Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Cardiopulmonary Exercise Testing for Prognostic Assessment of Clinical Outcomes in COPD: A Systematic Review and Meta-Analysis
Authors Staes M ![]() , Dong J, Gyselinck I, Everaerts S
, Dong J, Gyselinck I, Everaerts S ![]() , Janssens W
, Janssens W ![]()
Received 14 August 2025
Accepted for publication 9 March 2026
Published 1 April 2026 Volume 2026:21 560342
DOI https://doi.org/10.2147/COPD.S560342
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 6
Editor who approved publication: Prof. Dr. Richard Russell
Michaël Staes,1,2,* Jonas Dong,3,* Iwein Gyselinck,1,2 Stephanie Everaerts,1,2 Wim Janssens1,2
1Laboratory of Respiratory Diseases and Thoracic Surgery (BREATHE), Department of Chronic Diseases and Metabolism, KU Leuven, Leuven, Belgium; 2Clinical Department of Respiratory Diseases, University Hospitals Leuven, Leuven, Belgium; 3Faculty of Medicine, KU Leuven, Leuven, Belgium
*These authors contributed equally to this work
Correspondence: Wim Janssens, Laboratory of Respiratory Diseases and Thoracic Surgery (BREATHE), Department of Chronic Diseases and Metabolism, KU Leuven, Herestraat 49, Box 706, Leuven, 3000, Belgium, Email [email protected]
Abstract: Chronic obstructive pulmonary disease (COPD) is a heterogeneous, progressive lung disorder. Despite its high prevalence, predicting clinical outcomes remains challenging. Various cardiopulmonary exercise testing (CPET) variables have been suggested as prognostic markers in COPD, but their role in clinical practice remains unclear. After registration in PROSPERO (ID CRD42024569879), a literature search of the Pubmed, Embase, Web of Science, Cochrane library and Scopus databases was carried out in August 2024. Study selection followed the PRISMA guidelines. Prospective and retrospective cohort studies evaluating associations between CPET variables and clinical outcomes in patients with COPD were included. Risk of bias was evaluated using the QUIPS tool. Data were extracted and synthesized narratively. A random-effects meta-analysis was planned if multiple studies reported comparable CPET variables, outcomes, and effect measures. Sixteen articles were included, three of which had an overall high risk of bias. Peak oxygen uptake (VO2peak) was consistently associated with mortality in univariate analyses, but its independent prognostic value in multivariable models was inconsistent. A random-effects meta-analysis of three studies evaluating VO2peak expressed as mL/kg/min did not demonstrate a statistically significant independent association with mortality (pooled HR 0.94, 95% CI 0.87– 1.00; I2 = 63%). Ventilatory efficiency (VE/VCO2) was identified as a significant prognostic marker in multiple studies. Other CPET-derived variables failed to show an independent association with mortality, although heterogeneity in metrics and adjustment strategies limited comparability. Evidence for other CPET-derived variables and for predicting severe acute exacerbations of COPD (AECOPD) or hospitalization was limited and inconsistent. CPET-derived variables, particularly VO2peak and VE/VCO2, are associated with mortality in COPD, but evidence for their independent prognostic value and incremental benefit over established composite indices remains limited. Current data do not support routine use of CPET variables for prognostic stratification in COPD, apart from VO2peak as a marker of exercise capacity within the modified BODE index.
Keywords: pulmonary disease, chronic obstructive, cardiopulmonary exercise testing, prognosis, risk stratification
Introduction
Chronic Obstructive Pulmonary Disease (COPD) is a heterogeneous, progressive lung disorder, marked by persistent airflow obstruction and respiratory symptoms (eg. dyspnea, coughing and sputum production), which may acutely worsen during exacerbations. COPD is currently among the top three causes of death worldwide and represents a major global health burden.1,2
COPD severity is traditionally classified by the degree of airflow obstruction, assessed by the forced expiratory volume in one second (FEV1), but pulmonary function impairment alone is insufficient as a predictor of clinical outcomes such as mortality, lung transplantation and/or severe acute exacerbations.3 This limitation likely reflects the systemic nature of COPD, in which chronic inflammation also leads to extrapulmonary manifestations and/or comorbidities, such as skeletal muscle dysfunction and cardiovascular disease, negatively affecting functional capacity and prognosis.4 As a result, predicting outcomes in COPD remains challenging. To better capture this multisystemic involvement, composite prognostic scores are often used in clinical practice. The BODE index, which incorporates BMI, FEV1, dyspnea, and 6-minute walking distance (6MWD), predicts mortality more accurately than every individual component alone.2,3
Given its ability to provide detailed information on the integrative function of the respiratory, cardiovascular, muscular, and neurologic systems during exertion, the prognostic use of incremental cardiopulmonary exercise testing (CPET) in patients with COPD has been investigated.5,6 CPET is currently used in patients with COPD to detect coexisting conditions, to identify the mechanisms of exercise limitation and for exercise prescription, but not for risk stratification.2,6 The Global Initiative for Chronic Obstructive Lung Disease acknowledges peak oxygen uptake (VO2peak) as a measure of exercise capacity with prognostic relevance, but refrains from providing specific recommendations regarding its interpretation, thresholds, or clinical application.2 Moreover, CPET yields a wide range of additional physiological variables (Figure 1; Table 1), many of which reflect distinct pathophysiological domains of exercise intolerance and may therefore offer complementary prognostic information. Despite this physiological appeal and established use for other clinical indications, the prognostic value of CPET-derived variables in COPD has not been systematically synthesized.
 |
Table 1 Overview of Primary Noninvasive Cardiopulmonary Exercise Testing (CPET) Variables |
 |
Figure 1 Most common non-invasive measurements obtained during cardiopulmonary exercise testing (CPET), illustrated on a cycle ergometer. 1) Oxygen uptake (VO2), carbon dioxide production (VCO2) and ventilation (VE), 2) electrocardiogram (ECG) and heart rate (HR), 3) blood pressure, 4) peripheral oxygen saturation (SpO2), 5) work rate (W). |
The primary objective of this systematic review is to identify which CPET variables are most consistently associated with clinical outcomes in patients with COPD, including mortality, lung transplantation and severe acute exacerbations (AECOPDs). We aim to provide a comprehensive understanding of the clinical relevance of CPET as a prognostic tool for patients with COPD.
Methods
Study Registration and Search Strategy
The study protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO) on 16 July 2024 (ID CRD42024569879). A web-based literature search of the Pubmed, Embase, Web of Science, Cochrane library and Scopus databases was carried out on 5 August 2024. No date restrictions were applied. The complete search strategies for all databases are provided in the Supplementary Table 1. The search strategy was developed based on earlier work on search methods for prognostic factor systematic reviews.7,8
All search results were imported into EndNote 20 (Clarivate Analytics, Philadelphia, PA, USA), where duplicate records were identified and eliminated. The remaining articles were uploaded to the systematic review management platform Rayyan (Rayyan Systems Inc., Cambridge, MA, USA) for further screening.
Study Selection (Screening and Selection Criteria)
Study selection was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.9 Article screening was conducted in two stages: first based on article title and abstract and then followed by full-text screening. Both stages were independently carried out by two researchers (JD and MS). In case of disagreement, consensus was reached after discussion during a consensus meeting. Inclusion criteria were 1) prospective or retrospective cohort studies, 2) investigating patients with well-established diagnosis of COPD, 3) having performed at least one incremental CPET and 4) linking at least one CPET variable with a clinical outcome (eg. survival, lung transplantation, hospitalization rate or exacerbation rate), 5) published in English, Dutch, French or Spanish. Exclusion criteria were: 1) studies explicitly reporting inclusion of patients with overlapping conditions such as heart failure, asthma, or interstitial lung disease (ILD). Studies that did not report on comorbidities were retained unless overlap with other diseases was clearly described; 2) other publication types, including reviews, editorials, case reports, and conference abstracts; and 3) studies exclusively investigating invasive CPET measurements.
Data Extraction
All data from the included articles were extracted by one researcher (JD) into Microsoft Excel (version 16.0.17928.20336, Microsoft Corporation, Redmond, WA, USA) and subsequently verified by a second researcher (MS). If available, the extracted data included the first author, year of publication, country, study design, study dates, recruitment methodology, CPET methodology, study limitations, sample size and characteristics. Additionally, details on investigated CPET variables, statistical method(s) used and outcome(s) were recorded. Finally, key findings related to the prognostic value of CPET variables were also collected.
Risk of Bias Assessment
A bias assessment of the included articles was conducted independently by two reviewers (JD and MS) using the QUIPS tool.10 This tool evaluates the risk of bias across six domains: study participation, study attrition, prognostic factor measurement, outcome measurement for confounding variables, and statistical analysis and reporting. Each domain was rated as low, intermediate or high risk of bias. Disagreements between reviewers were resolved through discussion. Finally, an overall risk of bias was determined based on the ratings across domains. The overall risk of bias was at least as high as the highest risk of bias in any domain if at least two domains were rated at this level. Studies with a high overall risk of bias were retained in tables and figures for completeness and transparency. However, due to concerns regarding internal validity, these studies were not included in the narrative synthesis nor considered for quantitative pooling.11
Data Synthesis and Reporting
Study characteristics and key findings of all included studies were summarized descriptively in tabular form. A narrative, qualitative synthesis was planned for all included studies, except those with an overall high risk of bias, grouped by the investigated outcome and CPET variable. A meta-analysis was planned if at least two studies investigated the same CPET-derived variable using comparable definitions and units, assessed the same clinical outcome, and reported compatible effect estimates (eg. hazard ratios). Given the anticipated high heterogeneity among studies, a random-effects model was planned for statistical analysis. Statistical heterogeneity would be assessed using the I2 statistic, with predefined thresholds for low (<25%), moderate (25–50%), and high (>50%) heterogeneity. All analyses were planned to be performed using Python.
Results
Search results
The web-based literature search identified 8072 records. After identifying and removing duplicate records 5056 unique articles were screened. Title and abstract screening excluded 5033 articles, leaving 23 articles for full-text assessment. Of these, eight conference abstracts were excluded. Ultimately, 15 studies met the eligibility criteria and were included. One supplementary article (16) was added via reference tracking, bringing the total to 16 articles included in the systematic review (Table 2). The screening process is illustrated in a PRISMA flow diagram (Figure 2).
 |
Table 2 Key Characteristics of Included Studies |
 |
Figure 2 PRISMA flow diagram study selection.9 |
Study Characteristics
The included studies encompassed a wide range of COPD severity based on GOLD stages, with some primarily involving patients with mild COPD and others predominantly investigating patients with severe COPD. Among the 16 studies, seven (44%) were prospective12,14–16,24–26 and nine (56%) were retrospective.13,17–23,27 Sample sizes ranged from 30 to 449 patients, with a total study population of 2640 individuals. Overall, the study populations predominantly consisted of men (77%), with four out of 16 studies exclusively including male participants.12,13,24,25 The mean and median ages ranged from 61 to 70 years.
The majority of the studies (14/16; 88%) reported mortality as outcome. Most of them examined all-cause mortality (11/14; 79%),13–17,19,20,22–25 while two studies focused exclusively on respiratory-related mortality.12,26 One study additionally considered lung transplantation as a death-equivalent outcome.18 Severe AECOPD was reported in three out of 16 studies (19%).12,21,22 One study reported COPD-related hospitalization as outcome.27
Bias Assessment
Overall, the studies demonstrated a low risk of bias in the domains of prognostic and outcome measurement. In contrast, the domains of confounder adjustment, statistical analysis and reporting, and study participation more frequently showed a moderate to high risk of bias. No study was considered free of bias across all domains. Many prospective studies failed to adequately report information about the participants lost to follow-up, resulting in a high risk of bias in the study attrition domain. Because of a high overall risk of bias, three studies were described in Table 2 but not further included in the narrative review.12,14,25 The bias assessment for each domain across all studies is shown in Figure 3.
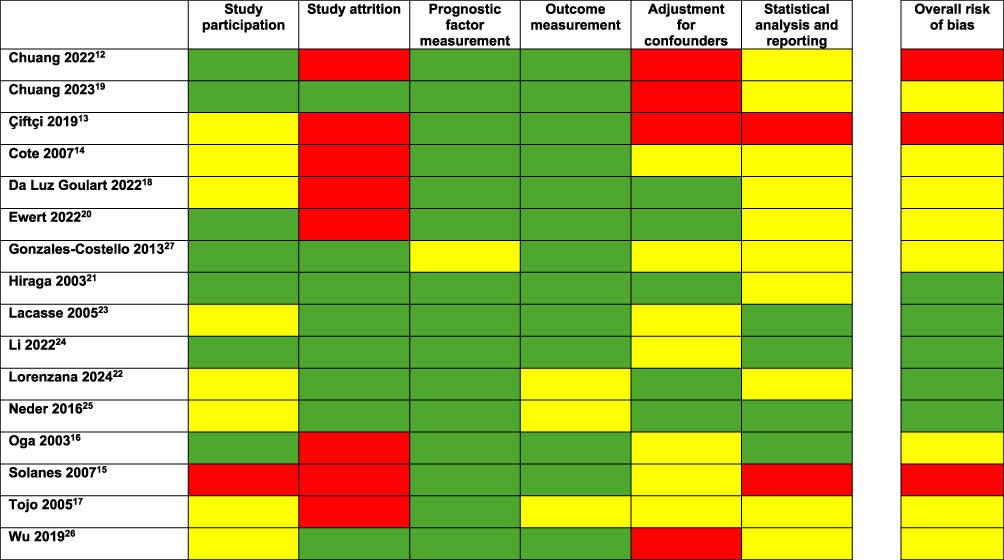 |
Figure 3 QUIPS bias tool assessment across all included studies. Green = Low risk of bias, Yellow = Moderate risk of bias, Red = High risk of bias. |
Prognostic Variables
Mortality
Maximal Oxygen Uptake (VO2peak)
The association between VO2peak and mortality was the most studied and was reported in 10 studies (of which one was excluded due to high risk of bias).12 There was substantial heterogeneity among studies in how VO2peak was analyzed (as a continuous or categorical variable), the metric used (percentage of the predicted value, mL/min/kg, or mL/min), the statistical methods applied, and the effect measures reported.
Figure 4 summarizes the results of all studies that reported VO2peak as a continuous variable using hazard ratios in relation to overall mortality. Three studies evaluated VO2peak expressed in mL/kg/min and reported multivariable-adjusted hazard ratios. In a random-effects meta-analysis of these studies, VO2peak was not significantly associated with mortality (pooled HR 0.94, 95% CI 0.87–1.00), with high heterogeneity (I2 = 63%). Five studies assessed VO2peak as a percentage of the predicted value.13,15,17,19,22 All five studies reported VO2peak as a predictor of mortality in univariate analysis, with only two studies reporting exact hazard ratios (0.97 and 0.98). However, after correcting for confounders, VO2peak remained significant in only two studies.17,22 Two studies found no correlation with overall survival in multivariate analysis13,15 and one study did not report it.19 Because several studies did not report (exact) effect estimates of multivariable findings, quantitative pooling of VO2peak expressed as percentage of the predicted value was not feasible. One study by González-Costello et al examined VO2peak as percentage of predicted in relation to a composite endpoint of death or lung transplantation (transplant-free survival) and reported a significant association in multivariate analysis (HR 0.98).18 Another study by Oga et al, who analyzed VO2peak as mL/min in 150 male patients, found a significant association with overall mortality in multivariate analysis (calculated RR 0.995).
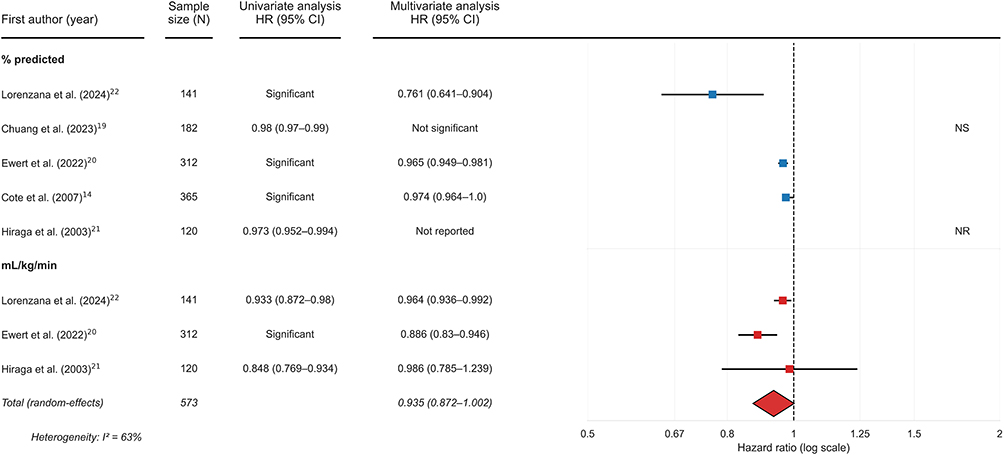 |
Figure 4 VO2peak as continuous variable using hazard ratios for overall mortality. A forest plot of the results from multivariate analysis is shown on the right, including a random-effects meta-analysis for the three studies reporting VO2 peak in mL/kg/min. Abbreviations: NS, not significant, NR, not reported. |
In addition, Neder et al analyzed VO2peak as a categorical variable using logistic regression.23 This study found that a VO2peak <75% of the predicted value was significantly correlated with overall mortality in univariate analysis. However, this association was lost after adjusting for confounders. In a study by da Luz Goulart et al, a VO2peak threshold of 13.8mL/kg/min was identified as a significant predictor of mortality, even after correction for age, sex, VE/VCO2 slope and peak ventilation.16
Peak Ventilation (VEpeak)
The prognostic value of VEpeak, in percentage of predicted or L/min, was reported in five studies.13,16,18,19,26 All but one studies examined all-cause or respiratory mortality as outcome, while González-Costello et al used transplant-free survival as outcome instead.18
In univariate analysis, a significant relationship with mortality was observed in all five studies. However, after adjusting for confounders, all four studies that analyzed VE peak as a continuous variable reported a loss of its predictive effect.13,18,19,26 In contrast, da Luz Goulart et al found that VEpeak ≤25.7L/min, when analyzed as a categorical variable, remained an independent predictor of prognosis in multivariate analysis.16 The variables adjusted for were largely the same across studies, including age and sex.
Ventilatory Efficiency (VE/VCO2)
The prognostic value of ventilatory efficiency was explored in four studies.13,16,18,23
Neder et al assessed the ventilatory efficiency as VE/VCO2 at nadir and found that a VE/VCO2 nadir >34 was an independent predictor of both all-cause and respiratory mortality, with a relative risk, in multivariate analysis, of 2.081 and 1.998, respectively. Similarly, Chuang et al evaluated VE/VCO2 at nadir or at anaerobic threshold as a continuous variable and also identified it as an independent predictor of mortality.
Da Luz Goulart et al and González-Costello et al examined the prognostic value of the VE/VCO2 slope. González-Costello et al evaluated a composite endpoint of survival or lung transplantation and constructed two multivariate regression models. The first model accounted for demographic variables as well as static and dynamic lung function parameters, resulting in the loss of VE/VCO2 slope’s predictive significance for all-cause mortality. However, given that 21% of patients lacked measurements of total lung capacity, diffusion capacity and/or residual volume, these variables were excluded in a second multivariate regression model, in which VE/VCO2 slope remained a significant independent predictor of mortality (HR 1.036). Da Luz Goulart et al similarly demonstrated a significant association between VE/VCO2 slope and mortality in multivariate analysis.
Peak Work Rate (Wpeak)
Wpeak was reported in four studies.13,20,22,26 Chuang et al and Lacasse et al reported Wpeak as percentage of the predicted value as a significant predictor in univariate analysis, however this significance was not maintained after adjustment for confounders. Lorenzana et al and Tojo et al examined Wpeak as watts. The findings of Lorenzana et al indicated that Wpeak was a significant independent predictor of all-cause mortality in univariate and multivariate analysis (HR 0.973). In contrast, Tojo et al did not observe a significant association with respiratory mortality in either univariate or multivariate analyses.26
Other Variables
Heart rate reserve (HRR, expressed as a percentage of the predicted or beats per minute) was examined in three studies.18–20 González-Costello et al (% predicted) reported a significant association with mortality, including lung transplantation as death equivalent, both in univariate and multivariate cox analysis. Similarly, Lacasse et al found that HRR (beats per minute), as a categorical variable with a threshold of 14 beats per minute, was an independent predictor of mortality, even after adjusting for confounders. In contrast, Hiraga et al (beats per minute) did not observe significant findings in their study.
Maximal oxygen pulse (O2P, measured as VO2 divided by heart rate) was examined in two studies.19,23 Hiraga et al and Neder et al investigated the value of maximal O2P, expressed as mL/beat, in predicting respiratory or all-cause mortality. Both studies showed significant results in univariate analysis. However, after adjusting for confounding variables these studies failed to identify O2P as an independent predictor of all-cause and respiratory mortality. The multivariate regression models adjusted for both static and dynamic lung function parameters as well as additional factors, including age and BMI.19,23
Dynamic hyperinflation, quantified either by the ratio of maximal tidal volume to total lung capacity or by the slope of the linear regression of end-expiratory lung volume as a function of time, was investigated in two studies.13,22 Both studies found a significant relationship between dynamic hyperinflation and mortality in multivariate analysis.
Breathing reserve (ratio of maximal ventilation (VE) to maximal voluntary ventilation (MVV),13 and the respiratory exchange ratio (ratio of VCO2 to VO2),18 were assessed in one study each. Both variables were not significant in multivariate analysis.
Severe AECOPD
Two studies investigated the role of CPET variables in predicting severe AECOPD.21,22
The value of VO2peak, expressed in mL/min, in predicting severe AECOPD was investigated by Li et al. This study failed to identify VO2peak as a significant independent predictor of severe AECOPD in multivariate analysis. Lorenzana et al examined the role of VO2peak as mL/min/kg and found that it was an independent predictor of severe AECOPD after adjustment for confounders, including sex, age, body mass index, pack-years and treatment with inhaled corticosteroids.
The association of Wpeak, expressed as watts or percentage of the predicted value, and severe AECOPD was also examined in both studies. Li et al failed to identify Wpeak as an independent predictor of severe AECOPD in multivariate analysis. Lorenzana et al, however, reported contradictory findings.
Li et al additionally investigated the predictive value of O2P peak (%pred). This study found a significant association with severe AECOPD in both univariate and multivariate analysis (odds ratio 1.062).
Hospitalization Rate
Wu et al used an independent t-test to evaluate differences in COPD-related hospitalizations between a group with normal peak O2P peak (≥80% pred) and a group with impaired peak O2P (<80% pred). The t-test resulted in a significant difference between the 2 groups, with the impaired O2P peak group experiencing significantly more COPD-related hospitalizations. However, no regression analysis was performed and subsequently no hazard or odds ratio was calculated.27
Discussion
This systematic review aimed to summarize the current evidence on the prognostic value of CPET in COPD. Following a rigorous screening and selection process, sixteen studies were included, each evaluating different CPET variables and outcomes.
Most evidence exists on the role of CPET to predict mortality, with VO2peak being the most studied variable. While all included studies show a clear association between VO2peak and mortality, its role as an independent risk factor is less clear. Our random-effects meta-analysis combining three studies that evaluated VO2peak expressed as mL/kg/min and reported multivariable-adjusted hazard ratios did not demonstrate a statistically significant independent association with mortality, despite a consistent direction of effect, and pooling of results expressing VO2peak as percentage of predicted could not be performed due to the lack of reporting of outcomes of nonsignificant findings. These findings reflect the integrative nature of exercise capacity, as measured by VO2peak, as it is determined by the interactive performance of multiple physiological systems, such as the respiratory, cardiovascular and muscle systems, and the presence of comorbid disease.28 As a result, even though its association with mortality is well established, VO2peak may lose statistical independence when its underlying components are corrected for in multivariable models.
Because of this association with mortality, exercise capacity is part of the most used prognostic composite score for patients with COPD, the BODE index. Therefore, comparing the use of only VO2 peak with such multidimensional score, already incorporating exercise capacity, does not seem useful. However, the original score used 6MWD as surrogate for exercise capacity, but a modified BODE index, replacing 6MWD with VO2peak was developed. Earlier studies comparing 6MWD and VO2peak found a significant but modest correlation.29,30 Additionally, Cote et al reported that both variables were equally good predictors of mortality in COPD.15 Studies by Cardoso et al and Lopez-Campos et al confirmed an excellent correlation between the modified BODE index and conventional BODE index, but its value to predict mortality was not investigated.31,32 In a retrospective cohort study, Cote et al found that the modified BODE index did not outperform the conventional BODE index in predicting mortality.33 Overall, these findings suggest that while VO2peak is a valuable prognostic marker, replacing 6MWD with VO2peak in the BODE index does not appear to provide additional predictive value. Furthermore, unlike the six-minute walking test, CPET requires expensive equipment and trained personnel, making the 6MWD the more practical and accessible option in clinical practice.34 However, in settings where CPET is already performed (eg., before pulmonary rehabilitation, during the work-up of unexplained dyspnea or to identify coexisting comorbidities), VO2peak can be used for prognostic assessment through the modified BODE index.
Elevated VE/VCO2, often interpreted as a marker of increased dead space ventilation, demonstrated consistent associations with mortality across all four included studies, often even after correcting for confounders. Unlike VO2peak, VE/VCO2, has the advantage of being a submaximal parameter, making it less dependent on patient effort. However, it should be noted that it may also be influenced by factors causing a lower arterial carbon dioxide tension set-point, such as hyperventilation.35 Because studies used different VE/VCO2 metrics - slope, nadir, or values at the anaerobic threshold- which can progress differently across COPD severity, quantitative pooling of findings was impossible. In advanced disease stages, mechanical constraints and hypercapnia often lead to a reduced VE/VCO2 slope (which is a well-established prognostic marker for patients with pulmonary hypertension36), while an increasing intercept may result in a stable nadir despite disease progression.37 From this physiological perspective, the VE/VCO2 intercept may represent an informative but currently unexplored parameter for risk stratification in COPD. Despite its promise, the current evidence base remains insufficient to support routine clinical use of VE/VCO2 for mortality prediction in COPD.
Other studied CPET variables, such as peak ventilation, peak work rate and peak oxygen pulse, failed to show an independent association with mortality and/or remain insufficiently studied, making them currently unsuitable as prognostic marker. Additionally, the role of CPET to predict severe AECOPD or hospitalization has been less explored. Several studies have been conducted regarding the association of VO2peak and severe AECOPD, yet all of them failed to identify VO2peak as an independent predictor of AECOPD. In a recent prospective study, published after the search period of this systematic review, Deng et al reported that impaired ventilatory efficiency, defined as a VE/VCO2 nadir above the upper limit of normal, was independently associated with an increased risk of moderate-to-severe AECOPDs, but not with total exacerbation frequency.38
Our study has several limitations. First, considerable heterogeneity across the included studies in terms of regression methods, patient populations, CPET equipment and testing protocols, investigated variables, and adjustment factors made direct comparison difficult. Additionally, all studies presented a certain degree of risk of bias and three studies were even excluded from the narrative review because of their high overall bias risk. Because of these factors, only a small meta-analysis combining three studies could be performed. Furthermore, 77% of the total study population in this systematic review were males, which limits the generalizability of our findings to female patients with COPD. This is particularly relevant given that, over the past decade, the age-adjusted prevalence of COPD has been consistently higher in females than in males, while potential sex-specific differences in exercise physiology and prognostic determinants remain incompletely understood.39 Lastly, potential publication bias cannot be excluded, as selective reporting could have led to skewed findings. Due to the small number of studies, formal assessment of publication bias using funnel plots was not feasible.
Taken together, the current evidence supports an association between select CPET-derived variables and relevant clinical outcomes in COPD, particularly mortality. However, these associations are primarily based on heterogeneous, often single-center studies, and robust evidence demonstrating additional prognostic value of individual CPET parameters over established prognostic indices is lacking. Importantly, the true potential of CPET may not lie in reliance on a single variable, but in the simultaneous availability of multiple exercise-derived parameters capturing distinct physiological aspects of exercise limitation. Although such parameters may show limited independent prognostic value when considered in isolation, their integrated assessment may allow development of multidimensional prognostic models. In a later stage, such models could potentially be further enriched by incorporation of complementary biomarkers or imaging-derived parameters.40 Future research in large, well-characterized cohorts with standardized CPET protocols and external validation across centers is needed to determine whether such integrated approaches can meaningfully enhance prognostic stratification beyond existing indices.
Conclusion
CPET-derived variables, particularly VO2peak and VE/VCO2, are associated with mortality in COPD, but evidence for their independent prognostic value and, more importantly, their incremental benefit over established composite indices remains inconsistent. Current data do not support routine use of CPET variables for prognostic stratification in COPD, apart from VO2peak as a marker of exercise capacity within the modified BODE index.
Disclosure
Prof. Dr. Stephanie Everaerts reports personal fees, non-financial support from PulmonX; grants from Chiesi; personal fees from GSK and Astra Zeneca; and non-financial support from Sanofi, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Christenson SA, Smith BM, Bafadhel M, Putcha N. Chronic obstructive pulmonary disease. Lancet Elsevier B V. 2022;399(10342):2227–18. doi:10.1016/S0140-6736(22)00470-6
2. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for prevention, diagnosis, and management of COPD: 2025 report. 2025. Available from: Https://Goldcopd.Org/2025-Gold-Report/.
3. Celli BR, Cote CG, Lareau SC, Meek PM. Predictors of survival in COPD: more than just the FEV1. Respir Med. 2008;102:S27–S35. doi:10.1016/S0954-6111(08)70005-2
4. Barnes PJ, Celli BR. Systemic manifestations and comorbidities of COPD. Eur Respir J. 2009;33(5):1165–1185. doi:10.1183/09031936.00128008
5. Boutou AK, Zafeiridis A, Pitsiou G, Dipla K, Kioumis I, Stanopoulos I. Cardiopulmonary exercise testing in chronic obstructive pulmonary disease: an update on its clinical value and applications. Clin Physiolog Funct Imaging. 2020;40(4):197–206. doi:10.1111/cpf.12627
6. Behnia M, Sietsema KE. Utility of cardiopulmonary exercise testing in chronic obstructive pulmonary disease: a review. Int J Chron Obstruct Pulmon Dis. 2023;18:2895–2910. doi:10.2147/COPD.S432841
7. Boulos L, Ogilvie R, Hayden JA. Search methods for prognostic factor systematic reviews: a methodologic investigation. J Med Libr Assoc. 2021;109(1):23–32. doi:10.5195/jmla.2021.939
8. Irvin E, Hayden J. Developing and testing an optimal search strategy for identifying studies of prognosis. In: Presented At: 14th Cochrane Colloquium. Dublin, Ireland; 2006.
9. Page MJ, Moher D, Bossuyt PM, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ Publishing Group. 2021:372. doi:10.1136/bmj.n160
10. Hayden JA, Van Der Windt DA, Cartwright JL, Cô P, Bombardier C. assessing bias in studies of prognostic factors. 2013. Available from: www.annals.org.
11. Harvey LA, Dijkers MP. Should trials that are highly vulnerable to bias be excluded from systematic reviews? Spinal Cord Nature Publishing Group. 2019;57(9):715–716. doi:10.1038/s41393-019-0340-y
12. Chuang M-L, Tsai C-F, Ueng K-C, et al. The impact of oxygen pulse and its curve patterns on male patients with heart failure, chronic obstructive pulmonary disease, and healthy controls—ejection fractions, related factors and outcomes. J Pers Med. 2022;12(5):703. doi:10.3390/jpm12050703
13. Chuang ML, Wang YH. Tidal volume expandability and ventilatory efficiency as predictors of mortality in Taiwanese male patients with chronic obstructive pulmonary disease: a 10-year follow-up study – is VO2peak or FEV1% the gold standard? Chron Respir Dis. 2023;20. doi:10.1177/14799731231220675
14. Çiftçi F, Şen E, Yıldız ÖA, Saryal S. Does exercise capacity, dyspnea level, or quality of life actually predict mortality in patients with COPD? 8-year follow-up. Tuberk Toraks. 2019;67(2):83–91. doi:10.5578/tt.67725
15. Cote CG, Pinto-Plata V, Kasprzyk K, Dordelly LJ, Celli BR. The 6-min walk distance, peak oxygen uptake, and mortality in COPD. Chest. 2007;132(6):1778–1785. doi:10.1378/chest.07-2050
16. da Luz Goulart C, Oliveira MR, Sendín FA, Mendes RG, Arena R, Borghi-Silva A. Prognostic value of key variables from cardiopulmonary exercise testing in patients with COPD: 42-month follow-up. Respir Med. 2022;197:106856. doi:10.1016/j.rmed.2022.106856
17. Ewert R, Obst A, Mühle A, et al. Value of cardiopulmonary exercise testing in the prognosis assessment of chronic obstructive pulmonary disease patients: a retrospective, multicentre cohort study. Respiration. 2022;101(4):353–366. doi:10.1159/000519750
18. González-Costello J, Armstrong HF, Jorde UP, et al. Chronotropic incompetence predicts mortality in severe obstructive pulmonary disease. Respir Physiol Neurobiol. 2013;188(2):113–118. doi:10.1016/j.resp.2013.05.002
19. Hiraga T, Maekura R, Okuda Y, et al. Prognostic predictors for survival in patients with COPD using cardiopulmonary exercise testing. Clin Physiol Funct Imaging. 2003;23(6):324–331. doi:10.1046/j.1475-0961.2003.00514.x
20. Lacasse M, Maltais F, Poirier P, et al. Post-exercise heart rate recovery and mortality in chronic obstructive pulmonary disease. Respir Med. 2005;99(7):877–886. doi:10.1016/j.rmed.2004.11.012
21. Li YX, Wang J, Wu B, et al. Effect of maximal oxygen pulse on patients with chronic obstructive pulmonary disease. Biomed Environ Sci. 2022;35(9):830–841. doi:10.3967/bes2022.107
22. Lorenzana I, Galera R, Casitas R, et al. Dynamic hyperinflation is a risk factor for mortality and severe exacerbations in COPD patients. Respir Med. 2024:225. doi:10.1016/j.rmed.2024.107597
23. Neder JA, Alharbi A, Berton DC, et al. Exercise ventilatory inefficiency adds to lung function in predicting mortality in COPD. COPD. 2016;13(4):416–424. doi:10.3109/15412555.2016.1158801
24. Oga T, Nishimura K, Tsukino M, Sato S, Hajiro T. Analysis of the factors related to mortality in chronic obstructive pulmonary disease: role of exercise capacity and health status. Am J Respir Crit Care Med. 2003;167(4):544–549. doi:10.1164/rccm.200206-583OC
25. Solanes I, Casan P, Sangenís M, Calaf N, Giraldo B, Güell R. Factores de riesgo de mortalidad en la EPOC. Archivos de Bronconeumología. 2007;43(8):445–449. doi:10.1157/13108784
26. Tojo N, Ichioka M, Chida M, Miyazato I, Yoshizawa Y, Miyasaka N. Pulmonary exercise testing predicts prognosis in patients with chronic obstructive pulmonary disease. Internal Med. 2005;44(1):20–25. doi:10.2169/internalmedicine.44.20
27. Wu C-W, Hsieh P-C, Yang M-C, Tzeng I-S, Wu Y-K, Lan -C-C. Impact of peak oxygen pulse on patients with chronic obstructive pulmonary disease. Int J Chronic Obstruct Pulmonary Di. 2019;14:2543–2551. doi:10.2147/COPD.S224735
28. Rowe SJ, Paratz ED, Foulkes SJ, et al. Understanding exercise capacity: from elite athlete to HFpEF. Canadian J Cardiol Elsevier Inc. 2023;39(11):S323–S334. doi:10.1016/j.cjca.2023.08.007
29. Montes De Oca M, Ortega Balza M, Lezama J, López JM. Enfermedad Pulmonar Obstructiva Crónica. Evaluación de La Tolerancia al Ejercicio Utilizando Tres Tipos Diferentes de Pruebas de Esfuerzo. Archivos de Bronconeumología. 2001;37(2):69–74. doi:10.1016/S0300-2896(01)75017-X
30. Swinburn CR, Wakefield JM, Jones PW. Performance, ventilation, and oxygen consumption in three different types of exercise test in patients with chronic obstructive lung disease. Thorax. 1985;40(8):581–586. doi:10.1136/thx.40.8.581
31. Cardoso F, Tufanin AT, Colucci M, Nascimento O, Jardim JR. Replacement of the 6-min walk test with maximal oxygen consumption in the BODE index applied to patients with COPD: an equivalency study. Chest. 2007;132(2):477–482. doi:10.1378/chest.07-0435
32. Luis Lopez-Campos J, Cejudo P, Marquez E, et al. International journal of COPD modified BODE indexes: agreement between multidimensional prognostic systems based on oxygen uptake. 2010. Available from: https://www.dovepress.com/.
33. Cote CG, Pinto-Plata VM, Marin JM, Nekach H, Dordelly LJ, Celli BR. The modified BODE index: validation with mortality in COPD. Eur Respir J. 2008;32(5):1269–1274. doi:10.1183/09031936.00138507
34. Neder JA. Cardiopulmonary exercise testing applied to respiratory medicine: myths and facts. Respir Med W B Saunders Ltd. 2023;214. doi:10.1016/j.rmed.2023.107249
35. Sun X-G, Hansen JE, Garatachea N, Storer TW, Wasserman K. Ventilatory efficiency during exercise in healthy subjects. Am J Respir Crit Care Med. 2002;166(11):1443–1448. doi:10.1164/rccm.2202033
36. Humbert M, Kovacs G, Hoeper MM, et al. ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension. J Euro Respirat Soc. 2023;61(1). doi:10.1183/13993003.00879-2022
37. Neder JA, Arbex FF, Alencar MCN, et al. Exercise ventilatory inefficiency in mild to end-stage COPD. Eur Respir J. 2015;45(2):377–387. doi:10.1183/09031936.00135514
38. Deng Z, Wu F, Wan Q, et al. Impaired ventilatory efficiency identifies high-risk mild-to-moderate chronic obstructive pulmonary disease. Arch Bronconeumol. 2026;62(1):10–19. doi:10.1016/j.arbres.2025.04.005
39. Czarnota P, MacLeod JL, Gupta N, Manichaikul A, Shim YM. Sex differences in chronic obstructive pulmonary disease: implications for pathogenesis, diagnosis, and treatment. Int J Mol Sci. 2025;26(6):2747. doi:10.3390/ijms26062747
40. Phillips DB, Elbehairy AF, James MD, et al. Impaired ventilatory efficiency, dyspnea, and exercise intolerance in chronic obstructive pulmonary disease: results from the CanCOLD study. Am J Respir Crit Care Med. 2022;205(12):1391–1402. doi:10.1164/rccm.202109-2171OC
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.