Back to Journals » Psychology Research and Behavior Management » Volume 18
Causal Relationship Between Depression, Sleep Disorders, and Constipation: A Mendelian Randomization and Mediation Analysis
Authors Wang JX, Wei KY, Lin W, Liu YJ
Received 24 March 2025
Accepted for publication 9 July 2025
Published 22 July 2025 Volume 2025:18 Pages 1611—1620
DOI https://doi.org/10.2147/PRBM.S529521
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Jun-Xi Wang,1,* Kai-Yan Wei,2,* Wei Lin,1 Yi-Juan Liu2
1Endoscope Center, The First Affiliated Hospital of Fujian Medical University, Fuzhou, 350005, People’s Republic of China; 2Department of Gastroenterology, The First Affiliated Hospital of Fujian Medical University, Fuzhou, 350005, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yi-Juan Liu, Department of Gastroenterology, The First Affiliated Hospital of Fujian Medical University, No. 20 Chazhong Road, Taijiang District, Fuzhou, 350005, People’s Republic of China, Tel +86 13599415881, Fax +86 0591-87981695, Email [email protected]
Objective: The study aims to investigate the causal relationship between depression, sleep disorders, and constipation using multivariable Mendelian randomization (MR) and mediation MR analysis. Additionally, the potential mediating effects of sleep disorders in the association between depression and constipation were evaluated.
Methods: Genome-wide association study (GWAS) data were utilized to identify genetic variants associated with depression, sleep disorders, and constipation as instrumental variables (IVs). The inverse-variance weighted (IVW) method was applied as the primary analytical approach. The mediating role of sleep disorders was assessed through multivariable MR and mediation MR analysis, and sensitivity analyses were conducted to assess the robustness of the findings.
Results: Depression was associated with a significantly increased risk of constipation (OR 1.26, 95% CI 1.11– 1.44, P = 0.00034, IVW). Reverse MR analysis did not demonstrate a significant effect of constipation on depression (P = 0.086). According to mediation MR analysis, sleep disorders significantly mediated the causal association between depression and constipation, with a mediation rate of 13%. Sensitivity analyses supported the consistency and robustness of the findings.
Conclusion: Findings from this study provide evidence of a causal relationship between depression and constipation, with sleep disorders serving as a partial mediator. These findings offer novel insights into the mechanisms of depression-related constipation, highlighting the potential role of sleep disturbances as a therapeutic target.
Keywords: constipation, depression, mediation, Mendelian randomization, sleep disorder
Introduction
Depression ranks among the most prevalent mental health disorders, with an estimated annual prevalence of approximately 7.2%, and continues to contribute significantly to global disease burden and mortality.1,2 Projections by the World Health Organization indicate that by 2030, depression will become the leading cause of global disease burden.3 The effects of depression extend beyond mental health, contributing to various physical health conditions, including sleep disorders and gastrointestinal disturbances such as constipation.
A strong association between depression and sleep disorders has been well-documented, with individuals experiencing depression frequently reporting sleep disturbances.4 Additionally, a link between depression and constipation has been observed.5 However, the causal pathways underlying the relationship between depression, sleep disorders, and constipation are not yet fully understood. While previous studies have investigated these associations, their findings have been limited by potential biases, including reverse causality and residual confounding. Furthermore, few studies have specifically examined the causal relationships among these three factors.
Mendelian randomization (MR) is an epidemiological approach that utilizes genetic variants as instrumental variables (IVs) to investigate causal relationships between clinical characteristics and disease phenotypes. This method assesses the effects of exposure factors on health outcomes by leveraging genetic variations. Since genetic variants are randomly classified during gametogenesis and are largely independent of environmental or lifestyle factors, MR is less susceptible to biases related to reverse causality and confounding. This characteristic provides a distinct advantage in controlling for confounding variables and mitigating reverse causation, thereby enhancing the reliability of research findings.6 Due to these methodological strengths, MR studies are often referred to as “nature’s randomized, double-blind trials” and serve as an important complement to randomized controlled trials (RCTs).
Given these advantages, the aim of the present study was to comprehensively examine the relationships among depression, sleep disorders, and constipation using MR analysis. Additionally, it was imperative in this study to elucidate potential causal pathways and assess whether sleep disorders mediate the effect of depression on constipation.
Materials and Methods
Research Design
A two-sample bidirectional MR analysis was conducted using publicly available summary datasets from genome-wide association studies (GWAS) of individuals of European ancestry to infer the causal relationship between depression and constipation. The research design is illustrated in Figure 1. Additionally, multivariable MR was performed to examine interaction effects among different variables, and mediation MR analysis was utilized to further investigate the mechanistic pathway linking depression and constipation.
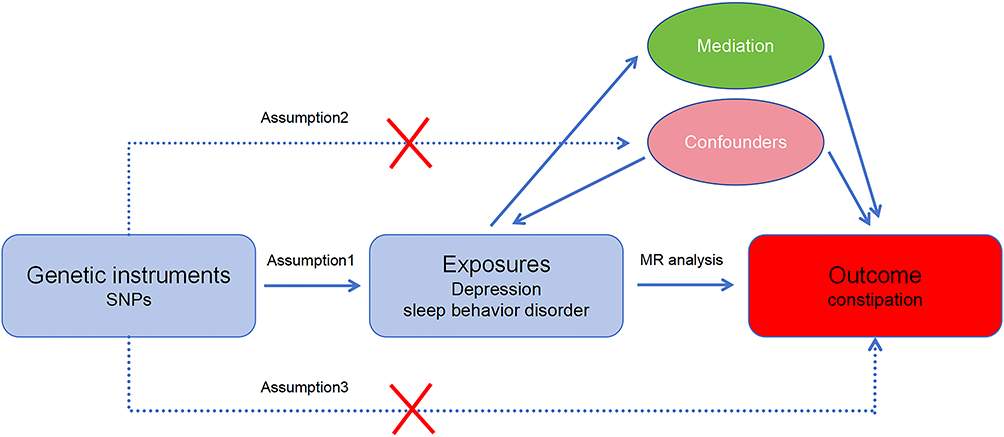 |
Figure 1 Study design. |
All original studies included in the analysis had received approval from their respective ethics standards committees. Therefore, no additional ethical approval or informed consent was required for this study. The analysis process adhered to the STROBE-MR guidelines.7
Data Sources
GWAS summary data were obtained from publicly available datasets provided by the Integrated Epidemiology Unit (https://gwas.mrcieu.ac.uk/). Genetic instruments for depression were derived from a study of 500,199 individuals of European ancestry, including 170,756 cases and 329,443 controls, conducted by the Psychiatric Genomics Consortium (PGC). Data on sleep disorders were sourced from a genome-wide summary analysis conducted in Finland, which recruited 216,700 participants (19,155 cases and 197,545 controls). GWAS data for constipation were also obtained from a Finland cohort, comprising 218,792 individuals (17,246 cases and 201,546 controls), with a total of 16,380,466 single nucleotide polymorphisms (SNPs). Additional details regarding data sources are provided in Supplementary Table 1.
Selection of Genetic Instrumental Variables
SNPs were utilized as IVs for MR analysis, adhering to the three fundamental assumptions of MR analysis:8 (1) The selected genetic variants must be strongly associated with the exposure factor (depression). To minimize bias, a threshold of p < 5×10−8 was applied for IV selection, and the F-statistic for each IV was required to exceed 10. (2) The instrumental variables should not be associated with any confounding factors that influence the relationship between the exposure and outcome. To address this, the study population was restricted to individuals of European ancestry. (3) The instrumental variables must influence the outcome solely through their association with the exposure, without horizontal pleiotropy.
Applying the p < 5×10−8 threshold and removing linkage disequilibrium (r2 = 0.001, 10,000 kb), a total of 49 SNPs associated with depression were selected, as detailed in Supplementary Table 2. The F-statistic for all selected SNPs exceeded 10, and the calculation method for the F-statistic followed previously established approaches.9,10
Data Analysis
All statistical analyses were performed using R software (version 4.2.1), with TwoSampleMR (version 0.5.7) and MRPRESSO (version 1.0) packages applied for MR analysis. When p value was < 0.05, it was considered statistically significant.
Two-sample MR analysis was initially conducted to investigate the causal effect of depression on constipation. The inverse-variance weighted (IVW) method served as the primary analytical approach for estimating the association between depression and constipation.11 To assess the robustness of the findings, sensitivity analyses were conducted using alternative MR methods, including the weighted median method,12 MR-Egger regression,13 and MR-PRESSO.14 The presence of horizontal pleiotropy was evaluated using MR-Egger regression, where a statistically significant intercept term indicated potential pleiotropic effects. Cochran’s Q test was performed to determine heterogeneity among SNPs, with a statistically significant result suggesting substantial heterogeneity in the analysis. A leave-one-out analysis was conducted to assess whether any single SNP disproportionately influenced the results.
The association between depression and constipation was expressed as an odds ratio (OR) with a 95% confidence interval (CI). A value of p ≤ 0.05 was interpreted as evidence supporting a potential causal relationship. Scatter plots, funnel plots, and forest plots were generated to visualize the results.
Given that causal estimates from univariable MR analysis reflect the overall impact of exposure on outcomes, multivariable MR analysis was performed to estimate the direct causal effect, considering potential mediating factors. The difference between causal estimates obtained from univariable MR (total effect) and multivariable MR analysis (direct causal effect) suggested that the causal pathway was at least partially mediated by an intermediate factor.15,16 Specifically, multivariable MR mediation analysis was employed to estimate the proportion of mediation by sleep disorders in the relationship between depression and constipation.17
Results
Causal Relationship Between Depression and Constipation
The causal relationship between depression and constipation was assessed using MR analysis, with depression as the exposure and constipation as the outcome. A total of 49 SNPs associated with depression were selected (Supplementary Table 2), with all IVs demonstrating F-statistic values greater than 10 (ranging from 30.3 to 78.4), indicating that weak instrument bias was unlikely. These variables were subsequently used to estimate the causal relationship between depression and constipation.
The results indicated that individuals with depression had a 1.26-fold higher risk of constipation compared to those without depression (inverse-variance weighted [IVW] method: OR 1.26, 95% CI 1.11–1.44, p = 0.00034), as shown in Figure 2. Sensitivity analyses were performed using the weighted median and MR-PRESSO methods, both of which supported the primary findings. MR-PRESSO further confirmed an increased risk of constipation among individuals with depression (OR 1.27, 95% CI 1.12–1.43, p = 0.00044). The p-value of 0.667 derived from the MR-Egger intercept indicated no evidence of pleiotropy. Additionally, both MR-PRESSO and leave-one-out plots detected no outliers, and neither heterogeneity nor pleiotropy test statistics reached statistical significance, as shown in Figure 3. Reverse MR did not demonstrate a significant relationship between constipation and depression (p = 0.086), as detailed in Supplementary Table 3.
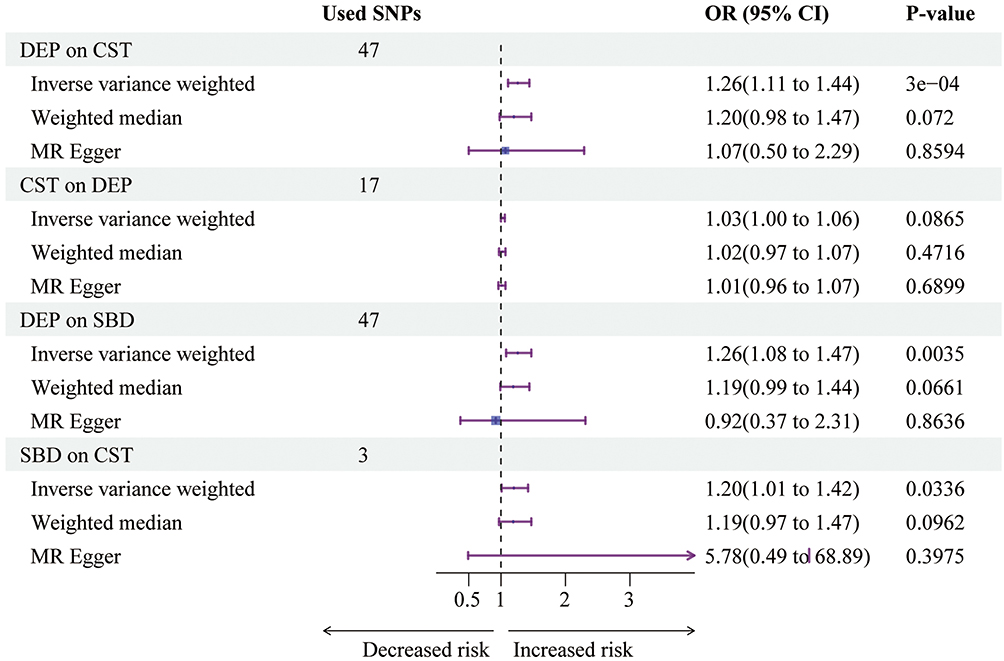 |
Figure 2 Causal relationship between depression, sleep behavior disorder, and constipation. A p < 0.05 was considered statistically significant. Abbreviations: DEP, Depression; CST, Constipation; SBD, Sleep behavior disorder; CI, Confidence Interval; OR, Odds Ratio. |
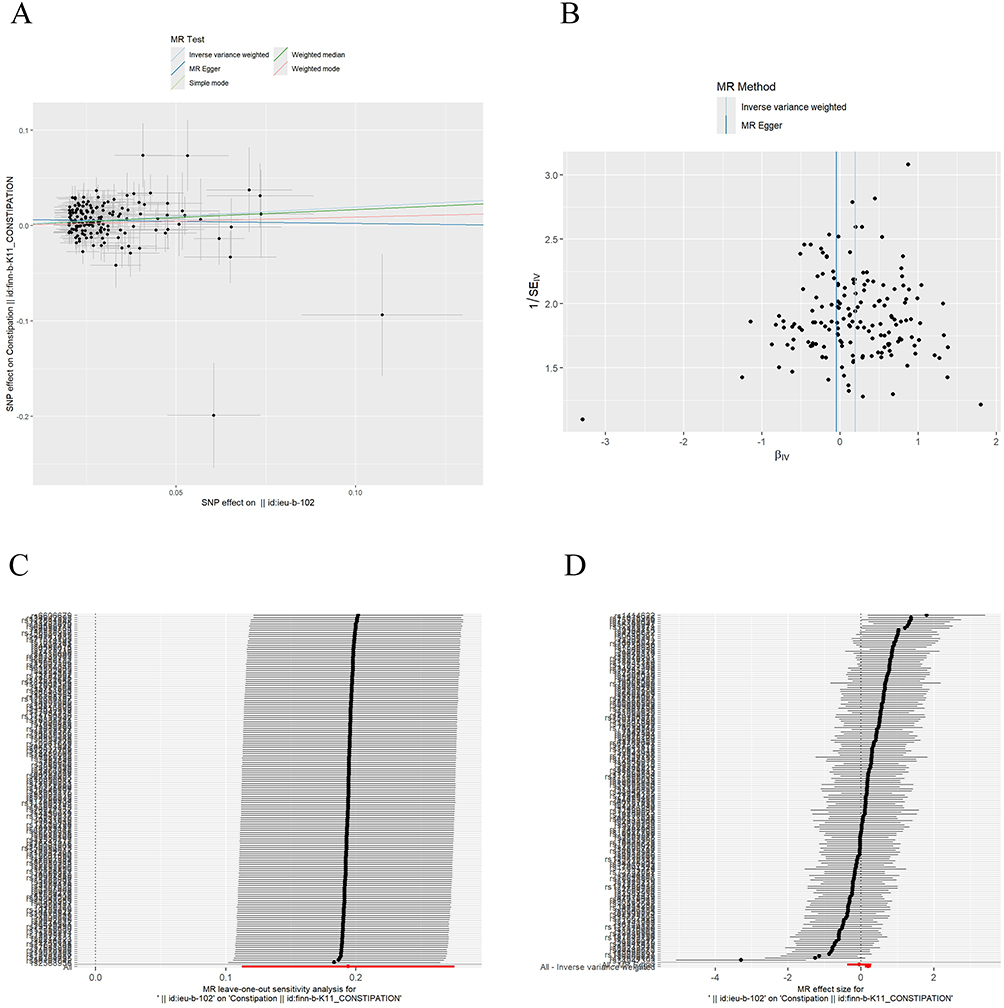 |
Figure 3 Visualization of Mendelian randomization (MR) analysis for depression and constipation. (A) Pleiotropy analysis. (B) Funnel plot. (C) Stability analysis using the leave-one-out method. (D) Forest plot displaying MR effect sizes obtained from MR-Egger and IVW methods. Abbreviation: MR, Mendelian randomization. |
To further minimize the influence of confounding factors and horizontal pleiotropy, multivariable MR analysis was performed (Supplementary Table 4). After adjusting for the influence of sleep disorders, the association between depression and constipation remained statistically significant (IVW: OR 1.23, 95% CI 1.08–1.40, p = 0.0021). However, after adjusting for depression, the direct causal relationship between sleep disorders and constipation was not statistically significant (IVW: OR 1.13, 95% CI 0.98–1.30, p = 0.0813), as shown in Figure 4.
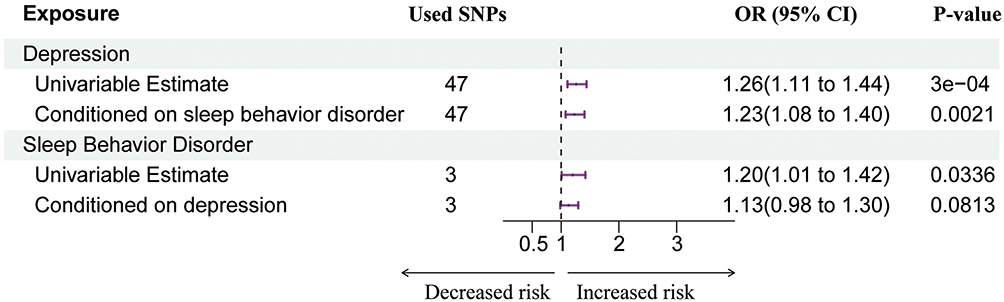 |
Figure 4 Multivariate Mendelian randomization analysis using the inverse variance-weighted method to investigate the relationships among depression, sleep behavior disorder, and constipation. A p < 0.05 was considered statistically significant. Abbreviations: CI, Confidence Interval; OR, Odds Ratio. |
Additionally, mediation analysis was conducted to determine whether sleep disorders mediated the causal relationship between the exposure variable (depression) and the outcome (constipation). The results indicated that the total effect of depression on constipation was 0.23 (p = 0.000349, Supplementary Table 3), while the direct effect of multivariable MR analysis (beta_direct) was 0.20 (p = 0.002089, Supplementary Table 4). Mediation analysis further demonstrated that sleep disorders significantly mediated the causal association between depression and constipation, with a mediation rate of 13%, as shown in Figure 5.
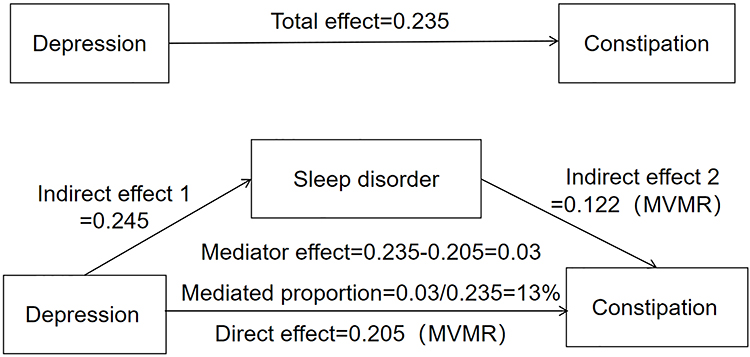 |
Figure 5 Mediation effect of sleep disorders in the causal relationship between depression and constipation. |
Discussion
The findings demonstrated a significant association between depression and constipation, with evidence suggesting a causal relationship, thereby supporting the research hypothesis. Mediation analysis further indicated that sleep disorders functioned as a key mediating variable in the causal pathway linking depression to constipation. This study was the first to employ mediation MR analysis to evaluate the potential mediating role of sleep disorders in the relationship between depression and constipation.
The findings of this study have significant implications for understanding the comprehensive impact of depression. A significant association between depression and constipation was observed, consistent with previous research, supporting the hypothesis of a correlation between these conditions.5 Clinically, constipation in individuals with depression is often attributed to the use of antidepressant medications. A meta-analysis reported a significantly higher incidence of constipation among individuals receiving antidepressants compared to those receiving a placebo; however, medication use represents only one contributing factor.18
Individuals with depression frequently exhibit somatic symptoms, such as delayed colonic transit, which may result in defecation disorders. A complex neural network exists between the brain and the gastrointestinal system, and depression has been proposed to influence this brain-gut axis through the release of specific factors, such as adrenaline and cortisol, which regulate gastrointestinal motility and increase susceptibility to gastrointestinal disorders.19 For instance, corticotropin-releasing factor has been identified as a key mediating factor between emotional regulation and digestive tract motor function, acting directly on the autonomic nervous system and playing a role in bowel habits and gastrointestinal motility.20 Furthermore, individuals with depression often experience reduced appetite and altered dietary habits, leading to inadequate intake of dietary fiber and fluids, thereby increasing the risk of constipation.21
Conversely, individuals with constipation have demonstrated a higher prevalence of depression, anxiety, and other psychiatric disorders. Recent research suggests that gut microbiota play a crucial role in the development of depression among individuals with functional constipation.22 The gut microbiome influences brain function through various pathways, such as endocrine (cortisol), immune (cytokines), and neural mechanisms (vagus nerve, enteric nervous system, spinal nerves), contributing to the regulation of the microbiota-gut-brain axis.23 Additionally, individuals with constipation have been reported to exhibit a lower abundance of short-chain fatty acid-producing bacteria, such as Clostridium and Lactobacillus species. Short-chain fatty acids play a role in modulating serotonin (5-hydroxytryptamine) synthesis and secretion in the intestine, influencing neuronal development, and regulating emotions through neural signaling pathways.24,25
In summary, the relationship between depression and constipation is complex and may involve bidirectional influences. Constipation in patients with depression is often attributed to the use of antidepressant medications. However, medication use is only one factor, as patients with depression frequently exhibit somatic symptoms. A deficiency of serotonin (5-HT) in the central nervous system of patients with depression may lead to reduced gut motility, resulting in constipation. Depression can activate the hypothalamic-pituitary-adrenal axis (HPA axis), releasing stress hormones such as cortisol, which inhibit intestinal motility and cause dysbiosis of the gut microbiota. Conversely, patients with constipation have a higher prevalence of depression, anxiety, and other psychiatric disorders. The gut microbiota plays a significant role in this context. The gut microbiota exerts a central influence on neuroendocrine, immune, and metabolic functions through the brain-gut axis. Short-chain fatty acids (SCFAs) and neurotransmitters (such as serotonin, 5-HT) produced by the microbiota can affect brain function via the vagus nerve or the bloodstream. Patients with depression often have dysbiosis of the gut microbiota, characterized by an increase in pro-inflammatory bacteria (such as Bacteroides) and a decrease in anti-inflammatory bacteria (such as butyrate-producing Faecalibacterium and Coprococcus). This imbalance may exacerbate neuroinflammation and depressive symptoms by triggering inflammatory responses (such as cytokine release) or by disrupting the intestinal barrier. Probiotics, prebiotics, or fecal microbiota transplantation may alleviate depressive symptoms by restoring microbial balance, enhancing 5-HT signaling pathways, or reducing inflammation. For example, L. paracasei NCU-04 may improve depressive behavior in constipated mice by promoting 5-HT synthesis in the colon. Through MR, there is evidence in this study supporting the causal impact of depression on constipation, and offering a novel perspective on the interplay between these interconnected conditions.
Depression and sleep disorders are closely interconnected conditions, with research evidence indicating that both are associated with an increased risk of chronic constipation. However, there have been limited studies that have examined the role of sleep disorders in the relationship between depression and constipation. The importance of sleep disorders in modulating the causal influence of depression on constipation through mediation analysis is highlighted in this study. These findings are consistent with those of Abbasi et al, who reported that depression is a major determinant of sleep disorders.26 Despite this, the gut microbiota, medications, neurodegenerative changes, and psychosocial factors also constitute a multifactorial explanation, the consistency of which can be partly elucidated by common neuroendocrine and immune mechanisms. The HPA axis dysregulation associated with depression not only leads to constipation but is also closely related to sleep disorders. Both depression and sleep disorders can alter the gut microbiota (eg, a reduction in Lactobacillus), inhibit colonic 5-HT synthesis, and thereby exacerbate constipation. The low-grade intestinal inflammation associated with depression may simultaneously affect sleep rhythms and gut motility through cytokine release. Therefore, the 5-HT system may be a key link between emotional disorders and gastrointestinal function.
Existing literature has established a strong correlation between sleep quality and constipation, with mechanisms believed to be similar to those underlying irritable bowel syndrome, including alterations in gut microbiota.27 Sleep disorders may interfere with circadian rhythms, leading to abnormal basal motility patterns in the colon, reducing the frequency and intensity of intestinal peristalsis, and thereby increasing the risk of constipation. Sleep disorders may also alter the composition or activity of the gut microbiota, affecting the signaling of the enteric nervous system and further inhibiting gut motility. Complement C4, as an immune regulatory factor, plays an important role in the association between sleep disorders and constipation. Studies have found that low levels of complement C4 are associated with an increased risk of sleep disorders, while patients with habitual constipation often have abnormalities in inflammatory factors such as complement C4, suggesting that the immune system may influence sleep and gut function through the gut microbiota–immune–brain axis. Additionally, psychological stress, anxiety, or depression may exacerbate both sleep disorders and constipation simultaneously. In summary, the association between sleep disorders and constipation is characterized by multifactorial and bidirectional regulation, involving the interplay of physiological rhythms, the brain-gut axis, immune inflammation, and psychological factors. Sleep disturbances have also been linked to abnormal gastrointestinal transit, which may result from immune-mediated responses to alpha-synuclein in submucosal colon nerve fibers or ganglia of the colon, as well as dysregulated abnormal expression and function of α2A adrenergic receptors in the distal ileum.28
However, caution should be exercised when considering pharmacological interventions for sleep disorders. From a cross-sectional study, a significant association between hypnotic drug use and constipation was established (OR, 2.33; 95% CI, 1.30–4.16; p = 0.004), potentially due to the adverse effects of these medications on gastrointestinal tract movement.29 Given the complexities of pharmacological treatment, biological therapies may offer a more favorable approach for managing sleep disorders while reducing the risk of constipation in individuals with depression.
A key strength of this study was the establishment of a causal relationship between depression and constipation using the MR method, while also identifying sleep disorders as a key mediating variable in this pathway. These findings may provide insights for the development of novel treatment strategies, highlighting the importance of addressing sleep disturbances in the management of constipation, particularly in individuals with depression.
Additionally, this study offers a foundation for further investigation into the biological mechanisms linking depression, sleep disorders, and constipation. Future research should focus on exploring the underlying neurobiological and immunological pathways involved in these associations, as well as assessing the effectiveness of various treatment strategies aimed at improving sleep quality, alleviating depression, and managing constipation.
The findings of this study have significant implications for enhancing public health awareness and formulating relevant policies. Depression and constipation are prevalent health concerns that substantially affect individuals’ quality of life and occupational functioning. A comprehensive investigation into their associations and underlying mechanisms may provide clinicians with valuable insights for improving diagnostic and therapeutic strategies, ultimately contributing to better patient outcomes.
Furthermore, government agencies and public health institutions should prioritize education and awareness campaigns regarding depression and constipation, promoting early recognition and the adoption of preventive measures.
However, certain limitations should be acknowledged. The MR analysis was restricted to individuals of European ancestry, and the generalizability of these findings to other populations requires further validation.
Conclusion
Multivariable MR and mediation analysis were utilized in this study to demonstrate that depression increases the risk of constipation through the mediating effect of sleep disorders. These findings carry important implications for clinical practice and public health for understanding the underlying mechanisms linking depression and constipation, improving diagnostic and therapeutic strategies, and enhancing patient quality of life. Future research should further investigate the biological mechanisms underlying the association between depression and constipation and conduct additional interventional studies to develop more effective treatment approaches.
Abbreviations
GWAS, Genome-Wide Association Studies; MR, Mendelian Randomization; IVW, Inverse-Variance Weighted; MVMR, Multivariable Mendelian Randomisation; OR, Odds Ratio; CI, Confidence Interval; RCT, Randomized Controlled Trial; STROBE-MR, Strengthening the Reporting of Observational Studies in Epidemiology using Mendelian Randomization; PGC, Psychiatric Genomics Consortium; SNP, Single Nucleotide Polymorphism; IV, Instrumental Variable; DEP, depression; CST, constipation; SBD, sleep behavior disorder.
Data Sharing Statement
All data generated or analysed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Ethics Approval and Consent to Participate
Our study used publicly available GWAS data from European-ancestry individuals. The original studies had ethics approvals and informed consent. Our Institutional Review Board at Fujian Medical University confirmed this study is exempt from additional approval under China’s Article 32 of the Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects (Feb 18, 2023), as it uses de-identified data.
Acknowledgments
We are particularly grateful to all the people who have given us help on our article.
Funding
Fujian Provincial Health Technology Project (No.2024GGA030). Startup Fund for Scientific Research of Fujian Medical University (No.2023QH1099).
Disclosure
The authors declare that they have no competing interests.
References
1. Lim GY, Tam WW, Lu Y, Ho CS, Zhang MW, Ho RC. Prevalence of depression in the community from 30 countries between 1994 and 2014. Sci Rep. 2018;8(1):2861. Erratum in: Sci Rep. 2022 Sep 1;12(1):14856. doi: 10.1038/s41598-022-19021-x. PMID: 29434331; PMCID: PMC5809481. doi:10.1038/s41598-018-21243-x
2. Nestler EJ, Barrot M, DiLeone RJ, Eisch AJ, Gold SJ, Monteggia LM. Neurobiology of depression. Neuron. 2002;34(1):13–25. PMID: 11931738. doi:10.1016/s0896-6273(02)00653-0
3. Malhi GS, Mann JJ. Depression. Lancet. 2018;392(10161):2299–2312. PMID: 30396512. doi:10.1016/S0140-6736(18)31948-2
4. Park SC, Kim JM, Jun TY, et al. Prevalence and clinical correlates of insomnia in depressive disorders: the CRESCEND study. Psychiatry Invest. 2013;10(4):373–381. PMID: 24474986; PMCID: PMC3902155. doi:10.4306/pi.2013.10.4.373
5. Adibi P, Abdoli M, Daghaghzadeh H, et al. Relationship between depression and constipation: results from a large cross-sectional study in adults. Korean J Gastroenterol. 2022;80(2):77–84. PMID: 36004635. doi:10.4166/kjg.2022.038
6. Sun X, Liu B, Liu S, et al. Sleep disturbance and psychiatric disorders: a bidirectional Mendelian randomisation study. Epidemiol Psychiatr Sci. 2022;31:e26. PMID: 35465862; PMCID: PMC9069588. doi:10.1017/S2045796021000810
7. Skrivankova VW, Richmond RC, Woolf BAR, et al. Strengthening the reporting of observational studies in epidemiology using mendelian randomisation (STROBE-MR): explanation and elaboration. BMJ. 2021;375:n2233. PMID: 34702754; PMCID: PMC8546498. doi:10.1136/bmj.n2233
8. Burgess S, Thompson SG. CRP CHD genetics collaboration. avoiding bias from weak instruments in Mendelian randomization studies. Int J Epidemiol. 2011;40(3):755–764. PMID: 21414999. doi:10.1093/ije/dyr036
9. Huang YF, Zhang WM, Wei ZS, et al. Causal relationships between gut microbiota and programmed cell death protein 1/programmed cell death-ligand 1: a bidirectional Mendelian randomization study. Front Immunol. 2023;14:1136169. PMID: 36969249; PMCID: PMC10034163. doi:10.3389/fimmu.2023.1136169
10. Zhao H, Han X, Zhang X, et al. Dissecting causal associations of diet-derived circulating antioxidants with six major mental disorders: a Mendelian randomization study. Antioxidants. 2023;12(1):162. PMID: 36671024; PMCID: PMC9855039. doi:10.3390/antiox12010162
11. Slob EAW, Burgess S. A comparison of robust Mendelian randomization methods using summary data. Genet Epidemiol. 2020;44(4):313–329. PMID: 32249995; PMCID: PMC7317850. doi:10.1002/gepi.22295
12. Bowden J, Davey Smith G, Haycock PC, Burgess S. Consistent estimation in Mendelian randomization with some invalid instruments using a weighted median estimator. Genet Epidemiol. 2016;40(4):304–314. PMID: 27061298; PMCID: PMC4849733. doi:10.1002/gepi.21965
13. Burgess S, Thompson SG. Interpreting findings from Mendelian randomization using the MR-Egger method. Eur J Epidemiol. 2017;32(5):377–389. Erratum in: Eur J Epidemiol: PMID: 28527048; PMCID: PMC5506233. doi:10.1007/s10654-017-0255-x
14. Verbanck M, Chen CY, Neale B, Do R. Detection of widespread horizontal pleiotropy in causal relationships inferred from Mendelian randomization between complex traits and diseases. Nat Genet. 2018;50(5):693–698. Erratum in: Nat Genet. 2018 Aug;50(8):1196. PMID: 29686387; PMCID: PMC6083837. doi:10.1038/s41588-018-0099-7
15. Sanderson E, Davey Smith G, Windmeijer F, Bowden J. An examination of multivariable Mendelian randomization in the single-sample and two-sample summary data settings. Int J Epidemiol. 2019;48(3):713–727. Erratum in: Int J Epidemiol. 2020 Jun 1;49(3):1057. PMID: 30535378; PMCID: PMC6734942. doi:10.1093/ije/dyy262
16. Relton CL, Davey Smith G. Two-step epigenetic Mendelian randomization: a strategy for establishing the causal role of epigenetic processes in pathways to disease. Int J Epidemiol. 2012;41(1):161–176. PMID: 22422451; PMCID: PMC3304531. doi:10.1093/ije/dyr233
17. Carter AR, Sanderson E, Hammerton G, et al. Mendelian randomisation for mediation analysis: current methods and challenges for implementation. Eur J Epidemiol. 2021;36(5):465–478. PMID: 33961203; PMCID: PMC8159796. doi:10.1007/s10654-021-00757-1
18. Oliva V, Lippi M, Paci R, et al. Gastrointestinal side effects associated with antidepressant treatments in patients with major depressive disorder: a systematic review and meta-analysis. Prog Neuropsychopharmacol Biol Psychiatry. 2021;109:110266. PMID: 33549697. doi:10.1016/j.pnpbp.2021.110266
19. Stasi C, Bellini M, Gambaccini D, et al. Neuroendocrine dysregulation in irritable bowel syndrome patients: a pilot study. J Neurogastroenterol Motil. 2017;23(3):428–434. PMID: 28460516; PMCID: PMC5503293. doi:10.5056/jnm16155
20. Mönnikes H, Tebbe JJ, Hildebrandt M, et al. Role of stress in functional gastrointestinal disorders. Evidence for stress-induced alterations in gastrointestinal motility and sensitivity. Dig Dis. 2001;19(3):201–211. PMID: 11752838. doi:10.1159/000050681
21. Hepsomali P, Groeger JA. Diet, sleep, and mental health: insights from the UK biobank study. Nutrients. 2021;13(8):2573. PMID: 34444731; PMCID: PMC8398967. doi:10.3390/nu13082573
22. Liang J, Zhao Y, Xi Y, et al. Association between depression, anxiety symptoms and gut microbiota in Chinese elderly with functional constipation. Nutrients. 2022;14(23):5013. PMID: 36501044; PMCID: PMC9740187. doi:10.3390/nu14235013
23. Asadi A, Shadab Mehr N, Mohamadi MH, et al. Obesity and gut-microbiota-brain axis: a narrative review. J Clin Lab Anal. 2022;36(5):e24420. PMID: 35421277; PMCID: PMC9102524. doi:10.1002/jcla.24420
24. Kelly JR, Clarke G, Cryan JF, Dinan TG. Brain-gut-microbiota axis: challenges for translation in psychiatry. Ann Epidemiol. 2016;26(5):366–372. PMID: 27005587. doi:10.1016/j.annepidem.2016.02.008
25. Yang C, Hu T, Xue X, et al. Multi-omics analysis of fecal microbiota transplantation’s impact on functional constipation and comorbid depression and anxiety. BMC Microbiol. 2023;23(1):389. PMID: 38057705; PMCID: PMC10701952. doi:10.1186/s12866-023-03123-1
26. Byrne EM, Timmerman A, Wray NR, Agerbo E. Sleep disorders and risk of incident depression: a population case-control study. Twin Res Hum Genet. 2019;22(3):140–146. PMID: 31203833. doi:10.1017/thg.2019.22
27. Baniasadi N, Dehesh MM, Mohebbi E, Hayatbakhsh Abbasi M, Oghabian Z. Assessing the sleep quality and depression-anxiety-stress in irritable bowel syndrome patients. Arq Gastroenterol. 2017;54(2):163–166. PMID: 28273275. doi:10.1590/S0004-2803.201700000-08
28. St Louis E, Boeve B. REM sleep behavior disorder: diagnosis, clinical implications, and future directions. Mayo Clin Proc. 2017;92(11):1723–1736. doi:10.1016/j.mayocp.2017.09.007
29. Ueki T, Nagai K, Mizukami Y, et al. Cross-sectional study on relationship between constipation and medication in consideration of sleep disorder. Yakugaku Zasshi. 2011;131(8):1225–1232. PMID: 21804327. doi:10.1248/yakushi.131.1225
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.