Back to Journals » Infection and Drug Resistance » Volume 16
Ceftazidime/Avibactam, Polymyxin or Tigecycline as a Rescue Strategy for the Treatment of Carbapenem-Resistant Klebsiella pneumoniae in Bloodstream Infection: A Retrospective Cohort Study
Authors Fang Y, Zhong Q, Chen Y, Hang Y, Fang X, Xiao Y, Cao X, Zhu H ![]() , Luo H, Peng S
, Luo H, Peng S ![]() , Gu S
, Gu S ![]() , Li F
, Li F ![]() , Zhu J, Xiong J, Hu L
, Zhu J, Xiong J, Hu L
Received 24 February 2023
Accepted for publication 3 May 2023
Published 12 May 2023 Volume 2023:16 Pages 2963—2971
DOI https://doi.org/10.2147/IDR.S409506
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Youling Fang,1,2 Qiaoshi Zhong,1 Yanhui Chen,1 Yaping Hang,1 Xueyao Fang,1 Yanping Xiao,1 Xingwei Cao,1 Hongying Zhu,3 Hong Luo,1 Suqin Peng,1 Shumin Gu,1 Fuxing Li,1 Junqi Zhu,1 Jianqiu Xiong,4 Longhua Hu1
1Department of Jiangxi Provincial Key Laboratory of Medicine, Clinical Laboratory of the Second Affiliated Hospital of Nanchang University, Nanchang, Jiangxi, People’s Republic of China; 2School of Public Health, Nanchang University, Nanchang, Jiangxi, People’s Republic of China; 3Clinical Laboratory of Ganzhou People’s Hospital, Ganzhou, Jiangxi, People’s Republic of China; 4Department of Nursing, The Second Affiliated Hospital of Nanchang University, Nanchang, Jiangxi, People’s Republic of China
Correspondence: Longhua Hu; Jianqiu Xiong, Email [email protected]; [email protected]
Objective: To analyze the clinical characteristics, outcomes, and risk factors of patients treated with ceftazidime/avibactam, polymyxin, or tigecycline (CPT) compared with those receiving a conventional therapy (CT) (ie, imipenem, levofloxacin, or gentamicin).
Methods: A single-center retrospective cohort study included patients with carbapenem-resistant Klebsiella pneumoniae bloodstream infection (CRKP-BSI) treated at one Chinese tertiary hospital between March 2012 and November 2022 was performed. Clinical characteristics, outcomes, and risk factors of patients treated with CPT or CT were compared. Predictors of 30-day mortality of patients with CRKP-BSI were also analysed in our study.
Results: Among 184 recruited patients with CRKP-BSI, 39.7% (73/184) were treated with CPT, while 60.3% (111/184) were treated with CT. Compared to patients treated with CT, patients treated with CPT had worse conditions, as evidenced by a higher rate of underlying diseases and invasive procedures; however, they also had a better prognosis and lower rates of 14-day treatment failure (p = 0.024). In addition, univariate analysis and multivariate analysis showed that SOFA score [odds ratio (OR) = 1.310, 95% confidence interval (CI) 1.157– 1.483; p < 0.001] and cold weather (OR = 3.658, 95% CI 1.474– 9.081; p = 0.005) were independent risk factors for 30-day mortality.
Conclusion: Compared to CRKP-BSI patients treated with CT, patients treated with CPT had worse conditions but better prognoses. CRKP-BSI occurred more frequently in hot weather; however, higher 30-day mortality was associated with cold weather. A randomized trial is needed to confirm these observational results.
Keywords: carbapenem-resistantKlebsiella pneumoniae, polymyxin, tigecycline, ceftazidime/avibactam, bloodstream infection, hot weather, cold weather
Introduction
Bloodstream infections (BSIs) were strongly associated with mortality, accounting for about 11–38% of infections, due to prolonged hospital stays, invasive medical procedures, and immunosuppression.1 Klebsiella pneumoniae (K. pneumoniae) was one of the major nosocomial pathogens and the second most common pathogen in Enterobacteriaceae bloodstream infections.2 Some studies showed that Klebsiella pneumoniae bloodstream infections (KP-BSIs) account for 6.6–9.9% of all bloodstream infections, with a mortality rate of 20–37%.2–4 With the increasing use of carbapenems in hospitals, the carbapenem-resistant Klebsiella pneumoniae (CRKP) had become an emerging cause of healthcare-associated infections.5 CRKP was widely resistant, often leading to clinical failure even with rescue antimicrobial agents (ie, fluoroquinolones, carbapenems, and aminoglycosides). In addition, although there were many studies showing that combination therapy with multiple in vitro active agents may be superior to monotherapy, the rate of clinical failure remains high.6–8 Because of the few antibiotics available, CRKP was associated with a longer hospital stay and increased mortality.9,10 So it is urged to identify effective treatment strategies for CRKP-BSI.
Recently, ceftazidime/avibactam, polymyxin, or tigecycline, have been proposed as salvage therapy for CRKP infections, whether alone or in combination.11–14 Nevertheless, studies investigating the outcomes and prognosis of these three antibiotics compared with other antibiotics are lacking. Therefore, this study analyzed the clinical characteristics, risk factors, and outcomes of patients treated with ceftazidime/avibactam, polymyxin, or tigecycline (CPT), compared with conventional therapy (CT). In addition, we also analyzed the risk factors of 30-day mortality of carbapenem-resistant Klebsiella pneumoniae bloodstream infection (CRKP-BSI).
Materials and Methods
Study Design and Patients
This retrospective, case–control study was conducted in the clinical laboratory of the Second Affiliated Hospital of Nanchang University from March 2012 to November 2022, which is a comprehensive tertiary hospital with 4000 beds in Jiangxi Province, China. Patients’ clinical information was collected through the Laboratory Information System (LIS) and Hospital Information System (HIS) database. The patient inclusion criteria were: (1) age ≥18 years old; (2) patients infected with CRKP; (3) samples were obtained from peripheral blood; only the first bacteremic episode was included; (4) complete clinical records and data.
Data Collection
Data from LIS and HIS included demographic data (gender, age), symptoms and diagnosis, laboratory and microbiological outcomes, potential diseases and complications, as well as data regarding antimicrobial therapy, clinical outcomes (cured and improved or died), and weather. Age-adjusted Charlson Comorbidity Index (aCCI), Pitt bacteremia score, and Sepsis-related Organ Failure Assessment (SOFA) score were analyzed at the time of BSI onset.
Definitions
Patients with at least one positive blood culture and with at least two symptoms were diagnosed with K. pneumoniae bloodstream infection (KP-BSI): (1) body temperature >38°Cor <36°C; (2) heart rate >90 beats per minute; (3) respiratory rate >20 breaths per minute; (4) the peripheral blood leukocyte >10×109 /L or <4×109 /L. If the first culture-positive sample was collected more than 48 h after hospital admission or within 48 h after discharge from the hospital, it was defined as a hospital-acquired infection; otherwise, the case was considered as community-acquired. Hot weather referred to the three hottest months in local, while cold weather referred to the three coldest months in local. Clinical outcomes included cure, improvement, and failure. If all symptoms and signs of the infection disappeared and no further antibiotic treatment was needed, a clinical cure was considered successful; if the complete or partial resolution of all symptoms and signs of infection occurred but further antibiotic treatment was needed, a clinical improvement was considered; treatment failure was defined as symptoms or signs of infection that persisted or worsened or in case of death.
Antimicrobial Susceptibilities
K. pneumoniae isolates were identified using the VITEK 2 Compact system (bioMérieux, France) or matrix-assisted laser desorption/ionisation time-of-flight mass spectrometry (MALDI-TOF/MS) system (bioMérieux). The antimicrobial resistance of isolates was detected by antimicrobial sensitivity tests using VITEK 2 Compact system and disc diffusion method on the Mueller-Hinton (MH) Agar plates. These antibiotics included ceftriaxone, ciprofloxacin, levofloxacin, tigecycline, amikacin, imipenem, meropenem, ceftazidime/avibactam, piperacillin/tazobactam, amoxicillin/clavulanate, cefoperazone/sulbactam, aztreonam, gentamicin, cefepime, cotrimoxazole, and tobramycin. The antimicrobial susceptibility of tigecycline was interpreted according to Food and Drug Administration (FDA). The antimicrobial susceptibility of other antibiotics was interpreted according to Clinical and Laboratory Standards Institute (CLSI).
Statistical Analysis
Data were analyzed using SPSS software, version 25.0 (IBM Inc., New York, USA). We expressed continuous variables as means ± standard deviations and reported categorical variables as medians and percentages. Student’s t-test and Mann–Whitney U-test were used to evaluate continuous variables. Categorical variables were assessed using the χ2 test or Fisher’s exact test. In order to determine independent risk factors for 30-day mortality, we included potential confounders and variables with a P-value of <0.05 in the univariable analysis into the multivariable regression analysis. P values of <0.05 were considered statistically significant.
Results
Demographic and Clinical Characteristics
A total of 939 cases of K. pneumoniae were isolated from blood culture. Among those, 184 patients with CRKP from blood sources were included in the final analysis. Among 184 patients, 39.7% (73/184) were treated with CPT and 60.3% (111/184) were treated with CT (Figure 1).
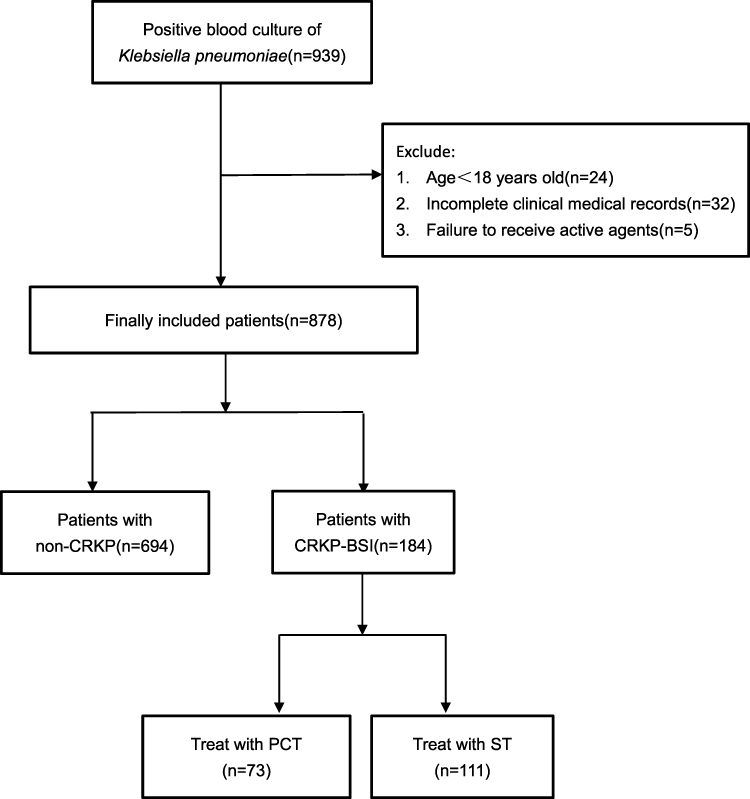 |
Figure 1 Flow chart of patients selected. |
The demographic data of enrolled patients are summarized in Table 1. Of the 184 patients, 131 (71.2%) were male and 53 (28.8%) were female (P = 0.045), and their mean age was 62 years (SD: 15.51). Hospital-acquired infection occurred in 94.6% (174/184) of patients. The most common co-morbidities were hypoproteinaemia (42.4%), followed by kidney disease (41.3%). The proportions of hypoproteinaemia (P = 0.031), hepatic disease (P = 0.013), anemia (P = 0.001), gastrointestinal disease (P = 0.007) and surgery within 3 months (P = 0.012) were higher in the CPT group compared to the CT group. However, there were more patients with biliary tract disease in the CT group than in the CPT group (P = 0.033). The CPT group usually had a better clinical outcome and a lower rate of 14-day treatment failure (P = 0.024). In addition, patients in the CPT group were cured in 90 days and had lower 30-day mortality, although there was no significant difference between the two groups (P > 0.05).
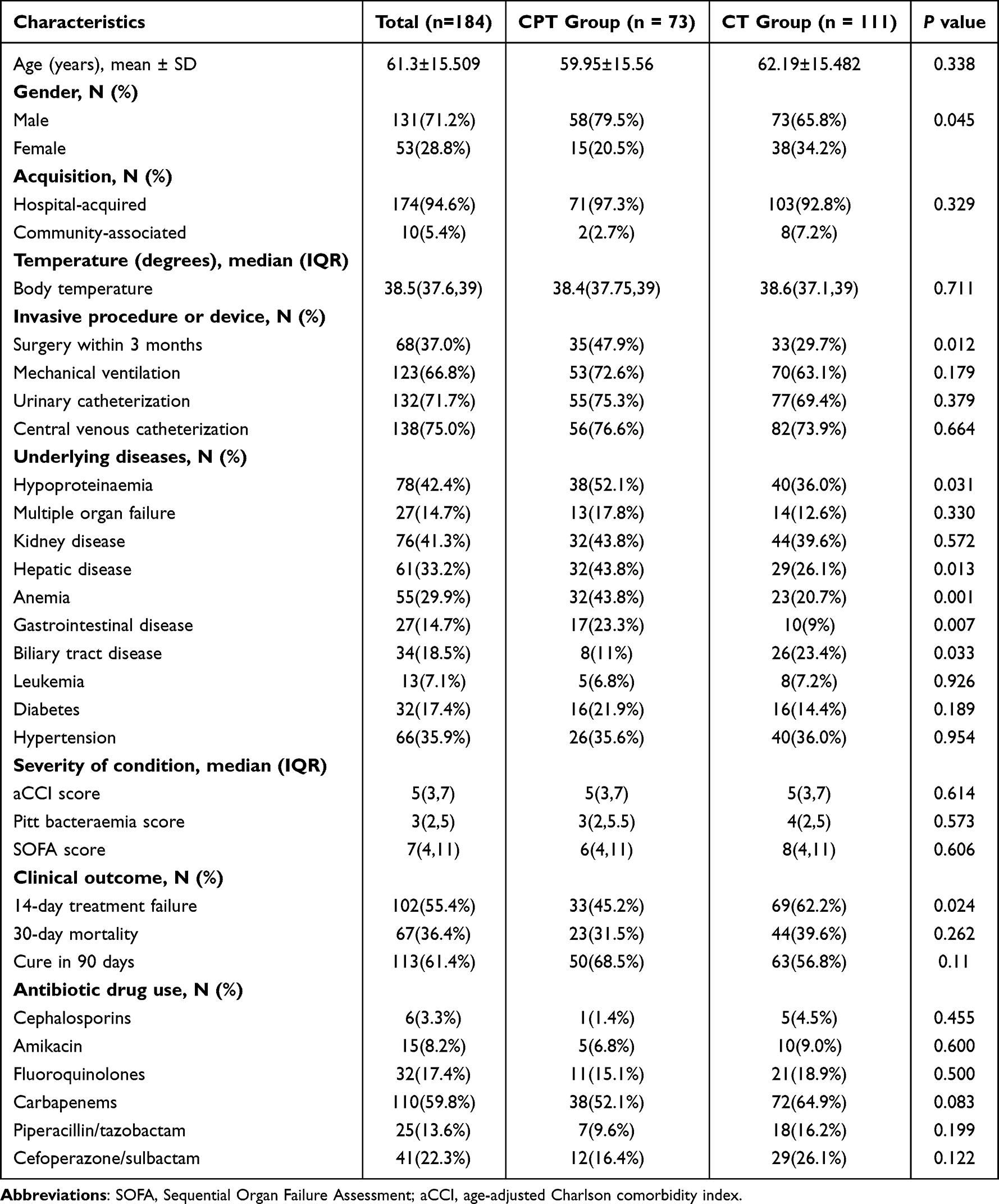 |
Table 1 Demographic and Clinical Characteristics of Patients Treated with CPT and CT |
Antibiotic Resistance and Antibiotic Treatment
The antibiotic resistance of the two groups is shown in Table 2. Among the CPT group, the highest rate of drug resistance was found for ceftriaxone, piperacillin/tazobactam, cefoperazone/sulbactam, imipenem, meropenem and amoxicillin/clavulanate, all of which were 100%, followed by aztreonam (99.1%), and the lowest rate of drug resistance was found for tigecycline (6.8%). The highest rate of drug resistance in the CT group was found for amoxicillin/clavulanate (98.5%), and the lowest drug resistance rate was found for tigecycline (19.1%). The resistance to aztreonam (97.3% vs 88.3%, P = 0.028), gentamicin (78.0% vs 58.5%, P = 0.019), cefepime (95.9% vs 87.3%, P = 0.049), cotrimoxazole (81.5% vs 49.2%, P < 0.001), and tobramycin (79.1% vs 58.3%, P = 0.004) occurred more frequently in CPT group than in CT group.
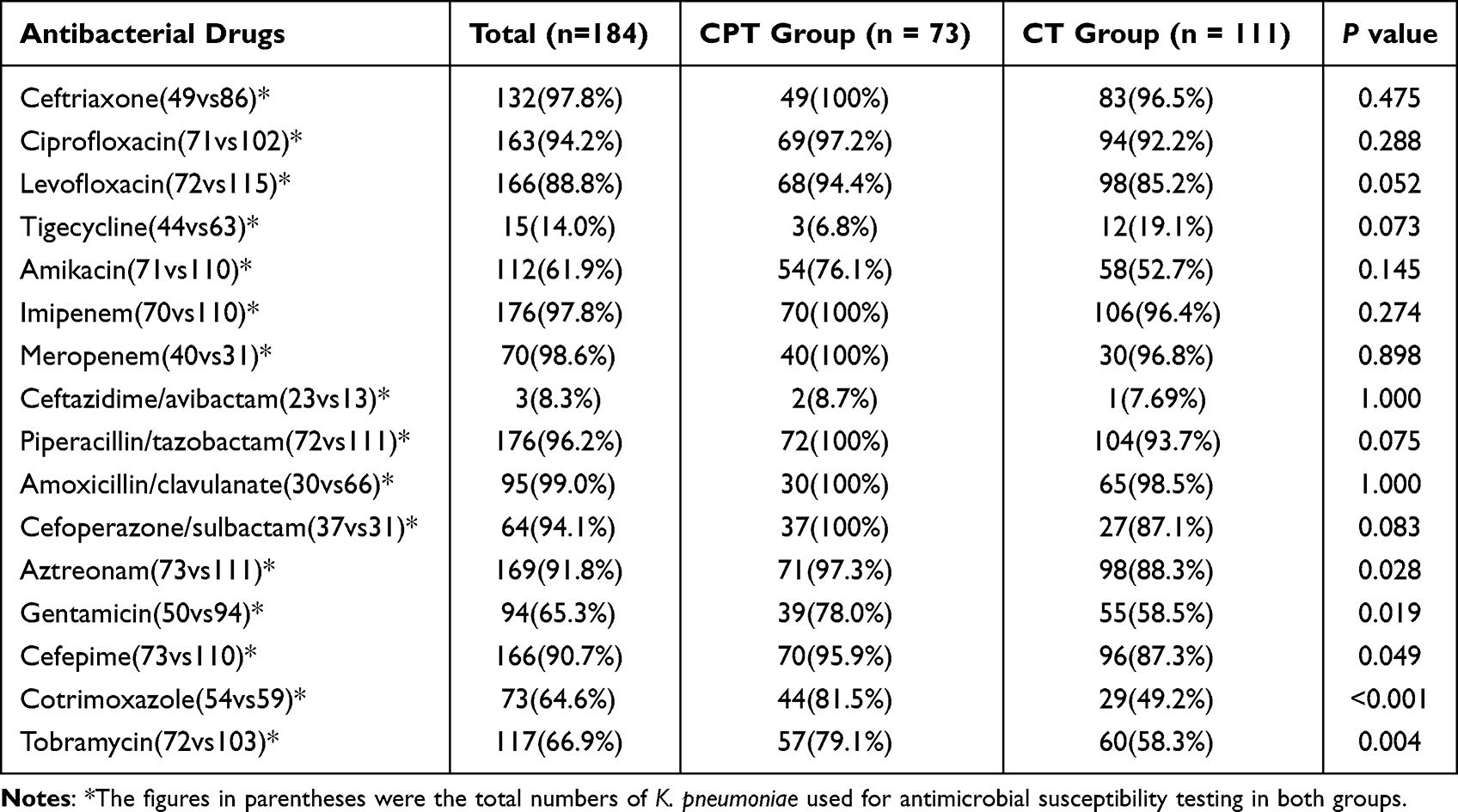 |
Table 2 Antimicrobial Resistance of Patients Treated with CPT and CT |
The antibiotic treatments of the two groups are shown in Table 1. The most commonly used antibiotics were carbapenems, followed by cefoperazone/sulbactam. There was no significant difference in the use of other antibiotics between the two groups (P > 0.05).
Univariate and Multivariate Analysis of 30-Day Mortality
The univariate and multivariate analysis of factors associated with 30-day mortality is summarized in Table 3. The 30-day mortality was 36.4%. CRKP-BSI occurred more frequently in hot weather than in cold weather (25.5% vs 21.2%), although there was no significant difference between the two kinds of weather (P > 0.05). The univariate analysis showed that 30-day mortality was significantly higher in the cold than in hot weather (29.9% vs 16.2%, P = 0.032). Other factors associated with mortality identified in the univariate analysis were multiple-organ failure (P = 0.01), central venous catheterization (P = 0.019), mechanical ventilation (p < 0.001), urinary catheterization (P = 0.036), SOFA score (p < 0.001), and Pitt bacteraemia score (p < 0.001). At the same time, therapy with ceftazidime/avibactam was a protective factor (p = 0.036). After adjusting for confounding factors via logistics regression analysis, risk factors of 30-Day mortality were independently associated with SOFA score (OR = 1.310, 95% CI 1.157–1.483; p < 0.001) and cold weather (OR = 3.658, 95% CI 1.474–9.081; P = 0.005).
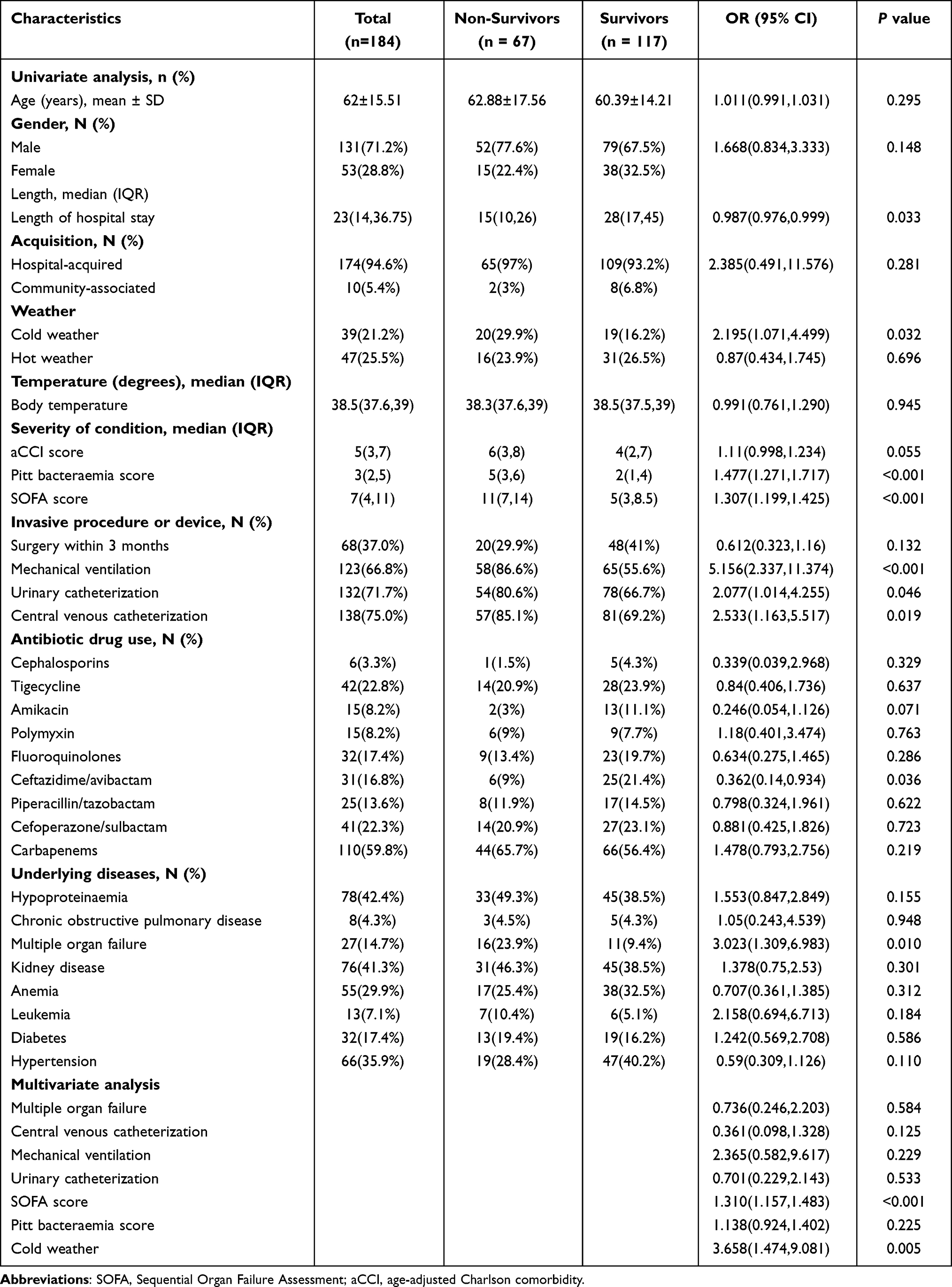 |
Table 3 Univariate and Multivariate Analysis of Factors for Mortality in Patients with CRKP-BSI |
Discussion
CHINET data showed a rapid increase in the prevalence of CRKP in China, from 2.9% in 2005 to 24.2% in 2020.15,16 Currently, ceftazidime/avibactam, polymyxin, and tigecycline are considered as effective treatment strategies for CRKP-BSI. So in this study, we evaluated the clinical and microbiological outcomes of patients treated with CPT compared with those treated with CT. Predictors of 30-day mortality of patients with CRKP-BSI were also analysed in this study.
The mortality of CRKP-BSI varies from 40% to 70%.17–19 The mortality of CRKP-BSI in this study was 36.4%. The increase in mortality might be related to host factors or the delay in appropriate treatment.20 Our study showed that CPT patients had worse conditions than CT patients; CPT patients often presented with diseases and underwent invasive procedures. However, patients in the CPT group had better prognosis, evidenced by a lower rate of 14-day treatment failure and 30-day mortality.
Some studies suggested that ceftazidime-avibactam was superior to other treatment options when treating CRKP.21–23 Studies also indicated that CRKP infections treated with ceftazidime/avibactam were associated with lower mortality rates than previously used drug regimens.22–26 In addition, polymyxin and tigecycline have also been associated with reduced mortality, improving the clinical cure and microbiological eradication rates, especially for those with critical conditions, such as severe sepsis and septic shock.27–30 However, in our study, only ceftazidime/avibactam resulted as a protective factor against 30-day mortality. In addition, some studies have found that patients treated with polymyxin or tigecycline might present side effects (eg, nephrotoxicity and neurotoxicity) and increased resistance during the treatment.31–34 These factors may affect treatment response and reduce survival benefit, which led to a lack of statistically significant association between polymyxin and tigecycline with mortality in the present study.
We also found that drug resistance rates were higher in the CPT group than in the CT group, which might be due to the following reasons: first, patients in the CPT group were in worse condition, and patients with underlying diseases had weak immunity and a long hospital stay, so that they were more likely to be invaded by pathogens. Second, critical patients were treated with higher doses and for a longer time, allowing more time for bacteria to develop resistance.
Patients had a higher incidence rate in hot weather than in cold weather, which was consistent with other literature.35 The optimal growth temperature for K. pneumoniae was >30°C (30°C–35°C). The rising temperature can increase bacterial growth and promote its transport and transfer.36 In addition to increased morbidity, high temperatures also increased antibiotic resistance. Seasonal environmental factors, such as temperature, were the main driving forces for the persistence and proliferation of antibiotic resistance in the environment, which could lead to the exchange of resistance genes or the uptake of genetic material with other bacteria.37,38 At the same time, low temperatures could inhibit microbial growth and enzyme expression.39,40 Interestingly, although the incidence was high in hot weather, the mortality was higher in cold weather. Our univariate and multivariate analysis showed that cold weather was independently associated with the 30-day mortality of CRKP-BSI. Low temperature could increase the incidence rate of complications related to the autonomic nervous system, blood pressure, thermogenesis, inflammatory response, and oxidative stress reaction of patients, thus aggravating the condition of patients.41,42 In addition, increased rates of respiratory infections and diseases in cold weather were also associated with mortality.43 This suggest that we should pay more attention to the patient’s condition and improve the treatment strategies when the weather is cold. Besides, understanding the relationship between weather and CRKP infection is helpful to develop effective control and prevention strategies.
Multiple studies have shown that SOFA can predict mortality in critically ill patients.44–47 It was also found that the SOFA score could be one of the most valuable tools in evaluating the severity of healthcare-associated pneumonia.48 In our study, the SOFA score resulted as one of the independent predictors of mortality in CRKP-BSI.
In summary, critical CRKP-BSI patients were more often treated with ceftazidime/avibactam, polymyxin, or tigecycline antibiotics and had higher survival chances. Ceftazidime/avibactam was the most effective antibiotic, especially for critical patients. Nevertheless, further studies are needed to confirm whether ceftazidime/avibactam, polymyxin, or tigecycline antibiotics can be effectively used to treat CRKP-BSI patients in poor conditions. In addition, we found that CRKP-BSI occurred more commonly in hot weather but was associated with higher mortality in cold weather. These results highlight the importance of studying the weather variation to better understand the epidemic trend of K. pneumoniae bloodstream infections and develop effective control and prevention strategies.
Data Sharing Statement
All the data are from the database of the second affiliated Hospital of Nanchang University. The raw data supporting the conclusions of this manuscript will be made available by the corresponding authors, without undue reservation, to any qualified researcher.
Ethics Statement
Informed consent was acquired from each participant included in the study. This study was approved by the Second Affiliated Hospital of Nanchang University Medical Research Ethics Committee (No. Review-2022-117). Our study complies with the Declaration of Helsinki.
Acknowledgments
This study was supported by a grant from National Natural Science Foundation of China (91200316), the Jiangxi Natural Science Foundation (No.2BAB205066) and the Jiangxi Provincial Department of Science and Technology (20181BBG70030).
Disclosure
The authors declare that they have no conflict of interest.
References
1. Trecarichi EM, Tumbarello M. Antimicrobial-resistant gram-negative bacteria in febrile neutropenic patients with cancer: current epidemiology and clinical impact. Curr Opin Infect Dis. 2014;27(2):200–210. doi:10.1097/QCO.0000000000000038
2. Diekema DJ, Hsueh PR, Mendes RE, et al. The microbiology of bloodstream infection: 20-year trends from the SENTRY antimicrobial surveillance program. Antimicrob Agents Chemother. 2019;63:7. doi:10.1128/AAC.00355-19
3. Marra AR, Wey SB, Castelo A, et al. Nosocomial bloodstream infections caused by Klebsiella pneumoniae: impact of extended-spectrum beta-lactamase (ESBL) production on clinical outcome in a hospital with high ESBL prevalence. BMC Infect Dis. 2006;6:24. doi:10.1186/1471-2334-6-24
4. Xu M, Fu Y, Kong H, et al. Bloodstream infections caused by Klebsiella pneumoniae: prevalence of bla(KPC), virulence factors and their impacts on clinical outcome. BMC Infect Dis. 2018;18(1):358. doi:10.1186/s12879-018-3263-x
5. Gupta N, Limbago BM, Patel JB, Kallen AJ. Carbapenem-resistant Enterobacteriaceae: epidemiology and prevention. Clin Infect Dis. 2011;53(1):60–67. doi:10.1093/cid/cir202
6. Tumbarello M, Trecarichi EM, De Rosa FG, et al. Infections caused by KPC-producing Klebsiella pneumoniae: differences in therapy and mortality in a multicentre study. J Antimicrob Chemother. 2015;70(7):2133–2143. doi:10.1093/jac/dkv086
7. Gutiérrez-Gutiérrez B, Salamanca E, de Cueto M, et al. Effect of appropriate combination therapy on mortality of patients with bloodstream infections due to carbapenemase-producing Enterobacteriaceae (INCREMENT): a retrospective cohort study. Lancet Infect Dis. 2017;17(7):726–734. doi:10.1016/S1473-3099(17)30228-1
8. Tzouvelekis LS, Markogiannakis A, Piperaki E, Souli M, Daikos GL. Treating infections caused by carbapenemase-producing Enterobacteriaceae. Clin Microbiol Infect. 2014;20(9):862–872. doi:10.1111/1469-0691.12697
9. Dautzenberg MJ, Wekesa AN, Gniadkowski M, et al. The association between colonization with carbapenemase-producing Enterobacteriaceae and overall ICU mortality: an observational cohort study. Crit Care Med. 2015;43(6):1170–1177. doi:10.1097/CCM.0000000000001028
10. Gutiérrez-Gutiérrez B, Salamanca E, de Cueto M, et al. A predictive model of mortality in patients with bloodstream infections due to carbapenemase-producing Enterobacteriaceae. Mayo Clin Proc. 2016;91(10):1362–1371. doi:10.1016/j.mayocp.2016.06.024
11. Andrade FF, Silva D, Rodrigues A, Pina-Vaz C. Colistin update on its mechanism of action and resistance, present and future challenges. Microorganisms. 2020;8(11):11. doi:10.3390/microorganisms8111716
12. Wentao N, Guobao L, Jin Z, et al. In vitro activity of minocycline combined with aminoglycosides against Klebsiella pneumoniae carbapenemase-producing K. pneumoniae. J Antibiot. 2018;71(5):506–513. doi:10.1038/s41429-017-0024-9
13. Karlowsky JA, Biedenbach DJ, Kazmierczak KM, Stone GG, Sahm DF. Activity of ceftazidime-avibactam against extended-spectrum- and ampc β-lactamase-producing Enterobacteriaceae collected in the INFORM global surveillance study from 2012 to 2014. Antimicrob Agents Chemother. 2016;60(5):2849–2857. doi:10.1128/AAC.02286-15
14. Shirley M. Ceftazidime-avibactam: a review in the treatment of serious gram-negative bacterial infections. Drugs. 2018;78(6):675–692. doi:10.1007/s40265-018-0902-x
15. Hu F, Guo Y, Yang Y, et al; China Antimicrobial Surveillance Network Study, Group. Resistance reported from China antimicrobial surveillance network (CHINET) in 2018. Eur J Clin Microbiol Infect Dis. 2019;38(12):2275–2281. doi:10.1007/s10096-019-03673-1
16. Hu FP, Guo Y, Zhu DM, et al. Resistance trends among clinical isolates in China reported from CHINET surveillance of bacterial resistance, 2005–2014. Clin Microbiol Infect. 2016;22(Suppl 1):S9–14. doi:10.1016/j.cmi.2016.01.001
17. Ben-David D, Kordevani R, Keller N, et al. Outcome of carbapenem resistant Klebsiella pneumoniae bloodstream infections. Clin Microbiol Infect. 2012;18(1):54–60. doi:10.1111/j.1469-0691.2011.03478.x
18. Borer A, Saidel-Odes L, Riesenberg K, et al. Attributable mortality rate for carbapenem-resistant Klebsiella pneumoniae bacteremia. Infect Control Hosp Epidemiol. 2009;30(10):972–976. doi:10.1086/605922
19. Patel G, Huprikar S, Factor SH, Jenkins SG, Calfee DP. Outcomes of carbapenem-resistant Klebsiella pneumoniae infection and the impact of antimicrobial and adjunctive therapies. Infect Control Hosp Epidemiol. 2008;29(12):1099–1106. doi:10.1086/592412
20. Amit S, Mishali H, Kotlovsky T, Schwaber MJ, Carmeli Y. Bloodstream infections among carriers of carbapenem-resistant Klebsiella pneumoniae: etiology, incidence and predictors. Clin Microbiol Infect. 2015;21(1):30–34. doi:10.1016/j.cmi.2014.08.001
21. Karakonstantis S, Kritsotakis EI, Gikas A. Treatment options for K. pneumoniae, P. aeruginosa and A. baumannii co-resistant to carbapenems, aminoglycosides, polymyxins and tigecycline: an approach based on the mechanisms of resistance to carbapenems. Infection. 2020;48(6):835–851. doi:10.1007/s15010-020-01520-6
22. Tumbarello M, Trecarichi EM, Corona A, et al. Efficacy of ceftazidime-avibactam salvage therapy in patients with infections caused by Klebsiella pneumoniae carbapenemase-producing K. pneumoniae. Clin Infect Dis. 2019;68(3):355–364. doi:10.1093/cid/ciy492
23. Shields RK, Nguyen MH, Chen L, et al. Ceftazidime-avibactam is superior to other treatment regimens against carbapenem-resistant Klebsiella pneumoniae bacteremia. Antimicrob Agents Chemother. 2017;61(8). doi:10.1128/AAC.00883-17
24. van Duin D, Lok JJ, Earley M, et al. Colistin versus ceftazidime-avibactam in the treatment of infections due to carbapenem-resistant Enterobacteriaceae. Clin Infect Dis. 2018;66(2):163–171. doi:10.1093/cid/cix783
25. Jorgensen SCJ, Trinh TD, Zasowski EJ, et al. Real-world experience with ceftazidime-avibactam for multidrug-resistant gram-negative bacterial infections. Open Forum Infect Dis. 2019;6(12):ofz522. doi:10.1093/ofid/ofz522
26. Tsolaki V, Mantzarlis K, Mpakalis A, et al. Ceftazidime-avibactam to treat life-threatening infections by carbapenem-resistant pathogens in critically ill mechanically ventilated patients. Antimicrob Agents Chemother. 2020;64(3). doi:10.1128/AAC.02320-19
27. Chang T, Tu YK, Lee CT, et al. Effects of polymyxin B hemoperfusion on mortality in patients with severe sepsis and septic shock: a systemic review, meta-analysis update, and disease severity subgroup meta-analysis. Crit Care Med. 2017;45(8):e858–e864. doi:10.1097/CCM.0000000000002362
28. Vincent JL, Laterre PF, Cohen J, et al. A pilot-controlled study of a polymyxin B-immobilized hemoperfusion cartridge in patients with severe sepsis secondary to intra-abdominal infection. Shock. 2005;23(5):400–405. doi:10.1097/01.shk.0000159930.87737.8a
29. Cantaluppi V, Assenzio B, Pasero D, et al. Polymyxin-B hemoperfusion inactivates circulating proapoptotic factors. Intensive Care Med. 2008;34(9):1638–1645. doi:10.1007/s00134-008-1124-6
30. Zha L, Pan L, Guo J, French N, Villanueva EV, Tefsen B. Effectiveness and safety of high dose tigecycline for the treatment of severe infections: a systematic review and meta-analysis. Adv Ther. 2020;37(3):1049–1064. doi:10.1007/s12325-020-01235-y
31. Doi Y, Paterson DL. Carbapenemase-producing Enterobacteriaceae. Semin Respir Crit Care Med. 2015;36(1):74–84. doi:10.1055/s-0035-1544208
32. Ezadi F, Ardebili A, Mirnejad R, Kraft CS. Antimicrobial susceptibility testing for polymyxins: challenges, issues, and recommendations. J Clin Microbiol. 2019;57(4):4. doi:10.1128/JCM.01390-18
33. Band VI, Weiss DS, Coers J. Heteroresistance: a cause of unexplained antibiotic treatment failure? PLoS Pathog. 2019;15(6):e1007726. doi:10.1371/journal.ppat.1007726
34. Tian Y, Zhang Q, Wen L, Chen J, Van Tyne D. Combined effect of polymyxin B and tigecycline to overcome heteroresistance in carbapenem-resistant Klebsiella pneumoniae. Microbiol Spectr. 2021;9(2):e0015221. doi:10.1128/Spectrum.00152-21
35. Kito Y, Kuwabara K, Ono K, et al. Seasonal variation in the prevalence of gram-negative bacilli in sputum and urine specimens from outpatients and inpatients. Fujita Med J. 2022;8(2):46–51. doi:10.20407/fmj.2021-003
36. Ratkowsky DA, Olley J, McMeekin TA, Ball A. Relationship between temperature and growth rate of bacterial cultures. J Bacteriol. 1982;149(1):1–5. doi:10.1128/jb.149.1.1-5.1982
37. Walsh TR, Weeks J, Livermore DM, Toleman MA. Dissemination of NDM-1 positive bacteria in the New Delhi environment and its implications for human health: an environmental point prevalence study. Lancet Infect Dis. 2011;11(5):355–362. doi:10.1016/S1473-3099(11)70059-7
38. Warnes SL, Highmore CJ, Keevil CW, Bassler B. Horizontal transfer of antibiotic resistance genes on abiotic touch surfaces: implications for public health. mBio. 2012;3(6). doi:10.1128/mBio.00489-12
39. Ducey TF, Vanotti MB, Shriner AD, Szogi AA, Ellison AQ. Characterization of a microbial community capable of nitrification at cold temperature. Bioresour Technol. 2010;101(2):491–500. doi:10.1016/j.biortech.2009.07.091
40. Cui D, Li A, Zhang S, et al. Microbial community analysis of three municipal wastewater treatment plants in winter and spring using culture-dependent and culture-independent methods. World J Microbiol Biotechnol. 2012;28(6):2341–2353. doi:10.1007/s11274-012-1041-2
41. Cai J, Meng X, Wang C, et al. The cold effects on circulatory inflammation, thrombosis and vasoconstriction in type 2 diabetic patients. Sci Total Environ. 2016;568:271–277. doi:10.1016/j.scitotenv.2016.06.030
42. Hintsala H, Kenttä TV, Tulppo M, et al. Cardiac repolarization and autonomic regulation during short-term cold exposure in hypertensive men: an experimental study. PLoS One. 2014;9(7):e99973. doi:10.1371/journal.pone.0099973
43. Liu Y, Guo Y, Wang C, et al. Association between temperature change and outpatient visits for respiratory tract infections among children in Guangzhou, China. Int J Environ Res Public Health. 2015;12(1):439–454. doi:10.3390/ijerph120100439
44. Vincent JL, de Mendonça A, Cantraine F, et al. Use of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units: results of a multicenter, prospective study. Working group on “sepsis-related problems” of the European society of intensive care medicine. Crit Care Med. 1998;26(11):1793–1800. doi:10.1097/00003246-199811000-00016
45. Jentzer JC, Bennett C, Wiley BM, Murphree DH, Keegan MT, Barsness GW. Predictive value of individual sequential organ failure assessment sub-scores for mortality in the cardiac intensive care unit. PLoS One. 2019;14(5):e0216177. doi:10.1371/journal.pone.0216177
46. Karakike E, Kyriazopoulou E, Tsangaris I, Routsi C, Vincent JL, Giamarellos-Bourboulis EJ. The early change of SOFA score as a prognostic marker of 28-day sepsis mortality: analysis through a derivation and a validation cohort. Crit Care. 2019;23(1):387. doi:10.1186/s13054-019-2665-5
47. Innocenti F, Tozzi C, Donnini C, et al. SOFA score in septic patients: incremental prognostic value over age, comorbidities, and parameters of sepsis severity. Intern Emerg Med. 2018;13(3):405–412. doi:10.1007/s11739-017-1629-5
48. Asai N, Watanabe H, Shiota A, et al. Could qSOFA and SOFA score be correctly estimating the severity of healthcare-associated pneumonia? J Infect Chemother. 2018;24(3):228–231. doi:10.1016/j.jiac.2017.10.004
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Poor Glycemic Control in Carbapenem-Resistant Klebsiella pneumoniae Infections: Impact on Epidemiological Features, Mortality Risks, and Polymyxin Resistance
Wang Q, Yan T, Ma C, Teng X, Shen C, Wang N, Yu K, Chu W, Zhou Q, Liu Z
Infection and Drug Resistance 2025, 18:647-660
Published Date: 1 February 2025
A Tentative Clinical Study: Colistin Combined with Ceftazidime/Avibactam in the Treatment of Carbapenem-Resistant Gram-Negative Bacilli Infection

Zhang R, Zheng Z, Lu Y, Shi K, Lin Z, Tang S, Shao Z, Yang X, Liu J
Infection and Drug Resistance 2025, 18:3977-3991
Published Date: 9 August 2025