connectivity showed that compared to migraine patients without ictal CA, migraine patients with ictal CA showed stronger functional connectivity of the periaqueductal gray and nucleus cuneiformis to other brainstem, thalamic, insular and cerebellar regions that participate in discriminative pain processing as well as higher order pain-associated regions, such as the frontal and temporal cortices.63 Rosso et al64 reported that abnormalities in the functional connectivity of the default mode network and central executive network as well as microstructural changes predicted CA incidence. In an fMRI study, increased activation of the contralateral pons, insula and thalamus in the ictal versus interictal state were observed in the generalized allodynia group but not in the no allodynia group.62
The complication rate of both CA and osmophobia is higher in patients with chronic migraine than in those with episodic migraine.65 Additionally, sound aversion thresholds were lower in migraine patients with allodynia than in those without allodynia, suggesting a link between phonophobia and CA.66 These observations indicate that CS evoked by recurrent headaches may cause hypersensitivity to olfactory, visual, and auditory stimuli in parallel with CA.
Implications for Treating Central Sensitization in Migraine
CS may be involved in the pathogenesis of migraine, including migraine chronicity and CA; thus, CS intervention may be important for treating migraine. In a retrospective study that included 1100 patients with migraine aged 18–75 and investigated the effect of preventive drugs, low headache frequency and absent or mild CA predicted better outcomes.67 Migraine patients who never developed allodynia were more likely to be made pain-free by triptan therapy at any time after the onset of pain.68 However, the role of CA in the triptan response is not conclusive.59 Interestingly, the presence of CA predicted responsiveness to erenumab, a calcitonin gene-related peptide (CGRP) receptor monoclonal antibody, along with male sex and baseline migraine frequency.69 In contrast, a subanalysis of a double-blind, randomized, placebo-controlled study, showed that the efficacy of erenumab in reducing monthly migraine days and acute migraine-specific medication days in chronic migraine patients was not affected by the presence of moderate to severe CA.70 In a rodent model of migraine, noninvasive stimulation of the vagus nerve inhibited mechanical nociception and downregulated expression of proteins associated with peripheral sensitization and CS of trigeminal neurons.71 Moreover, in patients with chronic migraine, severe CA is associated with a decreased response to treatment with occipital transcutaneous electrical stimulation.72 A preliminary study showed that an intravenous infusion of ketorolac, a central-acting COX1/COX2 inhibitor, effectively reversed CS induced by application of inflammatory soup to the dura of rats; intravenous administration of the same drug to migraine patients with CA who missed the critical period for triptan therapy provided a rescue therapy, possibly by suppressing CS.73
Because the release of CGRP may be involved in the enhancement of CS,37 it would be interesting to determine whether CGRP antagonists can alleviate CS. Melo-Carrillo et al74 demonstrated sensitization of central trigeminovascular neurons by CSD in high-threshold neurons of rats; this sensitization was prevented by administering the CGRP-monoclonal antibody fremanezumab. Clinically, fremanezumab not only significantly reduced the number of headache days in patients with episodic and chronic migraine but also significantly reduced the number of days with photophobia/phonophobia.75 This result would be even more interesting if there is a clear pathophysiologic relationship between photophobia/phonophobia and CS.
Botulinum toxin type A inhibits the release of glutamate and CGRP from primary nociceptive fibers, and one possible mechanism for its therapeutic effect on migraine is inhibition of peripheral and central trigeminal sensitization.76 Another topic of interest is the appropriate treatment of migraine comorbidities. For example, RLS is a CS-related condition, and in one study, the presence of RLS was a determinants of CS in migraine.52 The presence of RLS also predicted headache-related disability in migraine patients 7 years later.77 Although not yet proven, the management of sleep disturbances in migraine, especially RLS, may improve CS in migraine.
Conclusion
We described the involvement of CS in migraine, including various pathophysiological aspects and evidence from clinical studies. CS is associated with the chronification of migraine and CA; moreover, we believe clinical assessment and appropriately management of CS could further improve the quality of life of migraine patients. The limitations of this narrative review include selection bias, a subjective search and literature acquisition. Further placebo-controlled studies in which researchers evaluate changes in CS using brain imaging are needed to clarify the role of CS in the pathogenesis of migraine.
Acknowledgments
The authors thank Prof. Yasuo Haruyama, Integrated Research Faculty for Advanced Medical Science, Dokkyo Medical University School of Medicine, and Prof. Gen Kobashi, Department of Public Health, Dokkyo Medical University School of Medicine, for their comments on this study. The authors also thank Ms. Sanae Tani and Ms. Kaori Soma, Department of Neurology, Dokkyo Medical University, for their help with this study.
Funding
This work was supported by the Ministry of Health, Labour and Welfare’s Research Project on Rare and Intractable Diseases (grant number 20FC1056).
Disclosure
The authors declare that there are no conflicts of interest.
References
1. Arendt-Nielsen L, Morlion B, Perrot S, et al. Assessment and manifestation of central sensitisation across different chronic pain conditions. Eur J Pain. 2018;22(2):216–241. doi:10.1002/ejp.1140
2. Woolf CJ. Evidence for a central component of post-injury pain hypersensitivity. Nature. 1983;306(5944):686–688. doi:10.1038/306686a0
3. Woolf CJ. Pain amplification- A perspective on the how, why, when, and where of central sensitization. J Appl Biobehav Res. 2018;23(2):e12124. doi:10.1111/jabr.12124
4. Suzuki K, Haruyama Y, Kobashi G, et al. Central sensitization in neurological, psychiatric, and pain disorders: a multicenter case-controlled study. Pain Res Manag. 2021;2021:6656917. doi:10.1155/2021/6656917
5. Ashina M, Terwindt GM, Al-Karagholi MA, et al. Migraine: disease characterisation, biomarkers, and precision medicine. Lancet. 2021;397(10283):1496–1504.
6. Woolf CJ. Central sensitization: implications for the diagnosis and treatment of pain. Pain. 2011;152(3 Suppl):S2–S15. doi:10.1016/j.pain.2010.09.030
7. Nijs J, Torres-Cueco R, van Wilgen CP, et al. Applying modern pain neuroscience in clinical practice: criteria for the classification of central sensitization pain. Pain Physician. 2014;17(5):447–457. doi:10.36076/ppj.2014/17/447
8. Scerbo T, Colasurdo J, Dunn S, Unger J, Nijs J, Cook C. Measurement properties of the central sensitization inventory: a systematic review. Pain Pract. 2018;18(4):544–554. doi:10.1111/papr.12636
9. Mayer TG, Neblett R, Cohen H, et al. The development and psychometric validation of the central sensitization inventory. Pain Pract. 2012;12(4):276–285. doi:10.1111/j.1533-2500.2011.00493.x
10. Starkweather AR, Heineman A, Storey S, et al. Methods to measure peripheral and central sensitization using quantitative sensory testing: a focus on individuals with low back pain. Appl Nurs Res. 2016;29:237–241. doi:10.1016/j.apnr.2015.03.013
11. Jakubowski M, Silberstein S, Ashkenazi A, Burstein R. Can allodynic migraine patients be identified interictally using a questionnaire? Neurology. 2005;65(9):1419–1422. doi:10.1212/01.wnl.0000183358.53939.38
12. Bigal ME, Ashina S, Burstein R, et al. Prevalence and characteristics of allodynia in headache sufferers: a population study. Neurology. 2008;70(17):1525–1533. doi:10.1212/01.wnl.0000310645.31020.b1
13. Ruscheweyh R, Marziniak M, Stumpenhorst F, Reinholz J, Knecht S. Pain sensitivity can be assessed by self-rating: development and validation of the pain sensitivity questionnaire. Pain. 2009;146(1–2):65–74. doi:10.1016/j.pain.2009.06.020
14. Ruscheweyh R, Verneuer B, Dany K, et al. Validation of the pain sensitivity questionnaire in chronic pain patients. Pain. 2012;153(6):1210–1218. doi:10.1016/j.pain.2012.02.025
15. Adams GR, Gandhi W, Harrison R, van Reekum CM, Gilron I, Salomons TV. Do “central sensitization” questionnaires reflect measures of nociceptive sensitization or psychological constructs? Protocol for a systematic review. Pain Rep. 2021;6(4):e962. doi:10.1097/PR9.0000000000000962
16. Edwards RR, Quartana PJ, Allen RP, Greenbaum S, Earley CJ, Smith MT. Alterations in pain responses in treated and untreated patients with restless legs syndrome: associations with sleep disruption. Sleep Med. 2011;12(6):603–609. doi:10.1016/j.sleep.2010.09.018
17. Stiasny-Kolster K, Magerl W, Oertel WH, Moller JC, Treede RD. Static mechanical hyperalgesia without dynamic tactile allodynia in patients with restless legs syndrome. Brain. 2004;127(Pt 4):773–782. doi:10.1093/brain/awh079
18. Meeus M, Nijs J. Central sensitization: a biopsychosocial explanation for chronic widespread pain in patients with fibromyalgia and chronic fatigue syndrome. Clin Rheumatol. 2007;26(4):465–473. doi:10.1007/s10067-006-0433-9
19. Bradley LA, McKendree-Smith NL, Alberts KR, Alarcon GS, Mountz JM, Deutsch G. Use of neuroimaging to understand abnormal pain sensitivity in fibromyalgia. Curr Rheumatol Rep. 2000;2(2):141–148. doi:10.1007/s11926-000-0054-2
20. Vecchiet L, Montanari G, Pizzigallo E, et al. Sensory characterization of somatic parietal tissues in humans with chronic fatigue syndrome. Neurosci Lett. 1996;208(2):117–120. doi:10.1016/0304-3940(96)12559-3
21. Fernandez-de-las-Penas C, Galan-del-Rio F, Fernandez-Carnero J, Pesquera J, Arendt-Nielsen L, Svensson P. Bilateral widespread mechanical pain sensitivity in women with myofascial temporomandibular disorder: evidence of impairment in central nociceptive processing. J Pain. 2009;10(11):1170–1178. doi:10.1016/j.jpain.2009.04.017
22. Jensen R. Mechanisms of spontaneous tension-type headaches: an analysis of tenderness, pain thresholds and EMG. Pain. 1996;64(2):251–256. doi:10.1016/0304-3959(95)00114-X
23. Munakata J, Naliboff B, Harraf F, et al. Repetitive sigmoid stimulation induces rectal hyperalgesia in patients with irritable bowel syndrome. Gastroenterology. 1997;112(1):55–63. doi:10.1016/s0016-5085(97)70219-1
24. Andersson L, Claeson AS, Dantoft TM, Skovbjerg S, Lind N, Nordin S. Chemosensory perception, symptoms and autonomic responses during chemical exposure in multiple chemical sensitivity. Int Arch Occup Environ Health. 2016;89(1):79–88. doi:10.1007/s00420-015-1053-y
25. Alessandrini M, Micarelli A, Chiaravalloti A, et al. Involvement of subcortical brain structures during olfactory stimulation in multiple chemical sensitivity. Brain Topogr. 2016;29(2):243–252. doi:10.1007/s10548-015-0453-3
26. Lee MC, Zambreanu L, Menon DK, Tracey I. Identifying brain activity specifically related to the maintenance and perceptual consequence of central sensitization in humans. J Neurosci. 2008;28(45):11642–11649. doi:10.1523/JNEUROSCI.2638-08.2008
27. Baron R, Baron Y, Disbrow E, Roberts TP. Activation of the somatosensory cortex during Abeta-fiber mediated hyperalgesia. A MSI study. Brain Res. 2000;871(1):75–82. doi:10.1016/s0006-8993(00)02444-6
28. Cagnie B, Coppieters I, Denecker S, Six J, Danneels L, Meeus M. Central sensitization in fibromyalgia? A systematic review on structural and functional brain MRI. Semin Arthritis Rheum. 2014;44(1):68–75. doi:10.1016/j.semarthrit.2014.01.001
29. Barnden LR, Crouch B, Kwiatek R, et al. A brain MRI study of chronic fatigue syndrome: evidence of brainstem dysfunction and altered homeostasis. NMR Biomed. 2011;24(10):1302–1312. doi:10.1002/nbm.1692
30. Shan ZY, Kwiatek R, Burnet R, et al. Progressive brain changes in patients with chronic fatigue syndrome: a longitudinal MRI study. J Magn Reson Imaging. 2016;44(5):1301–1311. doi:10.1002/jmri.25283
31. Kobayashi Y, Kurata J, Sekiguchi M, et al. Augmented cerebral activation by lumbar mechanical stimulus in chronic low back pain patients: an FMRI study. Spine. 2009;34(22):2431–2436. doi:10.1097/BRS.0b013e3181b1fb76
32. Ashina M, Katsarava Z, Do TP, et al. Migraine: epidemiology and systems of care. Lancet. 2021;397(10283):1485–1495. doi:10.1016/S0140-6736(20)32160-7
33. Headache Classification Committee of the International Headache Society (IHS). The international classification of headache disorders, 3rd edition. Cephalalgia. 2018;38(1):1–211. doi:10.1177/0333102417738202
34. Dodick DW, Phase-by-Phase A. Review of Migraine Pathophysiology. Headache. 2018;58(Suppl 1):4–16. doi:10.1111/head.13300
35. Schulte LH, May A. The migraine generator revisited: continuous scanning of the migraine cycle over 30 days and three spontaneous attacks. Brain. 2016;139(Pt7):1987–1993. doi:10.1093/brain/aww097
36. Hadjikhani N, Sanchez Del Rio M, Wu O, et al. Mechanisms of migraine aura revealed by functional MRI in human visual cortex. Proc Natl Acad Sci USA. 2001;98(8):4687–4692. doi:10.1073/pnas.071582498
37. Iyengar S, Johnson KW, Ossipov MH, Aurora SK. CGRP and the trigeminal system in migraine. Headache. 2019;59(5):659–681. doi:10.1111/head.13529
38. Zhang X, Levy D, Kainz V, Noseda R, Jakubowski M, Burstein R. Activation of central trigeminovascular neurons by cortical spreading depression. Ann Neurol. 2011;69(5):855–865. doi:10.1002/ana.22329
39. Dodick D, Silberstein S. Central sensitization theory of migraine: clinical implications. Headache. 2006;46(Suppl 4):S182–91. doi:10.1111/j.1526-4610.2006.00602.x
40. Zhang L, Lu C, Kang L, et al. Temporal characteristics of astrocytic activation in the TNC in a mice model of pain induced by recurrent dural infusion of inflammatory soup. J Headache Pain. 2022;23(1):8. doi:10.1186/s10194-021-01382-9
41. Goadsby PJ, Holland PR, Martins-Oliveira M, Hoffmann J, Schankin C, Akerman S. Pathophysiology of migraine: a disorder of sensory processing. Physiol Rev. 2017;97(2):553–622. doi:10.1152/physrev.00034.2015
42. Park CG, Chu MK. Interictal plasma glutamate levels are elevated in individuals with episodic and chronic migraine. Sci Rep. 2022;12(1):6921. doi:10.1038/s41598-022-10883-9
43. de la Coba P, Bruehl S, Del paso GAR. Slowly repeated evoked pain (SREP) as a central sensitization marker in episodic migraine patients. Sci Rep. 2021;11(1):4582. doi:10.1038/s41598-021-84157-1
44. Di Antonio S, Castaldo M, Ponzano M, et al. Disability, burden, and symptoms related to sensitization in migraine patients associate with headache frequency. Scand J Pain. 2021;21(4):766–777. doi:10.1515/sjpain-2021-0050
45. Ishii R, Schwedt TJ, Dumkrieger G, et al. Chronic versus episodic migraine: the 15-day threshold does not adequately reflect substantial differences in disability across the full spectrum of headache frequency. Headache. 2021;61(7):992–1003. doi:10.1111/head.14154
46. Becerra L, Veggeberg R, Prescot A, et al. A ‘complex’ of brain metabolites distinguish altered chemistry in the cingulate cortex of episodic migraine patients. Neuroimage Clin. 2016;11:588–594. doi:10.1016/j.nicl.2016.03.020
47. Mungoven TJ, Henderson LA, Meylakh N. Chronic migraine pathophysiology and treatment: a review of current perspectives. Front Pain Res. 2021;2:705276. doi:10.3389/fpain.2021.705276
48. Kelman L, Tanis D. The relationship between migraine pain and other associated symptoms. Cephalalgia. 2006;26(5):548–553. doi:10.1111/j.1468-2982.2006.01075.x
49. Schwedt TJ, Chiang CC, Chong CD, Dodick DW. Functional MRI of migraine. Lancet Neurol. 2015;14(1):81–91. doi:10.1016/S1474-4422(14)70193-0
50. Stankewitz A, May A. Increased limbic and brainstem activity during migraine attacks following olfactory stimulation. Neurology. 2011;77(5):476–482. doi:10.1212/WNL.0b013e318227e4a8
51. Vincent M, Pedra E, Mourao-Miranda J, Bramati IE, Henrique AR, Moll J. Enhanced interictal responsiveness of the migraineous visual cortex to incongruent bar stimulation: a functional MRI visual activation study. Cephalalgia. 2003;23(9):860–868. doi:10.1046/j.1468-2982.2003.00609.x
52. Suzuki K, Suzuki S, Haruyama Y, et al. Central sensitization in migraine is related to restless legs syndrome. J Neurol. 2021;268(4):1395–1401. doi:10.1007/s00415-020-10295-7
53. Schurks M, Winter A, Berger K, Kurth T. Migraine and restless legs syndrome: a systematic review. Cephalalgia. 2014;34(10):777–794. doi:10.1177/0333102414537725
54. Danno D, Wolf J, Ishizaki K, Kikui S, Hirata K, Takeshima T. Cranial autonomic symptoms in migraine are related to central sensitization: a prospective study of 164 migraine patients at a tertiary headache center. BMC Neurol. 2022;22(1):89. doi:10.1186/s12883-022-02610-8
55. Aaron LA, Buchwald D. Chronic diffuse musculoskeletal pain, fibromyalgia and co-morbid unexplained clinical conditions. Best Pract Res Clin Rheumatol. 2003;17(4):563–574. doi:10.1016/s1521-6942(03)00033-0
56. Suzuki K, Okamura M, Haruyama Y, et al. Exploring the contributing factors to multiple chemical sensitivity in patients with migraine. J Occup Health. 2022;64(1):e12328. doi:10.1002/1348-9585.12328
57. Suzuki K, Suzuki S, Shiina T, et al. Investigating the relationships between the burden of multiple sensory hypersensitivity symptoms and headache-related disability in patients with migraine. J Headache Pain. 2021;22(1):77. doi:10.1186/s10194-021-01294-8
58. Lovati C, Mariotti C, Giani L, et al. Central sensitization in photophobic and non-photophobic migraineurs: possible role of retino nuclear way in the central sensitization process. Neurol Sci. 2013;34(Suppl 1):S133–5. doi:10.1007/s10072-013-1369-x
59. Minguez-Olaondo A, Quintas S, Morollon Sanchez-Mateos N, et al. Cutaneous allodynia in migraine: a narrative review. Front Neurol. 2021;12:831035. doi:10.3389/fneur.2021.831035
60. Mathew PG, Cutrer FM, Garza I. A touchy subject: an assessment of cutaneous allodynia in a chronic migraine population. J Pain Res. 2016;9:101–104. doi:10.2147/JPR.S103238
61. Burstein R, Cutrer MF, Yarnitsky D. The development of cutaneous allodynia during a migraine attack clinical evidence for the sequential recruitment of spinal and supraspinal nociceptive neurons in migraine. Brain. 2000;123(Pt 8):1703–1709. doi:10.1093/brain/123.8.1703
62. Maleki N, Szabo E, Becerra L, et al. Ictal and interictal brain activation in episodic migraine: neural basis for extent of allodynia. PLoS One. 2021;16(1):e0244320. doi:10.1371/journal.pone.0244320
63. Schwedt TJ, Larson-Prior L, Coalson RS, et al. Allodynia and descending pain modulation in migraine: a resting state functional connectivity analysis. Pain Med. 2014;15(1):154–165. doi:10.1111/pme.12267
64. Russo A, Silvestro M, Trojsi F, et al. Cognitive networks disarrangement in patients with migraine predicts cutaneous allodynia. Headache. 2020;60(7):1228–1243. doi:10.1111/head.13860
65. Lovati C, Giani L, Castoldi D, et al. Osmophobia in allodynic migraineurs: cause or consequence of central sensitization? Neurol Sci. 2015;36(Suppl 1):145–147. doi:10.1007/s10072-015-2141-1
66. Ashkenazi A, Yang I, Mushtaq A, Oshinsky ML. Is phonophobia associated with cutaneous allodynia in migraine? J Neurol Neurosurg Psychiatry. 2010;81(11):1256–1260. doi:10.1136/jnnp.2009.198481
67. Delussi M, Vecchio E, Libro G, Quitadamo S, de Tommaso M. Failure of preventive treatments in migraine: an observational retrospective study in a tertiary headache center. BMC Neurol. 2020;20(1):256. doi:10.1186/s12883-020-01839-5
68. Burstein R, Collins B, Jakubowski M. Defeating migraine pain with triptans: a race against the development of cutaneous allodynia. Ann Neurol. 2004;55(1):19–26. doi:10.1002/ana.10786
69. Barbanti P, Aurilia C, Cevoli S, et al. Long-term (48 weeks) effectiveness, safety, and tolerability of erenumab in the prevention of high-frequency episodic and chronic migraine in a real world: results of the EARLY 2 study. Headache. 2021;61(9):1351–1363. doi:10.1111/head.14194
70. Lipton RB, Burstein R, Buse DC, et al. Efficacy of erenumab in chronic migraine patients with and without ictal allodynia. Cephalalgia. 2021;41(11–12):1152–1160. doi:10.1177/03331024211010305
71. Hawkins JL, Cornelison LE, Blankenship BA, Durham PL. Vagus nerve stimulation inhibits trigeminal nociception in a rodent model of episodic migraine. Pain Rep. 2017;2(6):e628. doi:10.1097/PR9.0000000000000628
72. Bono F, Salvino D, Mazza MR, et al. The influence of ictal cutaneous allodynia on the response to occipital transcutaneous electrical stimulation in chronic migraine and chronic tension-type headache: a randomized, sham-controlled study. Cephalalgia. 2015;35(5):389–398. doi:10.1177/0333102414544909
73. Jakubowski M, Levy D, Goor-Aryeh I, Collins B, Bajwa Z, Burstein R. Terminating migraine with allodynia and ongoing central sensitization using parenteral administration of COX1/COX2 inhibitors. Headache. 2005;45(7):850–861. doi:10.1111/j.1526-4610.2005.05153.x
74. Melo-Carrillo A, Noseda R, Nir RR, et al. Selective inhibition of trigeminovascular neurons by fremanezumab: a humanized monoclonal anti-CGRP antibody. J Neurosci. 2017;37(30):7149–7163. doi:10.1523/JNEUROSCI.0576-17.2017
75. Ashina M, Cohen JM, Galic M, et al. Efficacy and safety of fremanezumab in patients with episodic and chronic migraine with documented inadequate response to 2 to 4 classes of migraine preventive medications over 6 months of treatment in the phase 3b FOCUS study. J Headache Pain. 2021;22(1):68. doi:10.1186/s10194-021-01279-7
76. Durham PL, Cady R. Insights into the mechanism of onabotulinumtoxinA in chronic migraine. Headache. 2011;51(10):1573–1577. doi:10.1111/j.1526-4610.2011.02022.x
77. Suzuki K, Suzuki S, Haruyama Y, Kobashi G, Shiina T, Hirata K. Restless legs syndrome is associated with headache-related disabilities in patients with migraine: a prospective 7-year follow-up study. Eur J Neurol. 2019;26(2):238–245. doi:10.1111/ene.13796
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.