")
Back to Journals » Nature and Science of Sleep » Volume 14
Can You Sleep? – Effect of Retrospective Recall of Child Maltreatment on Sleep Parameters and the Mediating Role of Psychological Distress Among Students of Two German Universities
Authors Jarczok M , Lange S, Domhardt M, Baumeister H, Jud A
Received 31 January 2022
Accepted for publication 14 June 2022
Published 18 July 2022 Volume 2022:14 Pages 1299—1310
DOI https://doi.org/10.2147/NSS.S360610
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sarah L Appleton
Marion Jarczok,1,* Stephanie Lange,1,* Matthias Domhardt,2 Harald Baumeister,2 Andreas Jud1,3
1Department of Child and Adolescent Psychiatry/Psychotherapy, University Medical Center Ulm, Ulm, Germany; 2Department of Clinical Psychology and Psychotherapy, Institute of Psychology and Education, Ulm University, Ulm, Germany; 3School of Social Work, Lucerne University of Applied Sciences and Arts, Lucerne, Switzerland
*These authors contributed equally to this work
Correspondence: Marion Jarczok, Department of Child and Adolescent, Psychiatry/Psychotherapy, University Medical Center Ulm, Steinhövelstraße 5, Ulm, BW, 89075, Germany, Tel +49 731 500-61610, Fax +49 731 500-61602, Email [email protected]
Purpose: Child maltreatment may be linked with long-term sleeping disorders and limited coping with stress. Yet, the potential relationships are only marginally studied.
Patients and Methods: Based on a sample of young adults (n = 312) this study aims at exploring the effects of child maltreatment and the experience of threat to personal safety and life in childhood on sleep disturbances in early adulthood. Data were collected at the two study sites, Ulm University and Bielefeld University, by an online survey. For both risk factors, child maltreatment and the experience of threat to personal safety and life in childhood, a direct impact on sleep disturbances and an indirect path via psychological distress were tested using Structural Equation Modelling (SEM).
Results: In these models, the direct path to sleep disturbances turned out to be significant for the experience of threat to personal safety and life (Path C: b = 0.18, p = 0.013), but not for child maltreatment (Path C: b = 0.05, p = 0.491). However, the current level of psychological distress was found to have a mediating effect on sleep disturbances for both risk factors, thereby confirming indirect significant effects.
Conclusion: Considering that the etiological pathway of child maltreatment on sleeping disturbances is mediated via psychological distress, this provides a venue to test in future research whether stress reduction interventions can reduce the negative consequences of child maltreatment on sleep disorders.
Keywords: sleep disorders, child maltreatment, stress, unsafety, structural equation modelling
Introduction
A safe and protective environment is essential for restful sleep. Sleep quality is important for physical and mental development, but also for an active vigilance system.1 However, a good many adults have been affected by maltreatment and threat to personal safety and life in their familiar environment during childhood [e.g.2,3]. These adverse experiences may provoke persistent stress and hyperarousal in the body. Consequently, they potentially lead to sleep disturbances that may persist into adulthood.
Sleep disorders are a common phenomenon and cause both adverse psychological and physical health effects [e.g.4,5]. First, sleep problems may cause restrictions in daily functioning like severe fatigue, exhaustion, pain or an increase in blood pressure. Second, they may excite long-term effects like difficulties in affective reactions and emotional regulation, concentration problems with associated underachievement in academic performance or substance use and are associated with a tendency to suicidal behavior.6
The fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) defines several categories of sleep-wake disorders like insomnia disorder, parasomnias, hypersomnia disorder, narcolepsy or the restless-legs syndrome.7 The present article focuses on insomnias and parasomnias. According to DSM-5, insomnia disorders cause dissatisfactions with the quality or quantity of sleep that negatively affect everyday live. The dissatisfaction may be linked to symptoms like the difficulty falling asleep, sleeping through the night or early awakening.8,9 Following DSM-5, parasomnias include nightmare disorders, pavor nocturnus, somnambulism, non-rapid-eye-movement-sleep arousal disorders and REM sleep behavior disorder.8,9 In the following analysis, parasomnias are mainly described by nightmare disorders.
Besides environmental factors, eg, noise,10,11 a great many of both sociodemographic characteristics like age or gender12,13 and individual behaviors (eg, drug consumption, lifestyle)14,15 were identified to have an effect on sleep quality. Previous research has also found that people with adverse childhood experiences are more likely to manifest sleep disorders.16–18 In addition, post-traumatic nightmares are integrated into dysphoric dream imagery as part of a neurocognitive model.19 Based on a life course epidemiological perspective on health, a history of child maltreatment influences health outcomes like sleep quality until adulthood [cf.20,21]. Nevertheless, there is a lack of empirical research focusing on the long-term impact of child maltreatment on sleep disorders.6
The US Centers of Disease Control (CDC) define child maltreatment as
any act or series of acts of commission (child abuse) or omission (child neglect) by a parent or other caregiver that results in harm, potential for harm, or threat of harm to a child.22 It includes all types of physical abuse, sexual abuse, and psychological abuse (acts of commission), as well as physical neglect, emotional neglect, medical/dental neglect, educational neglect, inadequate supervision, and exposure to violent environments. (acts of omission)
Among the different subtypes, physical and sexual abuses are sometimes conceptualized as event-typed, whereas neglect and psychological abuse are more strongly attributed to describing the relationship between caregiver and child.23 Findings support the notion that event-type abuse elicits particular effects on the brain, distinguishing it from those evoked by chronic emotional neglect and psychological abuse. Stress responses to violent incidents provide an explanatory model for these neurobiological findings.24
A prospective study showed that the prevalence of sleep problems is higher for young women with an experience of substantiated child sexual abuse compared to the unencumbered control group even 10 years after disclosure of the experience.25 Adolescents exposed to interpersonal violence are at risk for insomnia symptoms; exposure to rape carries the greatest risk compared to all other adversities.26 Additional empirical evidence for an independent effect of both child maltreatment and stressful life events on sleep disturbances while controlling for anxiety and depression was found.27 Another study found an association between very early adversities (0–6 years) and nightmare severity.28 A recent study of a cross-sectional German sample showed that impaired subjective sleep was significantly predicted by child maltreatment experiences and that this association was mediated by rumination and romantic relationship satisfaction.29 Yet, these examples cannot hide the lack of research exploring the various potential pathways between adverse experiences in childhood and sleep disturbances. In particular, the link between child maltreatment and parasomnias, such as nightmares, went unheeded so far, while the prevalence of nightmares seems to be higher for young adults with traumatic childhood experiences compared to those without liabilities.30
In line with previous findings,16,25,27 describing the relationship between adverse childhood experiences and sleep disturbances, the following hypothesis is derived (see Figure 1):
H1: Experiences of child maltreatment increase sleep disturbances in early adulthood.
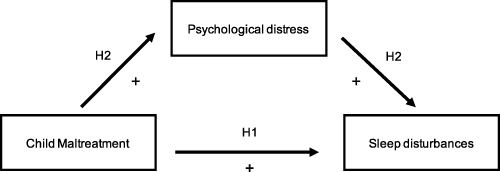 |
Figure 1 The effect of child maltreatment on sleep disturbances in early adulthood. Note: Arrows indicate conceptual pathways that illustrate probable causal connections. |
Protection and safety are central elements for humans to rest and sleep. The Generalized Unsafety Theory of Stress (GUTS) addresses this idea, stating that prolonged stress responses are not due to (conventional) stressors but to generalized and largely unconsciously perceived unsafety.31,32 Certain incidents of child maltreatment may cause persistent feelings of threat to personal safety and life. The threat to personal safety and life may be provoked either by the perception of an unsafe environment or a direct threat of killing. Feelings of unsafety and threat lead to a chronic state of (hyper) arousal of the body, which prevents restful sleep.33 Therefore, if the sense of protection or safety is disturbed in children or adolescents, this is likely to lead to a persistent disorder in sleep behavior [eg,6,25] (see Figure 2).
H3: Experiences in childhood that pose a threat to life or fundamental safety increase sleep disturbances in early adulthood.
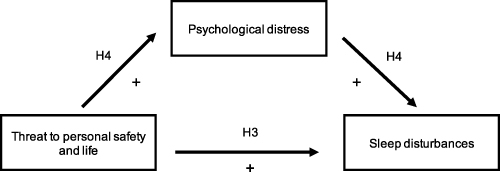 |
Figure 2 The effect of existential threat in childhood on sleep disturbances in early adulthood. Note: Arrows indicate conceptual pathways that illustrate probable causal connections. |
Besides an evoked state of (hyper-)arousal that causes physical stress, child maltreatment also impairs the processing of current stress like worry or overload. It is assumed that childhood victimization leads to long-term inappropriate coping behavior, which may cause problems in dealing and coping with stress in later life.34 Empirical research has found evidence for maltreatment that evokes maladaptive coping strategies concerning daily stressors35 and increasing adult work stress.36 Besides the impairment of daily routines, maltreatment has been found to elicit severe mental illness like adult depression,37 post-traumatic stress disorder,38 as well as excessive alcohol use.39 Going one step further, both a lack of stress management40,41 and mental illness42,43 are found to evoke sleep disorder.
Moreover, young adults regularly face a number of stressors associated with their period of life like examination stress, break-ups of romantic relationships or other changes in life situations. On top of that, recent research presented evidence that SARS-CoV-2-related stress through social restrictions or uncertainty was evoking sleep disorders.44,45
In line with the argumentation that child maltreatment and psychological (di)stress have an effect on sleep disturbances,25 the following hypotheses are derived (see Figures 1 and 2):
H2: The relationship between child maltreatment and sleep disturbances in early adulthood is mediated by psychological (di)stress. H4: The relationship between threat to personal safety and life in childhood and sleep disturbances in early adulthood is mediated by psychological (di)stress.
Materials and Methods
Data Collection Procedure
Data were collected from a cross-sectional online survey at the two study sites, Ulm University and Bielefeld University. The study retrospectively collected experienced child maltreatment as well as current psychological distress and sleep problems via self-report. The survey was programmed at Ulm University using the software Unipark (for information, see www.unipark.com). At the study site Ulm, it was conducted between March 13 and August 31, 2020, with an average duration for survey completion of 21 minutes. Participants were recruited via electronic mailing lists of the psychology faculty, as well as via Ulm University student groups on Facebook. Recruitment via Facebook groups was selected as an alternative pathway of communication due to the first Corona lockdown in Germany in 2020. At Bielefeld University, data were collected between the end of June and the end of August 2020 through recruitment via the social media messenger WhatsApp and the social media platform Facebook. At Bielefeld University, participating students were given credits on their trial search hours account and were rewarded with a raffle. At both sites, participation was voluntary and anonymous, ie no personal data was collected other than age, gender and study course; survey entries were not connected with data on credits. We have obtained informed consent from all participants via an online form on the starting page of the survey. The study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of Ulm University (333/19-FSt/Sta).
Participants
Our study included a sample size of 312 with 211 students from Ulm University (mean age 24.67) and 101 from Bielefeld University (mean age 23.24). Participants were recruited mainly in the study fields of medicine (Ulm University) and psychology (Ulm and Bielefeld universities). Thus, the subjects most frequently attended consequently were medicine (41.35%) and psychology (37.50%) with a total mean number of 4.65 semesters. A large majority of the sample (78.85%) was female (75.83% in Ulm and 85.15% in Bielefeld). To guarantee homogeneity in terms of age, we only included participants up to an age of 39 with a mean age of 24.21 for analysis. As sleep behavior changes, such as decreases in arousal parasomnias, around age 25,46 our sample is a suitable basis to analyze factors influencing the quality of sleep both for late adolescence and early adulthood.
Measures
Sleep Disturbances
Sleep disturbances were assessed firstly as general sleep quality with the Pittsburgh Sleep Questionnaire (PSQI) and secondly specifically for the subcategories “insomnia” with the Insomnia Questionnaire for Adults (IQA) and “nightmares (as part of parasomnias)” with the Nightmare Effects Questionnaire (NEQ). The PSQI is an instrument to measure sleep quality and disturbance for the preceding one-month period. It includes 19 items covering seven categories for score building: “subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medication, and daytime dysfunction” (40, p.193). The PSQI is operationalized by a global score consisting of individual scores for the seven categories.47 The IQA covers 11 items screening for insomnia symptoms on a binary scale.48 For operationalization, we added up non-zero values and divided them by the total number of items. The NEQ captures questions both on the frequency of nightmares and on the resulting daily disturbances at different scales for each section.49 For operationalization, we calculated a weighted measure (in the following, called nightmares): We used the first NEQ item with a four-point-scale on the frequency of nightmares during the preceding six months and weighted this frequency by multiplying it with the aggregated individual assessment of daily disturbance and well-being (item 38) on an 11-point-scale.
Child Maltreatment
Child maltreatment was assessed by using the ISPCAN Child Abuse Screening Tools Retrospective version (ICAST-R).50 Advantageously, for research studies on child maltreatment, data from retrospective responses have been shown to be trustworthy.51–53 The questionnaire was translated into German and used for piloting. The ICAST-R captures experiences of violence by adults and/or peers before the age of 18. Respondents are not asked broad terms such as “violence” or “abuse”, instead the items ask about the occurrence of specific behaviors, eg “When you were growing up (before age 18) did anyone ever beat you with an object like a stick, broom or belt?”. The ICAST-R aims to have respondents recall discrete and usually serious, undesirable actions, and, when prompted, recall some of the context.54 The ICAST-R screens for neglect and physical-, emotional- and sexual abuse as well as the perception of emotional and physical care. In addition, contextual information on frequency, age at the time of the act, subjective severity and information on perpetrators were collected. For operationalization, we weighted items on neglect and the different types of abuse by their frequency. Subsequently, we added up weighted items in each of the five categories mentioned above and divided the amount by the total number of items for each category. Though internationally broadly used,50,55–57 the ICAST-R had not previously been validated in German. Hence, a confirmatory factor analysis (CFA) was conducted to assess the usefulness of the latent construct. Threat to personal safety and life was operationalized by two ICAST-R variables from the neglect and emotional abuse categories: 1) threatened to be badly hurt or killed and 2) no safe place to live.
Psychological Stress
The literature reports empirical evidence on the relationship between (daily) stress and sleep disturbances (eg,58). We used the Perceived Stress Questionnaire (PSQ) to measure the current stress of participants. Items capture the subjective perception, evaluation and further processing of stressors. We used the 20-item short version59 to include questions on worries, tensions, joy and demands within the last four weeks. Each dimension is captured by five items on a four-point scale with 1 for “almost never” to 4 for “most of the time”. We used a calculation template for operationalization.60 To control for individual stress caused by the COVID-19 pandemic due to uncertainty and social isolation, we included a self-developed measure “How much do you worry about the coronavirus (COVID −19)?”. This item captures the extent of current worries due to pandemic on a ten-point-scale with 0 “I am not worried at all” to 9 “I am very worried”.
As described above, there is empirical evidence on the relationship between psychological distress and sleep disturbances (e.g.27,61). In order to measure somatization, depression and anxiety in the preceding week we used the short version of the Brief Symptom Inventory (BSI-18). The questionnaire includes six items per dimension. The total score, which is called “Global Severity Index (GSI)”, reflects the general psychological distress. All items are scored on a five-point Likert scale.62 Internal consistency of the latent construct mental (di)stress was given by Cronbach’s α = 0.83.
Sleep quality changes with age.63 To capture age-effects, we integrated a control variable that measured the age of participants on the day of survey completion. Previous findings indicate gender-related differences having an effect on sleep disorders.64,65 Therefore, we integrated a binary construct to capture gender-related effects in our model.
Statistical Analysis
Confirmatory factor analyses were applied to all latent constructs to evaluate the overall pattern of fit of the latent variables included in the model. The first mediation model focused on all experiences of abuse or neglect during childhood. The second model further explores the potential role of reporting the experience of threat to personal safety and life as a child. For evaluation of the models, we used the following criteria on goodness of fit based on the recommended cut-offs:66 Tucker–Lewis Index (TLI) above 0.95, Comparative Fit Index (CFI) above 0.90, and Root-Mean-Square Error of Approximation (RMSEA) below 0.08 as well as Chi-squared (χ2) and critical ratio (χ2/df) below 3.67
Mediation analysis was performed using the maximum likelihood estimation method with missing values. All statistical analyses were performed using STATA v15.1 SE (Stata Corp, LLC, College Station, TX); p < 0.05 was considered statistically significant.
Results
Descriptive Statistics and Estimation
The analytic sample includes 312 participants with the following prevalence of child maltreatment (see Table 1): 56.4% emotional abuse, 30.1% neglect, 23.7% sexual abuse, 20.2% physical abuse, 17.0% lack of emotional or physical care. Moreover, 1.92% of the sample marked the item “no safe place to live”, 5.1% the item “threatened to be killed”. Thus, a total of 215 (68.9%) participants experienced any type of child maltreatment and a total of 20 (6.4%) participants were threatened to personal safety or life during childhood. Correlations are presented in Supplementary Table 1 (see Supplemental Information).
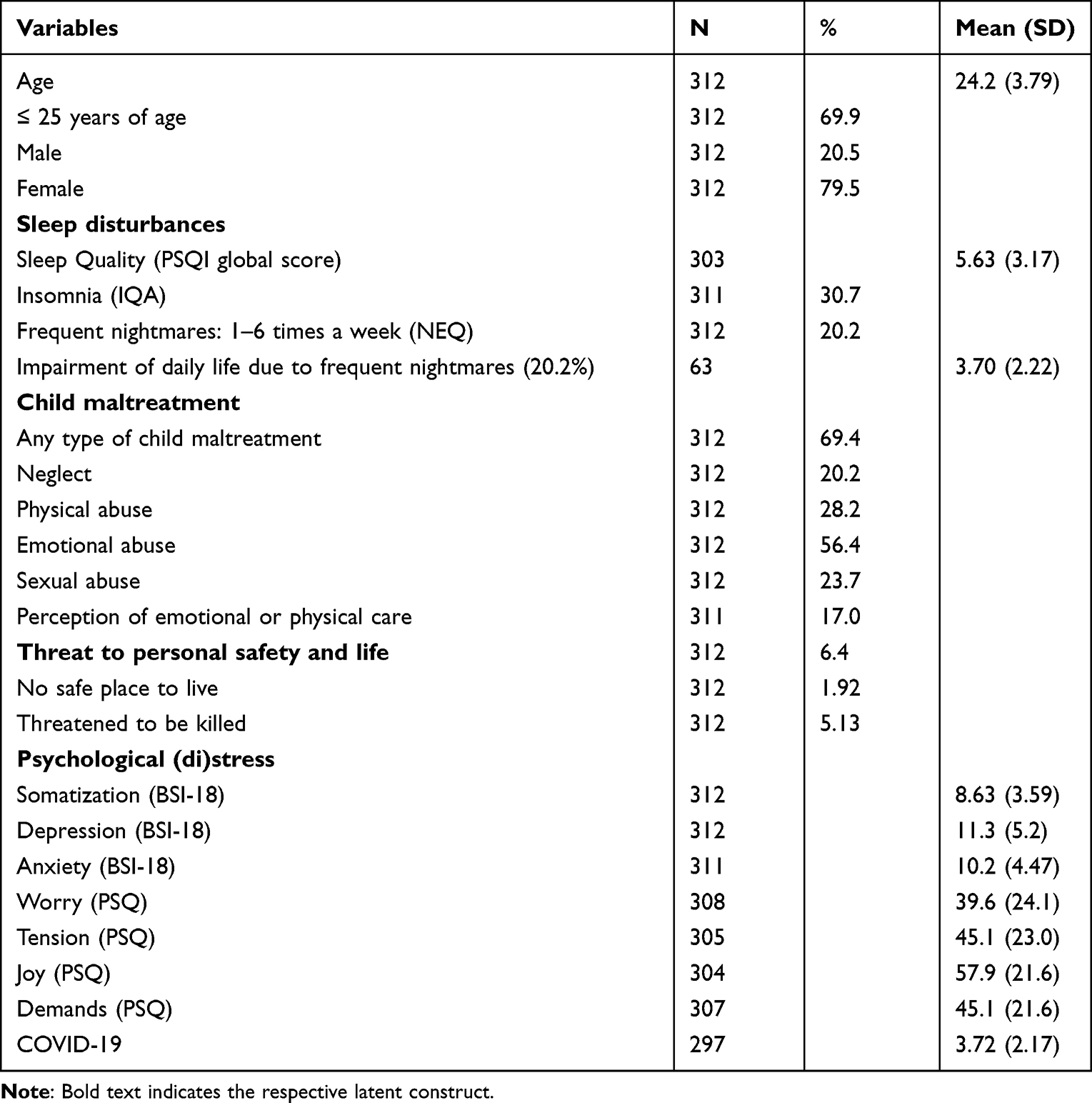 |
Table 1 Descriptive Statistics of Participants |
Results from Structural Equation Modelling
The CFAs showed that all observed variables loaded onto the latent constructs that were included in the models (see Supplementary Table 2). Mediation analysis results indicated that the direct effect between child maltreatment and sleep quality in early adulthood was mediated by psychological (di)stress (total effect: b = 0.39, p < 0.001). Individuals who were frequently exposed to child maltreatment had higher levels of perceived psychological (di)stress in early adulthood than individuals who experienced fewer incidents of child maltreatment (Path A: b = 0.51, p < 0.001). Furthermore, individuals who exhibited higher levels of mental (di)stress were more likely to experience sleep problems (Path B: b = 0.67, p < 0.001), see Figure 3.
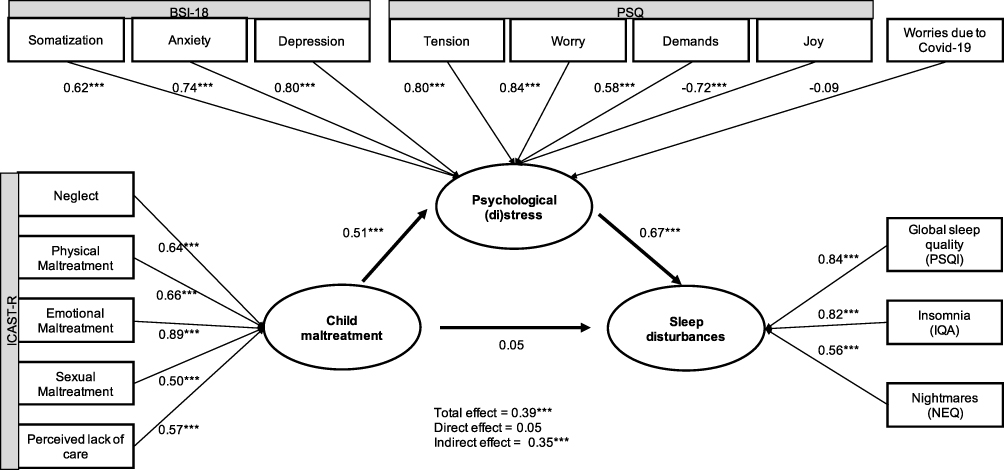 |
Figure 3 Mediation analysis of child maltreatment and psychological distress on sleep disturbances. Notes: Coefficients are standardized (β). Model fit: RMSEA = 0.052; CFI: 0.961; TLI = 0.949; Coefficient of determination (R2) = 0.871. χ2: 213.288 (df = 115; χ2/df = 1.855). Analyses control for gender and age (≤25). ***p ≤ 0.001, N = 312. Latent constructs are marked bold, and the corresponding names of the instruments are highlighted grey. |
The results showed no evidence that child maltreatment affects sleep quality independently of psychological (di)stress (Path C: b = 0.05, p = 0.491). The covariate age had no effect on the perception or development of psychological (di)stress (b = 0.060, p = 0.279), while it was significantly associated with sleep problems (b = 0.19, p < 0.001). In contrast, gender was significantly associated with psychological (di)stress (b = −0.14, p = 0.014), while it was not significantly associated with sleep problems.
To further investigate the potential moderating role of gender on psychological (di)stress, a moderated mediation was explored. The analyses showed that the interaction between child maltreatment and male gender on psychological (di)stress was not significant (b = −0.05, p = 0.389). Thus, the indirect effect of child maltreatment on sleep quality due to psychological (di)stress was not moderated by gender (data not shown). In summary, these results suggest a simple total mediation: the association between child maltreatment and sleep problems in early adulthood is mediated by psychological (di)stress. The model fits are all at a good level (see Figure 3).
The second mediation model further explores the role of threat to personal safety and life. Here, a direct association between threatening experiences on sleep disturbances (Path C: b = 0.18, p = 0.013) was observed.
Individuals who were frequently threatened had higher levels of psychological (di)stress in adulthood than individuals who experienced fewer experiences of threat to personal safety and life (Path A: b = 0.30, p < 0.001). Furthermore, individuals who exhibited higher levels of psychological (di)stress were more likely to experience sleep problems (Path B: b = 0.64, p < 0.001); see Figure 4. In sum, the association between threat to personal safety and life and sleep disturbances in early adulthood (total effect: b = 0.37, p < 0.001) was partly mediated by higher psychological (di)stress (b = 0.20, p < 0.001). The model fits were all at a good or acceptable level (see Figure 4). Here, the covariate age was significantly associated with the perception or development of psychological (di)stress (b = 0.12, p = 0.045) as well as with sleep problems (b = 0.19, p < 0.001). Gender was also significantly associated with psychological (di)stress (b = −0.17, p = 0.005), but it was not associated with sleep problems.
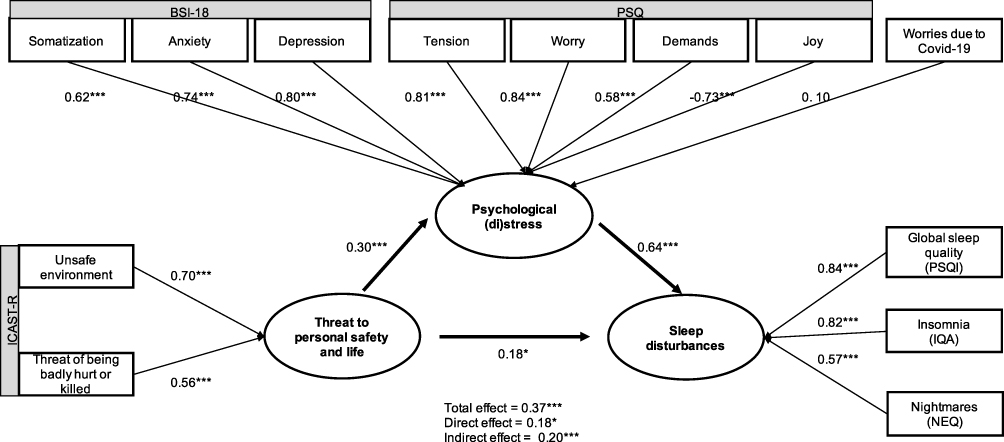 |
Figure 4 Mediation analysis of threat for personal safety and life and psychological distress on sleep disturbances. Notes: Coefficients are standardized (β). Model fit: RMSEA = 0.065; CFI: 0.950; TLI = 0.931; Coefficient of determination (R2) = 0.665. χ2: 172.941 (df = 75; χ2/df = 2.231). Analyses control for gender and age (≤25). *p < 0.05. ***p ≤ 0.001, N = 312. Latent constructs are marked bold, and the corresponding names of the instruments are highlighted grey. |
Discussion
This study analyzed the relationship between child maltreatment and long-term sleep disturbances. Child maltreatment epidemiology underlines the vast prevalence of these phenomena with long-term effects at all levels of health and personal well-being: In line with international literature,2,68 a recent, 2016 nationwide German survey reports lifetime-prevalence of child sexual abuse at 13.9%, physical abuse at 12.3%, emotional maltreatment at 18.6%, emotional neglect at 40.5% and physical neglect at 41.9%.3 The vast prevalence underscores the need to further explore the impact of child maltreatment on sleep symptomatology. To the best of our knowledge, this is the first study to combine instruments for measuring child maltreatment, current stress, parasomnia and insomnia symptoms in one model.
Besides a direct effect between child maltreatment and sleep disturbances, it was assumed that an indirect path is mediated by psychological (di)stress. Based on Structural Equation Modelling, the postulated direct effect of child maltreatment on sleep disturbances in Figure 1 could not be confirmed (H1), whereas the second model (Figure 2) yielded a direct effect of threat to personal safety and life on sleep disturbances in early adulthood (H3). In support of Hypotheses 2 and 4 the Structural Equation Models show a positive and significant effect of the mediating role of psychological (di)stress on the association of child maltreatment, respectively, threat to personal safety and life on sleep disturbances. The concept of general unsafety, as described in the GUTS and proxy-measured via the items on threat to personal safety and life, may provide a theoretical basis for the present findings, including the present direct effect of threat to personal safety and life and the lack of a direct effect of child maltreatment. In brief, GUTS conceptualizes the classical stress response as a physiological state that is inhibited by higher order brain centers from the central autonomic network in moments of safety perception. Moreover, GUTS explicitly addresses conscious and unconscious stress cognitions. The concept of “generalized unsafety” is more significant when it comes to the causes of prolonged activity than the stress responses to specific unsafeties as they appear in the conventional stress theory.31,32 Clearly, sleep is a state when someone cannot consciously worry or ruminate. Our results may show that worrying or rumination continues in an unconscious fashion due to the experience of threat to personal safety and life, and thus the physiological stress effects that lead to sleep disturbance continue to be present. The indirect effect of child maltreatment via higher psychological distress speaks for a primarily cognitive conscious type of rumination and worrying.
The results of this study are in line with the argumentation that current stress and mental health problems like, for example, depression are found to impair sleep quality. Depression is both a potential acute and long-term consequence of child (sexual) abuse.69 Moreover, behaviors associated with depression – cognitive hyperactivation such as excessive worrying, rumination, and negative attributions – lead to increased physical and mental arousal6 as well as depressive-like pathophysiology. Those are characterized by elevated plasma cortisol levels at the onset of sleep, increased sleep latency, or significant dysregulation of rapid eye movements.6 Thus, a high prevalence of sleep disturbances has been found among depressed individuals.27,70
By providing empirical evidence on the relationship between adverse childhood experiences and early adult sleep problems, this study contributes to bridging research gaps on the long-term effects of child maltreatment identified in a recent review.6 The empirical model furthermore shows age but not gender to have a significant effect on sleep disturbances.
There is a lack of research on parasomnias and child maltreatment that this study partially addresses with items on nightmares. The exploratory research is based on a sample with a selection bias as indicated by the extensive prevalences of child maltreatment that go well beyond the already marked prevalences of child maltreatment in the German general population.3 Also with regard to nightmares, students show a higher frequency (20%) compared to the German general population (2.4% of the sample with 1 or more nightmares a week).71 This finding might partly be associated with the elevated rate of child maltreatment in the sample but also fits into the international research picture: Studies focusing on sleep disorders among students show that especially this group of young adults is at increased risk.72–75 In particular, nightmares are reported as high as 19% among students.74 Studies have repeatedly pointed to the impact of the COVID-19 pandemic on psychological health and sleep disturbances.76,77 Somewhat surprisingly, we have not found a significant relation between worries related to the COVID-19 and psychological distress. This might both be associated with data collection in the early days of the spread of COVID-19 and a sample of persons in early adulthood who are much less at risk of fatal outcomes of COVID-19 than elderly people.
Strengths and Limitations
While the study explores novel pathways, it also comes with limitations. Note that the sample of this exploratory study is based on a student survey limited in size and does not claim to be representative of the generation of young adults in Germany. On top of recruitment via virtual lectures, snowballing sampling strategies have been used. The latter are particularly prone to biased sampling as victimized young adults are more likely to reach out to other victimized peers. As discussed above, in particular, the rates of several types of child maltreatment are rather elevated: In comparison to a German population survey,3 both the percentages of physical abuse and sexual abuse in the present sample are markedly elevated, and percentages of neglect decreased. Moreover, the distribution of genders in the sample is largely uneven. As women have been found to more readily disclose incidents of child maltreatment (e.g.78), they might more readily participate in exploratory surveys. The uneven gender distribution and small male sample might also be responsible for a lack of reproducing previously reported effects of gender on sleep disturbances.65,79
Previous research highlighted that adult survivors of child maltreatment, contrary to myths, may appreciate studies on the prevalence of child maltreatment as an opportunity for disclosure, as they identify benefits of participation and minimal distress while participating [e.g.80]. The decreased rate of neglect, on the other hand, may relate to the student sample as rates of neglect are increased among the economically disadvantaged families [e.g.81] with children less likely to advance to university degrees.
Second, other studies point to delayed “bedtimes and risetimes” during weekend, alcohol and caffeine consumption to have an effect on sleep quality in students [see15]. However, this study does not control for those individual behaviors or environmental factors. Third, when regarding the definition of parasomnia, this study captures only a small part of symptoms by operationalizing nightmares. Future research could work on this by analyzing the effects of child maltreatment on further parasomnia symptoms like, for example, sleepwalking or sleep-related eating disorders. Finally, it must be noted that a retrospective cross-sectional design is present, meaning that exposure and outcome were recorded simultaneously. Given the chronological fact that the child maltreatment experiences are past events (under 18 years of age) but the current sleep quality and psychological distress were assessed, the direction of association(s) between exposure and outcome is most likely plausible.
Conclusion
In conclusion, we have found a statistically significant indirect effect of child maltreatment on sleeping disturbances (via psychological distress) and both direct and indirect effects of the experience of threat to personal safety and life on sleeping disturbances. The exploratory analyses of potential pathways from child maltreatment and threat to personal safety and life to sleeping disturbances have to be both conceptually developed and further replicated with methodologically more rigorous sampling designs and controlled for additional variables. The high prevalence of sleep disorder symptoms following adverse childhood experience may be an indicator for an insufficient understanding of the needs of affected people. Considering that the etiological pathway of child maltreatment on sleeping disturbances is mediated via psychological distress, this provides a venue to test in future research whether stress reduction interventions can reduce the negative consequences of child maltreatment on sleep disorders.
Ethics Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of Ulm University (333/19-FSt/Sta). At both study sites, participation was voluntary and anonymous, ie no personal data was collected other than age, gender and study course; survey entries were not connected with data on credits. We have obtained informed consent from all participants via an online form on the starting page of the survey.
Acknowledgments
The authors would like to thank Prof. Angelika Schlarb for initiating and leading the data collection in Bielefeld and for her cooperation throughout the study.
Disclosure
All authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. World Health Organization. WHO Technical Meeting on Sleep and Health; 2004.
2. Stoltenborgh M, Bakermans-Kranenburg MJ, Alink LRA, van IJzendoorn MH. The prevalence of child maltreatment across the globe: review of a series of meta-analyses. Child Abus Rev. 2015;24(1):37–50. doi:10.1002/car.2353
3. Witt A, Glaesmer H, Jud A, et al. Trends in child maltreatment in Germany: comparison of two representative population-based studies. Child Adolesc Psychiatry Ment Health. 2018;12(1):24. doi:10.1186/s13034-018-0232-5
4. Morin CM, Drake CL, Harvey AG, et al. Insomnia disorder. Nat Rev Dis Prim. 2015;1(1):15026. doi:10.1038/nrdp.2015.26
5. Schlack R, Hapke U, Maske U, Busch M, Cohrs S. Häufigkeit und Verteilung von Schlafproblemen und Insomnie in der deutschen Erwachsenenbevölkerung [Prevalence and distribution of sleep disorders and insomnia in the German adult population]. Bundesgesundheitsblatt Gesundheitsforsch Gesundheitsschutz. 2013;56(5–6):740–748. doi:10.1007/s00103-013-1689-2
6. Giannakopoulos G, Kolaitis G. Sleep problems in children and adolescents following traumatic life events. World J Psychiatry. 2021;11(2):27–34. doi:10.5498/wjp.v11.i2.27
7. Riemann D, Baum E, Cohrs S, et al. S3-Leitlinie nicht erholsamer Schlaf/schlafstörungen [S3-Guideline on non-relaxing sleep/sleep disorders]. Somnologie. 2017;21(1):2–44. doi:10.1007/s11818-016-0097-x
8. Riemann D. Schlaf-Wach-Störungen im DSM-5. InFo Neurol Psychiatr. 2014;16(7–8):42–50. doi:10.1007/s15005-014-0787-5
9. Association AP. Diagnostic and Statistical Manual of Mental Disorders.
10. Röösli M, Brink M, Rudzik F, et al. Associations of various nighttime noise exposure indicators with objective sleep efficiency and self-reported sleep quality: a field study. Int J Environ Res Public Health. 2019;16(20):3790. doi:10.3390/ijerph16203790
11. Khaiwal R, Singh T, Tripathy JP, et al. Assessment of noise pollution in and around a sensitive zone in North India and its non-auditory impacts. Sci Total Environ. 2016;566:981–987. doi:10.1016/j.scitotenv.2016.05.070
12. van de Straat V, Buffel V, Bracke P. Medicalization of sleep problems in an aging population: a longitudinal cross-national study of medication use for sleep problems in older European adults. J Aging Health. 2018;30(5):816–838. doi:10.1177/0898264317696775
13. Moline M, Broch L, Zak R. Sleep problems across the life cycle in women. Curr Treat Options Neurol. 2004;6(4):319–330. doi:10.1007/s11940-004-0031-6
14. Zunhammer M, Eichhammer P, Busch V. Sleep quality during exam stress: the role of alcohol, caffeine and nicotine. PLoS One. 2014;9(10):e109490. doi:10.1371/journal.pone.0109490
15. Lund HG, Reider BD, Whiting AB, Prichard JR. Sleep patterns and predictors of disturbed sleep in a large population of college students. J Adolesc Heal. 2010;46(2):124–132. doi:10.1016/j.jadohealth.2009.06.016
16. Kajeepeta S, Gelaye B, Jackson CL, Williams MA. Adverse childhood experiences are associated with adult sleep disorders: a systematic review. Sleep Med. 2015;16(3):320–330. doi:10.1016/j.sleep.2014.12.013
17. Glod CA, Teicher MH, Hartman CR, Harakal T. Increased nocturnal activity and impaired sleep maintenance in abused children. J Am Acad Child Adolesc Psychiatry. 1997;36(9):1236–1243. doi:10.1097/00004583-199709000-00016
18. Nielsen T. the stress acceleration hypothesis of nightmares. Front Neurol. 2017;8:1–23. doi:10.3389/fneur.2017.00201
19. Nielsen T, Levin R. Nightmares: a new neurocognitive model. Sleep Med Rev. 2007;11(4):295–310. doi:10.1016/j.smrv.2007.03.004
20. Bader K, Schäfer V, Schenkel M, Nissen L, Schwander J. Adverse childhood experiences associated with sleep in primary insomnia. J Sleep Res. 2007;16(3):285–296. doi:10.1111/j.1365-2869.2007.00608.x
21. Greenfield EA, Lee C, Friedman EL, Springer KW. Childhood abuse as a risk factor for sleep problems in adulthood: evidence from a U.S. National Study. Ann Behav Med. 2011;42(2):245–256. doi:10.1007/s12160-011-9285-x
22. Leeb RT, Paulozzi LJ, Melanson C, Simon TR, Arias I. Child maltreatment surveillance: uniform definitions for public health and recommended data elements, version 1.0. Annu Rev Clin Psychol. 2008;1:409–438.
23. Glaser D, Prior V. Is the term child protection applicable to emotional abuse? Child Abus Rev. 1997;6(5):315–329. doi:10.1002/(SICI)1099-0852(199712)6:5<315::AID-CAR361>3.0.CO;2-A
24. Glaser D. Child abuse and neglect and the brain-a review. J Child Psychol Psychiatry. 2000;41(1):97–116. doi:10.1111/1469-7610.00551
25. Noll JG, Trickett PK, Susman EJ, Putnam FW. Sleep disturbances and childhood sexual abuse. J Pediatr Psychol. 2006;31(5):469–480. doi:10.1093/jpepsy/jsj040
26. Wang Y, Raffeld MR, Slopen N, Hale L, Dunn EC. Childhood adversity and insomnia in adolescence. Sleep Med. 2016;21:12–18. doi:10.1016/j.sleep.2016.01.011
27. Baddam SK, Olvera RL, Canapari CA, Crowley MJ, Williamson DE. Childhood trauma and stressful life events are independently associated with sleep disturbances in adolescents. Behav Sci. 2019;9(10):108. doi:10.3390/bs9100108
28. Nielsen T, Carr M, Picard-Deland C, et al. Early childhood adversity associations with nightmare severity and sleep spindles. Sleep Med. 2019;56:57–65. doi:10.1016/j.sleep.2019.03.004
29. Pfaff A, Schlarb AA. Child maltreatment and sleep: two pathways explaining the link. J Sleep Res. 2021. doi:10.1111/jsr.13455
30. Agargun MY, Kara H, Ozer OA, Selvi Y, Kiran U, Kiran S. Nightmares and dissociative experiences: the key role of childhood traumatic events. Psychiatry Clin Neurosci. 2003;57(2):139–145. doi:10.1046/j.1440-1819.2003.01093.x
31. Brosschot J, Verkuil B, Thayer J. Generalized unsafety theory of stress: unsafe environments and conditions, and the default stress response. Int J Environ Res Public Health. 2018;15(3):464. doi:10.3390/ijerph15030464
32. Brosschot JF, Verkuil B, Thayer JF. Exposed to events that never happen: generalized unsafety, the default stress response, and prolonged autonomic activity. Neurosci Biobehav Rev. 2017;74:287–296. doi:10.1016/j.neubiorev.2016.07.019
33. Dahl RE, Lewin DS. Pathways to adolescent health sleep regulation and behavior. J Adolesc Heal. 2002;31(6):175–184. doi:10.1016/S1054-139X(02)00506-2
34. Widom CS. Motivation and mechanisms in the “cycle of violence”. In: Hansen DJ, editor. Motivation and Child Maltreatment: Nebraska Symposium on Motivation.
35. Leitenberg H, Gibson LE, Novy PL. Individual differences among undergraduate women in methods of coping with stressful events: the impact of cumulative childhood stressors and abuse. Child Abuse Negl. 2004;28(2):181–192. doi:10.1016/j.chiabu.2003.08.005
36. Sampasa-Kanyinga H, Nilsen W, Colman I. Child abuse and work stress in adulthood: evidence from a population-based study. Prev Med. 2018;108:60–66. doi:10.1016/j.ypmed.2017.12.029
37. Bradley RG, Binder EB, Epstein MP, et al. Influence of child abuse on adult depression. Arch Gen Psychiatry. 2008;65(2):190. doi:10.1001/archgenpsychiatry.2007.26
38. Nemeroff CB. Paradise lost: the neurobiological and clinical consequences of child abuse and neglect. Neuron. 2016;89(5):892–909. doi:10.1016/j.neuron.2016.01.019
39. Widom CS, White HR, Czaja SJ, Marmorstein NR. Long-term effects of child abuse and neglect on alcohol use and excessive drinking in middle adulthood. J Stud Alcohol Drugs. 2007;68(3):317–326. doi:10.15288/jsad.2007.68.317
40. Dalgaard L, Eskildsen A, Carstensen O, Willert MV, Andersen JH, Glasscock DJ. Changes in self-reported sleep and cognitive failures: a randomized controlled trial of a stress management intervention. Scand J Work Environ Health. 2014;40(6):569–581. doi:10.5271/sjweh.3460
41. Herr R, Barrech A, Riedel N, Gündel H, Angerer P, Li J. Long-term effectiveness of stress management at work: effects of the changes in perceived stress reactivity on mental health and sleep problems seven years later. Int J Environ Res Public Health. 2018;15(2):255. doi:10.3390/ijerph15020255
42. Wallace DD, Boynton MH, Lytle LA. Multilevel analysis exploring the links between stress, depression, and sleep problems among two-year college students. J Am Coll Heal. 2017;65(3):187–196. doi:10.1080/07448481.2016.1269111
43. Schneiderman JU, Ji J, Susman EJ, Negriff S. Longitudinal relationship between mental health symptoms and sleep disturbances and duration in maltreated and comparison adolescents. J Adolesc Heal. 2018;63(1):74–80. doi:10.1016/j.jadohealth.2018.01.011
44. Silva E, Ono BHV, Souza JC. Sleep and immunity in times of COVID-19. Rev Assoc Med Bras. 2020;66(suppl2):143–147. doi:10.1590/1806-9282.66.s2.143
45. Altena E, Baglioni C, Espie CA, et al. Dealing with sleep problems during home confinement due to the COVID‐19 outbreak: practical recommendations from a task force of the European CBT‐I Academy. J Sleep Res. 2020;29(4). doi:10.1111/jsr.13052
46. Mason TBA, Pack AI. Pediatric Parasomnias. Sleep. 2007;30(2):141–151. doi:10.1093/sleep/30.2.141
47. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
48. Kater M-J, Schlarb AA. Smartphone usage in adolescents – motives and link to sleep disturbances, stress and sleep reactivity. Somnologie. 2020;24(4):245–252. doi:10.1007/s11818-020-00272-7
49. Schlarb AA, Zschoche M, Schredl M. Der Nightmare Effects Questionnaire (NEQ) [The Nightmare Effects Questionnaire (NEQ)]. Somnologie. 2016;20(4):251–257. doi:10.1007/s11818-016-0086-0
50. Dunne MP, Zolotor AJ, Runyan DK, et al. ISPCAN child abuse screening tools retrospective version (ICAST-R): delphi study and field testing in seven countries. Child Abus Negl. 2009;33(11):815–825. doi:10.1016/j.chiabu.2009.09.005
51. Hardt J, Rutter M. Validity of adult retrospective reports of adverse childhood experiences: review of the evidence. J Child Psychol Psychiatry. 2004;45(2):260–273. doi:10.1111/j.1469-7610.2004.00218.x
52. Kendall-Tackett K, Becker-Blease K. The importance of retrospective findings in child maltreatment research. Child Abuse Negl. 2004;28(7):723–727. doi:10.1016/j.chiabu.2004.02.002
53. Dube SR, Williamson DF, Thompson T, Felitti VJ, Anda RF. Assessing the reliability of retrospective reports of adverse childhood experiences among adult HMO members attending a primary care clinic. Child Abus Negl. 2004;28(7):729–737. doi:10.1016/j.chiabu.2003.08.009
54. Runyan D, Brandspigel S, Zolotor A, Dunne M. Manual for Administration: The ISPCAN Child Abuse Screening Tool (ICAST); 2015.
55. AL Silveira, Grassi-Oliveira DS. Semantic validation of the ISPCAN Child Abuse Screening Tools (ICAST) in Brazilian Portuguese. Trends Psychiatry Psychother. 2016;38(2):105–110. doi:10.1590/2237-6089-2016-0012
56. Chandraratne NK, Fernando AD, Gunawardena N. Cultural adaptation, translation and validation of the ISPCAN Child Abuse Screening Tool – retrospective Version (ICAST-R) for young adults in Sri Lanka. Child Abus Negl. 2018;84:11–22. doi:10.1016/j.chiabu.2018.07.009
57. Zolotor AJ, Runyan DK, Dunne MP, et al. ISPCAN Child Abuse Screening Tool Children’s Version (ICAST-C): instrument development and multi-national pilot testing. Child Abuse Negl. 2009;33(11):833–841. doi:10.1016/j.chiabu.2009.09.004
58. Chiang JJ, Cole SW, Bower JE, et al. Daily interpersonal stress, sleep duration, and gene regulation during late adolescence. Psychoneuroendocrinology. 2019;103:147–155. doi:10.1016/j.psyneuen.2018.11.026
59. Fliege H, Rose M, Arck P, Levenstein S, Klapp BF. Validierung des “Perceived Stress Questionnaire” (PSQ) an einer deutschen Stichprobe [Validation of the Perceived Stress Questionnaire (PSQ) in a German sample]. Diagnostica. 2001;47(3):142–152. doi:10.1026//0012-1924.47.3.142
60. Fliege H, Rose M, Arck P, Levenstein S, Klapp BF. PSQ. Perceived Stress Questionnaire. Leibniz Institute for Psychology Information (ZPID); 2009. doi:10.23668/psycharchives.2889
61. Sandman N, Valli K, Kronholm E, Revonsuo A, Laatikainen T, Paunio T. Nightmares: risk factors among the Finnish general adult population. Sleep. 2015;38(4):507–514. doi:10.5665/sleep.4560
62. Spitzer C, Hammer S, Löwe B, et al. Die Kurzform des Brief Symptom Inventory (BSI −18): erste Befunde zu den psychometrischen Kennwerten der deutschen Version [Short version of the Brief Symptom Inventory (BSI-18): first findings on psychometric properties of the German version]. Fortschritte der Neurol Psychiatr. 2011;79(09):517–523. doi:10.1055/s-0031-1281602
63. Brewster GS, Riegel B, Gehrman PR. Insomnia in the older adult. Sleep Med Clin. 2018;13(1):13–19. doi:10.1016/j.jsmc.2017.09.002
64. Boomsma DI, van Someren EJW, Beem AL, de Geus EJC, Willemsen G. Sleep during a regular week night: a twin-sibling study. Twin Res Hum Genet. 2008;11(5):538–545. doi:10.1375/twin.11.5.538
65. Schredl M, Reinhard I. Gender differences in nightmare frequency: a meta-analysis. Sleep Med Rev. 2011;15(2):115–121. doi:10.1016/j.smrv.2010.06.002
66. Hooper D, Coughlan J, Mullen MR. Structural equation modelling: guidelines for determining model fit. Electron J Bus Res Methods. 2008;6:53–60. doi:10.21427/D7CF7R
67. MacCallum RC, Browne MW, Sugawara HM. Power analysis and determination of sample size for covariance structure modeling. Psychol Methods. 1996;1(2):130–149. doi:10.1037/1082-989X.1.2.130
68. Sethi D. Overview: child maltreatment in the WHO European Region. In: Sethi D, Bellis M, Hughes K, Gilbert R, Mitis F, Galea G, editors. European Report on Preventing Child Maltreatment. WHO Regional Office for Europe; 2013:1–7.
69. Trickett PK, Noll JG, Reiffman A, Putnam FW. Variants of intrafamilial sexual abuse experience: implications for short- and long-term development. Dev Psychopathol. 2001;13(4):1001–1019. doi:10.1017/S0954579401004138
70. Morielli A, Ladan S, Ducharme FM, Brouillette RT. Can Sleep and wakefulness be distinguished in children by cardiorespiratory and videotape recordings? Chest. 1996;109(3):680–687. doi:10.1378/chest.109.3.680
71. Schredl M. Nightmare frequency and nightmare topics in a representative German sample. Eur Arch Psychiatry Clin Neurosci. 2010;260(8):565–570. doi:10.1007/s00406-010-0112-3
72. Gaultney JF. The prevalence of sleep disorders in college students: impact on academic performance. J Am Coll Heal. 2010;59(2):91–97. doi:10.1080/07448481.2010.483708
73. Tsai LL, Li SP. Sleep patterns in college students: gender and grade differences. J Psychosom Res. 2004;56(2):231–237. doi:10.1016/S0022-3999(03)00507-5
74. Schlarb AA, Friedrich A, Claßen M. Sleep problems in university students - An intervention. Neuropsychiatr Dis Treat. 2017;13:1989–2001. doi:10.2147/NDT.S142067
75. Owens H, Christian B, Polivka B. Sleep behaviors in traditional‐age college students. J Am Assoc Nurse Pract. 2017;29(11):695–703. doi:10.1002/2327-6924.12520
76. Tasnim S, Rahman M, Pawar P, et al. Epidemiology of sleep disorders during COVID-19 pandemic: a systematic scoping review protocol. MedRxiv. 2020;2020:1–6.
77. Hossain MM, Tasnim S, Sultana A, et al. Epidemiology of mental health problems in COVID-19: a review. F1000Research. 2020;9:636. doi:10.12688/f1000research.24457.1
78. Manay N, Collin-Vézina D. Recipients of children’s and adolescents’ disclosures of childhood sexual abuse: a systematic review. Child Abuse Negl. 2021;116:104192. doi:10.1016/j.chiabu.2019.104192
79. Krishnan V, Collop NA. Gender differences in sleep disorders. Curr Opin Pulm Med. 2006;12(6):383–389. doi:10.1097/01.mcp.0000245705.69440.6a
80. Jaffe AE, DiLillo D, Hoffman L, Haikalis M, Dykstra RE. Does it hurt to ask? A meta-analysis of participant reactions to trauma research. Clin Psychol Rev. 2015;40:40–56. doi:10.1016/j.cpr.2015.05.004
81. Kim H, Drake B, Jonson-Reid M. An examination of class-based visibility bias in national child maltreatment reporting. Child Youth Serv Rev. 2018;85:165–173. doi:10.1016/j.childyouth.2017.12.019
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.