Back to Journals » International Journal of Women's Health » Volume 17
Causal Associations Between Oral Microbiota and Gestational Diabetes Mellitus: A Two-Sample Mendelian Randomization Study
Authors Jin H, Wang Y, Li H, Cheng Y, Ma Y
Received 28 March 2025
Accepted for publication 1 August 2025
Published 30 August 2025 Volume 2025:17 Pages 2777—2791
DOI https://doi.org/10.2147/IJWH.S531088
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Hui Jin,* Yapei Wang,* Hongbin Li, Yinqin Cheng, Yumin Ma
Department of Internal Medicine, The Second People’s Hospital of Nantong, Nantong, 226000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yumin Ma, Department of Internal Medicine, The Second People’s Hospital of Nantong, Nantong, 226000, People’s Republic of China, Tel +86-13861995848, Email [email protected]
Background: Gestational diabetes mellitus (GDM) is associated with adverse pregnancy outcomes. The oral microbiota, influenced by genetic factors, may play a role in GDM development, but the causal association remains unclear.
Methods: We employed a two-sample Mendelian randomization (MR) approach using Genome-Wide Association Study (GWAS) data on GDM from FINN cohort data (ID: finngen_R10_GEST_DIABETES) and GWAS data on the Oral microbiota from the Danish ADDITION-PRO cohort. We screened SNPs significantly associated with Oral microbiota abundance as instrumental variables (IVs) and assessed their association with GDM risk. The study primarily used an inverse variance weighting (IVW) approach and further applied MR-Egger regression, weighted median, and weighted mode methods for robustness testing. Sensitivity analyses were conducted to evaluate the impact of heterogeneity and pleiotropy, including MR-Egger, MR-PRESSO, Cochran’s Q, and leave-one-out methods.
Results: We identified 267 IVs associated with Oral microbiota abundance. IVW analysis revealed a positive causal association between Genus Schaalia and GDM risk (OR = 1.03, 95% CI: 1.01– 1.06, P = 0.02) and a negative association between Genus Haemophilus and GDM risk (OR = 0.96, 95% CI: 0.93– 1.00, P = 0.034). Sensitivity analyses confirmed the robustness of these two results, showing no evidence of heterogeneity or pleiotropy.
Conclusion: Our study provides evidence for a causal association between Genus Schaalia and Haemophilus and GDM risk. This highlights the potential role of the Oral microbiota in GDM pathogenesis and suggests potential targets for GDM prevention and treatment.
Keywords: oral microbiota, gestational diabetes mellitus, Mendelian randomization, causal inference, European descent
Background
Gestational Diabetes Mellitus (GDM) is a disorder of glucose metabolism diagnosed for the first time during pregnancy and is among the most prevalent pregnancy complications, with a rising global prevalence.1 Clinical characteristics of GDM include increased insulin resistance and impaired glucose control, which not only heighten the risk of complications such as preterm birth and preeclampsia in pregnant women but may also result in fetal macrosomia and neonatal hypoglycemia.2 The development of GDM is associated with a multitude of factors, including genetics, obesity, age, ethnicity, and lifestyle.3 However, given the complexity and multifactorial nature of gestational diabetes mellitus (GDM), the current understanding remains incomplete. It necessitates continued exploration to identify new and previously unrecognized risk factors.
Oral microbiota is the community of bacteria, fungi, viruses, and protozoa that reside within the oral cavity. Oral microbiota may contribute to the development of GDM through multiple pathways. It can disrupt blood glucose metabolism, for instance, by triggering inflammation through the Toll-like receptor 2 (TLR2) pathway with certain bacterial overgrowth, thus impairing insulin signaling and causing glucose level fluctuations.4 Additionally, it can heighten systemic inflammation due to local oral inflammation, increasing GDM risk.5 Observational studies have revealed significant differences in the composition of oral microbiota between GDM patients and healthy pregnant women.6 Another study found that pregnant women with poor oral hygiene were at a higher risk of developing GDM.7 These findings suggest that oral microbiota may play a significant role in the pathogenesis of GDM. Inflammatory cytokines are key mediators in the interplay between oral microbiota dysbiosis and the development of GDM. Alterations in the oral microbiota of pregnant women with GDM often create a pro-inflammatory environment, which is characterized by increased levels of specific cytokines. These cytokines can influence both local oral health and systemic metabolic processes, contributing to the pathogenesis of GDM.8,9
Mendelian Randomization (MR) is a method of causal inference based on genetic principles. The central assumption of MR is that genetic variants can be used as “instrumental variables (IVs)” which can randomly assign exposure factors, thereby avoiding the influence of confounding factors and reverse causality inherent in traditional observational studies, and providing a more reliable assessment of the causal association between exposure factors and disease.10 Previous studies have used a two-sample MR to reveal causal associations between the gut microbiota and type 1 diabetes.11 However, the associations by which the oral microbiota may influence the pathogenesis of GDM remain unclear, and further studies are needed to explore these associations.
This study employs a two-sample Mendelian Randomization (MR) approach, integrating Genome-Wide Association Study (GWAS) data, to investigate the causal relationship between the oral microbiome and gestational diabetes mellitus (GDM). By identifying specific oral microorganisms that influence GDM pathogenesis, the research aims to optimize prevention strategies and advance personalized medicine. It also enhances diagnostic tools and innovates treatment options, potentially introducing microbial interventions as novel therapeutic targets. Furthermore, this work provides a scientific basis for public health policies and fosters interdisciplinary collaboration, ultimately improving health outcomes for pregnant women and their offspring.
Methods
This study was reported following the STROBE-MR checklist.12 The checklist is available as Supplementary Materials.
Study Design
In our study, we carefully selected single-nucleotide polymorphisms (SNPs) from Genome-Wide Association Studies (GWAS) to serve as IVs. As shown in Figure 1, our two-sample Mendelian Randomization (MR) investigation is specifically focused on exploring the causal associations between GDM and oral microbiota-related characteristics, based on three core assumptions:13 The relevance assumption: There is a strong association between the IVs and the oral microbiota factor under investigation. The independence assumption: The IVs are not associated with any confounding variables that might affect the oral microbiota or the GDM. The exclusion restriction assumption: the IVs affect the GDM only through their influence on the oral microbiota factor, without any other causal pathways. The need for ethical approval was waived by the committee of the Second People’s Hospital of Nantong because the study used publicly available aggregated data that did not allow the re-identification of the original participants, as supported by Article 32 of the Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects dated February 18, 2023, China, as well as various legislations around the globe.14
 |
Figure 1 Flowchart of the two-sample Mendelian randomization analysis for the association between salivary microbial exposure and gestational diabetes. The flowchart illustrates the steps involved in conducting a two-sample Mendelian randomization (MR) analysis to investigate the causal relationship between specific salivary microbial taxa and the risk of gestational diabetes, while accounting for potential confounders. In this legend, bold text is used to emphasize and highlight the key components and crucial steps of the analytical process depicted in the flowchart, facilitating quick identification of the core elements of the MR analysis. |
Data Sources
The outcome data for GDM were obtained from the FINN cohort data (ID: finngen_R10_GEST_DIABETES), which consisted of 14,718 cases and 215,592 controls. The exposure data were sourced from a published article15 that detailed the association between 43 oral microbial communities and host genotypes. These data were based on saliva samples from 610 adults in the Danish ADDITION-PRO cohort, who had the V4 region of the 16S rRNA gene sequenced on the Illumina HiSeq 2500 platform. Forty-three GWAS statistical abstracts were validated after stringent quality control measures. All study data were from European populations, with more specific details provided in Table 1.
 |
Table 1 Detailed Information for the GWAS Data |
Instrumental Variable Selection
In this study, the selection of IVs was based on the following criteria: (1) SNPs significantly associated with the whole genome of the oral microbiota were first identified with a threshold of P < 5 * 10−6.16 (2) Only SNPs with a minor allele frequency (MAF) greater than 0.01 were retained. (3) SNPs showing linkage disequilibrium (LD) were excluded using a threshold of R2 < 0.001 and a window size of 10,000kb. (4) If the selected IV was not present in the summary statistics of the results, a SNP with a strong LD (R2 > 0.8) to the IV was identified as a substitute and replaced with it.17 5) An F value was calculated for each SNP in the IV to assess its strength and to mitigate possible bias caused by weak IVs associated with the exposure factor. The F value was calculated as F = R2 * (N-2) / (1-R2), where R2 is the exposure variance explained by the SNP in the IV. An F-value greater than 10 is required.12 To ensure that the effective alleles are indeed from the same allele, we aligned the oral microbiota and GDM datasets, thereby removing any SNPs with discordant alleles and those with allele frequencies in the intermediate range.
MR Analyses
This study primarily employed the inverse variance weighted (IVW) method for analysis,18 calculating the odds ratio (OR) and its 95% confidence interval (CI) to evaluate the causal association between exposure and outcome risk. The IVW method, as the preferred approach for interpreting MR results, calculates the weighted average of effect sizes using the inverse variance of each SNP as weights. To assess the robustness of the results, we also used MR-Egger regression,19 weighted median,20 and weighted mode methods.21 MR-Egger regression considers the intercept term, providing accurate causal effect estimates even in the presence of pleiotropic bias. The weighted median method assumes that half of the IVs are valid, analyzing the causal association between exposure and outcome. All analyses were conducted using the “TwoSampleMR” in the R software package version 4.0.5, and the results were visualized with scatter plots and sensitivity analysis graphs.
Sensitivity and Pleiotropy Analysis
Sensitivity analysis was performed to detect potential pleiotropy in MR studies. We assessed the heterogeneity among IVs using Cochran’s Q test,22 with a P-value greater than 0.05 indicating low heterogeneity, suggesting that the estimates of IVs are randomly varied and have a minimal impact on the IVW results. Considering that the pleiotropy of genetic variants might affect the estimation of effects, we used MR-Egger regression to explore the presence of horizontal pleiotropy. An intercept close to zero or statistically insignificant in the MR-Egger regression suggests the absence of pleiotropy. Additionally, we employed the MR Pleiotropy RESidual Sum and Outlier (MR-PRESSO) method to detect possible outliers and re-estimated the causal associations after their removal to correct for horizontal pleiotropy.23 A leave-one-out analysis was conducted to evaluate the robustness and consistency of the results.
Result
Selection of IVs
In this study, we used IV analysis to gain insight into the oral microbiota community. After screening, we identified a total of 267 IVs associated with the abundance of the oral microbiota community and computed the corresponding F-statistics for each taxonomic unit. The mean of these F-statistics ranged from 21.51 to 27.10, with the minimum values ranging from 21.15 to 22.63, and the maximum values ranging from 21.51 to 38.10. To ensure the robustness of our analytical results, we specifically replaced SNPs inconsistent with summary data with suitable proxy SNPs in the analysis of oral microbiota community abundance (Table 2). For more detailed information, please refer to Table S1.
 |
Table 2 Information for Instrument Variable (IV) |
Mendelian Randomization Analysis
This study employed an MR approach to investigate the causal association between oral microbiota and GDM. The IVW analysis revealed a positive causal association between Genus Schaalia and GDM risk (Table 3 and Figure 2, OR = 1.03, 95% CI: 1.01–1.06; P=0.02), and a negative association between Genus Haemophilus and GDM risk (Table 3 and Figure 3, OR = 0.96, 95% CI: 0.93–1.00, P=0.034). However, no significant causal associations were identified between other oral microbiota and the risk of GDM.
 |
Table 3 Genetics Predicts Associations Between Oral Microbiota and the Risk of Gestational Diabetes |
 |
Figure 2 The association between Genus Schaalia and the risk of gestational diabetes is presented in (A) a forest plot, (B) a leave-one-out sensitivity analysis, (C) a scatter plot, and (D) a funnel plot. |
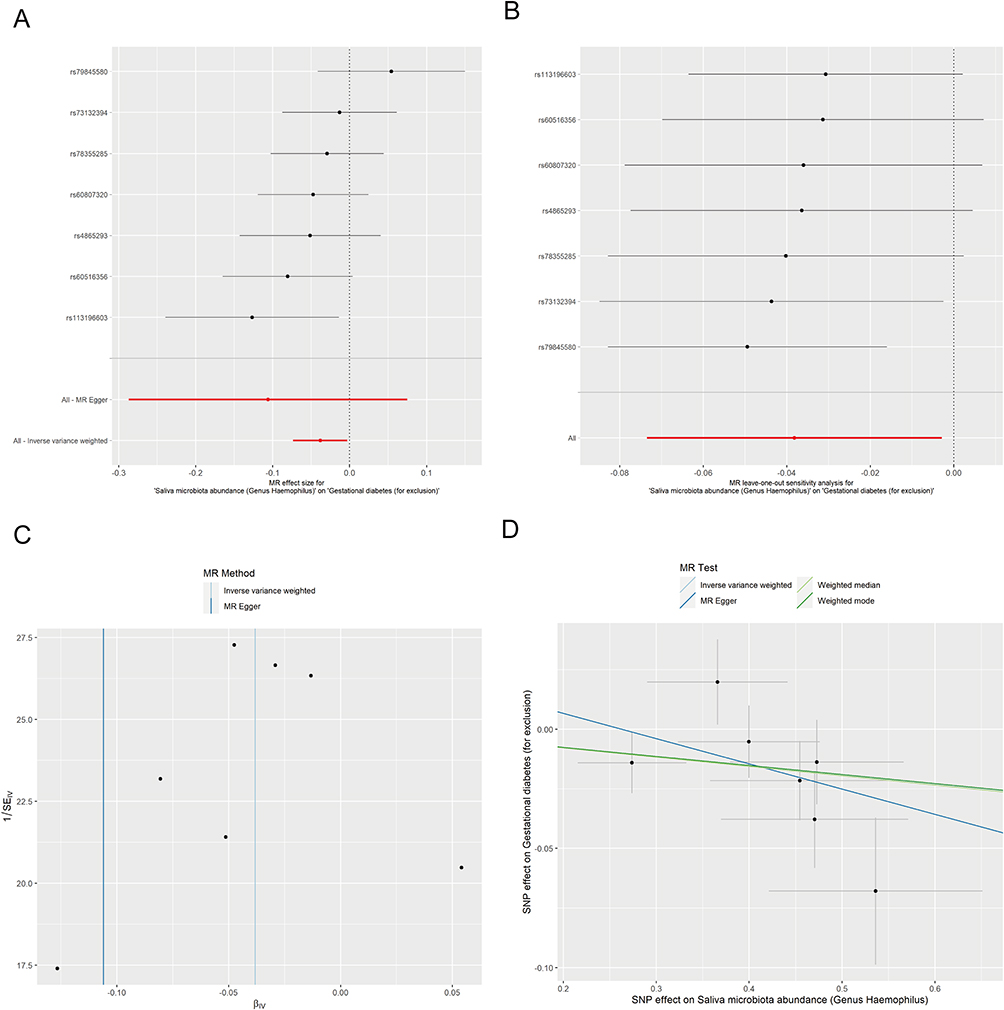 |
Figure 3 The association between Genus Haemophilus and the risk of gestational diabetes is presented in (A) a forest plot, (B) a leave-one-out sensitivity analysis, (C) a scatter plot, and (D) a funnel plot. |
Sensitivity Analysis
A sensitivity analysis was performed to determine the reliability of the IVW results. The MR-Egger indicated no pleiotropic effects in the analysis (Table 4, P > 0.05). The Cochran Q test (Table 4) for heterogeneity showed no heterogeneity in the MR analysis between Genus Schaalia and Genus Haemophilus and GDM (P > 0.05) (Table 2). However, the MR analysis between Genus Neisseria, Genus Porphyromonas, and Species micronuciformis and GDM exhibited heterogeneity (P<0.05) (Table 4). Pleiotropy and heterogeneity disappeared after the exclusion of outlier SNPs for Species micronuciformis and Genus Neisseria identified by MR-PRESSO (Tables 4 and 5). Notably, after the removal of abnormal SNPs, the results did not change, remaining consistent with those obtained before the sensitivity analysis (Table 3).
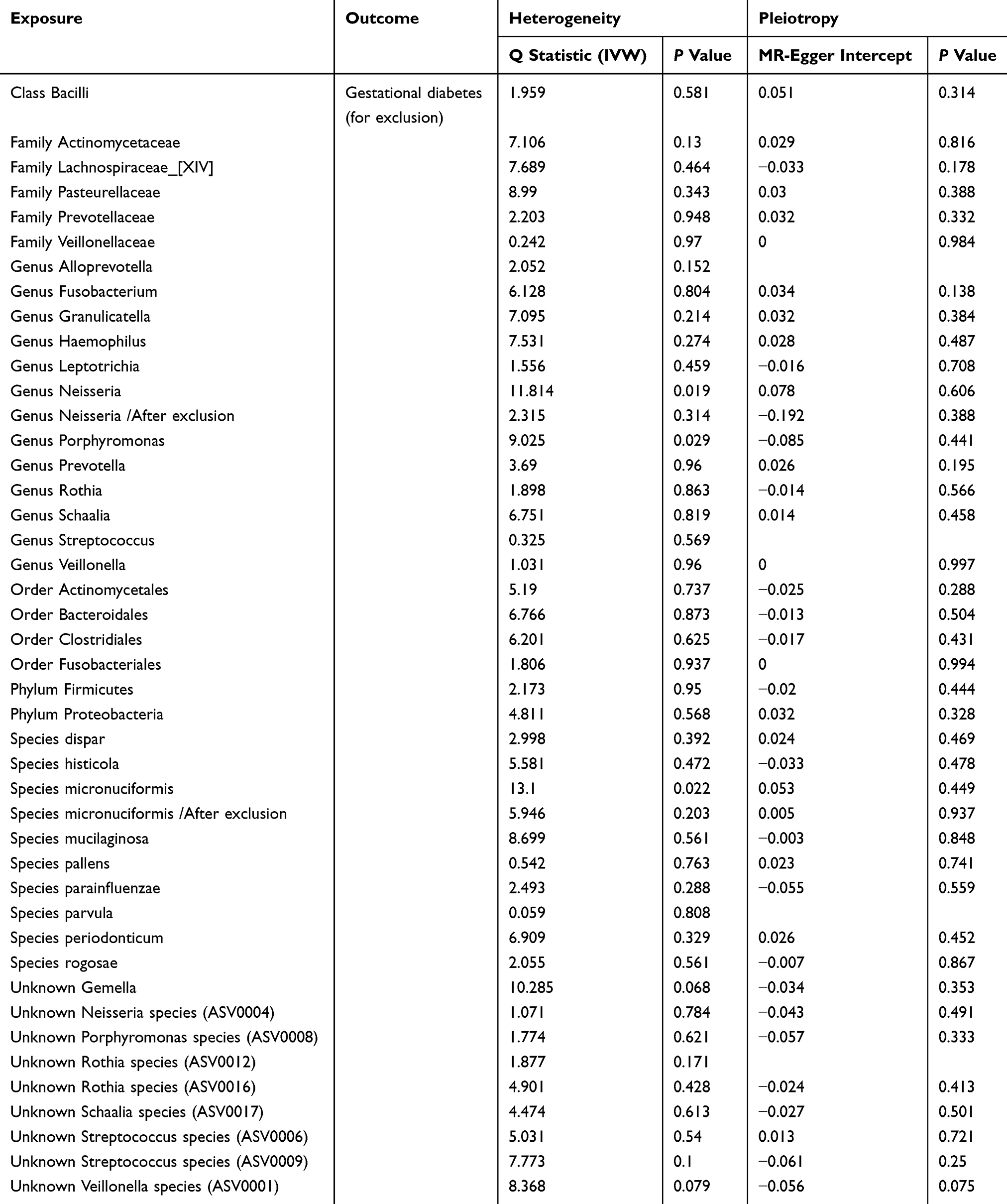 |
Table 4 Heterogeneity Tests and Pleiotropy Tests for Instrumental Variables |
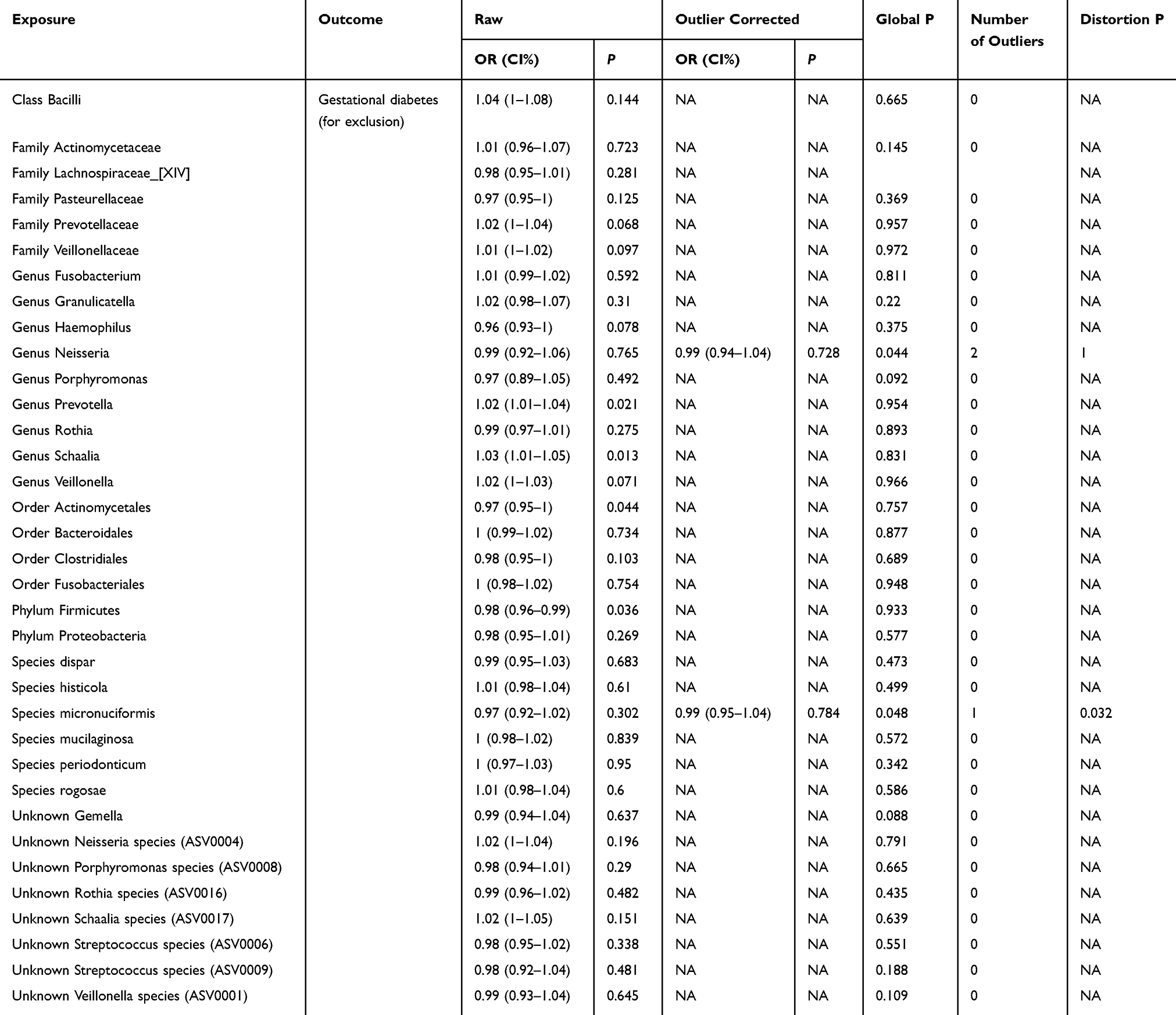 |
Table 5 MR-PRESSO Results |
Discussion
This study employed a two-sample MR approach to reveal the potential causal association between the oral microbiota and gestational GDM. The findings revealed a positive association between the genus Schaalia and the risk of GDM, while the genus Haemophilus was negatively associated with GDM risk. This finding suggests potential targets for future preventive and therapeutic strategies.
Schaalia bacteria, Gram-positive and facultative anaerobic microorganisms, predominantly colonize the oral ecosystems of humans and other animals. They play a pivotal role in biofilm formation, modulating host immune responses, and interacting with other microbes, which closely ties them to the pathogenesis of various infectious diseases.24 Schaalia bacteria are commonly found as commensals in the oral cavity and other mucosal sites. While typically harmless, Schaalia species can become pathogenic when mucosal barriers are breached, leading to inflammatory responses, inducing the production of inflammatory cytokines.25,26 Recent research indicates that in women with impaired glucose tolerance (IGT), a precursor to GDM, there is a significant reduction in gut microbiota diversity, along with an increase in the abundance of specific microbial species such as Schaalia turicensis. These alterations in microbial composition are closely associated with the development of IGT.27 This finding is consistent with our findings suggesting that the dysbiosis of the oral Schaalia genus may be associated with an increased risk of GDM. Therefore, future research should delve into the specific role of Schaalia bacteria in the development of GDM and reveal more about the biological mechanisms of the disease, while also assessing the potential of the Schaalia genus as a target for the prevention and treatment of GDM.
Haemophilus, a group of gram-negative, facultative anaerobic bacteria, resides on the mucosal surfaces of humans.28 They are well-known for their role in both localized and systemic infections, and their involvement in inflammation is central to their disease-causing potential and to trigger inflammation.29,30 The study of the association between GDM and the oral microbiota has revealed a connection, with significant differences in β-diversity observed in the gut microbiota of pregnant women with GDM compared to controls, characterized by an increase in Haemophilus species and a decrease in the α-diversity of the oral microbiota.31 Other research has shown a notable rise in the relative abundance of Haemophilus among women with GDM.32 This increase may be related to the metabolic status of patients with GDM, as Haemophilus was associated with fasting blood glucose and lipid levels in participants.33 Specifically, the rise in Haemophilus may be linked to the production of short-chain fatty acids, changes in incretin hormones, bile acid homeostasis, and the deficiency of peroxisome proliferator-activated receptor γ, which may affect insulin sensitivity and glucose metabolism.34 These findings suggest that changes in the oral microbial Haemophilus profile could serve as a non-invasive biomarker for monitoring GDM during pregnancy. Future research needs to further explore the mechanism of Haemophilus in GDM and how oral microbiota regulation can prevent and treat GDM.
Oral dysbiosis promotes local inflammation in periodontal tissues, leading to the production and release of pro-inflammatory cytokines such as TNF-α, IL-6, and CRP. They play central roles in mediating the association between oral microbiota dysbiosis and GDM. These cytokines are produced in response to pathogenic oral bacteria, enter systemic circulation, and contribute to insulin resistance and glucose intolerance. A feedback loop exists where hyperglycemia and inflammation perpetuate each other, worsening both oral and metabolic health in pregnancy. TNF-α and IL-6 are known to antagonize insulin signaling, impairing glucose uptake and promoting insulin resistance (a central feature of GDM). Chronic elevation of these cytokines disrupts carbohydrate metabolism, increasing the risk of glucose intolerance and the development of GDM.8 This mechanistic understanding highlights the importance of oral health and inflammation control in the prevention and management of GDM.8,9
This study used SNPs significantly associated with oral microbiota abundance as instrumental variables, which are controlled by genetic factors and unaffected by lifestyle and environmental influences.15 Thus, the MR method can effectively circumvent confounding biases inherent in traditional observational studies, providing a more accurate assessment of the causal association between the oral microbiota and GDM. However, MR also has its limitations, as its validity depends on the choice of instrumental variables. Weak associations or pleiotropy between the selected instruments and the exposure can lead to biased results.35 In addition, this study, which is based primarily on data from European populations, may have limitations when applied to other populations. Therefore, subsequent studies should aim for validation and in-depth analysis in larger sample sizes.
Future research could further investigate the causal association between the oral microbiota and GDM and delve into its underlying mechanisms. For example, mechanistic studies through cellular and animal experiments could explore the specific pathways by which Schaalia and Haemophilus influence GDM. Moreover, the development of drugs targeting specific bacterial species for the prevention and treatment of GDM could be pursued. Clinical trials could assess the impact of probiotic or antibiotic interventions on the prevention and treatment of GDM and explore the optimal intervention strategies.
Conclusions
The results of this study indicate a causal association between the oral microbiota and GDM risk, particularly involving the genera Haemophilus and Schaalia. This provides new insights for the prevention and treatment of GDM and suggests that oral health may play a significant role in the occurrence and progression of GDM.
Abbreviations
GDM, Gestational diabetes mellitus; MR, Mendelian randomization; GWAS, Genome-Wide Association Study; IVs, Instrumental variables; IVW, Inverse variance weighting; TLR2, Toll-like receptor 2; SNPs, Single-nucleotide polymorphisms; MR, Mendelian Randomization; MAF, Minor allele frequency; LD, Linkage disequilibrium.
Data Sharing Statement
All data generated or analysed during this study are included in this published article.
Ethics Approval and Consent to Participate
The study was submitted to the ethics committee of the Second People’s Hospital of Nantong, China. The need for ethical approval was waived by the committee because the study used publicly available aggregated data that did not allow the re-identification of the original participants, as supported by Article 32 of the Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects dated February 18, 2023, China, as well as various legislations around the globe.14
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by 2022 Nantong Basic Science Research and Social Livelihood Science and Technology Plan Project (mandatory) F3/Contact mechanism research in the pathophysiological process of diabetes cognitive impairment (No. JC1202209) and 2022 Youth Project of Nantong Health Commission “Research on Molecular Mechanism of Lilalutide Improving Painful diabetes Neuropathy Based on CX3CL1 Signal Pathway” (No. QN2022035).
Disclosure
The authors declare that they have no competing interests.
References
1. Sweeting A, Wong J, Murphy HR, Ross GP. A Clinical Update on Gestational Diabetes Mellitus. Endocrine Rev. 2022;43(5):763–793. doi:10.1210/endrev/bnac003
2. Kc K, Shakya S, Zhang H. Gestational diabetes mellitus and macrosomia: a literature review. Ann Nutr Metab. 2015;66(2):14–20. doi:10.1159/000371628
3. Giannakou K, Evangelou E, Yiallouros P, et al. Risk factors for gestational diabetes: an umbrella review of meta-analyses of observational studies. PLoS One. 2019;14(4):e0215372. doi:10.1371/journal.pone.0215372
4. Chang Y-R, Cheng W-C, Hsiao Y-C, et al. Links between oral microbiome and insulin resistance: involvement of MAP kinase signaling pathway. Biochimie. 2023;214(Pt B):134–144. doi:10.1016/j.biochi.2023.06.013
5. Kleinstein SE, Nelson KE, Freire M. Inflammatory Networks Linking Oral Microbiome with Systemic Health and Disease. J Dent Res. 2020;99(10):1131–1139. doi:10.1177/0022034520926126
6. Zhang X, Wang P, Ma L, et al. Differences in the oral and intestinal microbiotas in pregnant women varying in periodontitis and gestational diabetes mellitus conditions. J Oral Microbiol. 2021;13(1):1883382. doi:10.1080/20002297.2021.1883382
7. Pukkila J, Mustaniemi S, Lingaiah S, et al. Increased Oral Care Needs and Third Molar Symptoms in Women with Gestational Diabetes Mellitus: a Finnish Gestational Diabetes Case-Control Study. Int J Environ Res Public Health. 2022;19(17):10711. doi:10.3390/ijerph191710711
8. Corrêa JD, Faria GA, Fernandes LL. The oral microbiota and gestational diabetes mellitus. Front Clin Diabetes Healthc. 2023;4:1120920. doi:10.3389/fcdhc.2023.1120920
9. Camoni N, Conti G, Majorana A, et al. Oral Microbiota of Infants in Maternal Gestational Diabetes: a Systematic Review. Children. 2024;11(4):421. doi:10.3390/children11040421
10. Sekula P, Del Greco MF, Pattaro C, Köttgen A. Mendelian Randomization as an Approach to Assess Causality Using Observational Data. J Am Soc Nephrol. 2016;27(11):3253–3265. doi:10.1681/ASN.2016010098
11. Luo M, Sun M, Wang T, et al. Gut microbiota and type 1 diabetes: a two-sample bidirectional Mendelian randomization study. Front Cell Infect Microbiol. 2023;13:1163898. doi:10.3389/fcimb.2023.1163898
12. Skrivankova VW, Richmond RC, Woolf BA, et al. Strengthening the reporting of observational studies in epidemiology using Mendelian randomization: the STROBE-MR statement. JAMA. 2021;326(16):1614–1621. doi:10.1001/jama.2021.18236
13. Burgess S, Thompson SG, Collaboration CCG. Avoiding bias from weak instruments in Mendelian randomization studies. Int J Epidemiol. 2011;40(3):755–764. doi:10.1093/ije/dyr036
14. Scheibner J, Ienca M, Kechagia S, et al. Data protection and ethics requirements for multisite research with health data: a comparative examination of legislative governance frameworks and the role of data protection technologies. J Law Biosci. 2020;7(1):lsaa010. doi:10.1093/jlb/lsaa010
15. Stankevic E, Kern T, Borisevich D, et al. Genome-wide association study identifies host genetic variants influencing oral microbiota diversity and metabolic health. Sci Rep. 2024;14(1):14738. doi:10.1038/s41598-024-65538-8
16. Murphy N, Song M, Papadimitriou N, et al. Associations Between Glycemic Traits and Colorectal Cancer: a Mendelian Randomization Analysis. J National Cancer Inst. 2022;114(5):740–752. doi:10.1093/jnci/djac011
17. Yun Z, Guo Z, Li X, et al. Genetically predicted 486 blood metabolites in relation to risk of colorectal cancer: a Mendelian randomization study. Cancer Med. 2023;12(12):13784–13799. doi:10.1002/cam4.6022
18. Burgess S, Foley CN, Allara E, Staley JR, Howson JMM. A robust and efficient method for Mendelian randomization with hundreds of genetic variants. Nat Commun. 2020;11(1):376. doi:10.1038/s41467-019-14156-4
19. Bowden J, Del Greco MF, Minelli C, Davey Smith G, Sheehan NA, Thompson JR. Assessing the suitability of summary data for two-sample Mendelian randomization analyses using MR-Egger regression: the role of the I2 statistic. Int J Epidemiol. 2016;45(6):1961–1974. doi:10.1093/ije/dyw220
20. Brion M-JA, Shakhbazov K, Visscher PM. Calculating statistical power in Mendelian randomization studies. Int J Epidemiol. 2013;42(5):1497–1501. doi:10.1093/ije/dyt179
21. Xu J, Zhang S, Tian Y, et al. Genetic Causal Association between Iron Status and Osteoarthritis: a Two-Sample Mendelian Randomization. Nutrients. 2022;14(18). doi:10.3390/nu14183683.
22. Bowden J, Del Greco MF, Minelli C, et al. Improving the accuracy of two-sample summary-data Mendelian randomization: moving beyond the NOME assumption. Int J Epidemiol. 2018;48(3):728–742. doi:10.1093/ije/dyy258
23. Ong JS, MacGregor S. Implementing MR-PRESSO and GCTA-GSMR for pleiotropy assessment in Mendelian randomization studies from a practitioner’s perspective. Genetic Epidemiol. 2019;43(6):609–616. doi:10.1002/gepi.22207
24. Jang E-Y, Chun J, Kwack KH, Moon J-H, Lee J-H. Complete genome sequence of Schaalia odontolytica isolated from subgingival biofilm. BMC Genomic Data. 2024;25(1):15. doi:10.1186/s12863-023-01184-9
25. Chouhan D, Grossman AS, Kerns KA, et al. Episymbiotic Saccharibacteria suppresses epithelial immunoactivation through Type IV pili and TLR2 dependent endocytosis. bioRxiv. 2025. doi:10.1101/2025.05.30.656655
26. Bachtiar BM, Tahapary DL, Fath T, et al. Saccharibacteria (TM7) in saliva and subgingival microbiome as a predictor for gingivitis in individuals with type2 diabetes evaluated by qPCR. Front Dent Med. 2025;6:1550936. doi:10.3389/fdmed.2025.1550936
27. Dreisbach C, Prescott S, Alhusen J, Dudley D, Trinchieri G, Siega-Riz AM. Association between microbial composition, diversity, and function of the maternal gastrointestinal microbiome with impaired glucose tolerance on the glucose challenge test. PLoS One. 2022;17(12):e0271261. doi:10.1371/journal.pone.0271261
28. King P. Haemophilus influenzae and the lung (Haemophilus and the lung). Clin Transl Med. 2012;1(1):10. doi:10.1186/2001-1326-1-10
29. Huska B, Ulanova M. Inflammatory Responses to Non-Typeable Haemophilus influenzae Clinical Isolates from Invasive and Non-Invasive Infections. Pathogens. 2025;14(3). doi:10.3390/pathogens14030210
30. Choi J, Cox AD, Li J, McCready W, Ulanova M. Activation of innate immune responses by Haemophilus influenzae lipooligosaccharide. Clin Vaccine Immunol. 2014;21(5):769–776. doi:10.1128/CVI.00063-14
31. Xu Y, Zhang M, Zhang J, et al. Differential intestinal and oral microbiota features associated with gestational diabetes and maternal inflammation. Am J Physiol Endocrinol Metab. 2020;319(2):E247–E253. doi:10.1152/ajpendo.00266.2019
32. Ren Y, Hao L, Liu J, et al. Alterations in the Gut Microbiota in Pregnant Women with Pregestational Type 2 Diabetes Mellitus. mSystems. 2023;8(2):e0114622. doi:10.1128/msystems.01146-22
33. Liu H, Pan LL, Lv S, et al. Alterations of Gut Microbiota and Blood Lipidome in Gestational Diabetes Mellitus With Hyperlipidemia. Front Physiol. 2019;10:1015. doi:10.3389/fphys.2019.01015
34. Tsarna E, Christopoulos P. The role of gut microbiome in prevention, diagnosis and treatment of gestational diabetes mellitus. J Obstet Gynaecol. 2022;42(5):719–725. doi:10.1080/01443615.2021.1959534
35. Xue H, Shen X, Pan W. Constrained maximum likelihood-based Mendelian randomization robust to both correlated and uncorrelated pleiotropic effects. Am J Hum Genet. 2021;108(7):1251–1269. doi:10.1016/j.ajhg.2021.05.014
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Effect of Circulating Inflammatory Proteins on Endometriosis: A Mendelian Randomization Study
Wei Y, Zhao X, Li L
ImmunoTargets and Therapy 2024, 13:585-593
Published Date: 1 November 2024
Genetic Insights Into Lipid Traits and Lipid-Modifying Drug Targets in Pregnancy Complications: A Two-Sample Mendelian Randomization Study
Shao H, Xu C, Zhang C, Li L, Wu P, Chen Z, Guan R
International Journal of Women's Health 2025, 17:221-234
Published Date: 31 January 2025
Causal Associations Between Sarcopenia and Gestational Diabetes Mellitus

Huang Y, Zhao S, Hong J, Shen L, Wang Z, Wang D
International Journal of Women's Health 2025, 17:259-269
Published Date: 1 February 2025
Causal Effect of Fatty Fish Consumption on Influenza: Evidence From Two-Sample Mendelian Randomization
Huang X, Xie Z, Li J, Li S
Journal of Multidisciplinary Healthcare 2025, 18:1123-1133
Published Date: 24 February 2025
Research Advance of Causal Inference in Clinical Medicine: A Bibliometrics Analysis via Citespace
Qin G, Wei J, Sun Y, Du W
Journal of Multidisciplinary Healthcare 2025, 18:2603-2627
Published Date: 10 May 2025