Back to Journals » Infection and Drug Resistance » Volume 16
Case Report: Severe Diarrhea Caused by Cryptosporidium Diagnosed by Metagenome Next-Generation Sequencing in Blood
Authors Shan H, Wei C, Zhang J, He M, Zhang Z
Received 24 May 2023
Accepted for publication 23 August 2023
Published 1 September 2023 Volume 2023:16 Pages 5777—5782
DOI https://doi.org/10.2147/IDR.S422799
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Huifang Shan,1 Chunyan Wei,1 Jingyi Zhang,1 Min He,2 Zhongwei Zhang2
1Department of Pharmacy, West China Hospital, Sichuan University, Chengdu, People’s Republic of China; 2Department of Critical Care Medicine, West China Hospital, Sichuan University, Chengdu, People’s Republic of China
Correspondence: Zhongwei Zhang, Email [email protected]
Background: Cryptosporidium is one of the major pathogens causing diarrhea worldwide. At present, cryptosporidiosis is difficult to prevent and control, especially in immunocompromised hosts. It may cause life-threatening diarrhea and malabsorption among children and immunocompromised patients. Therefore, it is very important to explore rapid diagnostic tools and treatment methods for Cryptosporidium infection.
Case Presentation: We reported a case of severe diarrhea caused by cryptosporidiosis in a liver transplant recipient, whose condition was finally confirmed by metagenomic next-generation sequencing (mNGS) and fecal microscopy. His illness was resolved with immunosuppression regulation, nitazoxanide administration, and infection control.
Conclusion: So far, nitazoxanide is still the first choice for the treatment of cryptosporidiosis. Our institutional experience suggested that nitazoxanide alone may be effective on the basis of adjusting immunosuppressant. In addition, even though diagnosis of Cryptosporidium infection is a challenge, mNGS can serve as a rapid screening tool in low-prevalence setting.
Keywords: nitazoxanide, cryptosporidiosis, Cryptosporidium, transplant recipient, azithromycin
Introduction
Cryptosporidiosis is caused by Cryptosporidium, an intracellular protozoan parasite mainly infected and reproduced in the epithelial cells of the digestive tract.1 The most common mean of transmission is through contaminated an infected person or animal or from a fecally contaminated environment, such as a food or water source. Cryptosporidium parvum is one of the main species responsible for clinical disease in humans, destroying enterocytes, causing gastrointestinal symptoms such as watery diarrhea and abdominal cramps, first confirmed to be related to gastrointestinal disease in humans in 1976.2 This disease is generally self-limited with mild diarrhea occurring in immunocompetent patients, but the course of disease may be longer and more severe in immunocompromised hosts. For instance, chances are higher with patients with cellular and humoral immune deficiencies. These include HIV infection, organ transplantation, hypogammaglobulinemia, immunoglobulin (Ig)A deficiency, and genetic immune deficiencies including interleukin-21 receptor deficiency and CD40L deficiency, etc.3–6
A study evaluating the etiology of diarrhea in solid organ recipients reported that diarrhea caused by cryptosporidiosis accounted for 21.2% and 3% in the solid organ transplantation group and control group, respectively.7 However, the diagnosis and treatment of cryptosporidiosis are problematic.8 In terms of diagnosis, the gold standard for laboratory diagnosis is based on the identification of oocysts in stool samples by using light microscopy with staining-based techniques. Nevertheless, the method may lack specificity and sensitivity. Here we propose a new approach based on molecular diagnostic techniques utilizing fluid samples rather than feces. Cryptosporidium DNA fragments were detected in blood sample through metagenomic next-generation sequencing (mNGS). Additionally, in clinical treatment, nitazoxanide is the unique drug approved by US Food and Drug Administration to treat cryptosporidiosis.9,10 However, some studies have found that nitazoxanide alone may be less effective.11–13 The data of nitazoxanide alone involved in the treatment of cryptosporidiosis in transplant recipients is also limited and low-quality, with most cases reported in children.11,14 In this manuscript, we describe a case with symptoms subsided rapidly with nitazoxanide alone after azithromycin treatment failed on the basis of modulating cellular immunity.
Case Presentation
In July 2022, a 56-year-old Chinese male came to our hospital for 20 days of diarrhea. At the beginning, it is yellow loose stools, 6–8 times a day. Ten days ago, the patient had aggravated diarrhea, manifested as dark green watery stool, up to 10 times a day, accompanied by palpitations, shortness of breath, dizziness, dry mouth, dry skin, and sunken eye socket symptoms. A week before his admission, he had no history of fevering, abdominal pain or travelling. Two years ago, the patient received allograft in our hospital for liver cancer and hepatitis B cirrhosis. To avoid rejection, he took long-term immunosuppressive therapy of tacrolimus (1mg q12h), mycophenolic acid (750mg q12h) and sirolimus (1mg qd) after surgery.
On admission, the patient had a temperature of 37.9 °C, presented with septic shock and metabolic acidosis, and was intubated and transferred to the intensive care unit. Because the patient presented with oliguria and serum creatinine of 170 μmol/L, continuous renal replacement treatment (CRRT) was conducted for acute kidney injury. In addition, laboratory examination revealed white blood cell (WBC) count 13.46×109/L with an elevated neutrophil ratio of 87.9%. The concentration of procalcitonin (PCT) and C-reactive protein (CRP) were 3.32 ng/mL and 190 mg/L, respectively. Troponin-T (TPN-T) was 191.2 ng/L. It suggested possible abdominal or lung infection and myocardial injury. There were no significant changes in liver function test, blood coagulation test or platelet count. The tacrolimus concentration is within the target treatment range. As the patient’s temperature continued to rise to 38.5°C, no significant improvement was observed after empirical treatment with piperacillin/tazobactam, we collected bronchoalveolar lavage solution for culture. The results revealed Aspergillus fumigatus and carbapenem-resistant Klebsiella pneumoniae. Urine bacterial culture, venous blood culture and anaerobic blood culture were negative. According to drug sensitivity results, antibacterial agents were replaced by meropenem and voriconazole. In view of the severe infection of patients and the fact that the concentrations of tacrolimus and sirolimus can be affected by voriconazole, tacrolimus and sirolimus were discontinued. We collected stool for detection, and the results showed that intestinal bacterial culture, microscopic examination of parasite, clostridium difficile antigen were negative. Because of diarrhea, the patient was given compound berberine (a Chinese proprietary medicine, which has inhibitory effect on intestinal bacteria and can be used for intestinal infection) to decrease diarrhea, and at the same time, the electrolyte balance and acid-base balance in the patient’s body were corrected. Subsequently, the patient’s diarrhea was significantly mitigated, and enteral nutrition solution and probiotics were given to regulate intestinal function. Two days later, the patient again developed high frequency diarrhea (6–8 watery stools per day) with fever, with a temperature fluctuating around 39 °C. Subsequently, parasitic examination of stool and fecal bacterial cultures received negative results. For rapid detection of possible pathogens, the blood sample of the patient was sent to undergo PACEseq mNGS analysis (Genskey, Chengdu, China). Two days later, the mNGS result revealed the presence of Klebsiella pneumoniae and Cryptosporidium parvum, with reads of 19 and 33, respectively (Figure 1). In addition, we detected oval bodies in stool samples of patients by modified acid-fast stain, which were Cryptosporidium oocysts. At present, Cryptosporidium infection was well established, and we proposed to give nitazoxanide, but this drug is not readily available. Therefore, we temporarily chose azithromycin (0.5g qd) alone for treatment. At the same time, laboratory results indicated that the indices of the liver function and T lymphocyte count were elevated, which may be related to the rejection caused by the reduction of immunosuppressive drugs. Hence we added cyclosporine (150mg bid) into his prescription. Two days after taking cyclosporine, we determined that the trough concentration of cyclosporine was 194.00 μg/L, which exceeded the therapeutic concentration, possibly related to the combination of Voriconazole, and adjusted the cyclosporine dose to maintain around 100 ng/mL. After one week, the patient’s diarrhea did not improve, so azithromycin was stopped and nitazoxanide (500mg tid) was added. On the third day of medication, the patient’s diarrhea frequency was reduced to 3–4 times a day. After two weeks of treatment, the patient’s diarrhea subsided. The fecal samples were collected again for acid fast staining, and we found no Cryptosporidium oocysts and stopped providing nitazoxanide.
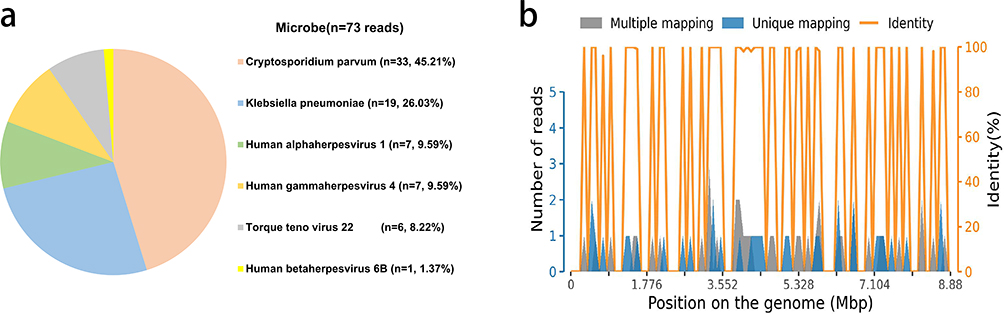 |
Figure 1 mNGS results of the patients. (a) A total of 33 specific reads of Cryptosporidium parvum were detected by mNGS in this case. (b) The coverage of Cryptosporidium parvum detected by mNGS was 0.0332%. |
The patient recovered slowly with immunosuppression and severe pulmonary infection. After 40 days of hospitalization, the patient’s systemic infection was obviously controlled, and he could be disconnected from the ventilator intermittently. At the same time, the creatinine slowly decreased to the normal baseline level, and the liver function gradually recovered. After 47 days in hospital, the patient’s condition gradually stabilized. He no longer relied on the ventilator and was transferred to the general ward to continue rehabilitation treatment. The timeline of the treatment is shown in Figure 2.
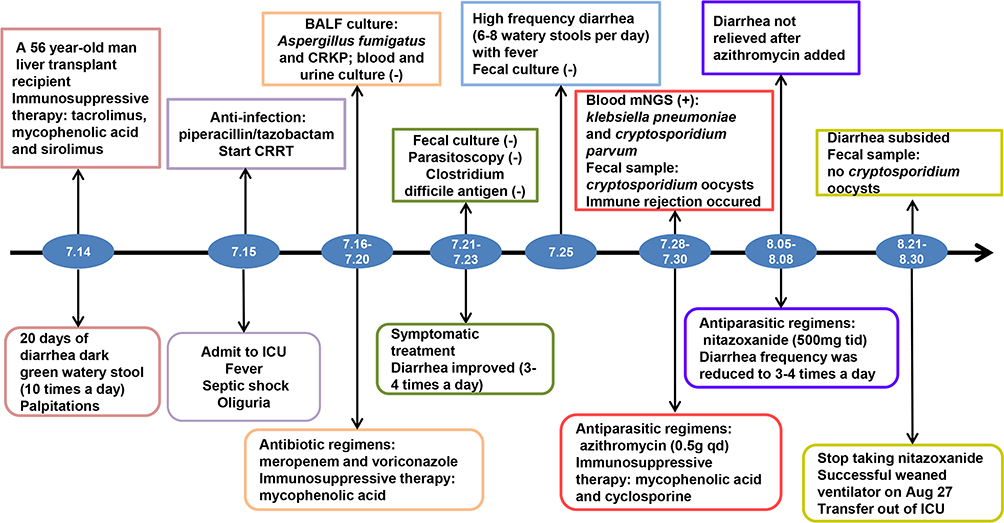 |
Figure 2 Timeline of disease progression. Abbreviations: CRRT, continuous renal replacement treatment; ICU, intensive care unit; BALF, bronchoalveolar lavage fluid, mNGS, metagenomic next-generation sequencing. |
Discussion
Tyzzer first found Cryptosporidium in experimental mice in 1907.15 In the following 70 years, Cryptosporidium infection in snakes, poultry, dogs, cats, cattle, sheep and other animals has been reported around the world. In 1976, the first case of Cryptosporidium infection resulting in self-limiting enteritis in humans was reported, suggesting that cryptosporidiosis had become one of the zoonotic diseases.16 The pathogenic mechanism of Cryptosporidium leading to diarrhea in immunocompromised patients is unclear, which may be related to a variety of factors.17,18 In general, most cryptosporidiosis patients have from mild to moderate symptoms, and they can maintain their body fluid balance without additional treatment. However, this disease may cause life-threatening diarrhea in immunocompromised patients.
Diarrhea is common in solid organ transplant patients, with a prevalence of about 20%-50%.19 In addition, diarrhea may be secondary to bacterial, viral, parasitic infections, and some immunosuppressive drugs, such as mycophenolic acid and tacrolimus.20 In this case, we tested for common pathogens that could cause diarrhea, but no positive results were found. At the same time, we also stopped tacrolimus and sirolimus, and the patient’s diarrhea did not stop. Eventually, we picked up Cryptosporidium parvum through Metagenomic sequencing.
Traditionally, the diagnosis of cryptosporidiosis mainly depended on microscopy and fecal immunoassay. Nowadays, molecular methods have been used to identify species, genotypes and subtypes of Cryptosporidium in patients with high specificity and sensitivity. The method shows high specificity and high sensitivity. In a study of 200 patients with diarrhea, fecal samples were examined using microscopy (modified acid-fast staining), sandwich enzyme-linked immunosorbent assay (ELISA), and nested PCR.21 Compared with ELISA and microscope, PCR has the highest detection rate (21%, 12.5% and 9.5% respectively). In this case, although the DNA sequence levels of C. parvum and C. hominis were similar (> 96%), we still found Cryptosporidium DNA in the blood of the patient via mNGS and identified its species, providing directions for subsequent treatment.
There is no high-quality evidence that nitazoxanide is more effective than placebo in HIV-infected patients, and also very little data on transplant recipients, but nitazoxanide remains the drug of choice for cryptosporidiosis. The American Society of Transplantation Infectious Diseases recommends that solid organ transplant patients with cryptosporidiosis receive antimicrobial treatment, usually with nitazoxanide monotherapy, and patients with severe disease receive combined treatment.14
In addition to nitazoxanide, drugs with anti-Cryptosporidium activity in vitro, animal models and patients include azithromycin, paromomycin and rifaximin.8 Rifabutin has been shown to be effective in HIV patients, but data are limited.22,23 Among them, azithromycin belongs to macrolides, which was used in the initial treatment of cryptosporidiosis because it is relatively easy to obtain. Azithromycin monotherapy has been reported to improve clinical outcomes in HIV-infected patients with cryptosporidiosis, but responses have been variable.24 Therefore, we proposed that azithromycin should be used in combination with other antiparasitic drugs for cryptosporidiosis.
Antiparasitic drugs are the suboptimal treatment for Cryptosporidium infection.9 Improving cellular immunity is an important prerequisite for treating cryptosporidiosis in immunodeficient patients. The American Society of Transplantation Infectious Diseases strongly recommends that immunosuppressants be reduced, if possible, for gastrointestinal infections of solid organ transplantation (SOT) recipients caused by Cryptosporidium.14 The use of tacrolimus has been demonstrated to increase the risk of cryptosporidiosis infection.25 Bonatti et al25 exhibited that compared with transplant recipients infected with community-acquired clostridium difficile (CDI), SOT recipients with cryptosporidiosis had increased tacrolimus levels and acute renal injury, which may be related to the change of drug metabolism in the small intestine caused by Cryptosporidium enteritis.
However, modulating immunosuppressant and monitoring immunosuppression levels can be challenging. Critically ill patients often have not only gastrointestinal infection caused by Cryptosporidium, but also concurrent infections induced by multi-drug resistant bacteria and fungi, and even Multiple Organ Dysfunction Syndrome (MODS). In our case report, the patient was discontinued from tacrolimus and sirolimus upon admission, but a few days later developed abnormal liver function, which we suspected was related to rejection due to immunosuppressant reduction and added the cyclosporine. Nevertheless, the trough level of cyclosporine exceeded the target treatment concentration after two days, which was considered to be a clinically significant interaction between voriconazole and cyclosporine. The label of voriconazole (VFEND) shows that voriconazole is a strong inhibitor of CYP3A4, which can significantly increase the AUCτ of cyclosporine. Finally, we resolved the diarrhea with nitazoxanide alone, which may benefit from the adjustment of the immunosuppressive regimen. Consequently, when transplant recipients suffer from severe infection, the adjustment of immunosuppressant is complicated, and the combination of other drugs and the patient’s liver and kidney function should be considered to avoid further deterioration of the patient’s disease.
Conclusions
Currently, cryptosporidiosis is highly reported in people with human immunodeficiency virus (HIV) infection, but the true prevalence of it in solid organ transplant patients is not yet known. Cryptosporidiosis after liver transplantation is difficult to diagnose at an early stage and may be overlooked. In this case, we found Cryptosporidium DNA in the blood of transplant recipients by mNGS. With this diagnostic method, the patient can receive immediate treatment and recover through this diagnostic technique. Although there is a lack of standardized effective treatment for cryptosporidiosis in immunodeficient patients, especially in SOT recipients, our case report suggested that nitazoxanide alone was effective on the premise of adjusting immunosuppressant. It provided our institutional experience in the diagnosis and treatment of cryptosporidiosis in a low-prevalence setting. And it is necessary to remind people with low immunity to maintain good personal hygiene habits and reduce, control or eliminate the pathogenic risk factors of other animals for the prevention and transmission of cryptosporidiosis.
Data Sharing Statement
The data and information are true and reliable. If you need this data, you can get it from Huifang Shan or the corresponding author.
Ethics Approval and Informed Consent
The treatment of this case was conducted in accordance with the Declaration of Helsinki. All procedures were performed in accordance with the ethical standards of the Clinical Research ethical committee of West China Hospital, Sichuan University (No.2023 (364)). Written informed consent was obtained from the patients for the publication of this case report. And the case report does not contain any pictures that could identify the patient. In addition, the organ was donated voluntarily with written informed consent, and that the organ donation was conducted in accordance with the Declaration of Istanbul.
Acknowledgments
The author would like to thank all the medical staff in the intensive care unit of West China Hospital, Sichuan University who participated in the patient.
Funding
This research received no external funding.
Disclosure
The authors declare that they have no competing interests.
References
1. Chen XM, Keithly JS, Paya CV, LaRusso NF. Cryptosporidiosis. N Engl J Med. 2002;346(22):1723–1731. doi:10.1056/NEJMra013170
2. Bouzid M, Hunter PR, Chalmers RM, Tyler KM. Cryptosporidium pathogenicity and virulence. Clin Microbiol Rev. 2013;26(1):115–134. doi:10.1128/CMR.00076-12
3. Fayer R, Ungar BL. Cryptosporidium spp. and cryptosporidiosis. Microbiol Rev. 1986;50(4):458–483. doi:10.1128/mr.50.4.458-483.1986
4. Lanternier F, Amazzough K, Favennec L, et al. Cryptosporidium spp. Infection in Solid Organ Transplantation: the Nationwide “TRANSCRYPTO” Study. Transplantation. 2017;101(4):826–830. doi:10.1097/TP.0000000000001503
5. Cagdas D, Mayr D, Baris S, et al. Genomic Spectrum and Phenotypic Heterogeneity of Human IL-21 Receptor Deficiency. J Clin Immunol. 2021;41(6):1272–1290. doi:10.1007/s10875-021-01031-5
6. Dupuy F, Valot S, Dalle F, Sterin A, L’Ollivier C. Disseminated Cryptosporidium infection in an infant with CD40L deficiency. IDCases. 2021;24:e01115. doi:10.1016/j.idcr.2021.e01115
7. Gerber DA, Green M, Jaffe R, Greenberg D, Mazariegos G, Reyes J. Cryptosporidial infections after solid organ transplantation in children. Pediatr Transplant. 2000;4(1):50–55. doi:10.1034/j.1399-3046.2000.00087.x
8. Checkley W, White AC, Jaganath D, et al. A review of the global burden, novel diagnostics, therapeutics, and vaccine targets for cryptosporidium. Lancet Infect Dis. 2015;15(1):85–94. doi:10.1016/S1473-3099(14)70772-8
9. Cabada MM, White AC. Treatment of cryptosporidiosis: do we know what we think we know? Curr Opin Infect Dis. 2010;23(5):494–499. doi:10.1097/QCO.0b013e32833de052
10. Rossignol JF, Kabil SM, el-Gohary Y, Younis AM. Effect of nitazoxanide in diarrhea and enteritis caused by Cryptosporidium species. Clin Gastroenterol Hepatol. 2006;4(3):320–324. doi:10.1016/j.cgh.2005.12.020
11. Abubakar I, Aliyu SH, Arumugam C, Hunter PR, Usman NK. Prevention and treatment of cryptosporidiosis in immunocompromised patients. Cochrane Database Syst Rev. 2007;1:Cd004932.
12. Amadi B, Mwiya M, Musuku J, et al. Effect of nitazoxanide on morbidity and mortality in Zambian children with cryptosporidiosis: a randomised controlled trial. Lancet. 2002;360(9343):1375–1380. doi:10.1016/S0140-6736(02)11401-2
13. Rossignol JF, Hidalgo H, Feregrino M, et al. A double-’blind’ placebo-controlled study of nitazoxanide in the treatment of cryptosporidial diarrhoea in AIDS patients in Mexico. Trans R Soc Trop Med Hyg. 1998;92(6):663–666. doi:10.1016/S0035-9203(98)90804-5
14. La Hoz RM, Morris MI. Intestinal parasites including Cryptosporidium, Cyclospora, Giardia, and Microsporidia, Entamoeba histolytica, Strongyloides, Schistosomiasis, and Echinococcus: guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin Transplant. 2019;33(9):e13618. doi:10.1111/ctr.13618
15. Tyzzer EE. A sporozoan found in the peptic glands of the common mouse. Exp Biol Med. 1907;5(1):12–13. doi:10.3181/00379727-5-5
16. Šlapeta J. Cryptosporidiosis and Cryptosporidium species in animals and humans: a thirty colour rainbow? Int J Parasitol. 2013;43(12–13):957–970. doi:10.1016/j.ijpara.2013.07.005
17. O’Donoghue PJ. Cryptosporidium and cryptosporidiosis in man and animals. Int J Parasitol. 1995;25(2):139–195. doi:10.1016/0020-7519(94)e0059-v
18. Pane S, Putignani L. Cryptosporidium: still Open Scenarios. Pathogens. 2022;11(5):515. doi:10.3390/pathogens11050515
19. Bunnapradist S, Neri L, Wong W, et al. Incidence and risk factors for diarrhea following kidney transplantation and association with graft loss and mortality. Am J Kidney Dis. 2008;51(3):478–486. doi:10.1053/j.ajkd.2007.11.013
20. Sellin JH. The pathophysiology of diarrhea. Clin Transplant. 2001;15(Suppl 4):2–10. doi:10.1111/j.1399-0012.2001.00002.x
21. Abdel Gawad SS, Ismail MAM, Imam NFA, Eassa AHA, Abu-Sarea EY. Detection of Cryptosporidium spp. in Diarrheic Immunocompetent Patients in Beni-Suef, Egypt: insight into Epidemiology and Diagnosis. Korean J Parasitol. 2018;56(2):113–119. doi:10.3347/kjp.2018.56.2.113
22. Fichtenbaum CJ, Zackin R, Feinberg J, Benson C, Griffiths JK. Rifabutin but not clarithromycin prevents cryptosporidiosis in persons with advanced HIV infection. AIDS. 2000;14(18):2889–2893. doi:10.1097/00002030-200012220-00010
23. Holmberg SD, Moorman AC, Von Bargen JC, et al. Possible effectiveness of clarithromycin and rifabutin for cryptosporidiosis chemoprophylaxis in HIV disease. HIV Outpatient Study (HOPS) Investigators. JAMA. 1998;279(5):384–386. doi:10.1001/jama.279.5.384
24. Hicks P, Zwiener RJ, Squires J, Savell V. Azithromycin therapy for Cryptosporidium parvum infection in four children infected with human immunodeficiency virus. J Pediatr. 1996;129(2):297–300. doi:10.1016/S0022-3476(96)70258-5
25. Bonatti H, Barroso LF, Sawyer RG, Kotton CN, Sifri CD. Cryptosporidium enteritis in solid organ transplant recipients: multicenter retrospective evaluation of 10 cases reveals an association with elevated tacrolimus concentrations. Transplant Infect Dis. 2012;14(6):635–648. doi:10.1111/j.1399-3062.2012.00719.x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.