")
Back to Journals » Infection and Drug Resistance » Volume 15
CD4(+) T Cell Count Progress and Influencing Factors of Recovery in AIDS Patients with Virological Failure in Sichuan Province: A Retrospective Cohort Study
Authors Yuan D , Zhang Y, Li Y , Li L, Yang H, Yang W, Yu H, Feng L, Liang S
Received 16 June 2022
Accepted for publication 13 October 2022
Published 1 December 2022 Volume 2022:15 Pages 6985—6999
DOI https://doi.org/10.2147/IDR.S378799
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Dan Yuan,* Yan Zhang,* Yiping Li, Ling Li, Hong Yang, Wei Yang, Hang Yu, Liao Feng, Shu Liang
Center for AIDS/STD Control and Prevention, Sichuan Center for Disease Control and Prevention, Chengdu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shu Liang; Liao Feng, Email [email protected]; [email protected]
Background: Choosing patients with HIV/AIDS (PLWH) with virologic failure observed in the course of treatment, and analyzing the CD4(+) T cell count of PLWH with different subtypes of virus and the risk factors of CD4 (+) T cell count recovery
Methods: Analyze and evaluate the change of median CD4(+) T cell count of PLWH infected with different HIV-1 subtypes in Sichuan Province after treatment by rank sum test. Univariate and multivariate logistic regression models were used to analyze the risk factors on CD4(+) T cell count growth after PLWH treatment.
Results: A total of 4977 cases were analysed, including CRF07_BC 2358 cases (47.38%), CRF01_AE 1507 cases (30.28%), CRF08_BC 577 cases (11.59%), CRF85_BC 303 cases (6.09%) and other subtypes 232 cases (4.66%). PLWH infected with CRF85_BC had lower median CD4(+) T cell count after treatment (p < 0.05). It was found that protective factors to increase CD4(+) T cell count (p < 0.05) including females, Yi people, married or cohabiting, educational level at primary school or above, initial and recent treatment with Tenofovir + Lamivudine + Nevirapine Wellen, the second-line regimen with lopinavir/ritonavir (LPV/r) and the treatment time is more than 24 months. However, over 50 years old, the disease course is in AIDS stage, the infection of CRF01_AE and CRF85_BC virus was the risk factor on CD4(+) T cell count increase (p < 0.05). PLWH with higher initial CD4 level had a lower ratio of CD4(+) T cell count increase (≥ 50 cells/μL) (p < 0.05).
Conclusion: Age, sex, ethnicity, marriage, education, disease status, treatment protocols, treatment time, initial CD4(+) T cell count, and virus subtype are the influencing factors of PLWH CD4(+) T cell count increase. The poor recovery of CD4(+) T cell count after treatment was observed in PLWH infected with CRF85_BC virus.
Keywords: HIV, AIDS, antiretroviral therapy, CD4(+) T cells count
Introduction
HIV/AIDS antiretroviral therapy (hereafter referred to as treatment) is the primary strategy to prevent the spread of AIDS.1 In recent years, cumulative survivors (including HIV infected people and PLWH) have been increasing in Sichuan province and total 200,000 people were still alive at the end of 2021. To improve the treatment effect and quality of life of AIDS patients has become the main goal of AIDS prevention and treatment. Previous studies in Sichuan Province have shown that receiving ART and the first CD4 (+) T cells level are factors that affect the survival of PLWH. The treatment effectiveness and survival rate are worse than those in regions with developed economy and medical technology in China.2,3 The treatment effect of PLWH directly affects their quality of life. At present, the method widely used in the laboratory to evaluate the efficacy of treatment is the detection of HIV-1 viral load. However, with the change of treatment compliance, the viral load fluctuates greatly in a short time and changes rapidly. CD4(+) T cell is an important immune cell of the immune system. Therefore, CD4(+) T cells count can directly reflect the immune function of PLWH being the accurate indicator for PLWH immune system status.4 When CD4(+) T cells decrease to a certain extent, PLWH are more susceptible to a variety of disease5, If without timely treatment and control, mortality is extremely high. To avoid opportunistic infections, higher CD4(+) T cells level of PLWH in a long term is an important factor. It was observed that CD4(+) T cells level has been increasing in a slowly upward trend with the better quality of treatment. In this retrospective cohort study, we screened the PLWH newly reported in Sichuan Province from 2014 to 2018, who had failed treatment and tested for HIV-1 genotypic drug resistance during treatment, and analyzed the changes of CD4(+) T cell count and influencing factors of CD4(+) T cells recovery. In addition, CD4(+) T cells recovery in PLWH infected with CRF07_BC, CRF08_BC and CRF01_AE strains was found to have different characteristics during treatment.6,7 In addition to the prevalence of the above subtypes of HIV in Sichuan Province, a new subtype of HIV, named CRF85_BC8, has been found in the south of Sichuan Province in recent years. The purpose of this study was to investigate the immune progression and immune recovery of PLWH associated with different subtypes of virus.
Methods
Study Design and Participants
PLWH was screened from the Chinese Center for Disease Control and Prevention’s AIDS comprehensive prevention and control information system, including following three inclusion criteria: (1) From January 2014 to December 2018, the new reports of PLWH in Sichuan Province, (2) HIV-1 viral load level >1000 copies/mL was observed at least once during treatment and HIV-1 genotypic drug resistance testing was completed; (3) These PLWH patients received antiviral therapy and CD4(+) T cell count testing within 3 months after diagnosis. For these PLWH, their information is derived from the medical records in the system, including sociodemography (eg, age, sex, race, marital status, education, occupation), HIV/AIDS-related indicators and disease progression (eg, initial CD4(+) T cell count, recent CD4(+) T cell count, disease stage, death or not), treatment status (eg, Initial treatment protocol, recent treatment protocol, change of medication, duration of treatment) and major routes of HIV transmission (heterosexual, homosexual, intravenous drug use, other routes of transmission), at the time of initial diagnosis, PLWH were consulted about the route of HIV infection through a clinical history or epidemiological investigation. Drug resistance results and subtypes were obtained from the HIV-1 genotypic drug resistance detection database of Sichuan Provincial Center for Disease Control and Prevention.
The research plan was approved by the Ethics Committee of Sichuan Provincial Center for Disease Control and Prevention, and all the subjects followed the principle of informed consent. The study complies with the Declaration of Helsinki.
Sample Collection and Preservation
5mL whole blood of PLWH were collected with anti-coagulation Vacutainer of EDTA-K2 and mixed thoroughly for the determination of CD4(+) T cell count. The blood samples were centrifuged for 1600 × g 10 min within 6h. The plasma was separated and stored temporarily at −70 °C for HIV-1 viral load detection and drug resistance was further detected in samples with viral load >1000 copies/mL.
Laboratory Tests
CD4(+) T cell count, viral load and genotypic drug resistance testing procedures and interpretation of the results were carried out in accordance with the guidelines for CD4(+) T cell count testing and quality assurance (2013)9, the guidelines for HIV-1 viral load testing and quality assurance (2013)10 and the guidelines for HIV-1 genotypic drug resistance testing and quality assurance (2013)11 developed by the Chinese Center for Disease Control and Prevention. CD4(+) T cell count and viral load tests were performed by regional centers for Disease Control and prevention or Sentinel treatment hospitals, and drug resistance tests were performed by Sichuan Provincial Centers for Disease Control and prevention.
Subtype Analysis
The sequence results of HIV-1 were edited and spliced by Sequencher 5.0, and then the spliced results were corrected by Bioedit 7.0. Multiple sequences of the POL gene of HIV-1 Group M, Group O and Group N reference strains12 were performed to construct the ML phylogenetic tree with the corrected sequence Fasttree 2.0.0 and the generated file was imported into FigTree 1.4.2 to determine the subtype.
Statistical Analysis
In order to make the initial CD4(+) T cell count of PLWH subtypes as consistent as possible, we set the initial CD4(+) T cell count difference of 100 cells/μL as a subvariable. The difference between the CD4(+) T cell count median and the initial CD4(+) T cell count median of PLWH of 2021 year in each population was analyzed by case screening according to the study conditions. The last CD4(+) T cell count median before death was taken as the last CD4(+) T cell count median for dead patients. Rank sum test was used for statistical analysis, P < 0.05 was statistically significant; According to the national manual on free anti-viral drug treatment for AIDS (Fourth Edition),13 when the viral load is completely suppressed, the average annual increase of CD4(+) T cell count in infected people is 50–150 cells/μL. Therefore, CD4(+) T cell count raise over 50 cells/μL was set as the outcome variable in this study, PLWH socio-demographic information, HIV/AIDS related indicators and disease progression (initial CD4(+) T cell count, drug resistance, disease stage, virus subtype), treatment information, and HIV transmission route were set as independent variables, univariate and multivariate logistic regression models were used to screen the factors affecting PLWH CD4(+) T cell count increase ≥50 cells/μL, and univariate logistic regression analysis was performed for each variable, the variables of P < 0.2 were included in the multivariate logistic regression analysis with P < 0.05 meaning significantly different.
Result
Baseline Characteristics of Study Participants
A total of 116,625 PLWH data were extracted from the information system. During the treatment of PLWH, there were 9421 cases of PLWH with HIV-1 viral load>1000 CPs/mL and HIV-1 genotypic drug resistance test. There were 5023 cases (53.31%) of these PLWHs receiving treatment within 3 months after the onset of the disease, including 4977 cases (52.83%) with complete information (Figure 1). A total of 4977 patients with PLWH were enrolled, including 2358 (47.38%) with CRF07_BC, 1507 (30.28%) with CRF01_AE, 577 (11.59%) with CRF08_BC, 303 (6.09%) with CRF85_BC, 232 (4.66%) with other subtypes, which including 79 (1.58%) with subtype B, 55 (1.11%) of CRF55_01B, 20 (0.40%) of CRF 77_cpx, 12 (0.24%) of C subtype, 10 (0.2%) of CRF 52_01B, and 56 (1.13%) of a few CRF and unknown subtypes. Including 1658 (33.31%) came from Chengdu Plain, drug resistance 2124 (42.6%), 50 years or above 2624 (52.72%), males 3630 (72.94%), Hans ethnicity 4378 (87.96%), married or cohabiting 2671 (53.67%), primary education 2174 (43.68%), farmers 3471 (69.74%), infection route for heterosexual transmission 4478 (89.97%), the disease course is in AIDS stage 2662 (53.49%), initial CD4(+) T cell count in 200–300 cells/μL 1221 (24.53%), the initial treatment regimen was Tenofovir + Lamivudine + Nevirapine Wellen (TDF + 3TC + NVP/EFV) 3967 (79.71%). The most recent treatment regimen included the second-line regimen of lopinavir/ritonavir (LPV/r) 1498 (30.10%), during the course of treatment, 1754 (35.24%) had changed the treatment plan, 2209 (44.38%) had been treated for 24–48 months, and 1021 (20.51%) died (Table 1).
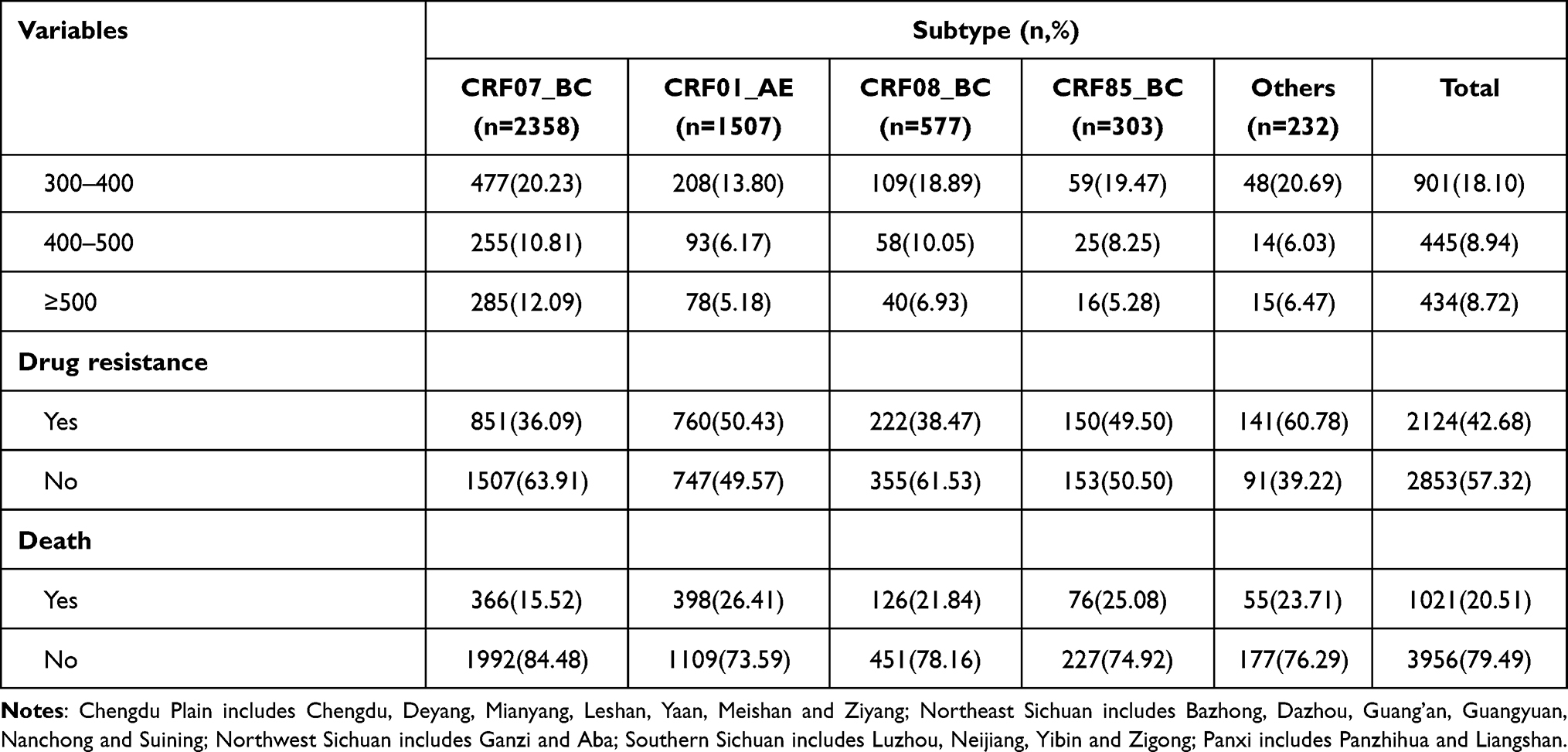 |
Table 1 Basic Information of Patients |
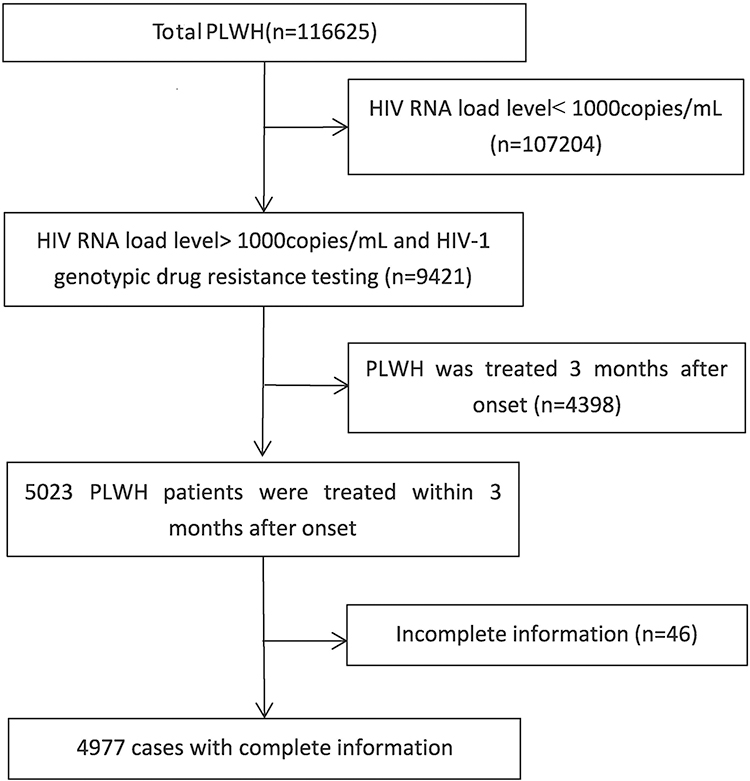 |
Figure 1 Sampling flowchart. |
Analysis of the change of CD4(+) T cell count median in the course of treatment. It was found that PLWH infected with CRF85_BC had a lower median increase in CD4(+) T cell count than PLWH infected with CRF01_AE, CRF07_BC, CRF08_BC and other subtypes (p < 0.05). Including the age is 15–29 years, Han nationality, junior high school culture, the infection route is heterosexual transmission, AIDS stage, the initial treatment program is TDF + 3TC + NVP/EFV, the treatment time is 48–72 months, the initial CD4(+) T cell count <200 cells/μL. In the following variables, Compared with PLWH infected with the other subtypes of virus, CD4(+) T cell count median was unchanged or decreased in CRF85_BC with HIV-1 subtypes (p < 0.05), including female, married or cohabiting, high school and above culture, farmer, the most recent treatment was TDF + 3TC + NVP/EFV, the treatment regimen was not changed, the treatment time was 24–48 months, the initial CD4(+) T cell count median at 200–300 cells/μL and drug resistance (Table 2).
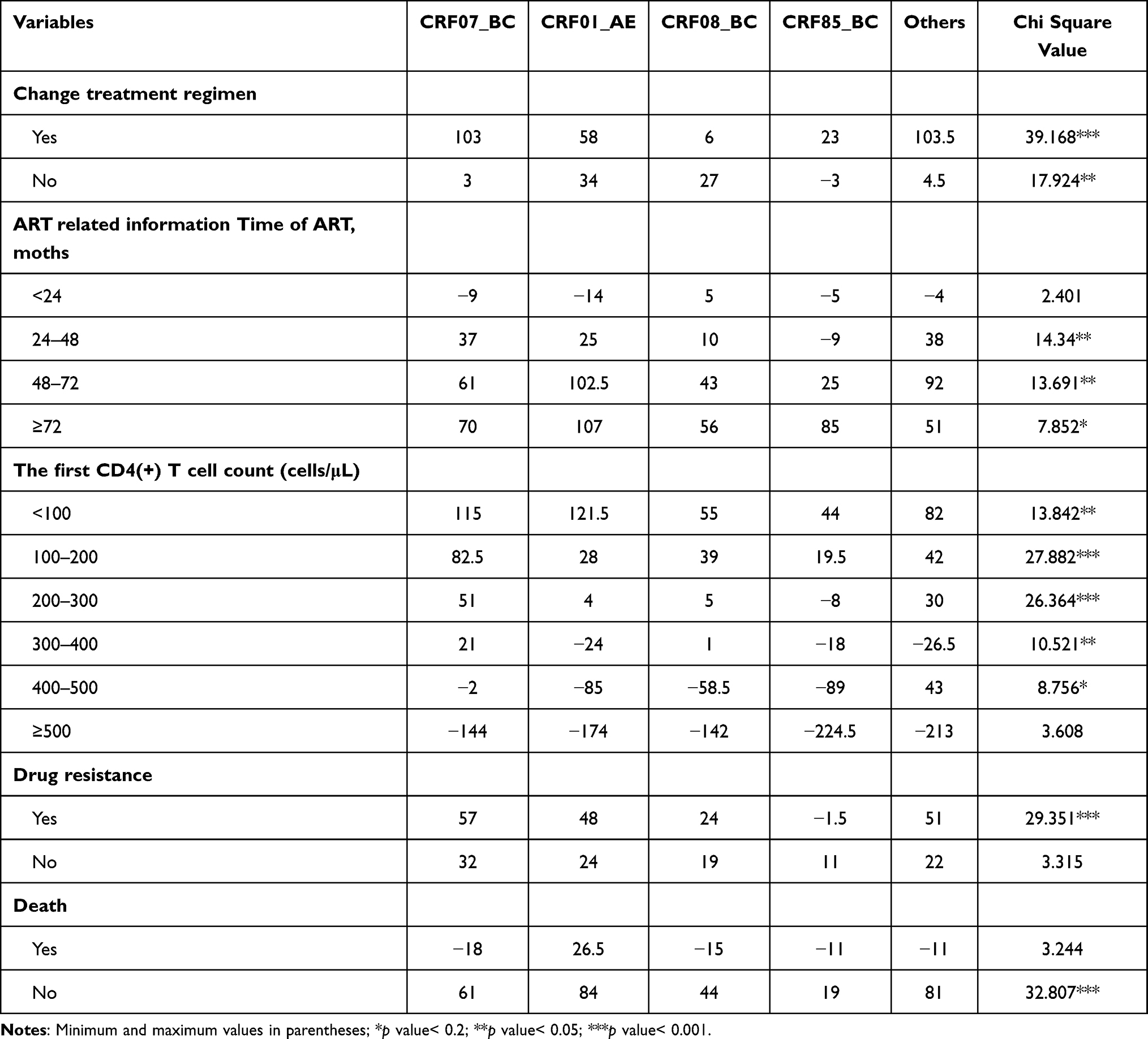 |
Table 2 Changes of Median CD4(+) T Cell Count During Treatment (Cells/μL) |
Analysis of factors influencing CD4(+) T cell count recovery during treatment. It was found that some factors could affect PLWH CD4(+) T cell count recovery by logistic regression model. The following variables are more likely to promote PLWH CD4(+) T cell count growth ≥50 cells/μL. Women (OR: 1.41, 95% CI: 1.22–1.64), Yi people (OR: 1.55, 95% CI: 1.17–2.06), married or cohabiting (OR: 1.27, 95% CI: 1.03–1.56), the education level is primary school (OR: 1.25, 95% CI: 1.04–1.51), junior high school (OR: 1.52, 95% CI: 1.22–1.88) and senior high school or above (OR: 2.30, 95% CI: 1.71–3.09), the initial treatment regimen was TDF + 3TC + NVP/EFV (OR: 1.32, 95% CI: 1.05–1.65), the most recent treatment regimen was TDF + 3TC + NVP/EFV (OR: 1.37, 95% CI: 1.03–1.83) and the second-line regimen with LPV/r (OR: 1.86, 95% CI: 1.22–2.84), the duration of treatment was 24–48 months (OR: 3.39, 95% CI: 2.69–4.28), 48–72 months (OR: 5.23, 95% CI: 4.09–6.69) and 72 months or more (OR: 5.89, 95% CI: 4.35–7.97). The following variables are more likely to prevent PLWH CD4(+) T cell count growth ≥50 cells/μL. Age ≥50 years (OR: 0.70, 95% CI: 0.54–0.91), AIDS stage (OR: 0.32, 95% CI: 0.26–0.40), infected with CRF01_AE strain (OR: 0.84, 95% CI: 0.72–0.98) and CRF85_BC strain (OR: 0.72, 95% CI: 0.55–0.95). Compared with the initial CD4(+) T cell count <100 cells/μL, the initial CD4(+) T cell count was 100–200 cells/μL (OR: 0.59, 95% CI: 0.48–0.72), 200–300 cells/μL (OR: 0.19, 95% CI: 0.15–0.25), 300–400 cells/μL (OR: 0.13, 95% CI: 0.10–0.17), 400–500 cells/μL (OR: 0.10, 95% CI: 0.07–0.13) and 500 cells/μL and above (OR: 0.04, 95% CI: 0.03–0.05) were more likely to prevent PLWH CD4(+) T cell count from increasing more than 50 cells/μL. (Table 3).
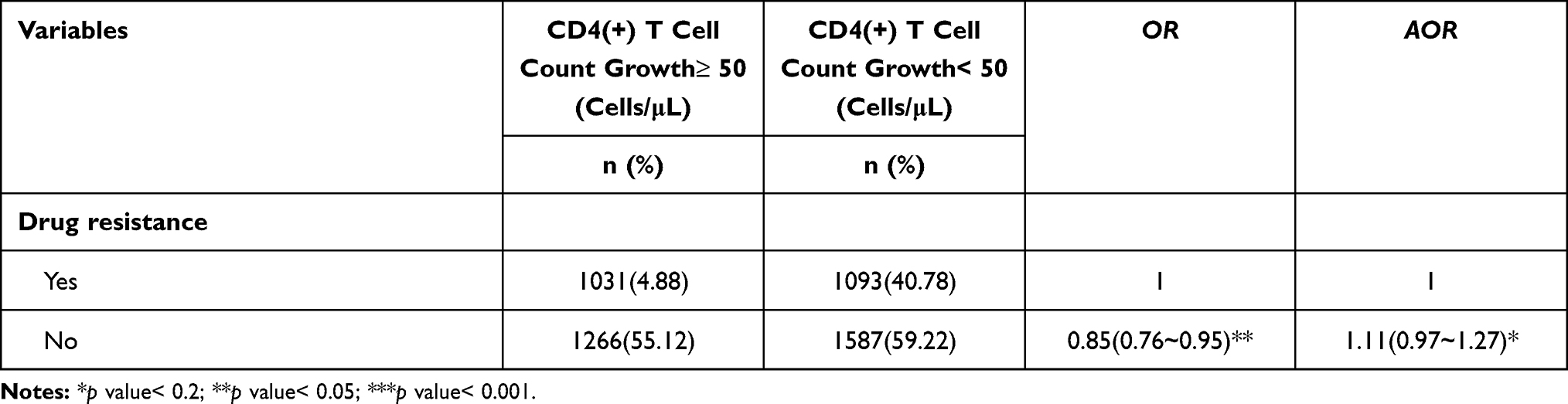 |
Table 3 Factors Influencing the Recovery of CD4(+) T Cell Count During Treatment |
Discussion
In 2014, the Joint United Nations Programme on HIV/AIDS proposed “three 90% prevention strategies”. In China’s 13th Five Year Plan of action to curb and combat AIDS, the “three 90%” targets were also proposed, of which the third target was to achieve a 90% success rate in PLWH treatment with antiviral therapy.14 Then, it is very important to explore the influencing factors of CD4(+) T cell progress in the treatment of AIDS patients and the differences of CD4(+) T cell progress. Responding to different subtype strains. This study was focused on PLWH with virological failure in the course of treatment. We obtained PLWH virus subtypes and previous drug resistance, in order to provide technical reference for improving the effect of follow-up treatment, the CD4(+) T cell recovery of the population and the related factors affecting the CD4(+) T cell recovery were analyzed.
We found that the CD4(+) T cell count median increase of PLWH infected with CRF85_BC was lower than that of PLWH infected with CRF01_AE, CRF07_BC and CRF08_BC. The subtype was found in Sichuan Province in 2014 when the province’s HIV molecular epidemiology survey was conducted, and was mainly found in southern Sichuan, especially in the elderly population in Yibin.8,15 Due to the short transmission time of this subtype of virus in this province, most studies are focused on HIV molecular transmission networks,16 while PLWH with this subtype of virus is monitored during treatment, such as immune cell progress and drug-resistant mutations being missing. This study suggests that in addition to strengthening the monitoring of molecular infectious disease and reducing the prevalence of CRF85_BC, the measures should be conducted to strengthen the monitoring of immune progress of PLWH infected with CRF85_BC, as to improve the treatment quality of PLWH.
It was also found that the median increase of CD4(+) T cell count in PLWH with initial CD4(+) T cell count at or above 300 cells/μL was lower than that in PLWH with initial CD4(+) T cell count below 300 cells/μL, especially with the higher the initial CD4(+) T cell count, the lower the median CD4(+) T cell count growth after treatment. The main reason is that high CD4(+) T cell level helps to reduce drug resistance and viral load, so it may reduce some PLWH tolerance to drug side effects, leading to stop taking drugs or reduce compliance, resulting in the reduction of CD4(+) T cell level; Second, the study population has experienced at least one virological failure, and the overall treatment compliance may be worse than PLWH which has maintained successful viral suppression, which resulted in reduce compliance when feeling better physically.
Through the analysis of the factors influencing the increase of CD4(+) T cell count, it was found that female, Yi people, married or cohabiting, primary school or above, and the initial treatment program was TDF + 3TC + NVP/EFV, the most recent treatment regimen was TDF + 3TC + NVP/EFV and the second-line regimen with LPV/r. Treatment duration of 24 months or more was a protective factor for increased CD4(+) T cell count growth. Women are less likely than men to stop treatment and have better adherence, ensuring long-term viral suppression and better immunity. In addition, women tend to have better health care seeking behaviour, higher levels of treatment and a lower risk of treatment failure;17 and women have lower body mass index, and they are more likely than men to maintain higher drug concentrations in their bodies, so they are more likely to achieve viral suppression that promotes CD4(+) T cell count growth;18 men are more likely than women to engage in unhealthy behaviors, such as smoking and drinking alcohol, which may aggravate antiviral drug’s liver toxicity, suppress immune system function.19 The Yi people population is mainly concentrated in Liangshan, and the 13th five-year plan has enhanced the treatment coverage and the treatment efficiency, and improved the treatment quality to a certain extent.20 When PLWH with good marital status suffers from the pain caused by disease, their spouses can give support and improve their sense of guilt and shame; However, PLWH who are single or divorced lack companionship and support from their partners, which can easily lead to shame, unwillingness to take the initiative to consult and poor treatment compliance.21 The higher the educational level, the better the ability to face aids and accept the knowledge related to the disease. The better the medical condition and living standard, the better the knowledge related to the disease and the higher the treatment compliance. TDF + 3TC + NVP/EFV is the first-line choice for the treatment of AIDS in China. Compared with the previous first-line Plan Containing Stavudine (D4T), TDF + 3TC + NVP/EFV has fewer side effects and promotes PLWH compliance. The composition of treatment regimens played a key role during the follow-up period, ie PLWH with a second-line treatment regimen containing LPV/r was more likely to improve treatment outcomes than PLWH with a first-line treatment regimen and this result is consistent with the results of a previous study in our province.22 In addition, the steady growth of CD4(+) T cell count was achieved with a longer treatment. It was found in previous study that PLWH treated for less than 12 months was more likely to fail virologically, leading to a decrease in CD4(+) T cell count, compared with PLWH treated for more than 12 months. pLWH had the highest mortality within 1 year after antiviral therapy.23 Therefore, standard treatment in the early stage of is to improve PLWH quality of life of effective measures.
The study found that the age of 50 years old, AIDS stage, infected with CRF01_AE and CRF85_BC, pre-treatment CD4(+) T cell count is higher will affect PLWH treatment process of CD4(+) T cell count growth. The results suggest that PLWH in the elderly is less effective than the young and middle-aged patients, which is related to the lower immune status of the elderly than the young and middle-aged. PLWH during the AIDS stage, its CD4(+) T cell count growth is not optimistic, these PLWH have more access to opportunistic infections, leading to more time at home or hospital, which will further increase the psychological burden of patients, leading to reduced compliance. This study found that PLWH infected with CRF01_AE had worse CD4(+) T cell count recovery than that infected with CRF07_BC, which was mainly due to the higher percentage of X4 gonotropic virus.6,7 In addition, the CD4(+) T cell count recovery rate of PLWH infected with CRF85_BC was lower than that of PLWH infected with CRF07_BC. As the subtype of the virus is currently mainly prevalent among the heterosexually transmitted elderly people in southern Sichuan,7 it is once again emphasized that the virus is needed to pay close attention of the health department. It is necessary to strengthen the prevention and control of AIDS among people infected with the virus, reduce the spread of the virus, and formulate effective measures to strengthen the treatment quality of PLWH. The study found that the percentage of CD4(+) T cell count increase of 50 cells/μL or more during treatment decreased with the increase of initial CD4(+) T cell count, because CD4(+) T cell count reached 500 cells/μL during treatment, it would enter the plateau stage, so CD4(+) T cell count growth curve will tend to smooth out gradually. However, this does not mean that low level CD4(+) T cell count in PLWH immune status can be significantly restored. Early studies have shown that CD4(+) T cell count increases when initial CD4(+) T cell count is below 350 cells/μL, but only up to 400–500 cells/μL after 6 years of treatment.4 Only when initial CD4(+) T cell count is above 350 cells/μL in PLWH, its CD4(+) T cell count is 829 cells/μL. Another reason is that the subjects in this study had at least one virological failure, and their overall treatment compliance may be at relatively low level, especially PLWH with high initial CD4(+) T cell count, probably because the immune condition at that time was relatively good and reduced the compliance to take medicine.
Limitations
In this study, PLWH were tested for HIV-1 drug resistance after HIV-1 virological failure in the course of treatment, so it can only reflect the recovery of CD4(+) T cell count in this population. In this study, CD4(+) T cell count was analyzed only in the initial and recent treatment of PLWH, with laboratory parameters and compliance during treatment not analyzed, which may bias the analysis of results.
Conclusion
Age, sex, ethnicity, marital status, educational level, disease status, treatment protocol, treatment duration, initial CD4(+) T cell count, and virus subtype are the factors that influence PLWH CD4(+) T cell count increase. In particular, PLWH infected with CRF85_BC virus has a poor recovery of CD4(+) T cell count in the course of follow-up treatment. The health department should formulate effective treatment measures according to the influencing factors and the characteristics of virus, improve the quality of life of PLWH and reduce the mortality.
Acknowledgments
We thank the Center for AIDS/STD Control and Prevention, Sichuan Center for Disease Control and Prevention to support data. We are also grateful to the editors and reviewers for their invaluable comments to improve this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was funded by the Science and Technology Project of Sichuan Provincial Health Committee (20PJ121); Sichuan Science and Technology program (2020YJ0449, 2022NSFSC1547). 2022 scientific research project of Sichuan Center for Disease Control and Prevention (zx202201, zx202112).
Disclosure
The authors declare that they have no competing interests.
References
1. Sun JP. Written at the closing year of the “three 90%” strategic goal for AIDS prevention and treatment. Chin J Prev Med. 2020;54(11):1180–1183. doi:10.3760/cma.j.cn112150-20200915-01204
2. Zeng YL, Tang HL, Li JM, et al. Survival analysis of people living with HIV/AIDS in Sichuan province, 1991–2017. Chin J Epidemiol. 2019;40(3):309–314. doi:10.3760/cma.j.issn.0254-6450.2019.03.010
3. Zeng YL, Yu H, Yang W, et al. Assessment of effectiveness of antiretroviral therapy in HIV-positive adults in Sichuan Province from 2003–2019. J Prev Med Inf. 2022;38(5):587–593.
4. Moore RD, Keruly JC. CD4+ cell count 6 years after commencement of highly active antiretroviral therapy in persons with sustained virologic suppression. Clin Infect Dis. 2007;44(3):441–446. doi:10.1086/510746
5. Chen ZQ, Liang L, Li BJ, et al. Analysis for the correlation between CD4+ cell counts and opportunistic in patients with HIV/AIDS. Hebei Med J. 2009;31(19):2552–2553. doi:10.3969/j.issn.1002-7386.2009.19.013
6. Zhangwen G, Feng Y, Kang L, et al. CRF01_AE and CRF01_AE cluster 4 are associated with poor immune recovery in Chinese patients under cART. Clin Infect Dis. 2020;8. doi:10.1093/cid/ciaa380
7. Jiang H, Lan G, Zhu Q, et al. Impacts of HIV-1 subtype diversity on long-term clinical outcomes in antiretroviral therapy in Guangxi, China. JAIDS. 2022;89(5):583–591. doi:10.1097/QAI.0000000000002906
8. Su L, Feng Y, Liang S, et al. The origin and spread of CRF85_BC, driven by heterosexual transmission among older people in Sichuan, China. BMC Infect Dis. 2020;20(1). doi:10.1186/s12879-020-05488-4
9. Chinese center for disease control and prevention. A guideline for CR4+T lymphocyte counting and quality assurance in people living with HIV/AIDS; 2013.
10. Chinese center for disease control and prevention. A guideline for HIV-1 viral load testing and quality assurance; 2013.
11. Chinese center for disease control and prevention. Guideline for HIV-1 genotyping drug resistance testing and quality assurance; 2013.
12. Simon F, Mauclere P, Roques P, et al. Identification of a new human immunodeficiency virus type I distinct from group M and group O. Nat Med. 1998;4(9):1032–1037. doi:10.1038/2017
13. Chinese center for disease control and prevention. The Fourth Edition of the National Free AIDS Antiviral Treatment Handbook. Bei Jing: People’s Health Publishing House; 2016.
14. General Office of the State Council. Action plan for containment and AIDS prevention in China in 13th five-year; 2017.
15. Su L, Yang H, Hu Y, et al. Molecular epidemiological study on HIV-1 in Sichuan Province in 2014. Chin J Aids Std. 2016;22(12):946–949.
16. Yuan D, Yu B, Liang S, et al. HIV-1 genetic transmission networks among people living with HIV/AIDS in Sichuan, China: a genomic and spatial epidemiological analysis. Lancet Reg Health West Pac. 2021;18:100318. doi:10.1016/j.lanwpc.2021.100318
17. Gupta A, Wood R, Kaplan R, et al. Prevalent and incident tuberculosis are independent risk factors for mortality among patients accessing antiretroviral therapy in South Africa. PLoS One. 2013;8(2):e55824. doi:10.1371/journal.pone.0055824
18. Tran DA, Wilson DP, Shakeshaft A, et al. Determinants of virological failure after 1 year’s antiretroviral therapy in Vietnamese people with HIV: findings from a retrospective cohort of 13 outpatient clinics in six provinces. Sex Transm Infect. 2014;90(7):538–544. doi:10.1136/sextrans-2013-051353
19. Lee MP, Zhou J, Messerschmidt L, et al. Impact of gender on long‐term treatment outcomes of highly active antiretroviral therapy (HAART) in the TREAT Asia HIV observational database. Aids Patient Care S Tds. 2015;29(5):229–231. doi:10.1089/apc.2014.0232
20. National Development and Reform Commission (NDRC), People’s Republic of China. The 13th five-year plan for economic and social development of the people’s republic of China. Available from: https://en.ndrc.gov.cn/policyrelease_8233/201612/P020191101482242850325.pdf.
21. Zhang YP. Influencing factors of stigma level in AIDS patients. Sichuan J Physiol Sci. 2021;43(3):419–422.
22. Liang S, Yang H, Ye L, et al. Efficacy of extended treatment and influencing factors of HIV drug resistance patients in Sichuan. J Prev Med Inf. 2018;34(7):898–907.
23. Yao SJ, Lv YN, Wang L, et al. The survival analysis in 7255 AIDS patients on antiretroviral therapy in Liaoning Province in 2003–2015. Chin J Dis Control Prev. 2016;20(12):1203–1207. doi:10.16462/j.cnki.zhjbkz.2016.12.005
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.