Back to Journals » Infection and Drug Resistance » Volume 15
Ceftazidime/Avibactam and Other Commonly Used Antibiotics Activity Against Enterobacterales and Pseudomonas aeruginosa Isolated in Poland in 2015–2019
Authors Zalas-Więcek P, Prażyńska M, Pojnar Ł, Pałka A, Żabicka D ![]() , Orczykowska-Kotyna M, Polak A, Możejko-Pastewka B
, Orczykowska-Kotyna M, Polak A, Możejko-Pastewka B ![]() , Głowacka EA
, Głowacka EA ![]() , Pieniążek I, Pawlik M, Grys M
, Pieniążek I, Pawlik M, Grys M ![]() , Bogiel M
, Bogiel M ![]()
Received 4 December 2021
Accepted for publication 19 February 2022
Published 25 March 2022 Volume 2022:15 Pages 1289—1304
DOI https://doi.org/10.2147/IDR.S344165
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Patrycja Zalas-Więcek,1 Małgorzata Prażyńska,1 Łukasz Pojnar,2 Anna Pałka,2 Dorota Żabicka,3 Monika Orczykowska-Kotyna,3 Aleksandra Polak,3 Barbara Możejko-Pastewka,4 Ewa Anna Głowacka,4 Izabela Pieniążek,5 Małgorzata Pawlik,5 Maciej Grys,5 Monika Bogiel4
1Department of Microbiology, Ludwik Rydygier Collegium Medicum; Department of Clinical Microbiology, University Hospital No. 1, Bydgoszcz, Poland; 2Department of Microbiology, University Hospital, Cracow, Poland; 3Department of Epidemiology and Clinical Microbiology, National Medicines Institute, Warsaw, Poland; 4Pfizer Polska Sp. z o.o., Warsaw, Poland; 5Arcana Institute, a Certara Company, Cracow, Poland
Correspondence: Monika Bogiel, Pfizer Polska sp. z o.o., Żwirki i Wigury 16B, Warszawa, 02-092, Poland, Tel +48 885557081, Fax +48 223356111, Email [email protected]
Purpose: Infections caused by resistant Gram-negative bacteria are becoming increasingly common and now pose a serious public health threat worldwide, because they are difficult to treat due to few treatment options and they are associated with high morbidity and mortality. The combination of ceftazidime with the beta-lactamase inhibitor avibactam – seems to be the right choice in this situation. The aim of the study was to evaluate the activity of ceftazidime/avibactam and other commonly used antibiotics against Enterobacterales and Pseudomonas aeruginosa strains isolated within last years in Poland.
Patients and Methods: This study analyzed the antibiotic susceptibility of 1607 Enterobacterales isolates and 543 nonfermenting P. aeruginosa strains collected between 2015 and 2019 in 4 medical laboratories participating in the ATLAS (Antimicrobial Testing Leadership And Surveillance) program in Poland. Unduplicated clinically significant Enterobacterales and P. aeruginosa strains were collected from patients with respiratory, skin and musculoskeletal, genitourinary, abdominal, bloodstream or other infections (ear, eye).
Results: The ceftazidime/avibactam combination demonstrates the highest activity against Enterobacterales (98.9%), in both adults and children, including strains presenting MDR (multidrug-resistant) (97.5%) and ESBL (extended spectrum β-lactamase) (96.3%) phenotypes. The activity of ceftazidime/avibactam increased to 100% when only MBL (metallo-β-lactamase)-negative subset of Enterobacterales was considered. This combination also achieved the second highest activity result (89.3%) after colistin in P. aeruginosa, including isolates of MDR (65.9%) and carbapenem-resistant (CR) phenotypes (54.8%). When MBL-positive isolates were excluded, susceptibility rate of P. aeruginosa increased to 94.7%. It is worth to note that susceptibility of the examined P. aeruginosa strains to ceftazidime/avibactam was very high in children (93.3%), especially in a pediatric intensive care unit (94.2%).
Conclusion: Enterobacterales and P. aeruginosa included in this analysis presented high susceptibility rates to ceftazidime/avibactam. Ceftazidime/avibactam showed the highest activity against Enterobacterales strains among all antibiotics studied, both for the total population as well as for MDR phenotype and ESBL phenotype. Ceftazidime/avibactam also achieved the second highest activity result against P. aeruginosa strains (including MDR and CR phenotypes). These results are much higher when excluding MBL-positive isolates that exhibit intrinsic resistance to ceftazidime/avibactam.
Keywords: ceftazidime/avibactam, drug resistance, Gram-negative rods, MDR, ESBL, carbapenem resistance
Introduction
Gram-negative multidrug-resistant (MDR) organisms, defined as resistant to at least one agent in three or more drug classes, cause significant morbidity and mortality, prolonged hospitalization, and increased costs compared with infections caused by susceptible organisms. Infections caused by this group of bacteria require the immediate introduction of effective antimicrobial therapy.1,2 Antimicrobial resistance of Gram-negative rods can result from a variety of mechanisms, however, production of beta-lactamases is one of the most common mechanisms of resistance observed in this group of bacteria.
Bacteria, such as: Escherichia coli, Klebsiella pneumoniae or Pseudomonas aeruginosa have varying pathogenic potential. However, any of these bacteria can be responsible for a severe infection, that is refractory to treatment with previously known therapeutic options.3 The World Health Organization (WHO) has listed the main priorities for the pharmaceutical industry in the search for antibiotics against the currently most resistant pathogens, in particular carbapenem-resistant Enterobacterales (CRE) and Pseudomonas spp.4 CRE has been also described as an “urgent threat”, a term formally used to describe the Centers for Disease Control and Prevention’s (CDC) highest level of concern to human health. MDR P. aeruginosa is classified as a “serious threat” to human health with resistance rates on the rise.1 The diversity of resistance mechanisms in P. aeruginosa make them difficult to eliminate from the hospital environment.5
In Poland, a high prevalence of β-lactamase-producing and carbapenem-resistant Gram-negative bacteria is observed. Moreover, Poland, together with Portugal and Slovakia, is one of the countries where a statistically significant increase in carbapenem resistance has been recorded in recent years.6 In 2015, Gram-negative Enterobacterales and non-fermentative rods were the etiological factor of 35.7% of nosocomial infections in Poland. The main species causing these infections were E. coli (37.0% of isolates) and K. pneumoniae (36.4% of isolates). Of particular concern, is the high ratio of MDR strains. Gram-negative, non-fermentative strains were the cause of 14.9% of nosocomial infections in Poland, and P. aeruginosa had the highest proportion among them (47.7%).7
One of the antibiotics available in Poland with the most extensive registered indications and activity against MDR Gram-negative strains is ceftazidime/avibactam. This antibiotic is a combination of a well-known third-generation, broad-spectrum cephalosporin (used for years for numerous indications) with a new beta-lactamase inhibitor. Avibactam effectively inactivates class A (ESBLs [Extended-spectrum beta-lactamases] and KPCs - K. pneumoniae carbapenemases), class C (cephalosporinases; AmpCs), and some class D (such as OXA-48 - oxacillinases) β-lactamases.8,9 Ceftazidime/avibactam is indicated in adults and pediatric patients aged 3 months and older for the treatment of complicated intra-abdominal infection (cIAI), complicated urinary tract infection (cUTI), including pyelonephritis, hospital-acquired pneumonia (HAP), including ventilator associated pneumonia (VAP) and is used for the treatment of adult patients with bacteremia that occurs in association with, or is suspected to be associated with, any of the infections listed above. This antibiotic is also indicated for the treatment of infections due to aerobic Gram-negative organisms in adults and pediatric patients aged 3 months and older with limited treatment options.4,10
The aim of the study was to compare the in vitro activity of the ceftazidime/avibactam and the most commonly used antibiotics in Poland against Enterobacterales and P. aeruginosa, using isolates collected by Polish centers participating in the ATLAS (Antimicrobial Testing Leadership and Surveillance) program between 2015 and 2019.
Materials and Methods
Bacterial Isolates
The data presented in this paper has been obtained as part of the ATLAS program, strictly with the project’s recommendations. The isolated strains were identified locally and a predefined number of selected bacterial species were collected by each participating center. Isolates were accepted into the study regardless of antimicrobial susceptibility. They were shipped to the central reference laboratory of International Health Management Associates (IHMA) for the further analysis. Non-duplicate, clinically significant Enterobacterales and P. aeruginosa strains were collected from patients with respiratory tract, skin and musculoskeletal tissue, genitourinary tract, intra-abdominal, bloodstream or other (ear, eye) infections by 4 centers located in Poland. A total of 1607 isolates of Enterobacterales (Citrobacter spp. n=94, Enterobacter spp. n=216, E. coli n=482, Klebsiella spp. n=572, Morganella spp. n=43, Proteus spp. n=103, Providencia spp. n=34, Raoultella spp. n=4, Serratia spp. n=59) and 543 P. aeruginosa strains were collected between 2015 and 2019. A large proportion of isolates (66.3% of Enterobacterales and 63.9% of P. aeruginosa) was collected from adults and approximately 40% were from elderly (>60 years) patients. Most isolates (70.9% of Enterobacterales and 67.4% of P. aeruginosa) were from patients located in wards that were not classified as intensive care units (ICU).
The predominant Enterobacterales and P. aeruginosa isolates sources were respiratory (24.8% vs 40.3%), genitourinary (27.6% vs 22.7%) and skin or musculoskeletal (23.4% vs 26.3%). Demographic information recorded for each isolate included specimen source, patient age and type of hospital setting.
Antimicrobial Susceptibility Testing and Screening for β-Lactamase Genes
Identification of the isolated strains to the species level were confirmed by the central reference laboratory (IHMA) by mass spectrometry, using MALDI-TOF technique (matrix-assisted laser desorption/ionization time-of-flight) (Bruker Biotyper MALDI-TOF, Bruker Daltonics, Billerica, MA, USA). MIC (minimum inhibitory concentration) assessments were performed by IHMA using broth microdilution method, in accordance with CLSI (Clinical Laboratory Standards Institute) guidelines (CLSI 2018).11 MIC values were interpreted using breakpoints according to European Committee on Antimicrobial Susceptibility Testing (EUCAST Clinical Breakpoint Tables v. 11.0), where available.
The percent susceptibility (% S) and, if applicable, susceptible with increased exposure (% I) strains, if any, and the minimum and maximum MIC values were analyzed. MIC90 values were determined for the antibiotics and chemotherapeutics tested, ie, the lowest concentration of the substances that inhibits the growth of 90% of the strains tested.
Avibactam was tested at a fixed concentration of 4 mg/L in combination with doubling dilutions of ceftazidime. According to EUCAST clinical breakpoints for carbapenems, imipenem MICs were interpreted using different values for Morganellaceae only and for Enterobacterales except Morganellaceae. Isolates naturally resistant to this antibiotic were excluded from the analysis for colistin. For tigecycline, EUCAST 11.0 recommendations have been applied. MDR was defined as resistance to at least one agent in three or more drug classes: aminoglycosides (amikacin, gentamicin), β-lactam/β-lactamase inhibitor combinations (piperacillin/tazobactam), monobactams (aztreonam), cephalosporins (cefepime, ceftazidime, ceftazidime/avibactam, ceftolozane/tazobactam), carbapenems (doripenem, imipenem, meropenem), glycylcyclines (tigecycline), fluoroquinolones (levofloxacin) and polymyxins (colistin).12
Isolates classified as DTR were defined as those with MICs above the susceptibility breakpoint for cefepime, ceftazidime, imipenem, meropenem, levofloxacin and ciprofloxacin.
Isolates were screened for the presence of genes encoding clinically relevant β-lactamases: carbapenemases (KPC, GES [Guiana extended-spectrum], NDM - New Delhi metallo-β-lactamase, IMP [Imipenemase], VIM - Verona integron-encoded metallo-β-lactamase, OXA-48-like), ESBLs (SHV, CTX-M, VEB), OSBLs [original-spectrum β-lactamase] (TEM and SHV) and plasmid-mediated AmpC β-lactamases (AmpC, CMY, DHA). MBL-positive isolates were identified as those with genes encoding NDM, IMP and VIM enzyme.
The presence of β-lactamase genes was determined using multiplex polymerase chain reaction (PCR) assays and sequencing according to Lob et al13 and Nichols et al.14 All detected β-lactamase genes were amplified using flanking primers and sequenced, and sequences were compared against publicly available databases.
Rates of isolates susceptible to ceftazidime/avibactam of subsets with genes encoding MBLs (MBL-positive) and when MBL-positive isolates were excluded (MBL-negative) were also determined.
Results
Enterobacterales
Susceptibility to ceftazidime/avibactam was assessed for 1523 strains including:
- 674 (44.3%) MDR isolates,
- 434 (28.5%) producing ESBL, and
- 23 (1.5%) CRE (carbapenem resistant Enterobacterales) isolates.
MIC values for ceftazidime/avibactam are shown in Figure 1 and Supplementary Table S1.
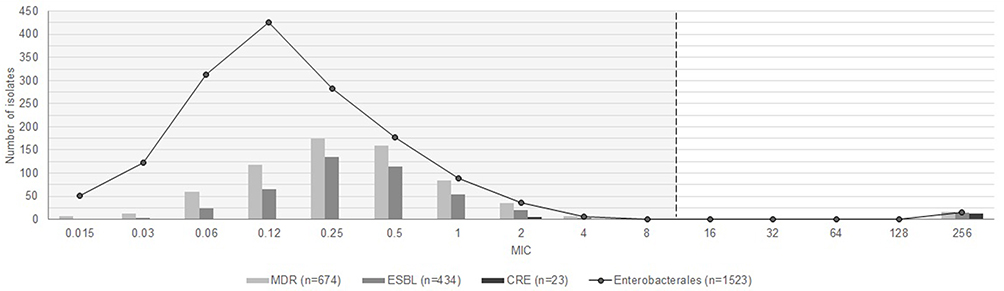 |
Figure 1 Ceftazidime/avibactam MIC distribution for Enterobacterales (n=1523) by phenotype. The dashed line shows the breakpoint for ceftazidime/avibactam according to EUCAST (EUCAST Clinical Breakpoint Tables v. 11.0). 17 isolates with MIC above the breakpoint was observed, including 1 strain with MIC90 = 64 µg/mL and 16 strains with MIC90 = 256 µg/mL; all of them were MDR strains, including 16 ESBL producers and 12 CRE. |
Almost all Enterobacterales strains tested (98.9%) were susceptible to ceftazidime/avibactam (MIC90 = 0.5 μg/mL). A similar high percentage (98.2%) of susceptible strains was found for tigecycline (MIC90 = 2 μg/mL). The high activity was observed also for doripenem (MIC90 = 0.25 µg/mL), imipenem (MIC90 = 1 µg/mL) and meropenem (MIC90 = 0.12 µg/mL). Most isolates (97.0%) were also susceptible to colistin (MIC90 = 1 µg/mL). The lowest susceptibility of this group of strains was found for aztreonam and levofloxacin. Detailed data on antibiotic susceptibility of Enterobacterales strains are presented in Table 1. When only MBL-negative isolates of Enterobacterales were considered the activity of ceftazidime/avibactam increased substantially up to 100% (MIC90 = 0.5 µg/mL) (Table 2).
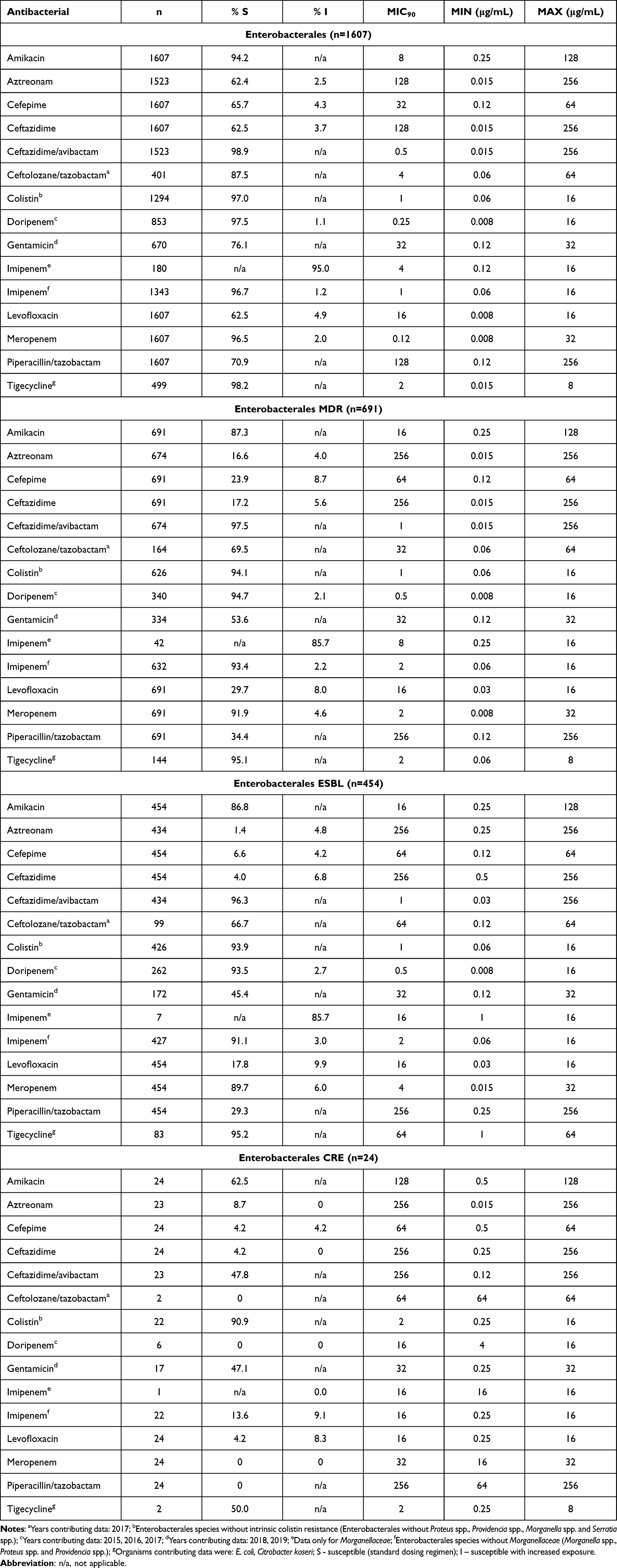 |
Table 1 In vitro Activity of Ceftazidime/Avibactam and Other Commonly Used Antibiotics Tested Against 1607 Enterobacterales Isolates Collected from 2015 to 2019 |
 |
Table 2 Susceptibility to Ceftazidime/Avibactam for MBL-Positive and MBL-Negative Subsets of Enterobacterales |
In general, ceftazidime/avibactam demonstrated the highest antibacterial activity compared to all other antibiotics tested against Enterobacterales strains. Susceptibility rates were similar in each age groups (Supplementary Table S2 and Figure S1). The percentage of susceptibility to ceftazidime/avibactam was superior for children (99.2%), as well as for adults (98.7%), especially elderly patients - 61+ (99.0%). In the elderly patients the highest susceptibility of CRE strains (61.5%) was observed. Very high susceptibility rates for ceftazidime/avibactam were observed also for patients admitted to the intensive care units: 99.2% for adults and 100% for pediatric patients.
Approximately two-thirds of the MDR (65.3%), ESBL-positive Enterobacterales (65.2%) and CRE (66.7%) were isolated from non-ICU patients.
The most common sources of resistant isolates were genital/urinary (MDR 29.8%, ESBL 32.2%, CRE 41.7%) and respiratory (MDR 26.8%, ESBL 29.5%, CRE 25.0%) tract. K. pneumoniae isolates were found to be the most prevalent species of those classified as MDR (46.0%), ESBL (67.2%) and CRE (62.5%). Other frequently occurring species were: E. coli (20.7% of MDR, 18.3% of ESBL and 8.3% of CRE isolates) and Enterobacter cloacae (12.7% of MDR and 5.1% of ESBL).
With respect to the antibiotics included in the analysis, most multidrug-resistant (MDR) Enterobacterales strains were susceptible to ceftazidime/avibactam (observed susceptibility was 97.5% (MIC90 = 1 μg/mL)). Relatively high susceptibility rates were also observed for tigecycline, doripenem, colistin, imipenem and meropenem. Susceptibility ratio was the lowest for aztreonam and ceftazidime (Table 1).
The susceptibility rate among the subset of ESBL-positive Enterobacterales strains was the highest for ceftazidime/avibactam (96.3% susceptible, MIC90 = 1 μg/mL). Most of these strains were susceptible to tigecycline, colistin, doripenem and imipenem. Less than tenth of strains were susceptible to aztreonam and ceftazidime (Table 1).
Ceftazidime/avibactam showed reduced activity (47.8% susceptible) against 23 CRE isolates. This result is explained by the observation that 52.2% of the meropenem resistant isolates were MBL-positive. CRE strains had the highest susceptibility for colistin (90.9% susceptibility, MIC90 = 2 μg/mL).
Table 3 shows the in vitro activity of ceftazidime/avibactam and other commonly used antibiotics against subsets of Enterobacterales isolates, that were molecularly characterized for β-lactamase genes. Ceftazidime/avibactam inhibited 100% of KPC-2, VEB, OXA-48 and plasmid-mediated AmpC-positive isolates, approximately 98% of SHV-OSBL, TEM-OSBL and CTX-M strains. In children, 100% of SHV-OSBL, TEM-OSBL and CTX-M strains were susceptible to ceftazidime/avibactam. Ceftazidime/avibactam was poorly active (5.6%) against isolates carrying metallo-β-lactamases (VIM, NDM); only tigecycline, colistin and amikacin retained activity against majority of MBL-positive isolates (Tables 2 and 3).
 |
Table 3 In vitro Activity of Ceftazidime/Avibactam and Other Commonly Used Antibiotics Tested Against Enterobacterales Isolates (n=1607) Collected from 2015 to 2019, Stratified by Genome (Ambler Classification of β-Lactamases) |
Among 23 isolates of non-susceptible to meropenem Enterobacterales (CRE), most presented more than one resistance mechanism. 14 of isolates were identified as carbapenemase-producing, while in 21 of 23 strains enzymes other than carbapenemases were found: CTX-M (n=17), SHV (n=15) and TEM (n=8). Ceftazidime/avibactam displayed activity against CRE isolates which meropenem-non-susceptibility was conferred primarily by serine carbapenemases: KPC-2 (n=1) and OXA-48 (n=1). A total of 12 CRE isolates identified as MBL were resistant to ceftazidime/avibactam and including NDM (n=8) and VIM (n=4). Among analyzed strains the most frequent producers of MBLs were K. pneumoniae (n=6) and E. cloacae (n=3).
In this study, a total number of 17 isolates of Enterobacterales resistant to ceftazidime/avibactam were observed (Table 2). All of them were MBL, including NDM-1 (n=7), NDM-5 (n=1), VIM-1 (n=7), VIM-4 (n=1) and VIM-44 (n=1). They were simultaneously resistant to patterns including 6–10 different antibiotics. Among them, 15 isolates showed the coexistence of MBL and other resistance mechanism (ESBL or OSBL).
The most frequent resistant bacteria were Klebsiella spp. and Enterobacter spp. strains. The antibiotic with the highest susceptibility outcome among ceftazidime/avibactam-resistant Enterobacterales isolates was colistin (82.4% susceptibility).
Pseudomonas aeruginosa
Susceptibility to ceftazidime/avibactam was assessed for 523 strains including:
- 164 (31.4%) MDR isolates,
- 96 (18.4%) DTR (difficult-to-treat) isolates, and
- 93 (17.8%) CR (carbapenem-resistant) isolates.
A detailed summary of MIC values is shown in Figure 2 and Supplementary Table S3.
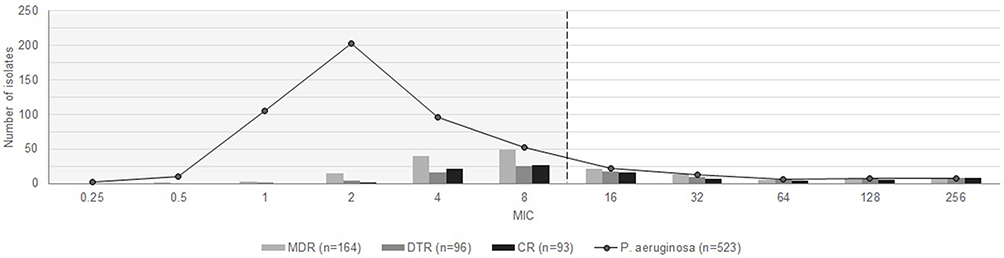 |
Figure 2 Ceftazidime/avibactam MIC distribution for P. aeruginosa (n=523) by phenotype. The dashed line shows the breakpoint for ceftazidime/avibactam according to EUCAST (EUCAST Clinical Breakpoint Tables v. 11.0). 56 isolates with MIC above the breakpoint was observed, among them 56 were MDR, 48 - DTR and 42 - CR. |
High proportion of P. aeruginosa strains tested (89.3%) were susceptible to ceftazidime with avibactam (MIC90 = 16 μg/mL). It was the second highest antibiotic activity among all analyzed in this study (Table 4). When MBL-positive isolates were removed from this latter set, the activity of ceftazidime/avibactam increased spectacularly to 94.7% (MIC90 = 8 μg/mL) (Table 5).
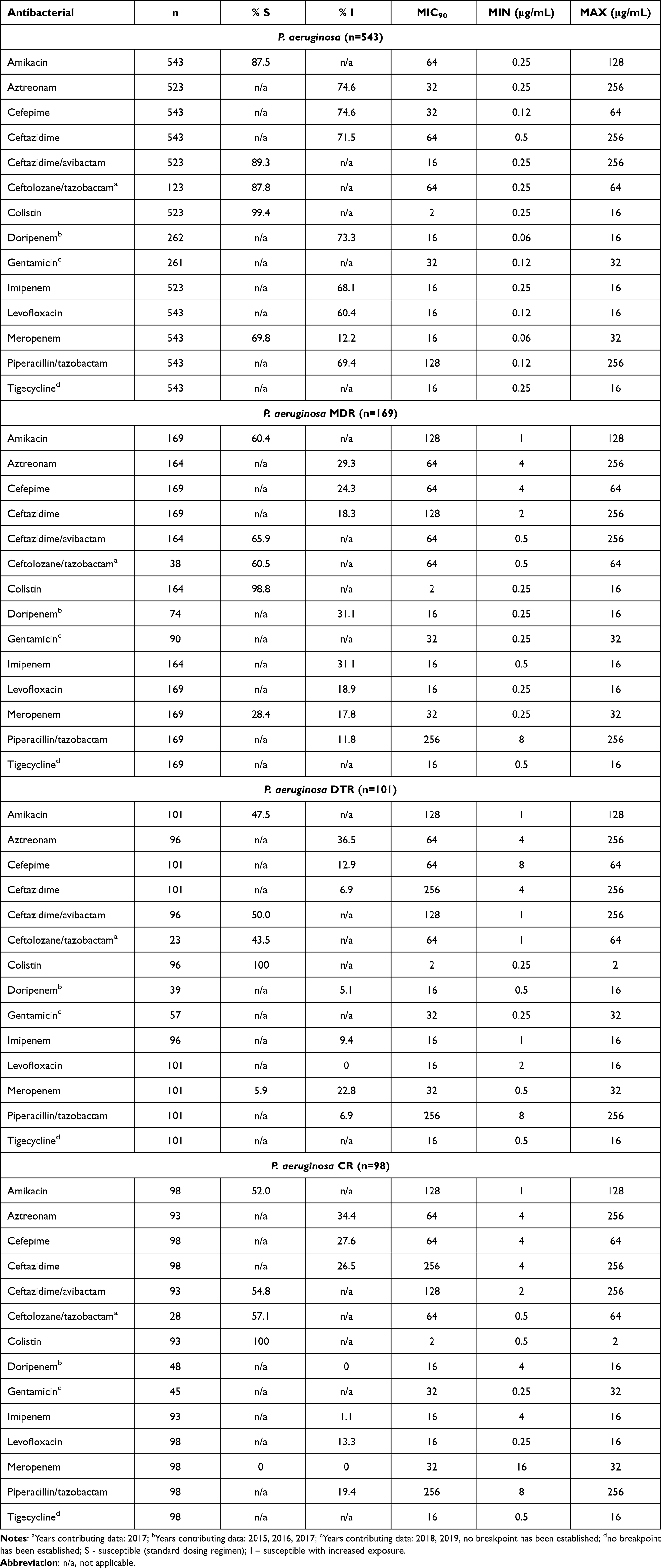 |
Table 4 In vitro Activity of Ceftazidime/Avibactam and Other Commonly Used Antibiotics Tested Against 543 Pseudomonas aeruginosa Isolates Collected from 2015 to 2019 |
 |
Table 5 Susceptibility to Ceftazidime/Avibactam for MBL-Positive and MBL-Negative Subsets of P. aeruginosa |
The highest percentage of susceptible strains (99.4%) was found for colistin (MIC90 = 2 μg/mL). 87.8% of the isolates (MIC90 = 64 µg/mL) were susceptible to ceftolozane/tazobactam (data limited to one year), 87.5% were susceptible to amikacin (MIC90 = 64 µg/mL) and 82.0% (including 12.2% susceptible with increased exposure) to meropenem (MIC90 = 16 µg/mL). P. aeruginosa strains were classified as susceptible only with increased exposure to the following antibiotics: aztreonam, cefepime, ceftazidime, doripenem, imipenem, levofloxacin and piperacillin/tazobactam (susceptibility range: 60.4–74.6%). Detailed data on antibiotic susceptibility of P. aeruginosa strains are presented in Table 4.
Some differences in P. aeruginosa susceptibility to ceftazidime/avibactam was observed between age groups (Figure 3 and Supplementary Table S4). The percent susceptibility was highest for children (93.3%), specifically in a pediatric intensive care unit (94.2%). For adults this value was 86.9% (and 86.7% in adult intensive care unit).
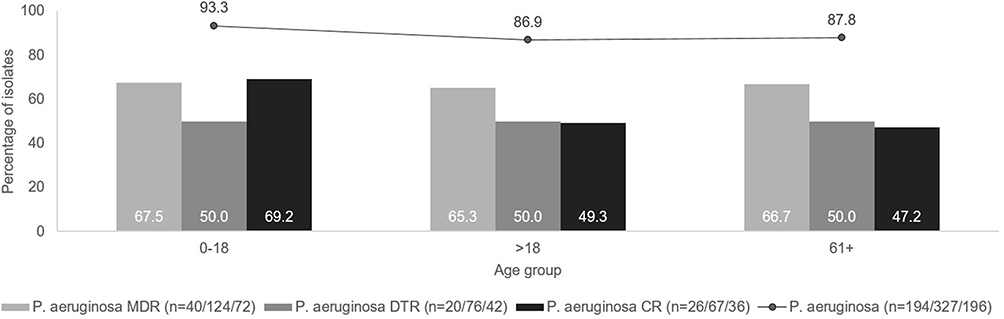 |
Figure 3 Antimicrobial susceptibility (P. aeruginosa) to ceftazidime/avibactam stratified by age. |
More than a half of the MDR (53.8%), DTR (56.4%), and CR (52.0%) isolates of P. aeruginosa were obtained from patients who were treated in non-intensive care units. The most common sources of isolates were the respiratory tract (52.5% of MDR, 56.4% of DTR, 60.2% of CR), genitourinary tract (15.4% of MDR, 12.9% of DTR, 12.2% of CR) and skin and musculoskeletal tissue (17.8% of MDR, 11.9% of DTR, 8.2% of CR).
Overall, 65.9% of MDR P. aeruginosa strains were susceptible to ceftazidime/avibactam (MIC90 = 64 μg/mL). Ceftazidime/avibactam remained the second most effective agent, after colistin (98.8% susceptibility, MIC90 = 2 μg/mL), regarding MDR P. aeruginosa. The percentages of isolates susceptible to ceftolozane/tazobactam (60.5% susceptibility, MIC90 = 64 µg/mL; data limited) and amikacin (60.4% susceptibility, MIC90 = 128 µg/mL) were slightly lower than the percentage of susceptibility to ceftazidime/avibactam observed for these strains. Only 46.2% of strains were susceptible to meropenem (in this 17.8% susceptible with increased exposure).
One-half of DTR P. aeruginosa strains were susceptible to ceftazidime/avibactam (MIC90 = 128 μg/mL). Analyzed DTR strains had the highest susceptibility for colistin (100% susceptibility, MIC90 = 2 μg/mL). Only 5.9% of DTR strains were susceptible to meropenem in standard dosing regimen, and 22.8% - with increased exposure.
Out of the CR P. aeruginosa strains, 54.8% (69.2% for children and 49.3% for adults) were susceptible to ceftazidime/avibactam. CR strains had the highest susceptibility for colistin (100% susceptibility, MIC90 = 2 μg/mL). 57.1% of isolates were susceptible to ceftolozane/tazobactam (data limited) and 52.0% of isolates were susceptible to amikacin.
In most cases, P. aeruginosa resistance was probably caused by non-enzymatic mechanisms or coexisting several resistance mechanisms. There were 35 isolates of P. aeruginosa that were screened for β-lactamase genes. Of these, 32 isolates were identified as MBLs (VIM-1, VIM-2, VIM-16, IMP-1). MBLs of the VIM type were the most frequently identified carbapenemases (84.4%). Ceftazidime/avibactam showed reduced activity against isolates carrying MBLs (6.3% susceptibility). These subsets of P. aeruginosa strains were susceptible for colistin (100% susceptibility).
Among 93 of non-susceptible to carbapenems/meropenem P. aeruginosa (CR P. aeruginosa), 30 isolates were identified as carbapenemase-producing (MBL-positive: VIM-1 (n=1), VIM-16 (n=1), VIM-2 (n=23), IMP-1 (n=5)), while 3 of 93 were found to be ESBLs belonging to the Ambler class A (GES-1 (n=1), VEB-9 (n=2)). 64.5% of isolates (n=60) contained non-enzymatic resistance mechanisms.
A total of 56 ceftazidime/avibactam-resistant P. aeruginosa isolates (10.7% of all isolates) were identified in this study (Table 5). All of them were simultaneously resistant to patterns including 5–11 different antibiotics. Among ceftazidime/avibactam-non-susceptible P. aeruginosa, 41.1% of isolates (n=23) contained non-enzymatic resistance mechanisms; 30 isolates were identified as carbapenemase-producing (VIM-2 was the most common carbapenemases, n=23) and 3 as non-carbapenemase-producing.
Discussion
According to recent estimates based on data from EARS-Net, more than 670,000 infections due to antibiotic-resistant bacteria occur annually in the EU/EEA and about 33,000 people die directly as a result of these infections. The associated costs to the healthcare systems of EU/EEA countries amount to approximately €1.1 billion.15 Infections caused by resistant Gram-negative bacteria are becoming increasingly common and are now a serious public health threat worldwide, as they are difficult to treat and are associated with high morbidity and mortality rates.16 According to the EARS-Net data for 2019, the most commonly reported bacterial species was E. coli (44%), followed by K. pneumoniae (11%) and P. aeruginosa (6%). In EU/EEA countries carbapenem resistance was prevalent in P. aeruginosa, at a higher ratio than in K. pneumoniae. The widespread of beta-lactamases conferring resistance to carbapenem has left physicians and patients with very few treatment options. The combination of ceftazidime with the beta-lactamase inhibitor - avibactam appears to be a promising therapeutic option.
In this study, we report in vitro antimicrobial susceptibility rates for ceftazidime/avibactam and other commonly used antibiotics to a collection of clinical isolates of Enterobacterales and P. aeruginosa from Poland. Susceptibility to ceftazidime/avibactam was highest for all Enterobacterales isolates, and similar susceptibility rates were observed for MDR and ESBL phenotypes. Nearly 99% of the strains tested were sensitive to this combination. This high activity was also observed regardless of age group and in patients admitted to the ICU. The results reported in our study are similar to the susceptibility rates observed for ceftazidime/avibactam in Enterobacterales isolates collected across Europe between 2012 and 2016 in the INFORM study. In this study also ceftazidime/avibactam was most effective against all Enterobacterales (98% susceptibility).17 This trend continued in Kaye et al16 another multinational study that evaluated the in vitro activity of ceftazidime/avibactam and comparators against Enterobacterales isolates from Central Europe and Israel in 2014–2017 and 2018. The susceptibility rates of Enterobacterales to ceftazidime/avibactam were highest in Central Europe (≥99%) and in Poland (almost 100%). Our study, with a susceptibility rate of almost 99% to ceftazidime/avibactam, is consistent with the sustained trend of high activity of this antibiotic combination observed over the years in Central Europe and Poland. Moreover, ceftazidime/avibactam achieved similar high activity in an American 4-year study by Sader et al1 where it inhibited 99.9% of all Enterobacterales.1
In our analysis, 28% of Enterobacterales isolates were identified as ESBL producers and 44% as MDR isolates. Ceftazidime/avibactam achieved the highest activity against them with susceptibility of 96.3% and almost 97.5%, respectively. K. pneumoniae isolates were among the most abundant organisms (46% of MDR and 67% of ESBL isolates) in these phenotypes. The same trend of high ceftazidime/avibactam susceptibility is maintained in the study by Kristof et al18 based on Central Europe, where MDR Enterobacterales had a susceptibility of almost 99% in Poland and 98% in all included countries. Similar results were obtained in the USA according to Hirsch et al, where ceftazidime/avibactam showed the highest activity against ESBL Enterobacterales with 92% susceptibility.19 The above confirms the consistently high activity of ceftazidime/avibactam against this group of bacteria.
According to our analysis, 47.8% of meropenem-resistant isolates (CRE) were susceptible to ceftazidime/avibactam, which was the third highest susceptibility result. This result is explained by the observation that 52% of the meropenem-resistant isolates were MBL-positive, which have innate resistance to this antibiotic combination. Among CRE isolates, most had more than one resistance mechanism: 61% of isolates were identified as carbapenemase-producing (14.3% susceptible) and 91% as non-carbapenemase-producing (47.6% susceptible). In the study by Spiliopoulou et al18 that examined Enterobacterales collected worldwide from 2015 to 2017 as part of the surveillance program INFORM, a total of 1460 meropenem non-susceptible isolates were collected and 73% of them were susceptible to ceftazidime/avibactam. This is due to the fact that only 27% of the isolates were MBL-positive, whereas this rate was almost double in our study. Among the isolates identified as carbapenemase-positive and MBL-negative or carbapenemase-negative and MBL-negative, susceptibility to ceftazidime/avibactam was highest (almost 100% and 96%, respectively).20 In our study, MBL-negative and carbapenemase-positive MBL-negative Enterobacterales isolates had similar susceptibility (100%), which consisted of 100% susceptibility of KPC−2, VEB, OXA-48, and plasmid-mediated AmpC-positive isolates and about 98% susceptibility of SHV-OSBL, TEM-OSBL, and CTX-M strains.
According to our analysis, ceftazidime/avibactam was the antibiotic with the second highest susceptibility outcome against P. aeruginosa among all antibiotics analyzed (89.3% susceptible), just after colistin. The susceptibility rate for ceftazidime/avibactam increased to 94.7% when only MBL-negative isolates of P. aeruginosa were considered. Ceftazidime/avibactam also retained the second highest activity among all antibiotics, just after colistin, in the MDR phenotype and third in CR phenotype. However, colistin due to its potential nephrotoxicity and neurotoxicity has limited use in its intravenous form. This antibiotic is mainly used as a rescue therapy in the treatment of life-threatening infections21 but according to the IDSA guidance colistin should be considered only as an alternate for treating DTR-P. aeruginosa cystitis.22
A similar trend of activity to P. aeruginosa was confirmed by Kristof et al16 (Central Europe and Israel, 2014–2018). The susceptibility rates of P. aeruginosa to ceftazidime/avibactam were second highest in Central Europe (≥92%) and Poland (92%).18 Our study with a susceptibility rate of almost 90% to ceftazidime/avibactam is consistent with the sustained trend of high activity of this antibiotic combination observed over years in Central Europe and Poland. In the study by Sader et al1 an American 4-year study, ceftazidime/avibactam also achieved the second highest activity against P. aeruginosa isolates among all agents. Ceftazidime/avibactam showed potent activity (97% susceptible), including MDR isolates (87% susceptible), which was higher than in our study. However, the study does not report the percentage of MBL-positive isolates which might affect the susceptibility to ceftazidime/avibactam. In the study INFORM, based on data from 2012 to 2016, ceftazidime/avibactam (92% susceptibility) was the second most effective agent against isolates of P. aeruginosa. The susceptibility of MDR isolates was ≤54% to all agents except colistin (95% susceptible) and ceftazidime/avibactam (68%). A subset of P. aeruginosa isolates was identified as ESBL-positive, and less than 10% of them were susceptible to all agents except ceftazidime/avibactam or colistin.23
In our study, the susceptibility of P. aeruginosa strains to ceftazidime/avibactam was high in children (93.3%), especially in a pediatric intensive care unit (94%). This was lower in adults (>18) with susceptibility of 86.9% and in patients over 61 years of age with susceptibility of 87.8%. Susceptibility rates decreased significantly with age for all agents except colistin. In the study by Sader et al24 based on data from INFORM from 2011 to 2015, ceftazidime/avibactam achieved very high activity against isolates from pediatric patients with susceptibility of 99%. Ceftazidime/avibactam activity against 6209 P. aeruginosa isolates from adult patients (≥18 years old) was lower, with susceptibility of 97%.
Among meropenem-resistant P. aeruginosa strains identified in our study, 54.8% of isolates were susceptible to ceftazidime/avibactam. The analysis showed that 65% of CR P. aeruginosa likely had a non-enzymatic resistance mechanism.
In the study by Sader et al1, ceftazidime/avibactam retained the second highest activity against P. aeruginosa isolates that were not susceptible to meropenem with 55% susceptibility, which is a similar result to our study. In the study INFORM, based on data from 2012 to 2016, 2975 isolates were non-susceptible to meropenem, in which no β-lactamase was detected by PCR screening. The susceptibility rate for ceftazidime/avibactam for this subgroup was 88%.23
According to the study by Nichols et al,14 based on data from INFORM from 2012 to 2014, the percentage of susceptibility to ceftazidime/avibactam among meropenem-non-susceptible isolates was 72%, of which 15.6% MBL-positive. This susceptibility increased to 85% when isolates with MBL genes were excluded. This result is much higher than in our study, where 55% of isolates were susceptible to ceftazidime/avibactam. The likely cause of this difference is the high proportion of MBL-positive isolates in our analysis (32%) showing innate resistance to this antibiotic combination.
Importantly, from the prevalence point of view, most of the strains analyzed in our study, including resistant ones, were isolated outside the ICU (Enterobacterales - 70.9%/CRE - 66.7%; P. aeruginosa - 67.4%/CR - 52.0%). A similar observation was made by Gill et al, in the study based on ERACE-PA Global Surveillance Program (2019–2021), stating that it might have an impact on appropriate empiric therapy for the non-ICU patient population, where early treatment active against carbapenem-resistant strains should be considered.25 Due to the involvement of the Central Laboratory in the study, the data obtained are of high quality, but there are some limitations to the current analysis. These limitations include: no information on prior antibiotic therapy, hospitalizations, and nursing home stays in patients from whom material was acquired. In addition, the specified number of isolates was collected from each center, so our observations of susceptibility rates cannot be interpreted as epidemiologic reports and the data for some antibiotics cover only a few years of the period studied. The material for the study also came from only four Polish centers, so the data may not be representative of the whole country. These factors may influence the results obtained.
This publication is consistent with the concept of antibiotic stewardship, which aims to optimize antimicrobial therapy in hospitalized patients to ensure cost-effective therapy and improve patient outcomes while curbing bacterial resistance. Relatively high rates of MDR and carbapenem-resistant strains demonstrate the need for continued surveillance to identify regional and local trends in antimicrobial resistance.
Conclusion
In conclusion, susceptibility rates to ceftazidime/avibactam in Poland appear to be high among the isolates of Enterobacterales and P. aeruginosa collected in this analysis. Ceftazidime/avibactam showed the highest activity against Enterobacterales strains among all antibiotics studied, equally for the total population, MDR phenotype and ESBL phenotype. Ceftazidime/avibactam also achieved the second highest activity result against P. aeruginosa strains, including MDR and CR phenotypes. These results are much higher after exclusion of MBL-positive isolates showing intrinsic resistance to ceftazidime/avibactam.
Our observations support the persistence of high ceftazidime/avibactam activity against pathogenic strains of Enterobacterales and P. aeruginosa, including those carrying different types of antibiotic resistance.
Abbreviations
AmpC, ampicillinase C; ATLAS, Antimicrobial Testing Leadership and Surveillance; CDC, Center for Disease Control and Prevention; cIAI, complicated intra-abdominal infections; CLSI, Clinical Laboratory Standards Institute; CR, carbapenem resistant; CRE, carbapenem resistant Enterobacterales; cUTI, complicated urinary tract infections; DBO, diazabicyclooctanes; DTR, difficult-to-treat; ESBL, extended spectrum β-lactamase; EUCAST, European Committee at Antimicrobial Susceptibility Testing; GES, Guiana extended-spectrum; HAP, hospital-acquired pneumonia; HGT, horizontal gene transfer; IHMA, International Health Management Associates;, IMP, Imipenemase; KPC, Klebsiella pneumoniae carbapenemase; MBL, metallo-β-lactamase; MDR, multidrug resistant; MIC, minimum inhibitory concentration; NDM, New Delhi metallo-β-lactamase; OXA, oxacillinase; PBP, Penicillin-binding proteins; SHV-OSBL, Original-spectrum β-lactamase, VAP, respiratory pneumonia; VIM, Verona integron-encoded metallo-β-lactamase.
Ethical Approval
The study was exempt from Institutional Review Boards approval as it is a non-patient-based antimicrobial surveillance study, and it follows the policies and guidelines from the ATLAS database managed by International Health Management Associates (IHMA). Informed Consent is not a requirement of surveillance initiatives due to the lack of direct involvement or monitoring of specific patients in the program.
Disclosure
P. Zalas-Więcek, M. Prażyńska, D. Żabicka, M. Orczykowska-Kotyna, and A. Polak report grants from International Health Management Associates, Inc (IHMA), during the conduct of the study and outside the submitted work. M. Prażyńska, Ł. Pojnar report personal fees from Pfizer Polska Sp. z o.o., outside the submitted work. B. Możejko-Pastewka, M. Bogiel, and EA. Głowacka are employees of Pfizer Polska Sp. z o.o. I. Pieniążek, M. Pawlik, and M. Grys are affiliated with Arcana Institute, a Certara company that provided medical writing support funded by Pfizer Polska Sp. z o.o. The authors report no other conflicts of interest in this work.
References
1. Sader H, Castanheira M, Shortridge D, Mendes R, Flamm R. Antimicrobial activity of ceftazidime-avibactam tested against multidrug-resistant enterobacteriaceae and Pseudomonas aeruginosa isolates from U.S. Medical Centers, 2013 to 2016. Antimicrob Agents Chemother. 2017;61(11). doi:10.1128/aac.01045-17
2. Zarkotou O, Pournaras S, Tselioti P, et al. Predictors of mortality in patients with bloodstream infections caused by KPC-producing Klebsiella pneumoniae and impact of appropriate antimicrobial treatment. Clin Microbiol Infect. 2011;17(12):1798–1803. doi:10.1111/j.1469-0691.2011.03514.x
3. Jean S, Gould I, Lee W, Hsueh P. New drugs for multidrug-resistant gram-negative organisms: time for stewardship. Drugs. 2019;79(7):705–714. doi:10.1007/s40265-019-01112-1
4. Kowalska-Krochmal B, Woroń J, Serednicki WT, et al. Ceftazidime with avibactam - the microbiological, pharmacological and clinical aspect of drug use in clinical practice. Forum Zakazen. 2019;10(6). doi:10.15374/FZ2019056
5. Wolska K, Kot B, Piechota M, Frankowska A. Resistance of Pseudomonas aeruginosa to antibiotics. Postepy Higieny i Medycyny Doswiadczalnej. 2013;67:1300–1311. doi:10.5604/17322693.1080803
6. Zalas-Więcek P, Gospodarek-Komkowska E. Antimicrobial susceptibility of multi-drug and extensively-drug-resistant Escherichia coli to ceftolozane-tazobactam and ceftazidime-avibactam: an in vitro study*. Postepy Higieny i Medycyny Doswiadczalnej. 2020;74:77–83. doi:10.5604/01.3001.0014.0859
7. Deptuła A, Trejnowska E, Ozorowski T, Pawlik K, Hryniewicz W. Spot study of healthcare associated infections and antibiotic use in acute care hospitals (PPS HAI & AU) in Poland. Report from a study conducted in 2014-2015. National Antibiotic Protection Program (online); 2016. Available from: http://antybiotyki.edu.pl/wp-content/uploads/dokumenty/raport_PPS_20160110.pdf.
8. Jean S, Lee W, Lam C, Hsu C, Chen R, Hsueh P. Carbapenemase-producing Gram-negative bacteria: current epidemics, antimicrobial susceptibility and treatment options. Future Microbiol. 2015;10(3):407–425. doi:10.2217/fmb.14.135
9. Falcone M, Paterson D. Spotlight on ceftazidime/avibactam: a new option for MDR Gram-negative infections. J Antimicrob Chemother. 2016;71(10):2713–2722. doi:10.1093/jac/dkw239
10. European Medicines Agency. Zavicefta: summary of product characteristics; 2018. Available from: http://www.ema.europa.eu.
11. Clinical and Laboratory Standards Institute. Methods for dilution antimicrobial susceptibility tests for bacteria that grow aerobically. Approved Standard—Eleventh Edition. CLSI document M07-A10. Wayne, Pennsylvania; USA: Clinical and Laboratory Standards InstituteCLSI; 2018.
12. Magiorakos AP, Srinivasan A, Carey RB. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18:1469–1691.
13. Lob S, Kazmierczak K, Badal R, et al. Trends in susceptibility of Escherichia coli from intra-abdominal infections to ertapenem and comparators in the United States according to data from the SMART program, 2009 to 2013. Antimicrob Agents Chemother. 2015;59(6):3606–3610. doi:10.1128/aac.05186-14
14. Nichols W, de Jonge B, Kazmierczak K, Karlowsky J, Sahm D. In vitro susceptibility of global surveillance isolates of Pseudomonas aeruginosa to Ceftazidime-Avibactam (INFORM 2012 to 2014). Antimicrob Agents Chemother. 2016;60(8):4743–4749. doi:10.1128/aac.00220-16
15. Antimicrobial resistance in the EU/EEA (EARS-Net) Annual Epidemiological Report for 2019. Available from: https://www.ecdc.europa.eu/sites/default/files/documents/surveillance-antimicrobial-resistance-Europe-2019.pdf.
16. Kaye K, Pogue J. Infections caused by resistant Gram-negative bacteria: epidemiology and management. Pharmacotherapy. 2015;35(10):949–962. doi:10.1002/phar.1636
17. Ramalheira E, Stone G. Longitudinal analysis of the in vitro activity of ceftazidime/avibactam versus Enterobacteriaceae, 2012–2016. J Glob Antimicrob Resist. 2019;19:106–115. doi:10.1016/j.jgar.2019.07.003
18. Kristóf K, Adámková V, Adler A, et al. In vitro activity of ceftazidime-avibactam and comparators against Enterobacterales and Pseudomonas aeruginosa isolates from Central Europe and Israel, 2014–2017 and 2018. Diagn Microbiol Infect Dis. 2021;101(1):115420. doi:10.1016/j.diagmicrobio.2021.115420
19. Hirsch E, Brigman H, Zucchi P, et al. Ceftolozane-tazobactam and ceftazidime-avibactam activity against β-lactam-resistant Pseudomonas aeruginosa and extended-spectrum β-lactamase-producing Enterobacterales clinical isolates from U.S. medical centres. J Glob Antimicrob Resist. 2020;22:689–694. doi:10.1016/j.jgar.2020.04.017
20. Spiliopoulou I, Kazmierczak K, Stone G. In vitro activity of ceftazidime/avibactam against isolates of carbapenem-non-susceptible Enterobacteriaceae collected during the INFORM global surveillance programme (2015–17). J Antimicrob Chemother. 2019;75(2):384–391. doi:10.1093/jac/dkz456
21. Martis N, Leroy S, Blanc V. Colistin in multi-drug resistant Pseudomonas aeruginosa blood-stream infections. J Infect. 2014;69(1):1–12. doi:10.1016/j.jinf.2014.03.001
22. Tamma P, Aitken S, Bonomo R, Mathers A, van Duin D, Clancy C. Infectious Diseases Society of America Guidance on the Treatment of Extended-Spectrum β-lactamase Producing Enterobacterales (ESBL-E), Carbapenem-Resistant Enterobacterales (CRE), and Pseudomonas aeruginosa with Difficult-to-Treat Resistance (DTR-P. aeruginosa). Clin Infect Dis. 2020;72(7):e169–e183. doi:10.1093/cid/ciaa1478
23. Stone G, Smayevsky J, Kazmierczak K. Longitudinal analysis of the in vitro activity of ceftazidime-avibactam vs. Pseudomonas aeruginosa, 2012–2016. Diagn Microbiol Infect Dis. 2020;96(1):114835. doi:10.1016/j.diagmicrobio.2019.05.007
24. Sader H, Huband M, Duncan L, Flamm R. Ceftazidime–avibactam antimicrobial activity and spectrum when tested against Gram-negative organisms from pediatric patients. Pediatr Infect Dis J. 2018;37(6):549–554. doi:10.1097/inf.0000000000001859
25. Gill C, Aktaþ E, Alfouzan W, et al. The ERACE-PA Global Surveillance Program: ceftolozane/tazobactam and ceftazidime/avibactam in vitro activity against a global collection of carbapenem-resistant Pseudomonas aeruginosa. Eur J Clin Microbiol Infect Dis. 2021;40(12):2533–2541. doi:10.1007/s10096-021-04308-0
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.