")
Back to Journals » Psychology Research and Behavior Management » Volume 12
Cardiorespiratory fitness as a mediator of the relationship between birth weight and cognition in school children
Authors Álvarez-Bueno C, Cavero-Redondo I, Díez-Fernández A , Pardo-Guijarro MJ, Sánchez-López M, Martínez-Vizcaíno V
Received 12 December 2018
Accepted for publication 21 February 2019
Published 10 April 2019 Volume 2019:12 Pages 255—262
DOI https://doi.org/10.2147/PRBM.S197945
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Celia Álvarez-Bueno,1 Iván Cavero-Redondo,1 Ana Díez-Fernández,1 Maria Jesús Pardo-Guijarro,1,2 Mairena Sánchez-López,1,3 Vicente Martínez-Vizcaíno1,4
1Health and Social Research Center, Universidad de Castilla-La Mancha, Cuenca, Castilla-La Mancha, Spain; 2School of Education, Universidad de Castilla-La Mancha, Cuenca, Castilla-La Mancha, Spain; 3School of Education, Universidad de Castilla-La Mancha, Ciudad Real, Castilla-La Mancha, Spain; 4Facultad de Ciencias de la Salud, Universidad Autónoma de Chile, Talca, Chile
Objectives: To examine differences in cognition parameters by birth weight categories and to analyze whether the relationships between birth weight and cognitive functions are mediated by cardiorespiratory fitness (CRF) in schoolchildren.
Methods: A cross-sectional study using a sample of 664 school children from the MOVI-Kids study. Variables: i) cognitive function measured by the Battery of General and Differential Aptitudes (BADyG); ii) birth weight, reported by parents; and iii) CRF (20-m shuttle run test). ANCOVA models were estimated to assess differences in cognitive function categories across birth weight and CRF categories. Mediation analysis was conducted with Hayes’ PROCESS macro.
Results: CRF is a full mediator of the association between birth weight with the verbal and numerical factors, and general intelligence; and is a partial mediator when logical reasoning and the spatial factor were the dependent variables. The available data suggest that, in schoolchildren, the influence of birth weight on cognitive function is mediated by CRF.
Conclusions: These findings highlight that children with lower birth weight values and lower fitness levels should be target subgroups to improve children’s cognition, in which long-life physical activity interventions at early ages are a priority.
Keywords: birth weight, fitness, academic performance, cognition, children
Introduction
Birth weight has become an international concern since according to WHO’s data 15.5% of all births, estimated as more than 20 million infants worldwide, are born with low birthweight.1 Birth weight is considered an absolute measure of intrauterine growth and an important neonatal outcome to ensure a children’s healthy start in life.2 Growing scientific evidence supports that birth weight is a predictor of physical and mental health,3 and that the increased risk of poorer health associated with lower birth weight values could be tracked from infancy to adulthood.4
Previous studies have described the association between birth weight and cognition; thus, lower birth weight could impair executive functions like flexibility, inhibition, planning and visuospatial and working memory.5 Additionally, lower birth weight values have been negatively related to general intelligence levels, learning processes and school behaviors,6 which are closely related with academic success.7 Furthermore, an inverse relationship between physical fitness parameters and birth weight has been established,8 especially for aerobic and neuromuscular fitness.9
Examining the effects of physical fitness on children’s cognition, it has been reported that higher levels of aerobic capacity have been associated to a better cognitive function and academic achievement.10–12 The positive association of aerobic capacity with cognition and academic achievement opens the possibility that cardiorespiratory fitness (CRF) could produce some effect in the relationship between birth weight and cognition. The mediation effect of CRF on the relationship between birth weight and academic achievement measured by grades has been previously explored among preadolescents.13 Nevertheless, it still remains unclear the possible mediator effect of CRF on the relationship between birth weight and schoolchildren’s specific cognition dimensions.
Thus, the aim of this study was twofold: i) to examine differences in cognition parameters by birth weight and CRF categories controlling for potential confounders or mediators and ii) to analyze whether the relationships between birth weight and cognitive functions are mediated by CRF in schoolchildren.
Methods
A cross-sectional study including baseline data from the MOVI-Kids study was conducted. This trial (NCT01971840) aimed to assess the effectiveness of a multidimensional physical activity intervention for preventing obesity, improving fitness and reducing cardiovascular risk in schoolchildren attending the last year of preschool and the first grade of primary school (aged 4–7 years). Recruitment, data collection and measurement procedures are extensively described elsewhere.14 The study protocol was approved by The Clinical Research Ethics Committee of the “Virgen de la Luz” Hospital in Cuenca, Spain. Children’s parents or legal tutors were informed about the objectives and methods of the study and asked for signing the written consent as a requirement to children participation in the study.
For the analyses of this study, we only included the primary school children (n=664), since cognition scale has not been validated for preschool children.
To minimize inter-observer variability, the variables were measured in each school in standardized conditions by trained investigators.
Height and weight were estimated twice with the kid shoeless and in light apparel. Height was measured with a wall stadiometer (Seca® 222, Vogel and Halke, Hamburg, Germany) with the child upstanding and the spine area contacting the backboard. Weight was estimated with a scale (Seca® 861, Vogel and Halke, Hamburg, Germany). The mean of the two estimations of height and weight was used to calculate body mass index (BMI [kg/m2]).
Birth weight was obtained by a self-administered questionnaire completed by the children’s parents.
Cognitive function was measured using the Battery of General and Differential Aptitudes (BADyG) scales, validated for Spanish children aged 6–8 years.15 This scale provides information for the following domains:
- Logical reasoning, which measures verbal intelligence and mental flexibility based on capacities of inductive reasoning (the process of using a rational, systematic series of steps based on procedures and previously given statements to arrive at a conclusion).
- Verbal factor, which measures the capacity of verbal reasoning and comprehension. Designed to provide a measure of overall verbal intellectual abilities.
- Numerical factor, which measures the speed and accuracy of simple mental calculation.
- Spatial factor, which measures the ability of less automatized reasoning, searching for changes in figures that maintain their size, distance, shape and relative positions.
- General intelligence, which summarizes positive correlations among different cognitive tasks, assuming that an individual’s performance in cognitive tasks is related to each other. It is calculated as the sum of two verbal tests, two numerical tests and two spatial tests.
The domains could score from 0 to 36 points, except for logical reasoning which could score a maximum of 54. Additionally, general intelligence could score a maximum of 108 points, including the domains of verbal, numerical and spatial factor.
The 20-m shuttle run test was performed to evaluate CRF.16 Children had to run between two lines 20 m apart following the rhythm established by beeps emitted with a pre-recorded audio track. Participants started to run at a velocity of 8.5 km/h, and this pace increased 0.5 km/h every minute. They continued the test until extenuation, where their last stage completed was recorded. Leger’s formula was used to obtain estimations of maximal oxygen consumption (VO2max) ((31.025+(3.238×velocity)–(3.248×age)+(0.1536×age×velocity)).
Parental socioeconomic status (SES) data were collected by either the father or the mother with different self-reported questions of occupation and education. An index of SES was calculated according to the scale proposed by the Spanish Society of Epidemiology,17 with the items referred to both, the education and occupation of the parents, obtaining the following SES categories: lower, lower middle, middle, upper middle and upper.
The normality of continuous variables was checked using both statistical (the Kolmogorov–Smirnov test) and graphical (normal probability plot) procedures. Descriptive data were presented as mean and standard deviation (SD). Differences between boys and girls in quantitative variables were tested using the Student’s t-test. To examine the relationship between BMI, birth weight and CRF by sex, controlling for age in months, partial correlations coefficients were calculated.
After categorizing birth weight as low (<2.500 g) and normal (>2.500 g), according to the World Health Organization (WHO),18 analysis of covariance (ANCOVA) models were calculated to assess mean differences in cognition variables between birth weight (low and normal) and CRF categories (poor: first quartile, medium: second and third quartiles, and good: fourth quartile) controlling for age in months, sex, BMI and SES (model 1); depending on the fixed factor, a further adjustment using CRF or birth weight was analyzed in model 2.
To examine whether the association between birth weight and cognition parameters was mediated by CRF, mediation models were calculated using the PROCESS macro, developed by Hayes for SPSS.19 A total (c) and direct effects (a, b, c’) were extracted from the analysis, as indicated by the unstandardized regression coefficient between the variables in each model. Finally, the indirect effect (IE), calculated as the product of the a*b coefficient was obtained, which indicates the change in cognition variables for every unit of change in birth weight that was mediated by the proposed mediator. Age in months, sex, BMI and SES were included as covariates in every mediation model.
A resampling procedure of 10,000 bootstrap samples was conducted for testing mediation hypotheses, as recommended by Preacher and Hayes.20 Point estimates and corresponding 95% confidence intervals were estimated for the IE. Additionally, we tested mediation according to Sobel,21 dividing the IE by its standard error and performing a z test under the null hypothesis that the IE is equal to zero. Finally, the percentage of mediation was calculated as a ratio of IE to total effect.
The statistical significance was set at p≤0.05, and the analyses were performed using the software IBM SPSS 24 (SPSS Inc., Chicago, IL).
Results
From a total sample of 1604 participants included in the MOVI-Kids study, 664 schoolchildren (343 girls, 51.65%) from the first grade (6–7 years) who had valid data were included in this study. Children who accepted to participate were not different in age or sex from those who did not. Table 1 presents the characteristics of the study sample. Mean birth weight and CRF is lower in girls compared to boys (p≤0.05). There are no statistically significant differences in BMI and cognition variables, except for numerical factor, in which boys scored higher (p=0.012).
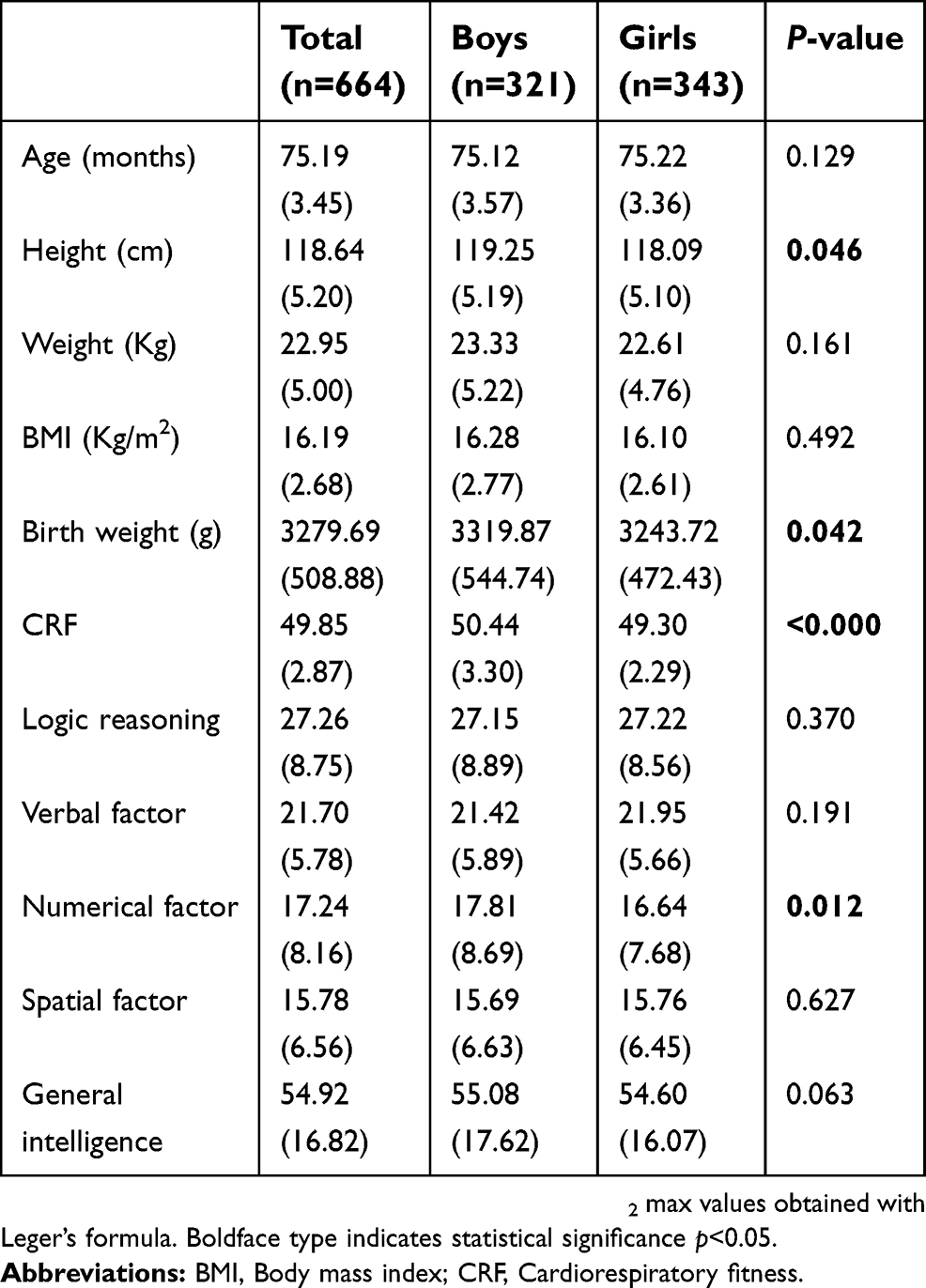 | Table 1 Characteristics of the study sample |
Table 2 shows partial correlation coefficients between CRF, birth weight and cognition variables, controlling for age and sex. Birth weight is positively associated to logical reasoning, spatial factor and general intelligence (p<0.05). CRF has a positive association with all cognition variables (range of values from 0.18 to 0.27; p<0.001).
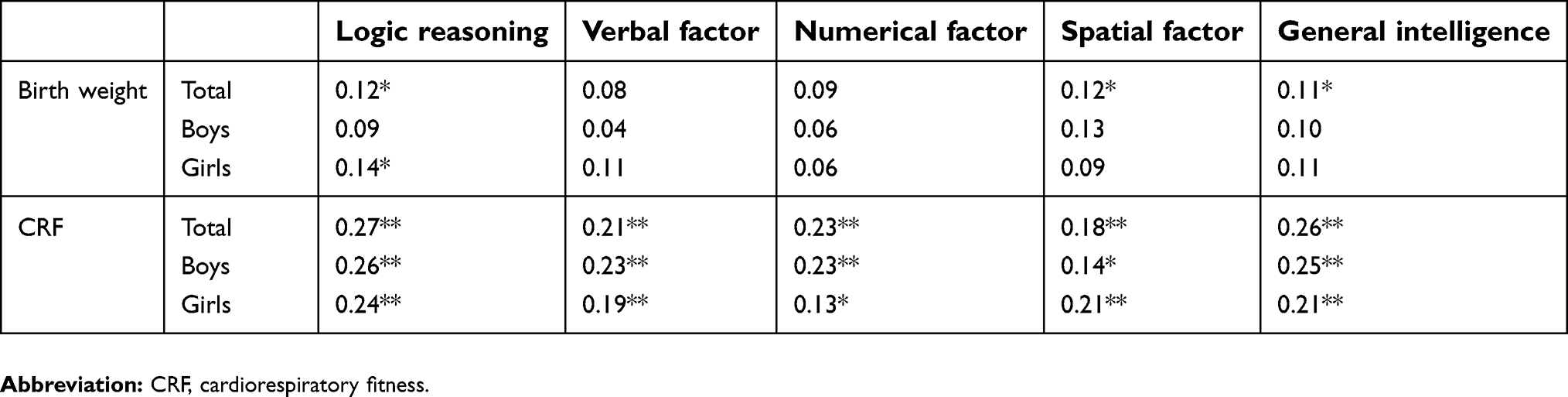 | Table 2 Pearson correlation coefficients (r) of cognition with birth weight and CRF parameters, controlling for age (in months) and sex |
Mean differences in cognition variables by CRF categories, controlling for age, sex, BMI and SES are shown in model 1 (Table 3). Overall, children in the higher CRF categories score better in all cognition variables (p<0.01), except for spatial factor, in which differences across CRF categories are not found (p=0.095). When birth weight is included as a covariate (model 2), differences remain similar in all variables.
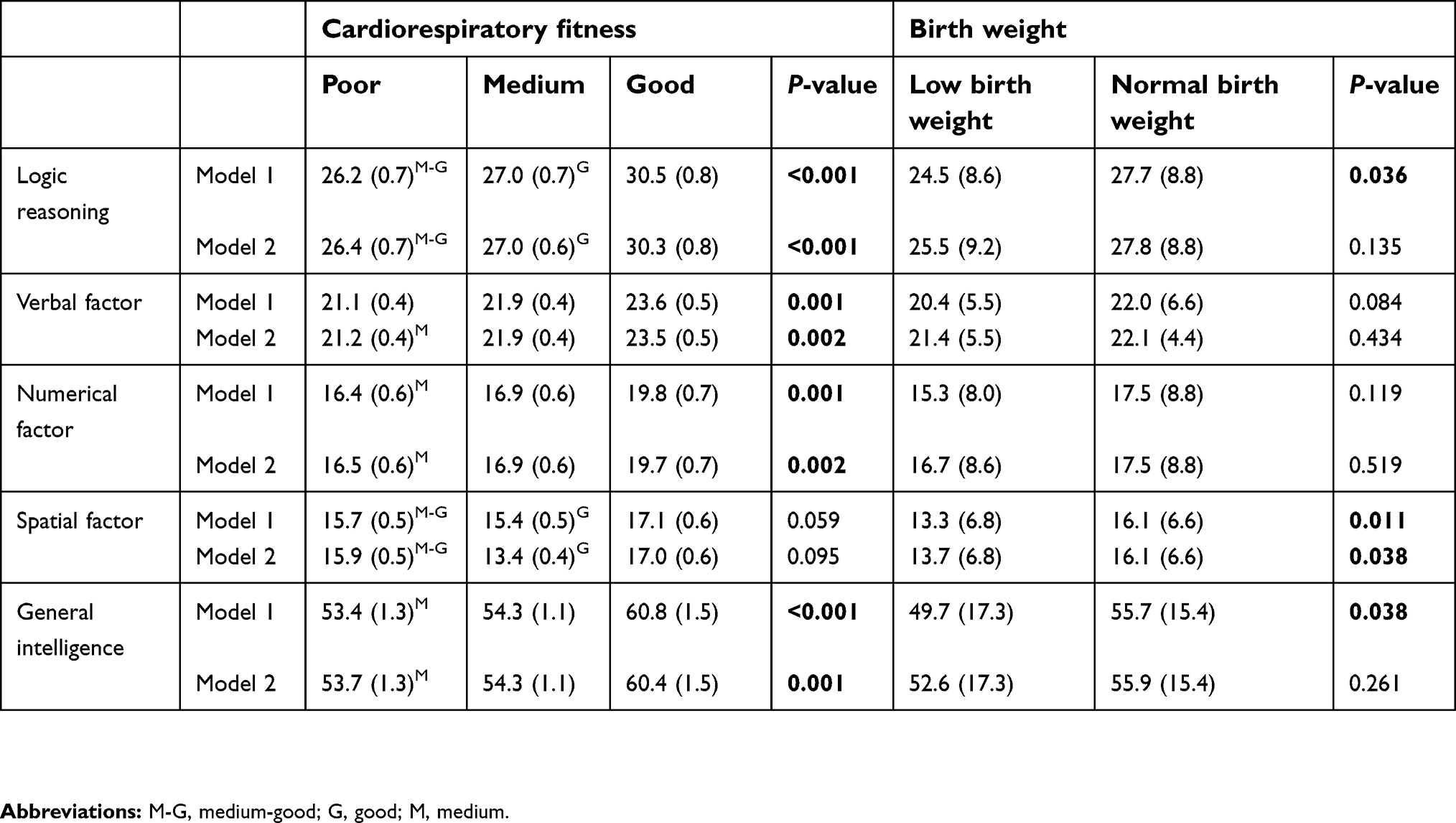 | Table 3 Mean differences (SE) in cognition variables by cardiorespiratory fitness and birth weight categories |
In addition, model 1 of birth weight categories (including age, sex, BMI and SES as covariates) shows that, as compared with low birth weight, children classified as normal birth weight score better in all cognition variables, although only differences in logical reasoning, spatial factor and general intelligence are statistically significant (p≤0.05). When CRF is included as a covariate (model 2), differences in the mean cognition parameters by birth weight categories are mitigated, remaining statistical significance only for the spatial factor dimension (p=0.038) (Table 3).
Mediation analysis results are presented in Figure 1. In general terms, CRF acts as a mediator between birth weight and all cognition variables. Birth weight is positively related with CRF (path a) (p<0.001). The total effect (path c) is also significant between birth weight and the dependent variable (logical reasoning, verbal factor, numerical factor, spatial factor or general intelligence) (p<0.05). The last step of the mediation process shows that the potential mediator has a positive relationship with the dependent variable (path b) (p<0.05), but when including both birth weight and CRF in the model (path c’), a significant decrease in the regression coefficient is shown. Finally, the IE is significant in all models, in such a way that CRF proved to be a full mediator between birth weight and verbal factor (percentage mediated [%Med]=35.5; p=0.008), numerical factor (%Med=31.7; p=0.009) and general intelligence (%Med=28.6; p=0.006). Likewise, CRF proved to be a partial mediator in logical reasoning (%Med=29.4, p=0.005) and spatial factor (%Med=16.2, p=0.029).
 | Figure 1 Mediation models testing whether the relationship between birth weight and cognition variables was mediated by cardiorespiratory fitness (CRF), controlling for age (months), sex, socioeconomic status and body mass index. Notes: *p<0.05; **p<0.001.Abbreviations: IE (95%CI), Indirect Effect (95% Confidence Interval); %Med, percentage mediated by proposed mediator. Symbols. |
Discussion
To our knowledge, this is the first study in primary schoolchildren that examines the influence of CRF in the relationship between birth weight and cognitive function using mediation analysis procedures. Our data show that low birth weight children scored lower in all cognition variables than their normal birth weight peers after controlling for potential confounders. Furthermore, children with higher CRF have better cognition functions than their lower aerobic capacity peers. Lastly, CRF fully mediates the relationship between birth weight and verbal factor, numerical factor and general intelligence; and partially the relationship with logical reasoning and spatial factor.
Our results support that children with lower birth weight scored worse in cognition domains than their normal weight peers. Birth weight has been shown to influence the development of the brain from in utero to the second decade of life.22 Previous research has suggested that structural brain alterations might be behind the cognitive impairments in lower birth weight infants.23 Although some compensatory brain mechanisms to cope with functional deficits have been described,24 these negative effects could be reflected in worst cognitive function and academic achievement scores.25
Furthermore, our findings indicate that children with higher CRF scored better in cognitive outcomes, this relationship remains after controlling for birth weight and other confounders. These results align with previous studies reporting that children with higher fitness levels score higher in reaction time and response accuracy,26 have better integrity of cognitive control processes27 and perform better on academic achievement, than their less fit peers.10–12,28 Additionally, longitudinal studies support that positive changes in aerobic capacity could be translated into better cognitive scores and academic achievement.29,30
Our study, using a battery including specific dimensions of cognition (general intelligence, logic reasoning, verbal factor, numerical factor and spatial factor), suggests that CRF has a mediation effect in between birth weight and cognition in 6–7-year-old children. Previous research has tested the mediation effect of aerobic capacity between birth weight and academic achievement in preadolescents.13 Together, these findings highlight that the negative effect of lower birth weight on cognition could be mitigated by improving children’s aerobic capacity and that the positive effect of CRF in the relationship between birth weight and cognition could be finally reflected in better academic achievement and behaviors .7
The effects of CRF on the brain structure and function have been related to better cognitive functions and have been proposed to explain the positive effects of CRF on cognition. First, CRF promotes structural changes in some brain-specific structures and enhance white matter, which are closely related to cognitive functions.31–33 Additionally, CRF promotes functional activity by increasing angiogenesis, neurogenesis and the levels of neurotransmitters.34
Overall, our findings support that CRF mediates the relationship between birth weight and specific cognition domains. Although cross-sectional in nature, these results suggest that the potentially deleterious effect of lower birth weight on brain structures and function could be partially or totally avoided through the effect of CRF. Improvements in CRF should be considered as useful mechanisms to reduce the negative effect of lower birth weight on cognition domains, which will be expressed on academic achievement since early age in life. These findings might attract attention to the development of different environment interventions of physical activity with the objective of increasing children’s CRF, since physical activity behaviors are acquired at early ages. Parents, schools and communities should provide children with novel opportunities to be active, particularly those with lower birth weight.
There are several limitations of the present study that should be stated; i) the cross-sectional design prevents us from making causal inferences. However, it is possible to argue that the temporal ambiguity that threatens cross-sectional study, could be minimized because birth weight precedes cognition levels at 6–7 years of age. Regardless, prospective studies should be implemented to clearly establish the temporality of these relationships. ii) Although 20-m shuttle run test has been proven to have good validity and reliability, we did not use the gold standard to measure CRF. iii) We did not take into account other health-related physical fitness components, which could have amplified the understanding of the benefits of physical fitness on academic achievement. Future advanced analysis with multiple mediator models or structural equation procedures might be carried out to enlighten the potential mediator role of different health-related fitness dimensions. iv) Children weighting more than 4,000 g at birth were included in this study; a sensitivity mediation analysis removing children who were macrosomic at birth showed similar results. v) Birth weight, cognition function and CRF relationships could be potentially confounded by other sociodemographic variables that we have not included in the statistical models. vi) Finally, children who were born preterm were not excluded from the analysis, and this fact should be cautiously considered when interpreting the results.
Our data revealed that after controlling for potential confounders, as compared to low birth weight, normal birth weight children scored higher in all cognition variables. Furthermore, children with higher CRF have better cognition functions than their lower aerobic capacity peers. Lastly, CRF fully mediates the relationship between birth weight and verbal factor, numerical factor and general intelligence; and partially the relationship with logical reasoning and spatial factor. These results alert for the importance of implementing interventions aimed at improving and maintaining schoolchildren’s health-related physical fitness. Specially, children with both lower birth weight values and low fitness levels, detected by screening programs in clinical or school settings, should be target subgroups in which long-life physical activity interventions are a priority.
Data sharing statement
The database generated and analyzed during the current cross-sectional study is available from the corresponding author after reasonable request.
Acknowledgments
We would like to thank all schools, families and pupils for their enthusiastic participation in the study. In addition to the authors in the Movi-Kids Study Group, the following are included: Fernando Salcedo Aguilar, Diana P. Pozuelo Carrascosa, Blanca Notario Pacheco, Jorge Cañete García Prieto, Coral Estefanía Torrijos Niño, Alberto González García, Pablo Franquelo Morales, José Luis Santos Gómez, Jorge Mota, María Martínez Andrés, Natalia Arias Palencia, Marta Guijarro Herraiz, Sergio Jiménez Suarez, Julián Gil Martínez, Javier Álvarez Álvarez, Carlos Javier Piera Cejalvo, Patricia Picazo Serrano, Ricardo Martínez Olivas, Pablo Diego Madrid, Jennifer Rosa Martínez Rey, Inmaculada Navalón Cañas, Sara Albadalejo Arribas, Pedro Miguel Ribeiro da Silva, Francisco J. García Sánchez, Inmaculada Díaz Jiménez, David Gutiérrez Díaz del Campo, Roberto Gulias González, Mª José González López, Verónica Artalejo de Mora, Alberto Bermejo Cantarero, Julia Muñoz Pinilla, Marta Terán Boabén, Santiago Amador Ruiz, Antonio Sánchez Gavidia, Alberto José Cerrillo Urbina, Paloma Moreno Escobar, Minerva Velasco Abellán, Mª Ángeles Suarez Gómez, Abel Ruiz de la Hermosa Fernández-Infante, Laura Ruiz Hidalgo, Ana Isabel Cobo Cuenca, Silvia García Maján and Cristina González Arévalo. This study was funded by the Ministry of Economy and Competitiveness – Carlos III Health Institute and FEDER funds (FIS PI12/02400 and FIS PI12/00761). Additional funding was obtained from the Research Network on Preventative Activities and Health Promotion (Ref. – RD12/0005/0009). CAB is supported by a grant from the Spanish of Ministry of Education, Culture and Sport (FPU13/03137). ICR is supported by a grant from the University of Castilla-La Mancha (FPU13/01582).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Wardlaw TM, editor. Low Birthweight: Country, Regional and Global Estimates. New York: Unicef; 2004.
2. Malin GL, Morris RK, Riley R, Teune MJ, Khan KS. When is birthweight at term abnormally low? A systematic review and meta‐analysis of the association and predictive ability of current birthweight standards for neonatal outcomes. BJOG. 2014;121(5):515–526. doi:10.1111/1471-0528.12517
3. Linsell L, Malouf R, Morris J, Kurinczuk JJ, Marlow N. Prognostic factors for poor cognitive development in children born very preterm or with very low birth weight: a systematic review. JAMA Pediatr. 2015;169(12):1162–1172. doi:10.1001/jamapediatrics.2015.2175
4. Martinussen M, Flanders DW, Fischl B, et al. Segmental brain volumes and cognitive and perceptual correlates in 15-year-old adolescents with low birth weight. J Pediatr. 2009;155(6):848–853. doi:10.1016/j.jpeds.2009.06.015
5. Luu TM, Ment L, Allan W, Schneider K, Vohr BR. Executive and memory function in adolescents born very preterm. Pediatrics. 2011;127(3):e639–e646. doi:10.1542/peds.2010-1421
6. Shenkin SD, Starr JM, Deary IJ. Birth weight and cognitive ability in childhood: a systematic review. Psychol Bull. 2004;130(6):989–1013. doi:10.1037/0033-2909.130.6.989
7. Tomporowski PD, McCullick B, Pendleton DM, Pesce C. Exercise and children’s cognition: the role of exercise characteristics and a place for metacognition. J Sport Health Sci. 2015;4(1):47–55. doi:10.1016/j.jshs.2014.09.003
8. Donnelly J, Hillman C, Castelli D, et al. Physical activity, fitness, cognitive function, and academic achievement in children: a systematic review. Med Sci Sports Exerc. 2016;48(6):1197–1222. doi:10.1249/MSS.0000000000000901
9. van Deutekom AW, Chinapaw MJM, Vrijkotte TGM, Gemke RJBJ. The association of birth weight and infant growth with physical fitness at 8–9 years of age–the ABCD study. Int J Obes. 2015;39(4):593–600. doi:10.1038/ijo.2014.204
10. Raine LB, Lee HK, Saliba BJ. The influence of childhood aerobic fitness on learning and memory. PLoS One. 2016;8(9):e72666. doi:10.1371/journal.pone.0072666
11. Raine LB, Scudder MR, Saliba BJ, Kramer AF, Hillman CH. Aerobic fitness and context processing in preadolescent children. J Phys Act Health. 2016;13(1):94–101. doi:10.1123/jpah.2014-0468
12. Torrijos-Niño C, Martínez-Vizcaíno V, Pardo-Guijarro MJ, García-Prieto JC, Arias-Palencia NM, Sánchez-López M. Physical fitness, obesity, and academic achievement in schoolchildren. J Pediatr. 2014;165(1):104–109. doi:10.1016/j.jpeds.2014.02.041
13. García-Hermoso A. Aerobic capacity as a mediator of the influence of birth weight and school performance. J Dev Orig Health Dis. 2016;7(4):337–341. doi:10.1017/S204017441600012X
14. Martinez-Vizcaino V, Mota J, Solera-Martinez M, et al. Rationale and methods of a randomised cross-over cluster trial to assess the effectiveness of MOVI-KIDS on preventing obesity in pre-schoolers. BMC Public Health. 2015;15(1):176. doi:10.1186/s12889-015-1512-0
15. Yuste C. Batería de aptitudes diferenciales y generales. BADyG Gráfico-I Infantil. Madrid: CEPE; 2008.
16. Léger LA, Mercier D, Gadoury C, Lambert J. The multistage 20 metre shuttle run test for aerobic fitness. J Sports Sci. 1988;6(2):93–101. doi:10.1080/02640418808729800
17. Chilet-Rosell E, Alvarez-Dardet C, Domingo-Salvany A. Use of Spanish proposals for measuring social class in health sciences. Gac Sanit. 2012;26:566–569. doi:10.1016/j.gaceta.2011.10.014
18.
19. Hayes A. Introduction to Mediation, Moderation, and Conditional Process Analysis a Regression-Based Approach. New York: Guildford Press; 2013.
20. Preacher KJ, Hayes AF. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav Res Methods. 2008;40(3):879–891.
21. Sobel E. Asymptotic confidence intervals for indirect effects in structural equation models. Sociol Methodol. 1982;13:290–312. doi:10.2307/270723
22. Allin M, Henderson M, Suckling J, et al. Effects of very low birthweight on brain structure in adulthood. Dev Med Child Neurol. 2004;46(1):46–53.
23. Egaña-Ugrinovic G, Sanz-Cortes M, Figueras F, Couve-Perez C, Gratacõs E. Fetal MRI insular cortical morphometry and its association with neurobehavior in late-onset small-for-gestational-age fetuses. Ultrasound Obstet Gynecol. 2014;44(3):322–329. doi:10.1002/uog.13360
24. van Ettinger-Veenstra H, Widén C, Engström M, Karlsson T, Leijon I, Nelson N. Neuroimaging of decoding and language comprehension in young very low birth weight (VLBW) adolescents: indications for compensatory mechanisms. PLoS One. 2017;12(10):e0185571. doi:10.1371/journal.pone.0185571
25. Reidy N, Morgan A, Thompson DK, Inder TE, Doyle LW, Anderson PJ. Impaired language abilities and white matter abnormalities in children born very preterm and/or very low birth weight. J Pediatr. 2013;162(4):719–724. doi:10.1016/j.jpeds.2012.10.017
26. Kramer AF, Erickson KI. Capitalizing on cortical plasticity: influence of physical activity on cognition and brain function. Trends Cogn Sci. 2007;11(8):342–348. doi:10.1016/j.tics.2007.06.009
27. Chaddock L, Pontifex MB, Hillman CH, Kramer AF. A review of the relation of aerobic fitness and physical activity to brain structure and function in children. J Int Neuropsychol Soc. 2011;17(6):975–985. doi:10.1017/S1355617711000567
28. Chaddock-Heyman L, Erickson KI, Kienzler C, et al. The role of aerobic fitness in cortical thickness and mathematics achievement in preadolescent children. PLoS One. 2015;10(8):e0134115. doi:10.1371/journal.pone.0134115
29. Chen LJ, Fox KR, Ku PW, Taun CY. Fitness change and subsequent academic performance in adolescents. J Sch Health. 2013;83(9):631–638. doi:10.1111/josh.12109
30. Raine LB, Biggan JR, Baym CL, Saliba BJ, Cohen NJ, Hillman CH. Adolescent changes in aerobic fitness are related to changes in academic achievement. Pediatr Exerc Sci. 2018;30(1):106–114. doi:10.1123/pes.2015-0225
31. Chaddock L, Erickson KI, Prakash RS, et al. Basal ganglia volume is associated with aerobic fitness in preadolescent children. Dev Neurosci. 2010;32(3):249–256. doi:10.1159/000316648
32. Erickson KI, Voss MW, Prakash RS, et al. Exercise training increases size of hippocampus and improves memory. Proc Natl Acad Sci. 2011;108(7):3017–3022. doi:10.1073/pnas.1015950108
33. Krafft CE, Schaeffer DJ, Schwarz NF, et al. Improved frontoparietal white matter integrity in overweight children is associated with attendance at an after-school exercise program. Dev Neurosci. 2014;36(1):1–9. doi:10.1159/000356219
34. Hillman CH, Erickson KI, Kramer AF. Be smart, exercise your heart: exercise effects on brain and cognition. Nat Rev Neurosci. 2008;9(1):58–65. doi:10.1038/nrn2298
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.