Back to Journals » International Journal of Women's Health » Volume 17
Association of Sleep Traits, Physical Activity, and Sedentary Leisure Behavior With Female Reproductive Health: A Two-Sample Mendelian Randomization Analysis
Authors Zhang J, Wang T, Yang P, Miao Y, Ge B, Sun J ![]()
Received 10 October 2024
Accepted for publication 24 January 2025
Published 20 February 2025 Volume 2025:17 Pages 497—506
DOI https://doi.org/10.2147/IJWH.S492065
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Jiaxin Zhang, Tao Wang, Pusheng Yang, Yaxin Miao, Beilei Ge, Jing Sun
Shanghai Key Laboratory of Maternal Fetal Medicine, Shanghai Institute of Maternal-Fetal Medicine and Gynecologic Oncology, Shanghai First Maternity and Infant Hospital, School of Medicine, Tongji University, Shanghai, 200092, People’s Republic of China
Correspondence: Jing Sun, Email [email protected]; Beilei Ge, Email [email protected]
Purpose: Living habits affect female endocrine function and fertility, along with aging and other life factors. Because of this, female reproductive health can be promoted through living habit adjustment.
Methods: We used two-sample Mendelian randomization analysis with summary datasets from a genome-wide association study to investigate the causal relationships between sleep traits, sedentary leisure behavior, physical activity, and reproductive health traits in women, calculating odds ratios (ORs) and 95% confidence intervals (CIs). Exposure genetic instruments were used for variants that were significantly related to traits. The inverse-variance weighted (IVW) method was used for the main analysis, and we also performed MR-Egger and weighted median analyses to supplement the sensitivity test. Horizontal pleiotropy was detected using the MRE intercept and MR-PRESSO methods, and heterogeneity was assessed using Cochran’s Q statistics, IVW, and MR-Egger.
Results: Insomnia showed a significant inverse causal association with endometriosis [OR (95% CI) IVW = 1.80 (1.16, 2.80), P = 0.009] and abnormal menstruation [OR (95% CI) IVW = 2.37 (1.34, 4.20), P = 0.003]. Sleep duration was negatively related to menopause age (beta IVW = − 0.034, P = 0.001), and long sleep duration could be a protective factor of endometriosis [OR (95% CI) IVW = 0.07 (0.01, 0.72), P = 0.024]. Strenuous sports were also negatively correlated with female infertility [OR (95% CI) IVW = 0.10 (0.02, 0.68), P = 0.019]. Sensitivity analysis revealed no signs of horizontal pleiotropy or heterogeneity.
Conclusion: Our findings suggest that insomnia is an adverse factor correlated with endometriosis and abnormal menstruation and that longer sleep duration protects against endometriosis. Adequate sleep and regular schedules may decrease the risk of endometriosis and abnormal menstruation, helping improve the reproductive health of women.
Keywords: Mendelian randomization, reproductive health, lifestyle factors
Introduction
Many genetic and environmental factors affect female reproductive health.1 Multiple lifestyle factors can be modified to enhance overall well-being and reproductive health; they are ultimately under each individual’s control.2 A recent study investigated whether sleeping habits, physical activity, and lifestyle affect reproductive health, which is a topic of great concern.3
In women, sleep affects reproductive health, and sleep disorders can emerge during the reproductive stage.4 Sleep changes over time in women and with alterations in hormone levels associated with the menstrual cycle and menopause.5 There also appears to be a relationship between sleep traits and female reproductive health; poor sleep is associated with menstrual cycle irregularity,6 sleep dysregulation may result in infertility, and circadian dysrhythmia is linked to the altered secretion of reproductive hormones.7–9
It has been proven that reductions in daily physical activity are the primary causes of many chronic diseases and that physical activity is a rehabilitative treatment for inactivity-caused dysfunctions.10 There is emerging evidence that physical activity and sedentary lifestyles in both females and males can influence reproductive and assisted reproductive technology success.11,12 In women, increased physical activity and decreased sedentary behavior may improve fertility by maintaining body weight and hormone levels.13 In contrast, high levels of physical activity can inhibit ovulation, leading to decreased fertility; however, little is known about whether sedentary leisure behavior is causally related to reproductive capacity.14,15
Mendelian randomization (MR) uses single-nucleotide polymorphisms (SNPs) as genetic instruments to estimate the causal effects of exposure on certain outcomes.16 According to Mendel’s law, alleles with genetic variation are randomly separated during gametophytogenesis and fertilization, making them independent of confounding factors.17 This allows bypassing of possible and potential biases from confounding and reverse causation and strengthens causal inference in exposure–outcome associations.
Previous MR studies have demonstrated the significant impact of smoking initiation and alcohol and coffee consumption on female reproductive health.18 However, no robust evidence has been provided to support the correlation between sleep traits, sedentary leisure behavior, physical activity, and female reproductive health traits. Here, we employed a two-sample MR approach to investigate the association of these three lifestyle behaviors with reproductive traits and abnormal menstrual phenotypes, to provide evidence for aiding the management of female reproductive health. Using female reproductive health factors as outcomes, we focused on common infertility diseases such as polycystic ovarian syndrome (PCOS), endometriosis, and female infertility.19 This study also assessed sex hormones (total testosterone (TT), bioavailable testosterone (bio-T), estradiol (E2), and anti-Müllerian hormone (AMH)) and menstrual phenotypes (menopausal age and irregular menstrual cycle/bleeding).
Materials and Methods
Study Design
In this study, sleep traits (sleep duration, long sleep duration, short sleep duration, and insomnia), physical activity (moderate-to-vigorous physical activity (MVAP), vigorous physical activity (VAP), and strenuous sports) and sedentary leisure behavior (television watching, computer use, driving) were used as exposure factors. Single nucleotide polymorphism (SNP) loci significantly associated with the above exposure factors were selected as instrumental variables (IVs); the outcome variables were PCOS, endometriosis, female infertility, abnormal menstruation, menopause age, bioT, TT, E2, and AMH. The causal association analysis between exposure and outcome was performed using a two-sample MR analysis based on a publicly available genome-wide association study (GWAS) database of large samples.
Correlation Analysis
MR analysis relies on three fundamental assumptions.20,21 The initial assumption posits a robust correlation between IVs and sleep traits, sedentary leisure behavior, and physical activity.22 The assumption of independence denotes that IVs and the outcome variable (female reproductive health) remained uncorrelated with any other confounding factors.23 The last assumption assumes that IVs can solely impact female reproductive health by modulating these life factors without the involvement of any additional pathways (Figure 1). The GWAS data related to sleep characteristics, leisure sedentary behavior, and physical activity as well as the GWAS data of female reproductive health-related traits are presented in Tables 1 and 2. This Mendelian randomization study is conducted within the framework provided by the STROBE-MR checklist, which ensures a systematic and transparent approach, which the detailed information was showed in Supplementary Table S1.
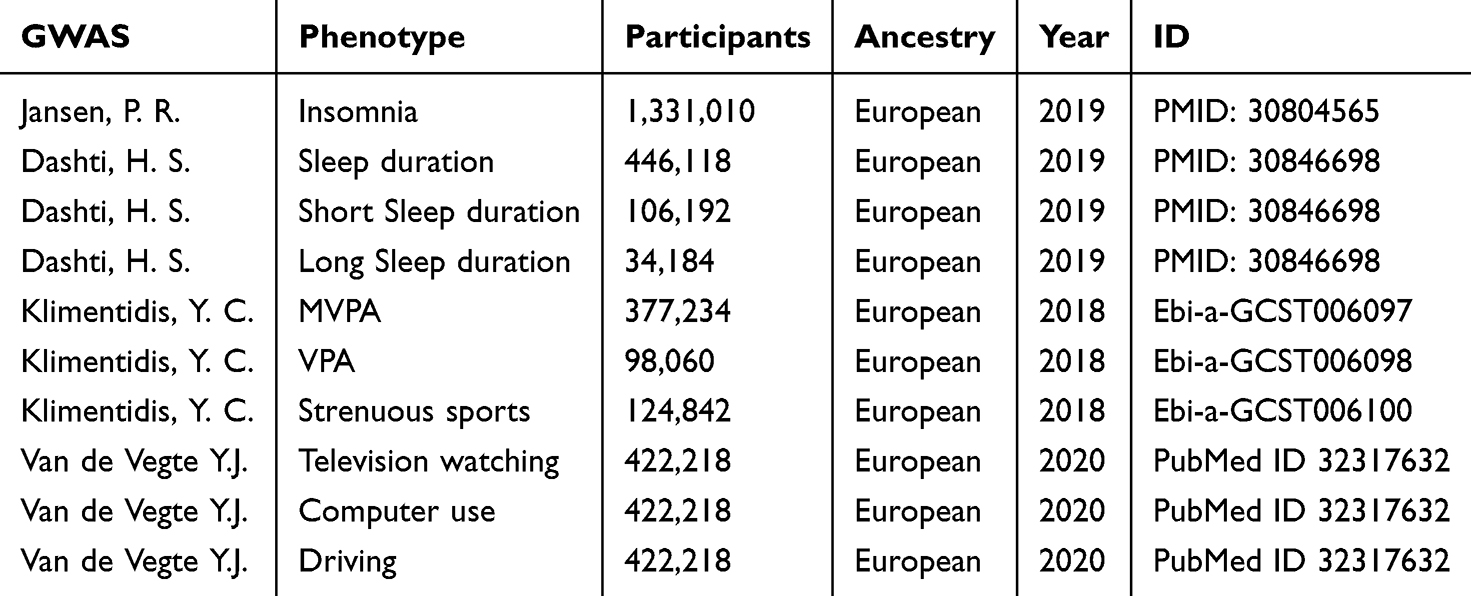 |
Table 1 GWAS Data Pertaining to Sleep Traits, Leisure Sedentary Behavior and Physical Activity |
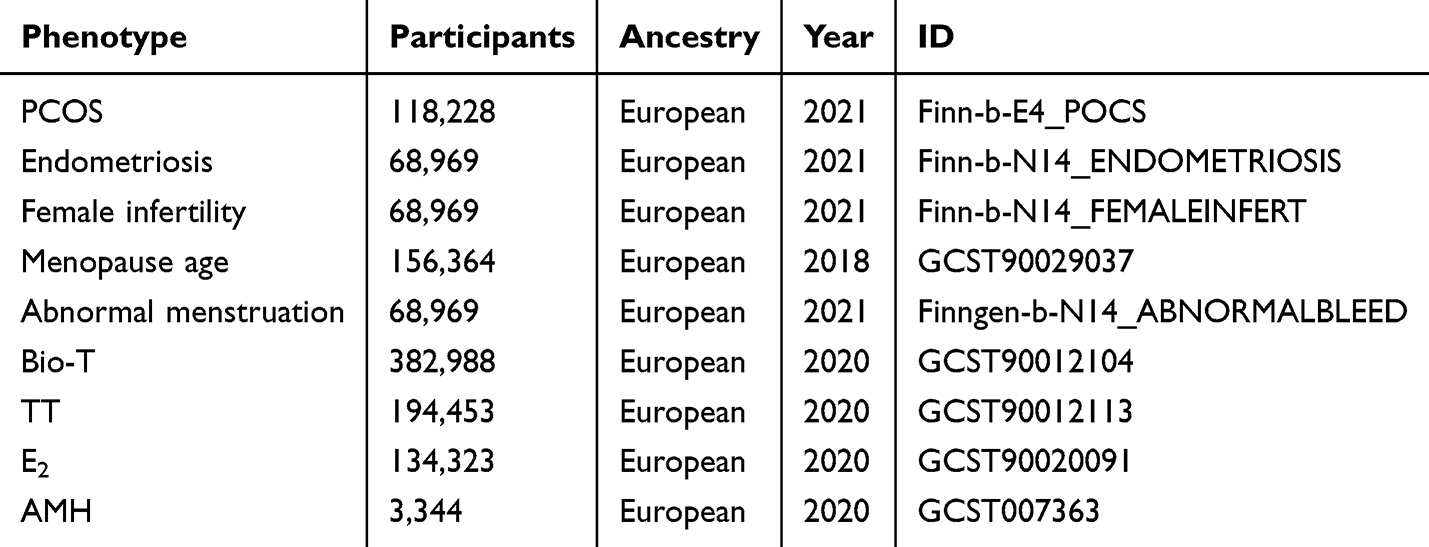 |
Table 2 GWAS Data Pertaining to Women’s Reproductive Health-Related Traits |
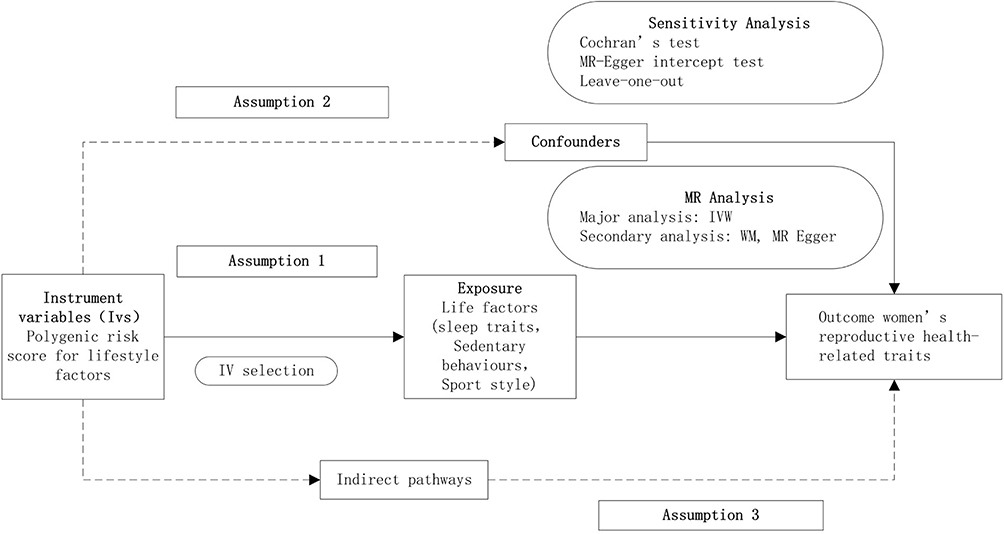 |
Figure 1 Flow chart of the two-samples MR analysis. |
To identify suitable IVs, we selected SNPs displaying strong associations as IVs. Rigorous screening and clumping of significant SNPs (p < 5e-08) for sleep traits and physical activity (p < 5e-07) were performed for sedentary behavior.21
Linkage Disequilibrium (LD)
LD indicates that genetic variants in close proximity tend to be inherited together, resulting in a greater likelihood that alleles from two or more loci will co-occur on a single chromosome. The screening criteria were as follows kb >10000bp and R2 < 0.01. To eliminate weak IVs, the F-statistic was used to assess their strength. When the F-value was less than ten, the IV was classified as weak, whereas an F-value greater than ten indicates a strong IV. The F-value and R2 (proportion of variance explained by the SNPs in the exposed database) were calculated using the following formulas:


R2 is the proportion of variance explained by the SNPs in the exposed database, EAF is the effect allele frequency, beta is the allele effect value, and SD is the standard deviation.
MR Analysis
Three main methods were employed to determine the causal relationship between exposure factors and reproductive health outcomes: inverse variance weighting (IVW), MR-Egger regression, and weighted median. The “Two-Sample MR” package in R language was used to visualize MR results with scatter, forest, and sensitivity analysis plots. Typically, the IVW method results are the primary gauge of MR analysis reliability, with a significance threshold of P < 0.05 indicating a positive outcome.22 The F-value of the SNPs was calculated using the R package “Mendelian Randomization”.
For the reliability of the final analysis results, the following screening criteria were used as filters for robust significant causality: IVW mainly suggested a significant causal relationship, the directions of the MR analysis result (beta values) were consistent among the three methods, and there was no heterogeneity or horizontal pleiotropy among the IVs. If the IVs meet the assumptions, the results were considered unbiased, and the standard error was less than that with the IVW. The main results with causal significance and without heterogeneity or pleiotropy are shown in forest plots, whereas the others are shown in the Supplementary Table S1.
Sensitivity Analysis
The IVW and MR-Egger tests were used to assess heterogeneity, with a significance level of P < 0.05, indicating the presence of heterogeneity in the studies. In cases where the IV influences the outcome through factors other than the exposure variable, it indicates the presence of pleiotropy. Pleiotropy can undermine the assumptions of independence and exclusivity as assessed using the MR-Egger intercept test. A P-value < 0.05 indicated the presence of pleiotropy in the data. We employed the “leave-one-out” method to conduct a sensitivity analysis. This approach entails systematically removing the results associated with individual SNPs, assessing whether they are outliers, and observing the stability of the results after the removal of each SNP. Additionally, a funnel plot was used to assess the symmetry of the SNPs and evaluate the reliability of the results.23
Results
The main results are presented in the text without heterogeneity or pleiotropy where the IVW suggested a significant causal relationship. We did not find a significant relationship between sedentary leisure behavior and female reproductive health. Physical activity might influence female sex hormones, though strong heterogeneity and pleiotropy were always present.
IV Screening
A total of 67 SNPs in “insomnia” displayed robust associations with ‘endometriosis’ and ‘abnormal menstruation’. Additionally, “long sleep duration” displayed ten SNPs associated with ‘endometriosis’ and six associated with ‘long sleep duration’ and ‘menopause age’. A total of six SNPs in “strenuous sports” demonstrated a robust association with female infertility. No weak IVs or confounding factors were detected in our analysis.
MR Analysis
We assessed the causal relationship between exposure factors and outcomes using IVW, MR-Egger regression, and weighted medians. The results showed that insomnia [odds ratio [OR] (95% confidence interval [CI]) IVW = 1.80 (1.16, 2.80), P = 0.009] was associated with endometriosis (Figure 2A) and abnormal menstruation [OR (95% CI) IVW = 2.37 (1.34, 4.20), P = 0.003; OR (95% CI) WM=2.64(1.24, 5.62), P = 0.012, respectively] (Figure 2B).
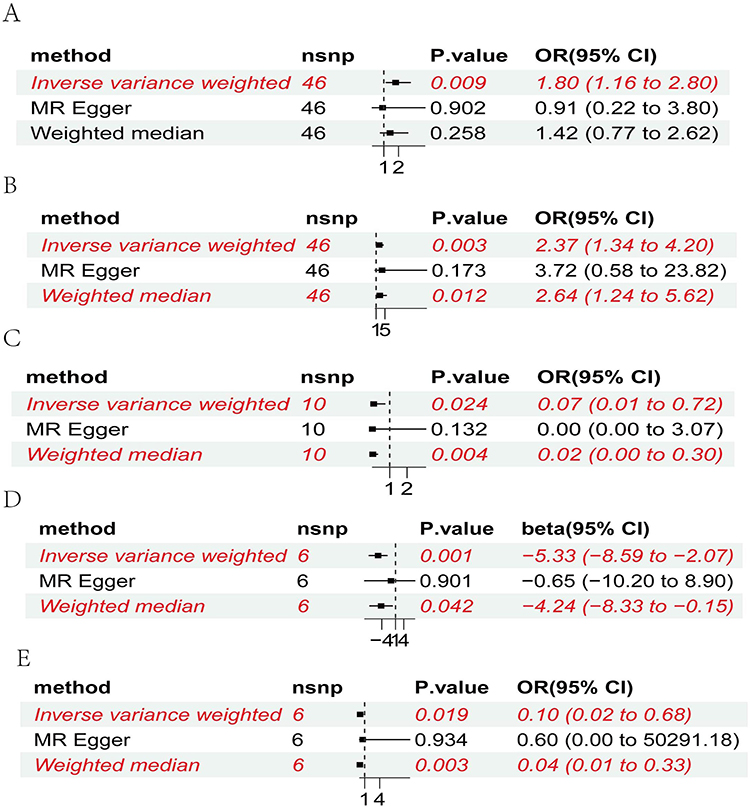 |
Figure 2 Forest plot of the causal relationship, primarily evaluated using the IVW method. (A) insomnia and endometriosis. (B) insomnia and abnormal menstruation. (C) long sleep duration and endometriosis. (D) long sleep duration and menopause age. (E) strenuous sports and female infertility. |
In addition, the IVW analysis suggested a positive association between long sleep duration and endometriosis [OR (95% CI) IVW = 0.07 (0.01, 0.72), P = 0.024; OR (95% CI) WM=0.02 (0.00, 0.30), P = 0.004] (Figure 2C). The long sleep duration initiation SNP IVW analysis showed potential causality for a positive effect on menopause age [beta (95% CI) IVW= −5.33 (0.00, 0.13), P = 0.001; beta WM=0.02, 95% CI = (0.00, 0.86), P = 0.042] (Figure 2D) after eliminating two SNPs with pleiotropy (rs55938136, rs3785884). Strenuous sports in women had a similar negative causality with female infertility [OR (95% CI) IVW = 0.1 (0.02, 0.68), P = 0.019; OR (95% CI) WM = 0.04 (0.00, 0.37), P = 0.004] (Figure 2E).
Sensitivity Analysis
We employed MR-Egger regression and IVW to assess the presence of heterogeneity; the results were P > 0.05, indicating the absence of heterogeneity. Subsequently, Egger regression was adopted to study whether directional pleiotropy existed. The results had P > 0.05 for all data sets, indicating that directional pleiotropy did not exist in any dataset.
A “leave-one-out” approach was employed to evaluate the influence of individual SNPs, and the results showed no significant impact on the effect size as shown in Supplementary Figure S1, it suggested robustness of the MR results. The linear relationship between exposure and outcome was assessed visually by the Scatter plot in Supplementary Figure S2. The funnel plot showed in Supplementary Figure S3 displays a symmetric distribution of SNPs, underscoring the relative stability of the results.
There is a certain degree of heterogeneity between insomnia and endometriosis, although it is not definite. However, the associations between insomnia and abnormal menstruation, long sleep duration and endometriosis, long sleep duration and menopause age, and strenuous sports and female infertility show relatively small heterogeneity, as indicated in Table 3.
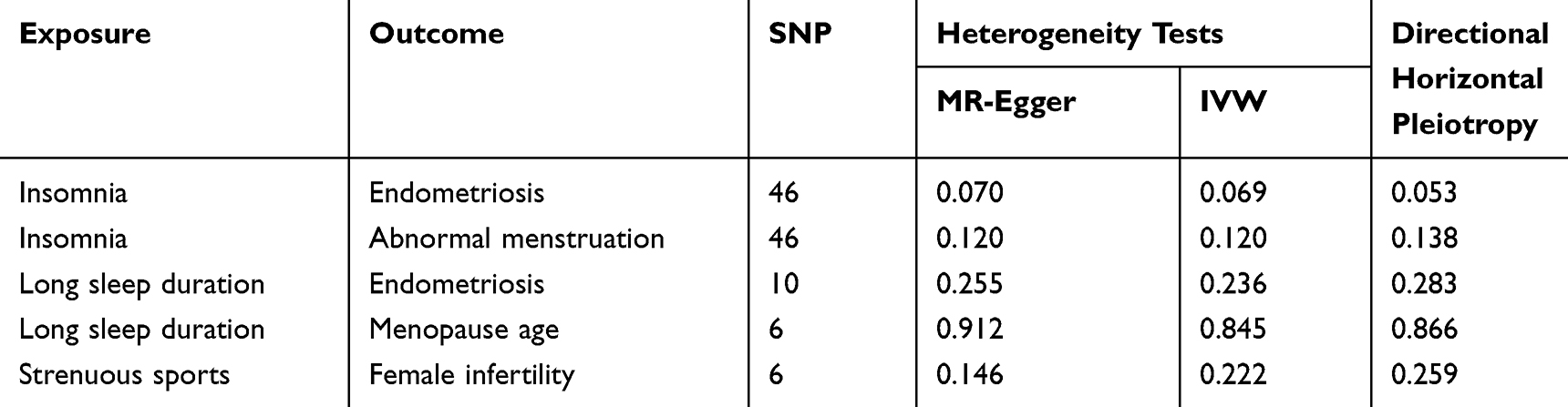 |
Table 3 Variation Scale and Heterogeneity Analysis |
Discussion
This study aimed to examine the causal relationship between sleep traits, physical activity, leisure sedentary behavior, and female reproductive health by utilizing publicly available large-sample GWAS data and conducting MR analysis using R. Most concomitant endometriosis symptoms, including dysmenorrhea, chronic pelvic pain, female infertility, and dyspareunia, are well-recognized; however, little attention has been given to insomnia symptoms.9 Studies have provided strong evidence that individuals with symptomatic endometriosis experience higher levels of sleep disturbance than those without,24,25 and a significant positive correlation exists between poor sleep quality and the intensity of dysmenorrhea or pelvic pain.26,27 Some authors have speculated that chronic pelvic pain or fatigue could potentially act as mediating factors in endometriosis and sleep disturbances.
In this study, a causal relationship between insomnia and endometriosis (OR (95% CI) IVW = 1.80 (1.16, 2.80); P = 0.009) was identified. Insomnia may be a risk factor for endometriosis, which adds weight to a previous study that revealed a significant association between night shift work, changes in sleep patterns during days off, and the risk of endometriosis.28 Additionally, long sleep duration was identified as a protective factor against endometriosis [OR (95% CI) IVW = 0.07 (0.01, 0.72), P = 0.024]. It is well known that endometriosis can impair sleep by increasing sleep disturbances and decreasing sleep duration and that long sleep might potentially prevent endometriosis. However, it is also possible that women with long sleep durations were more likely to escape endometriosis. Patients with insomnia are more likely to suffer from endometriosis, and those with endometriosis have a higher incidence of sleep disturbances. Collectively, these studies suggest a bidirectional relationship between sleep traits and endometriosis, possibly owing to changes in the immune or gynecologic endocrine systems.29 The chronic estrogen-dependent nature of endometriosis intensifies hormonal changes that may play a role in sleep disruption.30 One study demonstrated that hormonal treatment improved sleep disturbance but not sleep quality, daytime sleepiness, or insomnia;31 however, other studies have contradictory findings, and the mechanisms behind the effects of sleep traits on endometriosis require further investigation.
The association between sleep traits and the menstrual cycle has scarcely been studied. In this study, insomnia was found to have a positive causal relationship with abnormal uterine and vaginal bleeding (OR (95% CI), IVW = 2.37 (1.34, 4.20), p = 0.003), which is in agreement with a former systematic review.32 In a cross-sectional study, sleep duration and irregular menstrual cycles were significantly inversely correlated.33 One longitudinal study found that insomnia more than doubled the risk of menstrual cycle irregularity over a year; these associations became more predominant as the Insomnia Severity Index score increased.34 Individuals with sleep disturbances usually do not have regular circadian rhythms, which may be related to the irregular synthesis and secretion of female gonadal hormones. Sleep disorders inhibit gonadotropin-releasing hormone production in the pituitary gland, resulting in the reduced secretion of gonadal hormones.35,36 Lower estradiol levels and follicle-stimulating hormone levels are related to lower sleep variation, and luteinizing hormone pulse frequency is inhibited by sleep, showing a significant relationship between hormones and sleep traits, demonstrating the activation of the HPA axis.37–39 Consequently, during the activation of the HPA axis, corticotropin-releasing hormone inhibits gonadotropin-releasing hormone secretion, leading to hypothalamic amenorrhea.40 Female reproductive functions such as folliculogenesis, ovulation, menstruation, hormone synthesis, and secretion can be hindered by sleep deprivation, sleep disruption, and complex molecular genetics, and hormonal pathways play an important role in regulating these relationships.41 Similarly, sleep problems may exacerbate gynecological conditions; however, we found no relationship between short sleep duration and an abnormal menstrual cycle, in contrast to many other studies.42,43 In this study, we did not find evidence that rigorous exercise was a risk factor for menstrual cycle irregularities.44
Long sleep duration had negative causality with menopause age [beta (95% CI) IVW= −5.33 (0.00, 0.13), P = 0.001]. Sleep disturbance is a common condition during menopause transition.45 Regardless of sex, older adults exhibit poorer sleep consolidation than younger adults and menopausal transition causes poor sleep beyond the anticipated age-related effects.46 One study also found that short sleep duration was significantly associated with a later onset of menopause,28 possibly owing to the levels of neuroendocrine hormones. Cognitive behavioral therapy is the first-line treatment for insomnia in the general population; however, when vasomotor symptoms are present, menopausal hormone therapy should be considered.47
We observed a modest and significant genetic correlation between strenuous exercise and infertility [OR (95% CI) IVW = 0.1 (0.02, 0.68), P = 0.019]. Physically active females were more likely to be fertile, which is consistent with a previous observational study that reported that more females with normal fertility engaged in moderate to vigorous activity.14 However, other conservative studies have revealed that among females, excessive exercise may generally cause levels of engagement in physical activity to vary across individuals, and high levels of physical activity among females could result in an energy deficit, leading to hypothalamic amenorrhea, causing short-term infertility, and ultimately hindering fertility.48
One of the strengths of this study was that it leveraged a large sample of GWAS data, enhancing the reliability of the findings. Potential biases were also effectively mitigated through association analysis, LD analysis, elimination of weak IVs, and controlling for confounding factors. Additionally, a symmetrical distribution of SNPs was observed in the funnel plot, and both the pleiotropy and “leave-one-out” tests demonstrated the relative stability of the results. Despite this, there were also several limitations. We acknowledge that heterogeneity may originate from variations in analysis platforms, experimental conditions, population characteristics, and other IVs, even though both the MR-Egger regression and IVW methods yielded results with P-values > 0.05; consequently, a more comprehensive investigation of the sources of heterogeneity is warranted. This study also focused primarily on European populations, resulting in a paucity of GWAS data on Asian and African populations. The number of IVs for the SNPs within each dataset in this study was also relatively modest; is necessary to use large sample datasets to expand the pool of SNPs available as IVs for subsequent analyses. Additionally, although we employed MR to explore the causal relationship between exposure and outcomes, we did not investigate the underlying mechanisms.
In conclusion, our study suggests that insomnia and endometriosis might have reciprocal causations, and long sleep duration is a protective factor against endometriosis. It has also been genetically predicted that insomnia is a risk factor for abnormal uterine and vaginal bleeding. Improving sleep quality and prolonging sleep duration are potential intervention targets for the prevention of endometriosis and vaginal bleeding to improve female reproductive health.
Ethics Approval and Informed Consent
This study is based on Mendelian randomization, which involves the analysis of previously collected and anonymized genetic data from public databases. Given that the data are retrospective and do not involve any direct interaction with participants, the research is exempt from the need for ethical approval and informed consent. The data used are de-identified and have been ethically approved for research use by the original data collectors. Therefore, no additional ethical clearance or informed consent process is required for this particular study.
Acknowledgments
We express our gratitude to the IEU Open GWAS database (https://gwas.mrcieu.ac=/) for providing publicly available summary-level GWAS data for this study.
Author Contributions
All authors made substantial contributions to the reported work, covering conception, study design, execution, data acquisition, analysis, and interpretation. They participated in drafting, revising, or critically reviewing the article, gave final approval for publication, agreed on the submission journal, and are accountable for all aspects of the work.
Funding
This work was supported by grants from the Science and Technology Commission of Shanghai Municipality (22Y11906100) to Jing Sun and the Shanghai Outstanding Academic Leaders Plan to Jing Sun (Year 2019).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. This paper has been uploaded to ResearchSquare as a preprint: https://www.researchsquare.com/article/rs-4419372/v1.
References
1. Zoe B, Kirsty O, Courtney B, Emily M, Janice B, Yvonne H. Sexual and reproductive health education: midwives’ confidence and practices. Women Birth. 2021;35(4):360–366. doi:10.1016/j.wombi.2021.09.005
2. Rakesh S, Kelly RB, Jennifer MF, Ashok A. Lifestyle factors and reproductive health: taking control of your fertility. Reprod Biol Endocrinol. 2013;11:1–5.
3. Yoko U, Miyuki H, Shinnosuke K, et al. Lifestyle and fertility-specific quality of life affect reproductive outcomes in couples undergoing in vitro fertilization. Front Endocrinol. 2024;15:1346084.
4. Kathryn Aldrich L, Fiona CB. Sleep and Women’s Health Across the Lifespan. Sleep Med Clin. 2018;13(3):xv–xvi. doi:10.1016/j.jsmc.2018.06.001
5. Joyce AW. Women and sleep. Handb Clin Neurol. 2010;98:639–651.
6. Elin Rosenbek S, Thea Otte A, Agnete Skovlund D, et al. Night-time smartphone use, sleep duration, sleep quality, and menstrual disturbances in young adult women: a population-based study with high-resolution tracking data. Sleep Adv. 2023;4(1):zpad013. doi:10.1093/sleepadvances/zpad013
7. Meers JM, Nowakowski S. Sleep, premenstrual mood disorder, and women’s health. Curr Opin Psychol. 2020;34:43–49. doi:10.1016/j.copsyc.2019.09.003
8. Kloss JD, Perlis ML, Zamzow JA, Culnan EJ, Gracia CR. Sleep, sleep disturbance, and fertility in women. Sleep Med Rev. 2015;22:78–87. doi:10.1016/j.smrv.2014.10.005
9. Ishikura IA, Hachul H, Pires GN, Tufik S, Andersen ML. The relationship between insomnia and endometriosis. J Clin Sleep Med. 2020;16(8):1387–1388. doi:10.5664/jcsm.8464
10. Booth FW, Roberts CK, Laye MJ. Lack of exercise is a major cause of chronic diseases. Compr Physiol. 2012;2(2):1143–1211.
11. Leandro Fornias Machado DR, Maurício RL, Juan Pablo R-L, Victor Keihan Rodrigues M, Olinda Do Carmo L. Sedentary behavior and health outcomes: an overview of systematic reviews. PLoS One. 2014;9(8):e105620. doi:10.1371/journal.pone.0105620
12. Siret L, O FB, Theodora KK, et al. Physical and Sedentary Activities in Association with Reproductive Outcomes among Couples Seeking Infertility Treatment: a Prospective Cohort Study. Int J Environ Res Public Health. 2021;18(5):2718. doi:10.3390/ijerph18052718
13. Vickà V, Lara S, Dirk A, et al. Dietary intake, physical activity and sedentary behavior and association with BMI during the transition to parenthood: a prospective dyadic study. Front Public Health. 2023;11:1092843. doi:10.3389/fpubh.2023.1092843
14. Brinson AK, da Silva SG, Hesketh KR, Evenson KR. Impact of Physical Activity and Sedentary Behavior on Spontaneous Female and Male Fertility: a Systematic Review. J Phys Act Health. 2023;20(7):600–615. doi:10.1123/jpah.2022-0487
15. Dana NJ, Shannon W. Stress and the HPA Axis: balancing Homeostasis and Fertility. Int J mol Sci. 2017;18(10):2224. doi:10.3390/ijms18102224
16. Stephen B, Adam B, Simon GT. Mendelian randomization analysis with multiple genetic variants using summarized data. Genet Epidemiol. 2013;37(7):658–665. doi:10.1002/gepi.21758
17. Christopher JY, Su Yeon K, Chang Hyun N, et al. Estimation of intrafamilial DNA contamination in family trio genome sequencing using deviation from Mendelian inheritance. Genome Res. 2023;32(11–12):2134–2144.
18. Jiang Z, He R, Wu H, et al. The causal association between smoking initiation, alcohol and coffee consumption, and women’s reproductive health: a two-sample Mendelian randomization analysis. Front Genet. 2023;14:1098616. doi:10.3389/fgene.2023.1098616
19. Ling S, Dai Y, Weng R, et al. Epidemiologic and genetic associations of female reproductive disorders with depression or dysthymia: a Mendelian randomization study. Sci Rep. 2024;14(1):5984. doi:10.1038/s41598-024-55993-8
20. Jack B, George DS, Stephen B. Mendelian randomization with invalid instruments: effect estimation and bias detection through Egger regression. Int J Epidemiol. 2015;44(2):512–525. doi:10.1093/ije/dyv080
21. Zhang XB, Jiang HH, Zhang LL, et al. Potential causal associations between leisure sedentary behaviors, physical activity, sleep traits, and myopia: a Mendelian randomization study. BMC Ophthalmol. 2024;24(1):104. doi:10.1186/s12886-024-03367-z
22. Jin T, Huang W, Cao F, et al. Causal association between systemic lupus erythematosus and the risk of dementia: a Mendelian randomization study. Front Immunol. 2022;13:1063110. doi:10.3389/fimmu.2022.1063110
23. Zhu K, Shi J, Yang R, Zhou C, Liu Z. Evidence based on Mendelian randomization: causal relationship between mitochondrial biological function and lung cancer and its subtypes. Neoplasia. 2023;46:100950. doi:10.1016/j.neo.2023.100950
24. Pickup B, Coutts-Bain D, Todd J. Fear of progression, depression, and sleep difficulties in people experiencing endometriosis-pain: a cross-sectional study. J Psychosom Res. 2024;178:111595. doi:10.1016/j.jpsychores.2024.111595
25. Leone Roberti Maggiore U, Bizzarri N, Scala C, et al. Symptomatic endometriosis of the posterior cul-de-sac is associated with impaired sleep quality, excessive daytime sleepiness and insomnia: a case-control study. Eur J Obstet Gynecol Reprod Biol. 2017;209:39–43. doi:10.1016/j.ejogrb.2015.11.026
26. Baker F, Driver H, Rogers G, Paiker J, Mitchell D. High nocturnal body temperatures and disturbed sleep in women with primary dysmenorrhea. Am J Physiol. 1999;277(6):E1013–1021. doi:10.1152/ajpendo.1999.277.6.E1013
27. Dunlap K, Yu L, Fisch B, Nolan T. Polysomnographic characteristics of sleep disorders in chronic pelvic pain. Prim Care Update Ob Gyns. 2000;5(4):195. doi:10.1016/S1068-607X(98)00124-3
28. Nagata C, Wada K, Yamakawa M, Nakashima Y, Sugino M, Mori T. Sleep duration and the onset of menopause in Japanese women. Menopause. 2023;30(4):437–440. doi:10.1097/GME.0000000000002156
29. Facchin F, Buggio L, Roncella E, et al. Sleep disturbances, fatigue and psychological health in women with endometriosis: a matched pair case-control study. Reprod Biomed Online. 2021;43(6):1027–1034. doi:10.1016/j.rbmo.2021.08.011
30. Wang Y, Nicholes K, Shih IM. The Origin and Pathogenesis of Endometriosis. Annu Rev Pathol. 2020;15(1):71–95. doi:10.1146/annurev-pathmechdis-012419-032654
31. Bergqvist A, Theorell T. Changes in quality of life after hormonal treatment of endometriosis. Acta Obstet Gynecol Scand. 2001;80(7):628–637. doi:10.1034/j.1600-0412.2001.800708.x
32. Jeon B, Baek J. Menstrual disturbances and its association with sleep disturbances: a systematic review. BMC Women's Health. 2023;23(1):470. doi:10.1186/s12905-023-02629-0
33. Nam GE, Han K, Lee G. Association between sleep duration and menstrual cycle irregularity in Korean female adolescents. Sleep Med. 2017;35:62–66. doi:10.1016/j.sleep.2017.04.009
34. WonYang K, Keun-Ho J, Hyeong-Min L, Ji-Sung A, Won-Ju P. The menstrual cycle associated with insomnia in newly employed nurses performing shift work: a 12-month follow-up study. Int Arch Occup Environ Health. 2018;92(2):227–235. doi:10.1007/s00420-018-1371-y
35. Karen LG, David R, Carl Hirschie J. Shift work and circadian dysregulation of reproduction. Front Endocrinol (Lausanne). 2013;4:92.
36. Wen-Pei C, Yu-Pei C. Meta-Analysis Comparing Menstrual Regularity and Dysmenorrhea of Women Working Rotating Shifts and Fixed Day Shifts. J Women's Health (Larchmt). 2020;30(5):722–730. doi:10.1089/jwh.2020.8517
37. Vgontzas AN, Bixler EO, Lin HM, et al. Chronic insomnia is associated with nyctohemeral activation of the hypothalamic-pituitary-adrenal axis: clinical implications. J Clin Endocrinol Metab. 2001;86(8):3787–3794. doi:10.1210/jcem.86.8.7778
38. Hall JE, Sullivan JP, Richardson GS. Brief wake episodes modulate sleep-inhibited luteinizing hormone secretion in the early follicular phase. J Clin Endocrinol Metab. 2005;90(4):2050–2055. doi:10.1210/jc.2004-2033
39. Sandrine T, Muriel R, Hans B, Enriqueta B, René E. Relationship between sleep and secretion of gonadotropin and ovarian hormones in women with normal cycles. Fertil Steril. 2002;77(4):738–744. doi:10.1016/S0015-0282(01)03254-X
40. Marshall J. The menstrual cycle and disorders of ovulation. In: Endocrinology: Adult and Paediatric. Philadelphia: Elsevier Saunders Publishing; 2016:2231–2241.
41. Zhang Y, Luo Z, Jia Y, et al. Development and validation of a predictive model of abnormal uterine bleeding associated with ovulatory dysfunction: a case-control study. BMC Women's Health. 2023;23(1):536. doi:10.1186/s12905-023-02589-5
42. Lim AJR, Huang Z, Chua SE, Kramer MS, Yong E-L. Sleep Duration, Exercise, Shift Work and Polycystic Ovarian Syndrome-Related Outcomes in a Healthy Population: a Cross-Sectional Study. PLoS One. 2016;11(11):e0167048. doi:10.1371/journal.pone.0167048
43. Taeryoon K, Ga Eun N, Byoungduck H, et al. Associations of mental health and sleep duration with menstrual cycle irregularity: a population-based study. Arch Women's Ment Health. 2018;21(6):619–626. doi:10.1007/s00737-018-0872-8
44. Jensen T, Scheike T, Keiding N, Schaumburg I, Grandjean P. Fecundability in relation to body mass and menstrual cycle patterns. Epidemiology. 1999;10(4):422–428. doi:10.1097/00001648-199907000-00014
45. Baker FC, Lampio L, Saaresranta T, Polo-Kantola P. Sleep and Sleep Disorders in the Menopausal Transition. Sleep Med Clin. 2018;13(3):443–456. doi:10.1016/j.jsmc.2018.04.011
46. Shaver J, Woods N. Sleep and menopause: a narrative review. Menopause (New York, N.Y.). 2015;22(8):899–915. doi:10.1097/GME.0000000000000499
47. Proserpio P, Marra S, Campana C, et al. Insomnia and menopause: a narrative review on mechanisms and treatments. Climacteric: the Journal of the International Menopause Society. 2020;23(6):539–549. doi:10.1080/13697137.2020.1799973
48. Evenson KR, Hesketh KR. Studying the Complex Relationships Between Physical Activity and Infertility. Am J Lifestyle Med. 2016;10(4):232–234. doi:10.1177/1559827616641379
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Causal Association Between Sleep Traits and Endometriosis: A Mendelian Randomization Study
Li J, Wan W, Hu L, Ren Y, Ge L, Liu Y, Liu P, Cui L
International Journal of Women's Health 2026, 18:565217
Published Date: 6 February 2026