Back to Journals » Breast Cancer: Targets and Therapy » Volume 14
Central Nervous System Metastases from Triple-Negative Breast Cancer: Current Treatments and Future Prospective
Authors Kadamkulam Syriac A, Nandu NS, Leone JP ![]()
Received 27 September 2021
Accepted for publication 24 December 2021
Published 10 January 2022 Volume 2022:14 Pages 1—13
DOI https://doi.org/10.2147/BCTT.S274514
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pranela Rameshwar
Arun Kadamkulam Syriac,1 Nitish Singh Nandu,2 Jose Pablo Leone1
1Department of Medical Oncology, Dana-Farber Cancer Institute, Boston, MA, 02215, USA; 2Department of Hospice and Palliative Medicine, Montefiore Medical Center/ Albert Einstein College of Medicine, Bronx, NY, USA
Correspondence: Jose Pablo Leone
Department of Medical Oncology, Dana-Farber Cancer Institute, Boston, MA, 02215, USA
Email [email protected]
Abstract: It is estimated that approximately one-third of patients with triple-negative breast cancer (TNBC) will develop brain metastases. The prognosis for patients with breast cancer brain metastasis has improved in the recent past, especially for hormone receptor and human epidermal growth factor receptor 2 (HER) positive subtypes. However, the overall survival rate for patients with triple-negative subtype remains poor. The development of newer treatment options, including antibody-drug conjugates such as Sacituzumab govitecan, is particularly encouraging. This article reviews the clinical outcomes, challenges, and current approach to the treatment of brain metastasis in TNBC. We have also briefly discussed newer treatment options and ongoing clinical trials. The development of brain metastasis significantly decreases the quality of life of patients with TNBC, and newer treatment strategies and therapeutics are the need of the hour for this disease subgroup.
Keywords: triple-negative breast cancer, metastatic disease, brain metastasis, prognosis clinical outcomes, immunotherapy, stereotactic radiosurgery, whole-brain radiation therapy, antibody–drug conjugate, oligometastatic brain metastasis, clinical outcomes, prediction, prognosis, personalization, multi-omics, machine learning, individualized treatment algorithms, patient benefits
Introduction
Incidence of Female Breast Cancer
Breast cancer is the most common cancer in the United States (US), with estimated 284,200 new cases expected in 2021, accounting for 14.8% of newly diagnosed cancer cases in the US There will be 43,600 deaths attributable to breast cancer, accounting for 7.2% of all cancer-related deaths.1 Triple-Negative Breast Cancer (TNBC) accounts for about 15% to 20% of breast cancers diagnosed worldwide. They are most commonly seen in younger women and older African American women.2–5 When diagnosed, they are more likely to have lymph node involvement and are aggressive tumors with a higher relapse rate and a poor prognosis. A study by Lin et al reported the greatest risk of death in the first 2 years after initial diagnosis.6 The overall 5-year survival rate of TNBC is around 74.5–77%.7–10
CNS (Central Nervous System) Metastasis
Comparison of the Subgroups
Metastatic dissemination differs among the various subtypes of breast cancer, a higher incidence of brain metastasis is seen in TNBC and Human Epidermal Growth Factor Receptor 2 (HER 2)-positive breast cancer, whereas metastasis to the lungs and bones is more common in Luminal subtypes.11,12
The incidence of brain metastasis (BM) in TNBC is approximately 25–46%, a similar incidence was found in Metastatic Her2 positive breast cancer (11–48%), a lower incidence of BM was noted in Luminal A (8–15%) and B (11%).12–16 Thus, the risk of developing brain metastasis is 2–5 times higher in Her2 positive and TNBC cancers.17,18 With the advancement in breast cancer treatments in metastatic space, the number of patients developing brain metastasis appears to be increasing. A recent meta-analysis showed that approximately one-third of those with TNBC will eventually develop brain metastasis.19 A systematic review by Koniali et al identified younger age, hormonal and Her-2 receptor status, higher tumor stage and size, higher histological grade, high Ki67 labeling index as independent risk factors for Breast Cancer Brain Metastasis (BCBM).20 Symptoms are variable and can be nausea, headaches, personality changes, seizures, paralysis, and cognitive impairment.21
Prognosis of TNBC with BM
It is important to be able to predict the patient’s prognosis to customize treatment options as several factors can impact the response. The Karnofsky Performance Status (KPS) scale has been identified as a reliable prognostic tool with longer survival noted in patients with a KPS ≥ 70.22–24 One such tool is the Diagnosis-Specific Graded Prognostic Assessment (DS-GPA) tool that has been used to predict median survival in patients with brain metastases from various primary sites such as lung, breast, melanoma, gastrointestinal, and renal cell carcinoma.25 The prognostic criteria can be different for each tumor subtype.
Modified breast graded prognostic assessment is used as a prognostic index tailored for patients with BM from breast cancer. It comprises KPS scale, breast cancer subtype, age of the patient (≤50 years or >50 years), and the number of brain metastases (1 to 3 or >3). By integrating four independent patient variables, it has been shown to predict the prognosis of BM related to breast cancer. It, therefore, allows for identifying patients that can withstand treatment.26 Brain metastasis significantly impacts the quality of life and can have a mortality rate as high as 80% within 1 year.27,28 Treatment options for small solitary BM are curative with surgical resection and/or radiotherapy. However, treatment for large or multiple BM is palliative.13 The prognosis of patients with BM from breast cancer has improved over the past 20 years.29 However, the current overall survival rate in TNBC remains low at 4.4–4.9 months, whereas the overall survival in patients with Luminal and Her2 positive breast cancer, 7.1–18.9 months and 13.1–16.5 months, respectively.13,30–32
CNS Screening for the Detection of Brain Metastasis (BM)
Current NCCN (National Comprehensive Cancer Network) guidelines do not recommend screening for brain metastasis due to a lack of clinical benefit. Dana-Farber Cancer Institute trial (NCT04030507) will look into this question and has divided that patient into four cohorts, out of which one cohort is TNBC, who will be undergoing screening by Magnetic Resonance Imaging (MRI).33 Another trial includes TNBC and HER2 positive patients in which MRI screening will be done in three instances - initial diagnosis and change of treatment after the first line and second line.34 Finally, we present a SYMPToM trial with 50 women with TNBC or HER-2 positive breast cancer randomized to either clinical surveillance or MRI screening every 4 months.35 All of these trials will help us in answering the question of routine CNS screening for advanced TNBC patients and potential benefits for initiating early local treatment and reduction of WBRT.36,37
Treatment of Triple-Negative CNS Metastasis
The treatment of brain metastases can be categorized as loco-regional treatments and systemic therapies.
Loco-Regional Treatment
When systemic treatment options are available to the patient, loco-regional treatments provide survival benefit and improvement in quality of life.38,39 Loco-regional treatments can be broadly categorized into surgical and radiation therapies.
Surgical Resection
Surgical treatment can be a particularly beneficial treatment option if the systemic disease is well controlled and the brain lesions are symptomatic and ≤3. Surgical resection can relieve intracranial hypertension, improve symptoms, and provide tissue to perform histological and molecular analysis. However, surgical options may be limited by the location of the lesion.40 Surgery alone may be inadequate for local control and is usually followed by radiotherapy.32
A randomized control trial by Patchell et al assigned 48 patients with single brain lesion from different primaries to surgical removal followed by whole-brain radiation therapy (WBRT) or needle biopsy and WBRT. The study reported an overall length of survival to be 40 weeks in the surgical plus WBRT group compared to 15 weeks in the biopsy plus radiation group. The recurrence rate was also lower in the surgical group as compared to the radiation group (20% vs 52%). The study also reported a more extended period of functionality in the surgical plus WBRT group (38 weeks) as compared to the biopsy plus radiation group (8 weeks).41
A similar study by Vecht et al assigned 63 patients with single brain metastasis from various systemic cancers to surgery plus WBRT and WBRT alone and found an overall survival of 12 months vs 7 months in the surgery plus WBRT and WBRT alone groups, respectively.42 Other non-randomized studies have confirmed the benefit of adding surgery to radiation in a patient with solitary metastasis in patients with stable extracranial disease.43–45
Stereotactic Radiosurgery (SRS) and Whole-Brain Radiation Therapy (WBRT)
Stereotactic radiosurgery (SRS) or whole-brain radiation therapy (WBRT) can be used in addition or as an alternative to surgery. SRS is a minimally invasive ablative treatment option and is preferred over surgery for patients with small asymptomatic lesions that do not require surgery or lesions that are not surgically accessible.46
A retrospective study looked at 122 patients who underwent SRS for management of BM in different subtypes of breast cancer. The median number of lesions at the start of the treatment was 3. 21% of the patient were TNBC, 31% were ER+HER2− 23% were ER+HER2+, and 18% were ER−HER2+, and the median overall survival was found to be 7, 16, 26, and 23 months, respectively. Patients with TNBC had the shortest time to retreatment and the poorest survival. This shows that the benefit of SRS may not provide adequate control of BM, showing the need for developing more effective treatments.49
Another recent retrospective study from Johns Hopkins looked at the question of WBRT benefits in TNBC with BM specifically. Out of 85 patients who met the inclusion criteria, 25% had TNBC. 95% of patients received SRS, and 48% received WBRT. A Cox proportional hazard model showed that WBRT has no survival benefit in patients with TNBC (HR (Hormone Receptor) 1.48; 95% CI (Configuration Item) 0.47–4.67; p = 0.50). Another important finding from the study was that the average number of new brain metastasis from the time of initial brain imaging to radiation was 0.76 in non-TNBC patients when compared with 2.6 in TNBC patients, showing the extremely aggressive nature of TNBC.50 These findings agree with earlier studies, which showed a lack of survival benefit.51 Furthermore, WBRT is associated with toxicities, including a negative effect on health-related quality of life47 and neurocognition (learning and memory).48
The NCCTG N0574 trial looked at the benefit of adding WBRT to SRS on cognition of patients with 1–3 brain metastases and found that there were higher rates of cognitive deterioration after WBRT even though there was better intracranial control.49 The rationale for using SRS alone without WBRT is further supported by the fact that studies have not shown survival benefit in this setting.
Another Phase 3 clinical trial, NCCTG N107C/CEC.3, compared post-operative SRS with WBRT in patients after surgical resection of single brain metastases of less than 5 cm from all non-CNS brain metastasis. The study reported longer cognitive deterioration-free survival in patients receiving SRS compared to WBRT (3.7 months vs 3 months) and found no statistically significant difference in the overall survival between the groups.50
Although advances in the field allow the use of SRS in up to 10 lesions in the brain,51,52 WBRT is still considered a standard in patients with more than 4 lesions. Thus, formulating strategies to avoid cognitive toxicity is a priority, especially in this population.53
Hippocampal avoidance seems to be an effective strategy in addressing the issue of cognitive toxicity in WBRT. Phase III Trial NRG Oncology CC001 randomized patients to HA-WBRT plus memantine or WBRT plus memantine and found that for HA-WBRT cohort had better outcomes in terms of cognitive function and patient-reported symptoms with no difference in intracranial progression-free survival (PFS) or OS.54 (HIPPORAD) – a Phase II prospective randomized multicenter trial is currently evaluating patients with at least four brain metastases of solid tumors (at least one, but not exceeding 10 metastases ≥5 mm) and compared the effect on neurocognition. Patients are randomized to two arms- HA (hippocampus avoidance)-WBRT+SIB (simultaneous integrated boost), and WBRT+SIB.55 A Phase 3 clinical trial is currently underway comparing SRS to HA-WBRT plus memantine in patients with 5 or more brain metastases (with the largest metastasis measuring < 2.5cm) in patients with a non-hematopoietic malignancy.56 The study is due to be completed by June 2023.
Thus, SRS is preferred over WBRT for patients after surgery or for other non-resected brain metastases if the tumor volume is low (typically less than 4). It provides superior local control and lesser cognitive decline.46,57 For large volume tumors, WBRT with hippocampal sparing offers a better prognosis.54
Systemic Therapy
The development of drug therapies has also been hindered by the immediate referral of radiation therapy upon diagnosis, and hence the disease is more refractory when attempting systemic therapy.38
Patients with well-controlled extracranial can develop brain metastasis, and the lack of response of brain metastases to systemic therapy may be due to genetic divergence between primary and metastatic lesions.58
Systemic therapy is used for extensive intracranial disease and is based on the choice of agents against the primary tumor.38 Based on retrospective analysis, it is noted that the survival of patients with BM has improved due to advances in systemic therapies and better control of extracranial and intracranial disease for most subtypes of breast cancer except for TNBC.59–63 The current systemic chemotherapy for TNBC with BM is limited to etoposide, cisplatin, and /or high dose methotrexate with an uncertain treatment efficacy.64–68
The Overall Risk Reduction (ORR) for cisplatin and etoposide combination in the brain is around 38%,69 whereas for temozolomide and cisplatin was around 40% in patients with solid tumors.72
Chemotherapy
Single-agent use of capecitabine in CNS metastases from BC (Breast Cancer) was looked at retrospectively from MSKCC (Memorial Sloan Kettering Cancer Center). Out of seven patients, four had brain metastases alone, with the rest having leptomeningeal disease with or without brain metastasis. Three patients showed complete response, and three showed stable disease.73 Most of the data for capecitabine is from case reports.69 Capecitabine in combination with temozolomide had a response rate of 18%.70
The Response rates were noted to be 52% for patients receiving Cytoxan (cyclophosphamide) (C), 5-fluorouracil (F) and prednisone (P), 43% for methotrexate (M) and vincristine (V) and prednisone combination therapy, and 54% for the CFP-MV combination therapy and 16% for patients receiving Cytoxan and Adriamycin (CA) therapy.71
Eribulin is a microtubule inhibitor, and its anti-replicating properties were studied in-vitro in the breast. A prospective phase II single-arm study looked at 12-week CNS PFS in patients with MBC (Metastatic Breast Cancer) and CNS metastasis. Out of the nine patients enrolled (1 TNBC), four patients achieved stable disease, and one patient had a partial response.74 There are also case reports showing the benefit of combining WBRT and Eribulin, and it is speculated that WBRT facilitates and enhances the passage of Eribulin across the blood–brain barrier by inhibiting the activity of P-glycoprotein, an efflux drug transporter protein found in the endothelial cells of the blood–brain barrier.75–77
Combination chemotherapy with cisplatin plus gemcitabine was evaluated in 18 patients with brain metastasis from all breast cancer subtypes by Erten et al. The regimen was given as a first-line agent in 15 patients, second-line in two patients, and third line in one patient. The study reported an overall response rate of 66.6% in BM from TNBC and a median PFS of 7.4 months (95% CI, 2.4–12.3 months) in patients with BM from TNBC and a median PFS of 9.2 months (5.2–13.2 months, 95% CI) in patients with BM from TNBC who received the regimen as first-line therapy.72
Poly-ADP-Ribose-Polymerase (PARP) Inhibitors
PARP inhibitors re-sensitize cancer cells to DNA (deoxyribonucleic acid) Damage and repair rely on BRCA-pathway-dependent homologous recombination mechanisms, and approximately 20% of the patients with TNBC have BRCA1/2 mutations.78–80 A Post hoc analysis of the OlympiAD study showed that 18/205 patients randomized to the Olaparib arm and 8/97 in the physician choice treatment arm had brain metastasis. Although the study was not powered to detect differences in treatment effect, the benefit for Olaparib appeared to be continued to all the subgroups, including CNS metastasis (ORR 64.7 vs 20%) when compared with the standard arm.81 In the EMBRACA trial for Talazoparib, although CNS metastases were eligible, they had to have completed definitive local treatment and have stable lesions on repeat brain imaging.82 Currently, both Olaparib and Talazoparib are approved by FDA (Food and Drug Administration) in germline BRCA-mutated, HER2-negative locally advanced or metastatic breast cancer.83,84 A Multicenter Phase II trial of irinotecan-iniparib evaluated patients with progressive BM in TNBC patients and found a 30% intracranial clinical benefit rate and overall survival and PFS of 2.1 months and 8 months, respectively.85
Veliparib is another PARP inhibitor that is brain permeable and was evaluated in phase II clinical trial comparing cisplatin with or without Veliparib in patients with recurrent or metastatic TNBC with or without brain metastasis. For patients with germline BRCA (BReast CAncer) mutations, the PFS and overall survival were not significantly improved; however, the patients who were BRCA-like in biomarker analysis showed improvement from 4.2 months to 5.9 months and overall survival improved from 12 to 14 months.86 We are awaiting a detailed study of patients with brain metastasis.78
Immunothrerapy
There has been rapid advancement in the use of Immune Checkpoint Inhibitors (ICIs) in breast cancer, especially TNBC. IMPASSION-130 trial showed a benefit of Atezolizumab (in combination with nab-paclitaxel) for the treatment of TNBC. However, in subgroup analysis, there was no PFS benefit for BM patients. This could be from the fact that the population with BM was small in the study (6.3% of the population had BM).79
Another immunotherapy trial, the KEYNOTE-355 trial, showed that pembrolizumab plus chemotherapy improved PFS in PDL1 (Programmed death-ligand 1) positive (CPS>10) advanced or metastatic TNBC. However, it is to be noted that the trial did not exclude patients with BM if they were treated and stable (active central nervous system metastases or carcinomatous meningitis were excluded).3% of patients in both the treatment and control arm had stable BM.80
Some other phase 3 immunotherapy trials, such as IMPASSION 131 (NCT03125902) and KEYNOTE-119, have excluded active BM.81,82
Antibody–Drug Conjugate (ADC)
Sacituzumab Govitecan (SG) is a novel antibody–drug conjugate that has an anti-trop-2 monoclonal antibody conjugated to SN-38. Phase III ASCENT trial had shown improvements in PFS and overall survival in patients who had received at least two chemotherapy regimens for advanced disease.83 A subgroup analysis of patients with stable BM from the phase III ASCENT study showed that SG was numerically better than treatment of physician’s choice (TPC) for tumor response and PFS but not overall survival. A single-center non-randomized Phase 0 study is currently underway where SG is given preoperatively followed by craniotomy with surgery or biopsy of brain tumors (GBM (Glioblastoma Multiforme) and metastatic brain tumors from Breast) (NCT03995706). This study was preceded by a window of opportunity trial examining the intratumoral concentrations of Sacituzumab Govitecan (SG), SN-38, SN-38G. The results from the trial showed SG achieves therapeutically relevant concentrations of SN-38 at 150-fold mean IC50s for BCBM.93 This also led to a SWOG study that has started enrolling patients with a primary objective of evaluating the intracranial objective response rate in patients with brain metastasis from HER2-negative breast cancer.85 Other ADCs, such as Fam-Trastuzumab Deruxtecan-nxki, need further studies to evaluate efficacy in this treatment space.
Anti-Angiogenic Agents
To date, prospective studies have not revealed the impact of incorporating angiogenic inhibitor therapy on the overall survival of women with TNBC.39 Studies on Bevacizumab have shown an improvement in progression-free survival but have not demonstrated an impact on the overall survival of the patients.86–91 A Phase 2 trial of carboplatin and Bevacizumab had shown a CNS ORR of 63%, although out of the total of 38 patients, only 9 were HER2 negative.92 Similarly, Lu et al had shown in a single-arm phase 2 study, the effectiveness of bevacizumab preconditioning followed by etoposide and cisplatin in BMBC in patients progressing from whole-brain radiotherapy. In this case, only 6 out of 35 BMBC patients were TNBC.93
ANG1005 (paclitaxel trevatide) is a novel taxane derivative designed to cross the BBB and the BTB to enter the malignant cell through a lipoprotein receptor-related protein 1 transport system.39 A phase II trial with all subtypes of breast cancer patients with leptomeningeal disease and/or recurrent brain metastases revealed 77% intracranial benefit. The BM-TNBC subgroup had a clinical benefit ratio of 46%.87
Oligometastatic Brain Metastasis
This is a very distinct group of TNBC for whom, after treatment with local therapy, we do not have much data to guide the treatment. Some approaches used are to observe, and some advocate for treatment with agents that penetrate the blood–brain barrier. A non-randomized study from Korea had 112 breast cancer patients with brain metastasis (19% were isolated brain lesions). Out of this, 55% received systemic chemotherapy after some sort of local treatment (13% percent did not receive the local treatment) and showed benefit.94 It is important to note that majority of them had extracranial disease.
Challenges for Effective Treatments of BCBM
The challenge in using systemic treatments of TNBC for BM is due to the blood–brain barrier (BBB), preventing drugs and toxins from reaching the brain.95–97 The blood-brain barrier has multiple drug uptake and efflux mechanisms along with transporter proteins such as P-glycoprotein (ABCB1/MDR1) and ABCG2, which impacts the pharmacokinetics of systemic therapies by passive diffusion, active transport, and endocytosis.38 The passage of a drug through the BBB depends on the qualities such as polarity, charge, lipophilicity, molecular size, and hydrogen bonding.43 Animal knock-out models have also shown active efflux of anti-cancer drugs such as paclitaxel, doxorubicin lapatinib, and other tyrosine kinase inhibitors by the multidrug transporters ABCB1 and ABCB2.39–41 A study by Pardrigde et al reported the drug molecule needs to be lipid-soluble and under 400–500 Da size to cross the BBB.98
The BBB at the tumor site has been speculated to have altered permeability at the tumor site, and this tumor-capillary bed has been described as the blood tumor barrier (BTB).95 BTB is surrounded by a neuroinflammatory response, which impairs the transporter channel expression and function.95,99 These changes significantly impact the drug bioavailability and efficacy in the brain.99
BM from TNBC occurs earlier and is often associated with an aggressive extracranial disease, leading to worse outcomes as compared to other types of breast cancer. Though attempts are made to identify biomarkers for CNS metastases of TNBC, there still remains a deficit in these patients.100
Ongoing Clinical Trials and Future Prospects
Table 1 summarizes the various clinical trials currently underway, including details about treatment type, treatment targets, phase of clinical trial and treatment and control arms (if applicable), clinical trial.gov ID.
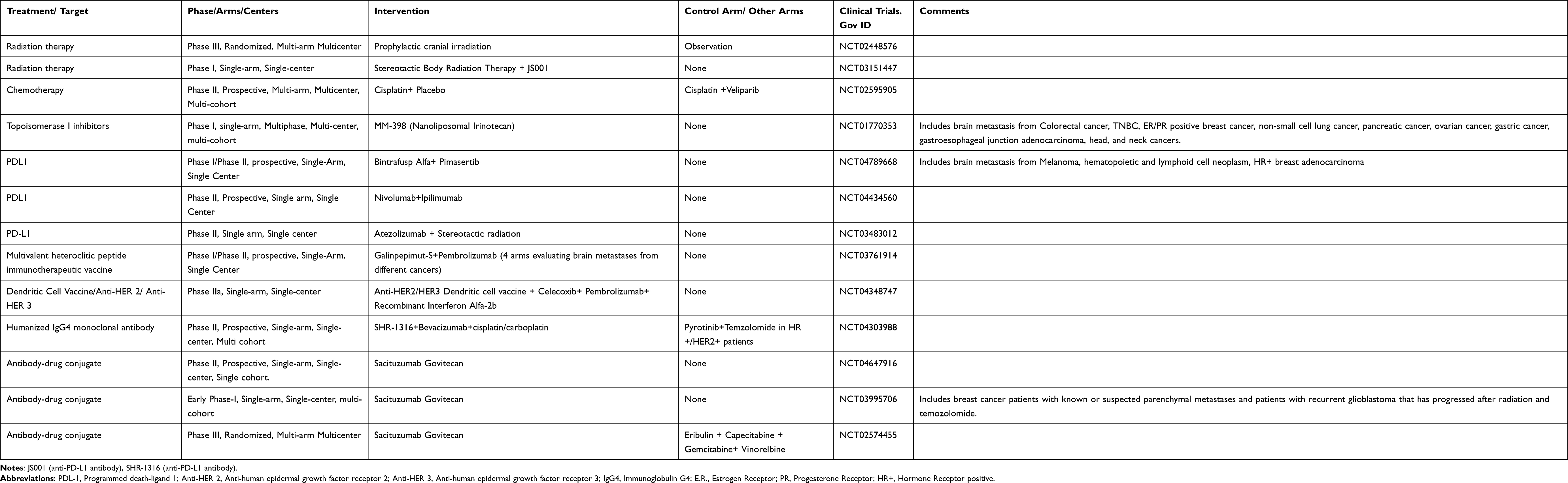 |
Table 1 Current Clinical Trials Involving Patients with Triple-Negative Breast Cancer with Brain Metastasis |
Other Future Prospective
Future developments in breast cancer will likely be based on multi-professional collaborations, individualized patient-centered approach, and treatments targeting the initial tumors in the breast to prevent metastasis.101 Several advances are in early phases of development, serving as new avenues in cancer care; however, their application in the management of TNBC is yet to be determined. Circulating tumor DNA (ctDNA) is secreted by tumor cells into the blood.102 Detection of ctDNA in plasma is currently being considered as a potent alternative to solid tumor biopsies.103 There are also several studies underway utilizing ctDNA as a tool for diagnosis, prediction, and prognosis of several malignancies.104 Studies have linked inferior distant disease-free survival to patients who had detectable ctDNA after neoadjuvant chemotherapy and were predictive of breast cancer recurrence. Further studies are required to adopt this into the mainstream practice, but the data so far has been promising.105,106
Multi-omics is the integration of Genomics (mapping of human genes and their interactions), transcriptomics (study of an organism’s RNA transcripts), proteomics (study of proteins) and metabolomics (the study of products of cell metabolism), epigenomics (study of changes in DNA and histone proteins), microbiomes (study of microbiota within the human tissues), system-biological approach, and multivariable algorithms for diagnosis, prognosis, and therapeutic purposes.107 The multi-omic approach integrated with machine learning has been studied as a tool to identify molecular signatures specific to premenopausal breast cancer women and was capable of stratifying patients into high and low breast cancer risk groups. Such an approach is important to predict, prevent, and personalize medicine to the individual.108 The Multiomics approach can hence help discover unique molecular signatures of the TNBC subtype and develop targeted prevention and treatment tailored to the patient in the near future.109
Conclusion
Metastatic breast cancer is the second most common cancer after metastatic lung cancer to be associated with brain metastases in the US.110 In recent years, there has been a significant advancement in treatment and surveillance options for various cancers leading to longer overall survival. The incidence of brain metastases appears to be increasing, with one meta-analysis suggesting that approximately one-third of patients with human epidermal growth factor receptor 2 (HER2)-positive, one-third of those with triple-negative, and 15% of those with hormone receptor-positive, HER2-negative metastatic breast cancer will develop brain metastases.19 Brain metastasis from triple-negative breast cancer has been largely unexplored as patients have been actively excluded from most clinical trials in the past. There are also currently no defined guidelines for surveillance of brain metastases, and the demands in this area remain unmet. The prognosis of BM from TNBC is lower as compared to metastasis from other subtypes of breast cancer. A multi-disciplinary team approach with a combination of various therapies is needed to achieve better results. The advances and innovations using multi-omics-based machine learning and ctDNA can help detect and develop therapies targeted at TNBC BM. Brain metastasis is still a challenging and uncharted territory. There is still a need for extensive research and encouragement to include more patients with brain metastases in clinical trials.
Disclosure
Dr Jose Pablo Leone reported grants from Kazia Therapeutics and received fees from Minerva Biotechnologies for consulting, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Howlader N, Noone AM, Krapcho M, et al, eds. SEER Cancer Statistics Review [Internet]. SEER Cancer Statistics Review. [cited June 12, 2021]. Available from: https://seer.cancer.gov/csr/1975_2018/.
2. DeSantis CE, Fedewa SA, Goding Sauer A, Kramer JL, Smith RA, Jemal A. Breast cancer statistics, 2015: convergence of incidence rates between black and white women. CA Cancer J Clin. 2016;66(1):31–42. doi:10.3322/caac.21320
3. Plasilova ML, Hayse B, Killelea BK, Horowitz NR, Chagpar AB, Lannin DR. Features of triple-negative breast cancer analysis of 38,813 cases from the national cancer database. Medicine. 2016;95:35. doi:10.1097/MD.0000000000004614
4. Kohler BA, Sherman RL, Howlader N, et al. Annual report to the nation on the status of cancer, 1975–2011, featuring incidence of breast cancer subtypes by race/ethnicity, poverty, and state. J Natl Cancer Inst. 2015;107(6). doi:10.1093/jnci/djv048
5. Kumar P, Aggarwal R. An overview of triple-negative breast cancer. Arch Gynecol Obstet. 2016;293(2):247–269. doi:10.1007/s00404-015-3859-y
6. Lin NU, Vanderplas A, Hughes ME, et al. Clinicopathologic features, patterns of recurrence, and survival among women with triple-negative breast cancer in the national comprehensive cancer network. Cancer. 2012;118(22):5463–5472. doi:10.1002/cncr.27581
7. Labrèche F, Goldberg MS, Hashim D, Weiderpass E. Breast cancer. In: Occupational Cancers; 2020:417–38.
8. Pistelli M, Pagliacci A, Battelli N, et al. Prognostic factors in early-stage triple-negative breast cancer: lessons and limits from clinical practice. Anticancer Res. 2013;33(6):2737–2742.
9. Ovcaricek T, Frkovic SG, Matos E, Mozina B, Borstnar S. Triple negative breast cancer - prognostic factors and survival. Radiol Oncol. 2011;45(1):46–52. doi:10.2478/v10019-010-0054-4
10. Tečić Vuger A, Šeparović R, Vazdar L, et al. Characteristics and prognosis of triple-negative breast cancer patients: a Croatian single institution retrospective cohort study. Acta Clin Croat. 2020;59(1):97–108. doi:10.20471/acc.2020.59.01.12
11. Niwińska A, Murawska M, Pogoda K. Breast cancer subtypes and response to systemic treatment after whole-brain radiotherapy in patients with brain metastases. Cancer. 2010;116(18):4238–4247. doi:10.1002/cncr.25391
12. Jin J, Gao Y, Zhang J, et al. Incidence, pattern and prognosis of brain metastases in patients with metastatic triple negative breast cancer. BMC Cancer. 2018;18(1):446. doi:10.1186/s12885-018-4371-0
13. Kim JS, Kim IA. Evolving treatment strategies of brain metastases from breast cancer: current status and future direction. Ther Adv Med Oncol. 2020;12:1–21. doi:10.1177/1758835920936117
14. Soni A, Ren Z, Hameed O, et al. Breast cancer subtypes predispose the site of distant metastases. Am J Clin Pathol. 2015;143(4):471–478. doi:10.1309/AJCPYO5FSV3UPEXS
15. Komorowski AS, Warner E, MacKay HJ, Sahgal A, Pritchard KI, Jerzak KJ. Incidence of brain metastases in nonmetastatic and metastatic breast cancer: is there a role for screening? Clin Breast Cancer. 2020;20(1):e54–e64. doi:10.1016/j.clbc.2019.06.007
16. Witzel I, Oliveira-Ferrer L, Pantel K, Müller V, Wikman H. Breast cancer brain metastases: biology and new clinical perspectives. Breast Cancer Res. 2016;18(1):1–9. doi:10.1186/s13058-015-0665-1
17. Kennecke H, Yerushalmi R, Woods R, et al. Metastatic behavior of breast cancer subtypes. J Clin Oncol. 2010;28(20):3271–3277. doi:10.1200/JCO.2009.25.9820
18. Achrol AS, Rennert RC, Anders C, et al. Brain metastases. Nat Rev Dis Primers. 2019;5(1):5. doi:10.1038/s41572-018-0055-y
19. Kuksis M, Gao Y, Tran W, et al. The incidence of brain metastases among patients with metastatic breast cancer: a systematic review and meta-analysis. Neuro-Oncology. 2021;23(6):894–904. doi:10.1093/neuonc/noaa285
20. Koniali L, Hadjisavvas A, Constantinidou A, et al. Risk factors for breast cancer brain metastases: a systematic review. Oncotarget. 2020;11(6):650–669. doi:10.18632/oncotarget.27453
21. Weil RJ, Palmieri DC, Bronder JL, Stark AM, Steeg PS. Breast cancer metastasis to the central nervous system. Am J Pathol. 2005;167(4):913–920. doi:10.1016/S0002-9440(10)61180-7
22. Ogawa K, Yoshii Y, Nishimaki T, et al. Treatment and prognosis of brain metastases from breast cancer. J Neurooncol. 2008;86(2):231–238. doi:10.1007/s11060-007-9469-1
23. Lentzsch S, Reichardt P, Weber F, Budach V, Dörken B. Brain metastases in breast cancer: prognostic factors and management. Eur J Cancer. 1999;35(4):580–585. doi:10.1016/S0959-8049(98)00421-3
24. Sperduto PW, Kased N, Roberge D, et al. Effect of tumor subtype on survival and the graded prognostic assessment for patients with breast cancer and brain metastases. Int J Radiat Oncol Biol Phys. 2012;82(5):2111–2117. doi:10.1016/j.ijrobp.2011.02.027
25. Nagtegaal SHJ, Claes A, Suijkerbuijk KPM, Schramel FMNH, Snijders TJ, Verhoeff JJC. Comparing survival predicted by the diagnosis-specific Graded Prognostic Assessment (DS-GPA) to actual survival in patients with 1–10 brain metastases treated with stereotactic radiosurgery. Radiother Oncol. 2019;138:173–179. doi:10.1016/j.radonc.2019.06.033
26. Griguolo G, Jacot W, Kantelhardt E, et al. External validation of modified breast graded prognostic assessment for breast cancer patients with brain metastases: a multicentric European experience. Breast. 2018;37:36–41. doi:10.1016/j.breast.2017.10.006
27. Brosnan EM, Anders CK. Understanding patterns of brain metastasis in breast cancer and designing rational therapeutic strategies. Ann Transl Med. 2018;6(9):163. doi:10.21037/atm.2018.04.35
28. Lv Y, Ma X, Du Y, Feng J. Understanding patterns of brain metastasis in triple-negative breast cancer and exploring potential therapeutic targets. Onco Targets Ther. 2021;14:589–607. doi:10.2147/OTT.S293685
29. Kotecha R. Modern-approaches-to-brain-cancer-metastases-in-breast-cancer; 2021 [cited September 19, 2021]. Available from: https://www.onclive.com/view/modern-approaches-to-brain-cancer-metastases-in-breast-cancer.
30. Darlix A, Louvel G, Fraisse J, et al. Impact of breast cancer molecular subtypes on the incidence, kinetics and prognosis of central nervous system metastases in a large multicentre real-life cohort. Br J Cancer. 2019;121(12):991–1000. doi:10.1038/s41416-019-0619-y
31. Niikura N, Hayashi N, Masuda N, et al. Treatment outcomes and prognostic factors for patients with brain metastases from breast cancer of each subtype: a multicenter retrospective analysis. Breast Cancer Res Treat. 2014;147(1):103–112. doi:10.1007/s10549-014-3090-8
32. Watase C, Shiino S, Shimoi T, et al. Breast cancer brain metastasis—overview of disease state, treatment options and future perspectives. Cancers. 2021;13(5):1078. doi:10.3390/cancers13051078
33. Screening magnetic resonance imaging of the brain in patients with breast cancer. Available from: https://ClinicalTrials.gov/show/NCT04030507.
34. Brain monitoring for high risk of brain metastases in metastatic breast cancer. Available from: https://ClinicalTrials.gov/show/NCT03617341.
35. MRI screening versus SYMptom-directed surveillance for brain metastases among patients with triple negative or HER2+ MBC. Available from: https://ClinicalTrials.gov/show/NCT03881605.
36. Bailleux C, Eberst L, Bachelot T. Treatment strategies for breast cancer brain metastases. Br J Cancer. 2021;124(1):142–155. doi:10.1038/s41416-020-01175-y
37. National Comprehensive Cancer Network. Breast cancer (version 7.2021); 2021 [cited August 31, 2021]. Available from: https://www.nccn.org/professionals/physician_gls/pdf/breast.pdf.
38. National Comprehensive Cancer Network. Central nervous system cancers (version 1.2021); 2021 [cited September 3, 2021]. Available from: https://www.nccn.org/professionals/physician_gls/pdf/cns.pdf.
39. Lee K-L, Chen G, Chen T-Y, Kuo Y-C, Su Y-K. Effects of cancer stem cells in triple-negative breast cancer and brain metastasis: challenges and solutions. Cancers. 2020;12(8):2122.
40. Leone JP, Leone BA. Breast cancer brain metastases: the last frontier. Exp Hematol Oncol. 2015;4(1):33. doi:10.1186/s40164-015-0028-8
41. Patchell RA, Tibbs PA, Walsh JW, et al. A randomized trial of surgery in the treatment of single metastases to the brain. N Engl J Med. 1990;322(8):494–500. doi:10.1056/NEJM199002223220802
42. Vecht CJ, Haaxma-Reiche H, Noordijk EM, et al. Treatment of single brain metastasis: radiotherapy alone or combined with neurosurgery? Ann Neurol. 1993;33(6):583–590. doi:10.1002/ana.410330605
43. Ampil FL, Nanda A, Willis BK, Nandy I, Meehan R. Metastatic disease in the cerebellum. The LSU Experience in 1981–1993. Am j Clin Oncol. 1996;19(5):509–511.
44. Rades D, Kieckebusch S, Haatanen T, Lohynska R, Dunst J, Schild SE. Surgical resection followed by whole brain radiotherapy versus whole brain radiotherapy alone for single brain metastasis. Int J Radiat Oncol Biol Phys. 2008;70(5):1319–1324. doi:10.1016/j.ijrobp.2007.08.009
45. Sause WT, Crowley JJ, Morantz R, et al. Solitary brain metastasis: results of an RTOG/SWOG protocol evaluation surgery + RT versus RT alone. Am J Clin Oncol. 1990;13(5):427–432. doi:10.1097/00000421-199010000-00013
46. Ewend MG, Morris DE, Carey LA, Ladha AM, Brem S. Guidelines for the initial management of metastatic brain tumors: role of surgery, radiosurgery, and radiation therapy. J Natl Compr Canc Netw. 2008;6(5):505–514. doi:10.6004/jnccn.2008.0038
47. Soffietti R, Kocher M, Abacioglu UM, et al. A European Organisation for research and treatment of cancer phase III trial of adjuvant whole-brain radiotherapy versus observation in patients with one to three brain metastases from solid tumors after surgical resection or radiosurgery: quality-of-lif. J Clin Oncol. 2013;31(1):65–72. doi:10.1200/JCO.2011.41.0639
48. Chang EL, Wefel JS, Hess KR, et al. Neurocognition in patients with brain metastases treated with radiosurgery or radiosurgery plus whole-brain irradiation: a randomised controlled trial. Lancet Oncol. 2009;10(11):1037–1044. doi:10.1016/S1470-2045(09)70263-3
49. Brown PD, Jaeckle K, Ballman KV, et al. Effect of radiosurgery alone vs radiosurgery with whole brain radiation therapy on cognitive function in patients with 1 to 3 brain metastases: a randomized clinical trial. JAMA. 2016;316(4):401–409. doi:10.1001/jama.2016.9839
50. Brown PD, Ballman KV, Cerhan JH, et al. Postoperative stereotactic radiosurgery compared with whole brain radiotherapy for resected metastatic brain disease (NCCTG N107C/CEC·3): a multicentre, randomised, controlled, phase 3 trial. Lancet Oncol. 2017;18(8):1049–1060. doi:10.1016/S1470-2045(17)30441-2
51. Ehrlich MI, Schiff E, Knisely JPS, et al. Tumor control and survival in patients with ten or more brain metastases treated with stereotactic radiosurgery: a retrospective analysis. J Neurooncol. 2019;143(1):167–174. doi:10.1007/s11060-019-03153-8
52. Ahn K-H, Yenice KM, Koshy M, Slavin KV, Aydogan B. Frame-based radiosurgery of multiple metastases using single-isocenter volumetric modulated arc therapy technique. J Appl Clin Med Phys. 2019;20(8):21–28. doi:10.1002/acm2.12672
53. Tsao MN, Xu W, Wong RK, et al. Whole brain radiotherapy for the treatment of newly diagnosed multiple brain metastases. Cochrane Database Syst Rev. 2018;1(1):CD003869. doi:10.1002/14651858.CD003869.pub4
54. Brown PD, Gondi V, Pugh S, et al. Hippocampal avoidance during whole-brain radiotherapy plus memantine for patients with brain metastases: phase III trial NRG oncology CC001. J Clin Oncol. 2020;38(10):1019–1029. doi:10.1200/JCO.19.02767
55. Grosu A-L, Frings L, Bentsalo I, et al. Whole-brain irradiation with hippocampal sparing and dose escalation on metastases: neurocognitive testing and biological imaging (HIPPORAD) - a phase II prospective randomized multicenter trial (NOA-14, ARO 2015-3, DKTK-ROG). BMC Cancer. 2020;20(1):532. doi:10.1186/s12885-020-07011-z
56. Stereotactic radiosurgery compared with Hippocampal-Avoidant Whole Brain Radiotherapy (HA-WBRT) plus memantine for 5–15 brain metastases. Available from: https://ClinicalTrials.gov/show/NCT03550391.
57. Churilla TM, Chowdhury IH, Handorf E, et al. Comparison of local control of brain metastases with stereotactic radiosurgery vs surgical resection: a secondary analysis of a randomized clinical trial. JAMA Oncol. 2019;5(2):243–247. doi:10.1001/jamaoncol.2018.4610
58. Brastianos PK, Carter SL, Santagata S, et al. Genomic characterization of brain metastases reveals branched evolution and potential therapeutic targets. Cancer Discov. 2015;5(11):1164–1177. doi:10.1158/2159-8290.CD-15-0369
59. Awada A, Colomer R, Inoue K, et al. Neratinib plus paclitaxel vs trastuzumab plus paclitaxel in previously untreated metastatic ERBB2-Positive breast cancer: the NEfERT-T randomized clinical trial. JAMA Oncol. 2016;2(12):1557–1564. doi:10.1001/jamaoncol.2016.0237
60. Freedman RA, Gelman RS, Anders CK, et al. TBCRC 022: a phase II trial of neratinib and capecitabine for patients with human epidermal growth factor receptor 2–positive breast cancer and brain metastases. J Clin Oncol. 2019;37(13):1081–1089. doi:10.1200/JCO.18.01511
61. Petrelli F, Ghidini M, Lonati V, et al. The efficacy of lapatinib and capecitabine in HER-2 positive breast cancer with brain metastases: a systematic review and pooled analysis. Eur J Cancer. 2017;84:141–148. doi:10.1016/j.ejca.2017.07.024
62. Bachelot T, Romieu G, Campone M, et al. Lapatinib plus capecitabine in patients with previously untreated brain metastases from HER2-positive metastatic breast cancer (LANDSCAPE): a single-group phase 2 study. Lancet Oncol. 2013;14(1):64–71. doi:10.1016/S1470-2045(12)70432-1
63. Hikino H, Yamada T, Johbara K, Obayashi N, Ozaki N. Potential role of chemo-radiation with oral capecitabine in a breast cancer patient with central nervous system relapse. Breast. 2006;15(1):97–99. doi:10.1016/j.breast.2005.03.006
64. Cocconi G, Lottici R, Bisagni G, et al. Combination therapy with platinum and etoposide of brain metastases from breast carcinoma. Cancer Invest. 1990;8(3–4):327–334. doi:10.3109/07357909009012049
65. Nieder C. Front-line chemotherapy with cisplatin and etoposide for patients with brain metastases from breast carcinoma, nonsmall cell lung carcinoma, or malignant melanoma. A prospective study. Cancer. 1999;86:900–903. United States. doi:10.1002/(SICI)1097-0142(19990901)86:5<900::AID-CNCR30>3.0.CO;2-5
66. Franciosi V, Cocconi G, Michiara M, et al. Front-line chemotherapy with cisplatin and etoposide for patients with brain metastases from breast carcinoma, nonsmall cell lung carcinoma, or malignant melanoma: a prospective study. Cancer. 1999;85(7):1599–1605.
67. Viñolas N, Graus F, Mellado B, Caralt L, Estapé J. Phase II trial of cisplatinum and etoposide in brain metastases of solid tumors. J Neurooncol. 1997;35(2):145–148. doi:10.1023/A:1005835430489
68. Lassman AB, Abrey LE, Shah GD, et al. Systemic high-dose intravenous methotrexate for central nervous system metastases. J Neurooncol. 2006;78(3):255–260. doi:10.1007/s11060-005-9044-6
69. Wang ML, Yung WK, Royce ME, Schomer DF, Theriault RL. Capecitabine for 5-fluorouracil-resistant brain metastases from breast cancer. Am J Clin Oncol. 2001;24(4):421–424. doi:10.1097/00000421-200108000-00026
70. Rivera E, Meyers C, Groves M, et al. Phase I study of capecitabine in combination with temozolomide in the treatment of patients with brain metastases from breast carcinoma. Cancer. 2006;107(6):1348–1354. doi:10.1002/cncr.22127
71. Rosner D, Nemoto T, Lane WW. Chemotherapy induces regression of brain metastases in breast carcinoma. Cancer. 1986;58(4):832–839. doi:10.1002/1097-0142(19860815)58:4<832::AID-CNCR2820580404>3.0.CO;2-W
72. Erten C, Demir L, Somali I, et al. Cisplatin plus gemcitabine for treatment of breast cancer patients with brain metastases; a preferential option for triple negative patients? Asian Pac J Cancer Prev. 2013;14(6):3711–3717. doi:10.7314/APJCP.2013.14.6.3711
73. Gonzalez-Angulo AM, Timms KM, Liu S, et al. Incidence and outcome of BRCA mutations in unselected patients with triple receptor-negative breast cancer. Clin Cancer Res. 2011;17(5):1082LP– 1089.
74. Hurvitz SA, Gonçalves A, Rugo HS, et al. Talazoparib in patients with a germline BRCA-mutated advanced breast cancer: detailed safety analyses from the phase III EMBRACA trial. Oncologist. 2020;25(3):e439–e450. doi:10.1634/theoncologist.2019-0493
75. FDA approves talazoparib for gBRCAm HER2-negative locally advanced or metastatic breast cancer; 2018 [cited February 10, 2021]. Available from: https://www.fda.gov/drugs/drug-approvals-and-databases/fda-approves-talazoparib-gbrcam-her2-negative-locally-advanced-or-metastatic-breast-cancer.
76. Food and Drug Administration. FDA approves olaparib for germline BRCA-mutated metastatic breast cancer; 2018 [cited February 10, 2021]. Available from: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-olaparib-germline-brca-mutated-metastatic-breast-cancer#:~:text=On January 12, 2018, the,gBRCAm),HER2-negative metastatic.
77. Anders C, Deal AM, Abramson V, et al. TBCRC 018: phase II study of iniparib in combination with irinotecan to treat progressive triple negative breast cancer brain metastases. Breast Cancer Res Treat. 2014;146(3):557–566. doi:10.1007/s10549-014-3039-y
78. Cisplatin with or without veliparib in treating patients with recurrent or metastatic triple-negative and/or BRCA mutation-associated breast cancer with or without brain metastases. Available from: https://ClinicalTrials.gov/show/NCT02595905.
79. Schmid P, Adams S, Rugo HS, et al. Atezolizumab and Nab-paclitaxel in advanced triple-negative breast cancer. N Engl J Med. 2018;379(22):2108–2121. doi:10.1056/NEJMoa1809615
80. Cortes J, Cescon DW, Rugo HS, et al. Pembrolizumab plus chemotherapy versus placebo plus chemotherapy for previously untreated locally recurrent inoperable or metastatic triple-negative breast cancer (KEYNOTE-355): a randomised, placebo-controlled, double-blind, phase 3 clinical trial. Lancet. 2020;396(10265):1817–1828. doi:10.1016/S0140-6736(20)32531-9
81. Winer EP, Lipatov O, Im S-A, et al. Pembrolizumab versus investigator-choice chemotherapy for metastatic triple-negative breast cancer (KEYNOTE-119): a randomised, open-label, phase 3 trial. Lancet Oncol. 2021;22(4):499–511. doi:10.1016/S1470-2045(20)30754-3
82. A study of atezolizumab and paclitaxel versus placebo and paclitaxel in participants with previously untreated locally advanced or metastatic Triple Negative Breast Cancer (TNBC). Available from: https://ClinicalTrials.gov/show/NCT03125902.
83. Bardia A, Tolaney SM, Loirat D, et al. LBA17 ASCENT: a randomized phase III study of sacituzumab govitecan (SG) vs treatment of physician’s choice (TPC) in patients (pts) with previously treated metastatic triple-negative breast cancer (mTNBC). Ann Oncol. 2020;31:S1149–S1150. doi:10.1016/j.annonc.2020.08.2245
84. Brenner AJ, Pandey R, Chiou J, et al. 373MO delivery and activity of SN-38 by sacituzumab govitecan in CNS tumours. Ann Oncol. 2020;31:S401. doi:10.1016/j.annonc.2020.08.482
85. Testing sacituzumab govitecan therapy in patients with HER2-negative breast cancer and brain metastases. Available from: https://ClinicalTrials.gov/show/NCT04647916.
86. Brufsky AM, Hurvitz S, Perez E, et al. RIBBON-2: a randomized, double-blind, placebo-controlled, phase III trial evaluating the efficacy and safety of bevacizumab in combination with chemotherapy for second-line treatment of human epidermal growth factor receptor 2-negative metastatic breast. J Clin Oncol. 2011;29(32):4286–4293. doi:10.1200/JCO.2010.34.1255
87. Kumthekar P, Tang S-C, Brenner AJ, et al. ANG1005, a brain-penetrating peptide-drug conjugate, shows activity in patients with breast cancer with leptomeningeal carcinomatosis and recurrent brain metastases. Clin Cancer Res. 2020;26(12):2789–2799. doi:10.1158/1078-0432.CCR-19-3258
88. Miles DW, Diéras V, Cortés J, Duenne -A-A, Yi J, O’Shaughnessy J. First-line bevacizumab in combination with chemotherapy for HER2-negative metastatic breast cancer: pooled and subgroup analyses of data from 2447 patients. Ann Oncol. 2013;24(11):2773–2780. doi:10.1093/annonc/mdt276
89. Bell R, Brown J, Parmar M, et al. Final efficacy and updated safety results of the randomized phase III BEATRICE trial evaluating adjuvant bevacizumab-containing therapy in triple-negative early breast cancer. Ann Oncol. 2017;28(4):754–760. doi:10.1093/annonc/mdw665
90. Miles DW, Chan A, Dirix LY, et al. Phase III Study of bevacizumab plus docetaxel compared with placebo plus docetaxel for the first-line treatment of human epidermal growth factor receptor 2–negative metastatic breast cancer. J Clin Oncol. 2010;28(20):3239–3247. doi:10.1200/JCO.2008.21.6457
91. Miller K, Wang M, Gralow J, et al. Paclitaxel plus bevacizumab versus paclitaxel alone for metastatic breast cancer. N Engl J Med. 2007;357(26):2666–2676. doi:10.1056/NEJMoa072113
92. Leone JP, Emblem KE, Weitz M, et al. Phase II trial of carboplatin and bevacizumab in patients with breast cancer brain metastases. Breast Cancer Res. 2020;22(1):131. doi:10.1186/s13058-020-01372-w
93. Lu Y-S, Chen T-W-W, Lin C-H, et al. Bevacizumab preconditioning followed by etoposide and cisplatin is highly effective in treating brain metastases of breast cancer progressing from whole-brain radiotherapy. Clin Cancer Res. 2015;21(8):1851–1858. doi:10.1158/1078-0432.CCR-14-2075
94. Chang WC, Eom YH, Lee SH, Chae BJ, Song BJ, Jung SS. The effectiveness of chemotherapy in breast cancer patients with brain metastases. Korean J Clin Oncol. 2014;10(2):103–111. doi:10.14216/kjco.14019
95. Deeken JF, Löscher W. The blood-brain barrier and cancer: transporters, treatment, and trojan horses. Clin Cancer Res. 2007;13(6):1663–1674. doi:10.1158/1078-0432.CCR-06-2854
96. Fong CW. Permeability of the blood-brain barrier: molecular mechanism of transport of drugs and physiologically important compounds. J Membr Biol. 2015;248(4):651–669. doi:10.1007/s00232-015-9778-9
97. Soffietti R, Ahluwalia M, Lin N, Rudà R. Management of brain metastases according to molecular subtypes. Nat Rev Neurol. 2020;16(10):557–574. doi:10.1038/s41582-020-0391-x
98. Pardridge WM. The blood-brain barrier: bottleneck in brain drug development. NeuroRx. 2005;2(1):3–14. doi:10.1602/neurorx.2.1.3
99. Gril B, Paranjape AN, Woditschka S, et al. Reactive astrocytic S1P3 signaling modulates the blood-tumor barrier in brain metastases. Nat Commun. 2018;9(1):2705. doi:10.1038/s41467-018-05030-w
100. Laimito KR, Gámez-Pozo A, Sepúlveda J, et al. Characterisation of the triple negative breast cancer phenotype associated with the development of central nervous system metastases. Ecancermedicalscience. 2016;10:632. doi:10.3332/ecancer.2016.632
101. Polivka J, Kralickova M, Polivka J, Kaiser C, Kuhn W, Golubnitschaja O. Mystery of the brain metastatic disease in breast cancer patients: improved patient stratification, disease prediction and targeted prevention on the horizon? EPMA J. 2017;8(2):119–127. doi:10.1007/s13167-017-0087-5
102. Stroun M, Anker P, Maurice P, Lyautey J, Lederrey C, Beljanski M. Neoplastic characteristics of the DNA found in the plasma of cancer patients. Oncology. 1989;46(5):318–322. doi:10.1159/000226740
103. Wu X, Li J, Gassa A, et al. Circulating tumor DNA as an emerging liquid biopsy biomarker for early diagnosis and therapeutic monitoring in hepatocellular carcinoma. Int J Biol Sci. 2020;16(9):1551–1562. doi:10.7150/ijbs.44024
104. Crigna AT, Samec M, Koklesova L, et al. Cell-free nucleic acid patterns in disease prediction and monitoring—hype or hope? EPMA J. 2020;11(4):603–627. doi:10.1007/s13167-020-00226-x
105. Pike J. ‘Liquid biopsy’ tech contributes to successful clinical trial for detecting breast cancer recurrence; 2020. Available from: https://www.purdue.edu/newsroom/releases/2020/Q3/liquid-biopsy-tech-contributes-to-successful-clinical-trial-for-detecting-breast-cancer-recurrence.html.
106. Radovich M, Jiang G, Hancock BA, et al. Association of circulating tumor DNA and circulating tumor cells after neoadjuvant chemotherapy with disease recurrence in patients with triple-negative breast cancer: preplanned secondary analysis of the BRE12-158 randomized clinical trial. JAMA Oncol. 2020;6(9):1410–1415. doi:10.1001/jamaoncol.2020.2295
107. Gerner C, Costigliola V, Golubnitschaja O. Multiomic patterns in body fluids: technological challenge with a great potential to implement the advanced paradigm of 3P medicine. Mass Spectrom Rev. 2020;39(5–6):442–451. doi:10.1002/mas.21612
108. Fröhlich H, Patjoshi S, Yeghiazaryan K, Kehrer C, Kuhn W, Golubnitschaja O. Premenopausal breast cancer: potential clinical utility of a multi-omics based machine learning approach for patient stratification. EPMA J. 2018;9(2):175–186. doi:10.1007/s13167-018-0131-0
109. Golubnitschaja O, Filep N, Yeghiazaryan K, et al. Multi-omic approach decodes paradoxes of the triple-negative breast cancer: lessons for predictive, preventive and personalised medicine. EPMA J. 2020;39(5–6):603–627. doi:10.1007/s00726-017-2524-0
110. Barnholtz-Sloan JS, Sloan AE, Davis FG, Vigneau FD, Lai P, Sawaya RE. Incidence proportions of brain metastases in patients diagnosed (1973 to 2001) in the metropolitan Detroit cancer surveillance system. J Clin Oncol. 2004;22(14):2865–2872. doi:10.1200/JCO.2004.12.149
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.