Back to Journals » Cancer Management and Research » Volume 15
CD73 Dysregulates Monocyte Anti-Tumor Activity in Multiple Myeloma
Authors Zhou L, Liu X, Guan T, Xu H, Wei F
Received 15 March 2023
Accepted for publication 6 July 2023
Published 19 July 2023 Volume 2023:15 Pages 729—738
DOI https://doi.org/10.2147/CMAR.S411547
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Kenan Onel
Video abstract presented by Lin Zhou.
Views: 78
Lin Zhou,1,* XiaoLan Liu,2,* Tao Guan,2 HaiLing Xu,1 Fang Wei1
1Department of Hematology, The First Hospital of Shanxi Medical University, Taiyuan, Shanxi, People’s Republic of China; 2Shanxi Key Laboratory of Precise and Diagnosis and Therapy of Lymphoma, Shanxi Province Cancer Hospital, Taiyuan, Shanxi, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Fang Wei, Department of Hematology, The First Hospital of Shanxi Medical University, 85 Jiefang South Road, Yingze District, Taiyuan, Shanxi, People’s Republic of China, Tel +86 15034078883, Email [email protected]
Purpose: Multiple myeloma (MM) is characterized by immune cell dysfunction in the tumor microenvironment (TME). We aimed at evaluating the effect of CD73, an overexpressed factor in some tumors, on anti-tumor immune function in the TME of MM.
Patients and Methods: We analyzed the expression of CD73 in T-, B-, and natural killer (NK)-lymphocytes and monocytes in bone marrow (BM), peripheral blood (PB) from MM patients and healthy controls, and residual CD138+ cells using flow cytometry. The anti-tumor activity of these monocytes was confirmed by co-culture with RPMI-8226 cells treated with a CD73 inhibitor. We determined the interleukin (IL)-2, IL-4, IL-6, IL-10, tumor necrosis factor (TNF)-α, and interferon (IFN)-γ levels using a cytometric bead array. Monocyte phagocytosis in cell culture sediment was then observed and measured.
Results: CD73 was highly expressed in T-, B-, and NK-lymphocytes and monocytes from the BM and PB isolated from patients with MM. Compared with healthy controls, MM samples exhibited significantly higher CD73 expression and TNF-α, IFN-γ, IL-10 levels in monocytes. Inhibiting CD73 in BM immune cells from MM samples significantly increased the secretion of IL-2, TNF-α, and IFN-γ, as well as the killing ability of immune cells. However, monocyte phagocytosis was seldom observed. Inhibiting CD73 in MM monocytes significantly increased the secretion of IL-2, TNF-α, and IFN-γ in monocytes and improved monocyte killing and phagocytosis.
Conclusion: Monocytes from MM exhibited weakened anti-tumor effects, and CD73 was involved in forming an immunosuppressive microenvironment. Inhibiting CD73 partly restored the anti-tumor activity of monocytes, a potential strategy for the treatment of MM.
Keywords: multiple myeloma, CD73, anti-tumor activity, monocytes, immune cells, phagocytosis
Introduction
Multiple myeloma (MM) is a plasma cell neoplasm in the bone marrow (BM). The global incidence of MM in 2020 was 176,000, an increase of 287.7% since 1990.1,2 Current myeloma therapies such as proteasome inhibitors, immunomodulatory agents, monoclonal antibodies, and BM transplantation, prolong the survival and improve the prognosis of patients; however, these methods are rarely curative and disease relapse is common.3 Therefore, new treatments are necessary to improve patient outcomes.
Immune dysregulation in the TME is a hallmark of MM.4 The interaction between MM cells and the TME creates a pro-tumor niche characterized by dysfunctional monocytes, impaired dendritic cell (DC) differentiation and maturation, high levels of myeloid-derived suppressor cells and regulatory T cells, an unbalanced Th1/Th2 cell ratio, and dysregulated NK cells.4 Immune checkpoints control anti-tumor immune responses in hematological malignancies, and targeting them represents an effective strategy for preventing tumor progression. However, the use of anti-PD-L1/PD-1 antibodies in patients with MM remains controversial, because of discordant PD-L1/PD-1 expression in MM and BM cell microenvironments.5
The CD73 metabolic immune checkpoint is crucial in maintaining extracellular adenosine levels that inhibit inflammatory responses within a stressed or damaged tissue microenvironment.6–10 CD73 hydrolyzes extracellular AMP into adenosine, which acts on P1 receptors (A1R, A2aR, A2bR, and A3R) that regulate inflammatory responses.11 In the TME, CD73 promotes adenosine accumulation that activates A2aR and inhibits the anti-tumor effect of immune cells. T-, B-, and NK-lymphocytes and monocytes are important participants in anti-tumor immunity. A2aR activation inhibits the cytotoxic activity of immune cells and decreases the production of anti-tumor cytokines such as TNF-α, IFN-γ, and IL-2, thereby limiting active immune responses and protecting tumors from immune attack.12–14 The expression and activity of CD73 are significantly increased in ovarian, triple-negative breast, prostate, and colorectal cancers,6–10 and high levels of CD73 are inversely correlated with overall patient survival and prognosis.7,9 Accumulating evidence has shown that in MM, CD73 is highly expressed in mesenchymal stem cells, lymphocytes, stromal cells, and DCs,15–17 and its overexpression in the TME creates an immunosuppressive environment that protects myeloma cells from the immune system.16,17 Thus, we analyzed the expression of CD73 in immune cells collected from patients with MM and the effect of CD73 on anti-tumor immune function in MM TME. We also explored the therapeutic potential of inhibiting CD73 in MM in vitro.
Materials and Methods
Patient Samples
We recruited patients with newly diagnosed MM (n = 40; mean age 61 y; 16 women, 24 men) who were admitted to The First Hospital Of Shanxi Medical University from October 2019 to September 2022. The diagnostic criteria from The International Myeloma Working Group (IMWG) Guidelines for The Diagnosis and Treatment of Multiple Myeloma (Revised 2020) were used to identify newly diagnosed MM. Samples were collected before patients received treatment. The healthy control group (n = 40; mean 48 y; 18 women, 22 men) was composed of healthy volunteers. All patients with MM and healthy volunteers provided signed informed consent. This study was conducted in accordance with the ethical standards formulated in The Declaration of Helsinki and was approved by the Ethics Committee of the First Hospital of Shanxi Medical University.
Bone Marrow Mononuclear Cells (BMMCs), PB Mononuclear Cells, Monocytes, and Human Myeloma Cell Lines
The BM from the iliac crest and PB from the radial vein were collected from the MM and control groups. BM samples were diluted 1:1 with phosphate-buffered saline and Human Lymphocyte Separation Medium (Solarbio Biotechnology Co Ltd, Beijing, China) to a density of 1.077 g/mL and centrifuged at 2000 rpm for 15 min to obtain BMMCs. An erythrocyte lysate was used to lyse redundant erythrocytes at a volume ratio of 5:1. PB mononuclear cells were obtained using the aforementioned method for BMMCs. To obtain monocytes from PB mononuclear cells, mononuclear cells (3×106 cells per well) were plated in 10-cm Petri dishes for 3 h, and the adherent monocytes were collected by gentle scraping. The human myeloma cell line RPMI-8226 (Fuheng Biotechnology Co Ltd, Shanghai, China) was cultured in RPMI 1640 (BOSTER Biological Technology Co, Ltd, Wuhan, China) supplemented with 10% fetal bovine serum (FBS) (Saiaomei Cell Technology Co, Ltd, Beijing, China), penicillin/streptomycin (Invitrogen), GlutaMax (Invitrogen), sodium pyruvate (Invitrogen), non-essential amino acids (Invitrogen), and β-mercaptoethanol (Sigma) at 37°C and 5% CO2.
Flow Cytometry and Software Analysis
Anti-human CD3-FITC-A, CD45-KO, CD4-PE-Cy-A, CD8-APC-Cy-A, CD19-APC-A, CD16/56-PE-A, CD14-PE-A, and CD73-PE (BD) antibodies were used to detect the markers on the surface of T-, B-, NK-lymphocytes and monocytes from both BM and PB. CD138-PERCP-CY55-A (BD) was used to detect MM cells. Anti-human monoclonal antibodies against IL-2, IL-4, IL-6, IL-10, TNF-α, and IFN-γ (Yuanmu Biological Co, Ltd, Shanghai, China) were used to detect immune-related proteins in cell culture supernatants. T-, B-, and NK-lymphocytes and monocytes, and CD138+ cells were detected using flow cytometry (BD CANTO plus). IL-2, IL-4, IL-6, IL-10, TNF-α, and IFN-γ were detected using a Cytometric Bead Array (Beckman FC500). The samples were analyzed using the FlowJo v10.4 software.
Evaluation of Monocyte Function
Evaluation of Myeloma Cell Killing by Monocytes
PB monocyte cells from patients with MM (M-MØ) or healthy controls (H-MØ) were co-cultured with RPMI-8226 for 12 h. Cell precipitates and supernatants were collected separately. The proportion of MM cells (CD138+ cells) in the precipitate was analyzed using flow cytometry.
Evaluation of Cytokine Secretion of Monocytes
We detected the levels of IL-2, IL-4, IL-6, IL-10, TNF-α, and IFN-γ in the supernatants obtained from all groups using the Cytometric Bead Array.
Evaluation of Phagocytosis by Monocytes
Cell precipitates from the co-culture of M-MØ or H-MØ with RPMI-8226 were treated with Giemsa dye (Shan Jingkang Biological Engineering Co, Ltd, Shanghai, China) and fixed for 30 min. The monocytes were counted using a microscope (Nikon E100) under a 10× objective. The phagocytic index was calculated as the number of phagocytosed myeloma cells per 100 macrophages. Images were obtained using a 100× objective. The index calculations were performed by three hematologists and each experiment was repeated at least three times.
Analysis of the Anti-Tumor Immunity of CD73 Inhibitor
The BMMCs from patients with MM were cultured in 6-well plates at a density of 2×106 cell per well with 50 μg/mL GM-CSF (Tebao Bioengineering Co, Ltd, Xiamen, China) in RPMI 1640 complete media, with or without 10 μg/mL PSB-12379 (CD73 inhibitor, Haoyuan Biomedical Technology Co, Ltd, Shanghai, China) for 12 h. The PB monocytes from patients with MM were co-cultured with RPMI-8226 cells in a 3:1 ratio with or without 10 μg/mL PSB-12379 in 48-well plates for 12 h. Then, the monocyte phagocytic index was calculated and mapping was conducted as described in the previous section.
Statistical Analysis
Statistical analysis was performed using GraphPad Prism 9 (GraphPad Software, San Diego, USA). Data were analyzed using nonparametric tests or paired-samples t-test, and are expressed as ( ). Differences were statistically significant at p < 0.05.
). Differences were statistically significant at p < 0.05.
Results
Immune Cells in the BM and PB of Patients with MM Express High Levels of CD73
Compared with healthy controls, patients with MM exhibited increased adenosine concentration in the immune environment,16,17 and CD73 is a key enzyme in this pathway.18 First, we found that CD73 was highly expressed in the BM immune cells of patients with MM. We also found that CD73 expression was high in the T-, B-, and NK-lymphocytes and monocytes from the PB of patients with MM (Figure 1A and B). Although these differences were not significant (Figure 1C), the high expression of CD73 in the immune cells of patients with MM implied that CD73 may dysregulate anti-tumor effect in these cells.
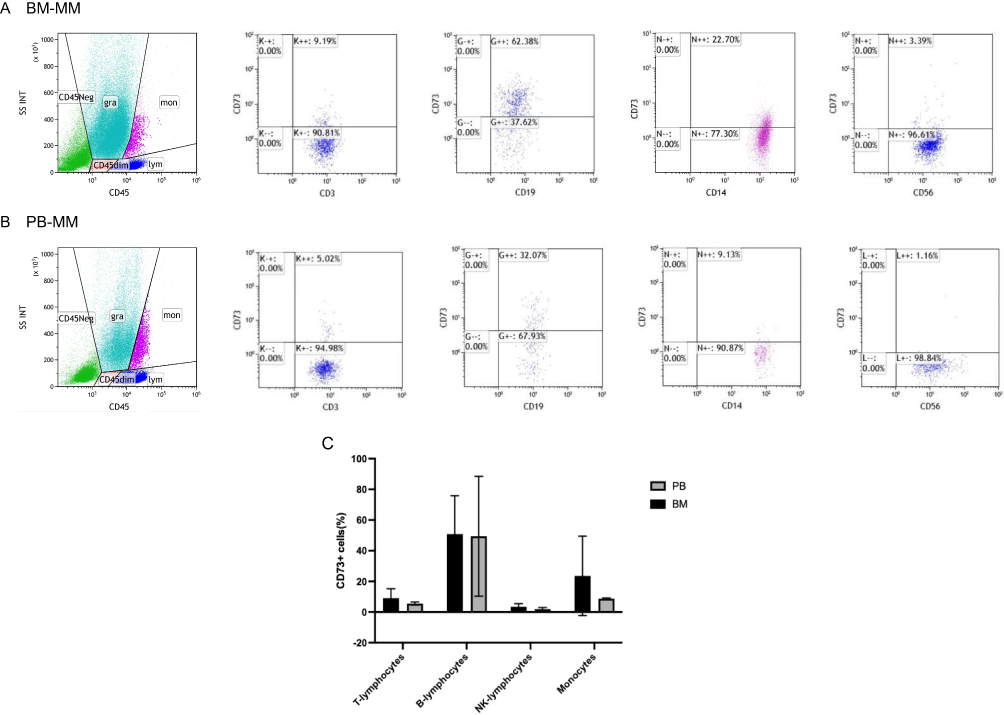 |
Figure 1 Immune cells in BM and PB from patients with MM expressed high levels of CD73. (A) Representative analysis of CD73 expression in T-, B-, and NK-lymphocytes and monocytes of BM. (B) Representative analysis of CD73 expression in T-, B-, and NK-lymphocytes and monocytes of PB. (C) Quantitative comparison of CD73 expression in T-, B-, and NK-lymphocytes and monocytes of BM and PB. Abbreviations: BM, bone marrow; PB, peripheral blood; MM, multiple myeloma. |
Monocytes of Patients with MM Express High Levels of CD73
We next compared CD73 expression in the PB immune cells between MM and healthy control groups. Flow cytometry revealed that patients with MM exhibited significantly higher CD73 expression in PB monocytes (p < 0.000; Figure 2A and B), and CD73 expression in PB monocytes from patients with MM was eight times higher than that in the healthy control. CD73 expression in the T-, B-, and NK-lymphocytes from the PB of patients with MM was lower than that of healthy controls(Figure 2B). The significant difference in CD73 expression in monocytes from patients with MM revealed that CD73 may contribute to the defective anti-tumor activity on the MM TME.
 |
Figure 2 Expression of CD73 in PB monocytes isolated from patients with MM. (A) Comparative analysis of CD73 expression in PB monocytes: healthy controls (top) vs patients with MM (bottom). (B) Quantitative comparison of CD73 expression in PB monocytes from healthy controls and patients with MM. The expression of CD73 in T-, B-, and NK-lymphocytes of PB from patients with MM lower than from healthy controls; ***P < 0.001/P < 0.000. Abbreviations: BM, bone marrow; PB, peripheral blood; MM, multiple myeloma. |
MM Monocytes Have a Defective Anti-Tumor Immune Function
Monocytes from patients with breast and colon cancer have a decreased anti-tumor immune function;19,20 therefore, we evaluated the anti-tumor activity of monocytes from patients with MM by co-culturing PB monocytes from patients with MM or healthy controls with RPMI-8226 human myeloma cell lines. The proportion of CD138+ cells significantly decreased in the healthy control group compared with that in the MM group (Figure 3A; p < 0.000). We then examined the changes in cytokine levels in the supernatant and cell sediment before and after the co-culture of monocytes from MM patients or healthy controls with RPMI-8226. Before co-culture, monocytes from patients with MM secreted higher levels of TNF-α (p = 0.003), IFN-γ (p = 0.031), and IL-10 (p = 0.023) than those of healthy controls (Figure 3B). After co-culture with RPMI-8226, monocytes from patients with MM secreted lower levels of IL-2 (p = 0.023), TNF-α (p = 0.009), and IFN-γ (p = 0.006) than those of healthy controls (Figure 3C). Furthermore, monocytes from patients with MM exhibited a lower phagocytic index (p = 0.001) in the cell sediment than those of healthy controls (Figure 3D). Although TNF-α (p = 0.039) and IFN-γ (p = 0.019) secretion significantly increased in healthy controls after co-culture (Figure 3E), no changes in TNF-α and IFN-γ secretion were observed in the MM group (Figure 3F). These findings indicated that the immune activity of monocytes from patients with MM was defective compared with that of the monocytes from healthy controls. Thus, we hypothesized that monocytes from patients with MM exhibit a defective anti-tumor immune function.
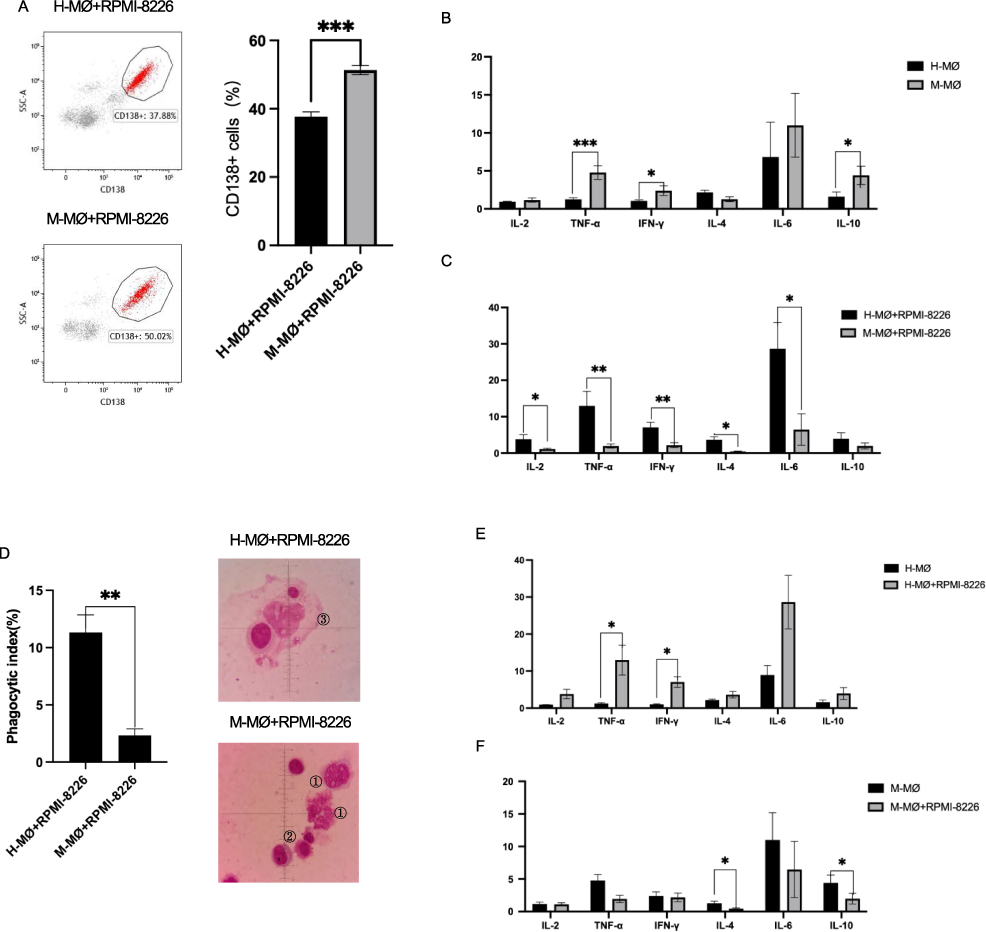 |
Figure 3 PB monocytes from patients with MM exert pro-tumor effects. The PB monocytes from patients with MM (M-MØ) or healthy control (H-MØ) samples were co-cultured with myeloma cells (RPMI-8226) for 12 h. (A) Flow cytometry analysis showing the residual CD138+ cells in the healthy control (top) and MM (bottom) groups. (B and C) Levels of IL-2, TNF-α, IFN-γ, IL-4, IL-6, and IL-10 in monocytes from patients with MM and healthy controls (B) before co-culture with RPMI-8226 cells and (C) after co-culture in the supernatant. (D) Phagocytic index in myeloma cells in the monocytes from patients with MM (bottom) and healthy controls (top) after co-culture with RPMI-8226 cells. ① Monocytes; ② myeloma cells; ③ monocyte phagocytosis of myeloma cells. (E and F) Levels of IL-2, TNF-α, IFN-γ, IL-4, IL-6, and IL-10 in monocytes from the (E) healthy controls group and (F) patients with MM group before and after the co-culture of the samples with RPMI-8226 cells; *P < 0.05, **P < 0.01, ***P < 0.001. Abbreviations: PB, peripheral blood; MM, multiple myeloma; RPMI, Roswell Park Memorial Institute; IL, interleukin; TNF-α, tumor necrosis factor alpha; IFN-γ, interferon gamma. |
We confirmed that the CD73 expression and anti-tumor immune function of monocytes were significantly different between patients with MM and healthy controls. However, we had to determine the association between the anti-tumor activity of immune cells in the TME and the expression of CD73.
Inhibiting CD73 Improved the Anti-Tumor Activity of Immune Cells in Patients with MM
We analyzed the changes in anti-tumor immunity after inhibiting CD73 in the BM immune cells from patients with MM. We cultured BMMCs from patients with MM treated with or without the CD37 inhibitor, PSB-12379, for 12 h and found that BM immune cells treated with the CD73 inhibitor had a significantly lower number of CD138+ cells (Figure 4A; p = 0.047) compared with those from untreated samples. We collected the supernatant and cell sediment after co-culture in the two groups, and found that cells treated with the CD73 inhibitor secreted more IL-2 (p = 0.026), TNF-α (p = 0.027), and IFN-γ (p = 0.022) than untreated immune cells (Figure 4B); however, no obvious monocyte phagocytosis of myeloma cells was observed in the cell sediment in either of the groups (Figure 4C). Therefore, inhibiting CD73 function partly improved the anti-tumor activity of BM immune cells in MM; however, the role of CD73 in monocytes for anti-tumor immunity requires validation.
 |
Figure 4 Inhibiting CD73 improves the anti-tumor immunity in BM immune cells isolated from patients with MM. BMMCs from patients were either untreated or treated with 10 μg/mL PSB-12379 for 12 h. (A) Flow cytometry analysis showing the residual CD138+ cells in the BMMCs culture of the groups treated with or without PSB-12379. The bar graph shows the quantitative comparison of the residual CD138+ cells in the BMMCs culture in the two groups. (B) Levels of IL-2, TNF-α, IFN-γ, IL-4, IL-6, and IL-10 in cells treated with or without PSB-12379. (C) The number of monocytes that underwent phagocytosis in myeloma cells was not significantly different between PSB-12379-treated and untreated groups; *P < 0.05. Abbreviations: BM, bone marrow; MM, multiple myeloma; BMMCs, bone marrow mononuclear cells; IL, interleukin; TNF-α, tumor necrosis factor alpha; IFN-γ, interferon gamma. |
Inhibiting CD73 Enhanced the Anti-Tumor Immunity of Monocytes in Patients with MM
We also examined the association between inhibiting CD73 in monocytes and anti-tumor immunity in MM. The PB monocytes from patients with MM were co-cultured with RPMI-8226 with or without PSB-12379 for 12 h. We found that PB monocytes treated with the CD73 inhibitor had a significantly reduced residual of CD138+ cells (Figure 5A; p = 0.003) than the untreated monocytes. We also extracted the supernatant and cell sediment from monocytes treated with and without the CD73 inhibitor and found that the treated PB monocytes secreted increased amounts of IL-2 (p = 0.013), TNF-α (p = 0.014), and IFN-γ (p = 0.003) than the untreated monocytes (Figure 5B). When PB monocytes were treated with the CD73 inhibitor (PSB-12379), a higher frequency of monocyte phagocytosis occurred (phagocytic index, p = 0.020) than in the cell sediment of untreated monocytes (Figure 5C). The significant increase in anti-tumor cytokines and monocyte phagocytosis indicated that inhibiting CD73 expression in monocytes improved anti-tumor immunity in MM.
 |
Figure 5 Inhibiting CD73 enhances the anti-tumor immunity of patient monocytes. Monocytes isolated from patients with MM were co-cultured with myeloma cells with or without 10 μg/mL PSB-12379. (A) Flow cytometry showing the residual CD138+ cells In the patient monocytes culture of the groups treated with or without PSB-12379. Monocytes treated with PSB-12379 (bottom) significantly increased the killing activity of CD138+ cells compared to the untreated cells (top). (B) Levels of IL-2, TNF-α, IFN-γ, IL-4, IL-6, and IL-10 in monocytes treated with or without PSB-12379. (C) Monocytes treated with PSB-12379 showing significantly higher monocyte phagocytosis in myeloma cells than in untreated monocytes. Almost no monocyte phagocytosis was observed when MM PB monocytes were co-cultured with myeloma cells (top), while significantly higher monocyte phagocytosis was observed when MM PB monocytes treated with PSB-12379 were co-cultured with myeloma cells (bottom). ① Monocytes; ② myeloma cells; ③ monocyte phagocytosis of myeloma cells. (D) The PB monocytes from healthy control samples had a significantly reduced residual of CD138+ cells compared with those treated with PSB-12379 from patients with MM. (E) The PB monocytes from healthy control samples had significantly higher TNF-α, IL-4, and IL-6 levels than those that were treated with PSB-12379 from patients with MM. (F) PB monocytes from healthy controls showing higher phagocytosis of CD138+ cells than those treated with PSB-12379 from patients with MM; *P < 0.05; **P < 0.01. Abbreviations: PB, peripheral blood; MM, multiple myeloma; IL, interleukin; TNF-α, tumor necrosis factor alpha; IFN-γ, interferon gamma. |
Although inhibiting CD73 in monocytes improved anti-tumor immunity to some extent, compared with PB monocytes isolated from patients with MM that were treated with CD73 inhibitors, those from healthy patients could kill more CD138+ cells (Figure 5D; P=0.004). Further, an increased monocyte phagocytosis (phagocytic index, p = 0.018) occurred in the cell sediment, and high levels of TNF-α (p = 0.033), IL-4 (p = 0.045) and IL-6 (p =0.024) were secreted in the supernatant after healthy control monocytes were co-cultured with myeloma cells (Figure 5E and F). These findings demonstrated that inhibiting CD73 partially restored the anti-tumor immunity of monocytes in MM; however, the gap in anti-tumor immunity between monocytes from healthy individuals and MM patients with MM needs further verification.
Discussion
Because MM is currently an incurable disease, its treatment can be complex. Although immune checkpoint therapies such as anti-PD1 or PD-L1 have limited clinical effects in MM,5,21 there is evidence that PD-1/PD-L1-blockade combined with lenalidomide enhances anti-MM immune effect.22 Therefore, an immune checkpoint away from the PD-1 axis could act as a crucial adjuvant that influences the anti-myeloma activity of immune-based treatments to achieve rapid and complete remission in patients with MM. CD73 is a nucleotidase attached to the plasma membrane that is highly expressed in many TMEs, where it participates in the growth, metastasis, and deterioration of various tumors.6–10,15–17 Increased expression of CD73 has been detected in malignant hematological immune cells,23 and CD73 is also expressed in MM BM cells such as mesenchymal stem cells, lymphocytes, stromal cells, and dendritic cells (DCs).15–17 We showed that CD73 is highly expressed in T-, B-, and NK-lymphocytes and monocytes in both BM and PB collected from patients with MM as compared to healthy controls. Patients with MM exhibited very high CD73 expression in PB monocytes, with expression levels eight times higher than those observed in healthy controls, revealing that CD73 is a potential therapeutic target for MM.
Immune cells in the TME participate in the pathogenesis of MM. Among others, monocytes are pivotal in the pathophysiology of MM and its resistance to treatment.24 Tumor-associated monocytes and macrophages promote tumor proliferation and metastasis by protecting the tumor from invasion by T- and NK-lymphocytes. 25 Monocytes in breast cancer, colon cancer, and hepatocellular carcinoma have weakened immune activity.19,20,26 Consistent with these reports, we found that monocytes from patients with MM secrete significantly lower amounts of anti-tumor cytokines than those from healthy controls after co-culture with MM cells. The high level of secretion of IL-10 in MM samples also showed that MM monocytes were partially involved in tumor promotion. These findings indicated that monocytes contribute to tumor progression.
The adenosine pathway is involved in immunosuppression in MM and its activation inhibits the anti-MM activity of immune cells.14,16,17 The expression level of CD73 was similar between patients and healthy controls in T-, B-, and CD45- stromal cells in BM, inhibition of CD73 increased the activation of CD8+T cells, and higher levels of IFN-γ and activated monocytes in spleen and BM were observed in myeloma-bearing mice.16 Moreover, MM cells cultured with pDCs exhibited increased CD73 expression in myeloma cells, while inhibiting CD73 decreased adenosine levels, activated DCs, and triggered cytotoxic T lymphocyte activity against autologous MM cells in DC-MM co-culture models.17 We detected that high levels of CD73 were expressed in the T-, B-, and NK-lymphocytes and monocytes in BM isolated from patients with MM, and when the PSB-12379 non-specific CD73 inhibitor27 was added to BMMCs isolated from patients with MM, improved levels of anti-tumor cytokines IL-2, TNF-α, and IFN-γ and the anti-tumor effect of BM immune cells on myeloma were observed. We also found that CD73 expression in MM monocytes was eight times that in healthy monocytes, and MM monocytes exhibited defective anti-tumor functions. We further verified that the anti-tumor activity of MM monocytes, when treated with PSB-12379, significantly increased; furthermore, the activity of anti-tumor cytokines, monocyte phagocytosis, and killing of myeloma cells were improved. The results reported by Arghya and Yang were consistent with our findings, suggesting that CD73 acts as an immune checkpoint in MM monocytes and influences their anti-tumor activity.16,17 Therefore, inhibiting CD73 restores the anti-tumor effect of these cells.
CD73 inhibitors have been applied in many tumor models.6,7,16,17 Inhibiting CD73 enhances the activity of anti-CTLA-4 and anti-PD-1 monoclonal antibodies against colon and prostate cancers.28 In this study, inhibiting CD73 of monocytes from MM patients promoted the secretion of anti-tumor cytokines and increased monocyte phagocytosis of myeloma cells. However, although inhibiting CD73 improved the anti-tumor activity of MM monocytes, there is still a gap in the anti-tumor activity between MM monocytes treated with CD73 inhibitor and healthy monocytes. Our findings reveal that there are other factors in addition to CD73 molecular signaling that affect anti-tumor activity in MM TME. A combination of anti-CD73 Ab and TLR-7 agonist triggered more robust autologous MM-specific CD8+CTL activity than either agent alone,17 and A2AR and CD73 inhibitors synergistically reduced MM load in patient samples.16 Thus, our results also help explain the complexity of the MM TME, further showing that single target drug strategies have limited therapeutic effects and multi-drug combination therapies are necessary and efficient in managing the disease in patients with MM. Our findings verified that high levels of CD73 expression in monocytes can dysregulate the anti-tumor effect of myeloma cells, while inhibiting CD73 in monocytes partly restores anti-tumor immunity in MM. Thus, CD73 inhibitors are an integral part of the combinational MM treatment strategies.
Data Sharing Statement
Data are available upon reasonable request to the corresponding author. All data relevant to the study are included in the article.
Acknowledgments
We thank the patients and volunteers who donated specimens for this research study, and the Shanxi Medical University and Shanxi Key Laboratory of Precise and Diagnosis and Therapy of Lymphoma for providing the experimental platform.
Funding
This work was supported by a grant from the Shanxi Science and Technology Department (Item No 201801D121223) and Fund Program for the Scientific Activities of Selected Returned Overseas Professionals in the Shanxi Province.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Cowan AJ, Allen C, Barac A, et al. Global burden of multiple myeloma: a systematic analysis for the global burden of disease study 2016. JAMA Oncol. 2018;4(9):1221–1227. doi:10.1001/jamaoncol.2018.2128
3. Sonneveld P, Broijl A. Treatment of relapsed and refractory multiple myeloma. Haematologica. 2016;101(4):396–406. doi:10.3324/haematol.2015.129189
4. Romano A, Conticello C, Cavalli M, et al. Immunological dysregulation in multiple myeloma microenvironment. Biomed Res Int. 2014;2014:198539. doi:10.1155/2014/198539
5. Costa F, Vescovini R, Marchica V, et al. PD-L1/PD-1 pattern of expression within the bone marrow immune microenvironment in smoldering myeloma and active multiple myeloma patients. Front Immunol. 2020;11:613007. doi:10.3389/fimmu.2020.613007
6. Häusler SF, Del Barrio IM, Diessner J, et al. Anti-CD39 and anti-CD73 antibodies A1 and 7G2 improve targeted therapy in ovarian cancer by blocking adenosine-dependent immune evasion. Am J Transl Res. 2014;6(2):129–139.
7. Loi S, Pommey S, Haibe-Kains B, et al. CD73 promotes anthracycline resistance and poor prognosis in triple negative breast cancer. Proc Natl Acad Sci USA. 2013;110(27):11091–11096. doi:10.1073/pnas.1222251110
8. Lu XX, Chen YT, Feng B, et al. Expression and clinical significance of CD73 and hypoxia-inducible factor-1α in gastric carcinoma. World J Gastroenterol. 2013;19(12):1912–1918. doi:10.3748/wjg.v19.i12.1912
9. Wu XR, He XS, Chen YF, et al. High expression of CD73 as a poor prognostic biomarker in human colorectal cancer. J Surg Oncol. 2012;106(2):130–137. doi:10.1002/jso.23056
10. Allard D, Allard B, Gaudreau PO, et al. CD73-adenosine: a next-generation target in immuno-oncology. Immunotherapy. 2016;8(2):145–163. doi:10.2217/imt.15.106
11. Idzko M, Ferrari D, Riegel AK, et al. Extracellular nucleotide and nucleoside signaling in vascular and blood disease. Blood. 2014;124(7):1029–1037. doi:10.1182/blood-2013-09-402560
12. Ohta A, Ohta A, Madasu M, et al. A2A adenosine receptor may allow expansion of T cells lacking effector functions in extracellular adenosine-rich microenvironments. J Immunol. 2009;183(9):5487–5493. doi:10.4049/jimmunol.0901247
13. Lappas CM, Rieger JM, Linden J. A2A adenosine receptor induction inhibits IFN-gamma production in murine CD4+ T cells. J Immunol. 2005;174(2):1073–1080. doi:10.4049/jimmunol.174.2.1073
14. Beavis PA, Stagg J, Darcy PK, et al. CD73: a potent suppressor of anti-tumor immune responses. Trends Immunol. 2012;33(5):231–237. doi:10.1016/j.it.2012.02.009
15. Zhu BD, Ren J, Wang XY, et al. Biological properties of mesenchymal stem cells derived from bone marrow of patients with multiple myeloma. Zhongguo Shi Yan Xue Ye Xue Za Zhi. 2006;14(6):1138–1142.
16. Yang R, Elsaadi S, Misund K, et al. Conversion of ATP to adenosine by CD39 and CD73 in multiple myeloma can be successfully targeted together with adenosine receptor A2A blockade. J Immunother Cancer. 2020;8(1):e000610. doi:10.1136/jitc-2020-000610
17. Ray A, Song Y, Du T, et al. Identification and validation of ecto-5’ nucleotidase as an immunotherapeutic target in multiple myeloma. Blood Cancer J. 2022;12(4):50. doi:10.1038/s41408-022-00635-3
18. Robson SC, Sévigny J, Zimmermann H. The E-NTPDase family of ectonucleotidases: structure function relationships and pathophysiological significance. Purinergic Signal. 2006;2(2):409–430. doi:10.1007/s11302-006-9003-5
19. Azizi E, Carr AJ, Plitas G, et al. Single-cell map of diverse immune phenotypes in the breast tumor microenvironment. Cell. 2018;174(5):1293–1308.e1236. doi:10.1016/j.cell.2018.05.060
20. Zhang L, Li Z, Skrzypczynska KM, et al. Single-cell analyses inform mechanisms of myeloid-targeted therapies in colon cancer. Cell. 2020;181(2):442–459.e429. doi:10.1016/j.cell.2020.03.048
21. Suen H, Brown R, Yang S, et al. The failure of immune checkpoint blockade in multiple myeloma with PD-1 inhibitors in a Phase 1 study. Leukemia. 2015;29(7):1621–1622. doi:10.1038/leu.2015.104
22. Görgün G, Samur MK, Cowens KB, et al. Lenalidomide enhances immune checkpoint blockade-induced immune response in multiple myeloma. Clin Cancer Res. 2015;21(20):4607–4618. doi:10.1158/1078-0432.CCR-15-0200
23. Pulte D, Furman RR, Broekman MJ, et al. CD39 expression on T lymphocytes correlates with severity of disease in patients with chronic lymphocytic leukemia. Clin Lymphoma Myeloma Leuk. 2011;11(4):367–372. doi:10.1016/j.clml.2011.06.005
24. Lévesque J-P, Summers KM, Millard SM, et al. Role of macrophages and phagocytes in orchestrating normal and pathologic hematopoietic niches. Exp Hematol. 2021;100:12–31.e11. doi:10.1016/j.exphem.2021.07.001
25. Qian BZ, Pollard JW. Macrophage diversity enhances tumor progression and metastasis. Cell. 2010;141(1):39–51. doi:10.1016/j.cell.2010.03.014
26. Zhang Q, He Y, Luo N, et al. Landscape and dynamics of single immune cells in hepatocellular carcinoma. Cell. 2019;179(4):829–845.e820. doi:10.1016/j.cell.2019.10.003
27. Bhattarai S, Freundlieb M, Pippel J, et al. α, β-Methylene-ADP (AOPCP) derivatives and analogues: development of potent and selective ecto-5’-nucleotidase (CD73) Inhibitors. J Med Chem. 2015;58(15):6248–6263. doi:10.1021/acs.jmedchem.5b00802
28. Allard B, Pommey S, Smyth MJ, et al. Targeting CD73 enhances the anti-tumor activity of anti-PD-1 and anti-CTLA-4 mAbs. Clin Cancer Res. 2013;19(20):5626–5635. doi:10.1158/1078-0432.CCR-13-0545
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A High-Throughput, Three-Dimensional Multiple Myeloma Model Recapitulating Tumor-Stroma Interactions for CAR-Immune Cell-Mediated Cytotoxicity Assay
Luanpitpong S, Janan M, Poohadsuan J, Rodboon N, Samart P, Rungarunlert S, Issaragrisil S
ImmunoTargets and Therapy 2025, 14:321-338
Published Date: 30 March 2025
Unveiling Theranostics: Nanocomplex-Assisted Photodynamic Eradication of Aggressive Cancer Cells and Modulation of Tumor-Associated Macrophages
Butkute A, Kazlauske E, Mlynska A, Peciukaityte E, Karabanovas V, Rotomskis R, Steponkiene S
International Journal of Nanomedicine 2025, 20:9787-9806
Published Date: 8 August 2025