Back to Journals » Clinical Epidemiology » Volume 8
Cardiac dysfunction among soft tissue sarcoma patients in Denmark
Authors Shantakumar S, Olsen M, Vo T, Nørgaard M ![]() , Pedersen L
, Pedersen L
Received 18 November 2015
Accepted for publication 17 February 2016
Published 15 April 2016 Volume 2016:8 Pages 53—59
DOI https://doi.org/10.2147/CLEP.S100779
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor H Sorensen
Sumitra Shantakumar,1 Morten Olsen,2 Thao T Vo,3 Mette Nørgaard,2 Lars Pedersen,2
1Worldwide Epidemiology Department, GlaxoSmithKline Pte Ltd, Singapore; 2Department of Clinical Epidemiology, Aarhus University Hospital, Aarhus, Denmark; 3Worldwide Epidemiology, GlaxoSmithkline, Research Triangle Park, USA
Purpose: Soft tissue sarcoma (STS) patients may experience post-treatment cardiotoxicity, yet no population-based data exist. We examined the incidence of left ventricular ejection fraction (LVEF) decline, heart failure, and cardiac death following STS diagnosis among adults, using Danish patient registries and medical record review.
Patients and methods: LVEF decline was examined in a regional cohort of STS patients diagnosed during 1997–2011 in Western Denmark for whom cardiac imaging data were available. LVEF decline was defined as an absolute decline from baseline to follow-up of 10% or more, or, where baseline imaging was not available, a decline below the lower limit of normal (or 40%) for a follow-up LVEF. Heart failure and cardiac death were investigated in a national Danish cohort of all STS patients diagnosed from 2000 to 2009. We followed patients from STS diagnosis until heart failure, cardiac death, emigration or December 31, 2012 (whichever occurred first).
Results: The incidence rate of LVEF decline for the regional cohort with follow-up data (N=100, five events) or baseline and follow-up measurements (N=75, 19 events) was 16.8 (95% confidence interval [CI]: 7.0–40.3) and 108 (95% CI: 69–170), respectively, per 1,000 person-years. In the national cohort (N=1,187), the incidence of heart failure (40 events) and cardiac death (15 events) was 7.3 (95% CI: 5.4–10.0) and 2.7 (95% CI: 1.6–4.5), respectively, per 1,000 person-years. The strongest predictors of heart failure were doxorubicin treatment (hazard ratio [HR] =2.2, 95% CI: 0.5–10.2) and pre-existing cardiovascular disease (HR=6.3, 95% CI: 0.98–40.6).
Conclusion: LVEF decline occurred more frequently compared to heart failure or cardiac death in a nationally representative cohort of Danish STS patients.
Keywords: sarcoma, heart failure, LVEF, cardiac death
Introduction
Management of soft tissue sarcoma (STS) is complex and requires a multidisciplinary approach using surgery, radiotherapy, and/or chemotherapy. In advanced disease, chemotherapy currently constitutes as the core treatment, but there is no accepted standard of care; available regimens have shown limited success regarding improving survival. Many of these treatments can cause cardiovascular complications, including left ventricular dysfunction and heart failure, myocardial ischemia, hypertension, and arrhythmias.1–5 The cardiotoxicity of anthracyclines is particularly well described, but other chemotherapeutic agents have cardiotoxic potential.1,3,6 Further, the thorax can damage the pericardium, myocardium, valves, and coronary vessels.7
The cardiotoxicity of anticancer agents can lead to significant complications with major impact on quality of life and survival.8 Toxicity severity may depend on many factors, such as the molecular site of action, the immediate and cumulative dose, the method of administration, the combination and sequence of therapies, the presence of underlying cardiac conditions, and patient demographics.9 Cardiotoxic effects can occur immediately during administration of the drug, or they may not manifest until months or years following treatment.10 In clinical oncology practice, an asymptomatic decrease in left ventricular ejection fraction (LVEF) is the most commonly encountered form of cardiotoxicity.8,11,12
Innovation in STS treatment has been limited in the past 30 years, but recent investigational drugs include mTOR inhibitors and TK inhibitors (TKIs). The TKIs, such as imatinib and sunitinib, are already available for treatment of gastrointestinal stromal tumors (GISTs); studies show imatinib has sustained objective responses in more than 50% of GIST patients.13 Since angiogenesis is important for the growth of STS, TKIs including sorafenib, sunitinib and pazopanib, which inhibit the VEGF or VEGFR pathway, have also been assessed as potential therapies for STS patients.14–16 Some cardiotoxicities have been observed among patients treated with VEGF targeting agents.17 Cardiac related events have been observed in clinical trials of STS patients treated with pazopanib.18
Although cardiotoxicity can be a significant complication in STS patients, there are no population-based data on the incidence of LVEF decline, heart failure, and cardiac death in STS patients. As part of the pharmacovigilance and risk management strategies for pazopanib, the objective of this study was to describe “real-world” background rates of cardiac events in the target population for pazopanib, STS patients.
Methods
A cohort study was conducted among all adult (age ≥18 years) STS patients in Denmark. STS patients were retrospectively identified in the Danish Cancer Registry or National Pathology Registry via relevant International Statistical Classification of Diseases 10th revision (ICD-10) diagnosis codes or Systematized Nomenclature of Medicine (SNOMED) morphology codes. The Danish Cancer Registry contains records of all incident cancers (~5.5 million) in Denmark since 1943 and the National Pathology Registry includes data on cancer pathology tests performed since 1997. Using the Danish Civil Registration Number, a unique identification number assigned to every Danish citizen at birth or immigration, linkages were made to other national databases for obtaining data on patient demographics (Danish Civil Registration System), outpatient and hospitalization diagnosis or procedure history (Danish National Registry of Patients [DNRP]), prescriptions and concomitant medications (Prescription Databases of the Central Denmark Region and North Denmark Region), and immigration or death (Danish Register of Causes of Death).
Only patients with STS indicated as a first primary cancer were included. Those who developed multiple primary cancers, before or at the time of the initial STS diagnosis, were excluded. To allow for a minimum of 12 months of follow-up time for each patient, the study population was limited to patients who were diagnosed, at minimum, 12 months prior to the last date in which data were available. The index date was defined as the date of initial STS diagnosis.
The incidence of heart failure and cardiac death was investigated in all STS patients diagnosed from 2000 to 2009 in Denmark (national cohort). Diagnosis of heart failure or congestive heart failure was identified from the DNRP using ICD-10 codes (I11.0, I13.0, I13.2, I42.0, I42.6, I42.7, I42.9, I50.0, I50.1, and I50.9). The DNRP does not include data related to disease stage or treatment. Cardiac death was determined from cause of death ICD-10 codes (I00-25, I27, I30-5) in the Danish Register of Causes of Death.
The incidence of cardiac dysfunction, as measured by LVEF decline, was evaluated among a subset of patients in Western Denmark (regional cohort) for whom cardiac imaging data were available. Since 1979, the treatment of STS patients in Western Denmark has been carried out at the Sarcoma Centre of Aarhus University Hospital. For the cardiac dysfunction analysis, all patients who had contact with this department from 1997 to 2011 were identified from the DNRP. For each patient, a detailed medical record review was conducted by physicians or nurses under doctors supervision to obtain cardiac imaging results. Abstracted data included LVEF measurements from multigated acquisition scans or echocardiography, the institutional lower limit of normal (LLN), and signs or symptoms of heart failure as these data are not recorded in existing registries. LVEF was recorded at baseline (between index date and initiation of first cancer treatment) and follow-up (any LVEF measurement after baseline). If multiple LVEF measurements were available at the time of baseline, the measurement closest to the index date was chosen. For those with only follow-up LVEF, cardiac dysfunction was defined as an LVEF measurement below the institutional LLN or LVEF below 40% when the institutional LLN was unavailable. Among patients with both baseline and follow-up LVEF measurements, LVEF decline was defined as an absolute drop from baseline to follow-up of 10% or greater. Patients with baseline LVEF below the institutional LLN, pre-existing cardiovascular disease or heart failure were excluded from LVEF decline analyses.
In both the national and regional cohorts, recorded covariates included patient demographics (age and sex), diagnosis year, sarcoma subtype, and date of death. Additional covariates available for the regional cohort through medical record review included STS stage, metastasis site (secondary STS, bone, brain, lymph nodes, liver lung, and other), radiation (yes/no), surgery (yes/no), chemotherapy (yes/no, type and dose, neo-adjuvant/adjuvant), and presence of pre-existing cardiovascular disease or cardiac risk factors. Conditions comprising pre-existing cardiovascular disease included coronary artery disease, congestive heart failure, arrhythmia, valvular disease, pulmonary embolism, chronic obstructive pulmonary disease, anemia, pericardial effusion, diabetes mellitus, hypercholesterolemia, hypertension, and concomitant cardiac medications (beta-blockers, ACE inhibitors, or angiotensin receptor blockers).
The incidence of heart failure and cardiac death was evaluated among all STS patients (national cohort); the LVEF decline analysis was limited to patients with cardiac imaging (regional cohort). Therefore, analyses were conducted separately for the national and regional cohorts, and the presence of any systematic differences between these two cohorts was assessed. Continuous variables were summarized with mean, standard deviation, median and range; number and proportion are provided for categorical variables.
To calculate incidence rates, the numerator comprised the number of STS patients with the outcome occurring during the follow-up period after cancer diagnosis (index date). The denominator was equal to the total person-years (PY) contributed to being at risk (ie, alive, had no cardiac dysfunction or heart failure) from the index date of STS diagnosis to the end of follow-up (date of heart failure diagnosis, cardiac death, emigration or December 31, 2012, whichever occurred first). Cox proportional hazards regression analysis was performed to identify predictors of heart failure or cardiac death among STS patients in the regional cohort.
No potentially identifying patient information was included, so written consent was not required. The study posed minimal privacy risk for patients, and was approved by the Danish Data Protection Agency. Access to medical records and abstraction of data by physicians/nurses for the regional cohort was approved by the Danish Board of Health.
Results
From 2000 to 2009, 1,187 patients diagnosed with STS were identified for the national cohort, with a mean and median follow-up time of 4.6 and 4.1 years, respectively. Among these STS patients, 45% were female and 49% were aged ≥60 years (Table 1). The most common subtypes of STS diagnoses were liposarcoma (33%) and leiomyosarcoma (32%).
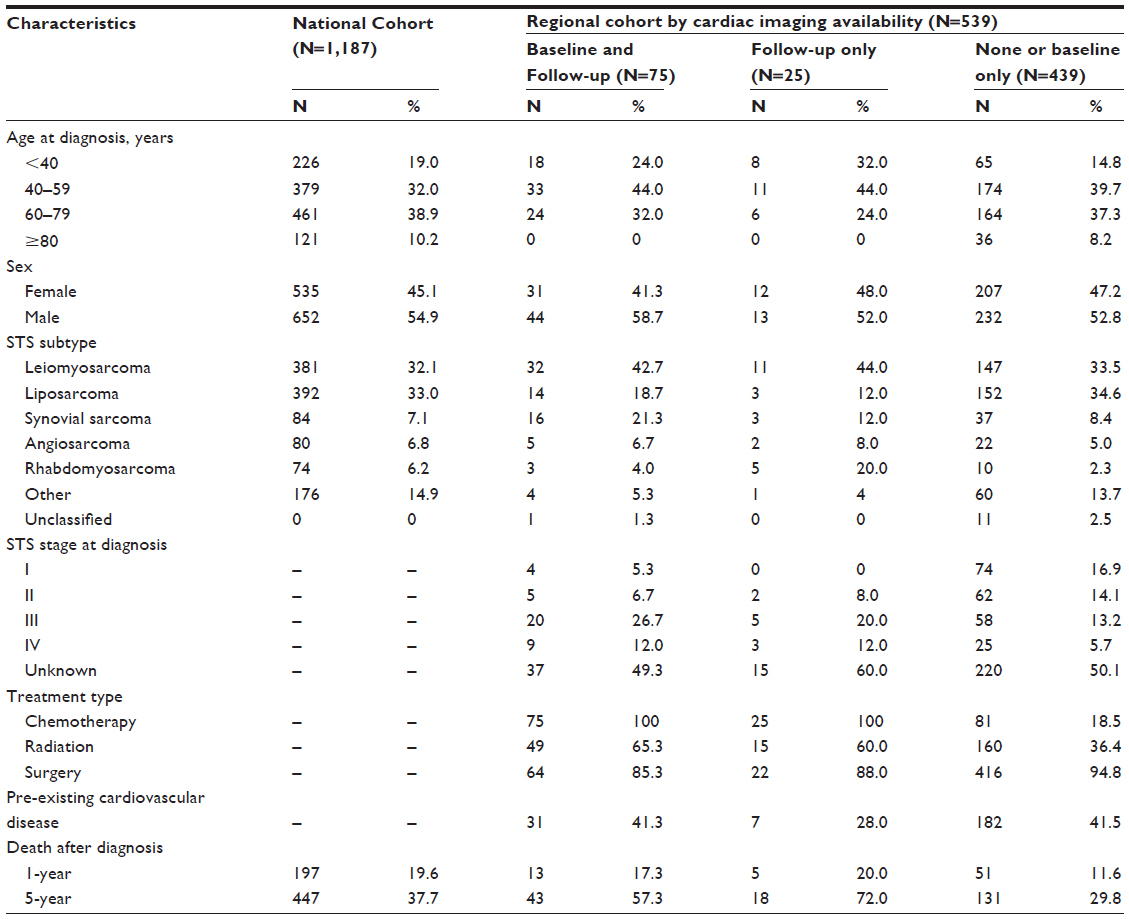 | Table 1 Baseline characteristics of soft tissue sarcoma (STS) patients in the national Danish cohort (2000–2009) and regional cohort in Western Denmark (1997–2011) by cardiac imaging availability |
For the regional cohort with cardiac imaging data, 670 patients with STS who had visited the oncology department in Aarhus from 1997 to 2011 were identified. Patients were excluded for having a previous diagnosis of a different cancer (N=109), having an STS diagnosis prior to 1997 (N=3), or having been diagnosed with osteosarcoma or GIST (N=9), thereby leaving 539 eligible patients. Among the eligible patients, 75 patients had both baseline and follow-up cardiac imaging data in their medical record, 25 had follow-up data only and the remaining 439 patients had only baseline measurements or no cardiac imaging performed. The regional cohort was followed for a mean of 4.7 years and median of 3.6 years.
Compared to the full regional cohort, patients with baseline and follow-up data were less likely to be female (41% vs 46%), aged ≥60 years (32% vs 42%), have liposarcoma (19% vs 31%), or have early stage I disease (5.3% vs 14.5%) (data not shown). Metastatic disease, chemotherapy, and radiation therapy were more commonly observed among patients with both baseline and follow-up cardiac imaging data (12%, 100%, 65%, respectively) compared to the full regional cohort (7%, 33%, 42%, respectively); the proportion of patients with pre-existing cardiovascular disease was similar (41%) in both groups.
Among 100 STS patients in the regional cohort with available follow-up cardiac imaging data, five patients experienced LVEF decline (20%–40% of LLN) during 298.4 PY of follow-up, corresponding to an incidence rate of 16.8 (95% confidence interval [CI]: 7.0–40.3) per 1,000 PY (Table 2). For 75 patients with both baseline and follow-up cardiac imaging data, LVEF decline (absolute drop ≥10%) occurred in 19 patients over 175.3 PY of follow-up, for an incidence rate of 108 (95% CI: 69–170) per 1,000 PY. Among the 19 patients with a documented event, 17 experienced an absolute drop in LVEF from baseline to follow-up between 10% and 20%; the remaining two patients had a decline in LVEF that was >20% (data not shown). Incidence of LVEF decline was higher for patients aged 60–79 years in both groups (44.9 and 294, respectively, per 1,000 PY). No consistent pattern in incidence rates by stage of disease was observed.
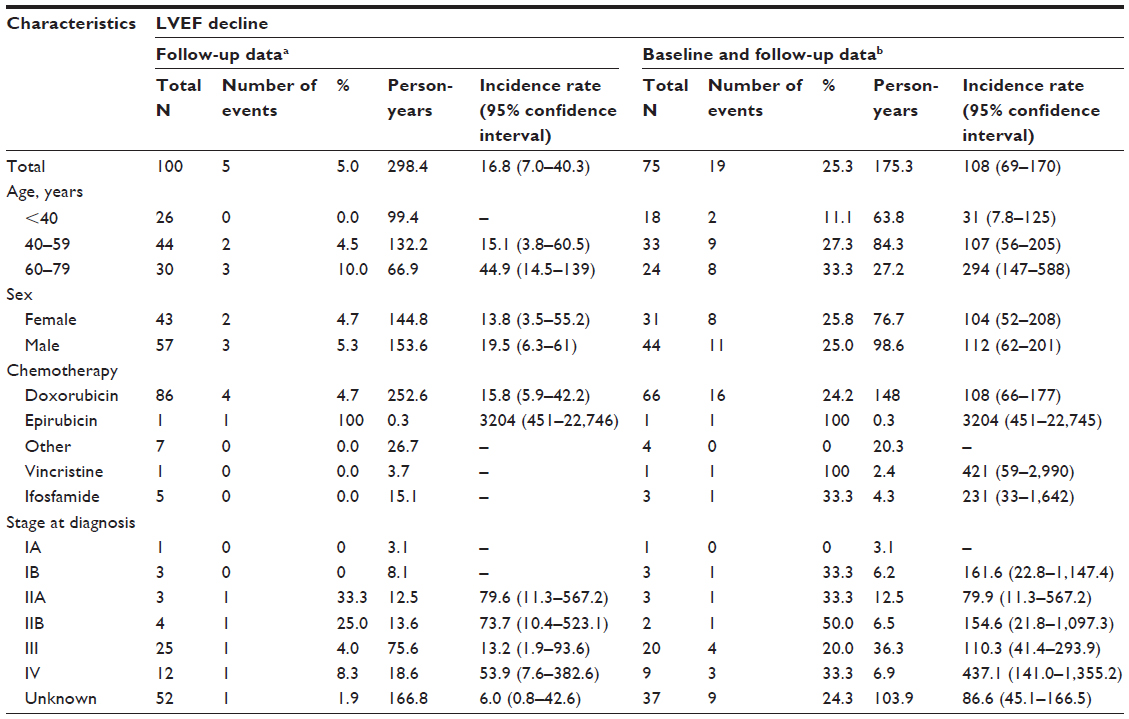 | Table 2 Incidence rate (per 1,000 person-years) of left ventricular ejection fraction (LVEF) decline among soft tissue sarcoma patients with cardiac imaging at follow-up in Western Denmark (regional cohort), 1997–2011 |
The cumulative incidence of heart failure and cardiac death in the national cohort of 1,187 STS patients was 3.4% and 1.3%, respectively. Heart failure occurred in 40 patients over 5,449 PY of follow-up for an overall incidence rate of 7.3 (95% CI: 5.4–10.0) per 1,000 PY (Table 3). Heart failure incidence increased with age, ranging from 0.8 per 1,000 PY in patients under age 40 to 35.2 per 1,000 PY among those aged ≥80 years. Heart failure was less common in males (6.6 per 1,000 PY) compared to females (8.3 per 1,000 PY). The incidence of heart failure was highest for patients diagnosed with hemangiosarcoma (21.2 per 1,000 PY) compared to the other subtypes of STS (range: 0–8.3 per 1,000 PY). During 5,510 PY of follow-up, 15 patients had cardiac death recorded. The cardiac-specific mortality was 2.7 (95% CI: 1.6–4.5) per 1,000 PY; mortality increased to 17.1 per 1,000 PY for those aged ≥80 years. Regarding STS subtypes, cardiac-specific mortality was highest for fibrosarcoma patients (5.1 per 1,000 PY).
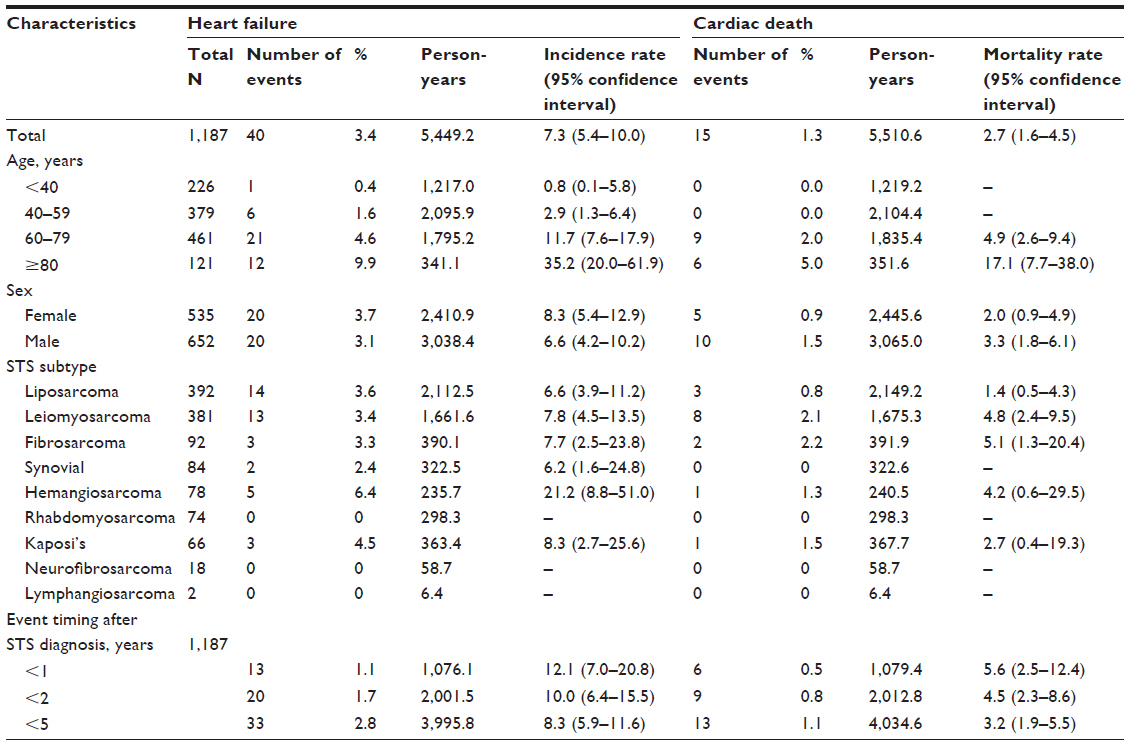 | Table 3 Incidence or mortality rate (per 1,000 person-years) of heart failure and cardiac death among soft tissue sarcoma (STS) patients in Denmark (national cohort), 2000–2009 |
In Table 4, predictors of heart failure, cardiac death, and overall mortality were assessed for STS patients in the full regional cohort. Pre-existing cardiovascular disease was the strongest predictor of heart failure (hazard ratio [HR] =6.31, 95% CI: 0.98–40.55) and cardiac death (HR =5.86, 95% CI: 0.82–42.06). Treatment with doxorubicin chemotherapy was strongly associated with overall mortality (HR =4.92, 95% CI: 3.67–6.59).
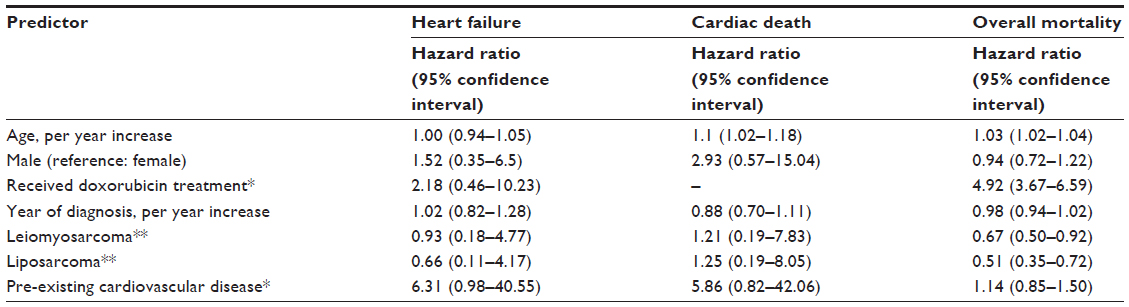 | Table 4 Cox proportional hazard modeling of predictors for heart failure and cardiac death among soft tissue sarcoma (STS) patients in Western Denmark (regional cohort, N=539), 1997–2011 |
Discussion
This study provides real-world data on the background rates of cardiac dysfunction, heart failure, and cardiac death in STS patients using nationwide Danish population-based registries. Overall, LVEF decline was relatively common, but few heart failure events or cardiac-related deaths were observed in the national cohort of Danish STS patients. It is possible that heart failure and cardiac death may manifest later in the post-treatment period and occur outside the follow-up period for STS patients in this study. However, the estimated incidence rates observed for these cardiac events in the present study are consistent with previously reported rates among the general population of adults in Demark or other Northern European countries.19–22 Doxorubicin treatment was a strong predictor for both heart failure and overall mortality in the regional cohort (for whom treatment data were available) which may be related to having more aggressive disease, use of the drug, or both.
The incidence of LVEF decline was considerably higher among patients with baseline and follow-up cardiac imaging measurements compared to patients with follow-up data only. It is possible that absolute decline of LVEF from baseline to follow-up is a more sensitive measure of cardiac dysfunction. Another possible explanation is that patients with baseline and follow-up cardiac imaging received additional medical intervention due to more severe disease or the presence of comorbidities. However, patients with follow-up data only had a higher 5-year death rate (72%) compared to patients with baseline and follow-up data available (57%).
Cardiac imaging data used to assess LVEF decline were only available for a relatively small number of patients from the Western Denmark region, covering approximately half of the Danish population. Further, few patients had both baseline and follow-up LVEF data available; using both data points is ideal for evaluating LVEF decline. Patients with no cardiac imaging or baseline data only generally had lower stage of disease, were less likely to receive chemotherapy or radiation, and had lower 1-year or 5-year death rates compared to patients with follow-up imaging data. Thus, it is possible these results overestimate the incidence of LVEF decline in the general STS population, assuming LVEF decline is less common in healthier STS patients. Information on STS stage, cancer treatments, and pre-existing cardiovascular disease was limited to medical record review in the regional cohort, leading to small sample sizes in some analytic subgroups. Nonetheless, these data were population-based and representative of all patients from Western Denmark.
Internal validity of this study is high due to the unique nature of the country-wide linked Danish health databases. However, the results from this study are not generalizable to other geographic regions or populations. While the data linkages are 100% complete, available information may not be comprehensive. For example, the data for pre-existing cardiovascular disease in the regional cohort are limited to conditions requiring hospital admissions or outpatient clinic visits. To more accurately measure pre-existing cardiac diseases, concomitant use of cardiac medications were assessed using the prescription databases to include a more sensitive measure of existing cardiac disease. However, the prescription databases do not include non-reimbursable drugs. Likewise, cancer treatments are not captured in the prescription databases and, therefore, those data in the regional cohort are based on medical record review. There is a potential for misclassification of the cause of cardiac death in terms of whether the cancer alone or pre-existing cardiac disease leads to cardiac death.
Conclusion
The Danish databases are among the very few patient databases that are able to link cardiac imaging data to other medical information, including data related to clinical outcomes, medications, and comorbidities. There is currently no published population-based study on LVEF decline or cardiac dysfunction in STS patients, possibly due to the difficulty in identifying data sources containing cardiac imaging data. These study results fill an important knowledge gap and may improve patient safety with regard to cardiac management among heavily treated STS patients.
Acknowledgments
This work was supported by GlaxoSmithKline. All aspects of the analysis were conducted by the Department of Clinical Epidemiology at Aarhus University Hospital in Denmark. The authors would like to thank Page Abrahamson for her help in drafting this manuscript.
Disclosure
Sumitra Shantakumar holds shares in GlaxoSmithKline. Thao Vo was employed by GlaxoSmithKline during the conduct of this study and is currently employed and owns shares at Merck. The authors have no other conflicts of interest to disclose.
References
Bonita R, Pradhan R. Cardiovascular toxicities of cancer chemotherapy. Semin Oncol. 2013;40(2):156–167. | |
Khawaja MZ, Cafferkey C, Rajani R, Redwood S, Cunningham D. Cardiac complications and manifestations of chemotherapy for cancer. Heart. 2014;100(4):1133–1140. | |
Pai VB, MC Nahata. Cardiotoxicity of chemotherapeutic agents: incidence, treatment and prevention. Drug Saf. 2000;22(4):263–302. | |
Svoboda M, Poprach A, Dobes S, Kiss I, Vyzula R. Cardiac toxicity of targeted therapies used in the treatment for solid tumours: a review. Cardiovasc Toxicol. 2012;12(3):191–207. | |
Yeh ET, Tong AT, Lenihan DJ, et al. Cardiovascular complications of cancer therapy: diagnosis, pathogenesis, and management. Circulation. 2004;109(25):3122–3131. | |
Smith LA, Cornelius VR, Plummer CJ, et al. Cardiotoxicity of anthracycline agents for the treatment of cancer: systematic review and meta-analysis of randomised controlled trials. BMC Cancer. 2010;10(1):337. | |
Veinot JP, Edwards WD. Pathology of radiation-induced heart disease: a surgical and autopsy study of 27 cases. Hum Pathol. 1996;27(8):766–773. | |
Swain SM, Whaley FS, Ewer MS. Congestive heart failure in patients treated with doxorubicin: a retrospective analysis of three trials. Cancer. 2003;97(11):2869–2879. | |
Yeh ET, Bickford CL. Cardiovascular complications of cancer therapy: incidence, pathogenesis, diagnosis, and management. J Am Coll Cardiol. 2009;53(24):2231–2247. | |
Lenihan DJ, Cardinale DM. Late cardiac effects of cancer treatment. J Clin Oncol. 2012;30(30):3657–3664. | |
Yoon GJ, Telli ML, Kao DP, et al. Left ventricular dysfunction in patients receiving cardiotoxic cancer therapies are clinicians responding optimally? J Am Coll Cardiol. 2010;56(20):1644–1650. | |
Telli ML, Hunt SA, Carlson RW, Guardino AE. Trastuzumab-related cardiotoxicity: calling into question the concept of reversibility. J Clin Oncol. 2007;25(23):3525–3533. | |
Demetri GD, von Mehren M, Blanke CD, et al. Efficacy and safety of imatinib mesylate in advanced gastrointestinal stromal tumors. N Engl J Med. 2002;347(7):472–480. | |
Jain A, Sajeevan KV, Babu KG, Lakshmaiah KC. Chemotherapy in adult soft tissue sarcoma. Indian J Cancer. 2009;46(4):274–287. | |
George S, Merriam P, Maki RG, et al. Multicenter phase ii trial of sunitinib in the treatment of nongastrointestinal stromal tumor sarcomas. J Clin Oncol. 2009;27(19):3154–3160. | |
Pacey S, Ratain MJ, Flaherty KT, et al. Efficacy and safety of sorafenib in a subset of patients with advanced soft tissue sarcoma from a Phase II randomized discontinuation trial. Invest New Drugs. 2011;29(3):481–488. | |
Bhave M, Akhter N, Rosen ST. Cardiovascular toxicity of biologic agents for cancer therapy. Oncology (Williston Park). 2014;28(6):482–490. | |
van der Graaf WT, Blay JY, Chawla SP, et al. Pazopanib for metastatic soft-tissue sarcoma (PALETTE): a randomized, double-blind, placebo-controlled phase 3 trial. Lancet. 2012;379(9829):1879–1886. | |
Guha K, McDonagh T. Heart failure epidemiology: European perspective. Curr Cardiol Rev. 2013;9(2):123–127. | |
Bleumink GS, Knetsch AM, Sturkenboom MC, et al. Quantifying the heart failure epidemic: prevalence, incidence rate, lifetime risk and prognosis of heart failure The Rotterdam Study. Eur Heart J. 2004;25(18):1614–1619. | |
Nichols M, Townsend N, Scarborough P, Rayner M. Trends in age-specific coronary heart disease mortality in the European Union over three decades: 1980–2009. Eur Heart J. 2013;34(39):3017–3027. | |
Mari-Dell’Olmo M, Gotsens M, Palencia L, et al. Socioeconomic inequalities in cause-specific mortality in 15 European cities. J Epidemiol Community Health. 2015;69(5):432–441. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.