Back to Journals » ClinicoEconomics and Outcomes Research » Volume 13
Centers of Excellence Implementation for Treating Rheumatoid Arthritis in Colombia: A Cost-Analysis
Authors Santos-Moreno P ![]() , Alvis-Zakzuk NJ
, Alvis-Zakzuk NJ ![]() , Villarreal-Peralta L, Carrasquilla-Sotomayor M, de la Hoz-Restrepo F, Alvis-Guzmán N
, Villarreal-Peralta L, Carrasquilla-Sotomayor M, de la Hoz-Restrepo F, Alvis-Guzmán N ![]()
Received 23 February 2021
Accepted for publication 13 May 2021
Published 23 June 2021 Volume 2021:13 Pages 583—591
DOI https://doi.org/10.2147/CEOR.S308024
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Dean Smith
Pedro Santos-Moreno,1 Nelson J Alvis-Zakzuk,2 Laura Villarreal-Peralta,1 Maria Carrasquilla-Sotomayor,3 Fernando de la Hoz-Restrepo,4 Nelson Alvis-Guzmán5,6
1Rheumatology, Biomab IPS, Bogotá, Colombia; 2Department of Health Sciences, Universidad de la Costa -CUC, Barranquilla, Colombia; 3Department of Health Technology Assessment, ALZAK Foundation, Cartagena, Colombia; 4Department of Public Health, Universidad Nacional de Colombia, Bogotá, DC, Colombia; 5Department of Health Sciences, Universidad de la Costa – CUC, Barranquilla, Colombia; 6Department of Economic Sciences, Universidad de Cartagena, Cartagena, Colombia
Correspondence: Pedro Santos-Moreno
Rheumatology, Biomab IPS, Calle 48 # 13-86, Bogotá, Colombia
Email [email protected]
Background: Health systems need to optimize the use of resources, especially in high-cost diseases as rheumatoid arthritis (RA). We aimed to evaluate the efficiency of using centers of excellence (CoE) as a strategy for improving RA treatment in Colombia.
Methods: A cost description analysis was carried out using the standard costing technique. We estimated the costs of medical consultations, laboratories, images, and medications for RA. Categories of care standards stratified by severity were defined using the disease activity score in 28 joints (DAS28). We evaluated the impact, in terms of costs (US dollars), for providing RA clinical care for a previously described cohort using the CoE approach. Statistical analyses were performed in Microsoft Excel®, and R.
Results: Expenditure on therapeutic drugs increases as the severity of RA increases. Drugs represent 53.6% of the total cost for the low disease activity (LDA) stage, 75.2% for moderate disease activity (MDA), 88.5% for severe disease activity (SDA) and 97% for SDA with biologic treatment (SDA+Biologic). Treating 968 patients would cost US$612,639 (US$487,978– 1,220,160) at baseline, per year. After a year of follow-up at the CoE, treating the same patients would cost US$388,765 (US$321,710– 708,476), which implies potential cost-savings of up to US$223,874 per year.
Conclusion: The strategy of providing clinical care for RA through CoE can save US$231.3 per patient-per year. The results of our study show that CoE could greatly impact the public policies dealing with treatment of RA in Colombia. Applying the CoE model in our country would both improve health outcomes, as well as being more efficient in terms of costs.
Keywords: rheumatoid arthritis, treat to target, cost-savings, cost-analysis
Introduction
Rheumatoid arthritis (RA) is a public health challenge around the world.1–3 RA is characterized by its chronicity and the progressive loss of joint function.1–3 This joint damage may occur in the early stages of the disease, and after 2 years, nearly 75% of the patients may develop joint damage with bone erosion.1–3
Health systems face the issue of having to guarantee both maximum care to the most people, while still being able to finance all the medical technologies required to do so.4,5 Resource shortage brings up challenges for economic and assignment efficiency, in the management of health services. To this extent, health systems need to design strategies that optimize resource utilization to improve the patient care. The principles that should guide the design of health system models are efficiency, equity, and effectiveness.4,5
In upper-middle-income countries such as Colombia, despite high health insurance coverage rates,6 there is evidence of fragmentation in health care processes,7 especially in chronic diseases like RA. This leads to increased health expenditures for both providers and families, as well as worse health outcomes for patients. A possible solution for this would be providing highly specialized service through what is called a Center of Excellence (CoE). A CoE centralizes the management of one, or multiple, disease(s) helping to reduce costs and improving clinical outcomes.8
Using CoEs for RA as example of clinical management, an initiative was suggested by the Pan American League of Associations of Rheumatology (PANLAR) to overcome the deficiencies of fragmented health systems and prioritize more effective RA care.9 In environments where health care is fragmented, there are many barriers for finding adequate care such as (a) geographical distribution of the patients, (b) low health insurance coverage, and (c) low availability of specialists for the management of chronic rheumatoid disease.8,9 Additionally, there is a need for standardized measurement parameters to obtain quantifiable clinical results in high-cost rheumatic pathologies such as RA. Consequently, in 2010, the first recommendations on treat-to-target (T2T) were made based on evidence and the opinions of experts.10 In 2014, these recommendations were revised and adjusted11; T2T allows for measuring the percentage of patients that achieve remission, both in individual and group populations.11
In Colombia RA is an important cause of mortality, morbidity, and burden of disease; more than 72,000 RA patients have high rates of work disability, absenteeism, and presenteeism.12,13 This also results in a high economic burden for the health systems and families, as it is associated with a higher use of health resources and higher costs.2,14
In this study, we present the results of an economic evaluation of the efficiency of a Colombian CoE providing a comprehensive model of patient-centered care (PCC) for RA under the T2T recommendations.
We believe that these results may contribute to the discussion about how to provide a better service to patients suffering from chronic high-cost pathologies.
Methods
This study is an integral part of the evaluation of the efficiency and effectiveness of implementing a CoE for the comprehensive clinical management of RA. Results of this evaluation were presented in a previous publication;15 in that study, health outcomes were prospectively collected in 968 patients followed-up for 24 months using a treat-to-target (T2T) strategy with a patient-centered care (PCC) model. Regarding DAS28, there was a statistically significant improvement (p < 0.001) in the average DAS28 comparing at the beginning of the time analysis and after 24 months, decreasing from 3.1 (SD 1.0) to 2.4 (SD 0.7). In all patients, the reduction of disease activity was about 65% (95% CI, 58–71).15
Here we present the measures of the efficiency of the CoE approach using a cost-analysis from the perspective of a third payer.16 Methods have been described in the previous paper15; in brief, we used the technique of standard costing17,18 for the regular RA patient care process. This method is analogous to the bottom-up approach (micro-costing), but has several advantages like allowing for the generalization of results obtained in different settings with variable levels of complexity because it does not consider structural or indirect costs.19,20
Care Standards of the CoE Model
The suggested CoE model is based on an adaptation of the clinical practice guidelines for the management of RA in Colombia.13 Care standards for each severity level of RA, which are defined by the DAS28 score, involve the use of different types and frequencies of health services.15
One patient is reviewed by different medical specialists and is subject to several laboratory and imaging tests depending on the severity of the disease activity. In addition, a patient safety program, supplementary to the above mentioned services, aimed to prevent adverse events and/or ensure the proper management of them when they occur has been put into place.15 Patients receive conventional disease-modifying antirheumatic drugs (cDMARDs) and biologic medications (bDMARDs), depending on the DAS28 and their response to treatment.
Cost-Analysis
We estimated the costs of medical consultations, laboratory tests, imaging tests, and pharmacological treatment measuring the health care resource utilization recommended in the CoE´s standard protocol by activity level of the disease.
Costs were estimated following the recommendations from the Economic Assessment Guideline of the Instituto de Evaluación Tecnológica en Salud (IETS) of Colombia;21 IETS (Institute of Technological Evaluation in Health) is the economic assessment agency of Colombia, and its mission is to produce information based on evidence in order to contribute to the development of better public and practical policies in health care (Law 1438 of 2011).22
Costs of pharmacological treatments were computed using official information from the following sources: a) Newsletters from the National Commission for Prices of Medications, and b) Information from the Drug Price Information System (Sistema de Información de Precios de Medicamentos, SISMED in Spanish) encompassing the period of January to December 2017.23 SISMED reports prices (minimum price, average price, maximum price, and number of units sold) for each drug allowed to be sold in Colombia. For this study, each drug price was assigned according to the SISMED reported prices, weighing them by the number of units sold in the country.21 Costs of laboratory and imaging tests, and medical consultations were calculated using the Instituto de Seguros Sociales’s price list (Social Security price list), adding 30%, as recommended by the IETS.21
We evaluated the impact in terms of health and economic results after the application of a CoE model in the patient cohort selected in a previous publication.15 To achieve this, we calculated the potential cost-savings of caring for a cohort of patients that was previously analyzed15 at different moments in time: baseline, follow-up at month 6, and follow-up after a year. This calculation was done by multiplying the number of people at each moment and the severity level by the estimated cost for each of the stages of the disease. The statistical analyses were carried out using Microsoft Excel® 2016 and R programming.
All costs were reported in United States dollars (US$), and using the average exchange rate reported by the Banco de la República de Colombia for 2017, which was US$1 = $2,951.3 Colombian pesos.24
Ethics
This study was approved by the Institutional Research Board of Biomab IPS, act 004–25042017. All patients had previously signed informed consent for data use. This study did not represent risks for the patients according to the Resolution 8430 of 1993 of the Ministry of Health of Colombia. All data that could identify a patient were anonymized.
Results
Baseline characteristics of the analyzed cohort are shown in Table 1. Nine hundred sixty-eight patients were included in these analyses, 19.8% were men. The median age was 64 years, and the mean of disease duration was 7.7 years (1–52). Table 2 reports the annual healthcare resource utilization and costs of medical consultation, laboratory, and imaging tests, per year, according to RA disease activity at the CoE. The annual cost of services is 2.1 times greater (US$293.8 vs US$141.6) in patients with severe disease activity, compared to patients in remission (REM).
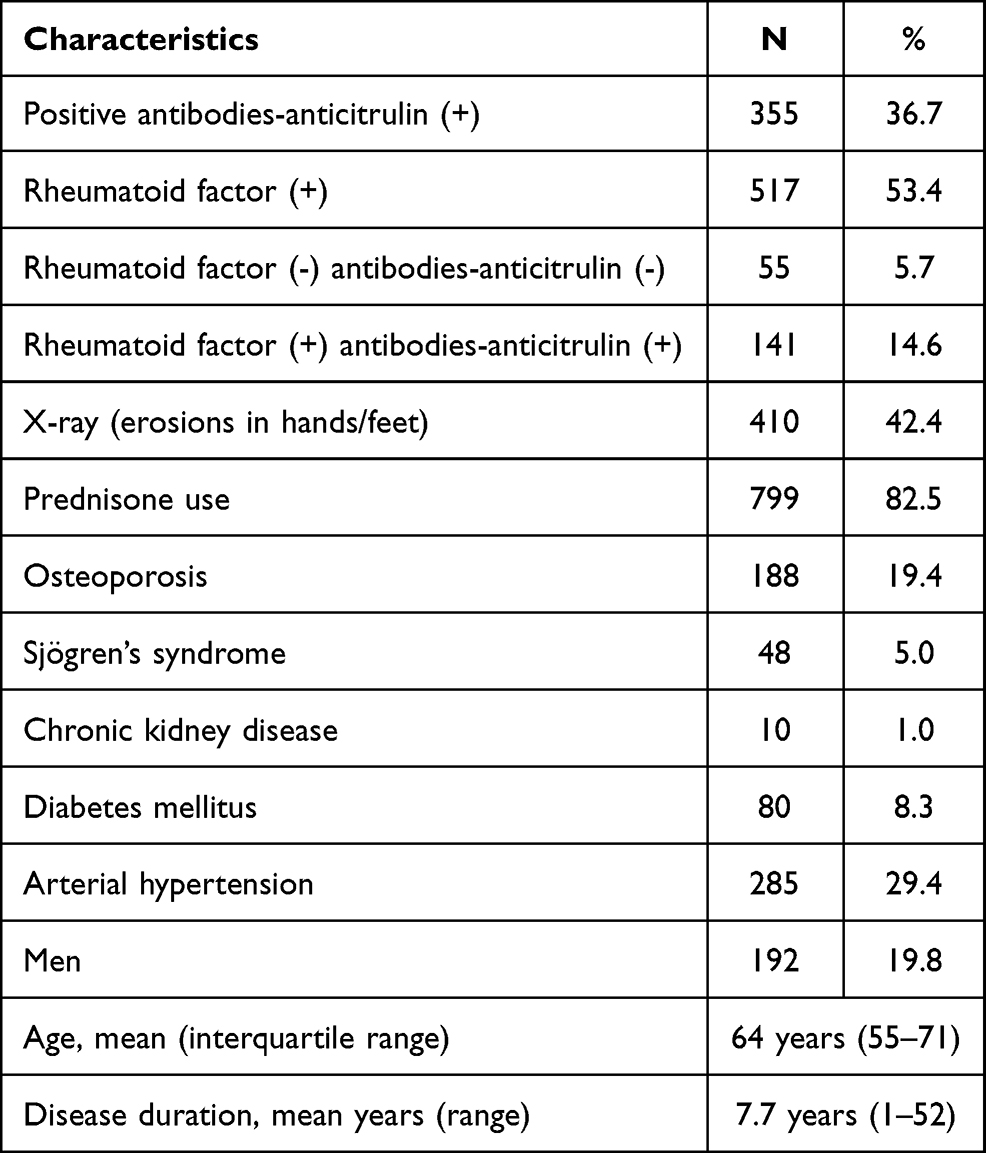 |
Table 1 Main Characteristics of the Studied Patients. N = 968 |
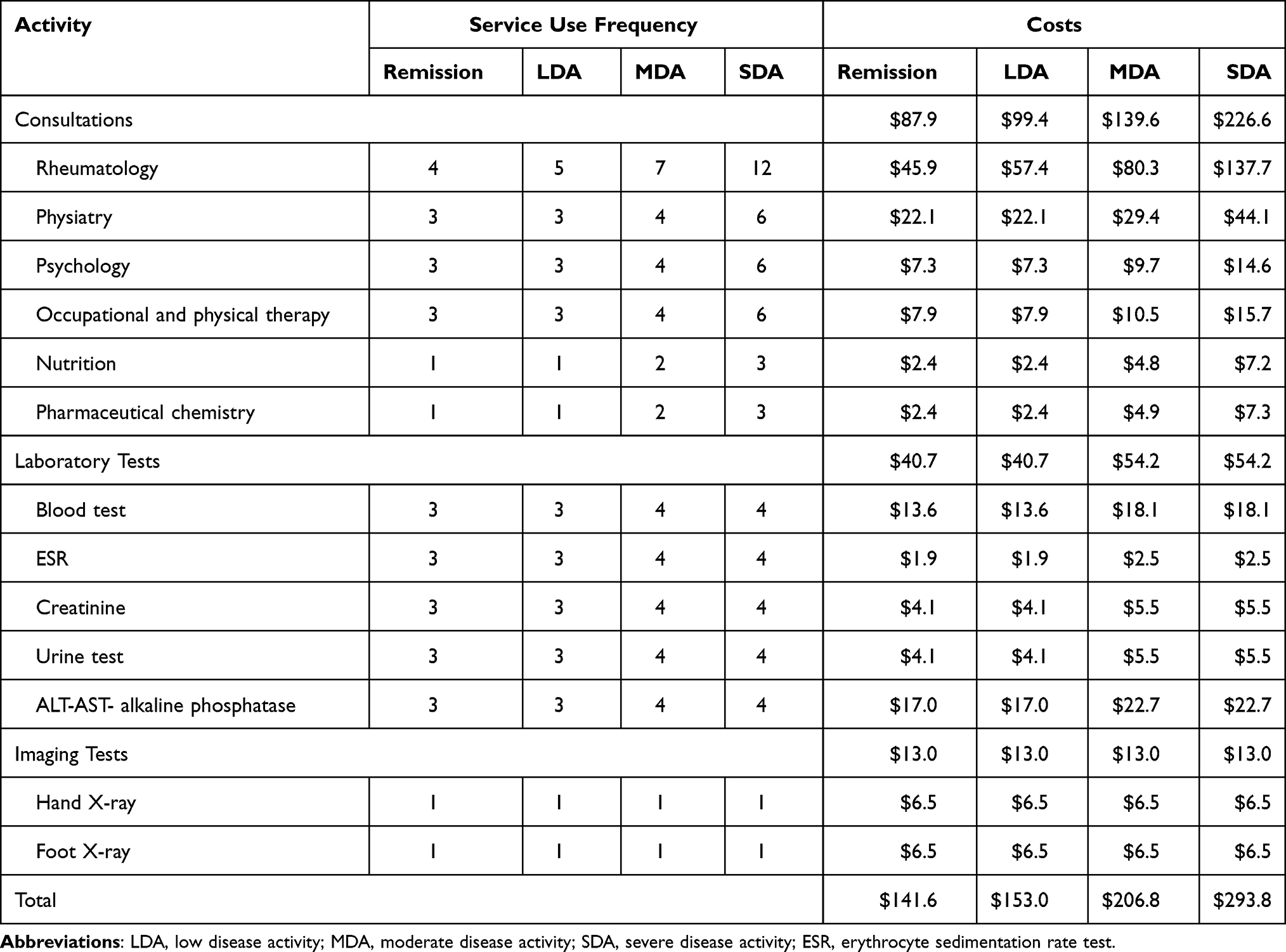 |
Table 2 Annual Costs of Consultation, Laboratory and Imaging Tests Associated with the Treatment of RA at a CoE |
The annual costs for the pharmaceutical treatment of a RA patient at the CoE through the different stages of the disease are presented in Table 3. Figure 1A shows the total annual costs of treating a patient at a CoE according to the various severity levels present. We observed that 39.9% of the costs of a patient in remission are spent on drugs, 37.3% on medical consultations, 17.2% on laboratory exams, and the rest on imaging. As the severity of the disease increases, drug costs represent a higher percentage of the overall costs. Among low disease activity (LDA) patients, drugs represent 53.6%, while medical consultations are 30.1% of the overall costs; on the other hand, for moderate disease activity (MDA) patients, drugs represent 75.2%, for severe disease activity (SDA) patients 88.5%, and for SDA+Biologic patients, drugs are 96.7% of the total expenditures (Figure 1B).
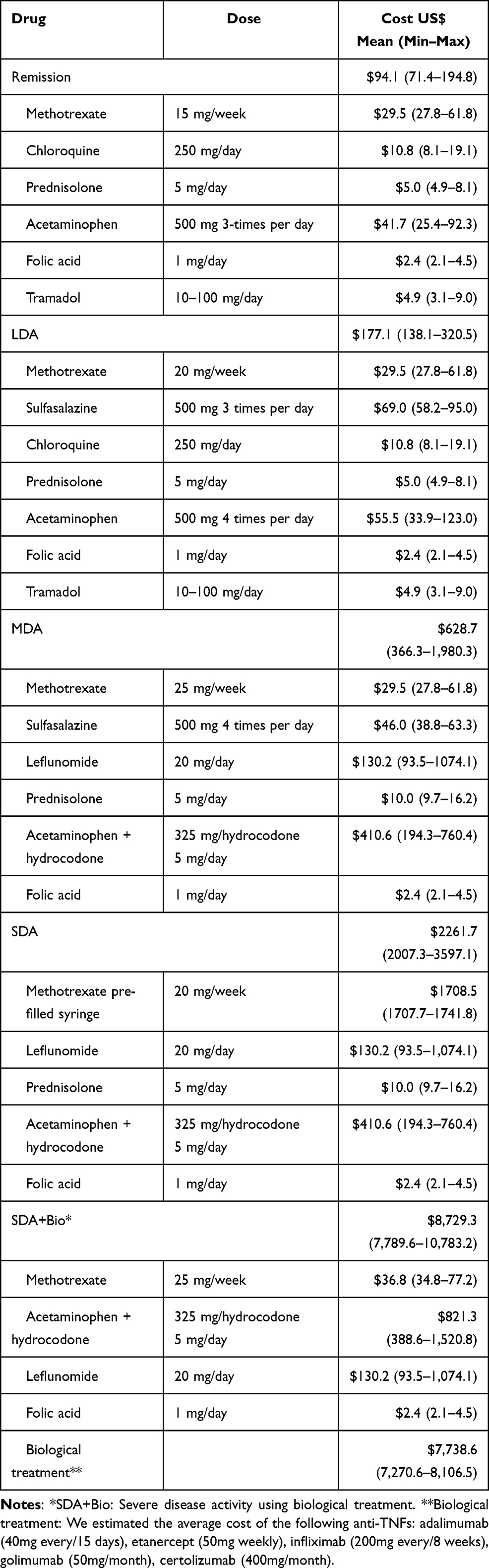 |
Table 3 Annual Costs of RA Treatment by Severity of the Disease at a CoE |
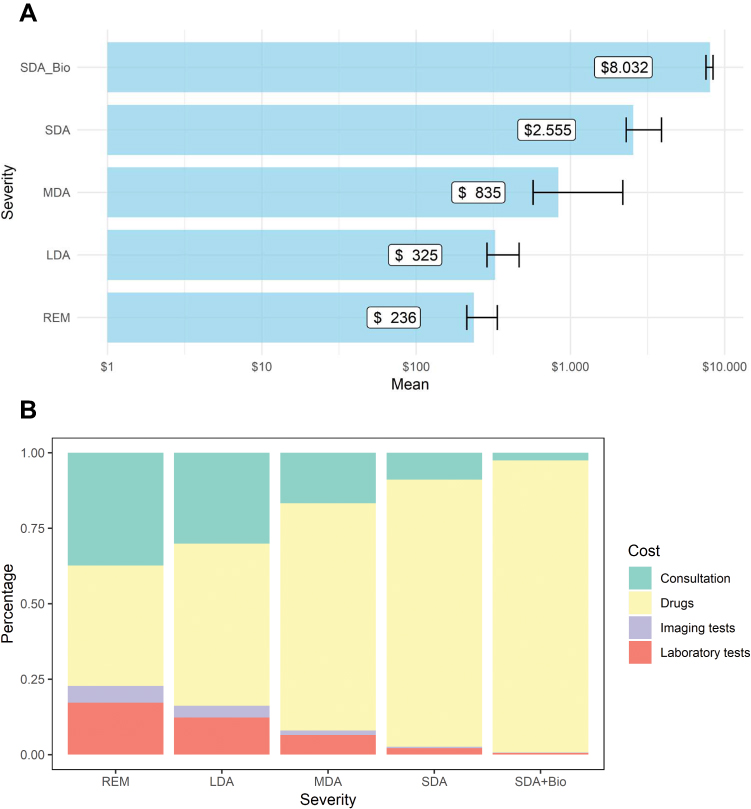 |
Figure 1 Annual costs of caring for a RA patient at a CoE and its percentual distribution. (A) Annual costs of caring for a RA patient. (B) Distribution of the costs of caring for a patient by RA severity. Abbreviations: LDA, low disease activity; MDA, moderate disease activity; REM, remission; SDA, severe disease activity; SDA+Bio, severe disease activity using biological treatment. |
At the start of follow-up (n = 968 patients), 41% were in REM, 17% in LDA, 38% in MDA, and the remaining 4% were in SDA. After 6 and 12 months of care at the CoE, 75% and 82% of the patients were in REM/LDA, respectively. Table 4 shows the cost of treating patients according to the severity of the disease beginning with a cost at baseline of US$612,639 (US$487,978–1,220,160), US$466,634 (US$382,140–870,912) at month six, and US$388,765 (US$321,710–708,476) after a year of follow-up, which implies potential cost-savings of up to US$223,874 per year (Figure 2).
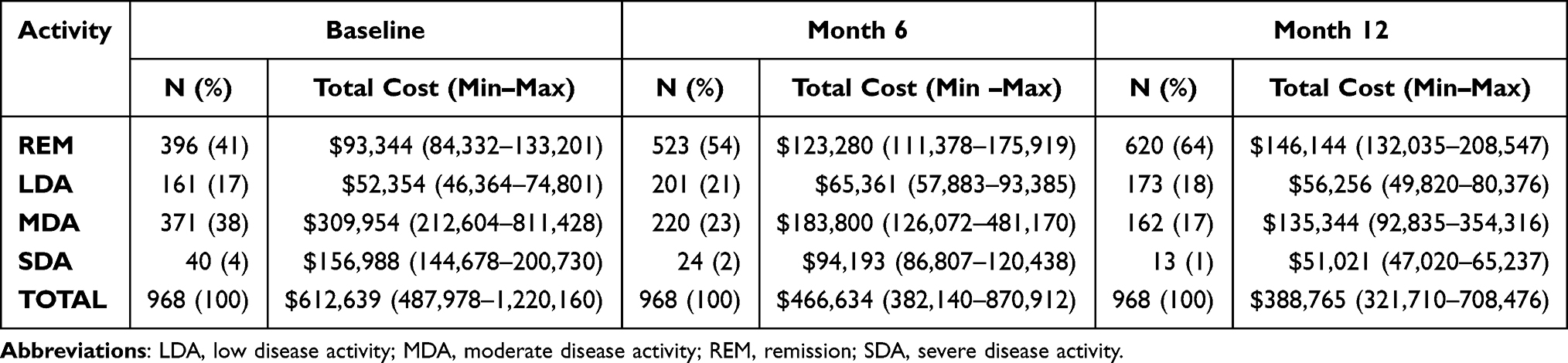 |
Table 4 RA Patient Treatment Costs by Severity of the Disease |
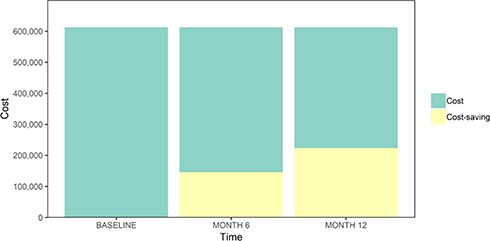 |
Figure 2 Cost-savings related to RA patient care at a CoE for RA. |
Discussion
There are no previous published studies estimating the potential cost-savings of caring for RA patients at a CoE in Colombia. In addition, there are very few studies costing RA by disease activity level from middle-income countries, like those in Latin America.
Clinical and sociodemographic features, such as sex of the cohort, presence of arterial hypertension, and disease duration were similar to those reported in other studies.25–28 Our main finding was that treating the 968 patients at the CoE would save 36.5% in the first year of enrollment, implying cost-savings of US$223,874 per year and US$231.3 per studied patient, equivalent to 87.4% of the monthly minimum wage in Colombia in 2018.29 Our study also suggests that better health results, expressed by comprehensive attention based on T2T strategy, guarantee lower health expenditures; increasing the number of patients in remission and low disease activity (less expensive severity levels), while reducing the number of patients in moderate and severe activity, would lead to a considerable reduction in costs for third-party payers.
Other Latin-American studies have shown significant changes in the evolution of the disease in settings without an integral management care for patients with RA.28,30 A study conducted in Colombia by Machado-Alba28 exhibited how patients receiving cDMARDs and bDMARDs improved the remission rate from 30.1% to 42.9% (an increment of 12.8%). In our study, the remission rate increased from 41% to 64%. This shows that in Colombian rheumatological centers, even without a comprehensive model of PCC that functions under the T2T recommendations, patients will still improve their condition. However, under a CoE model, improvement tends to be much greater, thus a greater potential for cost-saving is plausible. In Colombia, according to the RA patient registry (High Cost of Disease Office or Cuenta de Alto Costo - CAC, in Spanish), on average a patient with RA received three consultations for rheumatology during 2017.12 In contrast, the CoE model will guarantee more frequency of consultations with a rheumatologist, provide the attention of a multidisciplinary team, and assure strict follow-up on laboratories and imaging tests.
In this study, we also estimated direct medical costs of RA according to disease activity. In a meta-analysis carried out in 2018 by Hresko et al, when compared with studies in other countries, it was found that the average direct costs of care including all treatment regimens would be $3,723 (95% CI: 2,408–5,762), and for patients receiving biologic treatment it would be $20,262 (95% CI: 17,480–23,487),31 much higher than those estimated in our study. Also, the level of RA severity is a significant contributor to health care costs and the use of biologic treatment, as was reported in other settings.32
There are strategies to guarantee the efficiency of health systems in the world. Among them are the diagnosis-related groups, Pay for Performance (P4P) and CoE that apply the T2T strategy for RA based on PCC model.33 Previous evidence has shown that involving the patient as an individual with unique needs, concerns and preferences has an important impact on safety, effectiveness and costs.34 Our results prove that the CoE strategy would have great impact in terms of public policies for the treatment of RA in Colombia. By applying this model in our country, we would greatly improve health outcomes, and be even more efficient with health care costs.
This study has some limitations that should be considered. First, we used standard costing, which considered cost of treatment and regulated follow-up of the disease, but do not consider aspects such as treatment adherence. Nevertheless, we think that it is a good estimation of the real cost saved because patients are linked to the CoE, which is not common in a health system where care is as fragmented as it is in Colombia. In this case, health outcomes are improved because there is a strict follow-up depending on the severity levels of the disease. Additionally, it is fair to say this is a conservative estimation of the cost-savings, since the costs shown in the national price lists are the prices and rates on which hospitals and insurance agencies base their negotiations in the country. Another limitation related to standard costing is its inability to account for variability among patients. Standard costing gives a dollar value for the attention an “average” patient receives according to protocol, which changes depending on their health status. To fix this limitation, we reported minimum and maximum costs as a proxy of the uncertainty of the analysis.
Additionally, this study did not consider the costs of adverse effects of treatment. Some estimates suggest that, each year, more than 100,000 patients are hospitalized for nonsteroidal anti-inflammatory drugs (NSAIDs)-related gastrointestinal (GI) complications alone, with direct costs ranging from US$1,800-US$8,500 per patient/hospitalization. Moreover, it has been reported that 16,500 people die annually from these complications. In the elderly, the medical costs of adverse GI events associated with NSAID use likely exceed US$4 billion per year.35
The present study has several advantages too, one is that the costing of the annual follow-up and treatment of RA at the CoE was performed based on national price lists and institutional market price lists, which make the costs representative and comparable to the whole health system.
Cost studies are a central part of the economic assessment of health interventions.36–38They allow the economic quantification of the activities required in preventing, tending, and caring for a disease.36,39 They are essential because they estimate the amount of money that would be saved in the absence of the disease, and which could be directed to other sectors.37 Moreover, they help make informed decisions in public health and they are useful because they allow for obtaining the necessary supplies to carry out future complete economic evaluations of health technologies.36,38 Our study creates new questions and generates new research fields that value the cost-effectiveness of CoE models in the long-term treatment of chronic and high-cost diseases such as RA. One very important question is related to the value of the potential savings that could be obtained by treating the, roughly, 72,000 patients with RA in Colombia12 at a CoE with the T2T approach. Our results give enough evidence to help answer these types of questions.
Statements of Ethical Approval
This study was approved by the Institutional Research Board of Biomab IPS, act 004-25042017. All patients had previously signed informed consent for data use. This study did not represent risks for the patients according to the Resolution 8430 of 1993 of the Ministry of Health of Colombia. All data that could identify a patient were anonymized.
Acknowledgments
We would like to thank Mark Javier Makepeace for editing and reviewing this manuscript for English language.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
Pedro Santos-Moreno reports previous grants from AbbVie, personal fees and non-financial support from Biopas-UCB, Janssen, Pfizer, Bristol, Roche, and personal fees from Lilly. The other authors reported no potential conflicts of interest for this work.
References
1. Nell VPK, Machold KP, Eberl G, Stamm TA, Uffmann M, Smolen JS. Benefit of very early referral and very early therapy with disease-modifying anti-rheumatic drugs in patients with early rheumatoid arthritis. Rheumatology. 2004;43(7):906–914. doi:10.1093/rheumatology/keh199
2. van der Linden MPM, Le Cessie S, Raza K, et al. Long‐term impact of delay in assessment of patients with early arthritis. Arthritis Rheumatol. 2010;62(12):3537–3546. doi:10.1002/art.27692
3. Puchner R, Hochreiter R, Pieringer H, Vavrovsky A. Improving patient flow of people with rheumatoid arthritis has the potential to simultaneously improve health outcomes and reduce direct costs. BMC Musculoskelet Disord. 2017;18(1):7. doi:10.1186/s12891-016-1362-7
4. Hogan DR, Stevens GA, Hosseinpoor AR, Boerma T. Monitoring universal health coverage within the Sustainable Development Goals: development and baseline data for an index of essential health services. Lancet Glob Heal. 2018;6(2):e152–68. doi:10.1016/S2214-109X(17)30472-2
5. Evans DB, Etienne C. Health systems financing and the path to universal coverage. Bull World Health Organ. 2010;88(6):402. doi:10.2471/BLT.10.078741
6. Amaya-Lara JL. Catastrophic expenditure due to out-of-pocket health payments and its determinants in Colombian households. Int J Equity Health. 2016;15(1):182. doi:10.1186/s12939-016-0472-z
7. Castro-Rodríguez A, Machado-Duque ME, Gaviria-Mendoza A, Medina-Morales DA, Álvarez-vera T, Machado-Alba JE. Factors related to excessive polypharmacy (≥15 medications) in an outpatient population from Colombia. Int J Clin Pract. 2018;e13278. doi:10.1111/ijcp.13278
8. Santos-Moreno P, Castañeda O, Garro B, Flores D, Sánchez G, Castro C. From the model of integral attention to the creation of centers of excellence in rheumatoid arthritis. Clin Rheumatol. 2015;34(S1):71–77. doi:10.1007/s10067-015-3017-8
9. Santos-Moreno P, Galarza-Maldonado C, Caballero-Uribe CV, et al. REAL-PANLAR project for the implementation and accreditation of centers of excellence in rheumatoid arthritis throughout Latin America. JCR J Clin Rheumatol. 2015;21(4):175–180. doi:10.1097/RHU.0000000000000247
10. Smolen JS, Aletaha D, Bijlsma JWJ, et al. Treating rheumatoid arthritis to target: recommendations of an international task force. Ann Rheum Dis. 2012;69:631–637. doi:10.1136/ard.2009.123919
11. Smolen JS, Breedveld FC, Burmester GR, et al. Treating rheumatoid arthritis to target: 2014 update of the recommendations of an international task force. Ann Rheum Dis. 2015;1–13.
12. Cuenta de Alto Costo. Situación de la artritis reumatoide en Colombia [Internet]. 2017.
13. Ministerio de Salud y Protección Social. Guía de Práctica Clínica para la detección temprana, diagnóstico y tratamiento de la artritis reumatoide. 2014.
14. Alemao E, Al MJ, Boonen AA, et al. Conceptual model for the health technology assessment of current and novel interventions in rheumatoid arthritis. Nurmohamed M, editor. PLoS One. 2018;13(10):e0205013. doi:10.1371/journal.pone.0205013
15. Santos-Moreno P, Alvis-Zakzuk NJ, Villarreal-Peralta L, Carrasquilla-Sotomayor M, Paternina-Caicedo A, Alvis-Guzmán N. A comprehensive care program achieves high remission rates in rheumatoid arthritis in a middle-income setting. Experience of a Center of Excellence in Colombia. Rheumatol Int. 38(3):499–505. doi:10.1007/s00296-017-3903-2.
16. Drummond MF, Sculpher MJ, Claxton K, Stoddart GL, Torrance GW. Methods for the Economic Evaluation of Health Care Programmes. Oxford university press; 2015:445.
17. Rovira J, Antoñanzas F. Economic analysis of health technologies and programmes. Pharmacoeconomics. 1995;8(3):245–252. doi:10.2165/00019053-199508030-00007
18. Hjelmgren J, Berggren F, Andersson F. Health economic guidelines—similarities, differences and some implications. Value Heal. 2001;4(3):225–250. doi:10.1046/j.1524-4733.2001.43040.x
19. Loras C, Mayor V, Fernández-Bañares F, Esteve M. Study of the standard direct costs of various techniques of advanced endoscopy. Comparison with surgical alternatives. Dig Liver Dis. 2018;50(7):689–697. doi:10.1016/j.dld.2018.03.002
20. Amat O, Soldevila P, Aguilà S Contabilidad y gestión de costes. Profit; 2011.
21. Instituto de Evaluación Tecnológica en Salud-IETS. Manual para la elaboración de evaluaciones económicas en salud. Bogotá - Colombia: Instituto de Evaluación Tecnológica en Salud; 2014.
22. Instituto de Evaluación Tecnológica en Salud. Qué es el IETS. 2018.
23. SISPRO. Sistema Integral de Información de la Protección Social.
24. de la República B. Tasa de cambio representativa del mercado (TRM). Available from: https://www.banrep.gov.co/es/estadisticas/trm.
25. Viegas Brenol C, Mendonça Silva da Chakr R, Pamplona Bueno Andrade N, et al. Daily practice feasibility and effectiveness of treating long-standing rheumatoid arthritis to target with synthetic disease-modifying antirheumatic drugs: a prospective cohort study. Clin Rheumatol. 2015;34(10):1781–1785. doi:10.1007/s10067-015-2915-0
26. Santos-Moreno PI, De La Hoz-valle J, Villarreal L, Palomino A, Sánchez G, Castro C. Treatment of rheumatoid arthritis with methotrexate alone and in combination with other conventional DMARDs using the T2T strategy. A cohort study. Clin Rheumatol. 2015;34(2):215–220. doi:10.1007/s10067-014-2794-9
27. Ling E, Ofer-Shiber S, Goren O, Molad Y. Outcome of patients with rheumatoid arthritis: cross-sectional study of a single-center real-world inception cohort. Isr Med Assoc J. 2013;15(12):758–762.
28. Machado-Alba JE, Ruiz AF, Machado-Duque ME. Effectiveness of treatment with biologic- and disease-modifying antirheumatic drugs in rheumatoid arthritis patients in Colombia. Int J Clin Pract. 2016;70(6):506–511. doi:10.1111/ijcp.12809
29. Ministerio de Trabajo. Decreto número 2552 de 2015. 2015. Available from: https://www.funcionpublica.gov.co/eva/gestornormativo/norma.php?i=67555.
30. Gamboa-Cárdenas RV, Ugarte-Gil MF, Loreto M, et al. Clinical predictors of remission and low disease activity in Latin American early rheumatoid arthritis: data from the GLADAR cohort. Clin Rheumatol. 2019;38(10):2737–2746. doi:10.1007/s10067-019-04618-x
31. Hresko A, Lin T-C, Solomon DH. Medical care costs associated with rheumatoid arthritis in the US: a systematic literature review and meta-analysis. Arthritis Care Res (Hoboken). 2018;70(10):1431–1438. doi:10.1002/acr.23512
32. Baser O, Baser E, Altinbas A, Burkan A. Severity index for rheumatoid arthritis and its association with health care costs and biologic therapy use in Turkey. Health Econ Rev. 2013;3(1):5. doi:10.1186/2191-1991-3-5
33. Lakomek H-J, Krause A. “Treat-to-Target“ (T2T) aus der Sicht der stationären Rheumatologie. Z Rheumatol. 2011;70(8):656–663. doi:10.1007/s00393-011-0765-y
34. Voshaar MJH, Nota I, Van De Laar MAFJ, Van Den Bemt BJF. Patient-centred care in established rheumatoid arthritis. Best Pract Res Clin Rheumatol. 2015;29(4–5):643–663. doi:10.1016/j.berh.2015.09.007
35. Bidaut-Russell M, Gabriel SE. Adverse gastrointestinal effects of NSAIDs: consequences and costs. Best Pract Res Clin Gastroenterol. 2001;15(5):739–753. doi:10.1053/bega.2001.0232
36. Instituto Nacional de Salud - Observatorio Nacional de Salud. Quinto Informe ONS: Carga de enfermedad por enfermedades crónicas no transmisibles y discapacidad en Colombia. (Pág. 160). Bogotá, DC: Imprenta Nacional de Colombia; 2015.
37. Lenz-alcayaga R. Análisis de costos en evaluaciones económicas en salud: aspectos introductorios. 2010;138(Supl2):88–92.
38. Bernal-Aguirre C, Carvajal-Sierra H, Alvis-Zakzuk NJ. Costos económicos de la infección respiratoria aguda en un Municipio de Colombia. Rev La Univ Ind Santander Salud. 2017;49(3):470–477.
39. Rice DP. Estimating the Cost-Of-Illness. Washington, DC: US Department of Health, Education, and Welfare, Public Health Service; 1966.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.