Back to Journals » Cancer Management and Research » Volume 17

Case Report: A Rare EGFR 20 Insertion Variant, P772_H773insGNP Mediates Resistance to Sunvozertinib but Is Sensitive to Furmonertinib
Authors Wang Y, Zheng J, Wang J, Sheng L, Qu J ![]() , Zhou J
, Zhou J ![]()
Received 8 May 2025
Accepted for publication 23 September 2025
Published 1 October 2025 Volume 2025:17 Pages 2277—2285
DOI https://doi.org/10.2147/CMAR.S539254
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Chien-Feng Li
Yufang Wang, Jing Zheng, Jie Wang, Lingyan Sheng, Jingjing Qu, Jianya Zhou
Department of Respiratory Disease, Thoracic Disease Center, The First Affiliated Hospital, College of Medicine, Zhejiang University, Hangzhou, People’s Republic of China
Correspondence: Jianya Zhou, Department of Respiratory Disease, Thoracic Disease Center, The First Affiliated Hospital, College of Medicine, Zhejiang University, Hangzhou, People’s Republic of China, Tel/Fax +86 571 8723 6876, Email [email protected]
Background: EGFR exon 20 insertion (Exon 20ins) is the most common type among rare EGFR mutations. It involves over 100 identified subtypes. These mutations are generally insensitive to epidermal growth factor receptor tyrosine kinase inhibitors (EGFR-TKIs). The development of small-molecule targeted agents specifically designed for Exon 20ins has brought new hope to this patient population. However, responses to Exon 20ins targeting agents vary across different insertion subtypes, and there is currently a lack of research focused on treatment strategies specifically for near-loop mutations such as P772_H773insGNP.
Methods: To explore individualized treatment strategies, we reviewed the medical records of a patient with Exon 20ins P772_H773insGNP. Relevant medical history, laboratory and imaging findings, and treatment details were collected and analyzed.
Results: This case report describes a patient with advanced non-small cell lung cancer (NSCLC). The patient was diagnosed with adenocarcinoma of the right upper lobe (T3N1M1a, stage IV). Next-generation sequencing (NGS) detected an EGFR exon 20ins, specifically P772_H773insGNP. The patient experienced disease progression despite multiple lines of therapy. Following multidisciplinary discussion, furmonertinib was initiated as sixth-line therapy. The best overall response was assessed as partial response (PR), and as of the last follow-up, the patient had achieved a progression-free survival (PFS) of 10.5 months.
Conclusion: This case represents the first report of a favorable response to furmonertinib in a patient with the EGFR exon 20ins subtype P772_H773insGNP, a near-loop mutation. EGFR exon 20ins mutations are highly heterogeneous, and different subtypes exhibit varying sensitivities to targeted drugs. Exploring individualized treatment approaches is of great clinical importance.
Keywords: EGFR 20 insertion, non-small cell lung cancer, rare subtype, sunvozertinib, furmonertinib, case report
Introduction
Lung cancer remains one of the leading causes of cancer-related mortality worldwide, with high incidence and death rates also observed in China.1 Non-small cell lung cancer (NSCLC) is the predominant histological subtype, accounting for approximately 80–85% of all lung cancer cases.2 The epidermal growth factor receptor (EGFR) serves as a major driver gene in NSCLC, with a mutation prevalence exceeding 50% in the Asian population.3 Common EGFR mutations include exon 19 deletions (19Del) and the exon 21 L858R point mutation (L858R), collectively referred to as classical EGFR mutations. Among non-classical mutations, exon 20 insertion mutations (Exon 20ins) represent the most frequent subtype, accounting for 4–12% of all EGFR mutations. These mutations are highly heterogeneous, with over 100 distinct subtypes reported to date.4 According to Chinese Medical Association guideline for clinical diagnosis and treatment of lung cancer (2024 edition), epidermal growth factor receptor tyrosine kinase inhibitors (EGFR-TKIs) are recommended as first-line therapy for NSCLC patients with positive EGFR sensitive mutations.5 Furthermore, amivantamab in combination with chemotherapy has been approved by the US Food and Drug Administration (FDA) as a first-line treatment for NSCLC harboring EGFR exon 20ins.6
The first-generation EGFR-TKIs (such as gefitinib, erlotinib, and icotinib) are 4-anilinoquinazoline compounds that reversibly bind to the ATP-binding site of the EGFR kinase domain, inhibiting downstream signaling pathways and thereby exerting antitumor effects.7,8 These agents marked the beginning of the targeted therapy era for advanced NSCLC. However, although these drugs demonstrated certain clinical efficacy, the median overall survival (mOS) of patients did not significantly improve compared with conventional chemotherapy. This limitation prompted the development of the second-generation EGFR-TKIs (such as afatinib and dacomitinib). These agents irreversibly inhibit both homodimers and heterodimers including HER1–HER4, thereby reducing resistance caused by abnormal activation of other HER family members.9 Their covalent binding mode enhances binding stability to the target and prolongs the duration of inhibition. Nonetheless, the second-generation agents showed limited efficacy against resistance mediated by the Thr790Met (T790M) mutation. Resistance driven by the T790M mutation spurred the development of third-generation EGFR-TKIs, including osimertinib, furmonertinib, and sunvozertinib.10 These compounds form covalent bonds with the Cys797 residue in the EGFR kinase domain, overcoming the steric hindrance effect caused by the T790M mutation and providing sustained suppression of EGFR activity, thereby demonstrating potent antitumor efficacy.11 Currently, fourth-generation EGFR-TKIs are designed to target compound mutations such as T790M and C797S. These inhibitors employ novel chemical structures to enhance selectivity toward mutant EGFR while reducing inhibition of the wild-type receptor, thereby minimizing toxicity. Representative agents include Brigatinib, TQB3804, and BLU-945.12
It is noteworthy that Exon 20ins NSCLC is generally insensitive to first- and second-generation EGFR-TKIs. A Chinese multicenter clinical study revealed that Exon 20ins NSCLC patients (n = 23) treated with first-line gefitinib, icotinib, or afatinib had a median progression-free survival (mPFS) of only 2.9 months, significantly lower than the 6.4 months observed in the platinum-based chemotherapy group.13 Third-generation EGFR-TKIs (such as osimertinib, sunvozertinib, and furmonertinib) have demonstrated certain clinical activity in this population. The UNICORN study reported a mPFS of 9.4 months and a disease control rate (DCR) of 90.0% with osimertinib in Exon 20ins NSCLC patients (n = 40).14 Results from a study showed that furmonertinib as first-line treatment for Exon 20ins NSCLC patients (n = 53) yielded an objective response rate (ORR) of 37.7% and a DCR of 92.5%.15 Additionally, A single-arm, single-center, Phase 2 clinical trial (WU-KONG15) that evaluates sunvozertinib in the first-line treatment of Exon 20ins NSCLC reported a mPFS of 10.1 months and an ORR of 73.1%.16 Despite these advances, the efficacy of current targeted therapies for EGFR exon 20ins remains suboptimal, with variability in drug sensitivity across different insertion subtypes, frequent emergence of resistance, and limited options for subsequent-line treatments.
This study reports a case of advanced NSCLC harboring an EGFR exon 20ins P772_H773insGNP mutation, co-occurring with RB1 and TP53 mutations, and AKT1 copy number amplification. The patient developed short-term resistance after multiple lines of therapy and was ultimately treated with furmonertinib as sixth-line treatment, achieving a progression-free survival(PFS) of 10.5 months as of the last follow-up. This case is the first to report that the Exon 20ins P772_H773insGNP may exhibit heightened sensitivity to furmonertinib, providing a valuable reference for clinical drug selection in patients with this mutation.
Case Report
A 47-year-old male patient presented to the First Affiliated Hospital of Zhejiang University on August 8, 2020, following the detection of a pulmonary shadow during a health examination. He had a history of smoking for over 20 years, with a daily consumption of approximately 40 cigarettes.
A chest computed tomography (CT) scan performed on December 23, 2020 (Figure 1A), revealed a thick-walled cavity in the right upper lobe measuring approximately 2.5 cm × 1.6 cm, with a smooth inner margin and surrounding patchy high-density shadows, accompanied by traction of the adjacent pleura. Multiple solid small nodules were also observed in the right lung, the largest measuring about 6 mm in diameter with clear boundaries. Additionally, multiple patchy high-density shadows were noted in the left lower lobe. To confirm the diagnosis, endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA) was performed. The patient had quit smoking by this time.
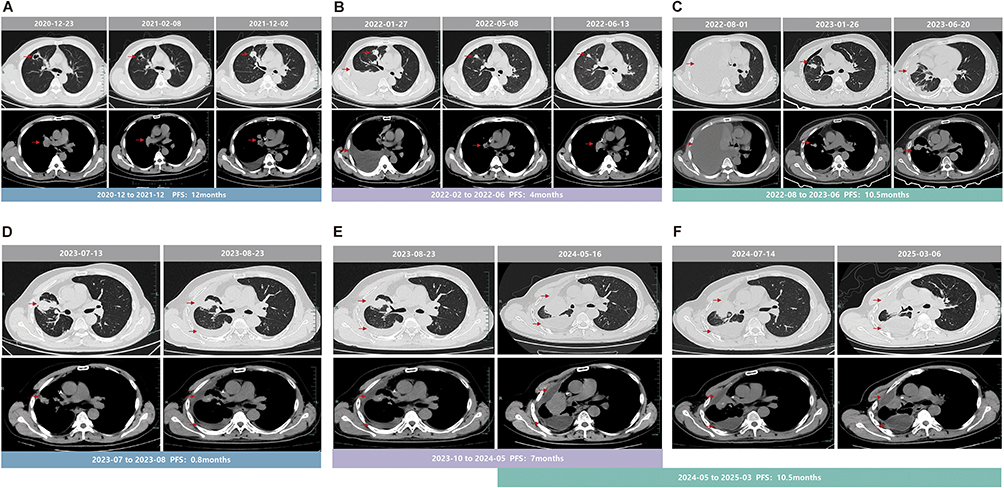 |
Figure 1 Computed tomography (CT) images at various points. →, the red arrow indicates the specific location of the lesion. (A) CT images during first-line treatment. (B) CT images during second-line treatment. (C) CT images during third-line treatment. (D) CT images during forth-line treatment. (E) CT images during fifth-line treatment. (F) CT images during sixth-line treatment. Abbreviation: PFS, progression-free survival. |
Pathology results dated December 11, 2020, indicated non-small cell carcinoma (from the right upper anterior segmental-subsegmental branch), morphologically consistent with adenocarcinoma. Immunohistochemistry showed CK7(+), TTF-1(+), NapsinA(+), P40(-), CDX2(-), and ALK Ventana(-). Integrated with findings from chest CT, cranial Magnetic Resonance(MRI) Imaging, abdominal ultrasound, and superficial lymph node ultrasound, the tumor was confirmed to involve the pleura with multiple pulmonary metastases. According to the International Association for the Study of Lung Cancer (IASLC) 8th edition TNM staging criteria, the patient was diagnosed with adenocarcinoma of the right upper lobe (T3N1M1a, Stage IV).
Due to financial constraints, the patient and his family initially declined genetic testing. After multidisciplinary team discussion, he was deemed eligible for a three-arm, randomized, double-blind, multicenter Phase III clinical trial (Protocol No: HLX10-002-NSCLC301). Starting December 17, 2020, the patient received first-line treatment consisting of pemetrexed, carboplatin, combined with HLX04 (a recombinant humanized anti-VEGF monoclonal antibody) and HLX10 (a recombinant humanized anti-PD-1 monoclonal antibody), as confirmed after unblinding. The best observed efficacy during the treatment period was assessed as stable disease (SD). A follow-up chest CT on December 2, 2021 (Figure 1A), showed enlargement of the primary lesion and increased size of multiple lymph nodes in the mediastinum and right hilum, indicating disease progression (PD). The PFS was approximately 12 months, and the patient was subsequently withdrawn from the study.
Following this, the patient experienced worsening cough and chest pain. A cranial MRI plain scan on December 14, 2021, revealed intracranial metastases. He underwent gamma knife radiosurgery on December 17, 2021, with a peripheral dose of 2–22 Gy and an isodose line of 50%. To guide further treatment, the patient consented to genetic testing. Next-generation sequencing(NGS) performed on January 22, 2022, identified an EGFR exon 20 insertion mutation: p.P772_H773insGNP.
After evaluation, he met the inclusion criteria for a clinical trial on targeted drugs for exon 20 insertions. He was enrolled in a Phase II, single-arm, multicenter clinical trial (Protocol No: DZ2020E0001). Beginning February 8, 2022, he received second-line treatment with DZD9008 (sunvozertinib) at a daily oral dose of 300 mg. On February 28, 2022, liver function tests indicated grade 2 abnormalities. Treatment with glutathione for liver protection yielded unsatisfactory results. The patient was hospitalized on March 4, 2022, due to abnormal liver function, which was identified as a serious adverse event (SAE). The dose of DZD9008 was reduced to 200 mg/day. During treatment, adverse events such as rash, elevated creatinine, fatigue, and vomiting occurred but were alleviated with symptomatic management without further dose adjustment. The best response during the treatment was assessed as partial response (PR). A follow-up chest CT on June 13, 2022 (Figure 1B), indicated disease progression, leading to discontinuation of DZD9008. The PFS for second-line treatment was approximately 4 months.
From August 2, 2022, to June 27, 2023 (Figure 1C), the patient received third-line treatment consisting of nab-paclitaxel, carboplatin, and bevacizumab (completing 7 cycles of chemotherapy combined with immunotherapy and 3 cycles of maintenance immunotherapy). The best response during the treatment was assessed as PR. Treatment was terminated due to disease progression, with a PFS of approximately 10.5 months.
On July 26, 2023, the patient participated in a multicenter, open-label phase I/IIa clinical trial (Protocol No: BR790-103), receiving BR790 50 mg combined with anlotinib hydrochloride 10 mg. On August 21, 2023, he experienced sudden throat pain, dysphagia, and generalized edema, which were considered a severe drug allergy reaction. Symptoms improved after treatment with methylprednisolone, calcium gluconate, and furosemide. The best response was assessed as SD. The patient withdrew from the study, with a PFS of approximately 0.8 months for the fourth-line treatment (Figure 1D).
Fifth-line treatment was initiated on October 23, 2023, consisting of gemcitabine, carboplatin, bevacizumab, and immunotherapy. The best response during treatment was assessed as SD. A follow-up chest CT on May 16, 2024 (Figure 1E), showed enlargement of the primary right lung lesion and pleural metastases, right pleural effusion with atelectasis, and enlarged mediastinal and right supraclavicular lymph nodes, indicating disease progression. The PFS was approximately 7 months.
The patient had undergone multiple lines of treatment, including chemotherapy combined with immunotherapy, targeted therapy, and chemotherapy alone, all of which were terminated due to disease progression. Following literature review and expert discussion, he started furmonertinib on May 17, 2024. A follow-up CT on July 14, 2024 (Figure 1F), showed reduction in the right lung lesions and metastases, with stable pleural effusion, assessed as PR. At the last follow-up in March 2025 (Figure 1F), the primary lesion remained stable, subjective symptoms had improved, and the patient continued on oral furmonertinib treatment with a PFS of 10.5 months to date. Following five lines of therapy, the patient achieved a favorable therapeutic response to sixth-line furmonertinib (Figure 2).
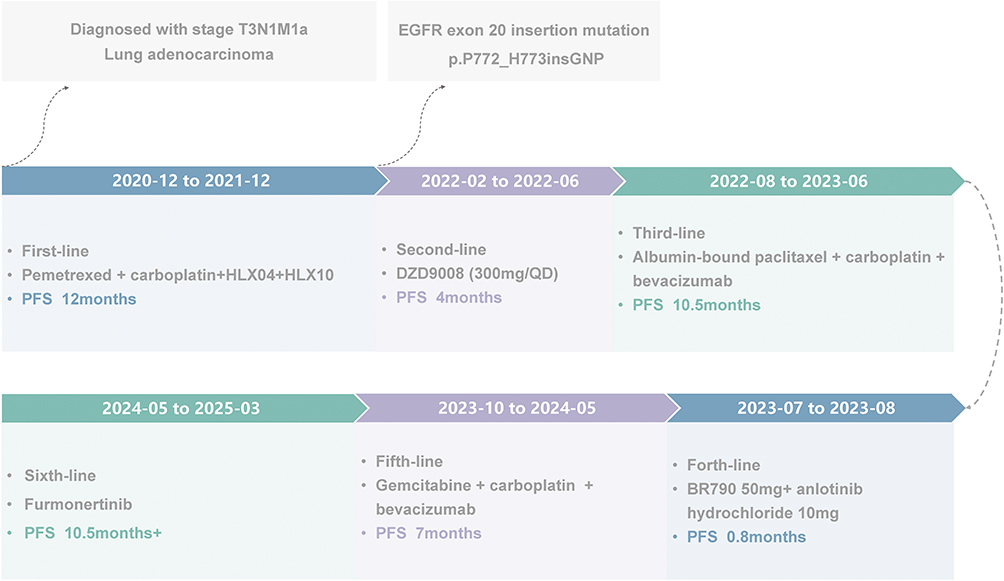 |
Figure 2 The timeline spans from the diagnosis of lung adenocarcinoma to the present. Abbreviations: PFS, progression-free survival; HLX04, a recombinant humanized anti-VEGF monoclonal antibody; HLX10, a recombinant humanized anti-PD-1 monoclonal antibody; DZD9008, sunvozertinib; BR790, small-molecule targeted drugs. |
Discussion
EGFR exon 20 encodes amino acid residues 762–823 of the protein, encompassing two core functional regions: the C-helix domain (residues 762–766) and the loop region downstream of the C-helix (residues 767–775). The loop region is further subdivided into the near-loop (residues 767–772) and far-loop (residues 773–775).15,17 Exon 20ins involve nucleotide insertions within these three regions (C-helix, near-loop, and far-loop), leading to an elongated amino acid sequence (Figure 3A). Approximately 90% of Exon 20ins are concentrated in the loop region downstream of the C-helix (residues 767–775), while only 10% occur within the C-helix domain itself (residues 762–766).18 Exon 20ins exhibit high heterogeneity, with over 100 distinct subtypes identified to date.4 The four most common subtypes include V769_D770insASV, D770_N771insSVD, H773_V774insNPH, and D770_N771insG.17 This alteration modifies the spatial conformation of the EGFR tyrosine kinase domain, creates steric hindrance around the drug-binding pocket, and ultimately impedes drug binding.19,20 The mutation carried by the patient in this case, P772_H773insGNP, belongs to the near-loop region.
 |
Figure 3 (A) The gene structure of EGFR 20 insertion. (B) The chemical structural of different drugs and their sites of action with EGFR. |
Both third-generation EGFR TKIs, sunvozertinib and furmonertinib, feature an aminopyrimidine core structure and demonstrate efficacy against certain Exon 20ins (Figure 3B). Sunvozertinib is derived from osimertinib but incorporates a more flexible aniline group at the C-4 position. This enables it to exert potent activity across various EGFR Exon 20ins subtypes, significantly surpassing the efficacy of traditional platinum-based doublet chemotherapy.21 Based on its notable clinical benefits, sunvozertinib was approved in August 2023 for the treatment of adult patients with locally advanced or metastatic NSCLC harboring EGFR Exon 20ins.22 In a single-arm, open-label, multicenter Phase II clinical trial (WU-KONG6), which enrolled 97 patients who had received at least one prior line of systemic therapy and covered 29 different Exon 20ins subtypes, sunvozertinib achieved an ORR of 61%, a DCR of 80%, and a mPFS of 9.7 months.23
Similarly, furmonertinib is structurally optimized from osimertinib by replacing a methyl group on the methoxy phenyl ring with a 2,2,2-trifluoroethyl moiety, enhancing metabolic stability and target affinity24 (Figure 3B). Phase Ib data from the FAVOUR study showed that furmonertinib, when administered at 240 mg, achieved ORR of 78.6% in treatment-naïve patients (n=28) and 46.2% in previously treated patients (n=26), along with DCR of 100% and 92.3%, respectively. In previously treated patients receiving a 160 mg dose (n=26), the ORR was 38.5% with a DCR of 84.6%.25 Based on these results, the US Food and Drug Administration (FDA) approved furmonertinib in October 2023 for the treatment of previously untreated advanced NSCLC patients with this mutation.26 In addition, data from a study showed that the ORR of furmonertinib as first-line therapy in NSCLC patients with EGFR exon 20ins mutations (n=53) reached 37.7%, and the disease control rate (DCR) was 92.5%.15
In the present case, the patient received sunvozertinib as second-line therapy but required dose reduction to 200 mg due to severe liver dysfunction, achieving only 4 months of PFS, suggesting a suboptimal response. However, after switching to furmonertinib as sixth-line treatment, the best response was assessed as PR, and the patient maintained a PFS of 10.5 months as of the last follow-up. This case is the first to report that the near-loop mutation P772_H773insGNP may be sensitive to furmonertinib. Consistent with this, a 2022 case report described an advanced NSCLC patient with an N771_P772insH mutation (also a near-loop mutation) who achieved a PFS of 10.0 months and an OS of 22.0 months with second-line furmonertinib.27 These findings collectively suggest that near-loop mutations within EGFR exon 20ins may exhibit favorable sensitivity to furmonertinib.
In recent years, collaborative efforts between academia and the pharmaceutical industry have led to the development of several new drugs targeting EGFR exon 20ins, such as mobocertinib, amivantamab, and zipalertinib.
Mobocertinib, an irreversible EGFR-TKI that inhibits EGFR activity by covalently binding to Cys797, was the first oral targeted agent approved for this population28 (Figure 3B). However, a phase III randomized controlled trial showed that in previously untreated advanced Exon 20ins-positive NSCLC patients, the mPFS of the mobocertinib group was similar to that of the chemotherapy group (9.59 months vs 9.63 months). Although mobocertinib showed slightly higher ORR (32% vs 30%) and DCR (87% vs 80%), the study did not meet its primary endpoint, leading to the drug’s early development termination and market withdrawal.29
In contrast, amivantamab(JNJ-61186372), a bispecific antibody, addresses EGFR mutations and MET amplification (Figure 3B). A phase III study comparing amivantamab combined with chemotherapy versus chemotherapy alone as first-line treatment for Exon 20ins NSCLC demonstrated that the combination therapy group (n=153) had significantly superior ORR (73% vs 43%) and longer mPFS (11.4 months vs 6.7 months) as assessed by an independent review committee (IRC).30 Consequently, amivantamab combined with chemotherapy has received full FDA approval as a first-line standard treatment for this patient population.6
Meanwhile, the novel oral TKI zipalertinib (CLN-081/TAS6417), which features a pyrrolopyrimidine core, has shown promising potential in a phase I/IIa study (Figure 3B). Across all dose groups (n=73), the mPFS was 10 months and the ORR was 38.4%. In the 100 mg twice-daily dose group (n=39), the mPFS reached 12 months and the ORR was 41%.31
It is important to note that multiple studies indicate that different Exon 20ins subtypes exhibit structural and functional variations, leading to significant heterogeneity in treatment response. Research has shown that high-dose osimertinib (160 mg/day) has an ORR of 25–28% and an mPFS of 6.8–9.7 months for mutations in the loop region downstream of the C-helix.32,33 Amivantamab alone exhibits greater activity against near-loop mutations than far-loop mutations, with ORRs of 41% and 25%, respectively.34 For the C-helix insertion mutation A763_Y764insFQEA, afatinib can achieve an mPFS of up to 24 months, similar to classical mutations.18 Therefore, treatment strategies must be individualized based on the specific mutation subtype in clinical practice.
Consistent with the findings in this case, while furmonertinib demonstrates overall lower efficacy in the general Exon 20ins compared to agents like amivantamab, it shows notable activity in the near-loop mutation P772_H773insGNP. This provides a valuable reference for clinical drug selection in patients with this subtype. It underscores that Exon 20ins should not be treated as a single disease entity due to its high heterogeneity. Clinical decision-making must be based on the mutation region and subtype, incorporating structural-functional models and clinical evidence to maximize therapeutic benefit.18 The limitation of this study is that it includes only a single patient, so the observed sensitivity of the P772_H773insGNP subtype to furmonertinib may be coincidental. Validating the efficacy of furmonertinib in treating Exon 20ins near-loop mutation requires more basic research to elucidate the underlying structural mechanisms and larger-scale clinical studies.
Conclusions
EGFR exon 20ins exhibit high heterogeneity, and their spatial conformational differences lead to significant variations in sensitivity to different targeted drugs. This case first identified potential sensitivity of the near-loop P772_H773insGNP mutation to furmonertinib, providing clinical evidence for precision treatment in patients with this subtype. It further underscores the importance of developing individualized treatment strategies based on the mutational structural domain and specific subtype. However, as a single-case report, the conclusions drawn from this study may represent a coincidental finding. To elucidate the underlying mechanisms, structural pharmacological studies are essential; moreover, confirmation in larger clinical cohorts is critically needed to validate these findings. We look forward to seeing increased emphasis on translational and clinical research focused on Exon 20 ins subtypes, which would contribute to advancing targeted therapeutic strategies for EGFR exon 20ins NSCLC.
Ethics and Consent
Written informed consent was obtained from the patient for the publication of this case report and any accompanying images.
This study was approved by the Ethics Committee of the First Affiliated Hospital, College of Medicine, Zhejiang University.
Funding
This work was supported by Key R&D Program of Zhejiang Respiratory Disease (No. 2023C03069, 2025C02092, 2025C02094).
Disclosure
All authors declare no potential conflicts of interest in this work.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–263. doi:10.3322/caac.21834
2. Abdelmaksoud-Dammak R, Ammous-Boukhris N, Saadallah-Kallel A, et al. Predominance of the rare EGFR mutation p.L861Q in Tunisian patients with non-small cell lung carcinoma. Genes. 2022;13(8):1499. doi:10.3390/genes13081499
3. Jiang Y, Fang X, Xiang Y, et al. Afatinib for the Treatment of NSCLC with Uncommon EGFR Mutations: a Narrative Review. Curr Oncol. 2023;30(6):5337–5349. doi:10.3390/curroncol30060405
4. Shi Y, Xu Y, Wang M. Current clinical practice and physicians’ insights on Chinese patients with advanced non-small cell lung cancer habouring epidermal growth factor receptor 20 insertion mutation. BMC Cancer. 2024;24(1):1043. doi:10.1186/s12885-024-12797-3
5. Oncology Society of Chinese Medical Association. Chinese Medical Association guideline for clinical diagnosis and treatment of lung cancer (2024 edition). Natl Med J China. 2024;104(34):3175–3213.
6. FDA approves amivantamab-vmjw for EGFR exon 20 insertion-mutated non-small cell lung cancer indications. FDA; 2024.
7. Wu YL, Zhou C, Liam CK, et al. First-line erlotinib versus gemcitabine/cisplatin in patients with advanced EGFR mutation-positive non-small-cell lung cancer: analyses from the Phase III, randomized, open-label, ENSURE study. Ann Oncol. 2015;26(9):1883–1889. doi:10.1093/annonc/mdv270
8. Wang L, Ma X, Zhou L, et al. Dual-targeting TrxR-EGFR alkynyl-Au(I) gefitinib complex induces ferroptosis in gefitinib-resistant lung cancer via degradation of GPX4. J Med Chem. 2025;68(5):5275–5291. doi:10.1021/acs.jmedchem.4c02252
9. Yang JCH, Wu YL, Schuler M, et al. Afatinib versus cisplatin-based chemotherapy for EGFR mutation-positive lung adenocarcinoma (LUX-Lung 3 and LUX-Lung 6): analysis of overall survival data from two randomised, Phase 3 trials. Lancet Oncol. 2015;16(2):141–151. doi:10.1016/S1470-2045(14)71173-8
10. Shi Y, Chen G, Wang X, et al. Furmonertinib (AST2818) versus gefitinib as first-line therapy for Chinese patients with locally advanced or metastatic EGFR mutation-positive non-small-cell lung cancer (FURLONG): a multicentre, double-blind, randomised phase 3 study. Lancet Respir Med. 2022;10(11):1019–1028. doi:10.1016/S2213-2600(22)00168-0
11. Kobayashi IS, Shaffer W, Viray H, et al. The impact of on-target resistance mediated by EGFR-T790M or EGFR-C797S on EGFR exon 20 insertion mutation active tyrosine kinase inhibitors. JTO Clin Res Rep. 2024;5(1):100614. doi:10.1016/j.jtocrr.2023.100614
12. Laudadio E, Mangano L, Minnelli C. Chemical Scaffolds for the clinical development of mutant-selective and reversible fourth-generation EGFR-TKIs in NSCLC. ACS Chem Biol. 2024;19(4):839–854. doi:10.1021/acschembio.4c00028
13. Yang G, Li J, Xu H, et al. EGFR exon 20 insertion mutations in Chinese advanced non-small cell lung cancer patients: molecular heterogeneity and treatment outcome from nationwide real-world study. Lung Cancer. 2020;145:186–194. doi:10.1016/j.lungcan.2020.03.014
14. Okuma Y, Kubota K, Shimokawa M, et al. First-line osimertinib for previously untreated patients with NSCLC and uncommon EGFR mutations: the UNICORN phase 2 nonrandomized clinical trial. JAMA Oncol. 2024;10(1):43–51. doi:10.1001/jamaoncol.2023.5013
15. Sa H, Shi Y, Ding C, et al. A real-world study of the efficacy and safety of furmonertinib for patients with non-small cell lung cancer with EGFR exon 20 insertion mutations. J Cancer Res Clin Oncol. 2023;149(10):7729–7742. doi:10.1007/s00432-023-04726-x
16. Xu Y, Chen M, Gao X, et al. Efficacy and safety of sunvozertinib monotherapy as first-line treatment in NSCLC patients with EGFR exon 20 insertion mutations: a phase 2, single-center trial. Cancer Lett. 2025;630:217904. doi:10.1016/j.canlet.2025.217904
17. Dorta-Suárez M, de Miguel M, Amor-Carro O, et al. The state of the art of EGFR exon 20 insertions in non-small cell lung cancer: diagnosis and future perspectives. Cancer Treat Rev. 2024;124:102671. doi:10.1016/j.ctrv.2023.102671
18. Zwierenga F, van Veggel BAMH, van den Berg A, et al. A comprehensive overview of the heterogeneity of EGFR exon 20 variants in NSCLC and (pre)clinical activity to currently available treatments. Cancer Treat Rev. 2023;120:102628. doi:10.1016/j.ctrv.2023.102628
19. Pacini L, Jenks AD, Vyse S, et al. Tackling drug resistance in EGFR exon 20 insertion mutant lung cancer. Pharmacogenomics Pers Med. 2021;14:301–317.
20. Geng D, Guo Q, Huang S, et al. Clinical and molecular characteristics of epidermal growth factor receptor exon 20 insertion mutations in non-small-cell lung cancer. Clin Transl Oncol. 2022;24(2):379–387. doi:10.1007/s12094-021-02701-x
21. Wang M, Yang JCH, Mitchell PL, et al. Sunvozertinib, a selective EGFR inhibitor for previously treated non–small cell lung cancer with EGFR exon 20 insertion mutations. Cancer Discov. 2022;12(7):1676–1689. doi:10.1158/2159-8290.CD-21-1615
22. Dhillon S. Sunvozertinib: first Approval. Drugs. 2023;83(17):1629–1634. doi:10.1007/s40265-023-01959-5
23. Wang M, Fan Y, Sun M, et al. Sunvozertinib for patients in China with platinum-pretreated locally advanced or metastatic non-small-cell lung cancer and EGFR exon 20 insertion mutation (WU-KONG6): single-arm, open-label, multicentre, phase 2 trial. Lancet Respir Med. 2024;12(3):217–224. doi:10.1016/S2213-2600(23)00379-X
24. Wu CP, Li YC, Murakami M, et al. Furmonertinib, a third-generation EGFR tyrosine kinase inhibitor, overcomes multidrug resistance through inhibiting ABCB1 and ABCG2 in cancer cells. Int J Mol Sci. 2023;24(18):13972. doi:10.3390/ijms241813972
25. Han B, Zhou C, Wu L, et al. 1210P preclinical and preliminary clinical investigations of furmonertinib in NSCLC with EGFR exon 20 insertions (20ins). Ann Oncol. 2021;32:S964. doi:10.1016/j.annonc.2021.08.1815
26. FDA grants breakthrough therapy designation to furmonertinib for EGFR exon 20 insertion+ NSCLC. 2025.
27. Zhang X, Han H, Zhao J, et al. Case report: a good response to furmonertinib second-line treatment of an advanced lung adenocarcinoma patient with a rare EGFR exon 20 N771_P772insH mutation: a case report and literature review. Front Pharmacol. 2022;13:964606. doi:10.3389/fphar.2022.964606
28. Zhou C, Ramalingam SS, Kim TM, et al. Treatment outcomes and safety of mobocertinib in platinum-pretreated patients with EGFR exon 20 insertion-positive metastatic non-small cell lung cancer: a Phase 1/2 open-label nonrandomized clinical trial. JAMA Oncol. 2021;7(12):e214761. doi:10.1001/jamaoncol.2021.4761
29. Piotrowska Z. Making progress along the challenging road of drug development for patients with EGFR exon 20 insertion-positive non-small cell lung cancer. J Clin Oncol. 2025;43(13):1523–1526. doi:10.1200/JCO-24-02656
30. Sabari JK, Girard N, Mansfield AS, et al. Plain language summary of PAPILLON: amivantamab plus chemotherapy in untreated EGFR-mutated non-small-cell lung cancer. Future Oncol. 2024;20(32):2409–2421. doi:10.1080/14796694.2024.2371698
31. Piotrowska Z, Tan DSW, Smit EF, et al. Safety, tolerability, and antitumor activity of zipalertinib among patients with non-small-cell lung cancer harboring epidermal growth factor receptor exon 20 insertions. J Clin Oncol. 2023;41(26):4218–4225. doi:10.1200/JCO.23.00152
32. Piotrowska Z, Wang Y, Sequist LV, Ramalingam SS. ECOG-ACRIN 5162: a phase II study of osimertinib 160 mg in NSCLC with EGFR exon 20 insertions. J Clin Oncol. 2025;38(15_suppl):9513. doi:10.1200/JCO.2020.38.15_suppl.9513
33. Zwierenga F, van Veggel B, Hendriks LEL, et al. High dose osimertinib in patients with advanced stage EGFR exon 20 mutation-positive NSCLC: results from the phase 2 multicenter POSITION20 trial. Lung Cancer. 2022;170:133–140. doi:10.1016/j.lungcan.2022.06.012
34. Park, Keunchilet al Amivantamab in EGFR exon 20 insertion-mutated non-small-cell lung cancer progressing on platinum chemotherapy: initial results from the CHRYSALIS Phase I study - PubMed Journal of Clinical Oncology. 2021 39, 3391-3402 DOI:10.1200/JCO.21.00662.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Crossing the River by Feeling the Stones: Experiences with PD-1 Inhibitors in Geriatric Oncology People, a Case Report and Literature Review
Yin H, Zhang X, Zhang M, Tang H, Zhang C, Li J
Cancer Management and Research 2024, 16:87-93
Published Date: 5 February 2024
Simultaneous Anti-Tuberculosis and Anti-Tumor Treatment with Immune Checkpoint Inhibitors for Co-Existent Pulmonary Tuberculosis and Advanced Lung Cancer
Wang H, Gao L, Cai X, Li J, Lang Y, Zheng R, Yang S
Infection and Drug Resistance 2025, 18:107-112
Published Date: 6 January 2025