Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
Cariprazine on Psychosis: Beyond Schizophrenia – A Case Series
Received 27 December 2021
Accepted for publication 26 May 2022
Published 5 July 2022 Volume 2022:18 Pages 1351—1362
DOI https://doi.org/10.2147/NDT.S355941
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Miguel Bajouco,1– 3 David Mota1,2
1Department of Psychiatry, Centro Hospitalar e Universitário de Coimbra, Coimbra, Portugal; 2Institute of Psychological Medicine, Faculty of Medicine, University of Coimbra, Coimbra, Portugal; 3Coimbra Institute for Biomedical Imaging and Translational Research (CIBIT), University of Coimbra, Coimbra, Portugal
Correspondence: Miguel Bajouco, Department of Psychiatry, Centro Hospitalar e Universitário de Coimbra, Coimbra, Portugal, Tel +351 239 400 454, Email [email protected]
Abstract: Cariprazine is an atypical antipsychotic that has D2 and D3 partial agonism properties in addition to the usual 5-HT2A receptor antagonist action of second-generation antipsychotics. It has a distinctly higher affinity for D3 receptors, which is 10-fold higher than for D2 receptors. Cariprazine is also a 5-HT1A partial agonist, with a potential antidepressant effect. Cariprazine has been approved for treatment of both positive and negative symptoms of schizophrenia and for treatment of bipolar disorder. It could potentially be used in depression as an add-on treatment. There are few data reporting effectiveness of cariprazine in the broader spectrum of psychosis. In this paper, the authors report three cases where cariprazine was used in the treatment of psychotic conditions other than schizophrenia, namely a first episode psychosis, a case of delusional disorder, and a case of a patient with borderline personality disorder and psychotic symptoms. The authors suggest that cariprazine may be effective in the treatment of psychosis in a broader sense and should be considered a first-line treatment option.
Keywords: antipsychotic treatment, borderline personality disorder, cariprazine, delusional disorder, first-episode psychosis, psychosis, schizophrenia spectrum disorders, tolerability
Introduction
Psychotic disorders are a heterogeneous group of mental disorders characterized by delusions and/or hallucinations, affecting up to 3.4% of the population over a lifetime and having an estimated crude incidence of 21.4 per 100,000 person-years.1–3 They are amongst the most severe psychiatric disorders, spanning from schizophrenia and related disorders to bipolar disorder and severe forms of depressive disorders. Notwithstanding the importance of non-pharmacological interventions like cognitive-behavioral therapy and psychoeducation, antipsychotics are considered the mainstay of treatment for psychotic disorders. First-generation antipsychotics (FGA) and second generation antipsychotics (SGA) show equivalent efficacy but SGAs are better tolerated since they are relatively free of typical FGA side-effects like extrapyramidal symptoms or tardive dyskinesia.4 Nonetheless, SGAs are associated with metabolic side-effects such as weight gain and diabetes, leading to increased risk cardiovascular complications.5 Moreover, although antipsychotics with D2 receptor antagonism are effective in controlling positive symptoms they have a lower impact on other symptoms, namely negative symptoms, the latter significantly impacting functional outcomes.6 Newer SGAs like aripiprazole, brexipiprazole, and cariprazine are dopamine D2 receptor partial agonists. and have the advantage of causing less metabolic side-effects than other SGAs while potentially improving negative symptoms and cognitive function.7 A unique feature of partial agonists is that they elicit differential activities depending on the environment: they block receptors in the presence of agonists with higher intrinsic activity but themselves act as agonists. This property of the D2 partial agonists accounts for improvement of psychotic symptomatology with little or no adverse effects, such as extrapyramidal symptoms or hyperprolactinemia.8
Cariprazine receptor profile includes partial agonism of D2 and D3 receptors with preferential binding to D3 over D2 receptors and also moderate histamine antagonism, low alfa-1a antagonism, and no significant affinity for muscarinic cholinergic receptors.9 Cariprazine is metabolized by CYP3A4 and to a lesser extent by CYP2D6 into two clinically relevant metabolites: desmethyl-cariprazine and didesmethyl-cariprazine, the latter having a longer half-life than cariprazine. Exposure to didesmethyl-cariprazine exceeded that of the parent drug. The long-life of this clinical active metabolite allows a once-a-day formulation and accounts for a lower risk of symptom exacerbation when a dose is missed when compared with shorter half-life drugs.9
Cariprazine is approved in the European Union, the US, and Canada for the treatment of schizophrenia and in the US and Canada for bipolar disorder, and it has been shown to be effective in acute mania.10–12 It has also been shown to be effective in the treatment of unipolar depression due to its antidepressant effect.13 In schizophrenia, cariprazine has proved to be effective not only in the treatment of positive symptoms but also of negative symptoms, being the only antipsychotic to effectively tackle the latter, to date.14 Like other partial dopamine receptor agonists it has a low incidence of side-effects which are usually related to antipsychotic treatment, such as extrapyramidal effects, hyperprolactinemia and galactorrhea, sedation and metabolic syndrome, as well as having a low impact on sexual function.15,16 The most common side-effects are akathisia and insomnia.17
Although the use of cariprazine in the treatment of schizophrenia and affective psychosis is already supported by substantial evidence, there is only limited data documenting its effectiveness in other psychotic conditions such as persistent delusional disorder or the first episode psychosis18,19 and in psychotic symptoms associated with borderline personality disorder.20
The first episode psychosis (FEP) is a critical life event that typically emerges during the sensitive developmental period of late adolescence and early adulthood. It has a significant impact on the individual’s life trajectory due to the cognitive, emotional, and behavioral dysfunction that implies, which significantly impacts social and occupational domains. Birchwood et al21 proposed the concept of a “critical period”, corresponding to the first 2–5 years after the first episode, considered an early phase where disability and long-term trajectories are formed. This concept provided the rationale of a new care paradigm for psychosis that emerged in the 1990s, focused on the early detection and specialized intervention with a goal of improving the early outcome for psychosis following the first episode.22 To prevent new psychotic episodes during the critical period, current consensus indicates that antipsychotics should be prescribed for 1–2 years after the first episode psychosis as follow-up studies showed that withdrawing antipsychotic treatment earlier led to a relapse rate of up to 75% within 12–18 months.23–25 A major cause of relapse, hospitalization, and increased risk of suicide after a first episode psychosis is non-adherence to antipsychotic treatment.26 Although non-adherence has many causes, lack of efficacy or poor tolerability of medication are modifiable factors which can be overcome by carefully considering the antipsychotic profile that most suits each patient.
Delusional disorder is a relatively rare psychotic illness, with a population prevalence around 0.03%.27 It is characterized by non-bizarre delusions with a plausible and possible content, as well as an absence of disorganized thought and negative symptoms characteristic of schizophrenia and deterioration. Hallucinations may be present at the beginning of the illness but are not dominant and are almost always absent during the whole course of the illness.28 Patients typically have a profound lack of insight and often avoid psychiatric care and antipsychotics. Antipsychotics represent the core of treatment, although lack of insight and nonadherence to treatment typically limit success, and it remains unclear whether certain agents are more effective than others.
A psychiatric condition usually less associated with psychotic symptoms is borderline personality disorder (BPD). BPD is conceptualized as a pervasive pattern of instability of interpersonal relationships, self-image, and affects, and marked impulsivity that begins by early adulthood and is present in a variety of contexts.29 Psychotic features in BPD are a long-known phenomenon. In fact, the name of the disorder itself was originally meant to describe patients who seemed to be on the border between neurosis and psychosis.30 Although current diagnostic criteria are mostly focused in emotional dysregulation or related features,29 it is estimated that 20–50% of patients with BPD experience psychotic symptoms.31 Psychotic symptoms in patients with BPD can broadly be divided into perceptual abnormalities and paranoid ideation, but there is currently no consensus on the phenomenology and severity of these experiences.31 Clinical definitions and operational diagnostic criteria suggest psychotic symptoms in BPD are usually transient or pseudo-psychotic and stress-related. However, studies examining the nature of these symptoms show that a significant proportion of BPD patients experience auditory verbal hallucinations similar to schizophrenia or longer-lasting paranoid episodes.31,32 The existing findings give moderate support to the use of atypical antipsychotics in BPD patients with psychotic symptoms,33 but there is a need for further studies on the efficacy of antipsychotics and other interventions in such clinical situations.
Here the authors report three cases of successful treatment with cariprazine in three non-schizophrenic psychotic disorders, one of a young patient with first episode psychosis, another of an elder patient with persistent delusional disorder, and finally a case of a patient with BPD presenting with psychotic symptoms.
Description of Cases
Case 1: First Episode Psychosis
JC, a 22-year-old male patient, was referred to our Early Intervention in Psychosis (EIP) team by his General Practitioner (GP) doctor. At the first appointment in May 2021, he reported that, since the beginning of the year, he progressively developed persistent feelings of sadness, a tendency to isolation, a decay in self-care, loss of appetite, significant weight-loss, and suicidal ideation without a clear-cut plan. During the psychiatric assessment, in the context of exploring the occurrence of significant life-events and experiences that could have contributed to these symptoms and functional impairment, the patient initially associated his emotional and behavioral manifestations to the COVID-19 pandemic confinement. However, he then stated
I have lost control over my life in the last 5 months … they are constantly giving me instructions and putting me down … I can hear them all the time, even when I am alone! That’s why I feel nervous and sad about my life.
He then went on to describe the presence of distressing auditory-verbal hallucinations, mainly in the form of second person voices making depreciative comments and commanding him. Furthermore, he presented non-systematized persecutory delusions involving friends and colleagues and self-referential delusions of erotomaniac content about a famous rap singer, who allegedly sent him messages about their relationship through the lyrics of his songs. He also mentioned that a photo was published in a social network in which apparently both he and the famous rap singer appeared together, although he then admitted they had never been close to each other in any situation. Along with these psychotic symptoms, he developed symptoms of avolition with reduced interest in spending time with family or friends or performing pleasurable activities, leading to progressive social withdrawal. His academic performance was also impaired, having stopped attending university classes of the Management degree not only because of feeling suspicious about his colleagues but also because he was unable to maintain attention and concentration during classes.
A month before the first appointment with the EIP team, one of his close friends convinced him to have a consultation with his GP who prescribed him Risperidone 3 mg. According to his GP the patient presented a good clinical response with a reduction of psychotic symptoms, but developed significant side-effects of somnolence, bradykinesia, superior limb pill-rolling tremor, and hypotension. As a result, the patient decided to stop the treatment after a week. This led to worsening of the psychotic symptoms, and he reported that, during the week before the initial EIP assessment, ”the voices were telling me I did not deserve to live and were telling me to harm myself”.
During our observation, we performed a psychometric evaluation using the Positive and Negative Symptom Scale (PANSS)34 and the Global Clinical Impression–Severity (CGI-S)35 scale for symptom and clinical assessment and the Personal and Social Performance scale (PSP)36 for functional assessment. The PANSS total score was 94 (Positive subscale =24; Negative subscale =26; General Psychopathology subscale =44), CGI-S global severity score was 5 (Markedly ill), and the PSP score was 45.
In terms of use of psychoactive substances, the patient acknowledged smoking cannabinoids daily since he went to university until 2 weeks before the initial appointment.
The patient did not have a personal history of psychiatric illness beyond the current episode. Family history of mental illness was also not identified.
Diagnostic workup to exclude non-psychiatric etiology of the described symptoms involved blood tests (general biochemistry, hemogram, coagulation, vitamin B12, folic acid, TSH, T4, autoimmunity panel), cranial CT, and EEG. All the complementary studies returned normal results.
Although the patient showed only partial insight into the pathological nature of his psychotic experiences, he was willing to try a new treatment given the significant distress caused by the symptoms. Therefore, cariprazine was prescribed in a rapid titration scheme up to 4.5 mg/day.
A follow-up evaluation was performed after 6 weeks. At that point the patient presented global remission of psychotic symptoms “the voices stopped … my thoughts are clearer, and I can focus”. When screened for possible treatment side-effects he denied having any “it seems almost as I’m not taking any medication”. He also exhibited improvement of his mood and emotions and reported having started to spend more time with family members and friends, doing physical exercise, and undertaking driving lessons for getting a license as a long-haul driver. This remarkable clinical and functional improvement was mirrored in the psychometric assessment, with a reduction of the PANSS total score to 50 (Positive subscale =10; Negative subscale =14; General Psychopathology subscale =25), a CGI-S score of 3 (Mildly ill), and a PSP score of 81 (Table 1).
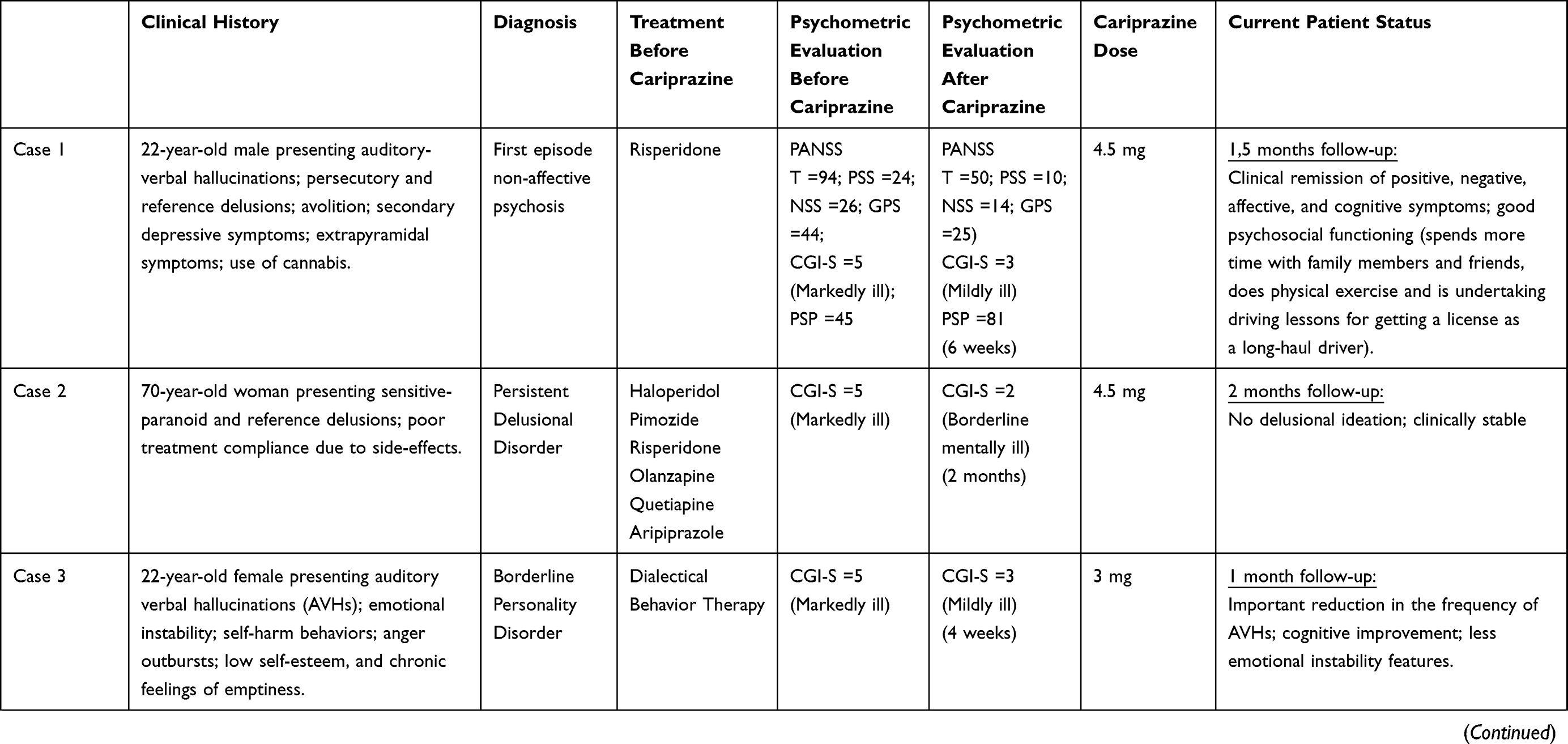 | 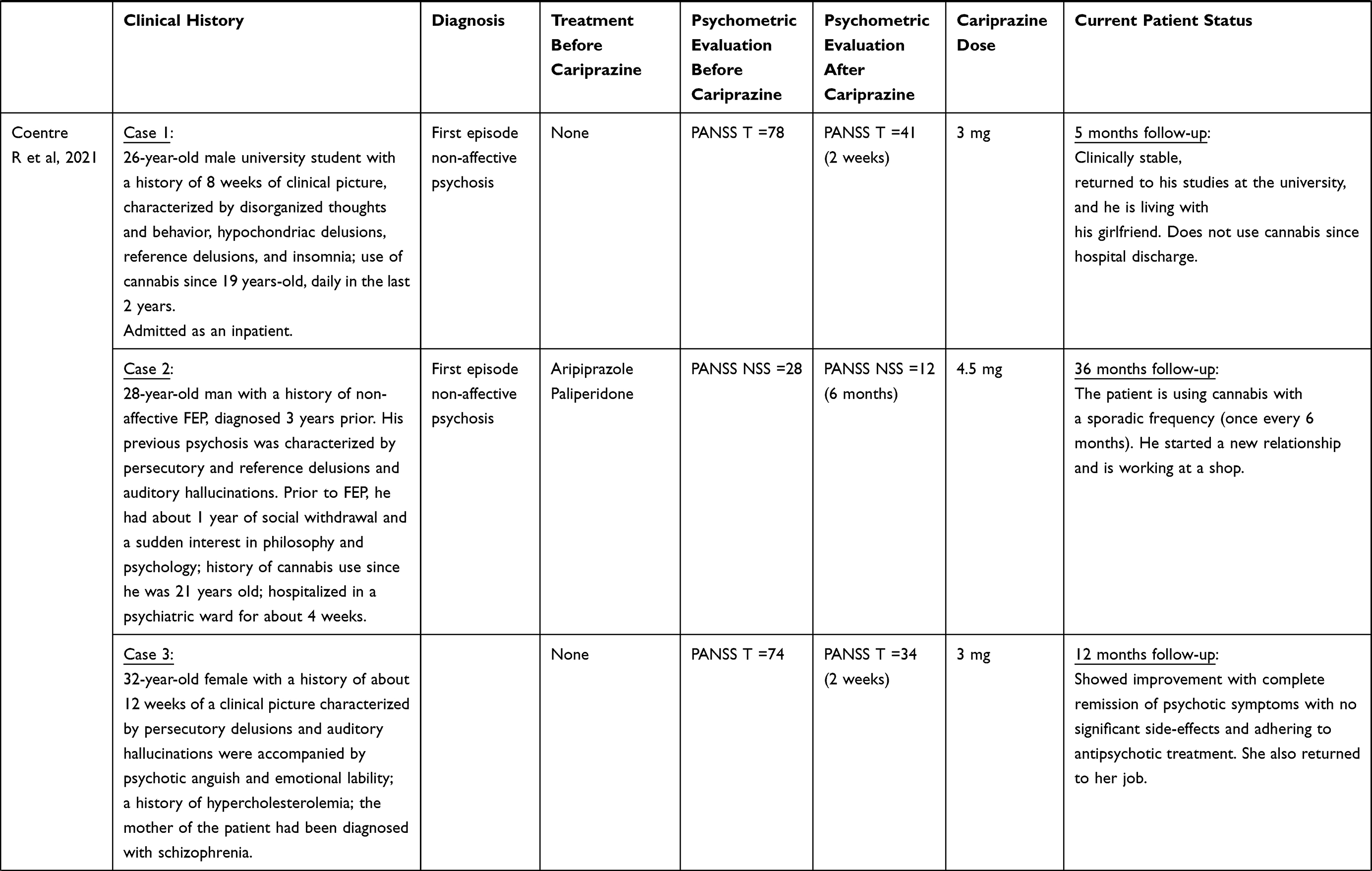 | 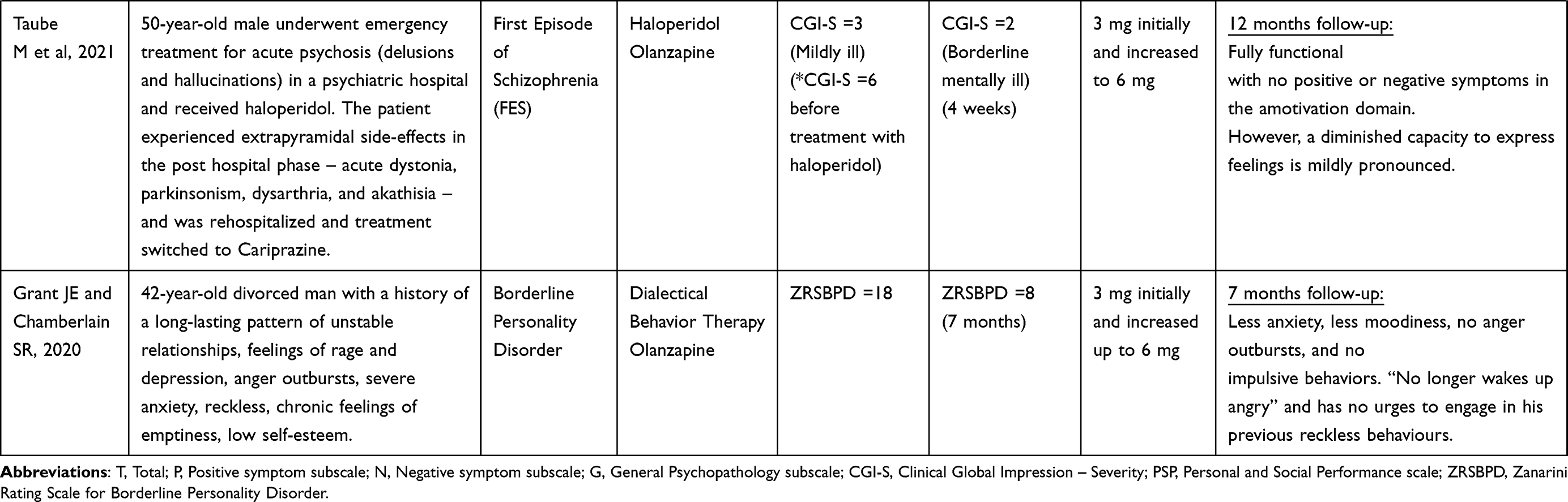 |
Table 1 | Summary of Clinical Cases and Comparison with Other Case-Reports |
Case 2: Persistent Delusional Disorder
The patient was a 70-year-old woman diagnosed with Persistent Delusional Disorder in 1977. She graduated as a medical doctor in 1975. The disease history started during her general residency year. The patient did not have any previous psychiatric history. She was raised in a strict conservative education and was married before graduating. She also had personality traits of sensitiveness, shyness, and rigidity of thought, with low openness to experience. The patient developed a sensitive-paranoid delusion during her general residency year after receiving a compliment from the ward director in a clinical meeting. After that episode, she started to worry about the possibility that her colleagues may think that she was having an affair with the director. These worries evolved quickly to a firm conviction that all her colleagues thought and gossiped about an affair between her and the ward director. The patient told her husband about these beliefs, and, after that, they consulted a psychiatrist who diagnosed her with a Delusional Disorder, sensitive-paranoid type. The patient never had other psychopathological phenomena, such as hallucinations or formal thought disorder. She has been functional in both professional and personal domains. She had and raised two children and specialized in Pathological Anatomy and worked in clinical and academic settings. Despite this, she has had some exacerbations from time to time that happened in different places where she worked, with different colleagues being the object of her delusion. She retired in 2013 and has been living in a small village with her husband since then. Between 1977 to 2018, she was treated with different oral antipsychotics such as haloperidol, pimozide, risperidone, olanzapine, and aripiprazole. Adherence to treatment was sparse, lasting only short periods of time, abandoning medication frequently due to self-perceived side-effects and subjective cognitive impairment, especially with first generation antipsychotics. From 2013 to 2018 she maintained treatment with aripiprazole 10 mg daily, considering that was the most well tolerated antipsychotic she had been prescribed with. However, in 2018 she stopped aripiprazole due to developing akathisia after a dose increment to 15 mg/day. She remained free of medication between 2018 and June 2020. In the beginning of 2020, she started a new relapse, developing the delusional belief that people of her village gossiped about her having an affair with a neighbor. She started to isolate herself at home, developing a reactive depressive episode with retardation, self-neglect, isolation, and emotional lability. She consulted a psychiatrist again because of the depressive symptoms. A detailed clinical history was collected at the appointment, confirming her previous diagnosis. The patient was very reluctant to start a new treatment with an antipsychotic due to her previous negative experiences. Treatment with cariprazine was proposed due to its similarity with aripiprazole, its established effectiveness in treating other psychotic disorders such as schizophrenia, its procognitive effect and, finally, its antidepressant effect. The patient accepted treatment with cariprazine and started with 3 mg daily in June 2020. She was evaluated in a new appointment after 1 month, showing important improvement of her clinical condition with resolution of depressive symptoms and with softening of her delusional beliefs and some insight improvement. Cariprazine dose was increased to 4.5 mg daily. The patient was assessed again in the following month. In this evaluation her delusional beliefs had nearly resolved, with a minor impact in her life. Accordingly, the CGI-S global severity dropped from a score of 5 (Markedly ill) before starting cariprazine to a score of 2 (Borderline mentally ill) after 2 months of treatment (Table 1). She tolerated cariprazine very well with no mention of side-effects, remaining stable since then.
Case 3: Borderline Personality Disorder
MC, a 21-year-old university law student, came to a first appointment at a private psychiatric outpatient clinic referred by her psychologist who followed her for a clinical picture of borderline personality disorder. She reported having difficulties in maintaining concentration during classes as her attention was diverted by frequent experiences of “voices of other people making negative comments about me”, compatible with auditory verbal hallucinations (AVH). Although AVHs first presented when MC was 16 years, they were not continuous, and their intensity was higher during periods of greater anxiety. Nonetheless, MC had good insight to these phenomena, recognizing “they sound real, but I know they are a product of my head”. In addition, MC referred sometimes to having thoughts that “other people are saying bad things about me”, especially when those people do not give her the attention, she considers necessary, perceiving their attitude as they are abandoning her when she most needs. This in turn leads to feelings of rage and depression as well as anger outbursts that often result in loss of friendships or the end of relationships. MC describes that when relationships come to an end, she is “filled with overwhelming emotional pain” which only has some relief when she performs self-harm behaviors like doing small cuts on her arms. She recognized placing high expectations in relationships and becoming enamored of people very quickly and very intensely as a way of dealing with her low self-esteem and chronic feelings of emptiness that have been present for as long as she could remember.
Psychiatric assessment concluded that the patient met the DSM-5 criteria for BPD. Differential diagnosis included major depressive disorder with mixed features, bipolar disorder, and schizophrenia spectrum disorders. The first two diagnostic hypothesis were ruled out as the pattern of interpersonal problems that MC described was longstanding and the mood symptoms were triggered by interpersonal conflicts. Schizophrenia and related disorders were excluded since, beyond AVHs, other symptoms necessary to meet diagnostic criteria were not present and AVHs were not present continuously or reached a duration threshold for diagnosis. Moreover, use of psychoactive substances was denied by the patient and therefore a diagnosis of substance-induced psychosis as an explanation for the occurrence of AVHs was excluded. Diagnostic hypothesis of a comorbid psychotic disorder due to a medical condition was excluded since symptoms or signs of systemic disease were absent.
At the time of presentation, MC was not under any pharmacological treatment. Ongoing treatment included individual third generation cognitive-behavioral psychotherapy (dialectical behavioral therapy) started 1 year before. The patient acknowledged having acquired more adequate coping strategies to deal with periods of intense negative emotional states, reporting that self-harm behaviors now occurred very rarely. However, she described still having significant emotional fluctuation and no improvement in what was concerned with the frequency or impact of AVHs. Treatment with cariprazine 3 mg once every day was prescribed. A month later, MC reported an important reduction in the occurrence of AVHs, allowing her to concentrate better during university classes. In addition, she described having less moodiness and no anger outbursts. This meant a reduction of the CGI-S global severity from a score of 5 (Markedly ill) before starting cariprazine to a score of 3 (Mildly ill) after 4 weeks of treatment (Table 1). Cariprazine was well tolerated as MC denied any adverse effect.
Discussion
Psychotic disorders have different clinical presentations. Nonetheless, positive, negative, affective, and cognitive symptoms are frequently present, although their preponderance may vary. Consequently, treatment approaches to any psychotic disorder must consider the need to target different types of symptoms. Cariprazine’s unique pharmacological profile makes it a multimodal antipsychotic with an efficacy that extends beyond psychotic symptoms per se, also improving negative, cognitive, and depressive symptoms, allowing to optimize treatment response.14,37 This broad therapeutic effect that reaches different symptoms may be important to create a positive impression of treatment which will eventually favor adherence.38
In the case of the patient with first-episode psychosis, cariprazine did not only improve positive symptoms but also negative, cognitive, and depressive symptoms. This efficacy on negative and cognitive symptoms has been associated with partial agonism and greater affinity for D3 over D2 receptors, which is a distinctive mechanism of cariprazine amongst other D2 partial agonists.39 In addition, notwithstanding that reduction of psychotic symptoms may have ameliorated the affective state, we can also hypothesize that the drug’s affinity with 5HT1A receptors also contributed to improving the patient’s mood.40 This treatment outcome is in agreement with previous trials and meta-analyses that demonstrated the efficacy of cariprazine in acute exacerbations of schizophrenia, with improvement of the PANSS total score, positive and negative subscale scores, and CGI score.41–43
Tolerability must also be considered a key determinant in the choice of treatment in the early stages of psychotic disorders as it appears to significantly influence adherence, which in turn exerts a fundamental role in the course of these disorders.44,45 Similarly to a recent case report,19 in case 1, cariprazine was as effective but without the side-effects caused by the antipsychotic drug previously used, restoring the patient’s trust in treatment, which can be crucial for a successful treatment outcome (Table 1). In agreement, a recent case series reported the use of cariprazine in early psychosis, showing that low doses of cariprazine were effective in treating positive and negative symptoms in FEP patients and were well tolerated. This is significant since FEP patients are drug-naïve and are usually sensitive to antipsychotic side-effects. Therefore, cariprazine’s effectiveness and tolerability make it an ideal drug in FEP, when the choice of first treatment can determine the course of the illness and treatment adherence.
Delusional disorder is a generally difficult to treat condition, mostly due to poor patient insight and consequent nonadherence to treatment. On the other hand, there is a lack of evidence-based treatment which sometimes makes the medical choice difficult. In fact, the available literature concerning treatment of delusional disorder is limited mostly to case reports and small case series.46 Antipsychotics are usually the treatment of choice, with about 35% responding.47 Older literature suggests that this condition responds better to specific types of antipsychotics, such as pimozide or haloperidol. However, most recent evidence points out that all antipsychotics are equally effective.48 There are several reports of delusional disorder successful treatment with atypical antipsychotics such as risperidone,49 olanzapine,50 paliperidone,51 and aripiprazole.52 In addition, there are some reports of successful treatment with selective serotonin reuptake inhibitors (SSRIs) and clomipramine in monotherapy or in association with atypical antipsychotics, as some serotoninergic deficit may be involved in delusional disorder.53 Noticeably, cariprazine also increases serotonin signaling in 5-HT1A receptors, suggesting why it may have a positive effect in this conditions improvement. To our knowledge, there are no other previous reports of delusional disorders treated with cariprazine. We chose cariprazine due to its antipsychotic action, to patient’s previous good response to antipsychotics, to its similarity with aripiprazole (the best tolerated antipsychotic by this patient before), less potential side-effects than other antipsychotics used by the patient in the past which compromised adherence to treatment, and to its well documented antidepressant effect (the patient had also depressive symptoms secondary to psychotic symptoms). Our patient had a dramatic improvement after treatment with cariprazine, showing no side-effects, maintaining to date adherence to treatment and clinical gains. Therefore, we think that cariprazine should be considered the treatment of choice for delusional disorder.
In the third clinical case, the effectiveness of cariprazine in controlling auditory verbal hallucinations in the context of BPD suggests it merits consideration as a valid treatment option for psychotic symptoms associated with BPD. Moreover, in agreement with a recent case report,20 cariprazine has shown a potential benefit in improving the typical emotional dysregulation and behavioral features of BPD.
Although the neurobiology of BPD is not well understood, it appears to involve dysfunctions in the serotoninergic and dopaminergic systems.54,55 Partial agonism at the dopamine D2 and D3 receptors and serotonin 5-HT1A receptor places cariprazine in a pivotal position to improve both psychotic symptoms and symptoms in the spectrum of emotional instability of BPD.
Overall, the three cases reported demonstrate the efficacy of cariprazine, not only in inducing remission of psychotic symptoms but also of other clusters of symptoms. Importantly all three patients recovered their functioning to normal levels. Tolerability was also remarkably favorable in the three clinical cases. Akathisia, the most frequent side-effect associated with cariprazine as well as anticholinergic, anti-adrenergic, antihistaminergic, and metabolic side-effects commonly caused by antipsychotics were not observed. This lower propensity for extrapyramidal and metabolic side-effects of cariprazine has been proposed to be a result from its distinct receptor binding properties of partial agonism at dopamine D2/D3 receptors, preferential binding to D3 receptors, and partial agonism at serotonin 5-HT1A receptors.7 Such a favorable global profile makes cariprazine an advantageous option for treatment of psychotic disorders.
Conclusion
Our three clinical cases showed the effectiveness of cariprazine in psychotic conditions other than schizophrenia with an excellent tolerability. Therefore, cariprazine should be considered for treatment of psychotic conditions in a broader sense, beyond schizophrenia. We emphasize that the promising findings reported here must be confirmed in additional studies performed in a larger number of patients.
Abbreviations
US, United States; 5-HT, serotonin receptor; D, dopamine receptor; mg, milligram; PANSS, Positive and Negative Syndrome Scale; GCI-S, Clinical Global Impressions Scale; PSP, Personal and the Social Performance Scale; ECG, electrocardiogram; EEG, electroencephalography; TSH, Thyroid Stimulant Hormone; T4, Thyroxine; BPD, Borderline Personality Disorder; LAI, Long Acting Injectable; FGA, First Generation Antipsychotic; SGS, Second Generation Antipsychotic; FEP, First Episode Psychosis; EIP, Early Intervention in Psychosis; GP, General Practitioner; CT, Cranial Tomography; COVID-19, Coronavirus Disease 2019; AVH, auditory verbal hallucinations; DSM-5, Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition.
Consent for Publication
Publication of this case series was granted institutional approval by Centro Hospitalar e Universitário de Coimbra, following ethical review by the local Ethics Committee. Patients provided written informed consent for publication.
Author Contributions
Both authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Recordati provided financial support for the writing of the manuscript and the open access fee for publication.
Disclosure
Dr Miguel Bajouco has served as consultant, advisor, or speaker for Recordati, Janssen-Cilag, Lundbeck and Bial. Dr David Mota has served as advisor or speaker for Recordati, Janssen-Cilag and Angelini. The authors report no other conflicts of interest in this work.
References
1. Maj M, van Os J, De Hert M, et al. The clinical characterization of the patient with primary psychosis aimed at personalization of management. World Psychiatry. 2021;20(1):4–33. doi:10.1002/wps.20809
2. Perälä J, Suvisaari J, Saarni SI, et al. Lifetime prevalence of psychotic and bipolar I disorders in a general population. Arch Gen Psychiatry. 2007;64(1):19–28. doi:10.1001/archpsyc.64.1.19
3. Jongsma HE, Gayer-Anderson C, Lasalvia A, et al. Treated incidence of psychotic disorders in the multinational EU-GEI study. JAMA Psychiatry. 2018;75(1):36–46. doi:10.1001/jamapsychiatry.2017.3554
4. Kahn RS, Fleischhacker WW, Boter H, et al. Effectiveness of antipsychotic drugs in first-episode schizophrenia and schizophreniform disorder: an open randomised clinical trial. Lancet. 2008;371(9618):1085–1097. doi:10.1016/S0140-6736(08)60486-9
5. Leucht S, Cipriani A, Spineli L, et al. Comparative efficacy and tolerability of 15 antipsychotic drugs in schizophrenia: a multiple-treatments meta-analysis. Lancet. 2013;382(9896):951–962. doi:10.1016/s0140-6736(13)60733-3
6. Fusar-Poli P, Papanastasiou E, Stahl D, et al. Treatments of negative symptoms in schizophrenia: meta-analysis of 168 randomized placebo-controlled trials. Schizophr Bull. 2015;41(4):892–899. doi:10.1093/schbul/sbu170
7. Orsolini L, De Berardis D, Volpe U. Up-to-date expert opinion on the safety of recently developed antipsychotics. Expert Opin Drug Saf. 2020;19(8):981–998. doi:10.1080/14740338.2020.1795126
8. Garnock-Jones KP. Cariprazine: a review in schizophrenia. CNS Drugs. 2017;31(6):513–525. doi:10.1007/s40263-017-0442-z
9. Citrome L. Cariprazine: chemistry, pharmacodynamics, pharmacokinetics, and metabolism, clinical efficacy, safety, and tolerability. Expert Opin Drug Metab Toxicol. 2013;9(2):193–206. doi:10.1517/17425255.2013.759211
10. Wesołowska A, Partyka A, Jastrzębska-Więsek M, Kołaczkowski M. The preclinical discovery and development of cariprazine for the treatment of schizophrenia. Expert Opin Drug Discov. 2018;13(8):779–790. doi:10.1080/17460441.2018.1471057
11. Yatham LN, Kennedy SH, Parikh SV, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) 2018 guidelines for the management of patients with bipolar disorder. Bipolar Disord. 2018;20(2):97–170. doi:10.1111/bdi.12609
12. Laszlovszky I, Barabássy Á, Németh G. Cariprazine, A broad-spectrum antipsychotic for the treatment of schizophrenia: pharmacology, efficacy, and safety. Adv Ther. 2021;38(7):3652–3673. doi:10.1007/s12325-021-01797-5
13. Durgam S, Earley W, Guo H, et al. Efficacy and safety of adjunctive cariprazine in inadequate responders to antidepressants: a randomized, double-blind, placebo-controlled study in adult patients with major depressive disorder. J Clin Psychiatry. 2016;77(3):371–378. doi:10.4088/JCP.15m10070
14. Németh G, Laszlovszky I, Czobor P, et al. Cariprazine versus risperidone monotherapy for treatment of predominant negative symptoms in patients with schizophrenia: a randomised, double-blind, controlled trial. Lancet. 2017;389(10074):1103–1113. doi:10.1016/S0140-6736(17)30060-0
15. Keks N, Hope J, Schwartz D, McLennan H, Copolov D, Meadows G. Comparative tolerability of dopamine D2/3 receptor partial agonists for schizophrenia. CNS Drugs. 2020;34(5):473–507. doi:10.1007/s40263-020-00718-4
16. Dieci M, Trama A, Mansi G. Resolution of citalopram sexual adverse effects with low dose of cariprazine: a case report. Clin Neuropharmacol. 2020;43(5):164–165. doi:10.1097/WNF.0000000000000409
17. Citrome L. Cariprazine for acute and maintenance treatment of adults with schizophrenia: an evidence-based review and place in therapy. Neuropsychiatr Dis Treat. 2018;14:2563–2577. doi:10.2147/NDT.S159704
18. Coentre R, Saraiva R, Sereijo C, Levy P. Cariprazine use in early psychosis: three case reports. Front Psychiatry. 2021;12:788281. doi:10.3389/fpsyt.2021.788281
19. Taube M. Case report: severe side effects following treatment with first generation antipsychotics while cariprazine leads to full recovery. Front Psychiatry. 2021;12:804073. doi:10.3389/fpsyt.2021.804073
20. Grant JE, Chamberlain SR. Cariprazine treatment of borderline personality disorder: a case report. Psychiatry Clin Neurosci. 2020;74(9):511–512. doi:10.1111/pcn.13094
21. Birchwood M, Todd P, Jackson C. Early intervention in psychosis. The critical period hypothesis. Br J Psychiatry Suppl. 1998;172(33):53–59. doi:10.1192/S0007125000297663
22. McGorry PD, Edwards J, Mihalopoulos C, Harrigan SM, Jackson HJ. EPPIC: an evolving system of early detection and optimal management. Schizophr Bull. 1996;22(2):305–326. doi:10.1093/schbul/22.2.305
23. American Psychiatric Association. The American Psychiatric Association Practice Guideline for the Treatment of Patients with Schizophrenia.
24. Correll CU, Rubio JM, Kane JM. What is the risk-benefit ratio of long-term antipsychotic treatment in people with schizophrenia? World Psychiatry. 2018;17(2):149–160. doi:10.1002/wps.20516
25. Kissling W. The current unsatisfactory state of relapse prevention in schizophrenic psychoses–suggestions for improvement. Clin Neuropharmacol. 1991;14(Suppl 2):S33–44.
26. Leucht S, Heres S. Epidemiology, clinical consequences, and psychosocial treatment of nonadherence in schizophrenia. J Clin Psychiatry. 2006;67(Suppl 5):3–8.
27. Kendler KS. Demography of paranoid psychosis (delusional disorder): a review and comparison with schizophrenia and affective illness. Arch Gen Psychiatry. 1982;39(8):890–902. doi:10.1001/archpsyc.1982.04290080012003
28. Muñoz-Negro JE, Ibáñez-Casas I, de Portugal E, Lozano-Gutiérrez V, Martínez-Leal R, Cervilla JA. A psychopathological comparison between delusional disorder and schizophrenia. Can J Psychiatry. 2018;63(1):12–19. doi:10.1177/0706743717706347
29. American Psychiatric Association. DSM-5 task force. In: Diagnostic and Statistical Manual of Mental Disorders: DSM-5.
30. Stern A. Psychoanalytic investigation of and therapy in the border line group of neuroses. Psychoanal Q. 1938;7(7):467–489. doi:10.1080/21674086.1938.11925367
31. Schroeder K, Fisher HL, Schäfer I. Psychotic symptoms in patients with borderline personality disorder: prevalence and clinical management. Curr Opin Psychiatry. 2013;26(1):113–119. doi:10.1097/YCO.0b013e32835a2ae7
32. Slotema CW, Daalman K, Blom JD, Diederen KM, Hoek HW, Sommer IE. Auditory verbal hallucinations in patients with borderline personality disorder are similar to those in schizophrenia. Psychol Med. 2012;42(9):1873–1878. doi:10.1017/S0033291712000165
33. Ingenhoven T, Lafay P, Rinne T, Passchier J, Duivenvoorden H. Effectiveness of pharmacotherapy for severe personality disorders: meta-analyses of randomized controlled trials. J Clin Psychiatry. 2010;71(1):14–25. doi:10.4088/jcp.08r04526gre
34. Kay SR, Fiszbein A, Opler LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull. 1987;13(2):261–276. doi:10.1093/schbul/13.2.261
35. US Department of Heath. Clinical Global Impressions. In: Guy W, editor. ECDEU Assessment Manual for Psychopharmacology. Education, and Welfare Public Health Service Alcohol, Drug Abuse, and Mental Health Administration. US Department of Heath; 1976:603.
36. Morosini PL, Magliano L, Brambilla L, Ugolini S, Pioli R. Development, reliability and acceptability of a new version of the DSM-IV Social and Occupational Functioning Assessment Scale (SOFAS) to assess routine social functioning. Acta Psychiatr Scand. 2000;101(4):323–329. doi:10.1111/j.1600-0447.2000.tb10933.x
37. Corponi F, Fabbri C, Bitter I, et al. Novel antipsychotics specificity profile: a clinically oriented review of lurasidone, brexpiprazole, cariprazine and lumateperone. Eur Neuropsychopharmacol. 2019;29(9):971–985. doi:10.1016/j.euroneuro.2019.06.008
38. Montes JM, Montes P, Hernández-Huerta D. Cariprazine in three acute patients with schizophrenia: a real-world experience. Neuropsychiatr Dis Treat. 2021;17:291–296. doi:10.2147/NDT.S298005
39. Calabrese F, Tarazi FI, Racagni G, Riva MA. The role of dopamine D. CNS Spectr. 2020;25(3):343–351. doi:10.1017/S109285291900083X
40. Earley W, Guo H, Daniel D, et al. Efficacy of cariprazine on negative symptoms in patients with acute schizophrenia: a post hoc analysis of pooled data. Schizophr Res. 2019;204:282–288. doi:10.1016/j.schres.2018.08.020
41. Durgam S, Cutler AJ, Lu K, et al. Cariprazine in acute exacerbation of schizophrenia: a fixed-dose, Phase 3, randomized, double-blind, placebo- and active-controlled trial. J Clin Psychiatry. 2015;76(12):e1574–82. doi:10.4088/JCP.15m09997
42. Kane JM, Zukin S, Wang Y, et al. Efficacy and safety of cariprazine in acute exacerbation of schizophrenia: results from an international, phase iii clinical trial. J Clin Psychopharmacol. 2015;35(4):367–373. doi:10.1097/JCP.0000000000000346
43. Corponi F, Serretti A, Montgomery S, Fabbri C. Cariprazine specificity profile in the treatment of acute schizophrenia: a meta-analysis and meta-regression of randomized-controlled trials. Int Clin Psychopharmacol. 2017;32(6):309–318. doi:10.1097/YIC.0000000000000189
44. Semahegn A, Torpey K, Manu A, Assefa N, Tesfaye G, Ankomah A. Psychotropic medication non-adherence and its associated factors among patients with major psychiatric disorders: a systematic review and meta-analysis. Syst Rev. 2020;9(1):17. doi:10.1186/s13643-020-1274-3
45. Verdoux H, Lengronne J, Liraud F, et al. Medication adherence in psychosis: predictors and impact on outcome. A 2-year follow-up of first-admitted subjects. Acta Psychiatr Scand. 2000;102(3):203–210. doi:10.1034/j.1600-0447.2000.102003203.x
46. Skelton M, Khokhar WA, Thacker SP. Treatments for Delusional Disorder. Schizophr Bull. 2015;41(5):1010–1012. doi:10.1093/schbul/sbv080
47. Muñoz-Negro JE, Cervilla JA. A systematic review on the pharmacological treatment of delusional disorder. J Clin Psychopharmacol. 2016;36(6):684–690. doi:10.1097/JCP.0000000000000595
48. Muñoz-Negro JE, Gómez-Sierra FJ, Peralta V, González-Rodríguez A, Cervilla JA. A systematic review of studies with clinician-rated scales on the pharmacological treatment of delusional disorder. Int Clin Psychopharmacol. 2020;35(3):129–136. doi:10.1097/YIC.0000000000000306
49. Fear CF, Libretto SE. Risperidone for the treatment of delusional disorder. Int J Psychiatry Clin Pract. 2002;6(2):113–116. doi:10.1080/136515002753724126
50. Freudenmann RW, Schönfeldt-Lecuona C, Lepping P. Primary delusional parasitosis treated with olanzapine. Int Psychogeriatr. 2007;19(6):1161–1168. doi:10.1017/S1041610207004814
51. Altınöz AE, Tosun Altınöz Ş, Küçükkarapınar M, Coşar B. Paliperidone: another treatment option for delusional parasitosis. Australas Psychiatry. 2014;22(6):576–578. doi:10.1177/1039856214546390
52. Iannuzzi GL, Patel AA, Stewart JT. Aripiprazole and delusional disorder. J Psychiatr Pract. 2019;25(2):132–134. doi:10.1097/PRA.0000000000000368
53. Hayashi H, Oshino S, Ishikawa J, Kawakatsu S, Otani K. Paroxetine treatment of delusional disorder, somatic type. Hum Psychopharmacol. 2004;19(5):
54. Friedel RO. Dopamine dysfunction in borderline personality disorder: a hypothesis. Neuropsychopharmacology. 2004;29(6):1029–1039. doi:10.1038/sj.npp.1300424
55. Hansenne M, Pitchot W, Pinto E, et al. 5-HT1A dysfunction in borderline personality disorder. Psychol Med. 2002;32(5):935–941. doi:10.1017/s0033291702005445
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.