")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 12
Catastrophic Out-of-Pocket Health Expenditure Among Rural Households in the Semi-Pastoral Community, Western Ethiopia: A Community-Based Cross-Sectional Study
Authors Shikuro D, Yitayal M , Kebede A, Debie A
Received 8 October 2020
Accepted for publication 22 December 2020
Published 31 December 2020 Volume 2020:12 Pages 761—769
DOI https://doi.org/10.2147/CEOR.S285715
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Dean Smith
Debelo Shikuro,1 Mezgebu Yitayal,2 Adane Kebede,2 Ayal Debie2
1Benshangul-Gumuz National Regional State Health Bureau, Assossa, Ethiopia; 2Department of Health Systems and Policy, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Correspondence: Mezgebu Yitayal
Department of Health Systems and Policy, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, P. O. Box 196, Gondar, Ethiopia
Tel +251 947057683
Email [email protected]
Background: Every year, 808 million people face catastrophic health expenditure (CHE), and 122 million people were pushed into poverty. It aggravates healthcare inequalities, incurs double burden opportunity costs, and pushes households to sit in a deep poverty trap. A few studies have been done so far; however, it is not enough to inform policy decisions. Therefore, this study aimed to assess the catastrophic out-of-pocket health expenditure and associated factors among rural households in Mandura District, Western Ethiopia.
Methods: We conducted a community-based cross-sectional study among the Mandura district’s 488 rural households from April to May 2017. We used a multistage systematic sampling technique to select the participants. We fitted a binary logistic regression model to identify the factors associated with catastrophic out-of-pocket health expenditure. We used the adjusted odds ratio (AOR) with 95% CI and the p-value < 0.05 to determine the variables associated with catastrophic out-of-pocket health expenditure.
Results: Catastrophic health expenditure (CHE) with a 40% capacity to pay (CTP) households in the study area was 22.5%. Female household head (AOR = 2.92; 95% CI: 1.44, 5.93) and household with chronic illnesses (AOR = 3.93; 95% CI: 1.78, 9.14) were positively associated with CHE and, while households who had adult household members (AOR = 0.32; 95% CI: 0.16, 0.63) were negatively associated.
Conclusion: The overall CHE, with a 40% CTP threshold, was high. Prevention of chronic illness might help to reduce the burden of the expenditure. Strengthening financial risk protection mechanisms, such as community-based health insurance, could help bring healthcare services equity.
Keywords: catastrophic out-of-pocket health expenditure, semi-pastoral community, Ethiopia
Background
Out-of-pocket (OOP) health expenditure refers to the payments made by households at the point they receive health services,1 and it is the principal payment methods for health care services in developing countries.1–3 Fee for service, capitation, case-based, and global budget- based provider payment mechanisms are other payment mechanisms for health care services.4 Out-of-pocket for healthcare is termed as catastrophic when the total health expenditure equals or exceeds 40% of the total household’s capacity to pay.1,2,5 The household’s capacity to pay (CTP) is the non-subsistence effective household income and the minimum requirement to maintain basic life in society. Households’ ability to pay for health care and the denominator is total household expenditure (or sometimes income), which assumes that all household resources are available for spending on health using the budget share method.1,2,6 A study conducted across 133 countries in 2010 indicated that more than 808 million people incurred catastrophic health expenditure (CHE)7 and 122 million people were pushed into poverty.8 Between 2000 and 2010, CHE incidence increased from 9.7% to 11.7%, proving the lack of financial protection progress.7,8 In low- and middle-income countries, CHE pulverizes households’ income and labor supply.9 It disrupts households’ welfare and pushes them into impoverishment, exacerbates their poverty, and hampers healthcare-seeking behaviors.10–13 It also creates socio-economic and health disparity among households; and compels them to cut spending on necessities, sell assets, and borrow from the wealthiest households; and makes them sink into the poverty trap.14
Studies showed that CHE with a 40% CTP threshold ranged from 4.12–73% [15–19], and CHE concentration among the poor was also high.15–18 Evidence also showed that socio-demographic and economic factors healthcare service and disease-related factors are significantly associated with CHE. These include wealth status, residence, employment and educational status of household head, working conditions of adults, vulnerable and aged members in the household, household size, age, and sex of the household head.12,14,19–21 Healthcare financing in Ethiopia is still dependent on OOP expenditure with low government spending, which may lead to inefficient and inequitable healthcare utilization, and households to be impoverished because of poorly harmonized and unpredictable donors.22 Community-Based Health Insurance (CBHI) schemes and subsidizing some priority interventions’ costs through exemptions22,23 can protect households from financial risks.
However, subsidizing some treatment costs on specific diseases remains unclear, and whether the subsidies have been providing reasonable financial protection to the target households. Previous studies conducted to assess the effect of disease-specific medical costs on household economic status have not well described which illnesses had the highest impact on household expenditures. Health facilities provided a fee waiver for the poorest households, but the health access for a fee waiver has not been adequately addressed because of unclear selection criteria.22
In developing countries, including Ethiopia, the payment mechanism for the healthcare cost is mainly OOP paid at the time of sickness or point of service delivery, which could inhibit healthcare access and lead to impoverishment.24 To curb this problem, the Government of Ethiopia began to implement the Community Based Health Insurance (CBHI) in 2010.25 The CBHI is a non-profit health insurance scheme for the informal sector, formed based on an ethic of mutual aid and the collective pooling of health risks, in which members participate in its management.26 In Ethiopia, the premium for CBHI has been the same (US$ 8.27 per annum) for all households, regardless of economic status.25
As such a flat premium is inequitable, the government is working to introduce a stratified premium based on households’ willingness and ability to pay. However, CBHI was not introduced in the study area at the time of our study, and the households in the district had been paid a fee for service to the health service provider facilities for the services received. A few studies have been done so far; however, the findings did not explain the local context. Therefore, this study aimed to assess the CHE and associated factors among rural households in Mandura district in western Ethiopia.
Materials and Methods
Study Design and Settings
We used a community-based cross-sectional study to assess CHE and associated factors among the Mandura District’s rural households in Benishangul-Gumuz National Regional State (BGNRS) from April May 2017. The district is located in the western part of Ethiopia, and it is 547 kilometers far away from Addis Ababa, the capital city of Ethiopia. It has 20 kebeles (the lowest administrative unit), of which two were urban and 18 rural kebeles. The 2017 Central Statistical Agency (CSA) report indicated that the district had a total population of 55,371 and total households of 12,304.
Population and Sampling Procedures
All households in the selected rural kebeles of Mandura District were the study population. We included all self-reliant households in the selected rural kebeles of Mandura District in the study. However, we excluded new couples who became a household for less than a month during the data collection period from the study.
The sample size was determined using the single population proportion formula with the assumptions of 10.3% proportion (p) of OOPHE in Kenya,27 4% margin of error, design effect of 2, and 10% non-response rate. As a result, the final sample was 488. We used a multistage systematic sampling technique to select the households. In this study, we randomly selected six kebeles from 18 rural kebeles, and the sample size, ie, we proportionally allocated 488 households for each selected kebele. Then, we used the most recent number of households in the district health office to determine the interval and a systematic random sampling technique to select households after a random selection of the first household.
Study Variables
Response Variable
The response variable for this study was CHE. It was categorized into two: Yes if the total health expenditure of a household equals or exceeds 40% of the total household’s capacity to pay, and No if the total health expenditure of a household is below 40% of the total household’s capacity to pay. We collected data on household’s food expenditure; household’s OOP payments for health, including direct health expenditures such as diagnosis and treatment, and health service utilization; and household’s capacity to pay; household’s subsistence expenditure; and equivalent household’s size to estimate CHE.
We assessed the household food expenditure by measuring the amount of money spent on all foodstuffs by the household, plus the values of home-made food consumptions within the household. On some occasions, we measured food expenditure using a day recall period. We used the six-month recall period to assess the cost of clothes’ expenditures to reduce recall bias. Finally, we converted the costs incurred daily for a month by multiplying by 30. However, the costs for alcoholic beverages, tobacco, and food consumption outside the home, such as hotels and restaurants, were excluded from the cost calculation.1 At last, we converted all the expenditures to a monthly figure.
A 30 days’ household OOPHE expenditure was estimated by asking the respondents how much their households had spent for consultation or diagnosis, drugs, other medical supplies, hospitalization, traditional healers, and home remedies. We calculated the household’s capacity to pay by subtracting subsistence expenditure for each household from the household’s total expenditure. We calculated subsistence expenditure for each household by multiplying the equivalent household size by the poverty line. Similarly, the equivalent household size was determined by multiplying the household size by the household scale multiplier (β) = 0.56.1
Explanatory Variables
The study’s explanatory variables were socio-demographic and economic characteristics and health-related characteristics of the participants. These included sex, marital status, ethnicity, educational status, family size, number of children, number of working adults, number of elderly, age and occupation of the head of household, vulnerable members, employment status of head of household, wealth status, perception towards healthcare seeking, type of disabilities, and occurrence of other co-morbidities including in the last 12 months before the actual data collection.28–33
Data Collection Procedures
A structured interviewer-administered questionnaire was developed by reviewing literature.20,21,27 The questionnaire (Appendix 1) was first developed in English and translated to Amharic and back to English to check its consistency. We gave one day of training to data collectors and supervisors on the basic techniques of data collection. The data were collected using six diploma graduated clinical nurses supervised by two BSc graduated clinical nurses and a medical laboratory technologist.
The questionnaire was pre-tested to check for its validity among 24 participants in Gigda Selase kebele. This kebele was excluded from the sample during the actual data collection period to reduce information contamination. We corrected any unclear and ambiguous findings during the pre-testing of the questionnaire. Then, in the final data collection, the data collectors supervised by the supervisors and the principal investigator filled in the questionnaire. All the collected data were checked for completeness, accuracy, and consistency by the supervisors and the principal investigator daily.
Data Management and Analysis
The collected data were entered into Epi Info version 7 and exported to SPSS version 20 for analysis. We used graphs and tables to present descriptive statistics. We fitted a binary logistic regression model and entered variables with a p-value of less than 0.2 in the bivariable logistic regression into multivariable logistic regression analysis. We used a p-value less than 0.05 and Adjusted Odds Ratio (AOR) with 95% CI to identify variables significantly associated with CHE.
Results
Socio-Demographic and Economic Characteristics
A total of 479 household heads participated in the study with a response rate of 98.2%. The study revealed that 84.8% of respondents’ household heads were males, 84.3% were married and lived together with their spouses, 62.8% were Gumuz ethnic groups and 87.5% had no formal education, and 50.5% were Orthodox Christian followers. Ninety percent of the households had at least one <5 children, and 51.1% had more than five family members. About 90% of the households had working adult HH members, and 40.08% were poor. The average HHs size was 5.7 ± (1.99 SD) (Table 1).
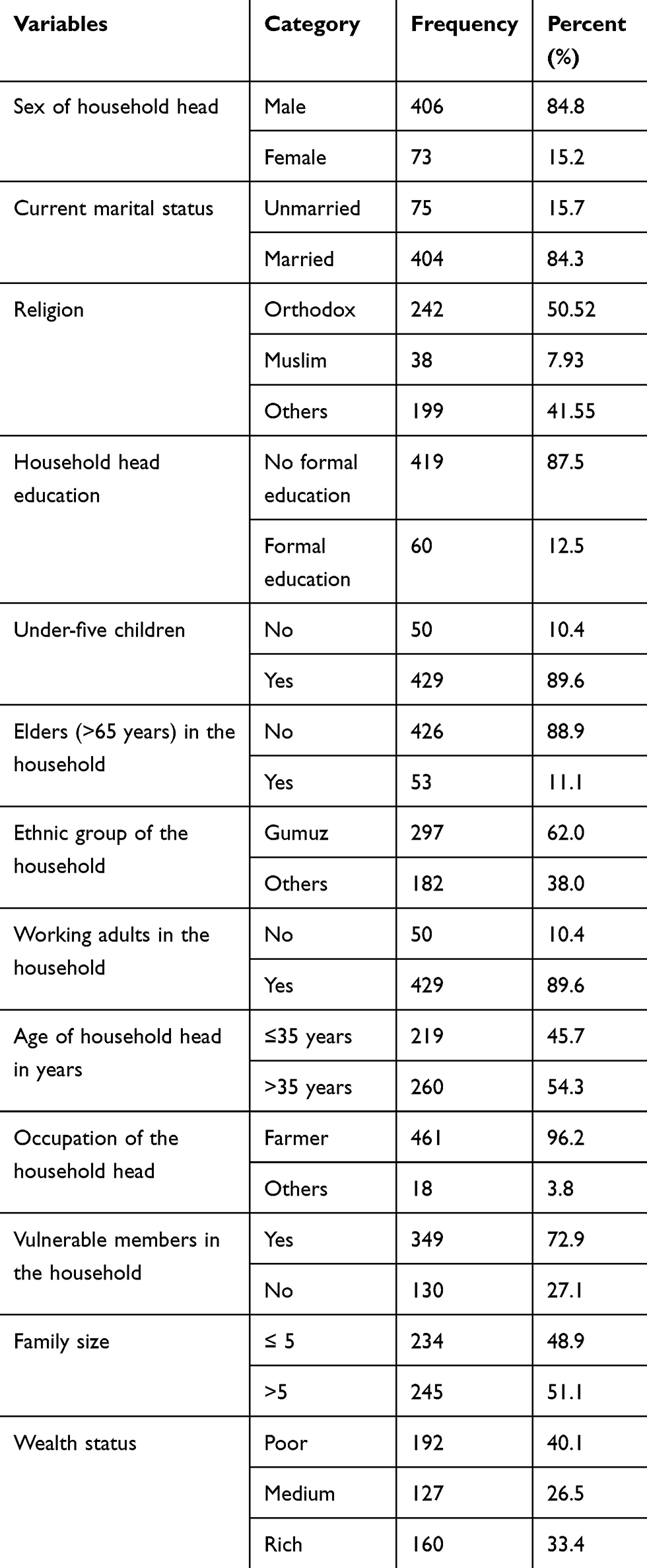 |
Table 1 Socio-Economic and Demographic Characteristics of Households in the Semi-Pastoral Community of Mandura District, Western Ethiopia, 2017 (n = 479) |
Disease and Service-Related Characteristics
The study revealed that 5.4% of the households had a household member with chronic illnesses, and 30.1% had a household member with acute illness and/or injury in the last month. Among those who had a chronic illness or acute and/o injury, 97.6% got medical treatment or counseling services for their illnesses, 75.3% got treatment from a public facility, and 86.1% were treated at the outpatient department. The study also revealed that 96.6% of the participants did not get any subsidies for their treatment cost, and the duration of treatment for 57.8% of the participants was shorter than six days (Table 2).
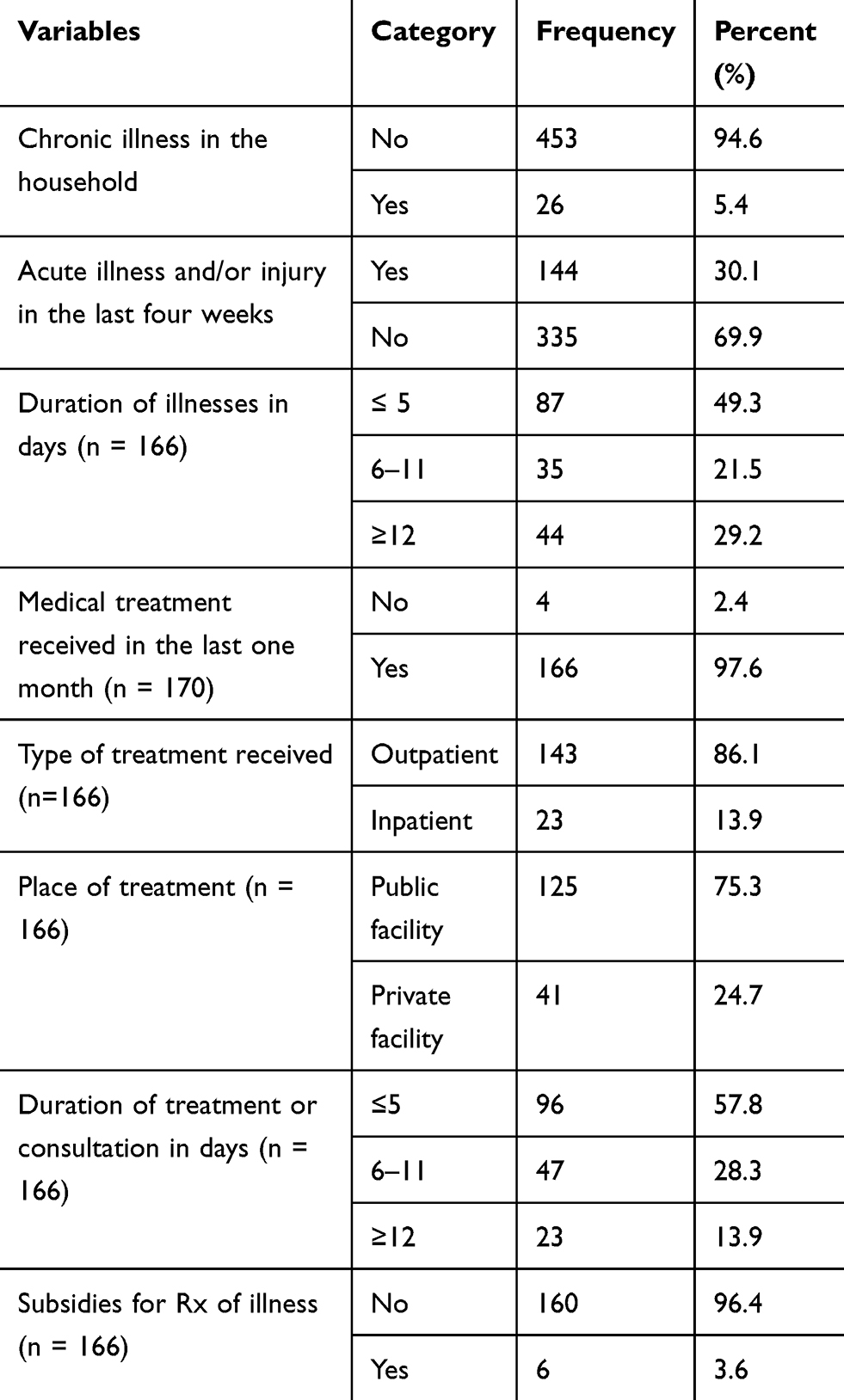 |
Table 2 Disease and Health Service-Related Characteristics of Participants in the Semi-Pastoral Community of Mandura District, Western Ethiopia, 2017 (n = 479) |
Distributions and Level of Catastrophic OOP Health Expenditures
The study revealed that 22.5% (95% CI: 19.0, 26.3) of the households had encountered CHE with a 40% capacity to pay threshold. The total average monthly household expenditure in this study was Ethiopian Birr (ETB) 1796± 927.90 ETB (Ethiopian Birr), which was equivalent to 64.88±33.52 US$ (United States of America Dollar). The respondents spent US$ 53.33± 18.49 or ETB 1476.09 ± 511.8 for food and US$ 6.39±22.69 or ETB 177.0 ± 628.0 for their health per household. The study also revealed that the mean subsistence expenditure that the households had spent on maintaining their basic life was US$ 53.76± 11.14 or ETB 1488.0 ± 308.30, and the mean of household’s ability to pay for healthcare services was US$ 15.53± 4.15 or ETB 429.9 ± 115.0 (Table 3).
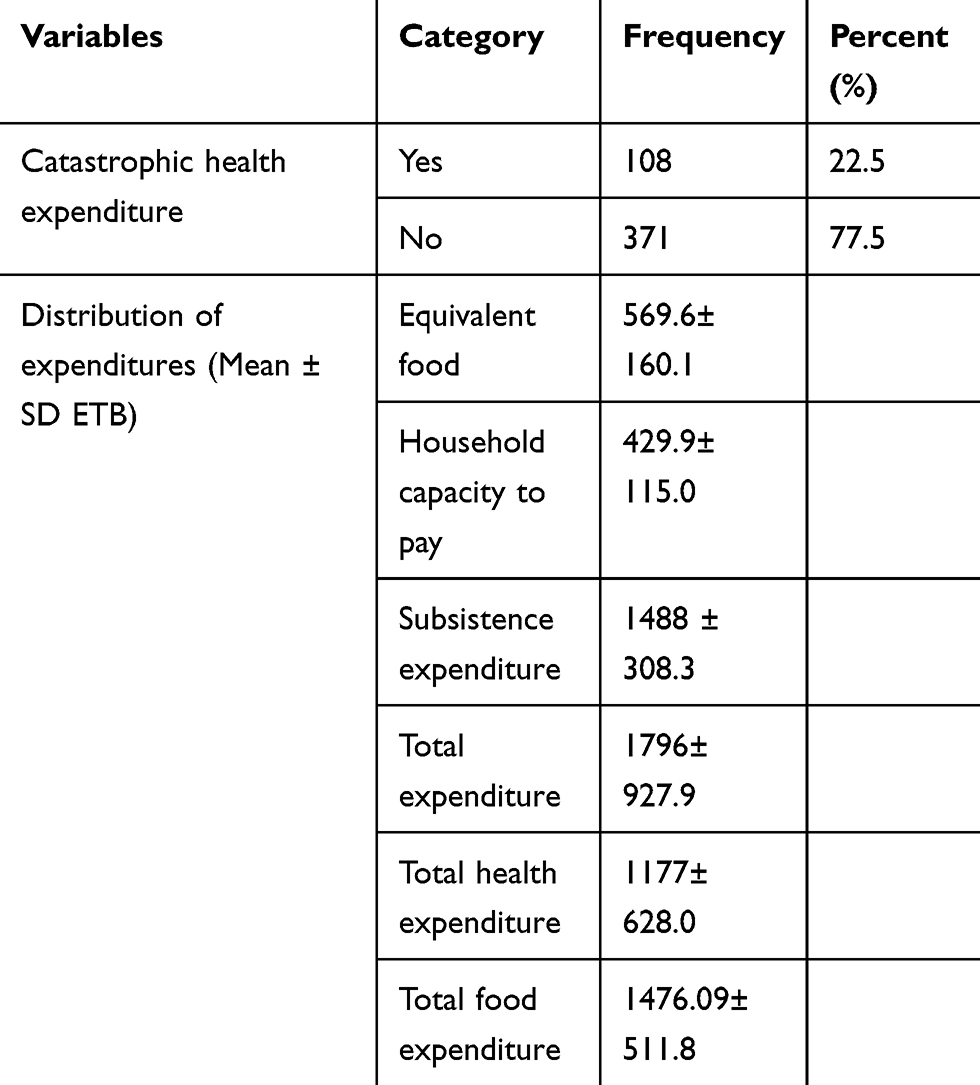 |
Table 3 Distributions of Household Expenditures and Level of Catastrophic OOP Health Expenditures in the Semi-Pastoral Community of Mandura District, Western Ethiopia, 2017 |
Factors Associated with Catastrophic Out-of-Pocket Health Expenditures
This study indicated that the sex of the household’s head, the presence of working adults in the household, and having members of the household with any chronic diseases were factors significantly associated with CHE with a 40% capacity to pay threshold. Households which had female household head were 2.92 times (AOR = 2.92; 95% CI: 1.44, 5.93) more likely to encounter CHE compared with male HH heads. Households that had a member of working adults were 68% (AOR = 0.32; 95% CI: 0.16, 0.63) times less likely to face CHE compared to households who had no working adults. Moreover, household members with any chronic illnesses were 3.93 (AOR = 3.93; 95% CI: 1.78, 9.14) times more likely to encounter CHE than their counterparts (Table 4).
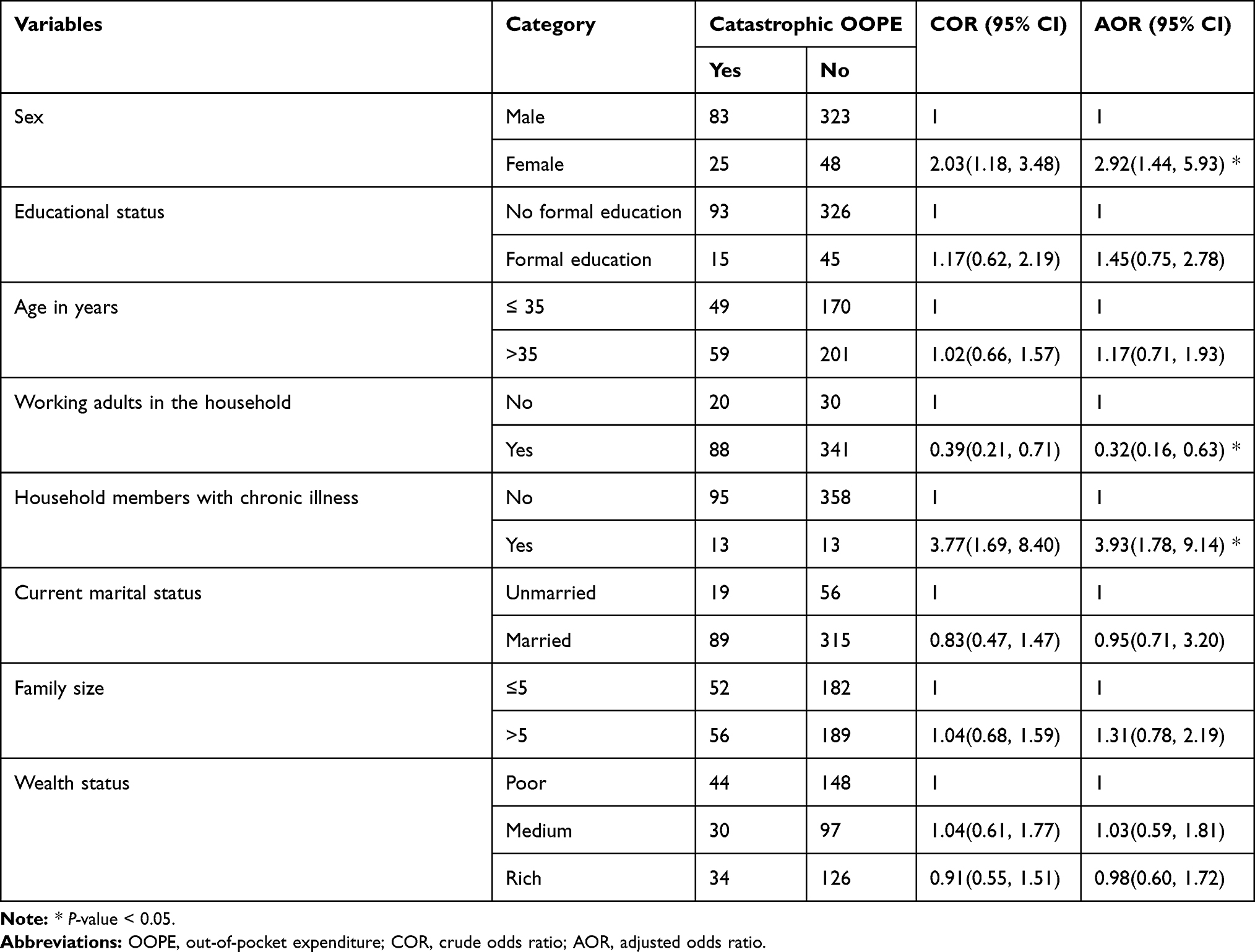 |
Table 4 Factors Associated with Catastrophic OOP Health Expenditure in Mandura District in Western Ethiopia, 2017 |
Discussion
CHE pulverizes households’ income and labor supply in low and middle-income countries.9 It disrupts households’ welfare and pushes them into impoverishment, and hampers healthcare-seeking behaviors.10–13 The level of CHE with 40% of the capacity to pay (CTP) in the Mandura district was 22.5% (95% CI: 19.0, 26.3). This study finding is consistent with CHE studies conducted in Iran (22.2%) and India (23.4%),30,31 and gastrointestinal cancer patients in Iran (73%).17 This finding was lower than the studies done in China (24.79%) and Kenya (28.3%).32,33 On the other hand, the CHE in this study was higher than studies done in Egypt (6.0%),12 Colombia (9.6%),14 Iran (4.12_17.7%),15–18,34,35 Nepal (13.8%),28 and Tanzania (18%).29 The possible reasons for these differences might be the variability in key preconditions for catastrophic health expenditures since the amount of OOP payments was reliant on the health service utilization.22 The other reason might be most rural dwellers had only hand-to-mouth living standards due to a lack of modern farming systems. As a result, they are economically deteriorated and might have a low capacity to pay for healthcare services. Similarly, the differences in thresholds, socioeconomic status, study participants, period, area and design might also affect the variability of catastrophic OOP health expenditure. Additionally, the practice of early treatment was not practiced in the study area; they usually waiting until the illnesses become severe. This might also affect the OOPHE as a result of the difference in healthcare seeking behavior.
In this study, female-headed households were more likely to face CHE compared with male-headed households. This finding is consistent with studies conducted in China and India.31,36,37 The reason might be due to better educational status, and male household heads’ jobs might enhance households’ capacity to cope with the healthcare costs and reduce households from CHE. On the contrary, this finding is contradicted with the results in India, Egypt, and Korea.12,31,38 The possible reasons might be that most female-headed households might not give too many births than male-headed households. As a result, the household members’ small size might incur less catastrophic OOPHE than larger household members.
Households who had productive adult household members were less likely to encounter catastrophic OOPHE compared with their counterparts. This finding is supported by studies done in Colombian and Kenyan slum communities.14,32 The possible justification might be that households with productive adults were economically better than households with no working adults. As a result, they can afford the cost of any medical expenditure. Furthermore, wealthier households emanated from working adults’ contribution, and they could pay for any medical expenses. Another major factor for catastrophic expenditure was the presence of vulnerable individuals in the household.
The study also indicated that households having a household member with any chronic illnesses were more likely to face CHE. This result is supported by the findings of studies done in Egypt, Tanzania, Cambodia, China, Korea, Iran, and India.12,29,31,35–38 The possible justification might be longer duration, and high treatment frequency might associate with higher medical costs and continuous medical care costs. As a result, this might drive to high healthcare service expenditure. This study’s potential limitation might be the presence of recall bias during the estimation of food and health expenditures by their requested items. Furthermore, seasonal variation of illnesses might cause high variability in CHE. The cross-sectional survey may also over or underestimate health expenditure.
Conclusion
This study revealed that the proportion of households facing catastrophic OOPHE was high. Variables, such as the sex of the household head, working adults, and having members with any chronic illnesses in the households, affected catastrophic OOPHE. Prevention of chronic diseases and introducing financial risk protection mechanisms, such as community-based health insurance, can help bring equity in healthcare services.
Abbreviations
AOR, adjusted odds ratio; BGRS, Benishangul Gumuz Regional State; CHE, Catastrophic Health Expenditure; CBHI, community-based health insurance; COR, crude odds ratio; OOP, out-of-pocket; OOPHE, out-of-pocket health expenditure; WHO, World Health Organization.
Data Sharing Statement
The datasets supporting the conclusions of this article are available upon request to the corresponding author. Data were not publicly available to protect participant confidentiality.
Ethical Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki. We obtained Ethical clearance from the Institute of Public Health Ethical Review Committee, University of Gondar. Similarly, we received an official permission letter from the Metekel Zonal Health Department and the Mandura District Health Office. After giving the data collectors training about how to maintain ethical aspects of the research process, we started the data collection procedures. During data collection, we briefly described the purpose of the research and the procedures to each respondent. After reading the information sheet and consent form for each participant before getting consent, we obtained written consent from each participant. Besides, we recruited data collectors from the same community to respect society’s social and cultural context.
Acknowledgments
We are very thankful to Benishangul-Gumuz Regional Health Bureau and Metekel Zonal Health Department for supporting this study financially, and the University of Gondar providing the ethical approval and facilitating to conduct this research project. We are also grateful to all data collectors and supervisors for their participation in the data collection process. As of last, we want to acknowledge the study households of Mandura district for their cooperation.
Authors’ Information
DS is a Health Economics professional at Benishangul-Gumuz Regional State Health Bureau, Assossa, Ethiopia.
MY is an Associate Professor of Health Management and Health Economics in the Department of Health Systems and Policy at the Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia.
AK is a Lecturer of Health Service Management in the Department of Health Systems and Policy at the Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia.
AD is an Assistant Professor of Health Service Management in the Department of Health Systems and Policy at the Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This manuscript is part of a master thesis funded by Benishangul Gumuz Regional Health Bureau and Metekel Zonal Health Department. We presented the preliminary findings of the study at the Institute of Public Health, University of Gondar. The funders had no role in the study design, data collection, analysis, decision to publish, or manuscript preparation.
Disclosure
The authors have declared that they have no conflicts of interest for this work.
References
1. Xu K. Distribution of health payments and catastrophic expenditures. Methodology. 2005.
2. Xu K, Evans D, Carrin G, Aguilar-Rivera AM. Designing health financing systems to reduce catastrophic health expenditure. 2005.
3. World Bank Group. Catastrophic payment for health care-World bank group.203-312. Available from: http://siteresources.worldbank.org/INTPAH/Resources/Publications/459843-1195594469249/HealthEquityCh18.pdf.
4. Alshreef A. Provider payment mechanisms: effective policy tools for achieving universal and sustainable healthcare coverage. 2019.
5. Wagstaff A, Doorslaer E. Catastrophe and impoverishment in paying for health care: with applications to Vietnam 1993–1998. Health Econ. 2003;12(11):921–933. doi:10.1002/hec.776
6. Cylus J, Thomson S, Evetovits T. Catastrophic health spending in Europe: equity and policy implications of different calculation methods. Bull World Health Organ. 2018;96(9):599. doi:10.2471/BLT.18.209031
7. Wagstaff A, Flores G, Hsu J, et al. Progress on catastrophic health spending in 133 countries: a retrospective observational study. Lancet Global Health. 2018;6(2):e169–e79. doi:10.1016/S2214-109X(17)30429-1
8. Wagstaff A, Flores G, Smitz M-F, Hsu J, Chepynoga K, Eozenou P. Progress on impoverishing health spending in 122 countries: a retrospective observational study. Lancet Global Health. 2018;6(2):e180–e92. doi:10.1016/S2214-109X(17)30486-2
9. Alam K, Mahal A. Economic impacts of health shocks on households in low and middle income countries: a review of the literature. Global Health. 2014;10(1):21. doi:10.1186/1744-8603-10-21
10. Rashad A, Sharaf M. Catastrophic economic consequences of healthcare payments: effects on poverty estimates in Egypt, Jordan, and Palestine. Economies. 2015;3(4):216–234. doi:10.3390/economies3040216
11. Dorjdagva J, Batbaatar E, Svensson M, Dorjsuren B, Kauhanen J. Catastrophic health expenditure and impoverishment in Mongolia. Int J Equity Health. 2016;15(1):105. doi:10.1186/s12939-016-0395-8
12. Rashad AS, Sharaf MF. Catastrophic and impoverishing effects of out-of-pocket health expenditure: new evidence from Egypt. Am J Econ. 2015;5(5):526–533.
13. Xu K, Evans DB, Kawabata K, Zeramdini R, Klavus J, Murray CJ. Household catastrophic health expenditure: a multicountry analysis. The Lancet. 2003;362(9378):111–117. doi:10.1016/S0140-6736(03)13861-5
14. Amaya-Lara JL. Catastrophic expenditure due to out-of-pocket health payments and its determinants in Colombian households. Int J Equity Health. 2016;15(1):182. doi:10.1186/s12939-016-0472-z
15. Piroozi B, Mohamadi-Bolbanabad A, Moradi G, et al. Incidence and intensity of catastrophic health-care expenditure for Type 2 diabetes mellitus care in iran: determinants and inequality. Diabetes Metabol Syndr Obesity. 2020;13:2865. doi:10.2147/DMSO.S263571
16. Rezaei S, Hajizadeh M. Measuring and decomposing socioeconomic inequality in catastrophic healthcare expenditures in Iran. J Prev Med Public Health. 2019;52(4):214. doi:10.3961/jpmph.19.046
17. Piroozi B, Zarei B, Ghaderi B, et al. Catastrophic health expenditure and its determinants in households with gastrointestinal cancer patients: evidence from new health system reform in Iran. Int J Human Rights Healthcare. 2019;12(4):249–257. doi:10.1108/IJHRH-01-2019-0008
18. Rezaei S, Hajizadeh M, Ahmadi S, et al. Socioeconomic inequality in catastrophic healthcare expenditures in Western Iran. Int J Soc Econ. 2019;46(9):1049–1060. doi:10.1108/IJSE-01-2019-0034
19. Fang K, Jiang Y, Shia B, Ma S. Impact of illness and medical expenditure on household consumptions: a survey in western China. PLoS One. 2012;7(12):e52928. doi:10.1371/journal.pone.0052928
20. Kumar K, Singh A, Kumar S, et al. Socio-economic differentials in impoverishment effects of out-of-pocket health expenditure in China and India: evidence from WHO SAGE. PLoS One. 2015;10(8):e0135051. doi:10.1371/journal.pone.0135051
21. Lee J-E, Shin H-I, Do YK, Yang EJ. Catastrophic health expenditures for households with disabled members: evidence from the Korean health panel. J Korean Med Sci. 2016;31(3):336–344. doi:10.3346/jkms.2016.31.3.336
22. Dibaba A, Ababor S, Assefa Y. Improving Health Care Financing in Ethiopia (SURE Policy Brief). Addis Ababa: Ethiopian Public Health Institute; 2014.
23. Ethiopian Federal Democratic Republic Ministry of Health. Household Health Service Utilization and Expenditure Survey. 2011.
24. Binnendijk HH. Designing Community-Based Health Insurance among Rural Poor in India: A novel time-and cost-effective method for data sourcing. 2014.
25. Agency EHI. Evaluation of Community‐based Health Insurance Pilot Schemes in Ethiopia. Ethiopian Health Insurance Agency Addis Ababa (Ethiopia); 2015.
26. Cripps G, Edmond J, Killian R. Guide to Designing and Managing Community-Based Health Financing Schemes in East and Southern Africa. Abt Associations, Partnerships for Health Reform; 2000.
27. Kimani D, Maina T. Catastrophic Health Expenditures and Impoverishment in Kenya. Washington, DC: Futures Group. Health Policy Project; 2015.
28. Saito E, Gilmour S, Rahman MM, Gautam GS, Shrestha PK, Shibuya K. Catastrophic household expenditure on health in Nepal: a cross-sectional survey. Bull World Health Organ. 2014;92:760–767. doi:10.2471/BLT.13.126615
29. Brinda EM, Andrés RA, Enemark U. Correlates of out-of-pocket and catastrophic health expenditures in Tanzania: results from a national household survey. BMC Int Health Hum Rights. 2014;14(1):5. doi:10.1186/1472-698X-14-5
30. Daneshkohan A, Karami M, Najafi F, Matin BK. Household catastrophic health expenditure. Iran J Public Health. 2011;40(1):94.
31. Mondal S, Kanjilal B, Peters DH, Lucas H. Catastrophic out-of-pocket payment for health care and its impact on households: experience from West Bengal, India. Fut Health Systems Innovations Equity. 2010.
32. Buigut S, Ettarh R, Amendah DD. Catastrophic health expenditure and its determinants in Kenya slum communities. Int J Equity Health. 2015;14(1):46. doi:10.1186/s12939-015-0168-9
33. Li X, Shen JJ, Lu J, et al. Household catastrophic medical expenses in eastern China: determinants and policy implications. BMC Health Serv Res. 2013;13(1):506. doi:10.1186/1472-6963-13-506
34. Rezaei S, Woldemichael A, Hajizadeh M, Karyani AK. Catastrophic healthcare expenditures among Iranian households: a systematic review and meta-analysis. Int J Human Rights Healthcare. 2019;12(2):105–115. doi:10.1108/IJHRH-02-2018-0017
35. Kavosi Z, Keshtkaran A, Hayati R, Ravangard R, Khammarnia M. Household financial contribution to the health System in Shiraz, Iran in 2012. Int j Health Policy Manage. 2014;3(5):243. doi:10.15171/ijhpm.2014.87
36. Li Y, Wu Q, Xu L, et al. Factors affecting catastrophic health expenditure and impoverishment from medical expenses in China: policy implications of universal health insurance. Bull World Health Organ. 2012;90:664–671. doi:10.2471/BLT.12.102178
37. Li Y, Wu Q, Liu C, et al. Catastrophic health expenditure and rural household impoverishment in China: what role does the new cooperative health insurance scheme play? PLoS One. 2014;9(4):e93253. doi:10.1371/journal.pone.0093253
38. Choi J-W, Choi J-W, Kim J-H, Yoo K-B, Park E-C. Association between chronic disease and catastrophic health expenditure in Korea. BMC Health Serv Res. 2015;15(1):26. doi:10.1186/s12913-014-0675-1
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.