Back to Journals » Journal of Blood Medicine » Volume 17
Care Patterns, Outcomes, and Costs in Peripheral T-Cell Lymphoma Patients with First-Line Treatment in Routine Clinical Practice in Europe
Authors Kristo F, Kelkar SS ![]() , Raina R, Schmier JK, Dalal MR, Ashaye AO
, Raina R, Schmier JK, Dalal MR, Ashaye AO
Received 17 July 2025
Accepted for publication 11 February 2026
Published 29 May 2026 Volume 2026:17 553046
DOI https://doi.org/10.2147/JBM.S553046
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Fjoralba Kristo,1 Sneha S Kelkar,2 Rutika Raina,2 Jordana K Schmier,2 Mehul R Dalal,1 Ajibade O Ashaye1
1Takeda Development Center Americas, Inc., Cambridge, MA, USA; 2Evidence and Access, OPEN Health, Bethesda, MD, USA
Correspondence: Fjoralba Kristo, Global Evidence and Outcomes, Takeda Development Center Americas, Inc., 500 Kendall Street, Cambridge, MA, USA, Email [email protected]
Purpose: Limited real-world data exist on care patterns in peripheral T-cell lymphoma (PTCL) patients. We report care patterns and outcomes among PTCL patients in France, the United Kingdom (UK), Germany, and Italy in the first-line setting.
Patients and Methods: A retrospective chart review was undertaken for adults with newly diagnosed PTCL. Eligible patients received ≥ 1 line of therapy (LOT) and had clinical data for ≥ 1 year after diagnosis or until death. Outcomes included treatments, best response at the end of 1LOT, progression-free survival (PFS) and overall survival (OS).
Results: Data from 195 patients (France=53; UK=56; Germany=56; Italy=30) were collected. Median age at diagnosis was 62.0 years, with 73.3% at stage III/IV. The most common histological subtype was PTCL–not otherwise specified (36.9%). For 1LOT, 49.7% and 36.4% of patients received CHOP and CHOEP regimens, respectively. A complete response was reported in 59.7% of patients. Median PFS from 1LOT initiation was 49.4 months; median OS was 77.1 months. First-line treatment costs were highest in the UK. The cost drivers were adjunctive therapy in France and Germany; stem cell transplant and hospitalization in the UK and Italy, respectively.
Conclusion: This analysis improves the understanding of treatment outcomes and costs in PTCL patients in Europe.
Keywords: peripheral T-cell lymphoma, retrospective, survival, real-world, Europe
Introduction
Peripheral T-cell lymphomas (PTCLs) are a subset of aggressive non-Hodgkin lymphomas (NHLs) that develop from mature T- and natural killer (NK) cells and account for approximately 6% of all newly diagnosed cases of NHL in Western populations.1 PTCL mostly affects adults 60 years and older, with a slightly higher incidence in men.
According to the 2016 World Health Organization (WHO) classification schema, there are over 25 subtypes of mature T- and NK cell neoplasms.2 Nodal subtypes, including PTCL-not otherwise specified (PTCL-NOS), angioimmunoblastic T-cell lymphoma (AITL), and anaplastic large cell lymphoma (ALCL), make up nearly 80% of PTCL cases in Europe.3 For patients with nodal subtypes, guidelines from the European Society for Medical Oncology (ESMO) recommend that treatment selection be guided by patient factors such as age, comorbidities, and International Prognostic Index (IPI) score.4 For patients suitable for intensive therapy, a combination of cyclophosphamide, hydroxydaunorubicin, vincristine, and prednisone with etoposide (CHOEP) or without etoposide (CHOP) is recommended, followed by autologous stem cell transplant (SCT) in eligible patients with chemo-sensitive disease. Five-year overall survival (OS) varies considerably across sub-types; as high as 70% in ALK-positive ALCL and as low as 7% for hepatosplenic PTCL.3
The development of new PTCL therapies has focused primarily on relapsed/refractory disease, with pralatrexate, brentuximab vedotin, and belinostat currently approved in the United States. Of these, only brentuximab vedotin is approved in Europe, as a component of a systemic first-line treatment (BV-CHP) and as monotherapy for patients with relapsed or refractory systemic anaplastic large-cell lymphoma (sALCL).5 For newly-diagnosed patients with CD30+ PTCL, brentuximab vedotin in combination with cyclophosphamide, doxorubicin, and prednisone (CHP) was shown to prolong progression-free and overall survival compared with CHOP in a trial population comprising 70% sALCL.6
There are limited real-world data on patterns of care, healthcare resource utilization and clinical outcomes for patients with newly diagnosed PTCL treated with first-line therapy. There is also interest in assessing progression-free survival (PFS) and OS with current PTCL treatments in routine clinical practice to establish benchmark outcomes for forthcoming therapies. The purpose of this study was to characterize real-world treatment patterns and outcomes among patients with PTCL in France, the United Kingdom (UK), Germany, and Italy in the first-line treatment setting and beyond.
Materials and Methods
Study Design
This retrospective, multicenter medical chart review study used de-identified patient chart data collected by PTCL-treating centers, recruited by local clinical research organizations in France, the UK, and Germany, while a sponsor-provided list was used for center recruitment in Italy. Data were collected from the time of PTCL diagnosis to the most recent patient visit or death. The study was conducted in accordance with local ethical requirements and the Declaration of Helsinki and ethics waiver and/or approval was secured according to requirements in each country. In the United Kingdom (UK), the study was submitted to Health Research Authority (HRA), Medical Research Council (MRC), and obtained an exemption as the study was retrospective in nature and classified as a service evaluation. In Germany, the study went through a process of notifications and was classified as an Anwendungsbeobachtung in accordance with Section 67 (6) of the Medicines Act. In accordance with French law, this non-interventional study was in compliance with the reference methodology MR-004 that is adopted by the French data protection authority (“Commission Nationale de l’Informatique et des Libertés - CNIL”) relating to health research and was approved without obtaining patient consent. In Italy, the study went through ethics approval process in accordance with the Italian Medicines Agency (AIFA).
Patients
Eligible patients included were i) ≥18 years old, diagnosed with PTCL between January 1, 2014, and December 31, 2016, ii) had ≥12 months of follow-up after PTCL diagnosis, unless they died during that period, and iii) received at least first-line treatment for PTCL. Patients enrolled in a clinical trial for first-line treatment of PTCL or had any prior diagnosis of another malignancy within 5 years of PTCL diagnosis and evidence of residual disease were excluded (except those with adequately treated non-melanoma skin cancer or an in-situ neoplasm, such as neoplastic bowel polyp, in situ breast cancer, or localized prostate cancer. In such cases, prior malignancy within 5 years did not forbid participation.
Study Variables and Outcomes
Data collected included patient demographics, clinical characteristics, PTCL treatment and outcomes. Treatment start- and end dates were used to classify regimens by line of therapy (LOT). For each LOT, response was assessed using the Lugano criteria applied to positron emission tomography-computed tomography (PET-CT) or computed tomography (CT) findings,7 and defined as: complete response (CR), partial response (PR), stable disease (SD), or progressive disease (PD). PFS and OS were measured from the start of each LOT to progression/death for PFS and until death for OS. Lastly, costs were determined from the government payor perspective. Country-specific unit costs were sourced from publicly available governmental sources, and published literature8–39 and applied to PTCL-related treatments and resource use collected in the study.7 Calculations were performed at the patient level, where each resource use variable was multiplied by the corresponding unit cost to calculate the total cost by resource type. Total cost calculations included data elements such as, but not limited to, imaging techniques at PTCL diagnosis, PTCL treatments, radiotherapy, stem cell transplant and transfusions. If the number of treatment cycles was missing, the cost for one cycle was assigned; no other imputations were made. All unit costs were inflated/reported to latest available 2024 values using the Harmonized Index of Consumer Prices. Costs were reported in Euros (€).
Statistical Analysis
Analyses were descriptive in nature. Categorical outcomes were summarized using count and percentages in each category. Continuous endpoints were summarized using the summary statistics of mean, standard deviation, median, and range. Time-dependent endpoints including PFS and OS were analyzed in terms of total number of events observed and the proportion of patients experiencing events, after accounting for censoring using Kaplan–Meier (KM) curves.
All analyses were conducted using SAS® software, version 9.4.
Results
Overall Population
Oncologists from fifty-nine participating centers (France, 15; UK, 17; Germany, 24; Italy 3) with a median of 14.8 years of clinical practice took part in the study. Most participating physicians in Germany were practicing at a university hospital or a regional hospital center (n = 18, 75.0%) during the study period. In the UK, almost half of the participating physicians (n = 8, 47.1%) were practicing at a specialist cancer/tertiary referral treatment center. Practice setting was not reported in France and Italy. The average number of patients treated annually per oncologist across the four countries was 14.4.
A total of 195 patients (France, 53; UK, 56; Germany, 56; Italy, 30) received at least 1LOT during the study period. The median duration of study follow-up was 34.6 months from the start of 1LOT. The median age at diagnosis was 62.0 years (range, 49.0 to 70.0 years), with a male predominance (n = 119, 61.0%) (Table 1). Eighty-one and a half percent of patients had an ECOG performance status of 0–1 at diagnosis (n = 159). B-symptoms were present in 60.0% (n = 117), and extranodal disease was present in 39.5% (n = 77) of patients at diagnosis. Most patients (n = 143, 73.3%) had stage III/ IV disease, and 63.1% were classified as intermediate risk (IPI score of 2–3, n = 123). The most common histological subtypes were PTCL-NOS (n = 72, 36.9%), AITL (n = 45, 23.1%) and ALK positive sALCL (n = 30, 15.4%). Of those tested for CD30, 63.4% of patients were positive (n = 116); information on CD30 threshold at each institution was requested of every site but no investigator responded. Only 16.4% of patients underwent cytogenetic testing (n = 32).
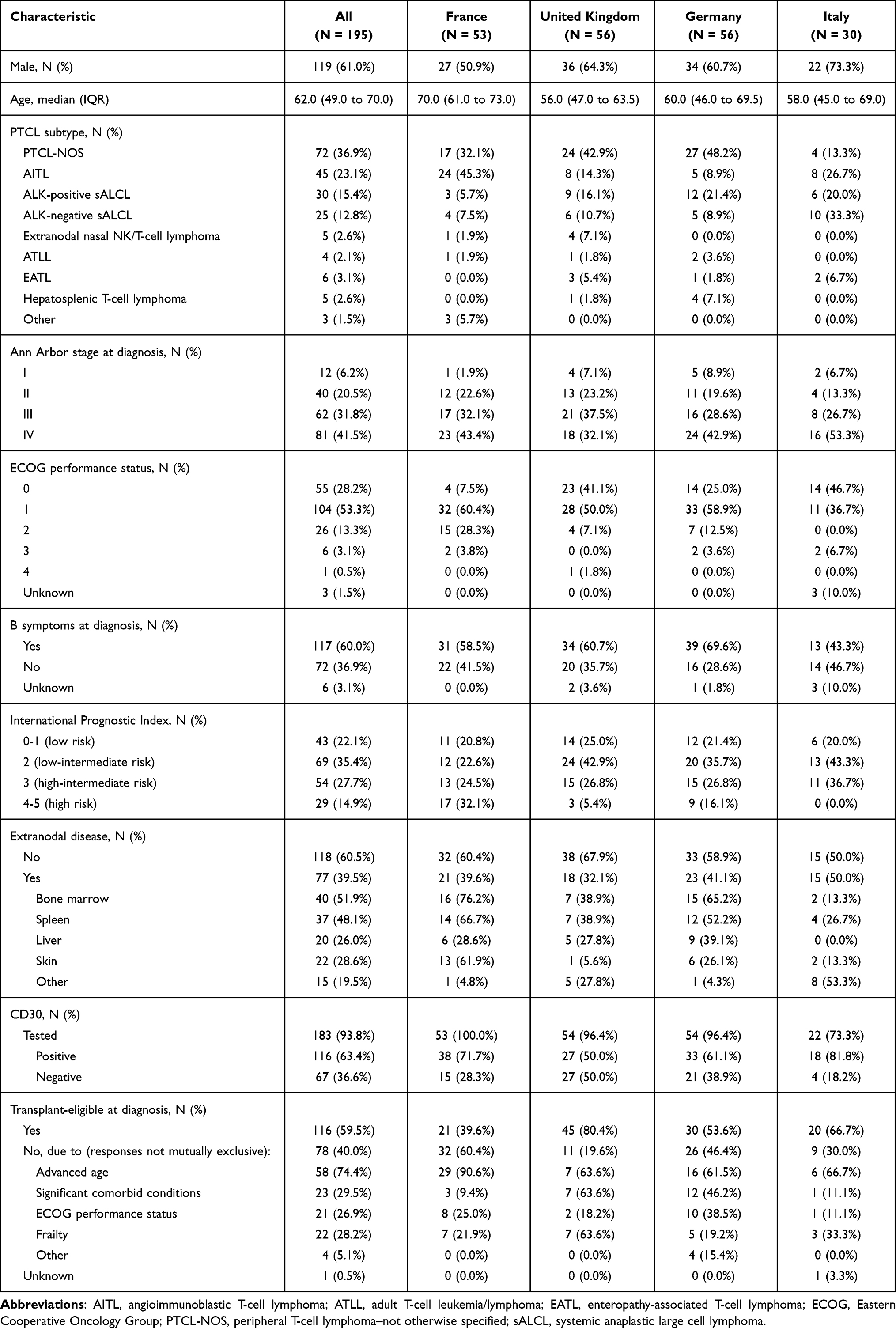 |
Table 1 Patient Characteristics at Peripheral T-Cell Lymphoma Diagnosis |
In the 1LOT setting, 49.7% of patients were treated with CHOP (cyclophosphamide, doxorubicin, vincristine, prednisolone) (n = 97) and 36.4% with CHOEP regimens (CHOP + etoposide; Figure 1) (n = 71). Treatment patterns were similar in France and Germany, with greater use of CHOP-21 in the UK and less use of it in Italy. In 90.3% (n = 176) of the patients, the treatment was planned to be administered for a fixed number of cycles (average 4.9 cycles), while in 6.2% (n = 12) of the patients, the treatment was planned until patients achieved best response, and in 3.1% (n = 6) patients, the treatment was planned until progression. Stem-cell transplantation was undertaken in 26.2% (n = 51) of patients as part of 1LOT (13.2% in France, 44.6% in the UK, 19.6% in Germany, 26.7% in Italy), of which 72.5% (n = 37) were autologous. Transplant rates for patients as part of 2LOT were 4.5% (n = 1), 30.0% (n = 6), 20.0% (n = 3), and 50% (n = 1) in France, the UK, Germany and Italy, respectively, with an overall rate of 18.6% (n = 11).
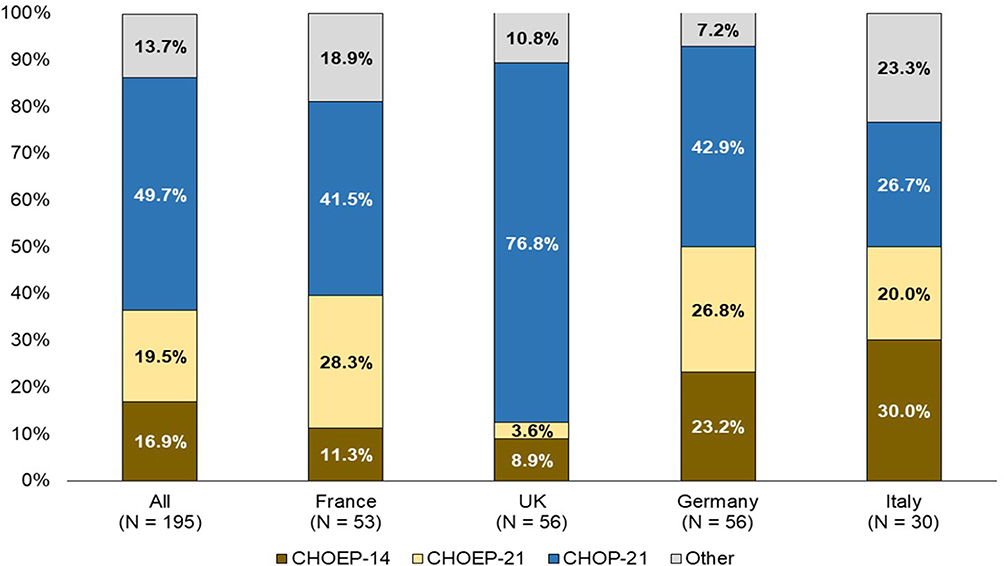 |
Figure 1 First-line Peripheral T-cell Lymphoma Regimens. Other regimens included bendamustine, DHAP, EPOCH, Gemcitabine, GemOX, ICE, IVE alternating with methotrexate, SMILE, and other (unspecified). Abbreviations: CHOEP-14, cyclophosphamide, doxorubicin, vincristine, etoposide, and prednisolone every 14 days; CHOEP-21, cyclophosphamide, doxorubicin, vincristine, etoposide, and prednisolone every 21 days; CHOP-21, cyclophosphamide, doxorubicin, vincristine, prednisolone every 21 days; UK, United Kingdom. |
Response was assessed within one year of completing 1LOT and before the start of 2L treatment in 149 patients; of these, 59.7% (n = 89) achieved complete response (Figure 2). Treatment response by PTCL subtypes is provided in Supplemental Table 1. However, robust conclusions for PTCL subtypes cannot be made due to the small sample sizes.
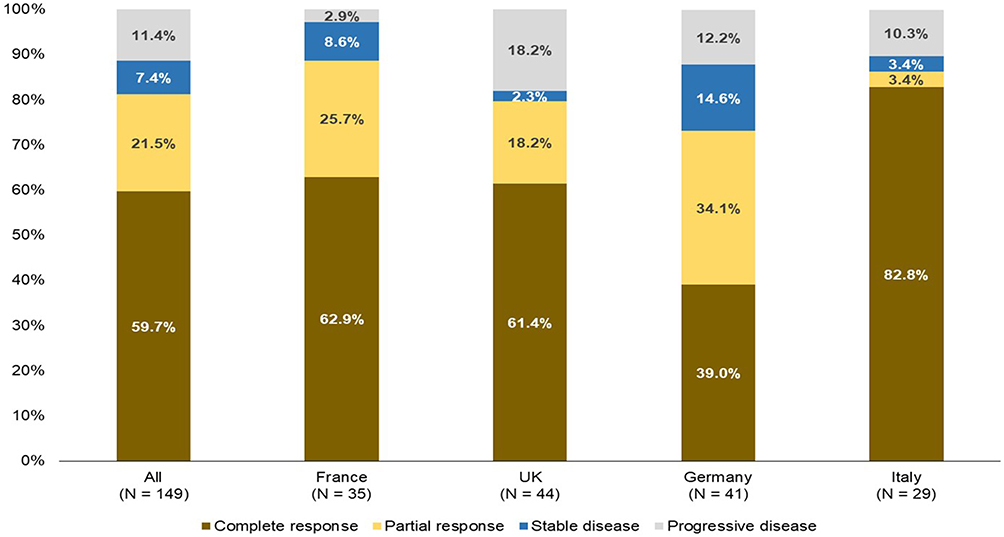 |
Figure 2 Response at End of First-line Therapy. Abbreviation: UK, United Kingdom. |
Median PFS from the start of 1LOT was 49.4 months (95% CI, 35.0 months to not estimable [NE]). Median OS from the start of 1LOT was 77.1 months (95% CI, 62.0 months to NE) with 99.0% of patients alive at 12 months and 70.0% at 36 months.
Fifty-nine patients received a second line of therapy (2LOT). Almost half of patients (49.2%) were planned to receive a fixed duration of therapy, with the remaining patients to be treated to best response (30.5%) or until progression (20.3%). Brentuximab vedotin (n = 14, 23.7%), DHAP (n = 10, 16.9%), and GemOx (n = 8, 13.6%) were the most administered regimens in 2LOT. Across all 2L treatments, median duration of therapy was 3.7 cycles (IQR, 2.7 to 5.0 cycles). Response at the end of 2LOT was available in 38 patients, of which 36.8% (n = 14) achieved complete response and 10.5% (n = 4) achieved partial response. Median PFS at the end of 2LOT was 7.5 months (95% CI, 4.4 to 13.5 months), and median OS at the end of 2LOT was 13.5 months (95% CI, 7.7 months to NE).
Total 2024 costs per patient for 1LOT were €13,730 in France, €36,801 in the UK, €25,069 in Germany, and €28,222 in Italy (Figure 3). Adjunctive therapy was the main driver of costs in France (€5,050) and Germany (€12,912), while stem cell transplant accounted for the greatest cost in the UK (€14,990). Costs for hospitalizations were the highest in Italy (€19,613). Costs per patient were much higher in patients diagnosed with PTCL who were 60 years or younger than patients diagnosed at 60 years or older (€31,894 and €20,352) primarily driven by stem cell transplant in younger patients (€11,488) and by adjunctive therapy in those who were older (€7,270) (Figure 4).
 |
Figure 3 Total cost of first-line therapy in 2024, by country. Abbreviations: UK, United Kingdom; PTCL, Peripheral T-cell lymphoma. Notes: Adjunctive therapies included Acyclovir, Allopurinol, Ciprofloxacin, Enoxaparin, Erythropoietin, Famciclovir, Fluconazole, Fondaparinux, Granulocyte-colony stimulating factor (G-CSF), Levofloxacin, Micafungin, Moxifloxacin, Rasburicase, Trimethoprim/sulfamethoxazole, Valacyclovir, and Voriconazole. |
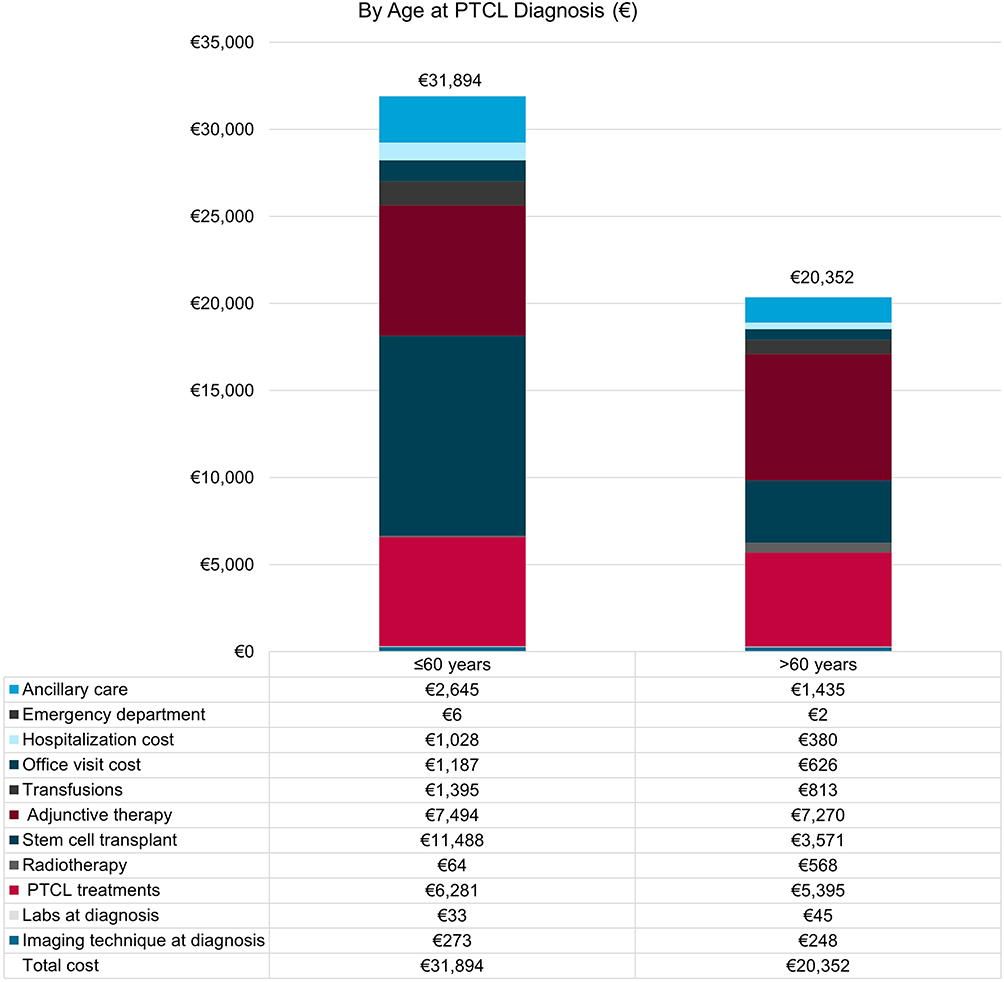 |
Figure 4 Total cost of first-line therapy in 2024, by age at PTCL diagnosis. Abbreviation: PTCL, Peripheral T-cell lymphoma. Notes: Adjunctive therapies included Acyclovir, Allopurinol, Ciprofloxacin, Enoxaparin, Erythropoietin, Famciclovir, Fluconazole, Fondaparinux, Granulocyte-colony stimulating factor (G-CSF), Levofloxacin, Micafungin, Moxifloxacin, Rasburicase, Trimethoprim/sulfamethoxazole, Valacyclovir, and Voriconazole. |
sALCL Subgroup
Fifty-five patients diagnosed with sALCL were included in the study. The median age of these patients at diagnosis was 61.0 years, 69.1% (n = 38) were male, 70.9% (n = 39) had stage III/ IV disease, and 74.5% (n = 41) were classified as intermediate risk (IPI score of 2–3). Almost all (92.7%) patients were CD30-tested, and 88.2% (n = 45) of those tested were positive. All 55 patients were tested for ALK status, 30 (54.5%) were ALK positive (ALK+) and 25 (45.5%) were ALK negative (ALK-) (Table 2). First-line therapy consisted of CHOP-21 (52.7%), CHOEP regimens (38.2%), or EPOCH (3.6%), with a median number of treatment cycles being 5.0 cycles (IQR, 4.0 to 6.0 cycles). Response data were available for 45 patients, of whom 55.6% (n = 25) achieved complete response, 17.8% (n = 8) partial response, 8.9% (n = 4) stable disease, and 17.8% (n = 8) progressive disease. Of those who were ALK+, 52.0% (n = 13) achieved complete response, 24.0% (n = 6) partial response, 8.0% (n = 2) stable disease, and 16.0% (n = 4) progressive disease, while among ALK- patients, 60% (n = 12) achieved complete response, 10.0% (n = 2) partial response, 10.0% (n = 2) stable disease, and 20.0% (n = 4) progressive disease. Median PFS from start of 1LOT was 57.1 months (95% CI, 31.1 months to NE) overall, 77.1 months (95% CI, 37.5 months to NE) for ALK+ patients, and 31.1 months (95% CI, 14.1 months to NE) for ALK- patients. OS was 95.9 months (95% CI, 77.1 months to NE) for patients with sALCL subtype, and 95.9 months (95% CI, 54.4 months to NE) for ALK- patients. Median OS was not evaluable for ALK+ patients. PTCL-related deaths were reported for 2 ALK+ patients, and 2 ALK- patients. Nineteen patients received 2LOT, of whom 11 (57.9%) received brentuximab vedotin. Treatment was planned to follow a fixed duration of therapy in a plurality of patients (42.1%), to best response (36.8%), or until progression (21.1%). Median duration of therapy was 3.9 cycles (IQR, 2.8 to 5.6 cycles), median PFS from initiation of 2LOT was 20.5 months (95% CI, 14.8 months to NE), 75.2 months (95% CI, 20.5 months to NE) for ALK+ patients, and 8.9 months (95% CI, 2.1 months to NE) for ALK- patients. OS from initiation of 2LOT was 75.2 months (95% CI, 23.2 months to NE) for patients with sALCL subtype and ALK+ patients, and was not reached for ALK- patients. Total cost per patient for 1LOT was €27,047 for patients with sALCL subtype and €25,707 for non-sALCL patients.
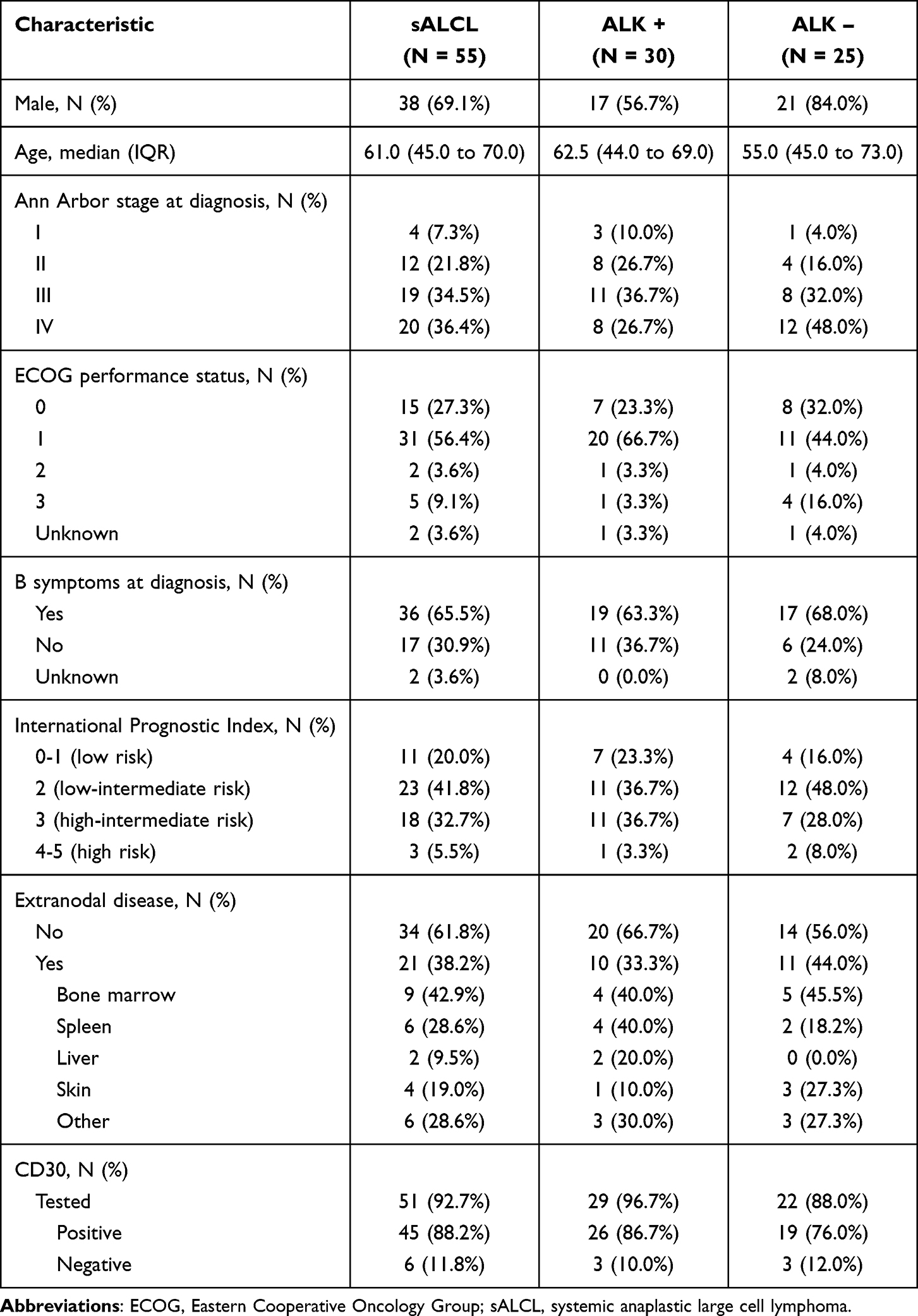 |
Table 2 Patient Characteristics at Peripheral T-Cell Lymphoma Diagnosis Among sALCL Subtype |
Discussion
In this real-world observational study using chart review data, CHOP and CHOEP/CHOEP-like regimens were the most common chemotherapeutic agents for PTCL and for the PTCL subtype sALCL in the first-line therapy setting in France, the UK, Germany, and Italy. These findings align with ESMO treatment guidelines4 at the time of treatment initiation and previous real-world studies conducted in Sweden,40 the Czech Republic,41 the UK,42 and Italy.43 Use of CHOEP was highest in Italy and also Germany, which is consistent with an early retrospective comparative analysis favouring CHOEP over CHOP by the German High-Grade Non-Hodgkin Lymphoma Study Group in 2010,44 and another study by the Nordic Lymphoma Group which concluded the use of CHOEP reasonably beneficial as compared to CHOP for patients diagnosed with ALK+ ALCL under the age of 65 years between 2000 and 2010.45 These real-world patterns mirrored randomized trial practice in PTCL. In the ACT-1 and ACT-2, two Phase III RCTs evaluating CHOP-based induction (with or without alemtuzumab) in younger and elderly PTCL populations, respectively, CHOP was used as the core control regimen and reflects its historical role as standard of care across age strata.46,47
Response rates in this study were higher, and OS and PFS were longer, compared with clinical trials in PTCL. In the control arm of the ECHELON-2 study, which compared A-CHP (brentuximab vedotin, cyclophosphamide, doxorubicin, and prednisone) with CHOP for the treatment of CD30-positive PTCL, the overall response rate was 72% in the control group receiving CHOP, compared with 81.2% of patients in this study.6 Median PFS in the CHOP arm was 23.8 months in the 5-year update of ECHELON-2 study, compared with 49.4 months in this study. Patient populations in the 2 studies differ in the distribution of PTCL subtypes, with more patients in this study diagnosed with PTCL-NOS compared with ECHELON-2 (36.9% vs. 19%) and fewer patients diagnosed with ALK- sALCL (12.8% vs. 46%). However, given that patients with ALK- sALCL have a better prognosis than those with PTCL-NOS,48 the difference in outcomes is inconsistent with prior findings. The transplant rate was 17% in the CHOP arm of ECHELON-2 compared with 26.2% in this study, which could partially explain the difference in outcomes between the two studies. A multicenter, retrospective study published in 2022 also observed better clinical outcomes, including PFS and OS, among patients with PTCL who received autologous SCT in complete remission after first-line chemotherapy. This bolsters the observed difference in outcomes between ECHELON-2 and our study, highlighting the benefits of SCT in improving outcomes among PTCL patients.49 Furthermore, a randomized phase III trial comparing autologous versus allogeneic SCT in first remission PTCL illustrates that post-induction treatment strategy can alter long-term outcome patterns, reinforcing that between-study differences in transplant rates could meaningfully shift OS/PFS estimates.50
The OS and PFS rates in our study are in general higher than previously published real-world studies. The Nordic Lymphoma Group reported 5-year OS and PFS of 78% and 64%, respectively, in patients with ALK+ sALCL.45 OS at 5 years was 74% in sALCL patients—55% of whom were ALK+ in this study. Five-year OS in the UK’s Hematological Malignancy Research Network was 75% in ALK+ sALCL patients, 17.6% in PTCL-NOS patients, and 24.2% in patients with AITL.51 The German High-Grade Non-Hodgkin Lymphoma Study Group reported 3-year OS of 89.8% for ALK+ALCL, 67.5% for AITL, 62.1% for ALK- ALCL, and 53.9% for PTCL-NOS, compared with 70% across all subgroups in this study.44 In comparison, the CHOP arms of recent randomized controlled trials (RCTs) found median PFS of 10.2 months52 and 23.8 months,6 compared to 49.4 months in this study. Differences in baseline characteristics are likely to have contributed; for example, the proportion of patients with stage III/IV disease at baseline in these studies ranged from 50.9% to 84.8%. Second-line therapy consisted of a mix of regimens, including multi-agent and single-agent chemotherapy regimens and brentuximab vedotin. In sALCL patients, of whom 88% were CD30+, BV was prescribed to nearly two-thirds of patients, again consistent with ESMO guidelines. Regardless of PTCL subtype, nearly all patients (94%) had CD30 testing performed at PTCL diagnosis. Unfortunately, study investigators were unable to report the definition of “positive CD30 expression” at their respective institutions; a similar question was also raised in analyses of the French named patient program.53 Lastly, over half of the sALCL positive cohort in this study were ALK+, and despite the relatively small sample size, overall study outcomes may have been driven by ALK+ patients generally having better outcomes compared with ALK- patients.6,44,54
We found that total costs during 1LOT were lower for non-sALCL patients than sALCL subtype patients. Total 1LOT costs per patient were numerically higher in the UK than the other countries (France: €13,730, UK: €36,801, Germany: €25,069, Italy: €28,222). Cost of PTCL treatment was nearly double in the UK than the costs in other countries (France: €4159, UK: €8467, Germany: €4598, Italy: €6080). Costs in Italy were primarily driven by patients who underwent hospitalization (€19,613), while there were no hospitalization costs in Germany. Cost variations in PTCL management across countries could be attributed to differences in national treatment guidelines, transplant eligibility, and healthcare delivery. Small sample sizes and variation in costs based on country-specific treatment patterns suggest that findings should be viewed with caution and may not be generalizable. However, given how little is known about costs associated with PTCL, these findings can help suggest opportunities for future research and identify which resources might be driving costs in specific countries or clinical populations.
This study has several strengths. To our knowledge, it is one of the first real-world historic study of patterns of care and cost among PTCL patients treated with first-line and subsequent lines of therapy. The chart review design allowed for the collection of detailed treatment, response, and adverse event data by physician investigators who were experienced in the care of PTCL patients. Finally, the study had a sufficient sample size to demonstrate clinically significant outcomes of OS and PFS.
In addition to its strengths, this study has certain limitations. Treatment patterns and clinical outcomes in PTCL study patients will represent the practices of participating study physicians/centers during those time horizons and may vary from practices of non-participating physicians—eg, those who refused study participation or were unresponsive to the screening invitation. PTCL patients of non-participating physicians may have profiles, treatments, and outcomes that differ from those of study patients; thus, the generalizability of clinical and cost outcomes may be limited and this may contribute to selection bias. Assessment of treatment response and disease progression may be different in the routine clinical setting as compared with the close monitoring that would be expected in a controlled trial setting. Although physicians seek to record all patient experiences in medical charts, there may be some undercounting of events that are unknown to physicians or that may have occurred outside the physician’s or center’s practice setting. This could lead to information bias. Further, treatment preferences for PTCL management were not evaluated in this study, thus specific reasons for variations in cost outcomes could not be assessed. Additionally, cost outcomes should be generalized with added caution due to the small sample size in each country and differences in treatment patterns across countries.
Conclusion
In conclusion, the results of this study suggest that prescribing in front-line PTCL is consistent with current evidence-based guidelines. Response and survival outcomes suggest a population with better prognoses compared with patients enrolled in clinical trials, and than most of the previous contemporaneous retrospective studies.
Data Sharing Statement
Upon request and subject to review, the corresponding author will provide the data that support the findings of this study.
Acknowledgments
Medical writing support for the development of this manuscript, under the direction of the authors, was provided by Bianca Jackson, funded by Takeda Pharmaceuticals USA, Inc., Cambridge, MA and complied with Good Publication Practice (GPP) guidelines.55
Funding
Takeda Pharmaceuticals, Cambridge, MA, USA, provided research funding to conduct the study.
Disclosure
AA, FK and MD are employees of Takeda Development Center Americas, Inc. and hold shares. SK, RR and JS are employees of OPEN Health, who received consulting fees from Takeda Development Center Americas, Inc. in conjunction with this study. The authors report no other conflicts of interest in this work.
References
1. Dearden CE, Johnson R, Pettengell R, et al. Guidelines for the management of mature T-cell and NK-cell neoplasms (excluding cutaneous T-cell lymphoma). Br J Haematol. 2011;153(4):451–13. doi:10.1111/j.1365-2141.2011.08651.x
2. Foss FM, Zinzani PL, Vose JM, Gascoyne RD, Rosen ST, Tobinai K. Peripheral T-cell lymphoma. Blood. 2011;117(25):6756–6767. doi:10.1182/blood-2010-05-231548
3. Vose J, Armitage J, Weisenburger D. International peripheral T-cell and natural killer/T-cell lymphoma study: pathology findings and clinical outcomes. J Clin Oncol. 2008;26(25):4124–4130. doi:10.1200/jco.2008.16.4558
4. d’Amore F, Gaulard P, Trümper L, et al. Peripheral T-cell lymphomas: ESMO clinical practice guidelines for diagnosis, treatment and follow-up 2020. Ann Oncol. 2015;26:v108–v115. doi:10.1093/annonc/mdv201
5. European Medicines Agency. Adcetris. Available from: https://www.ema.europa.eu/en/medicines/human/EPAR/adcetris#ema-inpage-item-topics.
6. Horwitz S, O’Connor OA, Pro B, et al. Brentuximab vedotin with chemotherapy for CD30-positive peripheral T-cell lymphoma (ECHELON-2): a global, double-blind, randomised, Phase 3 trial. Lancet. 2019;393(10168):229–240. doi:10.1016/S0140-6736(18)32984-2
7. Cheson BD, Fisher RI, Barrington SF, et al. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: the Lugano classification. J Clin Oncol. 2014;32(27):3059–3068. doi:10.1200/JCO.2013.54.8800
8. Heyries F, Chevreul K. Les patients en service de soins infirmiers à domicile (SSIAD) Le coût de leur prise en charge et ses déterminants [Patients in home nursing care services (SSIAD): The cost of their care and its determinants]. French. Available from: https://doc.irdes.fr/index.php?lvl=notice_display&id=75849.
9. l’Assurance Maladie. Convention médicale 2016 Facturation: ce qui change au 1er avril 2018 [Medical Convention 2016 Billing: what changes on April 1, 2018]. French. Available from: https://www.ameli.fr/sites/default/files/Documents/376153/document/convention_medicale_2016_-_1er_avril_2018_-metropole.pdf.
10. Agence technique de l’information sur l’hospitalisation. Agence technique de l’information sur l’hospitalisation. Tarif arrete 2020 [Technical Agency for Hospital Information. 2020 Schedule of Fees]. French. Available from: https://www.atih.sante.fr/sites/default/files/public/content/1568/tarif_arrete_2020.xlsx.
11. l’Assurance Maladie. Nomenclature Generale Des Actes Professionnels (NGAP) Assurance Maladie [71 General Nomenclature of Professional Acts (NGAP) Health Insurance]. French. Available from: https://www.ameli.fr/sites/default/files/Documents/697957/document/ngap-assurance-maladie-03-decembre-2020.pdf.
12. l’Assurance Maladie. Tarifs Conventionnels Applicables À L’activité des Infirmiers Libéraux [Standard Rates Applicable to the Activities of Self-Employed Nurses]. French. Available from: https://www.ameli.fr/infirmier/exercice-liberal/facturation-remuneration/tarifs-conventionnels/tarifs.
13. Centre Hospitalier Intercommunal du Pays de Cognac les Tarifs [Cognac Intercommunal Hospital Center - Rates]. French. Available from: http://www.ch-cognac.fr/Secteur-Medico-Social-Filiere-Personnes-Agees-Handicap-Reseaux-Cognac-Jarnac-Chateauneuf-nouveau-site-Internet-en-chantier-de-reconstruction/Unite-de-Soins-de-Longue-Duree-du-centre-de-gerontologie-clinique-de-COGNAC-Site-Montesquieu/Les-tarifs-tarifs-en-vigueur-au-1er-septembre-2018.
14. Cepparulo A, Giuriato L. The residential healthcare for the elderly in Italy: some considerations for post-COVID-19 policies. Eur J Health Econ. 2022;23(4):671–685. doi:10.1007/s10198-021-01388-9
15. Gesundheitswirtschaft - Fakten & Zahlen - Ausgabe 2015 [Healthcare industry - Facts & Figures - 2015 edition]. German. Available from: https://www.bundeswirtschaftsministerium.de/Redaktion/DE/Publikationen/Wirtschaft/gesundheitswirtschaft-handbuch.pdf?__blob=publicationFile&v=4.
16. Statista. Gesundheitskosten verstorbener pflegebedürftiger im jahr vor ihrem tod in Deutschland nach leistungsbereich 2015 (relative kosten in Euro) [Healthcare costs of deceased persons in need of care in the year before their death in Germany by service area 2015 (relative costs in euros)]. German. Available from: https://de.statista.com/statistik/daten/studie/631910/umfrage/gesundheitskosten-verstorbener-pflegebeduerftiger-im-jahr-vor-ihrem-tod/.
17. Un site au service des Citoyens. Revoir le mode de financement des urgences hospitalieres [A website serving citizens. Reviewing the funding model for hospital emergency services]. French. Available from: https://www.senat.fr/rap/r16-685/r16-6857.html.
18. l’Assurance Maladie. Tarifs conventionnels des médecins généralistes en France métropolitaine [Standard fees for general practitioners in metropolitan France]. French. Available from: https://www.ameli.fr/medecin/exercice-liberal/remuneration/consultations-actes/tarifs/tarifs-generalistes/tarifs-metropole.
19. Kosten für einen stationären Pflegeplatz in Deutschland nach Bundesländern im Jahr 2019 (in Euro pro Monat) [Costs for a residential care place in Germany by federal state in 2019 (in euros per month)]. German. Available from: https://de.statista.com/statistik/daten/studie/1040006/umfrage/kosten-fuer-einen-heimplatz-in-deutschland-nach-bundeslaendern/.
20. Hôpital de Villeneuve-de-Berg Claude Dejean. Tarifs - Unité De soins longue durée (USLD) [Rates - Long-Term Care Unit (USLD)]. French. Available from: https://www.ch-vdb.fr/services-soins/unite-soins-longue-duree-usld/prix.
21. Référentiel de coûts SSR 2017 [2017 SSR Cost Reference Guide]. French. Available from: https://www.scansante.fr/referentiel-de-couts-ssr-2017.
22. Laurt-Taxe [10 Laurt-Taxes]. French. Available form: https://www.cgm.com/deu_de/produkte/apotheke/lauer-taxe-en.html.
23. Institute for the Hospital Remuneration System. Fallpauschalenkatalog 2020 [DRG catalog 2020]. German. Available from: https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&ved=2ahUKEwi37p_Y-tmTAxVGFlkFHSLNDtgQFnoECAwQAQ&url=https%3A%2F%2Fwww.g-drg.de%2Fcontent%2Fdownload%2F8915%2Ffile%2FFallpauschalenkatalog_2020.pdf&usg=AOvVaw1ERL7VmjkyodrZJq9XsWRm&opi=89978449.
24. Statista. Anzahl der Rehabilitationsfälle bei Versicherten der gesetzlichen Krankenversicherung (GKV) in den Jahren von 2000 bis 2020 [Number of rehabilitation cases among those insured under the statutory health insurance scheme (GKV) in the years 2000 to 2020]. German. Available from: https://de.statista.com/statistik/daten/studie/323819/umfrage/anzahl-der-rehabilitationsfaelle-bei-versicherten-der-gkv/.
25. Altini M, Solinas L, Bucchi L, et al. Assessment of cancer care costs in disease-specific cancer care pathways. Int J Environ Res Public Health. 2020;17(13):4765. doi:10.3390/ijerph17134765
26. Haas C, Larbig M, Schöpke T, et al. Gutachten zur ambulanten Notfallversorgung im Krankenhaus - Fallkostenkalkulation und Strukturanalyse 2015 [106 Expert report on outpatient emergency care in hospitals - case cost calculation and structural analysis 2015]. German. Available from: https://www.dkgev.de/fileadmin/default/Mediapool/2_Themen/2.2_Finanzierung_und_Leistungskataloge/2.2.3._Ambulante_Verguetung/2.2.3.4._Ambulante_Notfallvehandlung_durch_Krankenhaeuser/2015-02-17_Gutachten_zur_ambulanten_Notfallversorgung_im_Krankenhaus_2015.pdf
27. Augustinum. Betreutes Wohnen Plus aus einer Hand [Assisted Living Plus from a single source]. German. Available from: https://augustinum.de/kleinmachnow-bei-berlin/leistungen-und-kosten/.
28. Liotta G, Gilardi F, Orlando S, et al. Cost of hospital care for the older adults according to their level of frailty. A cohort study in the Lazio region, Italy. PLoS One. 2019;14(6):e0217829. doi:10.1371/journal.pone.0217829
29. Statista. Ausgaben für Vorsorge- und Rehabilitationsleistungen der gesetzlichen Krankenversicherung (GKV) von 2008 bis 2020 (in Milliarden Euro) [Expenditure on preventive and rehabilitative services provided by statutory health insurance (SHI) from 2008 to 2020 (in billion euros)]. German. Available from: https://de.statista.com/statistik/daten/studie/155811/umfrage/gkv-ausgaben-fuer-vorsorge-und-rehabilitationsleistungen/.
30. Thériaque. Thériaque drug database. French. Available from: https://www.theriaque.org/apps/contenu/accueil.php.
31. l’Assurance Maladie. Classification Commune de Actes Médicaux version 67 [Common Classification of Medical Procedures version 67]. French. Available from: https://www.ameli.fr/fileadmin/user_upload/documents/CCAM_V67_02.xls.
32. L’assurance Maladie. Base des médicaments et informations tarifaires [Drug database and pricing information]. French. Available from: http://www.codage.ext.cnamts.fr/codif/bdm_it/index.php.
33. National Institute for health and Care Excellence. British national formulary (BNF). Available from: https://bnf.nice.org.uk/.
34. Vivamedia. Logement seniors, ehpad & résidences pour personnes agées [Senior housing, nursing homes and residences for the elderly]. French. Available from: https://www.logement-seniors.com/.
35. der Rote Liste® Service GmbH. Rote Liste. German. Available from: https://www.rote-liste.de/.
36. Einheitlicher Bewertungsmaßstab. EBM – einheitlicher Bewertungsmaßstab [36 EBM – Uniform Assessment Scale]. German. Available from: https://medizin.soellner.net/off/ebm.php?node_id=200205000000.
37. Curtis LA, Burns A. Unit Costs of Health & Social Care 2020. PSSRU, University of Kent; 2020.
38. NHS. National Tariff 2021/2022: documents and policies. Annex A. 2022. Available from: https://www.england.nhs.uk/publication/national-tariff-payment-system-documents-annexes-and-supporting-documents/.
39. Tremblay D, Lancman G, Moshier E, Bar N, Jagannath S, Chari A. Outcomes of salvage autologous stem cell transplantation for multiple myeloma with cytopenias and exposure to novel agents. Bone Marrow Transp. 2017;52(10):1468–1470. doi:10.1038/bmt.2017.160
40. Ellin F, Landström J, Jerkeman M, Relander T. Real-world data on prognostic factors and treatment in peripheral T-cell lymphomas: a study from the Swedish lymphoma registry. Blood. 2014;124(10):1570–1577. doi:10.1182/blood-2014-04-573089
41. Janikova A, Chloupkova R, Campr V, et al. First-line therapy for T cell lymphomas: a retrospective population-based analysis of 906 T cell lymphoma patients. Ann Hematol. 2019;98(8):1961–1972. doi:10.1007/s00277-019-03694-y
42. Gleeson M, Peckitt C, Cunningham D, et al. Outcomes following front-line chemotherapy in peripheral T-cell lymphoma: 10-year experience at The Royal Marsden and The Christie hospital. Leukemia Lymphoma. 2018;59(7):1586–1595. doi:10.1080/10428194.2017.1393671
43. Gritti G, Boschini C, Rossi A, et al. Primary treatment response rather than front line stem cell transplantation is crucial for long term outcome of peripheral T-cell lymphomas. PLoS One. 2015;10(3):e0121822. doi:10.1371/journal.pone.0121822
44. Schmitz N, Trümper L, Ziepert M, et al. Treatment and prognosis of mature T-cell and NK-cell lymphoma: an analysis of patients with T-cell lymphoma treated in studies of the German high-grade Non-Hodgkin Lymphoma study group. Blood. 2010;116(18):3418–3425. doi:10.1182/blood-2010-02-270785
45. Cederleuf H, Bjerregård Pedersen M, Jerkeman M, Relander T, d’Amore F, Ellin F. The addition of etoposide to CHOP is associated with improved outcome in ALK+ adult anaplastic large cell lymphoma: a Nordic lymphoma group study. Br J Haematol. 2017;178(5):739–746. doi:10.1111/bjh.14740
46. d’Amore F, Leppä S, Silva MGD, et al. Final analysis of the front-line Phase III randomized ACT-1 trial in younger patients with systemic peripheral T-cell lymphoma treated with CHOP chemotherapy with or without alemtuzumab and consolidated by autologous hematopoietic stem cell transplant. Blood. 2018;132(Supplement 1):998. doi:10.1182/blood-2018-99-110429
47. Wulf GG, Altmann B, Ziepert M, et al. Alemtuzumab plus CHOP versus CHOP in elderly patients with peripheral T-cell lymphoma: the DSHNHL2006-1B/ACT-2 trial. Leukemia. 2021;35(1):143–155. doi:10.1038/s41375-020-0838-5
48. Armitage JO. The aggressive peripheral T-cell lymphomas: 2017. Am J Hematol. 2017;92(7):706–715. doi:10.1002/ajh.24791
49. García-Sancho AM, Bellei M, López-Parra M, et al. Autologous stem-cell transplantation as consolidation of first-line chemotherapy in patients with peripheral T-cell lymphoma: a multicenter GELTAMO/FIL study. Haematologica. 2022;107(11):2675–2684. doi:10.3324/haematol.2021.279426
50. Schmitz N, Truemper L, Bouabdallah K, et al. A randomized phase 3 trial of autologous vs allogeneic transplantation as part of first-line therapy in poor-risk peripheral T-NHL. Blood. 2021;137(19):2646–2656. doi:10.1182/blood.2020008825
51. Smith A, Crouch S, Lax S, et al. Lymphoma incidence, survival and prevalence 2004–2014: sub-type analyses from the UK’s haematological malignancy research network. Br J Cancer. 2015;112(9):1575–1584. doi:10.1038/bjc.2015.94
52. Bachy E, Camus V, Thieblemont C, et al. Final analysis of the Ro-CHOP phase III study (conducted by LYSA): romidepsin plus CHOP in patients with peripheral T-cell lymphoma. Blood. 2020;136(Supplement 1):32–33. doi:10.1182/blood-2020-134440
53. Mathilde L, Céline B, Adrien C, et al. Brentuximab vedotin in refractory or relapsed peripheral T-cell lymphomas: the French named patient program experience in 56 patients. Haematologica. 2016;101(3):e103–e106. doi:10.3324/haematol.2015.135400
54. Savage KJ, Harris NL, Vose JM, et al. ALK- anaplastic large-cell lymphoma is clinically and immunophenotypically different from both ALK+ ALCL and peripheral T-cell lymphoma, not otherwise specified: report from the international peripheral T-cell lymphoma project. Blood. 2008;111(12):5496–5504. doi:10.1182/blood-2008-01-134270
55. DeTora LM, Toroser D, Sykes A, et al. Good publication practice (GPP) guidelines for company-sponsored biomedical research: 2022 update. Ann Intern Med. 2022;175(9):1298–1304. doi:10.7326/m22-1460
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Real-World Use of Loteprednol Etabonate 0.5%/Tobramycin 0.3% Ophthalmic Suspension for the Treatment of Ocular Surface Inflammatory Conditions
Deom JE, Kannarr S, Vollmer P
Clinical Ophthalmology 2022, 16:3803-3809
Published Date: 17 November 2022