Back to Journals » International Journal of Women's Health » Volume 18
Causal Association Between Sleep Traits and Endometriosis: A Mendelian Randomization Study
Authors Li J, Wan W, Hu L ![]() , Ren Y
, Ren Y ![]() , Ge L, Liu Y, Liu P, Cui L
, Ge L, Liu Y, Liu P, Cui L ![]()
Received 17 September 2025
Accepted for publication 9 January 2026
Published 6 February 2026 Volume 2026:18 565217
DOI https://doi.org/10.2147/IJWH.S565217
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Jincheng Li,1 Wenjing Wan,1– 8 Linlin Hu,2– 8 Yujia Ren,1– 8 Li Ge,1 Yue Liu,1 Peihao Liu,2– 8 Linlin Cui1
1Center for Reproductive Medicine, The Second Qilu Hospital of Shandong University, Jinan, Shandong, 250012, People’s Republic of China; 2State Key Laboratory of Reproductive Medicine and Offspring Health, Center for Reproductive Medicine, Institute of Women, Children and Reproductive Health, Shandong University, Jinan, 250012, People’s Republic of China; 3National Research Center for Assisted Reproductive Technology and Reproductive Genetics, Shandong University, Jinan, Shandong, 250012, People’s Republic of China; 4Key Laboratory of Reproductive Endocrinology (Shandong University), Ministry of Education, Jinan, Shandong, 250012, People’s Republic of China; 5Shandong Technology Innovation Center for Reproductive Health, Jinan, Shandong, 250012, People’s Republic of China; 6Shandong Provincial Clinical Research Center for Reproductive Health, Jinan, Shandong, 250012, People’s Republic of China; 7Shandong Key Laboratory of Reproductive Research and Birth Defect Prevention (Under Construction), Jinan, Shandong, 250012, People’s Republic of China; 8Research Unit of Gametogenesis and Health of ART-Offspring, Chinese Academy of Medical Sciences (No.2021RU001), Jinan, Shandong, 250012, People’s Republic of China
Correspondence: Linlin Cui, Center for Reproductive Medicine, The Second Qilu Hospital of Shandong University, No. 247, Beiyuan Road, Tianqiao District, Jinan, Shandong, People’s Republic of China, Tel +86 531 85651188, Email [email protected] Peihao Liu, State Key Laboratory of Reproductive Medicine and Offspring Health, Center for Reproductive Medicine, Institute of Women, Children and Reproductive Health, Shandong University, No. 157, Jingliu Road, Shizhong District, Jinan, Shandong, 250012, People’s Republic of China, Tel +86 531 87909000, Email [email protected]
Purpose: Previous studies suggested that irregular sleep-wake rhythms increased the risk of endometriosis. Mechanistically, sleep pattern dysregulation may promote the pathogenesis of endometriosis via neuroendocrine disturbances. However, the causal relationship between sleep traits and endometriosis remains unclear. We aim to investigate the potential causal associations between sleep traits and endometriosis, including its specific anatomical subtypes.
Patients and Methods: Two-sample Mendelian Randomization (MR) analyses were conducted. The primary exposure was insomnia, and the secondary exposures were getting up in the morning, nap during day, sleep disorders, chronotype, snoring, short sleep duration, and long sleep duration. The outcomes were endometriosis along with its anatomical subtypes: uterine, ovarian, vaginal, intestinal, peritoneal, and unspecified endometriosis. We applied inverse variance weighted (IVW), weighted median, simple mode, weighted mode, and MR-Egger regression to estimate causal relationships between sleep traits and the risk of endometriosis. Additionally, a series of sensitivity and validation analyses were performed to ensure robustness.
Results: For the primary exposure, IVW results suggested that insomnia was significantly associated with elevated risks of endometriosis (OR=1.83, 95% CI: 1.34– 2.50), uterine endometriosis (OR=2.22, 95% CI: 1.30– 3.80), ovarian endometriosis (OR=1.61, 95% CI: 1.03– 2.54), vaginal endometriosis (OR > 1.00, 95% CI: 1.03– 3.79) and unspecified endometriosis (OR=2.70, 95% CI: 1.45– 5.02). For the secondary exposure, most sleep traits showed no significant associations with endometriosis risk.
Conclusion: Our study demonstrated a causal relationship between insomnia and elevated risks of endometriosis across multiple anatomical subtypes. While no significant associations were observed for other sleep traits, the robust link with insomnia highlights the potential clinical value of sleep-focused interventions in mitigating the risk of endometriosis.
Keywords: endometriosis, genetic association, Mendelian randomization, insomnia, sleep traits
Introduction
Endometriosis, characterized by the presence of endometrial-like tissue outside the uterus,1 affects approximately 6–10% of women of reproductive age globally.2 Beyond causing symptoms such as pelvic pain, dysmenorrhea and infertility,3,4 endometriosis is associated with various long-term complications, including cardiovascular diseases, autoimmune diseases, and ovarian cancer.5–8 Anatomically, endometriosis can be classified based on lesion location, including uterus, ovary, vagina, intestine, peritoneum, and unspecified sites. The symptoms vary slightly by subtype. Despite extensive research into its pathophysiology, the etiology of endometriosis remains unknown.9
Insomnia, one of the most prevalent sleep disorders globally, affects an estimated 30–50% of adults at some point in their lives,10 with women demonstrating a significantly higher susceptibility than men.11 Clinically, insomnia is defined by difficulties in initiating or maintaining sleep, early morning awakening, and, in some cases, nonrestorative or poor-quality sleep.11–15 Emerging evidence suggests a potential association between insomnia and the occurrence of endometriosis. This association may be mediated through shared neuroendocrine pathways, given that insomnia frequently co-occurs with emotional disorders such as anxiety and depression.16 Notably, population-based studies indicate that individuals with stress-related disorders are at a higher risk of subsequent endometriosis diagnosis.17 This susceptibility may stem from the activation of the sympathetic nervous system (SNS) and the hypothalamic-pituitary-adrenal (HPA) axis in response to stress.18 The SNS subsequently promotes systemic inflammation via catecholamine release,19 while the HPA axis stimulates excessive glucocorticoid production, potentially driving inflammation and autoimmune diseases.20 These clinical observations corroborated by rodent studies, which demonstrates that chronic stress exposure accelerates endometriosis progression and exacerbates lesion severity.21,22
Beyond insomnia, other sleep traits including getting up in the morning, nap during day, sleep disorders, chronotype, snoring, short sleep duration, and long sleep duration may affect reproductive hormone regulation through disruptions in the sleep-wake cycle.23 Irregular sleep-wake rhythms have been shown to impair estrogen synthesis and metabolism,24,25 thereby increasing the risk of estrogen-related disorders, including endometriosis.26
Mendelian randomization (MR) is an epidemiological method that uses genetic variants as instrumental variables (IVs) to assess causal associations between exposures and outcomes.27 In this study, we employed a two-sample MR analysis to evaluate the causal relationship between sleep traits and endometriosis. By utilizing genetic variants identified in genome-wide association studies (GWASs), we aimed to determine whether sleep traits are a risk factor for endometriosis, with profound implications for prevention and therapeutic strategies.
Methods
Overview
We conducted a Two-Sample Mendelian randomization (TSMR) using summary level data from Genome-wide meta-analysis association studies.28 The MR analysis relies on three core assumptions. Assumption 1, named relevance hypothesis, states that the selected IVs are strongly related to insomnia. Assumption 2, named independence hypothesis, requires that these IVs remain unaffected by potential confounders. Assumption 3, named exclusionary hypothesis, posits that these IVs affect endometriosis solely through insomnia-related pathways.29,30
The study included a discovery analysis and a validation analysis. In the discovery analysis, we investigated the causal associations between sleep characteristics and endometriosis, including its anatomical subtypes: uterine, ovarian, vaginal, intestinal, peritoneal, and unspecified endometriosis. In the validation analysis, the causal association between insomnia and endometriosis was further verified. The overall study design is shown in Figure 1.
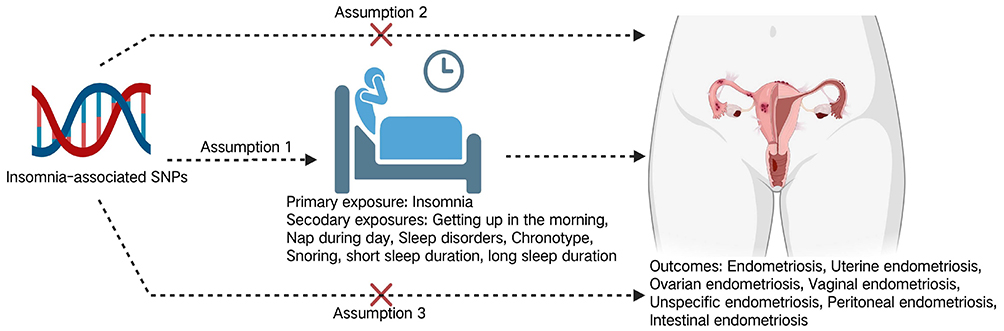 |
Figure 1 Framework for Evaluating the Causal Impact of Insomnia on Endometriosis Subtypes. |
Exposures
The primary exposure (insomnia) data were derived from the recent large-scale meta-analysis of GWASs conducted by the UK Biobank and 23andMe consortium.28 This analysis incorporated 593,724 insomnia cases and 1,771,286 controls, using a fixed-effect model in METAL. We identified 554 single-nucleotide polymorphisms (SNPs) associated with insomnia (Supplementary Table S1). Given that sex-specific meta-analyses revealed no significant differences in results between males and females, combined-sex summary statistics were employed to maximize statistical power. Additionally, to mitigate the impact of linkage disequilibrium (LD) on analysis outcomes, we set an r2 threshold of 0.001 and SNP distance of 10,000 kb.
The secondary exposures included seven sleep-related traits: getting up in the morning, nap during day, sleep disorders, chronotype, snoring, short sleep duration, and long sleep duration (Table 1). Instrumental variables for these traits were obtained from UK Biobank and FinnGen [IEU OpenGWAS project (mrcieu.ac.uk)]. For each trait, we selected SNPs meeting genome-wide significance (P<5e-6) and performed LD clumping with a threshold of 10,000 kb and r2 < 0.001.
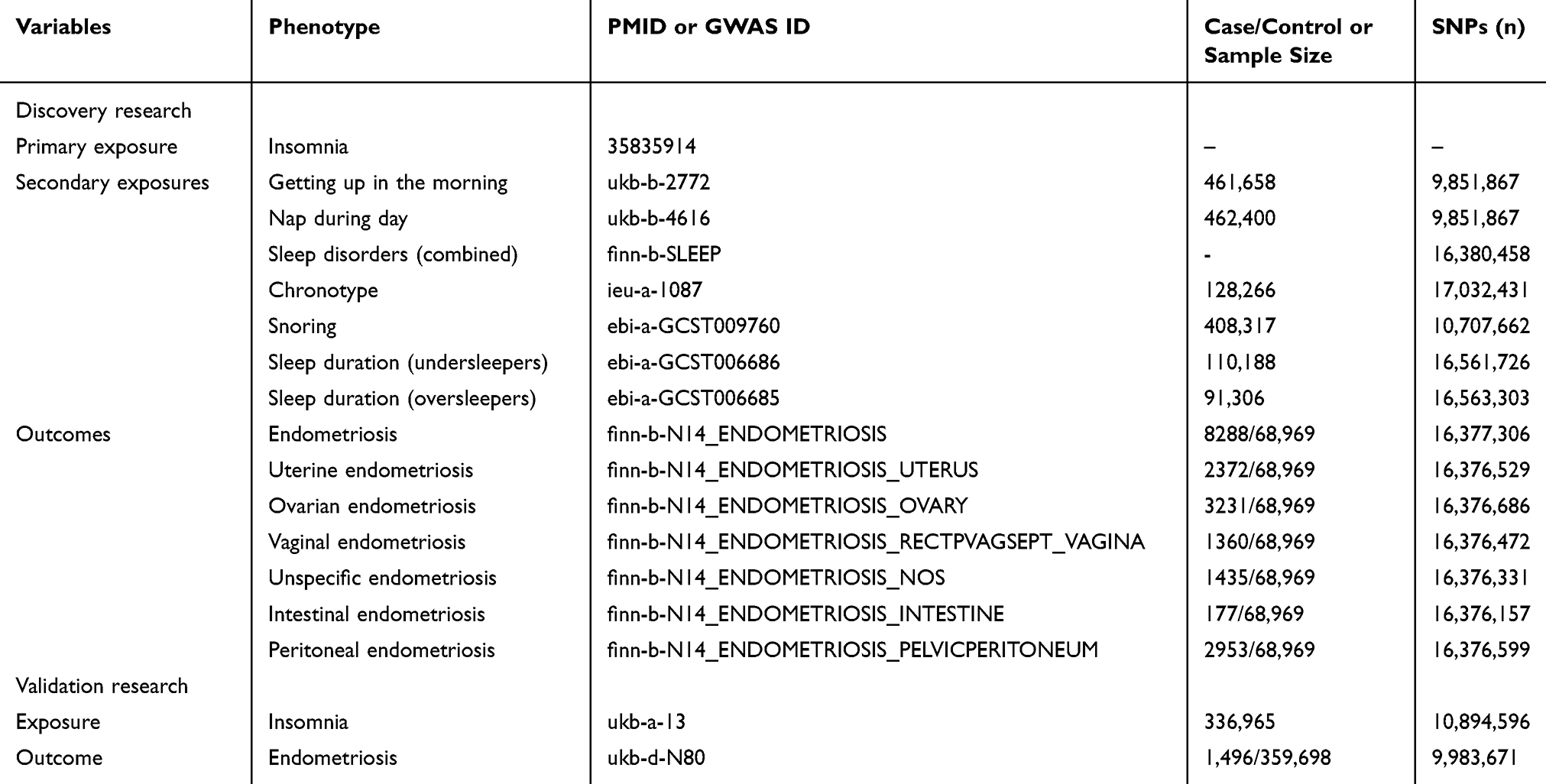 |
Table 1 The Data Source of Genetic Instruments for Exposures and Outcomes |
Outcomes
For outcome variables, we obtained GWAS summary statistics from the FinnGen Consortium [IEU Open GWAS project (mrcieu.ac.uk)] of European population, which comprised genetic and health data from 500,000 Finnish biobank participants. The FinnGen makes use of extensive longitudinal registry data of all Finnish residents, all of which are publicly available. The dataset included GWAS statistics for endometriosis (N=8288) and its subtypes: uterine (N=2372), ovarian (N=3231), vaginal (N=1360), unspecified (N=1435), peritoneal (N=177), and intestinal endometriosis (N=2953). A summary of GWAS data sources is provided in Table 1.
Statistical Analysis
MR analyses were performed using the TwoSample MR package in R version 4.2.3. Five common MR methods were utilized, including inverse variance weighted (IVW), weighted median,31 simple mode, weighted mode, and MR-Egger regression. The IVW method, implemented with a random-effects model to calculate a weighted average of the Wald ratio estimates, served as the primary analytical approach. To ensure the robustness, sensitivity analyses were performed to assess heterogeneity and horizontal pleiotropy. Heterogeneity was evaluated using Cochrane’s Q statistic, with a significance threshold of P < 0.05. Notably, the random-effects IVW model inherently accommodates potential heterogeneity. Horizontal pleiotropy was examined through MR-Egger regression, which tests whether IVs influence the outcome via pathways independent of sleep traits—a violation of MR assumptions 2 and 3. Furthermore, MR-pleiotropic Residuals and Outliers (MR-PRESSO) analysis was employed to identify and remove outlier SNPs (P < 0.05) exhibiting horizontal pleiotropy, thereby minimizing their confounding effects.32 Finally, a leave-one-out analysis was performed to evaluate whether the overall results were disproportionately driven by any single SNP. This comprehensive approach ensured the validity and reliability of the MR findings.
Independent Validation Analysis
To verify the causal association between insomnia and endometriosis, we performed a TSMR analysis using an independent, publicly available database. Genetic instruments for insomnia (n=10,894,596) and endometriosis (n=9,983,671) were obtained from the UK Biobank. We applied the same TSMR methodologies as those used in the discovery analysis.
Result
MR Analysis of Causal Links Between Sleep Traits and the Risk of Endometriosis
In the UK Biobank and 23andMe meta-analysis, a total of 544 independent SNPs (P < 5e-8) significantly associated with insomnia were selected as instrumental variables (IVs). As shown in Figure 2, IVW results indicated that insomnia was associated with increased risk of endometriosis (OR = 1.83, 95% CI: 1.34–2.50), uterine endometriosis (OR = 2.22, 95% CI: 1.30–3.80), ovarian endometriosis (OR = 1.61, 95% CI: 1.03–2.54), vaginal endometriosis (OR > 1.00, 95% CI: 1.03–3.79) and unspecified endometriosis (OR = 2.70, 95% CI: 1.45–5.02). However, no significant associations were observed for intestinal endometriosis (OR = 0.96, 95% CI: 0.17–5.41) and peritoneal endometriosis (OR = 1.49, 95% CI: 0.95–2.35). These findings were corroborated by supplementary analyses using weighted median, simple mode, weighted mode, and MR-Egger regression (Supplementary Tables S2–S9).
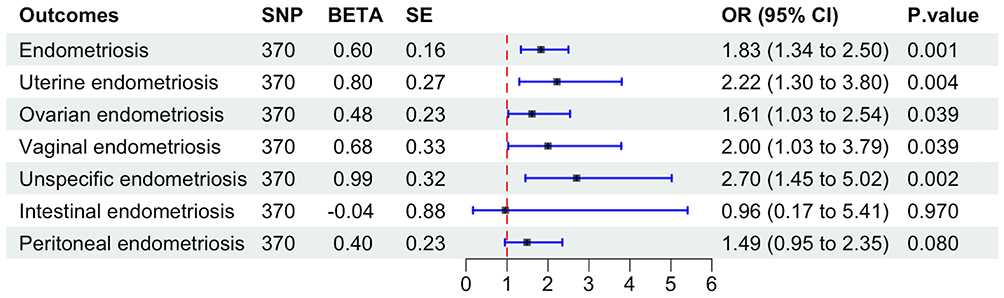 |
Figure 2 Forest plot of causality between insomnia and endometriosis. |
From the IEU openGWAS database, we screened independent SNPs associated with sleep traits (P < 5e-6), identifying 24 SNPs for sleep disorders, 201 for nap during day, 209 for getting up in the morning, 64 for chronotype, 131 for snoring, 11 for short sleep duration, and 18 for long sleep duration (Supplementary Table S10). Sleep disorders were associated with a reduced risk of unspecified endometriosis (OR = 0.74, 95% CI: 0.58–0.96). Getting up in the morning was associated with a reduced risk of ovarian endometriosis (OR = 0.56, 95% CI: 0.36–0.87). Sleep duration was associated with a reduced risk of intestinal endometriosis (OR = 0.02, 95% CI: < 0.001–0.86) (Figure 3).
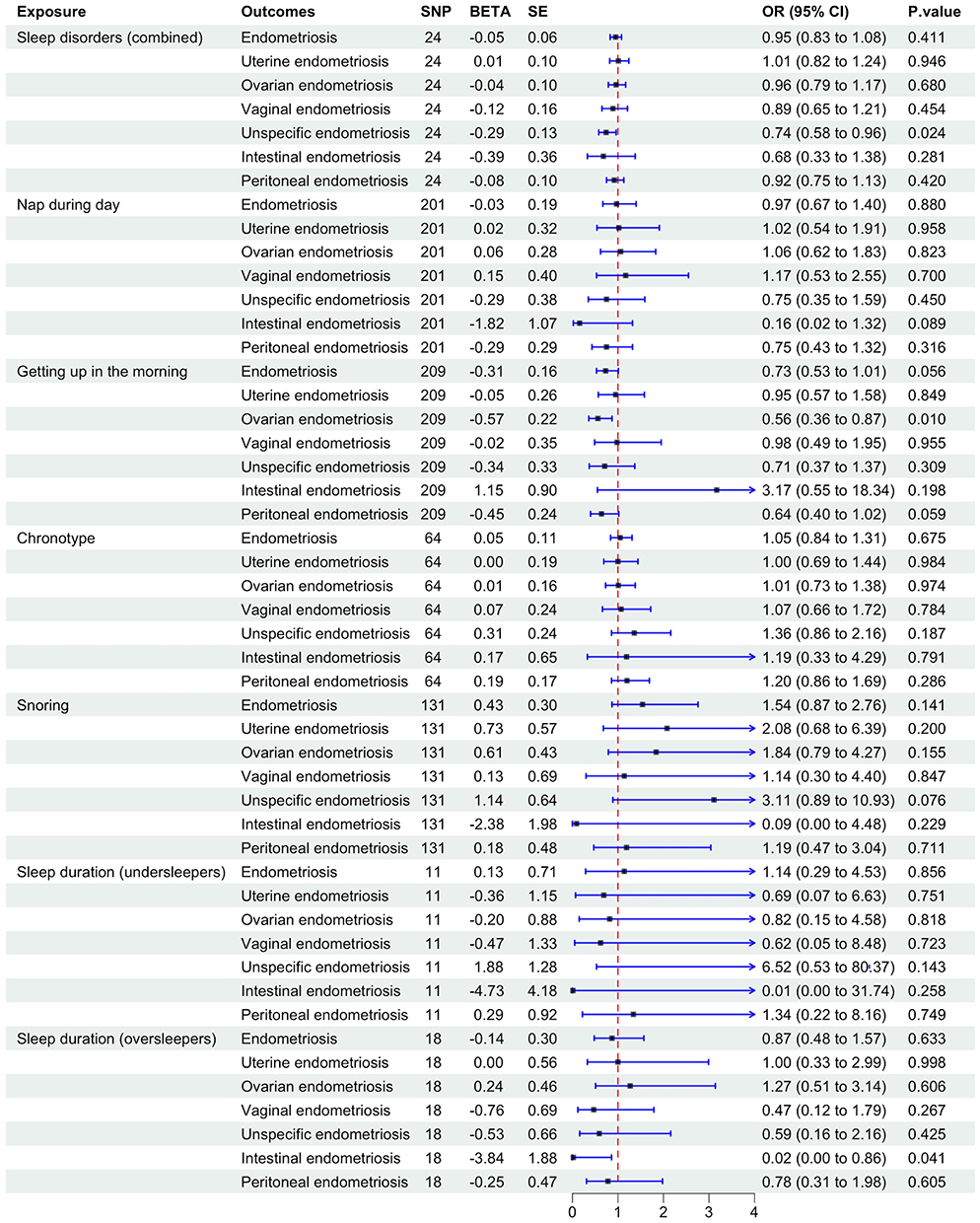 |
Figure 3 Forest plot of causality between sleep traits (except insomnia) and endometriosis. |
Sensitivity Analysis
To assess the robustness, we performed horizontal pleiotropy and heterogeneity tests (Table 2). The F statistic for insomnia-IVs was 49.8 (F > 10), indicating strong instrumental variables. No horizontal pleiotropy was observed for endometriosis and its anatomical subtypes (Egger intercept P > 0.05 for all outcomes). The Cochrane Q statistic indicated significant heterogeneity in the analyses of endometriosis, uterine endometriosis, and ovarian endometriosis (P < 0.05 for both MR Egger Q and IVW Q). Subsequent leave-one-out analysis and MR-PRESSO method did not identify any specific IVs driving heterogeneity, suggesting that the causal estimates remained robust. (Supplementary Figure 1A–G).
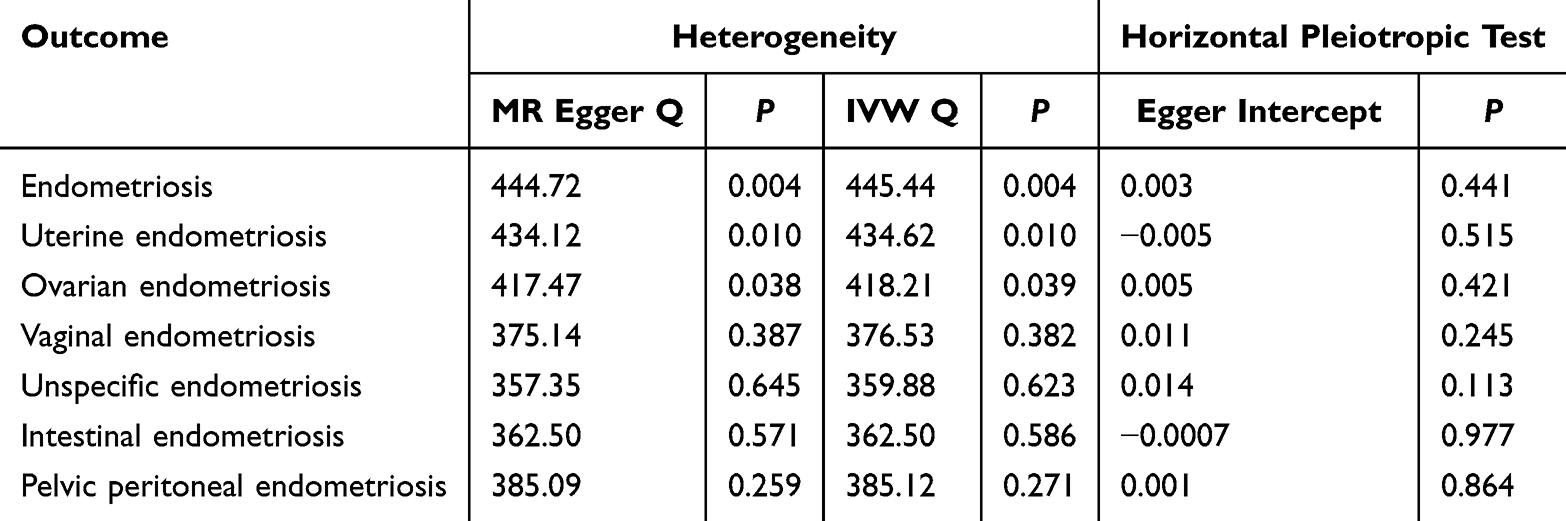 |
Table 2 Sensitivity MR Analyses Between Insomnia and Endometriosis Subtypes |
Validation Analysis
MR approaches validated the association between insomnia and endometriosis (Table 3). Consistent effects were observed via IVW method (OR = 1.01, 95% CI: 1.00–1.01), weighted median (OR = 1.01, 95% CI: 1.00–1.03), and MR-Egger regression (OR = 1.00, 95% CI: 1.00–1.01), strengthening evidence for causality.
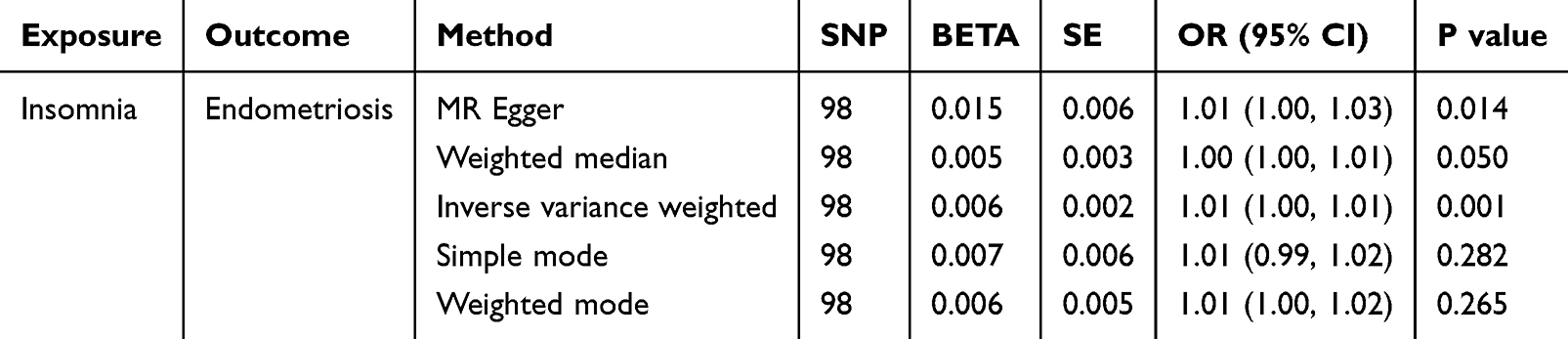 |
Table 3 Validation MR Analyses Between Insomnia and Endometriosis |
Discussion
In this study, we used TSMR Analysis to investigate the causal associations between sleep characteristics and endometriosis. Our results showed that insomnia was associated with an increased risk of overall endometriosis, as well as specific anatomical subtypes including uterine, ovarian, vaginal and unspecified endometriosis. These findings provide valuable evidence supporting preventive strategies and deepened our understanding of the potential role of sleep disorders in the etiology of endometriosis.
Our findings regarding the causal effect of insomnia on the risk of endometriosis are consistent with a recent Mendelian randomization study,33 which demonstrated that insomnia is a risk factor for overall endometriosis. However, our study extends this knowledge by further stratifying the analysis based on anatomical subtypes. We found that the impact of insomnia varies across different sites, showing a significant causal link specifically with uterine, ovarian, and unspecified endometriosis. This subtype-specific analysis provides novel insights into the heterogeneity of endometriosis etiology. Furthermore, previous epidemiological studies attributing endometriosis risk to sleep issues have largely focused on night-shift work, emphasizing circadian rhythm disruption as the primary mechanism.34–39 Notably, insomnia characterized by difficulties in both sleep initiation and maintenance involves distinct pathophysiological mechanisms beyond mere circadian disruption. Specifically, these mechanisms include dysregulated HPA axis activity and elevated cytokine levels. Previous studies suggested that abnormal HPA axis biomarkers related to insomnia were significantly associated with endometriosis,40 indicating a mechanistic pathway independent of occupational exposures. Consequently, these findings position insomnia as a modifiable risk factor, providing a new direction for the primary prevention of endometriosis.
Current evidence suggests insomnia may contribute to endometriosis through neuroendocrine dysregulation.40–43 Normal sleep progression is mediated by melatonin, a chronobiotic hormone synthesized predominantly in the pineal gland that governs circadian rhythmicity.44–46 Critically, melatonin dysregulation has been implicated in the pathogenesis of endometriosis.41–43 In endometriosis, melatonin enhances antioxidant defenses via the upregulation of superoxide dismutase (SOD) and catalase (CAT).41,42 Furthermore, melatonin directly inhibits endometriotic cell invasion by modulating the balance of MMP-3/MMP-9 and TIMP-1/TIMP-3.43 Clinical data reveal that sleep disturbances in patients with insomnia correlate with significant disruption in melatonin release.47 Moreover, clinical studies demonstrate that women with endometriosis exhibit significantly lower melatonin levels compared to healthy controls.48 These findings suggested that insomnia disrupts the integrated melatonin-mediated “circadian-antioxidant-invasive” regulatory network, providing a mechanistic basis for its role in endometriosis pathogenesis.
The insomnia-endometriosis connection may also operate through the “HPA axis activation-inflammation -endometriosis” cascade. Prolonged sleep disruption triggers hyperactivation of the HPA axis, elevating cortisol levels. As a stress hormone, sustained cortisol elevation is known to dysregulate immune function. Mechanistically, this may involve the persistent activation of inflammatory transcription factors like NF-κB, leading to the upregulation of pro-inflammatory genes. This neuroendocrine dysregulation also amplifies oxidative stress.20 This pathological milieu creates a permissive microenvironment for endometriosis development: inflammatory cytokines (e.g., IL-6) promote angiogenesis and cell adhesion in ectopic lesions, while oxidative DNA damage facilitates endometrial cell survival outside the uterine cavity.49,50 Together, these findings position insomnia as a significant contributor to endometriosis pathophysiology through interconnected neuroendocrine, inflammatory, and oxidative pathways.
Crucially, insomnia is a highly intervenable and modifiable risk factor. Identifying insomnia as a pathogenic driver suggests that sleep-focused interventions could serve as novel, non-hormonal strategies for the prevention of endometriosis or as adjunctive therapies to alleviate disease progression. This shifts the clinical paradigm from solely managing gynecological symptoms to addressing broader systemic dysregulation, underscoring the value of multidisciplinary management in women’s health.
In contrast to insomnia, other sleep characteristics including getting up in the morning, nap during day, sleep disorders, chronotype, snoring, short sleep duration, and long sleep duration showed no causal association with genetically predicted endometriosis risk. This lack of association might be explained by the fact that characteristics such as snoring and sleep duration share overlapping genetic factors with obesity or metabolic genes.51,52 Although we conducted horizontal pleiotropic tests, it remained possible that unmeasured pleiotropy could interfere with MR assumptions, leading to false-negative findings. Additionally, while insomnia may promote disease progression through inflammatory or hormonal pathways, other characteristics may lack direct interaction evidence with the core mechanism of endometriosis. Future observational studies or multi-omics analyses will be necessary to clarify mechanistic links between these sleep characteristics and the development of endometriosis.
Our study has several notable strengths. The insomnia exposure data were derived from a large-scale GWAS meta-analysis, which increased statistical power and enhanced the precision and robustness of our results. Importantly, as genetic variants are unlikely to be influenced by environmental or lifestyle factors in the same way as traditional exposures, this MR design strengthens the reliability of our finding by minimizing confounding. Notably, our study extends current knowledge by providing the first genetic evidence linking insomnia to specific anatomical subtypes of endometriosis, where previous observational studies had failed to establish this association. Several limitations warrant consideration. Primarily, both the discovery and validation analysis were limited to individuals of European ancestry, potentially restricting the generalizability of the findings to other ethnic groups. Furthermore, despite sensitivity analyses, MR results may still be influenced by heterogeneity and reverse causality, which represent inherent methodological limitations of the MR approach.
Conclusion
Insomnia is a clinically significant and modifiable risk factor for the development of endometriosis. These results highlight the critical importance of screening and intervening for poor sleep quality, positioning insomnia as a viable target for personalized prevention strategies in women’s reproductive health.
Abbreviations
MR, Mendelian randomisation; IVW, inverse variance weighting; MR-PRESSO, MR-pleiotropic residuals and outliers; SNS, sympathetic nervous system; HPA, the hypothalamic-pituitary-adrenal; TSMR, two-sample Mendelian randomization; IVs, instrumental variables; GWASs, genome-wide association studies; SNPs, single-nucleotide polymorphisms; LD, linkage disequilibrium; SOD, superoxide dismutase; CAT, catalase.
Data Sharing Statement
The data utilized in this study can be found in the public database. For additional details, please contact the two corresponding authors [Linlin Cui [email protected]; Peihao Liu [email protected]].
Ethics Approval and Informed Consent
This study utilized de-identified, publicly available summary statistics from large-scale consortia, including the UK Biobank, FinnGen, and 23andMe. Ethical approval and informed consent were previously obtained by the primary investigators of these original studies. Consequently, the Institutional Review Board (IRB) of the Second Hospital of Shandong University granted an exemption from ethical review for the current study. This exemption is in accordance with items 1 and 2 of Article 32 of the Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects (2023, China).
Acknowledgments
The authors thank the UK Biobank and FinnGen consortium for providing GWAS data. The authors thank the BioRender for creating figures.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Key Technology Research and Developmental Program of China (2022YFC2703000), CAMS Innovation Fund for Medical Sciences (2021-I2M-5-001), the Fundamental Research Funds of Shandong University (2023QNTD004), the National Natural Science Foundation of China (NSFC) Regional Innovation and Development Joint Fund (U24A20664), the National Key Technology Research and Developmental Program of China (2022YFC2704404), the National Key Technology Research and Developmental Program of China (2024YFC2706902), the National Key R&D Program of China (2024YFC2706700), the Shandong Provincial Natural Science Foundation (ZR2022JQ33), the Excellence Research Group Program of NSFC (32588201), and the National Special Support Program for High-level Talents.
Disclosure
The authors have no relevant financial or non-financial interests to disclose for this work.
References
1. Zhai J, Vannuccini S, Petraglia F, Giudice LC. Adenomyosis: mechanisms and pathogenesis. Semin Reprod Med. 2020;38(2–3):129–10. doi:10.1055/s-0040-1716687
2. Giudice LC, Kao LC. Endometriosis. Lancet. 2004;364(9447):1789–1799. doi:10.1016/S0140-6736(04)17403-5
3. Harada T, Khine YM, Kaponis A, Nikellis T, Decavalas G, Taniguchi F. The impact of adenomyosis on women’s fertility. Obstet Gynecol Surv. 2016;71(9):557–568. doi:10.1097/OGX.0000000000000346
4. Benson RC, Sneeden VD. Adenomyosis: a reappraisal of symptomatology. Am J Obstet Gynecol. 1958;76(5):1044–1057. discussion 1057-61. doi:10.1016/0002-9378(58)90186-8
5. Barnard ME, Farland LV, Yan B, et al. Endometriosis typology and ovarian cancer risk. JAMA. 2024;332(6):482–489. doi:10.1001/jama.2024.9210
6. Havers-Borgersen E, Hartwell D, Ekelund C, et al. Endometriosis and long-term cardiovascular risk: a nationwide Danish study. Eur Heart J. 2024;45(44):4734–4743. doi:10.1093/eurheartj/ehae563
7. Ma KS, Wang LT, Sasamoto N, et al. Endometriosis and Sjogren’s syndrome: bidirectional associations in population-based 15-year retrospective cohorts. Acta Obstet Gynecol Scand. 2024;103(10):2070–2080. doi:10.1111/aogs.14909
8. Tang T, Zhong Y, Xu S, Yu H. Causal effects of endometriosis on SLE, RA and SS risk: evidence from meta-analysis and Mendelian randomization. BMC Pregnancy Childbirth. 2024;24(1):162. doi:10.1186/s12884-024-06347-9
9. Zhang W, Li K, Jian A, Zhang G, Zhang X. Prospects for potential therapy targeting immune‑associated factors in endometriosis (Review). Mol Med Rep. 2025;31(3):57. doi:10.3892/mmr.2024.13422
10. Aernout E, Benradia I, Hazo JB, et al. International study of the prevalence and factors associated with insomnia in the general population. Sleep Med. 2021;82:186–192. doi:10.1016/j.sleep.2021.03.028
11. Roth T. Insomnia: definition, prevalence, etiology, and consequences. J Clin Sleep Med. 2007;3(5 Suppl):S7–10. doi:10.5664/jcsm.26929
12. Ferini-Strambi L, Auer R, Bjorvatn B, et al. Insomnia disorder: clinical and research challenges for the 21st century. Eur J Neurol. 2021;28(7):2156–2167. doi:10.1111/ene.14784
13. Morin CM, Jarrin DC. Epidemiology of insomnia: prevalence, course, risk factors, and public health burden. Sleep Med Clin. 2022;17(2):173–191. doi:10.1016/j.jsmc.2022.03.003
14. Wu F, Li X, Guo YN, Yan LZ, He RJ, Xu YH. Effects of insomnia treatments on cognitive function: a meta-analysis of randomized controlled trials. Psychiatry Res. 2024;342:116236. doi:10.1016/j.psychres.2024.116236
15. Van Someren EJW. Brain mechanisms of insomnia: new perspectives on causes and consequences. Physiol Rev. 2021;101(3):995–1046. doi:10.1152/physrev.00046.2019
16. Meyer N, Lok R, Schmidt C, et al. The sleep-circadian interface: a window into mental disorders. Proc Natl Acad Sci U S A. 2024;121(9):e2214756121. doi:10.1073/pnas.2214756121
17. Gao M, Koupil I, Sjoqvist H, et al. Psychiatric comorbidity among women with endometriosis: nationwide cohort study in Sweden. Am J Obstet Gynecol. 2020;223(3):415e1–415e16. doi:10.1016/j.ajog.2020.02.033
18. Becker L, Kaltenegger HC, Nowak D, Weigl M, Rohleder N. Biological stress responses to multitasking and work interruptions: a randomized controlled trial. Psychoneuroendocrinology. 2023;156:106358. doi:10.1016/j.psyneuen.2023.106358
19. Aboulata AA, Shatla IM. Physiology and immunology of the adrenergic anti-inflammatory pathway. Egyptian J Immunol. 2024;31(4):46–57.
20. Shimba A, Ikuta K. Control of immunity by glucocorticoids in health and disease. Semin Immunopathol. 2020;42(6):669–680. doi:10.1007/s00281-020-00827-8
21. Appleyard CB, Cruz ML, Hernandez S, Thompson KJ, Bayona M, Flores I. Stress management affects outcomes in the pathophysiology of an endometriosis model. Reprod Sci. 2015;22(4):431–441. doi:10.1177/1933719114542022
22. Cuevas M, Flores I, Thompson KJ, Ramos-Ortolaza DL, Torres-Reveron A, Appleyard CB. Stress exacerbates endometriosis manifestations and inflammatory parameters in an animal model. Reprod Sci. 2012;19(8):851–862. doi:10.1177/1933719112438443
23. Gamble KL, Resuehr D, Johnson CH. Shift work and circadian dysregulation of reproduction. Front Endocrinol. 2013;4:92. doi:10.3389/fendo.2013.00092
24. Simonneaux V, Bahougne T, Angelopoulou E. Daily rhythms count for female fertility. Best Pract Res Clin Endocrinol Metab. 2017;31(5):505–519. doi:10.1016/j.beem.2017.10.012
25. Sciarra F, Franceschini E, Campolo F, et al. Disruption of circadian rhythms: a crucial factor in the etiology of infertility. Int J Mol Sci. 2020;21(11):3943. doi:10.3390/ijms21113943
26. Davis S, Mirick DK, Stevens RG. Night shift work, light at night, and risk of breast cancer. J Natl Cancer Inst. 2001;93(20):1557–1562. doi:10.1093/jnci/93.20.1557
27. Bowden J, Holmes MV. Meta-analysis and Mendelian randomization: a review. Res Synth Methods. 2019;10(4):486–496. doi:10.1002/jrsm.1346
28. Watanabe K, Jansen PR, Savage JE, et al. Genome-wide meta-analysis of insomnia prioritizes genes associated with metabolic and psychiatric pathways. Nat Genet. 2022;54(8):1125–1132. doi:10.1038/s41588-022-01124-w
29. Birney E. Mendelian Randomization. Cold Spring Harb Perspect Med. 2022;12(4). doi:10.1101/cshperspect.a041302
30. Emdin CA, Khera AV, K S. Mendelian randomization. JAMA. 2017;318(19):1925. doi:10.1001/jama.2017.17219
31. Bowden J, Davey Smith G, Haycock PC, Burgess S. Consistent estimation in Mendelian randomization with some invalid instruments using a weighted median estimator. Genet Epidemiol. 2016;40(4):304–314. doi:10.1002/gepi.21965
32. Verbanck M, Chen CY, Neale B, Do R. Detection of widespread horizontal pleiotropy in causal relationships inferred from Mendelian randomization between complex traits and diseases. Nat Genet. 2018;50(5):693–698. doi:10.1038/s41588-018-0099-7
33. Zhang J, Wang T, Yang P, Miao Y, Ge B, Sun J. Association of sleep traits, physical activity, and sedentary leisure behavior with female reproductive health: a two-sample mendelian randomization analysis. Int J Womens Health. 2025;17:497–506. doi:10.2147/IJWH.S492065
34. Marino JL, Holt VL, Chen C, Davis S. Shift work, hCLOCK T3111C polymorphism, and endometriosis risk. Epidemiology. 2008;19(3):477–484. doi:10.1097/EDE.0b013e31816b7378
35. Marino JL, Holt VL, Chen C, Davis S. Lifetime occupational history and risk of endometriosis. Scand J Work Environ Health. 2009;35(3):233–240. doi:10.5271/sjweh.1317
36. Hsu HC, Tseng KY, Wang HC, Sung FC, Ma WF. Risk of endometriosis and subsequent ovary and breast cancers in nurses: a population-based cohort study in Taiwan. Int J Environ Res Public Health. 2019;16(18):3469. doi:10.3390/ijerph16183469
37. Schernhammer ES, Vitonis AF, Rich-Edwards J, Missmer SA. Rotating nightshift work and the risk of endometriosis in premenopausal women. Am J Obstet Gynecol. 2011;205(5):476e1–8. doi:10.1016/j.ajog.2011.06.002
38. D’Ettorre G, Pellicani V, Caroli A, Greco M. Shift work sleep disorder and job stress in shift nurses: implications for preventive interventions. Med Lav. 2020;111(3):195–202. doi:10.23749/mdl.v111i3.9197
39. Brown JP, Martin D, Nagaria Z, Verceles AC, Jobe SL, Wickwire EM. Mental health consequences of shift work: an updated review. Curr Psychiatry Rep. 2020;22(2):7. doi:10.1007/s11920-020-1131-z
40. Devine JK, Bertisch SM, Yang H, et al. Glucocorticoid and inflammatory reactivity to a repeated physiological stressor in insomnia disorder. Neurobiol Sleep Circadian Rhythms. 2019;6:77–84. doi:10.1016/j.nbscr.2018.06.001
41. Fischer TW, Kleszczynski K, Hardkop LH, Kruse N, Zillikens D. Melatonin enhances antioxidative enzyme gene expression (CAT, GPx, SOD), prevents their UVR-induced depletion, and protects against the formation of DNA damage (8-hydroxy-2’-deoxyguanosine) in ex vivo human skin. J Pineal Res. 2013;54(3):303–312. doi:10.1111/jpi.12018
42. Hardeland R. Aging, melatonin, and the pro- and anti-inflammatory networks. Int J Mol Sci. 2019;20(5). doi:10.3390/ijms20051223
43. Paul S, Bhattacharya P, Das Mahapatra P, Swarnakar S. Melatonin protects against endometriosis via regulation of matrix metalloproteinase-3 and an apoptotic pathway. J Pineal Res. 2010;49(2):156–168. doi:10.1111/j.1600-079X.2010.00780.x
44. Ding W, Xu Y, Ding W, et al. Research progress on melatonin, 5-HT, and orexin in sleep disorders of children with autism spectrum disorder. Biomol Biomed. 2024;25(3):525–533. doi:10.17305/bb.2024.11182
45. Comai S, Gobbi G. Melatonin, melatonin receptors and sleep: moving beyond traditional views. J Pineal Res. 2024;76(7):e13011. doi:10.1111/jpi.13011
46. Hosseinzadeh A, Alinaghian N, Sheibani M, Seirafianpour F, Naeini AJ, Mehrzadi S. Melatonin: current evidence on protective and therapeutic roles in gynecological diseases. Life Sci. 2024;344:122557. doi:10.1016/j.lfs.2024.122557
47. Brzecka A, Sarul K, Dyla T, et al. The association of sleep disorders, obesity and sleep-related hypoxia with cancer. Curr Genomics. 2020;21(6):444–453. doi:10.2174/1389202921999200403151720
48. Mosher AA, Tsoulis MW, Lim J, et al. Melatonin activity and receptor expression in endometrial tissue and endometriosis. Hum Reprod. 2019;34(7):1215–1224. doi:10.1093/humrep/dez082
49. Rapp J, Jung M, Klar RFU, et al. STAT3 signaling induced by the IL-6 family of cytokines modulates angiogenesis. J Cell Sci. 2023;136(1). doi:10.1242/jcs.260182
50. Donnez J, Binda MM, Donnez O, Dolmans MM. Oxidative stress in the pelvic cavity and its role in the pathogenesis of endometriosis. Fertil Steril. 2016;106(5):1011–1017. doi:10.1016/j.fertnstert.2016.07.1075
51. Chen Y, Li C, Cheng S, et al. The causal relationships between sleep-related phenotypes and body composition: a Mendelian randomized study. J Clin Endocrinol Metab. 2022;107(8):e3463–e3473. doi:10.1210/clinem/dgac234
52. Chen M, Ouyang Y, Yang Y, Liu Z, Zhao M. Impact of sleep problems on the cardiometabolic risks: an integrated epidemiological and metabolomics study. Diabetol Metab Syndr. 2024;16(1):267. doi:10.1186/s13098-024-01505-7
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Causal Relationship Between Endometriosis and Pelvic Inflammatory Diseases: Mendelian Randomization Study
Liu K, Liu X, Cao T, Cui X, Sun P, Zhang L, Wu X
International Journal of Women's Health 2024, 16:727-735
Published Date: 24 April 2024
The Effect of Circulating Inflammatory Proteins on Endometriosis: A Mendelian Randomization Study
Wei Y, Zhao X, Li L
ImmunoTargets and Therapy 2024, 13:585-593
Published Date: 1 November 2024
Causal Relationship Between Endometriosis, Female Infertility, and Primary Ovarian Failure Through Bidirectional Mendelian Randomization
Guo J, Wang Y, Chen G
International Journal of Women's Health 2024, 16:2143-2155
Published Date: 9 December 2024
Association of Sleep Traits, Physical Activity, and Sedentary Leisure Behavior With Female Reproductive Health: A Two-Sample Mendelian Randomization Analysis
Zhang J, Wang T, Yang P, Miao Y, Ge B, Sun J
International Journal of Women's Health 2025, 17:497-506
Published Date: 20 February 2025
Endometriosis Severity and Risk of Preeclampsia: A Combined Mendelian Randomization and Observational Study
Zu Y, Xie Y, Zhang H, Chen L, Yan S, Wang Z, Fang Z, Lin S, Yan J
International Journal of Women's Health 2025, 17:923-935
Published Date: 27 March 2025