")
Back to Journals » International Journal of Women's Health » Volume 15
Case Series of Diabetic Ketoacidosis in Late Pregnancy with Normal Glucose Tolerance
Authors Xu J, Liu C , Zhao W, Lou W
Received 31 July 2023
Accepted for publication 22 November 2023
Published 27 November 2023 Volume 2023:15 Pages 1857—1864
DOI https://doi.org/10.2147/IJWH.S429557
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
Jiwen Xu,1,* Chang Liu,1,2,* Weixiu Zhao,1 Weihua Lou1
1Department of Obstetrics and Gynecology, Renji Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, People’s Republic of China; 2Center for Reproductive Medicine, Renji Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Weixiu Zhao; Weihua Lou, Department of Obstetrics and Gynecology, Renji Hospital, School of Medicine, Shanghai Jiao Tong University, No. 160 Pujian Road, Shanghai, 200127, People’s Republic of China, Email [email protected]; [email protected]
Abstract: Diabetic ketoacidosis (DKA) is rare in pregnancy, especially in pregnant women with normal glucose tolerance examined in early pregnancy. Once DKA occurs in pregnancy, the disease progresses rapidly and can be life-threatening for both mother and fetus. We concluded three cases of DKA in late pregnancy. The clinical manifestations, progression, and prognosis of the three cases are different, but all of the cases have normal glucose tolerance. We summarized the characteristics of pregnant women with DKA and analyzed and discussed them in conjunction with literature for reference by clinical doctors.
Keywords: diabetic ketoacidosis, pregnancy, gestational diabetes mellitus
Introduction
Diabetic ketoacidosis (DKA) is a well-known clinical disease that can potentially be life-threatening. As a severe complication of diabetes mellitus (DM), its main manifestations are high blood sugar, metabolic acidosis with an elevated anion gap, and an increased serum concentration of ketone bodies.1 The precipitating factors of DKA includes infections, ischemia, drugs, and other medical and surgical conditions.1,2
DKA is a rare clinical emergency. Delayed diagnosis and treatment may result in adverse pregnancy outcomes, such as maternal and fetal mortality.3–6 DKA mostly occurred in pregnant women with type 1 diabetes mellitus (T1DM). A retrospective study performed by Martin found that 20 out of 560 type 1 diabetes patients had DKA during pregnancy, while none occurred in 3500 type 2 diabetes patients.7 It is rare in those with gestational diabetes mellitus (GDM) and occasionally seen in type 2 diabetes mellitus (T2DM),3 while it is extremely seldom seen in pregnant women with normal glucose tolerance.8 Hence, in the present paper, we shared the clinical data of 3 patients (general characteristics of the patients were generated in Table 1) with normal glucose tolerance in the second trimester who developed DKA in late pregnancy, to improve the understanding of this disease among physicians with attention in the diagnosis and treatment of such complications to avoid misdiagnosis.
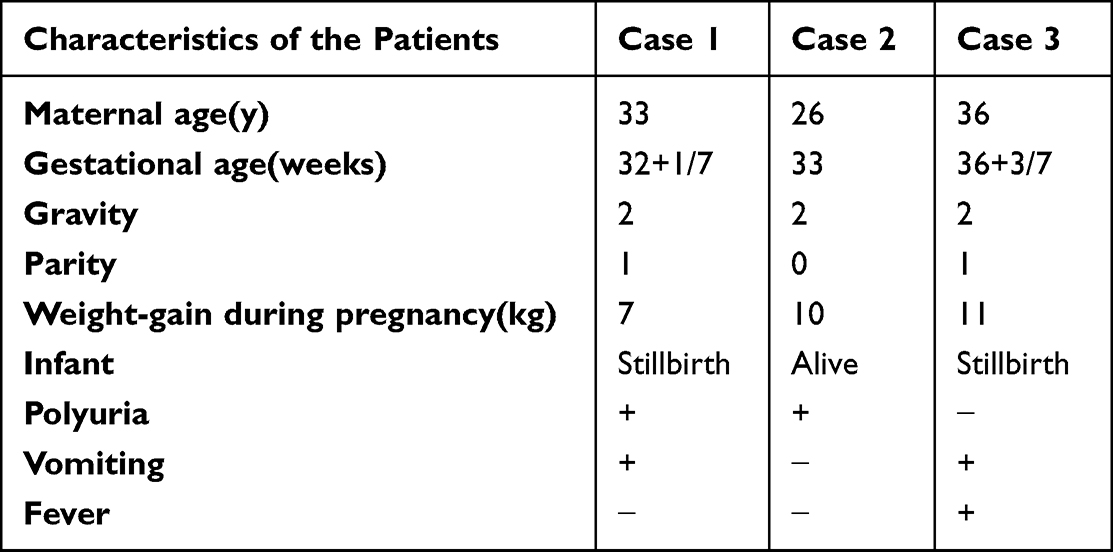 |
Table 1 Characteristics of the Patients |
Case Presentation
Case 1
The patient was a 33-year-old Chinese woman (G2P1) with 150cm in height and 62kg in weight (BMI 27.6). Her past medical, obstetrical histories and family history were unremarkable. Her first pregnancy and delivery were uneventful. During pregnancy, she had normal glucose tolerance at 24 weeks of gestation. At 32 weeks 1 day she presented at her local hospital. She complained of polyuria, dizziness, chest tightness, blurred vision and decreased fetal movement but without nausea, vomiting, abdominal pain, or diarrhea after eating porridge and cola. Initial laboratory investigations demonstrated severe glucosuria (4+) and ketonuria (4+), severe metabolic acidosis (pH 7.03) and extremely high plasma glucose (31.5 mmol/L). Based on her clinical features and laboratory data, she was diagnosed with DKA and treated with intravenous insulin and fluids. Then, she was transferred to our hospital, and a color Doppler Ultrasonography showed no fetal heartbeat at the initial visit, suggesting intrauterine stillbirth. B-ultrasound did not detect any signs of uterine rupture, and the placenta was located on the posterior wall of the uterus with no evidence of retroplacental hemorrhage.
On admission, physical examination revealed that the patient was alert and orientated. Her vital signs were as follows: body temperature 36.3°C, pulse 104 beats/min, respiratory rate 26 breaths/min and blood pressure 141/88 mmHg. Her abdomen was not tender, and there were no localized signs of infection. Laboratory data revealed severe hemoconcentration with hemoglobin 158g/L and hematocrit 47.9%. Plasma glucose level and was extremely high (20.8 mmol/L) and serum ketone was 2+. A derangement of serum electrolytes was noted: sodium and potassium were 133 mmol/L and 6.2 mmol/L, respectively. Urine analysis demonstrated ketonuria (3+) and glucosuria (4+). Arterial blood gas analysis demonstrated severe metabolic acidosis (pH 7.01). Additionally, insulin islet antibody (ICA), insulin autoantibody (IAA) and anti-glutamic acid decarboxylase (GAD) antibody were negative. A decreased serum C-peptide of 0.88 ng/mL, slightly elevated HbA1c of 5.7% and Glycated albumin of 16.9% were present. Trans-abdominal ultrasonography was normal.
After admission, she was given oxygen, intravenous insulin, sodium bicarbonate, and a large amount of fluid replacement therapy. Arterial pH returned to 7.33 and metabolic acidosis improved 9 hours after the treatment was started. The plasma glucose level was gradually lowered to 9.8 mol/L in 9 hours. Ketonuria disappeared after 21 hours. Her general condition was poor, and the patient herself refused to undergo a vaginal trial. Clearly inform the patient of fetal death in the uterus, she still refused vaginal delivery and request a cesarean section. After recovery from ketoacidosis and hyperglycemia, she was given induced labor with caesarean section and gave birth to a stillborn infant weighing 2000 g without any malformations. The placenta and umbilical cord appeared normal. After delivery, she was commenced on 60U/day subcutaneous administration of insulin. She was discharged after 16 days of treatment with the final diagnose as diabetic ketoacidosis.
Case 2
A 26-year-old Chinese woman (G2P0 with one biochemical pregnancy, 162cm in height and 66kg in weight, BMI 25.1) in her 32 weeks 6 days of gestation presented at her local hospital complaining of thirst, polydipsia, polyuria, dizziness, bodyweight loss (2kg) and gasp but without nausea, vomiting, abdominal pain, or diarrhea. She had no family history of diabetes mellitus. At 25 weeks of gestation, her glucose tolerance was normal. After initial laboratory investigations, severe glucosuria (4+), ketonuria (3+) and extremely high plasma glucose level (28 mmol/L) were found. Fetal cardiotocography was abnormal at presentation. And then she was diagnosed with DKA followed by transferring to our hospital.
On admission, the patient was alert and orientated. Her vital signs were still stable (body temperature 37°C, pulse 85 beats/min, respiratory rate 19 breaths/min and blood pressure 112/70 mmHg). Her plasma glucose level was extremely high (27 mmol/L). Severe metabolic acidosis (pH 7.125) and abnormal fetal cardiotocography (Figure 1) were found. There was a derangement of serum electrolytes with sodium at 130 mmol/L and potassium 4.9 mmol/L. Urine analysis demonstrated ketonuria (3+) and glucosuria (4+). Additionally, insulin islet antibody (ICA) and insulin autoantibody (IAA) were negative. A decreased serum C-peptide of 0.71 ng/mL, slightly elevated HbA1c of 6.1% and glycated albumin of 19.1% were present.
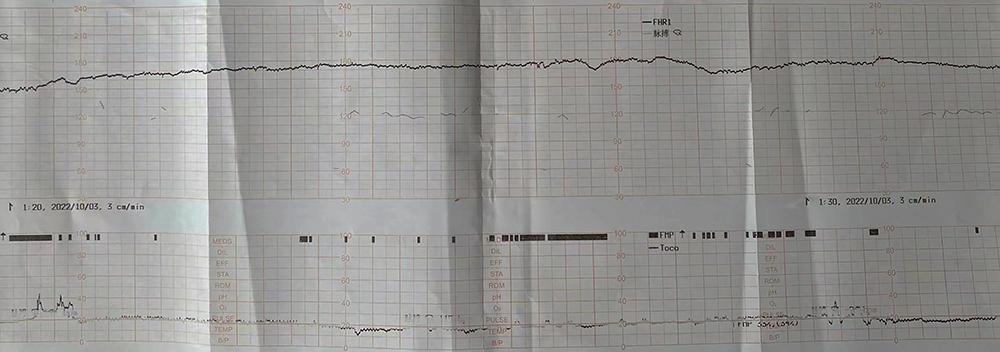 |
Figure 1 Fetal Cardiotocography of Case 2. |
Oxygen, intravenous insulin, sodium bicarbonate and a large amount of fluid replacement therapy were given. And an emergency Caesarean section was undertaken for fetal distress. The female neonate weighing 1885 g, had low Apgar scores (5 points at 1min, 8 points at 5 min, and 10 points at 10 min), with atresia of anal. The placenta and umbilical cord appeared normal. Arterial blood gas revealed pH 7.352 8 h after the treatment was started. The plasma glucose level was gradually reduced to 11.7mol/L in 4 h. Ketonuria disappeared in 13 h. After delivery, she was commenced on 38U/day subcutaneous administration of insulin. She was discharged 16 days postpartum. The patient was finally diagnosed diabetic ketoacidosis.
Case 3
The 36-year-old Chinese woman (G2P1) complained of sudden headache and vomiting at 36 weeks 3 days of gestation. She denied family history of diabetes before this pregnancy. She had no complicated diseases during the first pregnancy and end as vaginal delivery. The 75g oral glucose tolerance test at 25 weeks of the gestation was normal. The pregnancy was uneventful until she developed sudden headache and vomiting at 36 weeks 3 days of gestation. However, she did not present with pharyngitis, diarrhea, maculopapular non-pruritic rash, nausea, or flu-like symptoms such as a sore throat, cough, or rhinorrhea.
On admission, the patient was alert and orientated with normal vital signs: body temperature 37.6°C, pulse 80 beats/min, respiratory rate 20 breaths/min and blood pressure 133/70 mmHg. She was 158cm tall, weighting 67kg (BMI 26.8). Fetal heart rate deceleration was observed in a normal range but the fetal cardiotocography was abnormal (Figure 2), for which an emergency caesarean section was undertaken. A stillborn female infant without any malformations was given birth, weighing 2800 g. The placenta appeared normal. The umbilical cord was knotted. The laboratory findings revealed diabetic ketoacidosis (DKA), with a random sample glucose of 22.1 mol/l, severe metabolic acidosis (pH 7.01), serum ketone of 3.1 mmol/L. A derangement of serum electrolytes was noted: sodium, potassium and chloride were 136 mmol/L, 6.2 mmol/L and 115 mmol/L, respectively. Additionally, insulin islet antibody (ICA), insulin autoantibody (IAA) and anti-glutamic acid decarboxylase (GAD) antibody were negative. A normal serum C-peptide of 0.87 ng/mL, slightly elevated HbA1c of 6.3% and Glycated albumin of 17.58% were present. The serum pancreatic enzymes slightly elevated (179 U/L), serum lipase was elevated (736 U/L) and serum calcium level were normal. CT scan was performed to rule out acute pancreatitis and no significant finding was noted. Continuous insulin therapy and fluid infusion with normal saline were commenced. Arterial pH was 7.45 in 7 h. The plasma glucose level gradually decreased to 12.7mol/L in 8 h. And ketonuria disappeared in 30 h. After DKA resolution treatment with subcutaneous administration of insulin was begun. However, following 31U/day subcutaneous administration of insulin initially, the patient developed symptoms of hypoglycemia. Therefore, subcutaneous insulin was withdrawn and replaced with oral hypoglycemic agents. She was discharged after 9 days of treatment as diabetic ketoacidosis.
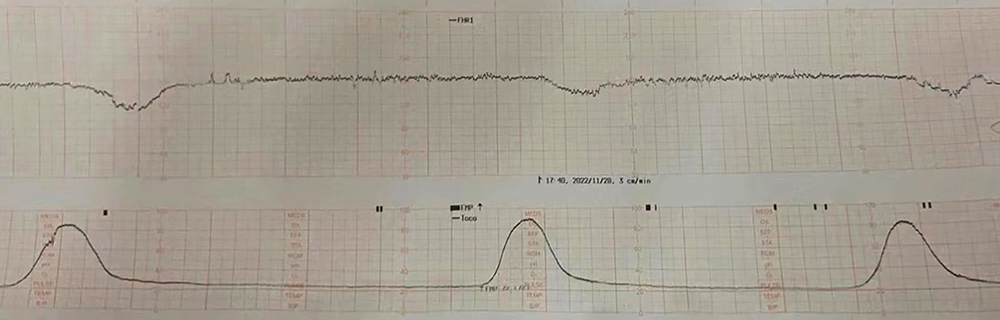 |
Figure 2 Fetal Cardiotocography of Case 3. |
Discussion
Diabetic ketoacidosis (DKA) is the most common acute emergency in diabetes mellitus patients, presenting as hyperglycemia, ketonemia and metabolic acidosis.9,10 Ketones are produced by free fatty acids in the liver. Ketosis is the result of reduced ketone consumption, and clinically, it can be demonstrated by an increase in the blood concentration of ketones (beta-hydroxybutyrate, acetoacetate, and acetone). When DKA occurs, there is a disruption in the balance between glucagon and insulin, typically due to an absolute or more commonly relative deficiency in circulating insulin levels in the presence of excess counterregulatory hormones (particularly catecholamines, glucagon, cortisol, and growth hormone), resulting in the release of free fatty acids from adipose tissue and excessive production of glucose and ketones in the liver.10
The definition of diabetic ketoacidosis includes the following criteria: 1) ketonemia >3.0 mmol/L or significant ketonuria (more than 2+ on standard urine strips); 2) blood glucose >11.0 mmol/L or known diabetes; 3) bicarbonate (HCO3-) <15.0 mmol/L and/or venous blood pH <7.3.2
The causes of diabetic ketoacidosis (DKA) include: 1) new diagnosis of type 1 diabetes mellitus (T1DM); 2) poor compliance with insulin therapy; 3) inadequate insulin treatment in the hospital; 4) infection, commonly in the chest, urinary tract, or skin; and 5) acute coronary artery/vascular events. In addition, there’s a well-known cause of pregnancy associated DKA: fulminant type 1 diabetes mellitus (FT1DM).11 The American Diabetes Association (ADA) and World Health Organization (WHO) classify type 1 diabetes into autoimmune type 1 diabetes (type 1A) and non-autoimmune type 1 diabetes (type 1B). FT1DM is defined as a new subtype of type 1B diabetes, characterized by rapid onset hyperglycemia and ketoacidosis due to rapid failure of pancreatic islet cells, typically preceded by prodromal symptoms (fever, flu-like symptoms, and gastrointestinal symptoms) lasting only a few days. The diagnostic criteria for FT1DM are based on the 2012 diagnostic standards proposed by the Japan Diabetes Society.12 FT1DM can be diagnosed if the following three conditions are met:
- The onset of diabetic ketosis or ketoacidosis occurs shortly after the appearance of hyperglycemic symptoms (with urine ketones and/or elevated serum ketones) (about 7 days).12,13
- Plasma glucose at the first diagnosis is ≥16.0 mmol/L (≥288 mg/dL), and glycated hemoglobin level is <8.7%.12,13
- At the onset of illness, urinary C-peptide is <10 μg/day or fasting serum C-peptide is <0.3 ng/mL (<0.10 nmol/L). After intravenous injection of glucagon (or meals), the serum C-peptide is <0.5 ng/mL (<0.17 nmol/L).12,13
If the patient meets both the second and third conditions described above, but the course of illness lasts more than one week, FT1DM should also be highly suspected. In addition, fulminant type 1 diabetes also has the following clinical features: 1) pancreatic-related autoantibodies are negative, such as glutamic acid decarboxylase antibody, islet antigen 2, and insulin antibody; 2) the duration of illness before starting insulin therapy may be 1–2 weeks; 3) 98% of patients have varying degrees of elevation in serum pancreatic enzymes (amylase), lipase, or elastase-1 levels before treatment; 4) 70% of patients have prodromal symptoms before onset, such as flu-like symptoms (fever, upper respiratory symptoms) or gastrointestinal symptoms (upper abdominal pain, nausea, and/or vomiting); 5) onset occurs shortly after pregnancy or delivery; 6) it is associated with a specific type of HLA (HLA DRB104:05-DQB104:01).12,13
Our patients are all pregnant women in the late stages of pregnancy with very high plasma glucose levels (average >16 mmol/L), but only a slight increase in glycated hemoglobin (average <8.7%), indicating that the onset of diabetes was sudden with a short course. Additionally, all three patients had negative islet-associated autoantibodies, suggesting the possibility of FT1DM. However, their serum C-peptide levels were all >0.3ng/mL, excluding the possibility of acute onset of type 1 diabetes. When admitted to the hospital, all three patients had elevated infection test indicators (Table 2). We considered the possibility of infection being a contributing factor to the development of DKA, and besides the confirmed pulmonary infection in case 2, no other specific site of infection was found in the other two patients.
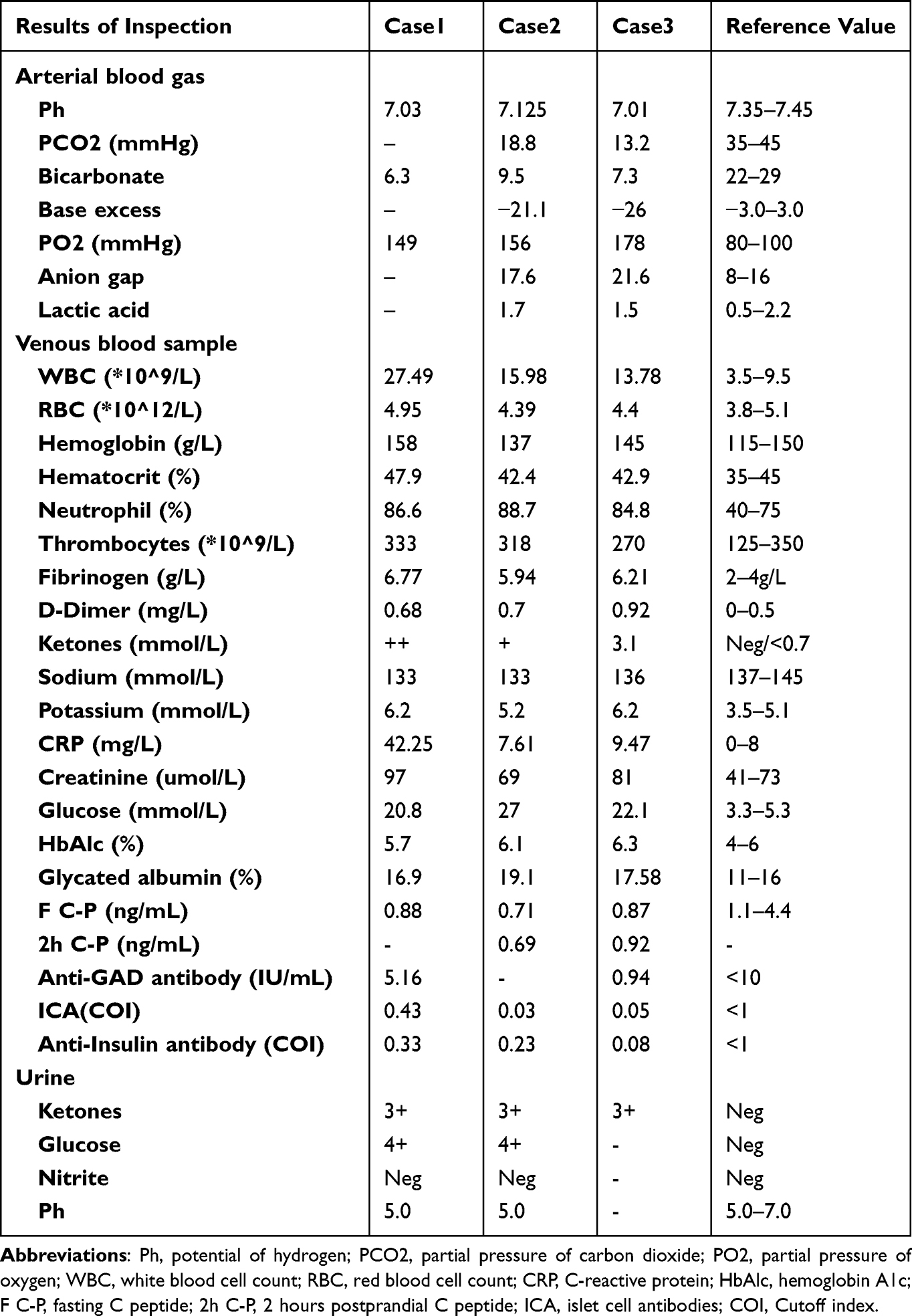 |
Table 2 Patients’ Laboratory Results at Admission |
It is rare for women with normal blood sugar levels in early and mid-pregnancy to develop type 1 diabetes in late pregnancy.8 Our patients all had normal glucose tolerance in mid-pregnancy but developed DKA in late pregnancy. It is well known that pregnancy promotes insulin resistance. As pregnancy progresses, normal counter-regulatory hormones (such as human placental lactogen) synthesized and released into the circulation from the syncytiotrophoblast layer decrease maternal sensitivity to insulin and increase postprandial blood sugar levels.14,15 Progesterone can slow gastrointestinal motility and increase glucose intake.14,15 In addition, hormonal changes that occur during pregnancy (such as increased secretion of estrogen, progesterone, human placental lactogen, and TNF-α) lead to decreased insulin sensitivity, especially in late pregnancy.16 All these mechanisms can induce gestational hyperglycemia.15,17–20 On the other hand, the placenta and fetus absorb a large amount of glucose, which decreases blood glucose levels during fasting. At the same time, insulin resistance accelerates fat breakdown, leading to increased levels of free fatty acids in the mother’s body and the production of ketones, which can trigger DKA.16,18,21 Insulin sensitivity can decrease up to 56% during the 36th week of pregnancy. In addition, changes in inflammation in adipose tissue are also associated with insulin resistance in late pregnancy.21 Early identification and treatment of DKA are crucial for preventing adverse pregnancy outcomes. However, predicting the occurrence of this disease is a challenge because these pregnant women often have no family history or personal history of poor glucose tolerance. Therefore, late-pregnancy DKA requires more detailed examination and differential diagnosis. When a healthy pregnant woman suddenly experiences dry mouth, thirst, polyuria, vomiting, inability to eat or drink (excluding illness), and is accompanied by flu-like or acute gastroenteritis-like symptoms, if blood sugar remains >250 mg/dL after appropriate measures are taken, urinary or blood ketones should be measured to determine whether DKA has occurred, in order to timely treat and reduce the risk to pregnant women and newborns.
The treatment of DKA includes aggressive fluid resuscitation, insulin infusion, and close electrolyte monitoring. However, common complications during DKA treatment include hypoglycemia due to insulin excess and hypokalemia due to insulin administration. Therefore, potassium supplementation through intravenous infusion must be provided during DKA treatment, while carefully monitoring electrolyte levels. If the serum potassium level is <3.3 mmol/L, potassium replacement therapy should be initiated immediately before starting insulin therapy once the serum potassium concentration is restored to >3.3 mmol/L to prevent arrhythmias, cardiac arrest, and respiratory muscle weakness. Our patients were immediately given sufficient fluid resuscitation, dietary control, insulin infusion, and close electrolyte monitoring after the diagnosis of DKA was confirmed. At the end of active treatment, the target blood glucose levels were achieved. The timing and method of terminating pregnancy are flexible. In our case 1, the patient requested strongly for a cesarean section, despite the fetal death. In Case 2, owing to fetal distress, a cesarean section was performed immediately, and a live delivery was obtained. In case 3, a cesarean section was performed since fetal distress, and although the fetus still had a heartbeat before the surgery, the dead baby was delivered during the operation. The conflict situation is that the maternal blood glucose level needs to be controlled as soon as possible. Surgery is not ideal when DKA is not controlled, but blood glucose is often difficult to control in a short period of time. Not performing a cesarean section in time may lead to prolonged hypoxia in the fetus, and early surgery may save the fetus. In order to achieve the balance in which, individualized evaluations for each patient must be conducted.
Some studies have shown that DKA during pregnancy is associated with a variety of fetal complications, both in the short and long term. Short-term complications include decreased uterine perfusion, fetal hypoxia, frequent late decelerations, and even fetal mortality (stillbirth and perinatal death, up to 9–60%).14,16,18,22 Our patient presented with frequent late decelerations at the time of admission, reflecting the severity and duration of acidosis. During DKA, maternal acidosis, hyperglycemia, severe hypovolemia, and severe electrolyte imbalances can cause decreased uteroplacental perfusion, and ketones and glucose can pass through the placental barrier into the fetal body, causing fetal hyperglycemia and osmotic diuresis and fetal hypovolemia, leading to fetal acidosis.14,22 Due to the decrease in 2,3-DPG, the affinity of hemoglobin for oxygen increases, resulting in a decrease in the amount of oxygen available to the fetus, leading to fetal hypoxia. This series of pathophysiological changes promotes the occurrence of fetal hypokalemia, arrhythmias, and cardiac arrest, ultimately leading to fetal loss.23 Therefore, severe DKA patients, especially comatose pregnant women, are at high risk of IUFD. Although no studies have shown the long-term consequences of live-born infants, changes in neurodevelopment have been observed. After DKA occurs during pregnancy, the risk of fetal death decreases over time but is still significantly higher than the baseline risk in women with type 1 diabetes. Emergency delivery during DKA is harmful to the fetus compared to other pregnancy complications. It is recommended to stabilize the mother’s condition first, including correcting hypovolemia, insulin infusion, monitoring and correcting electrolyte imbalances, identifying and treating triggering factors, and continuous fetal monitoring. Once maternal acidosis is corrected, the fetal condition will improve, and pregnancy can continue. Emergency cesarean section should only be attempted if the mother’s condition continues to deteriorate.2,17,21,24
Conclusion
As a complication of diabetes, diabetic ketoacidosis (DKA) is extremely rare, but it is an endocrine emergency that threatens the lives of patients. Pregnant women are at higher risk of developing DKA than non-pregnant women with diabetes. Pregnant women with normal glucose tolerance are also at risk of developing ketoacidosis during subsequent pregnancy. The occurrence of DKA during pregnancy and its treatment pose risks to the fetus, and early recognition and prompt initiation of appropriate drug therapy and appropriate obstetric care, combined with promptly terminate pregnancy once remission of DKA, are key to reducing maternal mortality and fetal loss.
Data Sharing Statement
The dataset used during the present study is available from the corresponding author (Weihua Lou, email: [email protected]) upon a reasonable request.
Ethics Approval and Consent to Participate
The study was approved by the Ethics Committee of Ren Ji Hospital, Shanghai Jiao Tong University School of Medicine. Written informed consent to participate was obtained from the patients.
Consent for Publication
Written informed consent has been obtained from the patients for publication of this paper and accompanying images.
Acknowledgments
All the authors would like to thank the patient who agreed to the case presentation. The authors are grateful to all the members in the department.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no conflicting interests in this work.
References
1. Modi A, Agrawal A, Morgan F. Euglycemic diabetic ketoacidosis: a review. Curr Diab Rep. 2017;13(3):315–321. doi:10.2174/1573399812666160421121307
2. Diguisto C, Strachan MWJ, Churchill D, Ayman G, Knight M. A study of diabetic ketoacidosis in the pregnant population in the United Kingdom: investigating the incidence, aetiology, management and outcomes. Diabet Med. 2022;39(4):e14743. doi:10.1111/dme.14743
3. Kitabchi AE, Umpierrez GE, Miles JM, Fisher JN. Hyperglycemic crises in adult patients with diabetes. Diabetes Care. 2009;32(7):1335–1343. doi:10.2337/dc09-9032
4. Dargel S, Schleußner E, Kloos C, Groten T, Weschenfelder F. Awareness of euglycaemic diabetic ketoacidosis during pregnancy prevents recurrence of devastating outcomes: a case report of two pregnancies in one patient. BMC Pregnancy Childbirth. 2021;21(1):552. doi:10.1186/s12884-021-04035-6
5. Parker JA, Conway DL. Diabetic ketoacidosis in pregnancy. Obstet Gynecol Clin North Am. 2007;34(3):533–43, xii. doi:10.1016/j.ogc.2007.08.001
6. Eshkoli T, Barski L, Faingelernt Y, Jotkowitz A, Finkel-Oron A, Schwarzfuchs D. Diabetic ketoacidosis in pregnancy - Case series, pathophysiology, and review of the literature. Eur J Obstet Gynecol Reprod Biol. 2022;269:41–46. doi:10.1016/j.ejogrb.2021.12.011
7. Montoro MN, Myers VP, Mestman JH, Xu Y, Anderson BG, Golde SH. Outcome of pregnancy in diabetic ketoacidosis. Am J Perinatol. 1993;10(1):17–20. doi:10.1055/s-2007-994692
8. Barski L, Eshkoli T, Brandstaetter E, Jotkowitz A. Euglycemic diabetic ketoacidosis. Eur J Intern Med. 2019;63:9–14. doi:10.1016/j.ejim.2019.03.014
9. Nyenwe EA, Kitabchi AE. The evolution of diabetic ketoacidosis: an update of its etiology, pathogenesis and management. Metabolism. 2016;65(4):507–521. doi:10.1016/j.metabol.2015.12.007
10. Dhatariya KK, Glaser NS, Codner E, Umpierrez GE. Diabetic ketoacidosis. Nature Reviews Disease Primers. 2020;6(1):40. doi:10.1038/s41572-020-0165-1
11. Shimizu I, Makino H, Osawa H, et al. Association of fulminant type 1 diabetes with pregnancy. Diabetes Res Clin Pract. 2003;62(1):33–38. doi:10.1016/s0168-8227(03)00147-5
12. Imagawa A, Hanafusa T, Uchigata Y, et al. Fulminant type 1 diabetes: a nationwide survey in Japan. Diabetes Care. 2003;26(8):2345–2352. doi:10.2337/diacare.26.8.2345
13. Imagawa A, Hanafusa T, Awata T, et al. Report of the Committee of the Japan Diabetes Society on the Research of fulminant and acute-onset type 1 diabetes mellitus: new diagnostic criteria of fulminant type 1 diabetes mellitus (2012). J Diabetes Investig. 2012;3(6):536–539. doi:10.1111/jdi.12024
14. de Veciana M. Diabetes ketoacidosis in pregnancy. Semin Perinatol. 2013;37(4):267–273. doi:10.1053/j.semperi.2013.04.005
15. Sibai BM, Viteri OA. Diabetic ketoacidosis in pregnancy. Obstet Gynecol. 2014;123(1):167–178. doi:10.1097/aog.0000000000000060
16. Jaber JF, Standley M, Reddy R. Euglycemic diabetic ketoacidosis in pregnancy: a case report and review of current literature. Case Rep Crit Care. 2019;2019:8769714. doi:10.1155/2019/8769714
17. Pinto ME, Villena JE. Diabetic ketoacidosis during gestational diabetes. A case report. Diabetes Res Clin Pract. 2011;93(2):e92–e94. doi:10.1016/j.diabres.2011.05.014
18. Kamalakannan D, Baskar V, Barton DM, Abdu TA. Diabetic ketoacidosis in pregnancy. Postgrad Med J. 2003;79(934):454–457. doi:10.1136/pmj.79.934.454
19. Gayle K, Suarez T, Tan G. A . Endocr Pract. 2019;24. doi:10.1016/S1530-891X(20)47069-7
20. Smati S, Mahot P, Bourdiol A, Ploteau S, Hadjadj S, Cariou B. Euglycaemic ketoacidosis during gestational diabetes with concomitant COVID-19 infection. Diabetes Metab. 2021;47(2):101181. doi:10.1016/j.diabet.2020.07.008
21. Dalfrà MG, Burlina S, Sartore G, Lapolla A. Ketoacidosis in diabetic pregnancy. J Matern Fetal Neonatal Med. 2016;29(17):2889–2895. doi:10.3109/14767058.2015.1107903
22. Chauhan SP, Perry KG, McLaughlin BN, Roberts WE, Sullivan CA, Morrison JC. Diabetic ketoacidosis complicating pregnancy. J Perinatol. 1996;16(3 Pt 1):173–175.
23. Himuro H, Sugiyama T, Nishigori H, et al. A case of a woman with late-pregnancy-onset DKA who had normal glucose tolerance in the first trimester. Endocrinol Diabetes Metab Case Rep. 2014;2014:130085. doi:10.1530/edm-13-0085
24. Schneider MB, Umpierrez GE, Ramsey RD, Mabie WC, Bennett KA. Pregnancy complicated by diabetic ketoacidosis: maternal and fetal outcomes. Diabetes Care. 2003;26(3):958–959. doi:10.2337/diacare.26.3.958
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.