Back to Journals » Clinical Epidemiology » Volume 13
Cardiovascular Risk Associated with Methotrexate versus Retinoids in Patients with Psoriasis: A Nationwide Taiwanese Cohort Study
Authors Tsai MH ![]() , Chan TC, Lee MS
, Chan TC, Lee MS ![]() , Lai MS
, Lai MS
Received 3 February 2021
Accepted for publication 22 July 2021
Published 11 August 2021 Volume 2021:13 Pages 693—705
DOI https://doi.org/10.2147/CLEP.S305126
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Irene Petersen
Ming-Hsueh Tsai,1 Tom C Chan,2 Meng-Sui Lee,3,4 Mei-Shu Lai5
1Department of Internal Medicine, Taipei City Hospital, Taipei, Taiwan; 2Department of Dermatology, National Taiwan University Hospital and College of Medicine, Taipei, Taiwan; 3Department of Dermatology, Taipei City Hospital, Taipei, Taiwan; 4Faculty of Medicine, National Yang Ming Chiao Tung University, Taipei, Taiwan; 5Institute of Epidemiology and Preventive Medicine, College of Public Health, National Taiwan University, Taipei, Taiwan
Correspondence: Meng-Sui Lee
Department of Dermatology, Taipei City Hospital, No. 33, Sec. 2, Zhonghua Road, Taipei, 100, Taiwan
Tel/Fax +886 2 23889595 Ext 2225
Email [email protected]
Mei-Shu Lai
Institute of Epidemiology and Preventive Medicine, College of Public Health, National Taiwan University, 5Fl. No. 17, Hsu Chow Road, Taipei, 100, Taiwan
Tel +886 2 33668018
Email [email protected]
Purpose: Psoriasis is an inflammatory disease associated with cardiovascular disease. Methotrexate (MTX) is a first-line systemic anti-psoriatic agent that may also protect against cardiovascular disease. We examined the cardiovascular risks among patients with psoriasis who were receiving MTX or the comparator, retinoids.
Patients and Methods: We analysed data from the Taiwanese National Health Insurance database. The primary outcome was a composite of hospitalisation for ischaemic heart disease, ischaemic stroke and all-cause mortality (composite cardiovascular outcome). Propensity score-weighted analyses were used to evaluate patients who were followed from therapy initiation to the earliest instance of outcome occurrence, insurance disenrollment, death or study termination.
Results: We identified 13,777 patients who received MTX and 6020 patients who received retinoids from 2000 to 2012. Compared to retinoids, MTX was associated with lower crude incidences of cardiovascular outcomes, hospitalisation for ischaemic heart disease, ischaemic stroke and all-cause mortality. In intention-to-treat analyses, MTX was associated with lower risks of composite cardiovascular outcomes (adjusted hazard ratio [HR]: 0.84, 95% confidence interval [CI]: 0.76– 0.94), ischaemic heart disease (HR: 0.87, 95% CI: 0.71– 1.06), ischaemic stroke (HR: 1.06, 95% CI: 0.89– 1.27) and all-cause mortality (HR: 0.75, 95% CI: 0.66– 0.85). Similar results were found in as-treated analyses.
Conclusion: In this nationwide cohort of patients with psoriasis, compared to retinoids, MTX was associated with a modestly lower risk of cardiovascular events.
Keywords: cardiovascular events, inflammation, psoriasis, pharmacoepidemiology
Introduction
Psoriasis is an immune-mediated inflammatory hyperproliferative skin disease that affects 0.5–5.5% of the industrialised world’s population.1 Patients with psoriasis have an increased risk of cardiovascular morbidity and mortality,2–4 which are higher among patients with severe psoriasis.5 In addition to the higher prevalence of traditional cardiovascular risk factors among patients with psoriasis, characteristic systemic inflammation may play a role in increasing the cardiovascular risk by accelerating atherosclerosis.6 However, many anti-inflammatory treatments have emerged as potential therapies for atherosclerosis.7 Therefore, effective systemic anti-inflammatory medication may help reduce cardiovascular risk among patients with psoriasis.6
Both methotrexate (MTX) and retinoids are first-line systemic anti-psoriatic agents that can be used for long-term treatment of psoriasis, whereas cyclosporine and biological agents are reserved as second-line agents. Additionally, cyclosporine is not indicated for continuous chronic use.8,9
The anti-inflammatory properties of MTX10–12 and retinoids13–18 may be beneficial in reducing cardiovascular risk. However, long-term MTX therapy may promote hyperhomocysteinaemia, and dyslipidaemia is a common adverse effect of retinoid therapy. Hyperhomocysteinaemia and dyslipidaemia are both associated with increased cardiovascular risk.19,20 Thus, MTX and retinoids both produce opposing effects on cardiovascular events.
Although the current evidence from observational studies suggests that MTX is associated with a reduced risk of cardiovascular events compared to other therapies for rheumatoid arthritis and psoriasis,21–26 a recent randomised clinical trial, the Cardiovascular Inflammation Reduction Trial (CIRT), showed that low-dose methotrexate did not reduce cardiovascular events compared with placebo among patients with previous coronary artery disease.27
MTX and retinoids have been the most commonly used conventional systemic agents for psoriasis.28 However, studies that directly examined cardiovascular risks associated with retinoid therapy are scarce.22,24 Moreover, the effects of MTX on the cardiovascular risk in patients with psoriasis, compared to those of retinoids, have not been explored. Therefore, the aim of the present study was to perform a head-to-head comparison of the cardiovascular risks associated with initial MTX and with retinoid therapy in patients with psoriasis using a nationwide population-based registry in Taiwan.
Patients and Methods
Data Source
We evaluated data from the National Health Insurance (NHI) database,29 which is a population-level claims dataset that includes demographic characteristics, treatment, prescription drug use, disease diagnosis records and dates of services provided from different clinical settings (outpatient and emergency department visits and hospitalisations) for 99.6% of the Taiwanese population. Information regarding disease outcomes was linked to the National Death Registry to determine mortality. In order to protect the privacy of individuals, the database contains de-identified data, and the requirement for obtaining informed consent was, therefore, waived. The study was approved by the institutional review board of Taipei City Hospital.
Study Population
For this retrospective nationwide cohort study, we evaluated patients who had been diagnosed with psoriasis (International Classification of Diseases, Ninth Revision, Clinical Modification [ICD-9-CM] codes 696.0 and 696.1) in the outpatient and inpatient claims data of the NHI database between January 1, 2000, and December 31, 2012. The diagnosis of psoriasis was verified using records that contained at least 3 claims for psoriasis that had been validated by a dermatologist or rheumatologist and treated using either MTX or retinoid monotherapy. The identification algorithm of psoriasis in the NHI database has been validated in previous studies, which have obtained a high positive predictive value over 98%.30
We applied a new user design and defined the exposure groups according to the patients’ initial anti-psoriatic systemic treatment and the index date as the date for the first prescription of MTX or retinoids. Patients were excluded from the study population if they (1) were <18 years old or had missing sex or age information, (2) had not visited before the date of the first psoriasis diagnosis, (3) did not have continuous insurance coverage for one year before the index date or (4) had received anti-psoriatic systemic therapy during the year before the index date. In order to estimate the effects of MTX or retinoid therapy on incident cardiovascular disease, patients who had experienced hospitalisation for cardiovascular morbidities (ICD-9-CM codes 410, 411, 413, 414, 433 or 434) during the baseline period were also excluded (the detailed information is provided in Table S1 in the Supplementary Data).
Outcome Evaluations and Follow-Up
The primary study outcome, defined as the composite cardiovascular outcome, consisted of hospitalization for ischaemic heart disease (ICD-9-CM codes 410, 411, 413, or 414), ischaemic stroke (ICD-9-CM codes 433 or 434) and/or all-cause mortality. The ICD-9 diagnosis codes of ischaemic heart disease and ischaemic stroke identified from the discharge diagnosis columns of inpatient claims data in the NHI database have been validated and obtained high positive predictive values (0.88–0.92).31,32 Secondary outcomes were defined as each component of cardiovascular composite outcome, including the first hospitalisation for ischaemic heart disease, hospitalisation for ischaemic stroke, and all-cause mortality.
Patients were followed from the index date to the earliest instance of outcome occurrence, death, disenrollment from the NHI or the end of the study.
Covariate Assessment and Propensity Score Estimation
Inpatient and outpatient diagnoses and prescription records during the 12-month baseline period were used to identify the patients’ relevant comorbidities (the pertinent ICD-9-CM codes are provided in Table S1 in the Supplementary Data) and to calculate the Charlson Comorbidity Index.33 Pharmacy dispensing data were also obtained (the relevant Anatomical Therapeutic Chemical codes are provided in Table S1 in the Supplementary Data), as well as data regarding the use of dermatological phototherapy and demographic data, such as age, sex and medical resource utilisation (number of outpatient clinic visits, and number of admission). In constructing the propensity score (PS) derived from the predicted probabilities of the initiation of MTX or retinoid treatment, we included variables that are related to cardiovascular outcome and treatment assignment.34,35 The year-specific PSs36 were estimated using logistic regression models separately for each year during the study period.
We estimated the calendar-time-specific propensity scores (PSs)36 derived from the predicted probabilities of the initiation of MTX or retinoid treatment using non-parsimonious logistic regression models that contained all of the confounding covariates associated with treatment receipts separately for each year during the study period.
Statistical Analysis
All statistical analyses were performed using SAS software (version 9.3; SAS Institute, Cary, NC). Crude incidence rates for the cardiovascular outcomes were calculated as the number of each event divided by the relevant person-time and the 95% confidence intervals [CIs], which were estimated based on the assumption of a Poisson distribution. In addition, we plotted adjusted event-free survival curves for the time-to-event analyses as a function of the duration of use of the index anti-psoriatic drug based on the inverse probability-of-treatment weighting (IPTW).37
We trimmed the non-overlap area of the PS and weighted each study participant by using the inverse of the year-specific PS of the actual receipt of treatment multiplied by the proportion of the study population receiving that drug (stabilized IPTW) to generate a pseudo-population of the same size as the original population in which the distribution of the measured baseline covariates was independent of drug assignment.38 We assessed the performance by calculating the standardized mean differences of the baseline covariates.39 We constructed a Cox proportional hazard model to estimate the adjusted hazard ratio (HR) and 95% CI with a robust variance estimator to account for within-person correlation. To ensure robustness, a goodness-of-fit test was performed. Crude analyses in the origin population and IPTW analyses were performed. The primary analysis was performed as an intention-to-treat analysis in which the treatment group was identified based on the first prescription of MTX or retinoid therapy regardless of whether the patients subsequently changed, stopped or had another drug added to the regimen. The secondary analysis was performed as an as-treated analysis in which the patients were censored from the date on which they discontinued MTX or retinoid therapy for 8 weeks, had another treatment added or were switched to a different drug. For reducing the potential informative censoring, we extended a follow-up for 6 months after the duration of the last prescription.
We also performed subgroup analyses to evaluate the potential effect modification. Participants were grouped according to sex, age (< 65/≥ 65 years old) and hypertension status in order to determine the effect of MTX on the risk of cardiovascular outcomes in these patient subsets. We compared CIs between the subgroups and suggested a significant interaction when the CIs of the two subgroups did not overlap. We conducted a sensitivity analysis to assess the influence of an unmeasured confounder on cardiovascular events.40,41 We also conducted an analysis stratified by PS quintiles to determine whether the results were similar. Additional information about the development of the PS model, the equation of stabilized weights and sensitivity analyses are available in the Appendix 1 and Appendix 2 in the Supplementary Data.
Results
This study’s cohort included 80,167 patients with psoriasis (37% women) who had been first diagnosed between January 1, 2001, and December 31, 2012. A total of 13,777 MTX and 6020 retinoid initiators were included in the study (Figure 1). In the as-treated arms analyses, the median cumulative dose for MTX groups was 105mg [interquartile range (IQR) 30–330] and that for retinoids group was 1200mg (IQR 560–2790). As reported in Table 1, various baseline characteristics differed between the two treatment groups. The MTX group was younger and had a higher proportion of dyslipidaemia with fewer outpatient visits, longer psoriasis duration and a higher Charlson comorbidity score. The MTX group was also less likely to receive anti-platelet agents, anti-hypertensive agents and anti-depressants. However, the baseline characteristic distributions were similar between the two groups after PS weighting. All covariates were well balanced because the differences were less than 0.1 standardized difference (Table 1).39
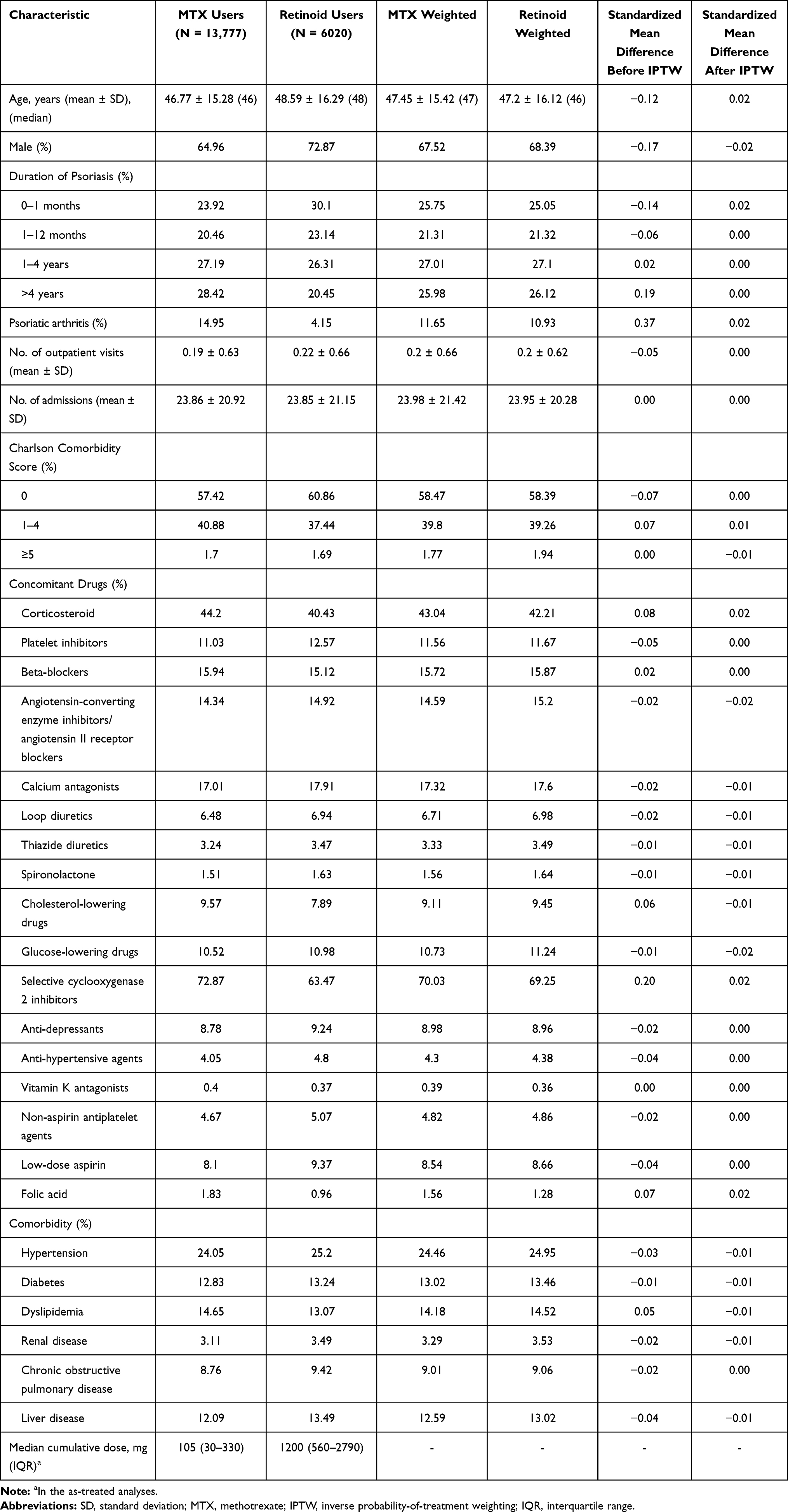 |
Table 1 Baseline Characteristics of Patients with Psoriasis Who Were Receiving Methotrexate or Retinoids Before and After Propensity Score Weighting |
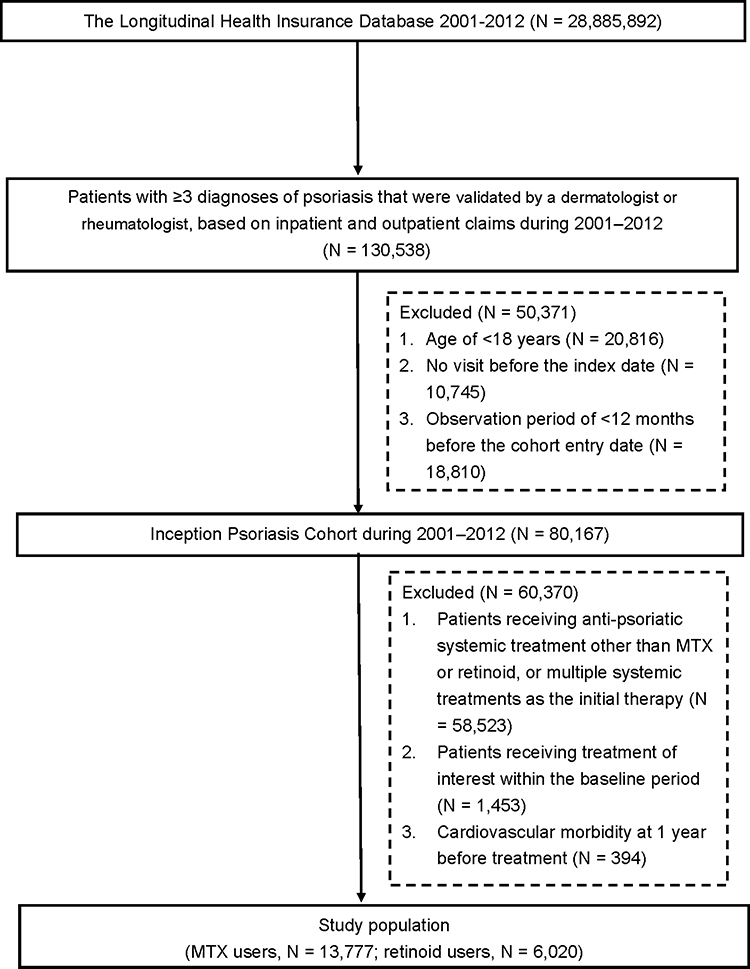 |
Figure 1 Study flow chart. |
During a mean follow-up of 4.4 years, cardiovascular outcomes were observed in 1108 patients who had received MTX and in 826 patients who had received retinoids. In the intention-to-treat and as-treated analyses results reported in Table 2, it can be seen that the MTX group had lower crude incidences of cardiovascular outcomes, hospitalisation for ischaemic heart disease, ischaemic stroke and all-cause mortality compared to the retinoid group.
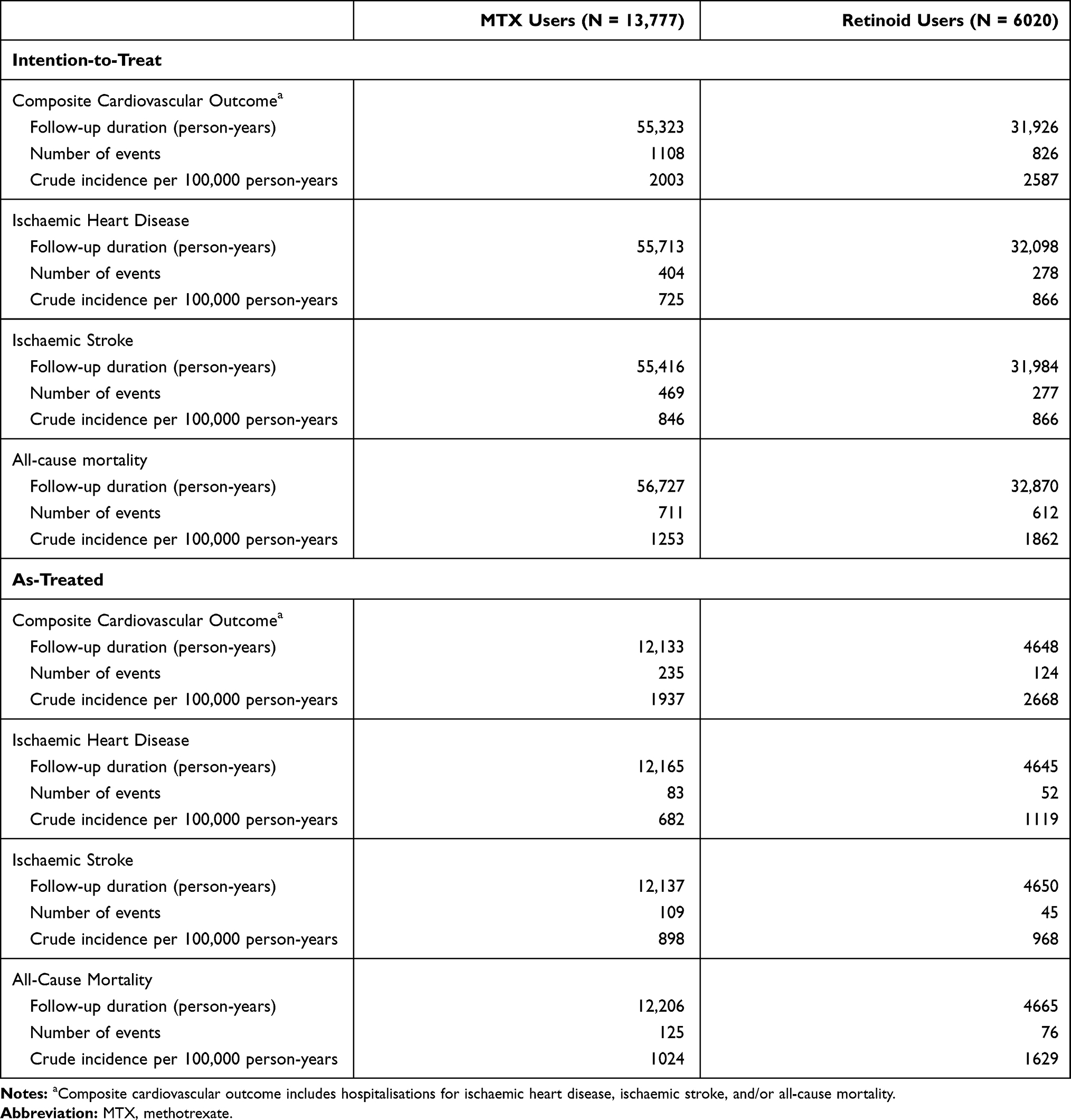 |
Table 2 Numbers of Events, Person-Days, and Crude Incidence Rates Among Patients with Psoriasis Who Were Receiving Methotrexate or Retinoids |
In the intention-to-treat (Figure 2A) and as-treated (Figure 2B) analyses, the IPTW adjusted estimates for cardiovascular event-free survival curves diverge over the short-term and then become nearly parallel. Log rank tests revealed modest differences (P < 0.001 for the intention-to-treat analysis and P = 0.049 for the as-treated analysis).
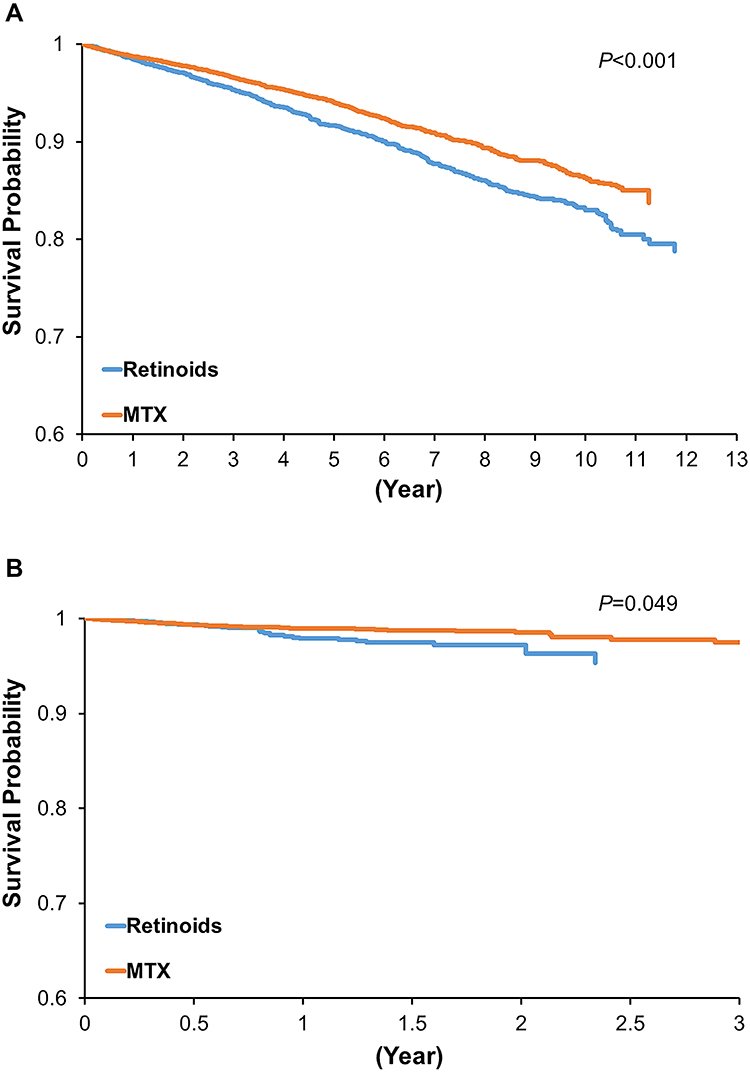 |
Figure 2 The inverse probability-weighted event-free survival curves for cardiovascular outcome-free survival among methotrexate or retinoid users. (A) Intention-to-treat analysis and (B) as-treated analysis. Abbreviation: MTX, methotrexate. |
Table 3 presents the results from the Cox regression analyses based on the retinoid group as the reference group. In the crude analysis, MTX was associated with lower risks of cardiovascular outcomes (HR: 0.78; 95% CI: 0.71–0.85), ischaemic heart disease (HR: 0.83; 95% CI: 0.71–0.97) and all-cause mortality (HR: 0.69; 95% CI: 0.62–0.77). In the PS-weighted intention-to-treat analyses, MTX was also associated with lower risks of cardiovascular outcomes (HR: 0.84; 95% CI: 0.76–0.94) and all-cause mortality (HR 0.75; 95% CI: 0.66–0.85), but not for ischaemic heart disease (HR 0.87; 95% CI: 0.71–1.06) and ischaemic stroke (HR 1.06; 95% CI: 0.89–1.27). Similar results were found in the as-treated analyses that censored patients at drug discontinuation or switching.
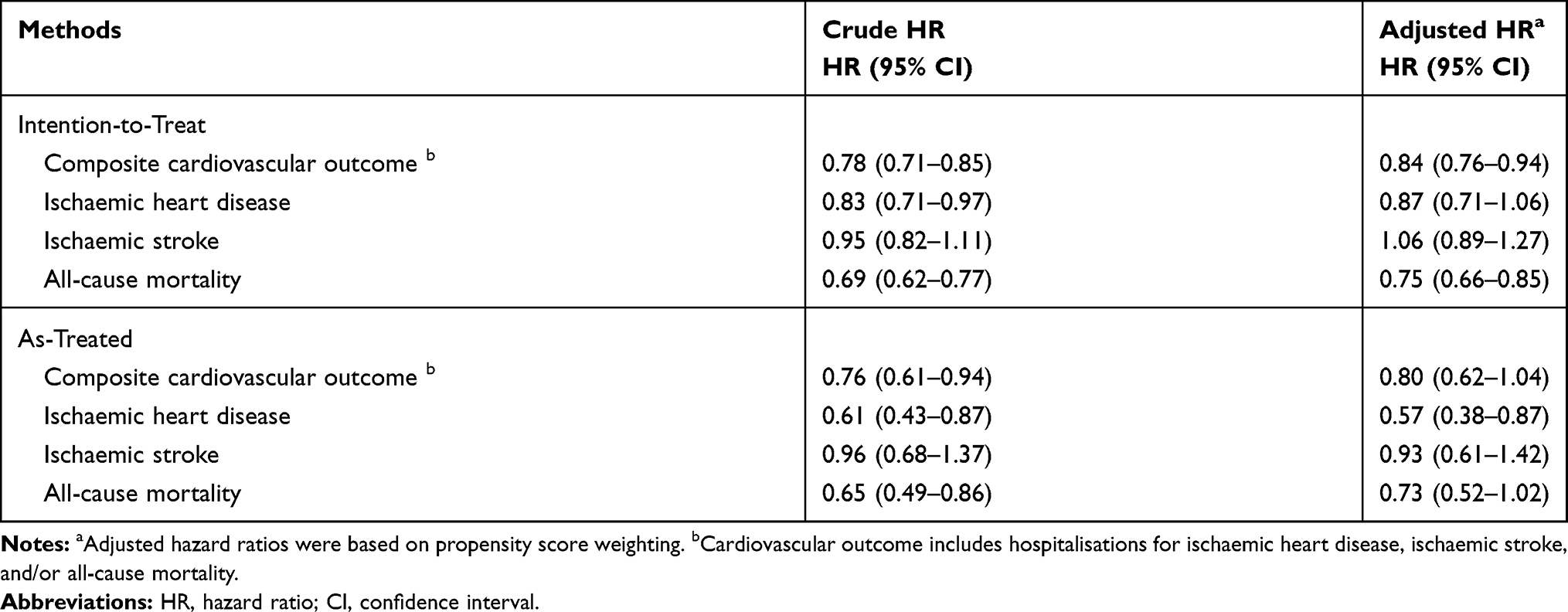 |
Table 3 Hazard Ratios of Cardiovascular Outcomes Comparing Methotrexate (n=13,777) with Retinoids (n=6020) Use in Psoriasis Patients Weighted by Propensity Score |
Subgroup analyses did not reveal any modifications based on the patient characteristics, although the HR estimates were slightly lower among patients who were < 65 years old (Figure 3). Similar results were found in propensity score-stratified analyses (Appendix 2 Table S2 in the Supplementary Data). Sensitivity analyses revealing only a strong unmeasured confounder with a risk of cardiovascular events equal to 2.0 or more together with a large prevalence difference among the study groups would have biased estimates downward. For instance, if 26% of retinoids users and 5% of MTX users had a risk factor that increased the risk of cardiovascular event twofold, the true effect would be toward the null value. (Appendix 2 Figure S1 in the Supplementary Data)
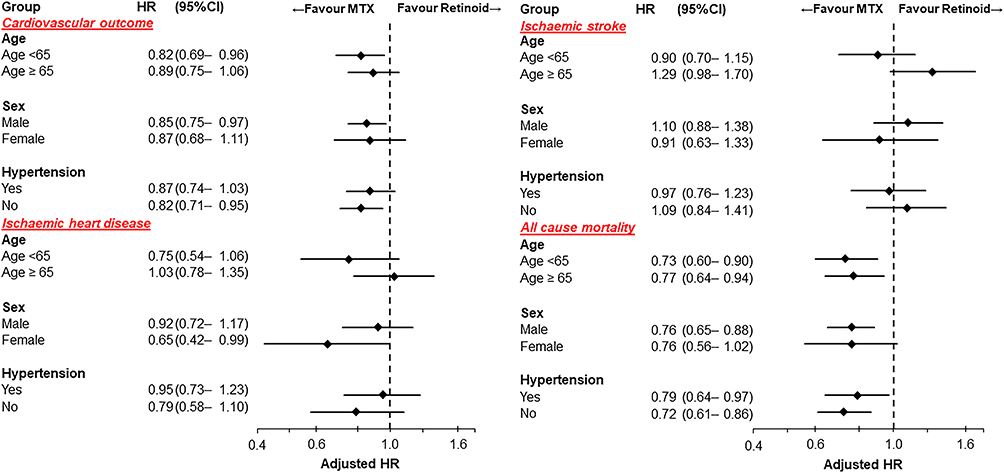 |
Figure 3 Adjusted hazard ratios for cardiovascular outcomes among methotrexate and retinoid users according to different subgroups using an intention-to-treat approach with weighted propensity score. Abbreviations: HR, hazard ratios; CI, confidence interval. |
Discussion
The findings of this nationwide study provide evidence that patients with psoriasis receiving MTX therapy are less likely to develop a composite cardiovascular outcome than patients receiving retinoid therapy. However, the effects were less evident after adjustment for potential confounding factors in the PS-based models. The IPTW adjusted cardiovascular event-free survival curves showed the risk of cardiovascular outcomes was significantly lower in MTX users than in retinoids users during the study period.
We included all-cause mortality in the composite cardiovascular outcome because psoriasis is associated with several conditions that result in an increased risk of death, mainly cardiovascular disorders, cancer, renal failure, and infectious diseases; however, the National Death Registry of Taiwan is limited to a single leading cause of death, which is selected from all diseases mentioned in the death certificate according to international coding rules. Therefore, our study included all-cause mortality in the composite cardiovascular outcome to avoid missing other contributing causes of death that is not listed as the leading cause of death.
The National Health Insurance regulation of Taiwan recommends a conventional oral drug as the first-line systemic treatment for moderate-to-severe psoriasis. In real-world setting, MTX and retinoids have been the most widely used systemic anti-inflammatory therapy for psoriasis in Taiwan28 and share similar clinical characteristics, such as disease severity and contraindication. Patients with hepatic impairment are relatively contraindicated for receiving retinoids or MTX.9,42 Unlike MTX, retinoids are not indicated for the treatment of psoriatic arthritis in patients with an increased risk of cardiovascular events and all-cause mortality.43
MTX theoretically reduces the risk of cardiovascular events through a systemic anti-inflammatory effect even though it might also increase cardiovascular risk. The results of our study reveal that MTX use is associated with a reduced risk of cardiovascular outcomes among patients with psoriasis; similar results have been found in large observational studies of patients with psoriasis and rheumatoid arthritis.22,25,44,45 This effect of MTX may be related to the drug’s anti-inflammatory properties and/or may lead to improved physical activity that subsequently results in a lower risk of diabetes, high blood pressure and obesity, as these are important cardiovascular risk factors. Therefore, our results also moderately support the hypothesis that targeted anti-inflammatory therapy may be feasible for preventing cardiovascular events among patients with psoriasis.46 However, MTX can also induce hyperhomocysteinaemia through folic acid depletion, while hyperhomocysteinaemia promotes coagulation and has toxic effects on the endothelium that can increase cardiovascular risk.19 Therefore, folic acid therapy is advised for patients with MTX-treated psoriasis as it prevents MTX-induced hyperhomocysteinaemia while possibly reducing their cardiovascular risk.47
Retinoids comprise an anti-inflammatory effect14–17 and an anti-proliferative effect for psoriasis.13 Dyslipidemia is a frequent consequence of the use of retinoids. Although dyslipidaemia might have played a crucial role in cardiovascular risk in the retinoid group in the present study, conflicting results were reported by Stern,48 in which the incidence of myocardial infarction when assessing the safety of long-term retinoid therapy for psoriasis was no different from the expected number on the basis of population-based incidence data (13 vs 13.3–15.7).49,50 It is commendable to add lipid-lowering therapy and lifestyle education to reduce cardiovascular risk factors.9,51
Our findings agree with those from a Danish cohort study in which the authors found a beneficial effect of MTX therapy (vs topical agents or phototherapy) for psoriasis on cardiovascular outcomes among patients with psoriasis.22 However, the magnitude of the protective effect was more prominent in the Danish study. This difference may be related to the different study groups as unmeasured confounders (eg, frailty) may reduce the likelihood of MTX treatment if physicians focus on the patient’s chief medical concern rather than systemic therapy for psoriasis. It is plausible that this effect may explain the better protective effects of MTX observed in the Danish study. In a previous Taiwanese cohort study,23 the authors investigated the effects of MTX (vs other non-biological systemic treatments) on newly-developed ischaemic heart disease and suggested that the adjusted effects were comparable between the two groups. However, a lack of mortality data might have resulted in an underestimation of MTX’s effect.
However, in contrast to the above mentioned studies, the findings of the CIRT trial did not confirm the cardioprotective role of MTX.27 Differences in the study design could explain the contrasting results. The study population for the CIRT trial included patients with previous coronary disease but without chronic inflammatory burden, such as psoriasis or rheumatoid arthritis. Our study, by contrast, enrolled psoriasis patients who were not hospitalised for cardiovascular morbidities. It is possible that a larger effect would happen in patients with a higher inflammatory load under the strong anti-inflammatory effect of MTX.52
Our study design has several strengths compared to previous research. By embedding an IPTW with year-specific PS36 within an observational study, the design not only created a cohort of patients who shared similar observed characteristics but also reduced bias due to channelling when the calendar year is a confounder or a proxy of confounders. The probability of receiving MTX or retinoid treatment may change over the study period while prescribing patterns and clinical practice guidelines can also change over time, which can lead to the calendar year becoming a confounder or a predictor of treatment receipt. Compared with previous research using multivariable-adjusted Cox regression, matching or stratification,22,23,25,44,45 PS semiparametric inverse probability-weighted estimators need fewer distributional assumptions regarding the underlying data.
The present study additionally had other strengths. Firstly, the data were obtained from the NHI database, which provides detailed information regarding the patients, physicians, hospitals and prescribed drugs and other medical care. Thus, the study population is representative of the psoriasis population and real-world clinical practice in Taiwan, which allows for precise estimation of the incidences that we evaluated. Secondly, the long-term patient outcomes were verified using links to the NHI and the National Death Registry. Thirdly, we evaluated newly diagnosed psoriatic patients and used a new-user design to reduce potential selection bias, along with multiple strategies to assemble comparable groups of patients. Fourth, all information regarding exposure, outcomes and covariates was recorded before the study commenced, which eliminates the possibility of bias from recall or reconstruction of clinical history.
The present study also had several limitations. Firstly, the NHI database did not have information regarding the Psoriasis Area and Severity Index, lifestyle, body mass index or a family history of metabolic syndrome. Thus, differing risk factors may arise from confounding by indication, as psoriasis severity, comorbidities and contraindications can influence the initial drug choice. There might have been residual measured or unmeasured confounding factors even though we used retinoid therapy as the active comparison group and PS to adjust for a wide range of potential confounders that might introduce confounding by indication.35,53 To compensate for the missing comorbidity and socioeconomic data, we used a sensitivity analysis to determine how the imbalance of a strong unmeasured confounder among the drug exposure categories might affect the observed HRs. However, only a strong unmeasured cardiovascular risk factor combined with a very large prevalence difference between the two groups could lead to our findings.40,41 Secondly, intention-to-treat analyses in studies with long follow-up periods are especially susceptible to non-adherence bias as a consequence of exposure misclassification. This might lead to a conservative result. However, the as-treated approach, in which follow-up ends at the time of drug switching or discontinuation, could have introduced potential informative censoring. To reduce this, we extended a follow-up for 6 months after the duration of the last prescription. The use of different analytical techniques made it possible to indicate the potential range of effect estimates for our analyses.53 Nevertheless, misclassification regarding psoriasis diagnosis or drug exposure is likely not related to the exposure-outcome association. Finally, we did not conduct multiple tests in our study, because the Bonferroni corrections are too conservative and other methods such as global tests or approaches for controlling P-values are usually of little value.54,55 However, all clinical outcomes of interest are closely related, and we have defined a composite cardiovascular outcome as the primary outcome, with the consequence that all other aggregated endpoints are subsidiary in order to present the holistic concept of cardiovascular risk. The selection of an aggregated outcome might provide a rationale for dealing with the statistical problem of multiple outcome measures.56
Conclusion
In conclusion, we found that initial MTX therapy was associated with a modestly lower risk of cardiovascular disease in patients with psoriasis compared to retinoid therapy. Therefore, future research of systemic anti-psoriatic treatments is needed to explore the effects of these drugs on cardiovascular outcomes and to support better clinical decision-making for patients with psoriasis.
Acknowledgments
All data used in this study were released and approved by the Health and Welfare Data Science Center, Taiwan.
The authors would like to thank the support from staff of the Eighth Core Lab, Department of Medical Research, National Taiwan University Hospital.
Funding
This work was supported by the Taiwan Ministry of Science and Technology (Grants MOST 103-2314-B-532-002). Role of the Funding Source: None.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Raychaudhuri SP, Farber EM. The prevalence of psoriasis in the world. J Eur Acad Dermatol Venereol. 2001;15:16–17. doi:10.1046/j.1468-3083.2001.00192.x
2. Salahadeen E, Torp-Pedersen C, Gislason G, Hansen PR, Ahlehoff O. Nationwide population-based study of cause-specific death rates in patients with psoriasis. J Eur Acad Dermatol Venereol. 2015;29:1002–1005. doi:10.1111/jdv.12523
3. Gelfand JM, Neimann AL, Shin DB, Wang X, Margolis DJ, Troxel AB. Risk of myocardial infarction in patients with psoriasis. JAMA. 2006;296:1735–1741. doi:10.1001/jama.296.14.1735
4. Gelfand JM, Dommasch ED, Shin DB, et al. The risk of stroke in patients with psoriasis. J Invest Dermatol. 2009;129:2411–2418. doi:10.1038/jid.2009.112
5. Armstrong EJ, Harskamp CT, Armstrong AW. Psoriasis and major adverse cardiovascular events: a systematic review and meta-analysis of observational studies. J Am Heart Assoc. 2013;2:e000062. doi:10.1161/JAHA.113.000062
6. Boehncke WH, Boehncke S, Tobin AM, Kirby B. The ‘psoriatic march’: a concept of how severe psoriasis may drive cardiovascular comorbidity. Exp Dermatol. 2011;20:303–307. doi:10.1111/j.1600-0625.2011.01261.x
7. Charo IF, Taub R. Anti-inflammatory therapeutics for the treatment of atherosclerosis. Nat Rev Drug Discov. 2011;10:365–376. doi:10.1038/nrd3444
8. Menter A, Gelfand JM, Connor C, et al. Joint american academy of dermatology–national psoriasis foundation guidelines of care for the management of psoriasis with systemic nonbiologic therapies. J Am Acad Dermatol. 2020;82:1445–1486.
9. Carretero G, Ribera M, Belinchon I, et al. Guidelines for the use of acitretin in psoriasis. Psoriasis group of the spanish academy of dermatology and venereology. Actas Dermosifiliogr. 2013;104:598–616. doi:10.1016/j.ad.2013.01.003
10. Cronstein BN. Low-dose methotrexate: a mainstay in the treatment of rheumatoid arthritis. Pharmacol Rev. 2005;57:163–172. doi:10.1124/pr.57.2.3
11. Zhang Z, Zhao P, Li A, et al. Effects of methotrexate on plasma cytokines and cardiac remodeling and function in postmyocarditis rats. Mediators Inflamm. 2009;2009:389720. doi:10.1155/2009/389720
12. Lacki JK, Klama K, Mackiewicz SH, Mackiewicz U, Muller W. Circulating interleukin-10 and interleukin-6 serum levels in rheumatoid-arthritis patients treated with methotrexate or gold salts - preliminary-report. Inflamm Res. 1995;44:24–26. doi:10.1007/BF01630483
13. Gottlieb S, Hayes E, Gilleaudeau P, Cardinale I, Gottlieb AB, Krueger JG. Cellular actions of etretinate in psoriasis: enhanced epidermal differentiation and reduced cell-mediated inflammation are unexpected outcomes. J Cutan Pathol. 1996;23:404–418. doi:10.1111/j.1600-0560.1996.tb01430.x
14. Yu J, Shao LE, Frigon NL, Lofgren J, Schwall R. Induced expression of the new cytokine, activin A, in human monocytes: inhibition by glucocorticoids and retinoic acid. Immunology. 1996;88:368–374. doi:10.1046/j.1365-2567.1996.d01-675.x
15. Mehta K, McQueen T, Tucker S, Pandita R, Aggarwal BB. Inhibition by all-trans-retinoic acid of tumor necrosis factor and nitric oxide production by peritoneal macrophages. J Leukoc Biol. 1994;55:336–342. doi:10.1002/jlb.55.3.336
16. Hayashi S, Hashimoto S, Kitamura N, Hanazawa S, Horie T. Retinoic acid regulates differentially the expression of IL-1 beta and IL-1 receptor antagonist (IL-1ra) in PMA-activated human monocytes. Biochem Biophys Res Commun. 1996;224:574–578. doi:10.1006/bbrc.1996.1066
17. Na SY, Kang BY, Chung SW, et al. Retinoids inhibit interleukin-12 production in macrophages through physical associations of retinoid X receptor and NFkappaB. J Biol Chem. 1999;274:7674–7680. doi:10.1074/jbc.274.12.7674
18. Chadwick CC, Shaw LJ, Winneker RC. TNF-alpha and 9-cis-retinoic acid synergistically induce ICAM-1 expression: evidence for interaction of retinoid receptors with NF-kappa B. Exp Cell Res. 1998;239:423–429. doi:10.1006/excr.1997.3913
19. De Bree A, Verschuren WM, Kromhout D, Kluijtmans LA, Blom HJ. Homocysteine determinants and the evidence to what extent homocysteine determines the risk of coronary heart disease. Pharmacol Rev. 2002;54:599–618. doi:10.1124/pr.54.4.599
20. van Ede AE, Laan RF, Blom HJ, et al. Homocysteine and folate status in methotrexate-treated patients with rheumatoid arthritis. Rheumatology (Oxford). 2002;41:658–665. doi:10.1093/rheumatology/41.6.658
21. Roubille C, Richer V, Starnino T, et al. The effects of tumour necrosis factor inhibitors, methotrexate, non-steroidal anti-inflammatory drugs and corticosteroids on cardiovascular events in rheumatoid arthritis, psoriasis and psoriatic arthritis: a systematic review and meta-analysis. Ann Rheum Dis. 2015;74:480–489. doi:10.1136/annrheumdis-2014-206624
22. Ahlehoff O, Skov L, Gislason G, et al. Cardiovascular outcomes and systemic anti-inflammatory drugs in patients with severe psoriasis: 5-year follow-up of a Danish nationwide cohort. J Eur Acad Dermatol Venereol. 2015;29:1128–1134. doi:10.1111/jdv.12768
23. Chen YJ, Chang YT, Shen JL, et al. Association between systemic antipsoriatic drugs and cardiovascular risk in patients with psoriasis with or without psoriatic arthritis: a nationwide cohort study. Arthritis Rheum. 2012;64:1879–1887. doi:10.1002/art.34335
24. Lan CC, Ko YC, Yu HS, et al. Methotrexate reduces the occurrence of cerebrovascular events among Taiwanese psoriatic patients: a nationwide population-based study. Acta Derm Venereol. 2012;92:349–352. doi:10.2340/00015555-1283
25. Prodanovich S, Ma F, Taylor JR, Pezon C, Fasihi T, Kirsner RS. Methotrexate reduces incidence of vascular diseases in veterans with psoriasis or rheumatoid arthritis. J Am Acad Dermatol. 2005;52:262–267. doi:10.1016/j.jaad.2004.06.017
26. Ahlehoff O, Skov L, Gislason G, et al. Cardiovascular disease event rates in patients with severe psoriasis treated with systemic anti-inflammatory drugs: a Danish real-world cohort study. J Intern Med. 2013;273:197–204. doi:10.1111/j.1365-2796.2012.02593.x
27. Ridker PM, Everett BM, Pradhan A, et al. Low-dose methotrexate for the prevention of atherosclerotic events. N Engl J Med. 2019;380:752–762. doi:10.1056/NEJMoa1809798
28. Chang YT, Chen TJ, Liu PC, et al. Epidemiological study of psoriasis in the national health insurance database in Taiwan. Acta Derm Venereol. 2009;89:262–266. doi:10.2340/00015555-0642
29. Hsieh C-Y, Su -C-C, Shao S-C, et al. Taiwan’s national health insurance research database: past and future. Clin Epidemiol. 2019;11:349–358. doi:10.2147/CLEP.S196293
30. Lee MS, Yeh YC, Chang YT, Lai MS. All-cause and cause-specific mortality in patients with psoriasis in taiwan: a nationwide population-based study. J Invest Dermatol. 2017;137:1468–1473.
31. Hsieh CY, Chen CH, Li CY, Lai ML. Validating the diagnosis of acute ischemic stroke in a national health insurance claims database. J Formos Med Assoc. 2015;114:254–259. doi:10.1016/j.jfma.2013.09.009
32. Cheng CL, Lee CH, Chen PS, Li YH, Lin SJ, Yang YH. Validation of acute myocardial infarction cases in the national health insurance research database in taiwan. J Epidemiol. 2014;24:500–507. doi:10.2188/jea.JE20140076
33. Quan H, Sundararajan V, Halfon P, et al. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med Care. 2005;43:1130–1139. doi:10.1097/01.mlr.0000182534.19832.83
34. Benedetto U, Head SJ, Angelini GD, Blackstone EH. Statistical primer: propensity score matching and its alternatives. Eur J Cardiothorac Surg. 2018;53:1112–1117. doi:10.1093/ejcts/ezy167
35. Austin PC. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behav Res. 2011;46:399–424. doi:10.1080/00273171.2011.568786
36. Seeger JD, Williams PL, Walker AM. An application of propensity score matching using claims data. Pharmacoepidemiol Drug Saf. 2005;14:465–476. doi:10.1002/pds.1062
37. Cole SR, Hernan MA. Adjusted survival curves with inverse probability weights. Comput Methods Programs Biomed. 2004;75:45–49. doi:10.1016/j.cmpb.2003.10.004
38. Hernan MA, Robins JM. Estimating causal effects from epidemiological data. J Epidemiol Community Health. 2006;60:578–586. doi:10.1136/jech.2004.029496
39. Austin PC. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat Med. 2009;28:3083–3107.
40. Lee WC. Bounding the bias of unmeasured factors with confounding and effect-modifying potentials. Stat Med. 2011;30:1007–1017. doi:10.1002/sim.4151
41. Schneeweiss S. Sensitivity analysis and external adjustment for unmeasured confounders in epidemiologic database studies of therapeutics. Pharmacoepidemiol Drug Saf. 2006;15:291–303. doi:10.1002/pds.1200
42. Kalb RE, Strober B, Weinstein G, Lebwohl M. Methotrexate and psoriasis: 2009 national psoriasis foundation consensus conference. J Am Acad Dermatol. 2009;60:824–837. doi:10.1016/j.jaad.2008.11.906
43. Ahlehoff O, Gislason GH, Charlot M, et al. Psoriasis is associated with clinically significant cardiovascular risk: a Danish nationwide cohort study. J Intern Med. 2011;270:147–157.
44. Choi HK, Hernan MA, Seeger JD, Robins JM, Wolfe F. Methotrexate and mortality in patients with rheumatoid arthritis: a prospective study. Lancet. 2002;359:1173–1177. doi:10.1016/S0140-6736(02)08213-2
45. Solomon DH, Avorn J, Katz JN, et al. Immunosuppressive medications and hospitalization for cardiovascular events in patients with rheumatoid arthritis. Arthritis Rheum. 2006;54:3790–3798. doi:10.1002/art.22255
46. Back M, Hansson GK. Anti-inflammatory therapies for atherosclerosis. Nat Rev Cardiol. 2015;12:199–211. doi:10.1038/nrcardio.2015.5
47. Whittle SL, Hughes RA. Folate supplementation and methotrexate treatment in rheumatoid arthritis: a review. Rheumatology (Oxford). 2004;43:267–271. doi:10.1093/rheumatology/keh088
48. Stern RS, Fitzgerald E, Ellis CN, Lowe N, Goldfarb MT, Baughman RD. The safety of etretinate as long-term therapy for psoriasis: results of the etretinate follow-up study. J Am Acad Dermatol. 1995;33:44–52. doi:10.1016/0190-9622(95)90008-X
49. Lerner DJ, Kannel WB. Patterns of coronary heart disease morbidity and mortality in the sexes: a 26-year follow-up of the Framingham population. Am Heart J. 1986;111:383–390. doi:10.1016/0002-8703(86)90155-9
50. Elveback LR, Connolly DC, Melton LJ
51. Menter A, Korman NJ, Elmets CA, et al. Guidelines of care for the management of psoriasis and psoriatic arthritis: section 4. Guidelines of care for the management and treatment of psoriasis with traditional systemic agents. J Am Acad Dermatol. 2009;61:451–485. doi:10.1016/j.jaad.2009.03.027
52. Atzeni F, Rodríguez-Carrio J, Popa CD, Nurmohamed MT, Szűcs G, Szekanecz Z. Cardiovascular effects of approved drugs for rheumatoid arthritis. Nat Rev Rheumatol. 2021;17:270–290.
53. Schneeweiss S. A basic study design for expedited safety signal evaluation based on electronic healthcare data. Pharmacoepidemiol Drug Saf. 2010;19:858–868. doi:10.1002/pds.1926
54. Pocock SJ. Clinical trials with multiple outcomes: a statistical perspective on their design, analysis, and interpretation. Control Clin Trials. 1997;18:
55. Rothman KJ. No adjustments are needed for multiple comparisons. Epidemiology. 1990;1:43–46. doi:10.1097/00001648-199001000-00010
56. Feise RJ. Do multiple outcome measures require p-value adjustment? BMC Med Res Methodol. 2002;2:8. doi:10.1186/1471-2288-2-8
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.