")
Back to Journals » International Journal of General Medicine » Volume 13
Case Report: Sudden Splenic Rupture in a Plasmodium falciparum-Infected Patient
Authors Kassam N , Michael S, Hameed K, Ali A, Surani S
Received 11 June 2020
Accepted for publication 18 August 2020
Published 9 September 2020 Volume 2020:13 Pages 595—598
DOI https://doi.org/10.2147/IJGM.S267197
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Nadeem Kassam,1 Steven Michael,2 Kamran Hameed,1 Athar Ali,2 Salim Surani3
1Department of Internal Medicine, Aga Khan University Medical College East Africa, Dar-es-salaam, Tanzania; 2Department of General Surgery, Aga Khan University Medical College East Africa, Dar-es-salaam, Tanzania; 3Department of Internal Medicine, Texas A&M University, College Station, TX, USA
Correspondence: Nadeem Kassam Email [email protected]
Abstract: Spontaneous splenic rupture is a rare and life-threatening complication of severe malaria. It demands particular attention since delayed or missed diagnosis can be potentially fatal. The exact incidence is unknown largely due to underreporting. Acute malarial infection accounts for most of the spontaneous splenic rupture. Plasmodium vivax has been associated with the majority of them; however, on rare occasion, other Plasmodium infections have also resulted in splenic rupture. We report the case of a 74-year-old male who was diagnosed with severe malaria caused by Plasmodium falciparum (P. falciparum) infection and developed an acute abdomen while on treatment due to spontaneous splenic rupture which necessitated emergency splenectomy.
Keywords: spontaneous splenic rupture, Plasmodium falciparum
Introduction
Malaria is a critical endemic parasitic disease transmitted to humans by a bite from an infected female Anopheles mosquito.1 Different studies have shown that the prevalence of malaria has increased since 2015.2 In 2018, the World Health Organization (WHO) reported 228 million cases of malaria worldwide with 405 000 deaths, in which the Africa region was home to 93% of cases and 94% of malaria-related deaths.3 However according to the reporting by the National Ministry, the incidence of malaria in Tanzania has greatly reduced from 14% in 2016 to 7.3% in 2018.
The range of clinical presentation of malaria varies considerably from asymptomatic parasitemia to severe life-threatening disease.4 The function of the spleen against malaria is well-studied particularly in endemic regions and plays an important immunological role.5 Splenomegaly is a usual physical finding in malarial infection. Nevertheless, malarial splenic rupture (MSR) is a rare but lethal and dangerous complication of severe malarial infection with an estimated incidence of 2%.6,7 This case has been published to generate awareness of such a spontaneous complication which could be potentially fatal if not diagnosed early. We present the case of a 74-year-old man with splenic rupture due to Plasmodium falciparum (P. falciparum) infection.
Case Report
A 74-year-old gentleman, known to have hypertension and diabetes mellitus, presented to our emergency department with a 4-day history of intermittent subjective fever of no specific periodicity and rigors associated with generalized headache, altered mentation, body malaise, nausea, and vomiting. He reported no history of loss of consciousness, abdominal pain, or change in stool habits/urine color. The patient denied history of recent trauma or falls, and the rest of the systemic review was unremarkable. The patient resided in a malaria-endemic region and reported to have previous uncomplicated malarial infections that were successfully treated with oral anti-malarials.
On clinical examination, he was an elderly gentleman febrile (38.7 °C), tachypneic, and disoriented with good nutritional status. He was not jaundiced or cyanosed. Initial vitals were pulse rate of 103 beats/min in sinus rhythm, respiratory rate of 23 breaths/min, with slightly borderline low blood pressure of 96/60 mmHg and saturating at 98% on room air. On systemic examination he had normal vesicular breath sounds and a normal abdominal examination. While awaiting initial work up, in view of the findings the patient received intravenous (IV) resuscitation and analgesia.
The complete blood count (CBC) revealed a white blood cell count (WBC) of 8.2 × 103/μL, hemoglobin (Hb) of 11.5 g/dL, and thrombocytopenia of 46,000/mm3. The renal profile revealed elevated creatinine 117 μmol/L and BUN 10.5 mmol/L with slightly low sodium of 131 mmol/L. The rest of serum electrolytes, liver, and coagulation profile were normal. Chest X-ray was normal. Peripheral blood smear for malaria demonstrated P. falciparum with high parasitemia with more than 1000 trophozoites/200 WBC, HPF (high power field). He was subsequently admitted to the intensive care unit (ICU) as a case of severe malaria evident by high parasitemia and altered mentation.
He was then commenced on an intravenous artesunate-based regimen as per the national malaria treatment protocol with other supportive measures. With marked improvement in both clinical status and lab parameters, he was subsequently shifted to the general ward after 3 days of ICU stay. While in the ward (day 5 post admission), he acutely developed features of acute abdomen characterized by progressive, dull, constant generalized abdominal pain more so on the left upper quadrant associated with nausea and several episodes of non-bilious vomiting. The rest of the review was unremarkable.
On review, he was lying still in bed, anxious, afebrile, diaphoretic, tachycardic, tachypneic, and hypotensive but saturating well on room air. He had a slightly distended abdomen which was tender on superficial palpation with inaudible bowel sounds on auscultation. In view of the above, urgent CBC, grouping/crossmatch, formal abdominal ultrasound, and contrast-enhanced CT scan of the abdomen were performed. CBC revealed a low Hb of 7.1 g/dL (compared to 8.9 mg/dl the day prior). Ultrasound showed hypoechoic nodular cystic area (Figure 1A and B) and CT scan revealed hyperdense intrasplenic hematoma surrounded by hypodense subcapsular hematoma. Post-contrast CT images demonstrated splenic laceration on the superolateral aspect in addition to the hematoma as well as intraperitoneal free fluid. These findings were in line with grade 3 splenic injury (Figure 2A and B).
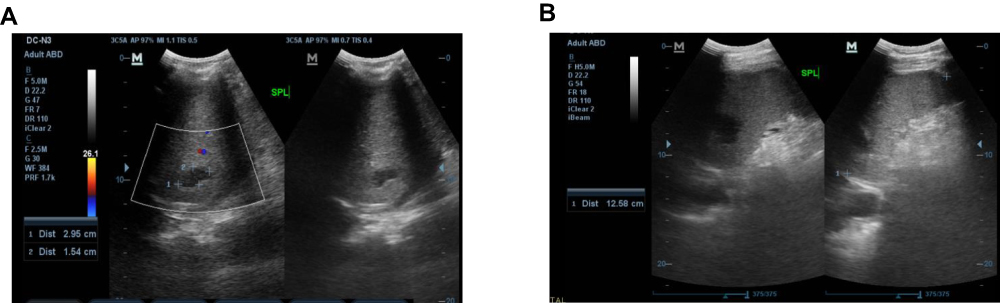 |
Figure 1 (A) Abdominal ultrasound showing hypoechoic nodular cystic area measuring 2.91 cm × 1.62 cm. (B) Indicating splenomegaly, spleen measured 12.58 cm. |
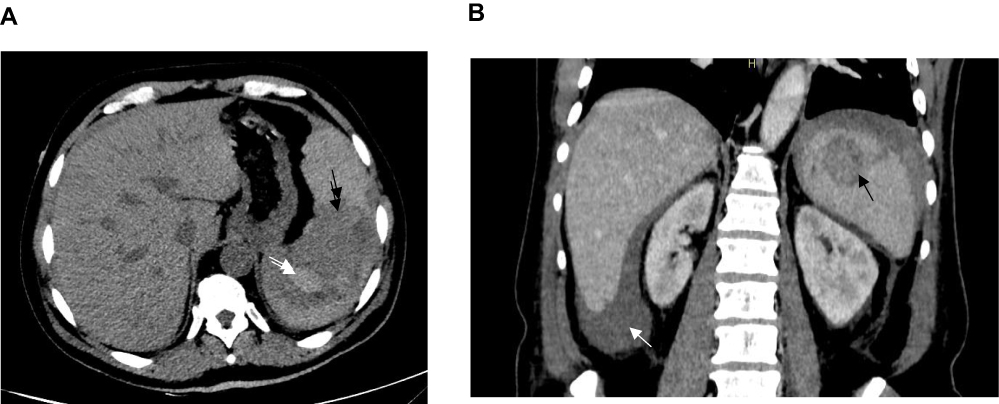 |
Figure 2 (A) Axial images obtained through the upper abdomen prior to contrast administration revealed hyperdense intrasplenic hematoma (white arrow) surrounded by hypodense subcapsular hematoma (black arrow). (B) Post-contrast images demonstrating splenic laceration on the superolateral aspect (marked by a black arrow) with intraperitoneal free fluid (white arrow). These findings were in line with grade 3 splenic injury. |
The findings of spontaneous splenic rupture were attributed to the consequence of severe malaria due to P. falciparum infection as there was no evidence of other documented etiologies such as trauma or other infectious causes. Blood products were mobilized, adequate resuscitation was done, and after thorough discussion with the patient and family the patient was taken to the operating theatre for explorative laparotomy and splenectomy.
Intra-operatively 2.5 L of frank blood without purulence was evacuated. The spleen was enlarged and very firm with a long laceration on the upper pole extending laterally involving the fine covering capsule and not much of the splenic parenchyma. Splenectomy was done. He had an uneventful postoperative period and 7 days later he was discharged home fully recovered with scheduled clinic visits for post-splenectomy care.
Discussion
Malaria can present with several complications. P. falciparum is however known as the most common cause of severe complications in malaria.8 The spleen plays an important immunological role in malaria infection, but it also encompass a range of pathological outcomes ranging from splenomegaly to hematoma formation, splenic infarctions, rupture, and infrequently abscess formation.9 According to a review conducted by Osman et al, 252 cases of MSR had been reported, whereby P. vivax and P. falciparum species were reported in the majority of cases.5–7
The mechanism of MSR is a poorly understood phenomenon. It is hypothesized that a combination of three primary factors are mainly implicated: 1) cellular hyperplasia; 2) vascular congestion; and 3) increase in intraabdominal pressure that exerts more stress on the tensed and friable spleen, eventually resulting in subcapsular haematoma formation and subsequently rupture.10 Triggers such as minor activities have been reported that can elicit a capsular tear that results in splenic rupture.7 MSR is usually seen in the patient with acute infection, as recurrent infection can cause gradual and steady building of tension and will have less chance of splenic rupture,10,11 which is not in line with our patient. Spontaneous splenic rupture can also be secondary to neoplastic, hematological, and inflammatory causes which account for more than 50% of cases.13
In terms of duration, MSR can occur acutely any time during the course of illness. Most studies have suggested the median duration of 5 days but it can vary anywhere from day 0 to day 37.6 MSR generally presents as circulatory shock with peritonitis due to intra-abdominal bleeding.5,6 However, the typical presentation can be absent in most of the cases, therefore a high index of clinical suspicion is warranted in patients with severe malaria who presents with signs of acute abdomen.9,11
Splenectomy was historically performed for all MSR cases; however in the modern era, a nonoperative management can be safely followed for hemodynamically stable patients with serial ultrasonography or CT scan to assess the healing which is usually complete in 2–3 weeks13 and splenectomy being indicated or reserved for hemodynamically unstable patients.6 Alternatively in well-resourced centers, in patients with splenic rupture who are hemodynamically stable, interventional radiology can help embolize the splenic artery or one of its branches.14
The risk of post-splenectomy sepsis is a well-established, potentially lethal complication of splenectomy, especially in children, and this has driven the change in practice toward a non-operative management when the hemodynamic stability of the patient is objectively satisfactory. Our patient met the four criteria for spontaneous splenic rupture by Orloff and Peskin as the histopathology just revealed slight enlargement but otherwise grossly and microscopically normal. Additionally, our patient had no history of trauma and no other disease affecting the spleen.15
Conclusion
In conclusion, although numerous diseases can result in splenic complications, such as splenic rupture, malarial infection is known as the most common cause but it is likely underdiagnosed and underreported. Our patient underwent a surgical approach due to lack of an interventional radiologist who can perform this procedure in our country. Early diagnosis and appropriate disease management is essential. In the clinical case presented here, the availability of resources and timely intervention may have saved the patient’s life.
Ethical Consideration
Informed written consent was obtained from the study participant to publish the case details. Institutional approval was not required to publish the case details.
Acknowledgment
Zameena Kassam, Department of Radiology, Aga Khan Hospital, Dar-es-salaam, Tanzania.
Funding
There is no funding to report.
Disclosure
None of the authors have any conflict of interest to disclose.
References
1. Suh KN, Kain KC, Keystone JS. Malaria. CMAJ. 2004;170(11):1693–1702. doi:10.1503/cmaj.1030418
2. Dhiman S. Are malaria elimination efforts on right track? An analysis of gains achieved and challenges ahead. Infect Dis Poverty. 2019;8(1):14. doi:10.1186/s40249-019-0524-x
3. Streatfield PK, Khan WA, Bhuiya A, et al. Malaria mortality in Africa and Asia: evidence from INDEPTH health and demographic surveillance system sites. Glob Health Action. 2014;7:25369. doi:10.3402/gha.v7.25369
4. Svenson JE, MacLean JD, Gyorkos TW, Keystone J. Imported malaria. Clinical presentation and examination of symptomatic travelers. Arch Intern Med. 1995;155(8):861–868. doi:10.1001/archinte.1995.00430080109013
5. Waweru P, Macleod J, Gikonyo A. Complicated malaria and a covert ruptured spleen: a case report. J Surg Case Rep. 2014;2014(11):rju122–rju122. doi:10.1093/jscr/rju122
6. Osman MF, Elkhidir IM, Rogers SO, Williams M. Non-operative management of malarial splenic rupture: the Khartoum experience and an international review. Int J Surg. 2012;10(9):410–414. doi:10.1016/j.ijsu.2012.06.001
7. Patel MI. Spontaneous rupture of a malarial spleen. Med J Aust. 1993;159(11–12):835–836. doi:10.5694/j.1326-5377.1993.tb141386.x
8. Trampuz A, Jereb M, Muzlovic I, Prabhu RM. Clinical review: severe malaria. Crit Care. 2003;7(4):315–323. doi:10.1186/cc2183
9. Rabie ME, Hashemey AA, El Hakeem I, et al. Spontaneous rupture of malarial spleen: report of two cases. Mediterr J Hematol Infect Dis. 2010;2(3):e2010036. doi:10.4084/mjhid.2010.036
10. Hershey FB, Lubitz JM. Spontaneous rupture of the malarial spleen: case report and analysis of 64 reported cases. Ann Surg. 1948;127(1):40–57. doi:10.1097/00000658-194801000-00005
11. Saad E, Elsamani E, Abdelrahman W. Spontaneous splenic rupture complicating severe P. falciparum infection: a case report and literature review. Case Rep Infect Dis. 2019;2019:2781647.
12. Hyun BH, Varga CF, Rubin RJ. Spontaneous and pathologic rupture of the spleen. Arch Surg. 1972;104(5):652–657. doi:10.1001/archsurg.1972.04180050028007
13. Papua New Guinea Splenic Injury Study Group. Ruptured spleen in the adult: an account of 205 cases with particular reference to non-operative management. Aust N Z J Surg. 1987;57(8):549–553. doi:10.1111/j.1445-2197.1987.tb01419.x
14. Kim NH, Lee KH, Jeon YS, Cho SG, Kim JH. Spontaneous splenic rupture in a vivax malaria case treated with transcatheter coil embolization of the splenic artery. Korean J Parasitol. 2015;53(2):215–218. doi:10.3347/kjp.2015.53.2.215
15. Orloff MJ, Peskin GW. Spontaneous rupture of the normal spleen; a surgical enigma. Int Abstr Surg. 1958;106(1):1–11.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.