")
Back to Journals » Orthopedic Research and Reviews » Volume 15
Capital Femoral Epiphysis with Acute Unstable Valgus Type Slip Managed with Closed Reduction and Percutaneous Fixation: A Case Report
Authors Cheok T , Jennings M, Berman M, Williams K, Rawat JS, Foster BK
Received 10 July 2023
Accepted for publication 19 October 2023
Published 4 November 2023 Volume 2023:15 Pages 207—213
DOI https://doi.org/10.2147/ORR.S429844
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Clark Hung
Tim Cheok,1– 3 Matthew Jennings,1,4 Morgan Berman,1 Kanishka Williams,1,3 Jaideep Singh Rawat,1,5,6 Bruce K Foster1,5
1Department of Trauma and Orthopaedics, Alice Springs Hospital, Alice Springs, Northern Territory, Australia; 2Department of Orthopaedic Surgery, Palmerston North Hospital, Palmerston North, New Zealand; 3College of Medicine and Public Health, Flinders University, Adelaide, South Australia, Australia; 4Department of Plastics and Reconstructive Surgery, Women’s and Children’s Hospital, Adelaide, South Australia, Australia; 5Department of Orthopaedic Surgery, Flinders Medical Centre, Adelaide, South Australia, Australia; 6Department of Orthopaedic Surgery, Women’s and Children’s Hospital, Adelaide, South Australia, Australia
Correspondence: Tim Cheok, Email [email protected]
Case: We present a case of acute unstable valgus slipped capital femoral epiphysis (SCFE) in an 8-year-old female who presented after a trip and fall. The patient was managed with emergent closed reduction and percutaneous screw fixation and prophylactic fixation of contralateral side after 6 weeks. At 18-month follow-up, the patient was symptom free with a good range of movement and no evidence of slip progression, chondrolysis or avascular necrosis of the femoral head.
Conclusion: We demonstrate that, in this case, closed reduction and percutaneous fixation provided satisfactory outcome at 18-month follow-up. This case highlights the need for both anteroposterior and lateral radiographs.
Keywords: SCFE, closed reduction, percutaneous pinning, valgus slip
Introduction
Slipped capital femoral epiphysis (SCFE) is a relatively common paediatric hip condition, whereby metaphysis slips relative to epiphysis. Presentation is typically with hip and/or knee pain. Valgus SCFE are uncommon and characterised by posterior displacement of the epiphysis in relation to metaphysis, but lateral displacement may be absent.1,2 The prevalence of valgus slips has been reported to be between 1.9% and 4.7% of all SCFEs,3,4 with only 96 known cases in literature.1
There are two commonly utilised classification systems for SCFE: Loder’s classification and temporal classification.5 Loder et al classified SCFE into stable and unstable slips, depending on the child’s ability to bear weight.6 The temporal classification is based on the duration of symptoms, where the duration of symptoms in acute slips is fewer than 3 weeks and chronic slips is greater than 3 weeks. A review of literature revealed three reported cases of acute valgus slips7–9 and one case of acute, of which none were unstable. These studies are displayed in Table 1.
 |
Table 1 Acute Valgus Slip in Literature |
Management of acute unstable slips remains controversial.10,11 Although in-situ fixation remains the accepted gold standard,12 some authors have advocated for emergent closed reduction and percutaneous pinning,13,14 or open reduction using the modified Dunn’s procedure15 to mitigate the risk of developing impingement and early arthritis. We present a rare case of acute unstable valgus SCFE. The patient and her carers provided consent for the case to be published. Institutional approval was not required for publication of this case report. The report that follows has been written in accordance with the Case Report (CARE) guidelines.16
Case Report
An 8-year-old female presented with an acute onset of left hip pain after tripping over her dog at home. She had a history of hypermobility syndrome (hyperextended knee, pes planus and broad-based gait), foetal alcohol spectrum disorder and attention deficit hyperactivity disorder. The patient was of Australian Aboriginal descent without a known history of endocrine disorders. Her body mass index (BMI) was 18.6 kg/m2 (height of 135 cm and weight of 33.9 kg).
She was unable to bear weight on presentation. Her roentgenograms, shown in Figure 1, demonstrated bilateral coxa valga with an intact Klein’s line and slight effacement of the left femoral epiphysis. The femoral head appeared to be more spherical compared to the contralateral side. Lateral radiographs revealed posterior displacement of the epiphysis in relation to the metaphysis. The posterior slip angle was measured to be 45 degrees.
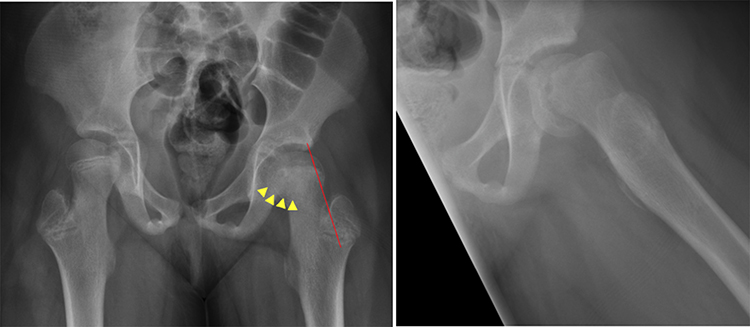 |
Figure 1 Preoperative roentgenograms. Anteroposterior (AP) radiograph demonstrating an intact Klein’s line (Red). There is subtle effacement of the physis compared to the contralateral side resulting in a more spherical appearance of the femoral head (Yellow). Lateral radiographs confirm posterior displacement of the epiphysis in relation to the femoral neck. The posterior slip angle was measured to be 43. |
The decision was made to proceed emergently for closed reduction and percutaneous fixation. With the patient positioned supine in a traction table, closed reduction was performed by providing longitudinal traction and internal rotation. Under fluoroscopic guidance, entry point was confirmed utilising two 1.8 mm K-wires placed perpendicular to each other on the skin. The entry point was challenging as it was far more medial and anterior than for a varus-type SCFE placing the neurovascular bundle at risk. The line of the guidewire was felt to be most appropriate anteromedially to allow for maximum capture of the femoral head. Preoperative sonography was utilised to mark the position and note the depth of the femoral vessels. Cephazolin prophylaxis was given, and standard skin preparation and draping was performed. The skin and facia were incised, and a careful subfascial dissection was performed to gain access to the anterior femur. A cannulated guide wire was inserted, and position confirmed by fluoroscopy. The guide wire was placed in the centre of the head and measured, and a 7.3 mm partially threaded screw (Synthes, USA) was inserted. Approach withdrawal technique was utilised to confirm that the screw had not penetrated the epiphyses. A second screw was inserted just superior and parallel to the first to achieve greater biomechanical stability. Aspiration of the hip joint was not performed.
Postoperatively, the patient was instructed to non-weight bear for 6 weeks, followed by partial weight-bearing for further 6 weeks. Low dose computed tomography (CT) scan was performed to confirm screw position. Screening for endocrine disorders (thyroid and parathyroid dysfunction, growth hormone disorders and renal osteodystrophy) revealed Vitamin D deficiency (39 nmol/L). Replacement therapy was commenced at 1000 IU/day for 3 months. Postoperative radiographs taken at 6 weeks following fixation are shown in Figure 2, showing sustained improvement in the posterior slope angle. Contralateral prophylactic fixation with 7.3 mm cannulated shaft screw (Synthes, USA) was performed 6 weeks following her initial operation. This was in line with institutional-based practice.
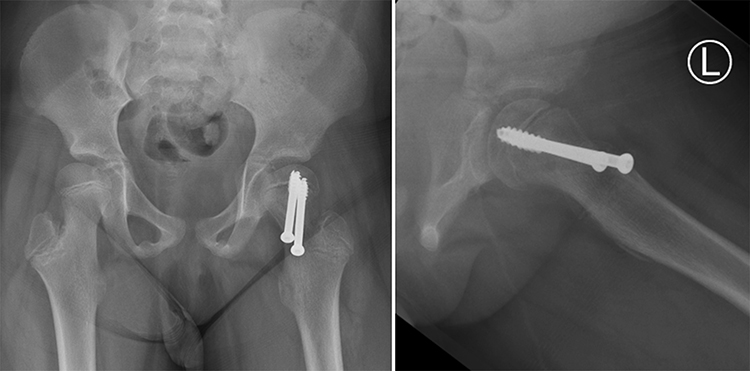 |
Figure 2 Six-weeks postoperative roentgenograms. Radiographs demonstrating fixation in the left Hip with two partially threaded cancellous screws (Synthes, USA). The anteroposterior (AP) radiograph shows reversal of physeal effacement, and the lateral radiographs confirms improvement of the posterior displacement of the epiphysis. The posterior slip angle was measured to be 18. |
We followed-up with this patient at 3 weeks, 6 weeks, 6 months, 12 months, and 18 months postoperatively. The range of movement in each of her follow-up appointments is detailed in Table 2. At her recent 18-month follow-up, the patient had equal range of movement with her contralateral side. There was no evidence of slip progression, avascular necrosis, or chondrolysis. Vitamin D levels following treatment were 65 nmol/L. Epiphyseal escape of the prophylactically pinned side was noted at her one-year follow-up, which was revised. Her one-year roentgenograms are shown in Figure 3.
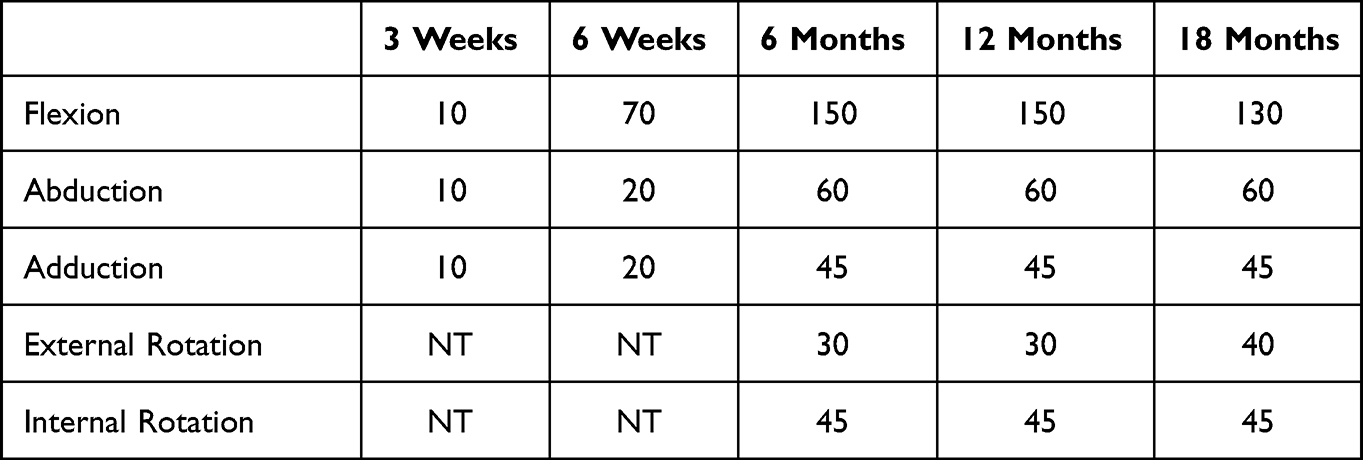 |
Table 2 Postoperative Range of Movement |
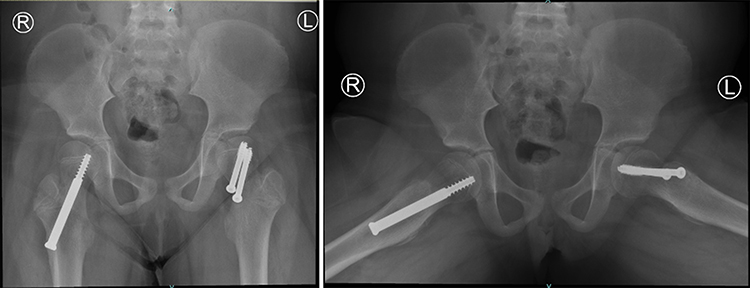 |
Figure 3 One-year postoperative roentgenograms. Radiographs demonstrating fixation in the left Hip with two partially threaded cancellous screws (Synthes, USA) and prophylactic pinning of the right Hip with cannulated shaft screw (Synthes, USA). The radiographs demonstrate no evidence of slip progression, avascular necrosis or chondrolysis of the left femoral head. On the right side, there was evidence of epiphyseal escape from the prophylactic fixation. |
Discussion
Although SCFE is one of the most common disorders affecting adolescent hips, valgus-type slips are uncommon. Some authors doubt its existence but rather believe it is an illusion and simply represents differences in rotation position of the proximal femur.3 Multiple general risk factors for SCFE have been described. This includes patients who have Vitamin D deficiency and are of Aboriginal Australian descent.17,18 Additionally, Shank et al have shown that coxa valga is a risk factor for valgus slips.4 When they do occur, it is more common on the left hip.19 A previous biomechanical study by Yngve et al showed that certain anatomical factors resulted in an increased physeal shear force in the posterolateral direction, predisposing to valgus SCFE. Our patient had very similar values to their published results.20 These are displayed in Table 3.
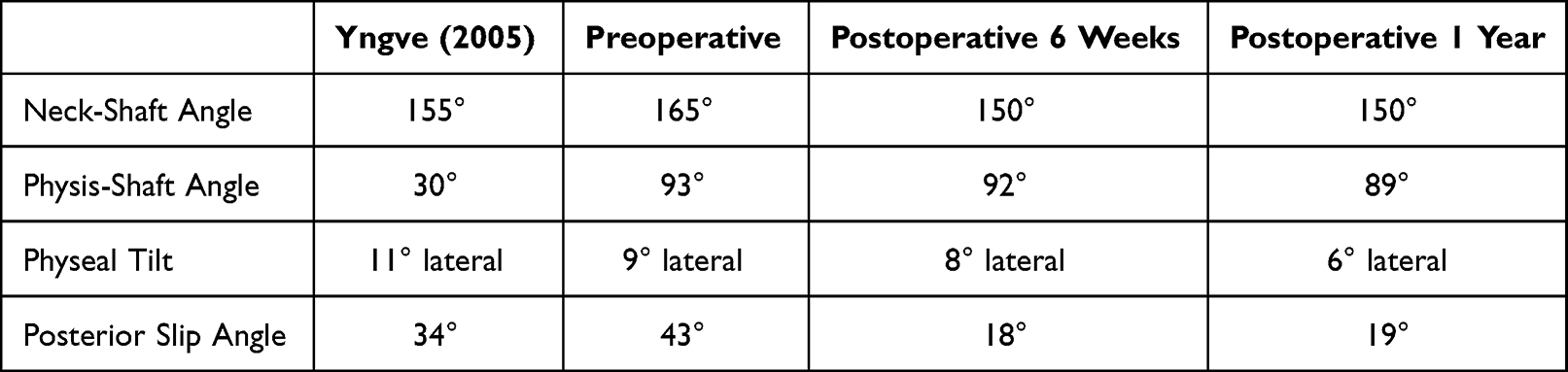 |
Table 3 Radiographical Measurements |
Our literature review did not identify any case reports or studies describing the presentation and management of acute, unstable valgus SCFE. We only identified three cases of acute stable valgus SCFE7–9 and one case report of acute-on-chronic unstable valgus SCFE.21 The three cases with stable valgus SCFE were managed with in-situ fixation, whereas the latter was managed with a modified Dunn’s procedure. All these studies have demonstrated positive outcomes following their chosen method of treatment. However, they were limited by a relatively short follow-up period. Radiologically, anteroposterior roentgenograms for valgus slip SCFEs always show an intact Klein’s line. We observe that there is a subtle effacement of the physis and a more circular appearance of the femoral head than the contralateral, of which the latter has yet to be described in literature.
In line with Loder’s classification of physeal stability, as our patient was unable to bear weight, it was deemed that the patient likely had unstable physes.22 In our case, following a discussion of the potential risks and expected benefits of surgery, a shared decision was made with the patient and her family for emergent stabilisation. In grossly unstable SCFE, there is a significant increase in the risk of avascular necrosis of the femoral head.23 Given the significant posterior slip angle, we performed a closed reduction. Two screws were utilised to provide additional mechanical stability.24 Although a previous series have shown favourable results following capital realignment surgery in the context of valgus SCFE,25 other authors have cautioned against performing such a procedure in low-volume centres.26
The main concern for the passage of cannulated screws in valgus SCFE is the proximity of the femoral vessels to the medial entry point for percutaneous pinning. We took care to protect the neurovascular bundle by identifying the position and depth of the bundle under sonographic guidance preoperatively and ensuring that our entry point remained lateral to this. Once the skin incision was made, we used a nick and spread technique. A drill sleeve was also used to prevent inadvertent damage to the bundle. Finally, the vascularity was assessed by palpation of distal pulses, at the end of the procedure. Unfortunately, despite aiming the guidewire at the centre of the femoral head, it was apparent from postoperative radiographs that the screw was lateral to its ideal position. This highlights the technical challenge in performing lateral percutaneous pinning in patients with valgus slips. We utilised the approach withdraw technique, as well as postoperative low-dose CT to mitigate the risk of screw penetration, which can cause chondrolysis.27,28
Prophylactic pinning was performed for this patient as she had a few identified risk factors for contralateral slip, specifically coxa valga and posterior slope angle of greater than 13 degrees.1,29 Additionally, this patient resided in a remote community, where timely access to medical services is a known barrier.30 Although there is a risk of chondrolysis and fracture, guidance from the American Orthopaedic Association is in favour of prophylactic pinning in patients with risk factors.31 In our patient, this was unfortunately complicated by epiphyseal escape, necessitating revision after a year of follow-up.
In conclusion, we present a rare case of acute unstable valgus slip that was managed with closed reduction and percutaneous pinning. This case highlights the need for both anteroposterior and lateral radiographs, as well as the technical challenges in managing this presentation. At 18 month follow-up, the patient was doing well with no slip progression.
Data Sharing Statement
The data supporting the findings of this study can be obtained from the corresponding author according to reasonable request, and the corresponding author can be directly contacted for further inquiry.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Assi C, Mansour J, Kouyoumdjian P, Yammine K. Valgus slipped capital femoral epiphysis: a systematic review. J Pediatr Orthop B. 2021;30(2):116–122. doi:10.1097/BPB.0000000000000758
2. Muller W. Coxa valga caused by a dislocation of the epiphysis. Beitr Klin Chir. 1926;137:148–164.
3. Loder RT, O’Donnell PW, Didelot WP, Kayes KJ. Valgus slipped capital femoral epiphysis. J Pediatr Orthop. 2006;26(5):594–600. doi:10.1097/01.bpo.0000230331.96157.14
4. Shank CF, Thiel EJ, Klingele KE. Valgus slipped capital femoral epiphysis: prevalence, presentation, and treatment options. J Pediatr Orthop. 2010;30(2):140–146. doi:10.1097/BPO.0b013e3181d076b6
5. Millis MB. SCFE: clinical aspects, diagnosis, and classification. J Child Orthop. 2017;11(2):93–98. doi:10.1302/1863-2548-11-170025
6. Loder RT, Richards BS, Shapiro PS, Reznick LR, Aronson DD. Acute slipped capital femoral epiphysis: the importance of physeal stability. J Bone Joint Surg Am. 1993;75(8):1134–1140. doi:10.2106/00004623-199308000-00002
7. Amiraian DE, Sarwar Z, Bireley WR, Moran E. Valgus slipped capital femoral epiphysis with contralateral pre-slip. Skeletal Radiol. 2017;46(9):1261–1265. doi:10.1007/s00256-017-2654-1
8. García-Mata S, Hidalgo-Ovejero A. Valgus slipped capital femoral epiphysis. Iowa Orthop J. 2010;30:191–194.
9. Segal LS, Weitzel PP, Davidson RS. Valgus slipped capital femoral epiphysis. Fact or fiction? Clin Orthop Relat Res. 1996;322:91–98. doi:10.1097/00003086-199601000-00011
10. Cheok T, Smith T, Berman M, et al. Is the modified Dunn’s procedure superior to in situ fixation? A systematic review and meta-analysis of comparative studies for management of moderate and severe slipped capital femoral epiphysis. J Child Orthop. 2022;16(1):27–34. doi:10.1177/18632521221078864
11. Hassan T, Abdelmaguid T, Ahmed Z. The modified Dunn procedure for unstable slipped capital femoral epiphysis: a systematic review and meta-analysis. QJM. 2020;113(Supplement_1):
12. Lykissas MG, McCarthy JJ. Should all unstable slipped capital femoral epiphysis be treated open? J Pedia Orthopaed. 2013;33(Supplement 1):S92–S98. doi:10.1097/BPO.0b013e318274f716
13. Peterson MD, Weiner DS, Green NE, Terry CL. Acute slipped capital femoral epiphysis: the value and safety of urgent manipulative reduction. J Pedia Orthopaed. 1997;17(5):648–654. doi:10.1097/01241398-199709000-00013
14. Gordon JE, Abrahams MS, Dobbs MB, Luhmann SJ, Schoenecker PL. Early reduction, arthrotomy, and cannulated screw fixation in unstable slipped capital femoral epiphysis treatment. J Pedia Orthopaed. 2002;22(3):352–358. doi:10.1097/01241398-200205000-00017
15. Novais EN, Maranho DA, Heare T, Sink E, Carry PM, O’Donnel C. The modified Dunn procedure provides superior short-term outcomes in the treatment of the unstable slipped capital femoral epiphysis as compared to the inadvertent closed reduction and percutaneous pinning: a comparative clinical study. Int Orthop. 2019;43(3):669–675. doi:10.1007/s00264-018-3993-9
16. Gagnier JJ, Kienle G, Altman DG, Moher D, Sox H, Riley D. The CARE guidelines: consensus-based clinical case reporting guideline development. BMJ Case Rep. 2013;2013(1):bcr2013201554. doi:10.1136/bcr-2013-201554
17. Nguyen AR, Ling J, Gomes B, Antoniou G, Sutherland LM, Cundy PJ. Slipped capital femoral epiphysis: rising rates with obesity and aboriginality in South Australia. J Bone Joint Surg Br. 2011;93(10):1416–1423. doi:10.1302/0301-620X.93B10.26852
18. Madhuri V, Arora SK, Dutt V. Slipped capital femoral epiphysis associated with vitamin D deficiency: a series of 15 cases. Bone Joint J. 2013;95(6):851–854. doi:10.1302/0301-620X.95B6.30806
19. Liu RW, Fraley SM, Morris WZ, Cooperman DR. Validity and clinical consequences of a rotational mechanism for slipped capital femoral epiphysis. J Pedia Orthopaed. 2016;36(3):239–246. doi:10.1097/BPO.0000000000000438
20. Yngve DA, Moulton DL, Burke Evans E. Valgus slipped capital femoral epiphysis. J Pediatr Orthop B. 2005;14(3):172–176. doi:10.1097/01202412-200505000-00006
21. Venkatadass K, Shetty AP, Rajasekaran S. Valgus slipped capital femoral epiphysis: report of two cases and a comprehensive review of literature. J Pediatr Orthop B. 2011;20(5):291–294. doi:10.1097/BPB.0b013e328346d2ec
22. Ziebarth K, Domayer S, Slongo T, Kim Y-J, Ganz R. Clinical stability of slipped capital femoral epiphysis does not correlate with intraoperative stability. Clin Orthop Relat Res. 2012;470(8):2274–2279. doi:10.1007/s11999-012-2339-y
23. Loder RT. What is the cause of avascular necrosis in unstable slipped capital femoral epiphysis and what can be done to lower the rate? J Pediatr Orthop. 2013;33(Suppl 1):S88–91. doi:10.1097/BPO.0b013e318277172e
24. Kishan S, Upasani V, Mahar A, et al. Biomechanical stability of single-screw versus two-screw fixation of an unstable slipped capital femoral epiphysis model: effect of screw position in the femoral neck. J Pediatr Orthop. 2006;26(5):601–605. doi:10.1097/01.bpo.0000230328.06460.be
25. Kalhor M, Gharanizadeh K, Rego P, Leunig M, Ganz R. Valgus slipped capital femoral epiphysis: pathophysiology of motion and results of intracapsular realignment. J Orthop Trauma. 2018;2018:32.
26. Upasani VV, Matheney TH, Kim Y-J, Millis MB, Kasser JR, Kasser JR. Complications after modified Dunn osteotomy for the treatment of adolescent slipped capital femoral epiphysis. J Pedia Orthopaed. 2014;34(7):661–667. doi:10.1097/BPO.0000000000000161
27. Moseley C. The “approach-withdraw phenomenon” in the pinning of slipped capital femoral epiphysis. Orthop Trans. 1985;9:497.
28. Senthi S, Blyth P, Metcalfe R, Stott NS. Screw placement after pinning of slipped capital femoral epiphysis: a postoperative CT scan study. J Pediatr Orthop. 2011;31(4):388–392. doi:10.1097/BPO.0b013e318217270d
29. Park S, Hsu JE, Rendon N, Wolfgruber H, Wells L. The utility of posterior sloping angle in predicting contralateral slipped capital femoral epiphysis. J Pediatr Orthop. 2010;30(7):683–689. doi:10.1097/BPO.0b013e3181efb888
30. Morrissy RT. Lovell and Winter’s Pediatric Orthopaedics. Philadelphia: Philadelphia: Lippincott Williams & Wilkins; 2006.
31. Tornetta P, Kocher MS, Probe RA, Foster TE, Silvestri L. Myth busters: an AOA symposium: AOA critical issues. J Bone Joint Surg Am. 2014;96(19):e170. doi:10.2106/JBJS.L.01536
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.