")
Back to Journals » Cancer Management and Research » Volume 12
Cardiotoxic Profile and Arterial Stiffness of Adjuvant Chemotherapy for Colorectal Cancer
Authors Visvikis A, Kyvelou SM, Pietri P, Georgakopoulos C, Manousou K, Tousoulis D, Stefanadis C, Vlachopoulos C, Pektasides D
Received 12 July 2019
Accepted for publication 3 October 2019
Published 13 February 2020 Volume 2020:12 Pages 1175—1185
DOI https://doi.org/10.2147/CMAR.S223032
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Antonella D'Anneo
A Visvikis,1 SM Kyvelou,2 P Pietri,2 C Georgakopoulos,2 K Manousou,1 D Tousoulis,2 C Stefanadis,2 C Vlachopoulos,2 D Pektasides3
1Third Department of Medical Oncology, Agioi Anargyroi General Oncology Hospital of Kifissia, Athens, Greece; 2Cardiology Department, First Cardiology Clinic, Athens Medical School, Hippokration Hospital, Athens, Greece; 3Second Department of Internal Medicine, School of Medicine, University of Athens, Athens, Greece
Correspondence: SM Kyvelou
Cardiology Department, First Cardiology Clinic, Athens Medical School, Hippokration Hospital, Perikelous 97B, Kato Xalandri, Athens 15231, Greece
Tel +30 697283751
Email [email protected]
Background and Purpose: Even though new cancer therapies have improved the overall survival, in some cases they have been associated with adverse effects, including increased cardiotoxicity. The purpose of the present study was to assess the cardiovascular effects of adjuvant chemotherapy for colorectal cancer and mainly the impact on arterial stiffness indices.
Material and Methods: A total of 70 patients with non-metastatic colorectal cancer who were treated either with FOLFOX (n=16) or with XELOX (n=54) adjuvant chemotherapy were included in the study. All patients were subjected to full cardiovascular evaluation at the beginning and the end of chemotherapy. Arterial stiffness was assessed by means of pulse wave velocity (PWV) and augmentation index (Aix) and full laboratory examinations were conducted prior to, and soon after, the termination of chemotherapy.
Results: Patients exhibited significantly higher levels of carotid-radial PWV, carotid femoral RWV and Aix post-chemotherapy (p< 0.001); these findings remained significant when examined separately in each treatment subgroup (FOLFOX, XELOX). The observed changes were independent of treatment regimen and baseline patient characteristics. Univariate regression analyses showed that baseline PWVc-r and PWVc-f were the only factors associated with PWVc-r and PWVc-f change, while Aix change was independent of its baseline value.
Conclusion: There is a clear burden in arterial stiffness indices post-adjuvant chemotherapy for colorectal cancer in both chemotherapy groups. This is a finding of important clinical significance, however more prospective studies are required in order to encode the possible mechanisms involved.
Keywords: arterial stiffness, adjuvant chemotherapy, colorectal cancer
Introduction
Colorectal cancer remains a major cause of cancer mortality in the Western world regardless the gender. Despite that, the overall mortality has declined in the last 40 years in the developed world, mainly due to early diagnosis and better treatment modalities.1,2
Adjuvant chemotherapy aims at reducing the risk of relapse and death by eliminating residual micro-metastatic disease and according to the guidelines should be considered for all patients with high risk stage II disease (ie, presence of lymph nodes sampling <12, poor differential tumor, vascular lymphatic or perineural invasion, obstruction or perforation and pT4 stage) and patients with stage III.3
FOLFOX is an abbreviation for chemotherapy regimes 5-fluorouracil and oxaliplatin, whereas XELOX stands for chemotherapy with oxaliplatin and capecitabine. Common clinical adverse effects of 5-FU include myelosuppression, diarrhea, mucositis and for capecitabine hand and foot syndrome. Cardiotoxicity is less frequent and its prevalence varies between 1.6% and 8.5% for both chemotherapy strategies, mainly in patients without previous history of cardiovascular disease. The mechanisms involved are not fully exploited. To what extend the malignancy itself attributes to the cardiotoxicity remains unclear.4–6
Many researchers have speculated that cancer may share several risk factors with cardiovascular disease.7,8 It has been previously reported that patients with colorectal adenomas also have increased arterial stiffness indices which was attributed to a pathophysiologic interaction between obesity, cardiovascular risk factors and colon pathology.9
In this prospective study, we aimed to investigate changes in the cardiovascular profile and arterial stiffness indices in patients with non-metastatic colorectal cancer who received adjuvant chemotherapy and exploit possible mechanisms linked to the malignancy itself or the chemotherapy regime.
Materials and Methods
For the purposes of the study, 92 patients were recruited with non-metastatic colorectal cancer stages II and III who according to the guidelines were eligible to receive adjuvant chemotherapy. The study protocol, which was contacted between 2010 and 2016, has been revised and approved in 2010 by the Ethics Committee of Hippokration Hospital, Athens, Greece. The study protocol was designed and executed according to the Declaration of Helsinki. All patients provided their written consent prior to recruitment.
Past medical history was obtained from all the patients in order to exclude those who had known ischemic heart disease, recent (<6 months) cerebrovascular events, known heart failure, electric rhythm disturbances and background history of ventricular arrhythmia. Blood samples were collected from the antecubital vein between 0800 and 1000 hrs, with the patient in the sitting position for at least 10 mins and at least after an overnight fast. All tests were conducted in the same laboratories using the criteria of the World Health Organization.
Cardiovascular Evaluation
All patients prior to the initiation of chemotherapy and immediately after the completion of it were subjected to full cardiovascular evaluation including:
Blood Pressure Evaluation
For the diagnosis of arterial hypertension, we used the cut-off limits of (>140 mmHg) for systolic and (>90 mmHg) for diastolic blood pressure. Three separate measurements, 1 week apart, were conducted. A 2-week washout period preceded for every patient already on antihypertensive treatment. In each visit, blood pressure was measured three times with the patient in a sitting position after a 10–15 mins relaxation period. A mercury sphygmomanometer was used for all measurements, while the size of the cuff was adjusted accordingly. A 24 hrs ambulatory blood pressure monitoring (24hABPM, Spacelabs@) was carried out whenever considered appropriate.
Measurement of Arterial Properties
Arterial stiffness indices were assessed in the morning, in a special room with stable temperature. Subjects were requested to abstain from caffeine, smoking, and alcohol for at least 12 hrs prior to measurements. Systolic BP, diastolic BP, and heart rate were measured three times in both arms with an automatic mercury sphygmomanometer (Omron M4-I, CE 0197, Netherlands).
The arterial pulse was assessed by means of a validated system (SphygmoCor; AtCor Medical, Sydney, Australia), which uses the principle of applanation tonometry and appropriate acquisition and analysis software for noninvasive recording. A high fidelity micromanometer was placed under gentle pressure to the non-dominant hand radial artery. Twenty waveforms were applied and subsequently the software performed the analysis and Aix and ascending aortic pressure was obtained.
Augmentation indices of the central waveform were used as indices of wave reflection. AI was defined as augmented pressure divided by pulse pressure and expressed as a percentage. We calculated the time between the foot of the pressure wave and the injection point from which the aortic pulse pressure was finally derived. The interpretation of results was based upon the rule that higher AI levels suggest increased wave reflection peripherally and/or earlier return of the reflected wave second to increased PWV, and vice versa. Given that heart rate may affect AI levels, all values were automatically corrected for heart rate by the SphygmoCor software and therefore the AoAIx75 index was derived.15,16
Pulse wave velocity is the velocity at which the arterial pulse propagates through the circulation and it is by definition the distance traveled (Δχ) by the wave divided by the time (Δt) which allows the wave to travel that distance. The anatomy and the elastic properties of the arterial wall affect the final speed. For the calculation of PWVc-f, the pulse transit time was measured as well as the distance travelled between 2 recording sites (PWV = distance (m)/transit time (s)) with the Complior device (Complior; Dupont Medical, Pantin, France). Two different pulse waves were measured simultaneously at 2 sites (at the base of the neck for the common carotid and over the right-femoral artery) with 2 transducers. The distance was defined as (distance from the suprasternal notch to femoral artery) − (distance from the carotid artery to the suprasternal notch). It is generally considered as a simple noninvasive technique with good reproducibility. According to the European Society of Hypertension PWV values greater than 10 m/s can be considered as an independent marker of end-organ damage; however, there is still no universal agreement on fixed PWV threshold values.17,18
Other Measurements
All patients had a baseline electrocardiogram (ECG) followed by a repeat one after the completion of chemotherapy. Baseline echocardiographic studies were performed prior and after the end of chemotherapy cycles. Standard M-mode, 2-dimensional and Doppler images were obtained during breath-hold at end-expiration and measurements were obtained from the mean of 3 consecutive beats. Left ventricular systolic and diastolic function were assessed pre- and post-chemotherapy. Echocardiographic studies were performed in the cardiology department by the same operator each time. Tumor markers specific for each malignancy were also assessed before and after the last cycle of chemotherapy.
Chemotherapy
The patients included in the study were subjected to chemotherapy with either FOLFOX (Oxaliplatin and 5-FU infusion) for minimum of 6 cycles and with XELOX (oxaliplatin and capecitabine tablets) for 6 cycles. Precisely FOLFOX regime included Oxaliplatin 85mg/m2, leucovorin 200mg/m2, 5FU bolus dose of 400mg/m2 and 48 hrs 5FU infusion of 1200mg/m2. XELOX regime included Oxaliplatin 130mg/m2 followed by Xeloda 2gr/m2 oral tablets for 14 consecutive days. Patients who experienced severe side effects or did not present in the follow up measurements after the termination of therapy was excluded from the study. Twenty-two patients failed to continue the study. Twelve failed to attend cardiovascular follow up after the completion of chemotherapy, mainly because of commuting issues, since they were based in rural areas of Greece, whereas 10 experienced severe diarrhea and/or severe hand and foot syndrome, therefore chemotherapy was either adjusted or terminated prematurely.
Statistical Analysis
Mean (SD), median, IQR and range are used for presenting continuous variables, while categorical variables are presented as frequencies. To evaluate changes in parameters of interest after chemotherapy compared to baseline, the Wilcoxon signed-rank test was used. Univariable linear regression analyses were performed in order to identify factors significantly associated with the changes in SBP, Aix75, PWVc-r and PWVc-f, the change (after-before chemotherapy) was used as the dependent variable and baseline patient, treatment and laboratory characteristics (including gender, age, BMI, treatment type, treatment duration) were included as independent variables. All statistical analyses were performed using SAS University. Statistical significance was set at p=0.05 (two-sided).
Results
A total of 70 patients with non-metastatic colorectal cancer treated with adjuvant chemotherapy were finally included in the present study. Patients baseline characteristics are presented in Table 1, overall and by the treatment regimen (FOLFOX, N=16; XELOX N=54). The majority of patients were males (N=55, 78.6%) with mean age of 65 years.
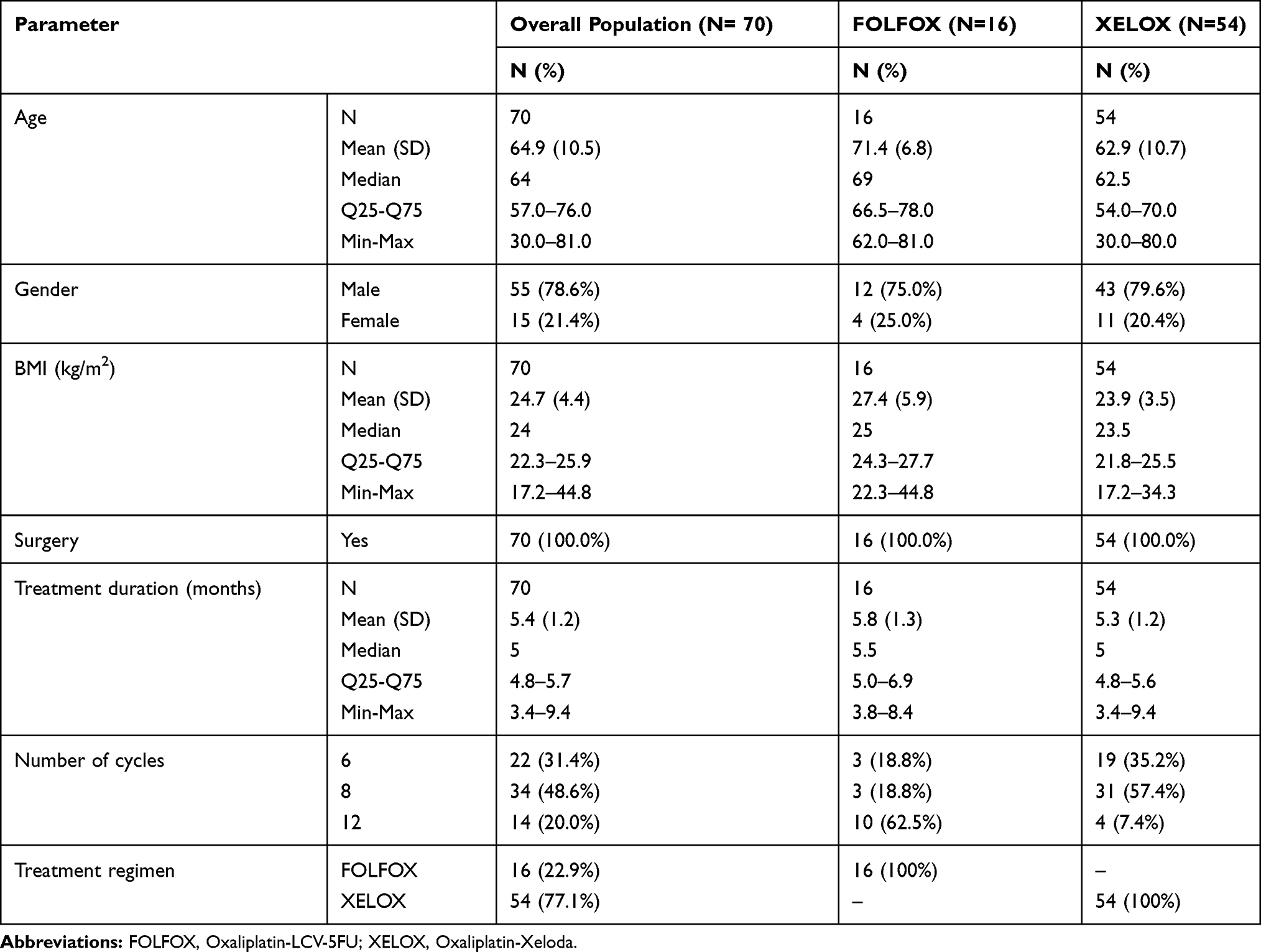 |
Table 1 Selected Patient and Treatment Characteristics in the Entire Cohort and by Treatment Regimen |
Vital signs, hemodynamic measurements and basic laboratory parameters pre- and post-chemotherapy are presented in Tables 2 and 3. In the entire cohort, a significant change post-chemotherapy was demonstrated for SBP (pre-chemotherapy: Median (min-Max)=130 (110–140)mmHg; post-chemotherapy: 135 (112–160)mmHg; p<0.001). No significant change in DBP was observed, while changes in the EF could not be evaluated due to all patients having the same EF measurement after chemotherapy (Table 2).
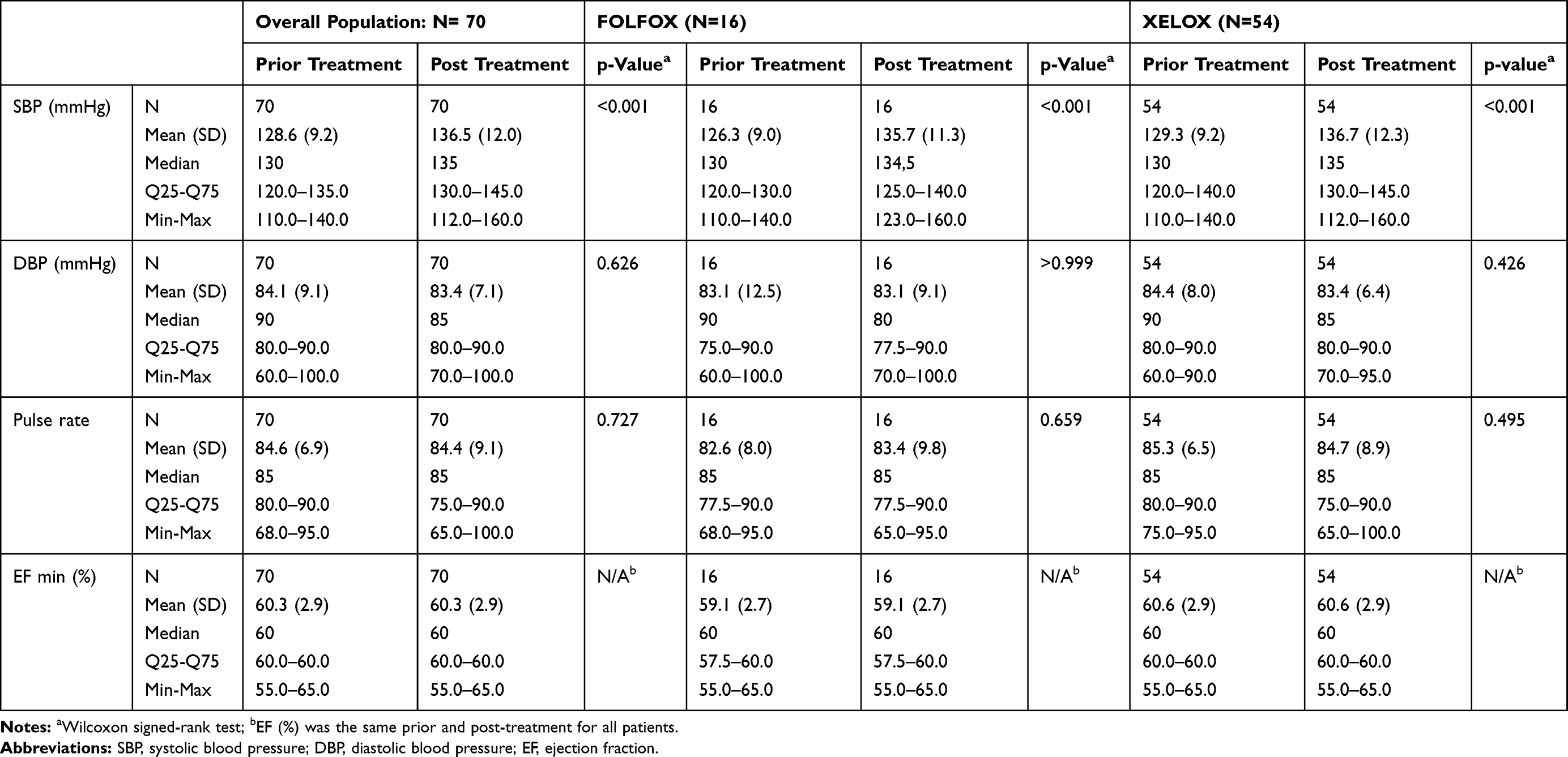 |
Table 2 Vital Signs (SBP, DBP, Pulse Rate and Ejection Fraction) Before and After Chemotherapy, in the Overall Population and by Treatment Cohort |
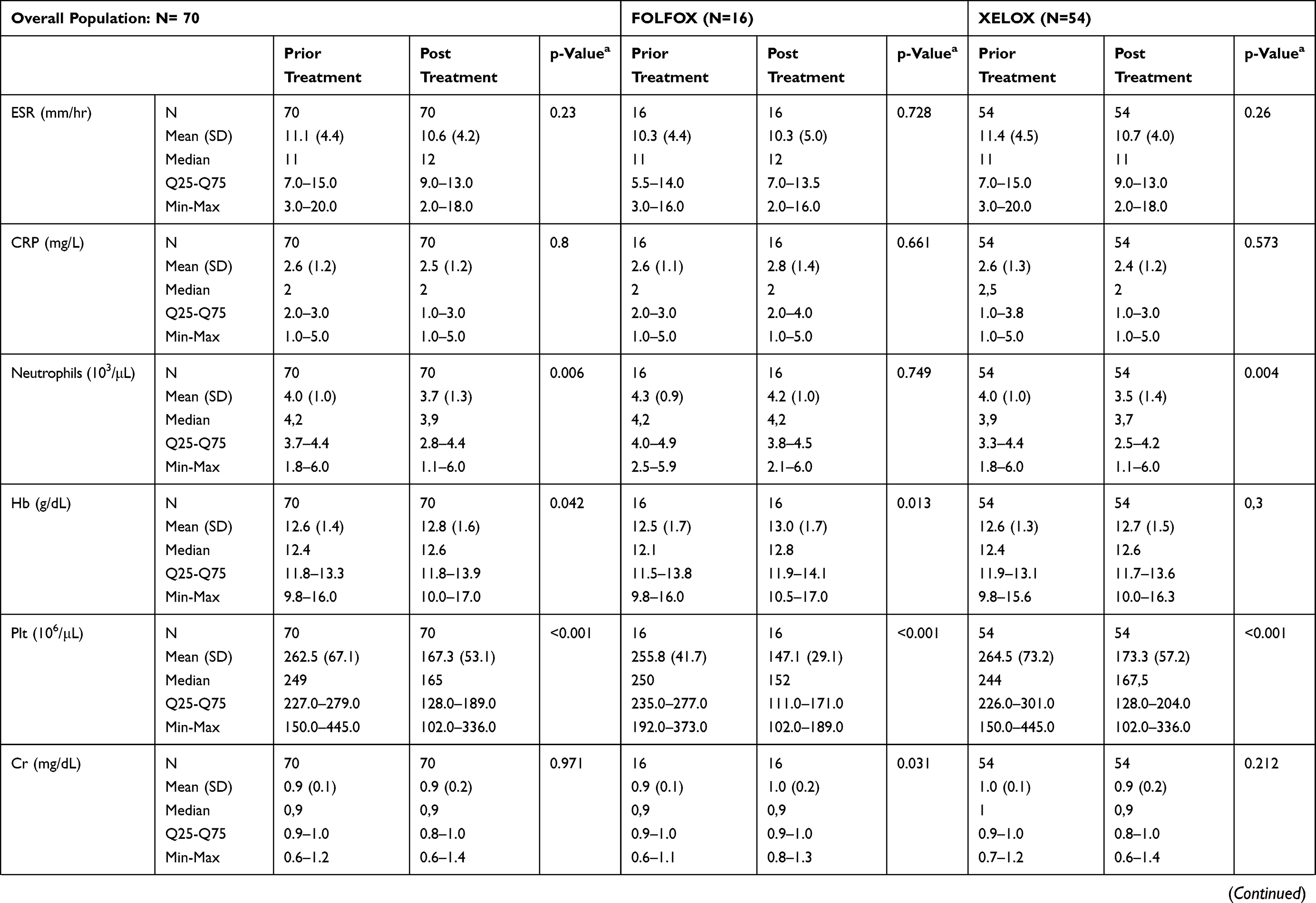 | 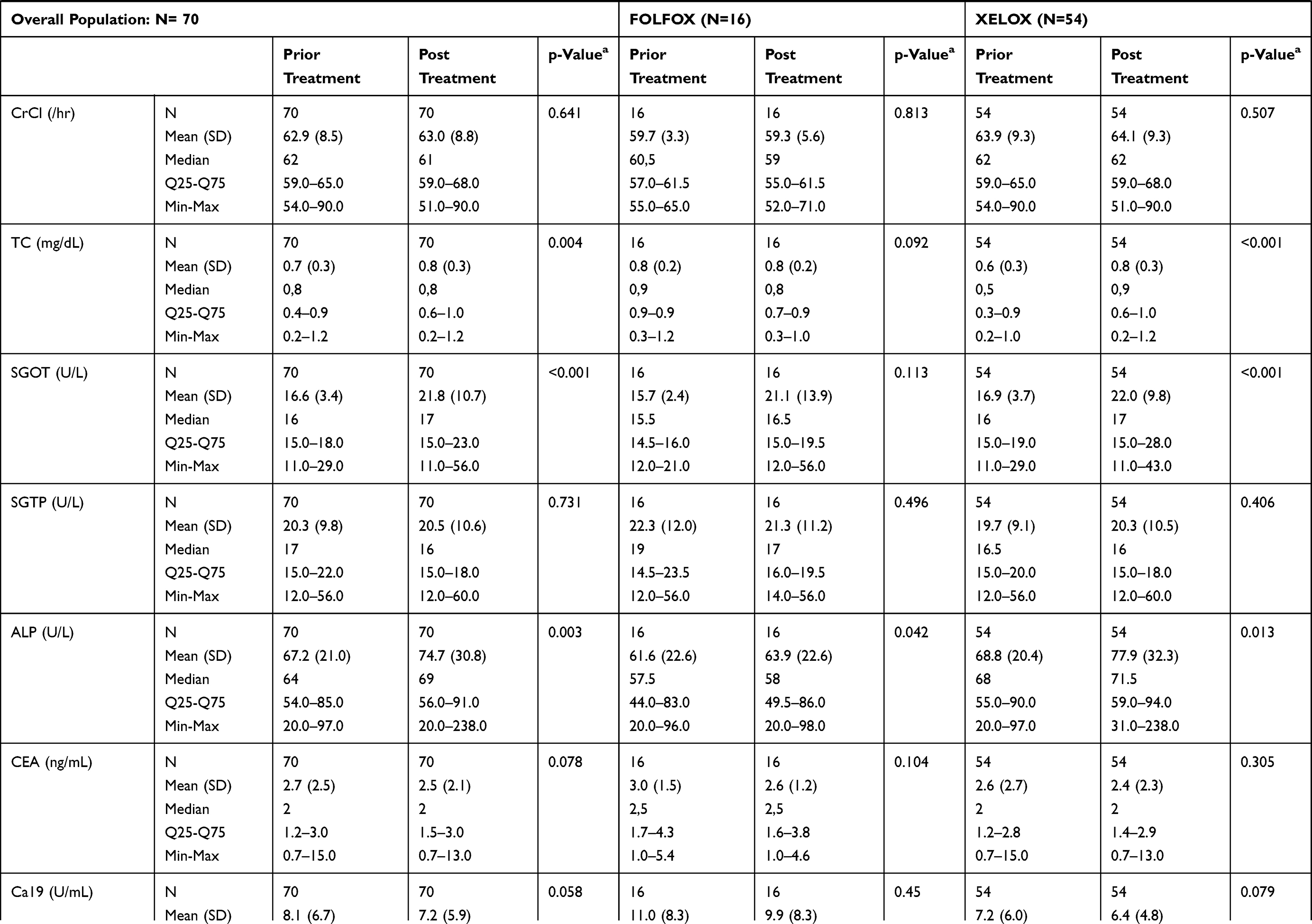 | 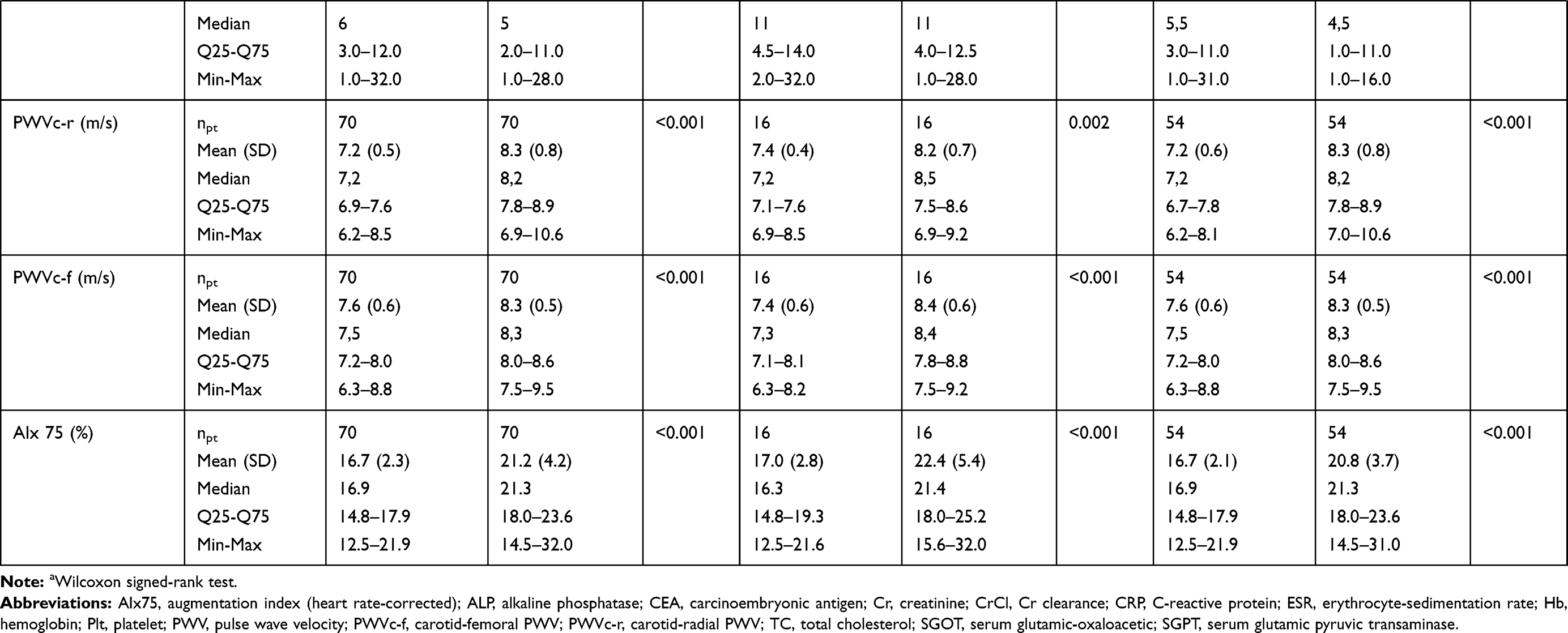 |
Table 3 Hemodynamic Measurements and Basic Laboratory Parameters Before and After Chemotherapy |
Regarding arterial stiffness indices, a significant change was observed in Aix75 (16.9% (12.5–21.9) vs 21.3% (14.5–32.0); p<0.001), PWVc-r (7.2(6.2–8.5) m/second vs 8.2 (6.9–10.6) m/second, p<0.001) and PWVc-f (7.5 (6.3–8.8) m/second vs 8.3 (7.5–9.5)m/second, p<0.001) (Table 3; Figures 1–3). The aforementioned changes were evident when examined separately in the subgroups defined by treatment regimen.
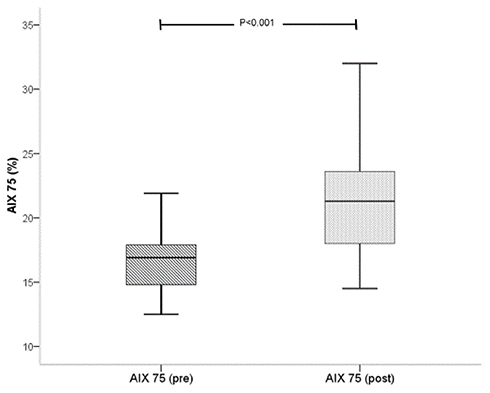 |
Figure 1 Distribution of AIX 75 (%) values pre- and post-chemotherapy. |
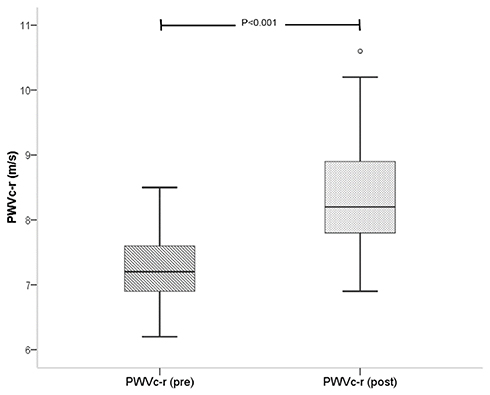 |
Figure 2 Distribution of PWVc-r (m/s) values pre- and post-chemotherapy. |
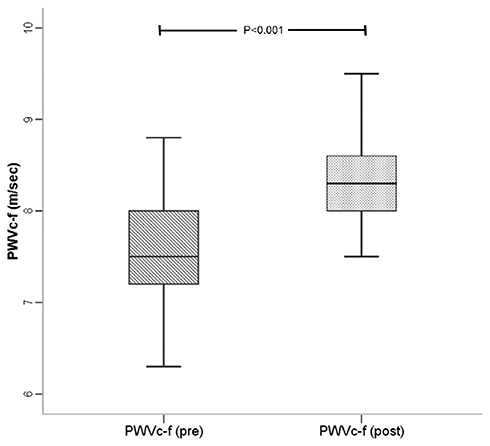 |
Figure 3 Distribution of PWVc-f values (m/s) pre- and post-chemotherapy. |
None of the factors examined in univariate regression analyses was significantly associated with SBP change post-chemotherapy. Regarding the arterial stiffness parameters, baseline PWVc-r (b=−0.91; 95% CI (−1.27, −0.56); p<0.001) and PWVc-f (b=−0.52; 95% CI: (−0.69, −0.34); p<0.001 were the only factors associated with PWVc-r and PWVc-f change, respectively. Finally, baseline Aix75 was not associated with Aix75 change (p=0.314); the only factor significantly associated with Aix75 change was baseline ALP (b=0.04; 95% CI: 0.00, 0.07, p=0.043).
Discussion
The main findings of this prospective study are shaped as follows: patients with non-metastatic colorectal cancer who are subjected to adjuvant chemotherapy have higher SBP levels post minimum 6 cycles of chemotherapy, whereas DBP and HR are not affected; arterial stiffness indices values increase significantly post-chemotherapy in the overall population as well as in the subgroup of each chemotherapy strategy. This rise in the values is affected by the baseline levels of PWV yet no such association was demonstrated for Aix. No difference was noted in EF pre- and post-chemotherapy. Up to date, this is the first study designed to assess arterial stiffness indices pre and post adjuvant chemotherapy for non-metastatic colorectal cancer.
Cardiovascular disease and colon adenomas, which can lead to colorectal cancer, share common pathophysiological mechanisms including inflammation, oxidative stress and insulin resistance.10 Arterial stiffness plays a pivotal role in atherosclerosis; therefore, PWV is an established marker of vascular damage and a leading marker to the diagnosis of atherosclerotic disease.11 It has been previously suggested that patients with colorectal adenomas have higher PWV12 indicating a causative relationship between cardiovascular disease and adenomas and a point of interest for bigger studies in order to unmask possible mechanisms and deem PWV as a risk predictor marker for colon adenomas.
In our study, PWV in patients with colorectal cancer rise post-chemotherapy and the rise noted was higher among those with greater PWV baseline values irrespectively of the chemotherapy strategy that was chosen. This suggests that there is an acute rather than a chronic effect on vascular damage on these patients (immediately post 6 to 8 cycles of chemotherapy). This could be explained by acutely induced endothelial dysfunction, increase in the smooth muscle tone, vasospasm, reduced NO synthesis which is in line with previous studies in metastatic malignancies and anthracycline chemotherapy.13,14 Similarly Aix, which is an indirect measurement of arterial stiffness, was higher post-chemotherapy irrespectively of HR and baseline Aix values. AI is a composite measure which is known to be largely affected by age, gender, height and heart rate.15,16 In our study, there was a clear burden post-chemotherapy in AI irrespectively of these cofounders which in turn points that malignancy itself and chemotherapy used can alter central hemodynamics in these patients. The rise in SBP noted post-chemotherapy as well as acute vasoconstriction caused by the chemotherapy regimen could possibly account for the rise in Aix75 values. This acute vascular toxicity noted could also be attributed to increased platelet-endothelial cell adhesion, enhanced procoagulant activity of macrophages, impaired protein C anticoagulant pathway and activation of tissue factor which all can potentially result in microthrombi formation and compromised blood flow, mechanisms that are common In malignancies.17,18
In our study, there was no difference noted in PWV and AIX change post-chemotherapy between FOLFOX and XELOX chemotherapy group.
FOLFOX cardiotoxicity has been mainly attributed to 5-FU infusion and its metabolites which is known to cause coronary vasospasm as well as direct cardiotoxicity on the myocytes and endothelial damage. The usual clinical presentation is that of angina during the infusion with codominant ECG changes. In our study, none of the 16 patients experienced angina and EF remained stable post-chemotherapy. However, the increase in arterial stiffness indices noted could be attributed to 5FU toxicity induced by endothelial damage and platelet and fibrin accumulation with increased thrombus formation which are experimentally linked to 5-FU.19–21 Additionally, the generation of metabolites of 5-FU is also known to serve as another mediator of cardiotoxicity.22,23
XELOX cardiotoxicity has mainly been attributed to capecitabine which is an oral prodrug of 5-fluorouracil. Even though capecitabine is considered an alternative to 5FU and its adverse effects still there are case reports of cardiovascular implication through coronary spasm, arrhythmias and acute cardiomyopathy. In our study population, none of the 54 patients who received XELOX experience any such adverse effects. However, the rise in the arterial stiffness markers could possibly be explained by the same mechanisms as 5-FU infusion.
The present study is prospective however its main limitation is the small number of participants. The lack of control group in obviously unethical still though a limitation. Further larger studies should be contacted in order to reproduce our results, therefore allow a safe generalization. Additionally, patients follow-up was after the termination of the chemotherapy. However, to assess the possible reversibility of the arterial stiffness increase seen in these patients, further measurement should have been contacted at least 6 months to a year post-chemotherapy. This could be a point of future analysis.
In conclusion, assessment of Aix and PWV and monitoring of cardiovascular risk factors in patients under adjuvant chemotherapy for non-metastatic colorectal cancer can identify asymptomatic patients with increase cardiovascular burden, possibly induced by chemotherapy, and therefore justify a closer monitor during and after chemotherapy. However, larger cohort studies with a more prolonged follow up should be conducted in order to strengthen the initial hypothesis.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ferlay J, Steliarova-Foucher E, Lortet-Tieulent J, et al. Cancer incidence and mortality patterns in Europe: estimates for 40 countries in 2012. Eur J Cancer. 2013;49:1374–1403. doi:10.1016/j.ejca.2012.12.027
2. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015. CA Cancer J Clin. 2015;65:5–29. doi:10.3322/caac.21254
3. Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A. AJCC Cancer Staging Manual.
4. de Forni M, Malet-Martino MC, Jaillais P, et al. Cardiotoxicity of high-dose continuous infusion fluorouracil: a prospective clinical study. J Clin Oncol. 1992;10:1795–1801. doi:10.1200/JCO.1992.10.11.1795
5. Akhtar SS, Salim KP, Bano ZA. Symptomatic cardiotoxicity with high-dose 5-fluorouracil infusion: a prospective study. Oncology. 1993;50:441–444. doi:10.1159/000227226
6. Alter P, Herzum M, Soufi M, Schaefer JR, Maisch B. Cardiotoxicity of 5-fluorouracil. Cardiovasc Hematol Agents Med Chem. 2006;4:1–5. doi:10.2174/187152506775268785
7. Abdel-Rahman O. 5-Fluorouracil related cardiotoxicity; Findings from five randomized studies of 5-fluorouracil-based regimens in metastatic colorectal cancer. Clin Colorectal Cancer. 2019;1:58–63. doi:10.1016/j.clcc.2018.10.006
8. Murphy TK, Calle EE, Rodriguez C, Kahn HS, Thun MJ. Body mass index and colon cancer mortality in a large prospective study. Am J Epidemiol. 2000;152:847–854. doi:10.1093/aje/152.9.847
9. Komninou D, Ayonote A, Richie JP
10. Frezza EE, Wachtel MS, Chiriva-Internati M. Influence of obesity on the risk of developing colon cancer. Gut. 2006;55:285–291. doi:10.1136/gut.2005.073163
11. Yamashina A, Tomiyama H, Arai T, et al. Brachial-ankle pulse wave velocity as a marker of atherosclerotic vascular damage and cardiovascular risk. Hypertens Res. 2003;26:615–622. doi:10.1291/hypres.26.615
12. Lim YJ, Kwack WG, Lee YS, Hahm KB, Kim YK. Increased pulse wave velocity reflecting arterial stiffness in patients with colorectal adenomas. J Clin Biochem Nutr. 2010;47:261–265. doi:10.3164/jcbn.10-70
13. Res E, Kyvelou SM, Vlachopoulos C, et al. Metastatic malignancies and the effect on arterial stiffness and blood pressure levels: the possible role of chemotherapy. Onco Targets Ther. 2018;11:6785–6793. doi:10.2147/OTT
14. Xaplanteris P, Vlachopoulos C, Protogerou AD, et al. A clinical score for prediction of elevated aortic stiffness: derivation and validation in 3943 hypertensive patients. J Hypertens. 2019;37:339–346. doi:10.1097/HJH.0000000000001904
15. O’Rourke M, Adji A, Nichols WW, Vlachopoulos C, Edelman ER. Application of arterial hemodynamics to clinical practice: a testament to medical science in London. Artery Res. 2017;18:81–86. doi:10.1016/j.artres.2017.03.003
16. Janner JH, Godtfredsen NS, Ladelund S, Vestbo J, Prescott E. The association between aortic augmentation index and cardiovascular risk factors in a large unselected population. J Hum Hypertens. 2012;26:476–484. doi:10.1038/jhh.2011.59
17. Ben Aharon I, Bar Joseph H, Tzabari M, et al. Doxorubicin-induced vascular toxicity-targeting potential pathways may reduce procoagulant activity. PLoS One. 2013;8:9. doi:10.1371/journal.pone.0075157
18. Woodley-Cook J, Shin LY, Swystun L, Caruso S, Beaudin S, Liaw PC. Effects of the chemotherapeutic agent doxorubicin on the protein C anticoagulant pathway. Mol Cancer Ther. 2006;12:3303–3311. doi:10.1158/1535-7163.MCT-06-0154
19. Tsibiribi P, Bui-Xuan C, Bui-Xuan B, et al. Cardiac lesions induced by 5-fluorouracil in the rabbit. Hum Exp Toxicol. 2006;25:305–309. doi:10.1191/0960327106ht628oa
20. Thalambedu N, Khan Y. Fluorouracil (5FU)-induced cardiomyopathy. Cureus. 2019;11:7.
21. Guclu O, Doganlar O, Yuskel V, Dognalar ZB. FOLFIRI mediated toxicity in human aortic smooth muscle cells and possible amelioration with curcumin and quercetin. Cardiovasc Toxicol. 2019; 5. [epub ahead of print].
22. Muneoka K, Shirai Y, Yokoyama N, Wakai T, Hatakeyama K. 5-fluorouracil cardiotoxicity induced by alpha-fluro-beta-alanine. Int J Clin Oncol. 2005;10:441–443. doi:10.1007/s10147-005-0516-7
23. Chong JH, Ghosh AK. Coronary artery vasospasm induced by 5-fluorouracil: proposed mechanisms, existing management options and future directions. Interv Cardiol. 2019;2:89–94. doi:10.15420/icr.2019.12
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.