Back to Journals » Patient Related Outcome Measures » Volume 11
Can Patient Reported Outcomes (PROs) from Population Surveys Provide Accurate Estimates of Pre-Admission Health Status of Emergency Hospital Admissions?
Authors Kwong E ![]() , Abel G
, Abel G ![]() , Black N
, Black N ![]()
Received 13 May 2019
Accepted for publication 13 November 2019
Published 11 February 2020 Volume 2020:11 Pages 39—48
DOI https://doi.org/10.2147/PROM.S215513
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Robert Howland
Esther Kwong,1 Gary Abel,2 Nick Black1
1Department of Health Services Research & Policy, London School of Hygiene and Tropical Medicine, London WC1H 9SH, UK; 2College of Medicine and Health, University of Exeter, Exeter EX4 4PY, UK
Correspondence: Esther Kwong
Department of Health Services Research & Policy, London School of Hygiene and Tropical Medicine 15-17 Tavistock Place, London WC1H 9SH, UK
Tel +44 207 958 8285
Email [email protected]
Introduction: The use of PROs for assessing the outcomes of emergency hospital admissions requires a means of estimating patients’ pre-admission health status. A possible alternative to asking patients to recall how their health was before the incident causing admission is to use estimates derived from matched samples from population surveys. Our aims were to explore the impact of different methods of matching and to compare the results with estimates based on retrospective reporting.
Methods: First, elective hip arthroplasty patients were matched to respondents to the General Practice Patient Survey using age, sex, socio-economic status and number of comorbidities. The impact of restricting matching for locality and specific co-morbidities was explored. Second, the best matching method was applied to emergency admissions for laparotomy and for percutaneous coronary intervention (PCI) after acute myocardial infarction. Data were stratified by patient characteristics. Differences in mean EQ-5D scores between the patients and matched population respondents were tested using t tests.
Results: Modifying the most basic form of matching by also taking locality and the specific comorbid conditions into account made no significant difference to the mean EQ-5D score for hip arthroplasty patients. Even using the most detailed matching possible, patients’ mean EQ-5D score was significantly different to that of the general population for all three cohorts. The difference was greatest for elective hip arthroplasty (0.22 v 0.64), less so for emergency laparotomy (0.56 v 0.72) and least for PCI (0.79 v 0.71). This reflects hip arthroplasty patients having a long-standing condition characterised by pain and limited mobility, whereas the other two cohorts may have enjoyed reasonable health until an unexpected acute episode led to their emergency admission.
Conclusion: Routine PRO data acquired from population surveys cannot be used as an accurate alternative to retrospectively reported PROMs by patients during their emergency admission episode.
Keywords: patient-reported outcome measures, health status, health-related quality of life, self- report, retrospective, hospital admission, general population patient survey
Introduction
Patient-Reported Outcomes (PROs) have the potential to enhance the clinical management of patients and to assess the quality of providers’ performance.1,2 To date, use of PROs in assessing the outcome of hospital admissions has been largely restricted in elective surgery where before and after measurements of patients’ symptoms, functional status and health-related quality of life can be compared. The challenge for use in emergency admissions is how to measure a patient’s health status prior to an unexpected incident that caused an emergency admission.
It is not feasible to collect a pre-admission PRO but the use of retrospective or recalled assessment by patients has been established as a reliable alternative method. Studies of elective admissions have shown that retrospective PRO scores have high agreement with scores collected from patients before admission. Strong associations were found between retrospective and contemporary PROs in 21 out of 30 comparisons (correlation coefficients over 0.68) and 20 of 24 showed strong agreement (intraclass correlations over 0.75). A further study demonstrated the feasibility of using retrospective PROs in the NHS in England. That study found strong agreement between retrospective and contemporary disease-specific PROs and EQ-5D, with intra-class correlation coefficients of 0.8 for the disease-specific PROs (Oxford Hip Score and Oxford Knee Score), and 0.6 for the EQ-5D.3,4
An alternative approach that has been suggested is to derive expected PRO scores from respondents to general population surveys. Nine of the ten studies that have compared retrospective and population PRO scores have been conducted with trauma patients. Seven studies reported that, on average, patients recalled their health status as being better than that derived from age-sex-matched population samples5–11 while three reported no difference.12–14 These findings probably reflect that many trauma cases are from road traffic accidents among relatively healthy young adults. The only study that has considered non-trauma patients (intensive care unit patients with acute lung injury) reported their recalled health status was, on average, worse than that derived from population norms.15
Although the use of population norms has cost advantages, including less patient and staff burden of data collection, there is uncertainty as to whether it would provide a relevant and accurate assessment of pre-admission health status for groups of patients admitted to hospitals. It may be that with more extensive matching techniques, meaningful estimations of baseline health are possible for certain groups of patients, conditions and diseases. It is plausible that the baseline health status of patients admitted with sudden onset unexpected emergencies may have greater similarity with those in the population than is true for trauma admissions.
In this study, we make use of data from the English General Practice Patient Survey (GPPS), which included the EQ-5D instrument between 2011 and 2017 along with basic demographic information and self-reported co-morbidities.16 This rich population-based dataset offers the possibility of matching for several patient characteristics.
Our first aim was to explore the benefits of matching by comparing retrospective self-reported health status (mean EQ-5D scores) of hip arthroplasty patients with that of the general population of England. The second aim was to test the benefits of different matching techniques. The third aim was to test the impact of the optimum matching method by comparing mean differences between population EQ-5D scores and those reported retrospectively by patients admitted for elective hip arthroplasty, emergency laparotomy and acute myocardial infarction.
Methods
Patients who participated in one of three cohort studies (receiving either an elective hip arthroplasty, emergency laparotomy for gastro-intestinal conditions (excluding appendicitis) or emergency percutaneous coronary intervention (PCI) after a myocardial infarction) were matched to GPPS respondents using several patient characteristics. Each patient was matched to as many GPPS respondents as fitted the matching criteria. The mean GPPS EQ-5D score for all those matched to a patient was used to compare with the patient’s retrospectively reported EQ-5D.
Population Sample from GPPS
Data from the 2011–2012 GPPS (held at the University of Exeter) included the EQ-5D-3L, the same version as that used for the patient cohort. Questionnaires were sent in two waves, July 2011 and January 2012, to approximately 1.40 and 1.36 million patients, respectively. Non-responders were mailed a reminder in each of the two months following the initial questionnaire. Of the 2.76 million patients surveyed, 38% responded resulting in a sample of 1,037,946. Patients sent the GPPS comprise a stratified random sample of all adults registered with a general practice. Full details of the survey and its development are published elsewhere.17
Alongside patient experience items, patients were asked to report any long-standing health condition from a list of twelve common conditions: angina or long-term heart problem, arthritis or long-term joint problem, asthma or long-term chest problem, cancer in the last 5 years, deafness or severe hearing impairment, diabetes, epilepsy, high blood pressure, kidney or liver disease, long-term back problem, long-term mental health problem, long-term neurological problem and “another” long-term condition.18 They also reported age (18–24, 25–34, 35–44, 45–54, 55–64, 65–74, 75–84, and 85+ years) and sex. Further, their postcode of residence was used to assign a measure of socio-economic status, the Index of Multiple Deprivation (IMD).
EQ-5D
The EQ-5D-3L is a generic PRO on a three-level ordinal scale (no problems, moderate problems and severe problems) for each of its five dimensions (mobility, self-care, usual activities, pain/discomfort and anxiety/depression).19 UK tariffs of utility were used to obtain an index score which ranges from −0.59 (the worst possible health state) to 1 (indicates best possible health state). The value of 0 is equal to death and negative values represent health states worse than death.20
Patient Cohorts: Hip Arthroplasty, Emergency Laparotomy and PCI
EQ-5D from patients (n= 244) who had undergone hip arthroplasty (primary operation or revision surgery) in one of four NHS hospitals reported their pre-operative health status retrospectively in the immediate post-operative period prior to their discharge from hospital (Health Research Authority ethics approval was obtained from North East - Newcastle & North Tyneside 2 Research Ethics Committee (REC Ref: 16/NE/0081)).4 The mean EQ-5D score of the cohort was similar to that for all patients’ in a national audit in England. Information on comorbidity had previously been collected in a pre-operative questionnaire and covered: heart disease (for example, angina, heart attack or heart failure), high blood pressure, problems caused by a stroke, leg pain due to poor circulation, lung disease, diabetes, kidney disease, liver disease, cancer (within in the last 5 years), diseases of the nervous system (for example, Parkinson’s disease or multiple sclerosis), depression.
Emergency laparotomy patients (n= 261) and PCI patients (n= 396) were recruited from 11 and five NHS hospitals, respectively. Patients completed a retrospective questionnaire in the immediate period prior to their discharge from hospital following their emergency admission. The study received ethics approval from South East Coast - Brighton & Sussex Research Ethics Committee (REC reference: 16/LO/2053).21 The questionnaire included the same question about comorbidity as used for the hip arthroplasty study.
Matching Patients to Population Sample
Patients were matched to GPPS population on sex, age, socioeconomic status and number of co-morbidities. The sample sizes were large enough, relative to the number of matching characteristics, to permit exact one-to-many matching. Age was categorised: 18–24, 25–34, 35–44, 45–54, 55–64, 65–74, 75–84, and 85+ years. Socioeconomic status (SES) was derived from the Index of Multiple Deprivation (IMD) of a patient’s local area (LSOAs) based on postcode, which was then grouped into quintiles based on the national ranking of areas by IMD to match the GPPS variable.22 Co-morbid conditions reported in the patient cohorts were mapped to the categories collected in the GPPS (Table 1).
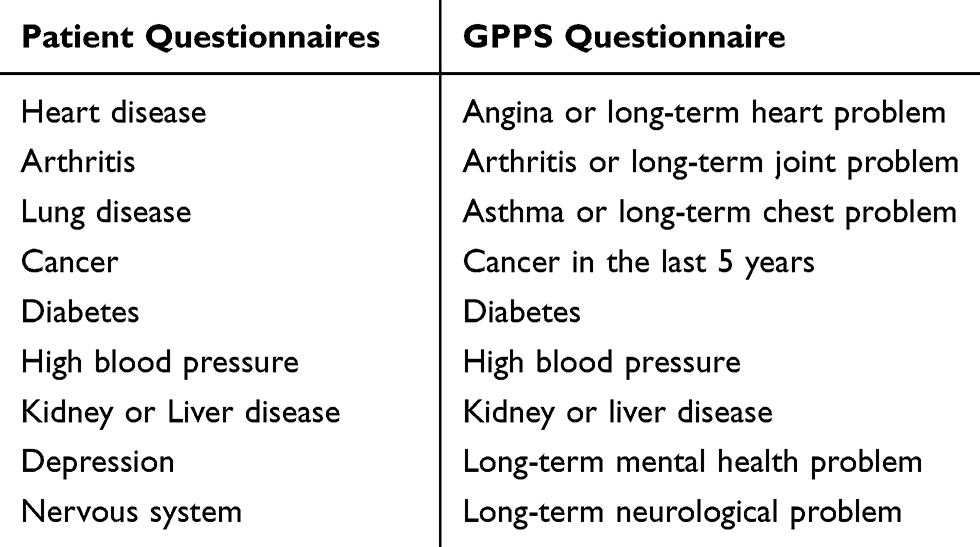 |
Table 1 Co-Morbidities Reported in Patient and in the GPPS Questionnaires |
Patients were matched to GPPS using personal characteristics available in both datasets. One-to-many matching was conducted, with one patient matched to as many GPPS respondents as fitted the matching criteria. The mean EQ-5D score of all GPPS respondents matched to a patient was used in the comparison between patients’ reported EQ-5D and GPPS EQ-5D. Mean EQ-5D scores for patients and for the population were compared.
First, exploratory matching was conducted with hip arthroplasty patients to determine whether the specific way of matching would change the differences between population and patients’ mean EQ-5D scores. Matching for age, sex, SES and number of comorbidities was compared with (i) restricting matching to GPPS respondents living in the same local authority and (ii) matching patients on the basis of specific combinations of co-morbidities. Data were stratified by patient characteristics and t tests were carried out to compare differences between patients’ EQ-5D means and population EQ-5D means by patient characteristics. As is customary, a p value of less than 0.05 was deemed statistically significant.
Second, influenced by the findings of the first phase, analysis of the emergency laparotomy and PCI patients was conducted. Similarly, data were stratified by patient characteristics and t tests were carried out to compare differences between patients’ EQ-5D means and population EQ-5D means by patient characteristics.
Despite the left skew of the EQ-5D data, we opted to use the paired t-test for comparisons between the three patient groups and population for three reasons. First, it enabled preservation of consistency in our comparisons between all the comparators. Second, the sample sizes satisfied guidelines for using parametric comparisons. And third, the t-test does not require the assumption of equal dispersion (equal variance) in the data when comparing between groups.
Results
Comparison of Matching Methods with Hip Arthroplasty Patients
Of 244 hip arthroplasty patients (80 men with mean age of 66 (range 35–90); 160 women with a mean age of 69 (range 29–90)). 25 were excluded because of missing data: 4 incomplete EQ-5D; 20 missing co-morbidities; one missing data on SES. Analyses were conducted with three different matching strategies:
Matched for Age, Sex, SES and Number of Comorbidities
The median number of matches per patient was 2434 (range 0–8052) though three patients could not be matched. The difference in EQ-5D scores between patients and the population was large (between 0.26 and 0.40) across all categories of patient characteristics.
Matched for Age, Sex, SES, Number of Comorbidities and Local Authority
The median number of matches per patient was 241 (range 0–1305); 17 patients could not be matched. The difference in mean EQ-5D between patients and the population was the same when matching was restricted to the same local authority and remained highly statistically significant (p<0.001) (Figure 1). Differences still ranged from 0.21–0.35 for different age, sex and SES categories (not shown).
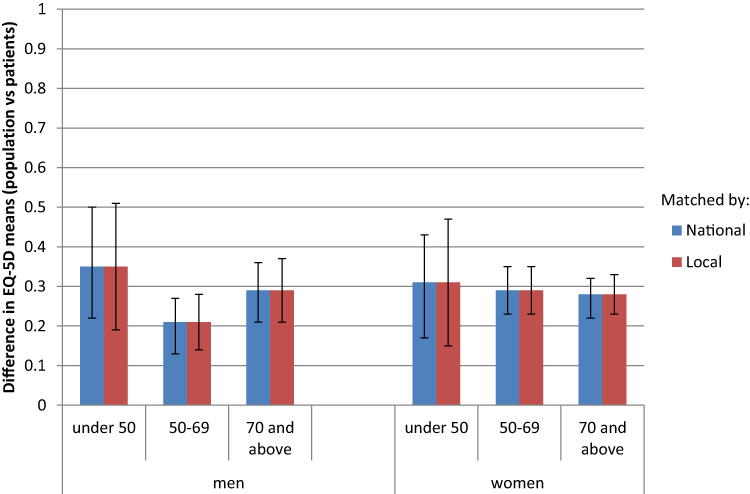 |
Figure 1 Impact of matching by local authority: comparison of difference in mean EQ-5D between hip arthroplasty patients and population reports (by age and sex). |
Matched for Age, Sex, SES and Specific Comorbidities
The median number of matches per patient was 336 (range 0–9832); seven patients could not be matched. The matched population mean EQ-5D was 0.64 (SD 0.23) which was significantly higher than the patients’ mean of 0.22 (SD 0.35); difference 0.42 (CI 0.39–0.44; p<0.001) (Table 2). Matching for specific comorbidities did not change the extent of the differences between population and patients' EQ-5D scores overall compared with matching by number of co-morbidities (Figure 2). The difference for age and sex sub-groups ranged from 0.21–0.35 using specific comorbidities compared with 0.26–0.40 using the number of conditions.
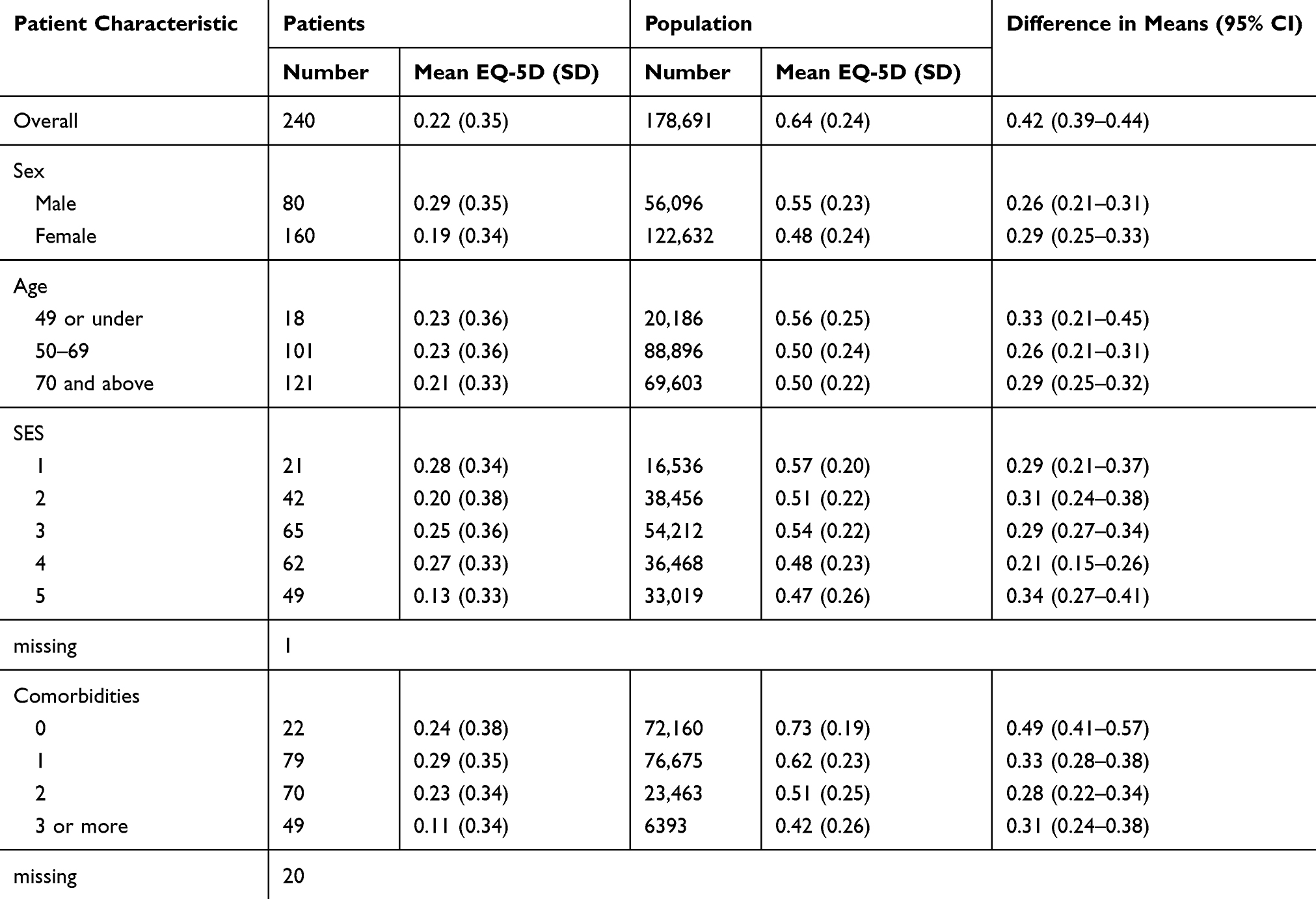 |
Table 2 Comparison of Mean EQ-5D (95% CI) of Hip Arthroplasty Patients and Population (Matched for Age, Sex, SES, and Specific Comorbidities) |
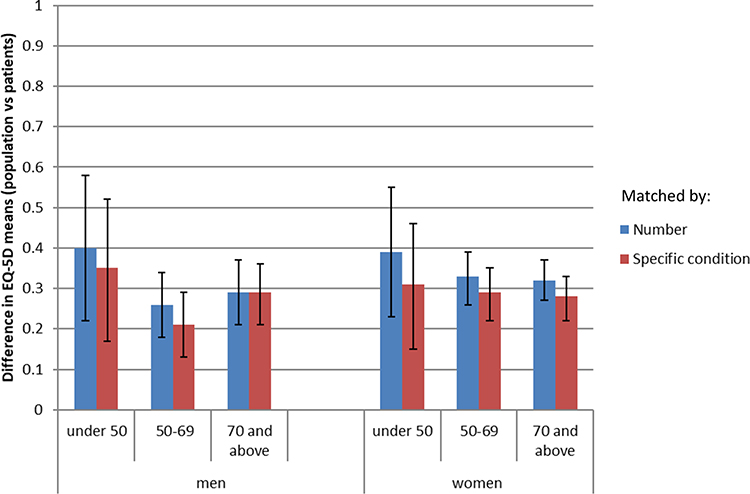 |
Figure 2 Impact of matching by specific comorbid condition: comparison of difference in mean EQ-5D between hip arthroplasty patients and population reports (by age and sex). |
Comparisons of Patients’ and Population EQ-5D for Three Patient Groups
Of 261 emergency laparotomy patients (121 men with mean age of 61 (range 18–90); 131 women with a mean age of 62 (range 21–91)). Nine were missing a complete baseline EQ-5D score, 19 were missing SES and four were missing co-morbidities. The median number of matches was 250 (range 0–11,421); five patients could not be matched. Of 396 PCI patients (305 men with mean age of 61 (range 27–92); 85 women with a mean age of 66 (range 44–94)). Six were missing a complete baseline EQ-5D score, 23 were missing SES, and one was missing comorbidities. The median number of matches 139 (range 0–11,541); six could not be matched.
The significant difference between hip arthroplasty patients’ mean EQ-5D and that of a matched population already reported (0.42; CI 0.39–0.44) (Table 2) was also observed for emergency laparotomy patients, although the size of the difference was smaller (0.13; CI 0.10–0.15, p<0.001) (Table 3). While the difference for PCI patients was also statistically significant, the direction of difference was reversed with the patients reporting better health than the matched population (−0.09; Cl −0.12 to −0.07, p<0.001) (Table 4).
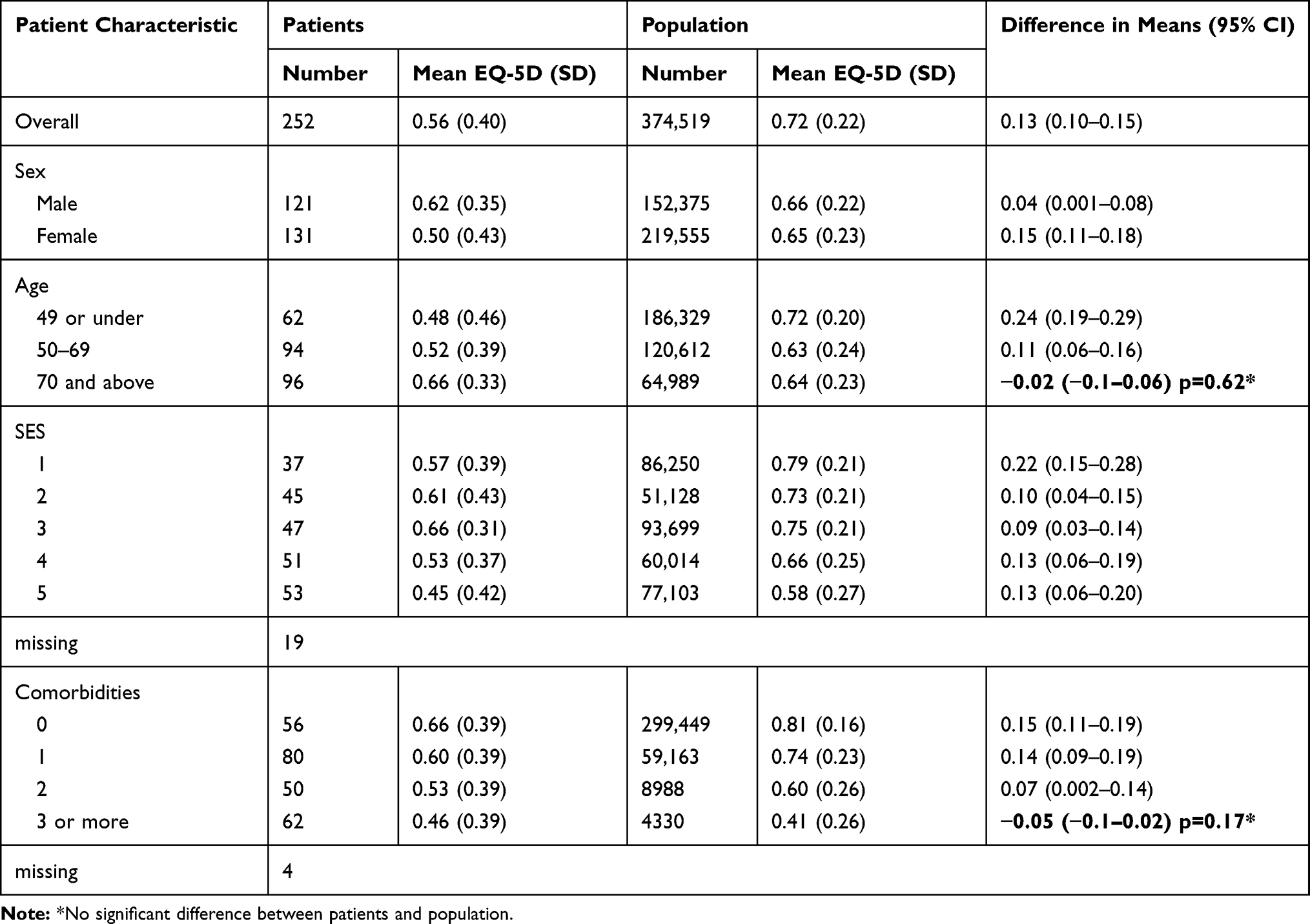 |
Table 3 Comparison of Mean EQ-5D (95% CI) of Emergency Laparotomy Patients and Population (Matched for Age, Sex, SES, Local Authority and Specific Comorbidities) |
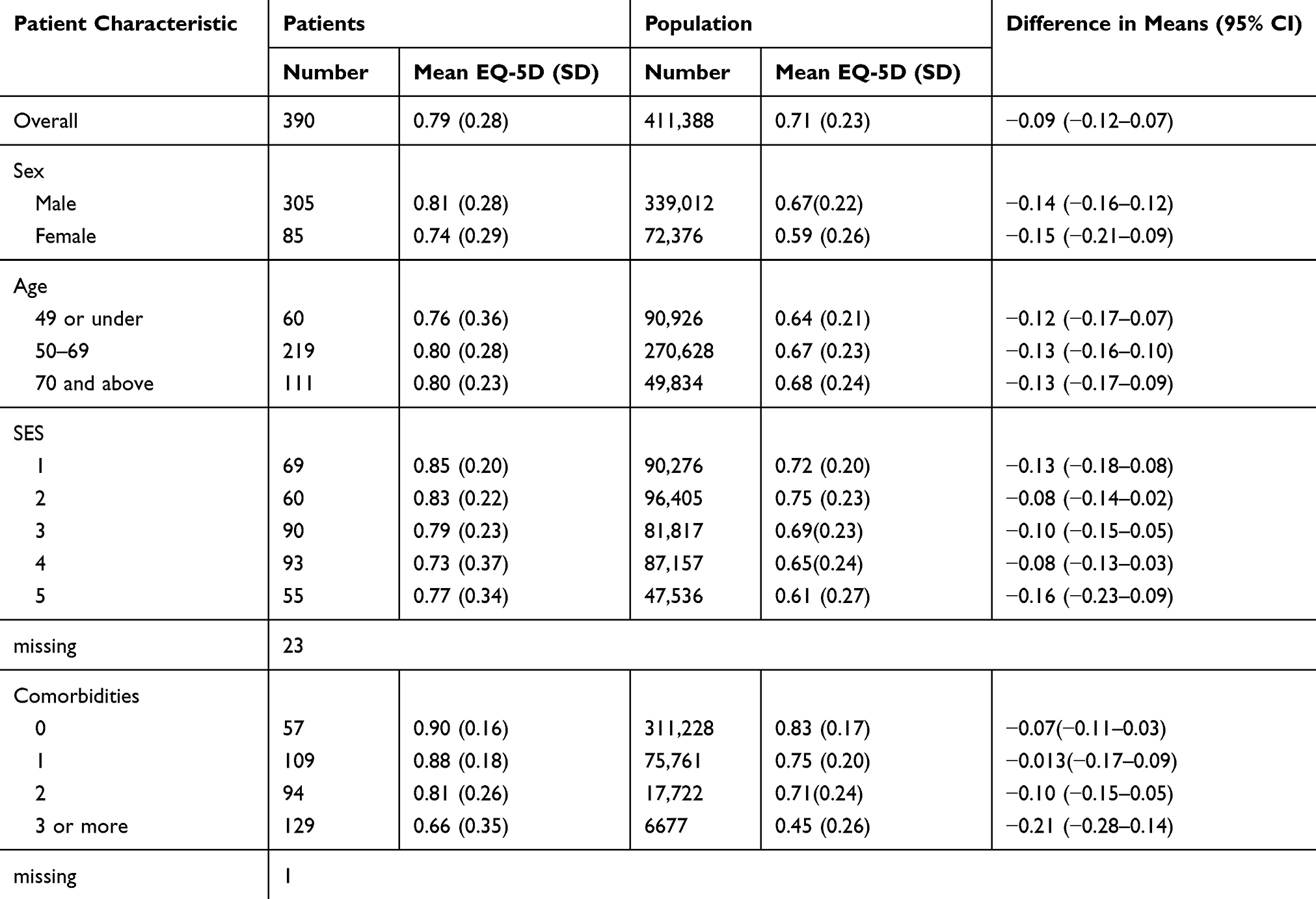 |
Table 4 Comparison of Mean EQ-5D (95% CI) of PCI Patients and Population (Matched for Age, Sex, SES, Local Authority and Specific Comorbidities) |
When stratified by patient characteristics, the mean differences of patients’ EQ-5D from that of their matched populations were significantly different across nearly all stratified groups for all three patient groups. With the exception of PCI patients, patients’ reported a lower baseline EQ-5D than that for the matched population. The only categories for which there was no significant difference were for emergency laparotomy patients over 70 years of age, and with 3+ co-morbidities (Table 3).
Discussion
Main Findings
Modifying the most basic form of matching (using the whole population adjusted for sex, age, SES and number of comorbidities) by also taking locality and the specific comorbid conditions into account made no substantial difference to the estimated EQ-5D mean score. Given the larger sample available when using national data, matching using the whole population is the preferred option.
Despite the use of specific comorbidities conferring no benefit over a simple count from the exploratory matching with hip patients, the former was chosen for comparing differences between patients and the population as co-morbidity has been shown to influence the health status of respondents in the GPPS in prior published research.23
Patients’ mean EQ-5D score was significantly different than that of the general population for all three cohorts. The difference was greatest for elective hip arthroplasty patients (0.22 v 0.64), less for emergency laparotomy (0.56 v 0.72) and least for PCI (0.79 v 0.71) in whom the direction of difference was reversed with patients reporting higher baseline EQ-5D than the population. This corresponds to the clinical context in which hip arthroplasty patients have a long-standing condition characterised by pain and limited mobility, whereas the other two cohorts of emergency patients may have enjoyed reasonable health until an unexpected acute episode led to their emergency admission. This is particularly true for the PCI patients, many of whom had no prior symptoms making it plausible they had better health status than those in the matched population of respondents to the GPPS. The only sub-groups in whom their self-reported EQ-5D did not differ significantly from that of the matched population were those emergency laparotomy patients who were least healthy (aged over 70 years, and with two or more comorbidities).
Our findings differ from most published studies which have reported general populations being healthier than patients.5–7,9–11 This reflects that most of those studies were limited to trauma patients rather than patients with long-term illnesses or conditions.5–7,9–14 The one exception was a study of medical inpatients which reported similar findings to our study.15 Thus, our findings are consistent with the suggestions by other authors that the acute injury population may be healthier, whereas patients with medical and surgical needs are less healthy compared to the general population.
These findings confirm that routine PRO data acquired from population surveys cannot be used as an accurate alternative to retrospectively reported PROs by medical and surgical patients during their emergency admission episode.
Strengths and Limitations
There are three limitations to consider. First, the validity of the GPPS data. Although it is a large national survey, the response rate in 2011–2012 was only 38%, albeit similar to that achieved in other surveys using a similar methodology.17 In addition, co-morbidity data were missing for 13% and EQ-5D scores were incomplete for 20%.23 Responders are more likely to be women, middle-aged and those in affluent areas, factors that will influence the mean EQ-5D score. However, given that in this study the data were matched for sex, age and SES, any response bias will be limited to any other characteristics such as ethnic group or educational attainment or indeed health status itself.24 Although it is not possible to estimate the impact of bias due to these variables, published meta-analyses on probability sampled surveys suggest that response rates are not a strong predictor for response bias.25
Second, comorbidity data in both the retrospective patient cohorts and the GPPS are based on respondents’ reports. In both samples, it is possible that respondents might under or over-report conditions. However, previous studies suggest that the incidence of comorbidities reported by patients is similar to that from medical records except for diabetes, high blood pressure and long-term back problems.23
Finally, the stratified analysis used may not have been adequate to control for confounding as EQ-5D is age-dependent; however, cross tabulation of stratified age (ten-year bands) of EQ-5D scores revealed no significant associations with sex or SES.
Implications for Policy
These exploratory findings show that use of the GPPS is not suitable for use in place of a retrospective PRO in three particular patient groups. Population and groups of patients remain significantly different even with specific matching and only in certain sub-segments of the population were they similar. It would, therefore, not be appropriate to assess the outcome of care for those admitted as emergencies by comparing their PRO scores with that derived from the general population. In the situation of hip arthroplasty and EL patients, given that before their admission the health status of these patients is, on average, significantly worse than their matched peers in the population, it is not reasonable to expect that they will attain the mean level of health status of the population. To assume that may suggest that the care they receive both during their emergency admission and subsequently in the community is sub-optimal. The reverse is true of PCI patients. Thus the use of PROs in emergency admissions needs to incorporate retrospectively collected PROs. The challenge is how this can be done routinely in a cost-effective way.
Ethical Approval and Informed Consent
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and national research committee (NHS Health Research Authority) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. NHS ethical approval obtained from Health Research Authority North East - Newcastle & North Tyneside 2 Research Ethics Committee (REC Ref: 16/NE/0081) and South East Coast - Brighton & Sussex Research Ethics Committee (REC reference: 16/LO/2053). Written Informed consent was obtained from all individual participants included in the study. Only anonymised large GPPS population means data were used.
Acknowledgments
We thank the patients and staff of the 20 hospitals that participated in the three patient cohort studies, the Site and Study leads.
Site and study leads collaborators: Mike Grocott, David Murray, David Saunders, Jose Lourtie, Steffen Petersen, Fares Haddad, Mahbub Alam, Rej Bumbra, Joyti Saksena, Jamila Kassam, Ursula Knight, Mark Vertue, Joanne Riches, Julie Saunders, Mervyn Andiapen, Jonathan Breeze, Amy Hoare, Alison Pottle, Paula Rogers, Claire Prendergast, Michael Lewis, Gill Pout, Patricia Dickens, James Kirkby-bott, Pauline Bartlett, Guy Titley, Emma Willett, Nina Barratt, Tanuja Shah, Kathleen Holding, Lianne Hufton, Veeranna Shatkar, Ruwan Weerakkody, Caron Baldwin, Sarah Hare, Annette Woods, Ewen Griffiths, Arlo Whitehouse, Jugdeep Dhesi, Jane Okello, Philip Braude, Karen Wilson, Kirsty Gibson, Abdul Quddus, Davina Ross-Anderson, Katherine MacGloin, Hasan Mukhtar, Kathryn Simpson, Kayleigh Gilbert, Mark Vertue, Joanne Riches, Julie Saunders, Mervyn Andiapen, Jonathan Breeze, Amy Hoare, Alison Pottle, Paula Rogers, Claire Prendergast, Michael Lewis, Gill Pout, Patricia Dickens, James Kirkby-bott, Pauline Bartlett, Guy Titley, Emma Willett, Nina Barratt, Tanuja Shah, Kathleen Holding, Lianne Hufton.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
EK is funded by Economic & Social Research Council doctoral fellowship. Grant Reference: ES/J500021/1.
The research was supported by the National Institute for Health Research (NIHR) Collaboration for Leadership in Applied Health Research and Care North Thames at Barts Health NHS Trust. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Black N. Patient reported outcome measures could help transform healthcare. BMJ. 2013;346:19–21. doi:10.1136/bmj.f167
2. Greenhalgh J, Dalkin S, Gooding K, et al. Functionality and feedback: a realist synthesis of the collation, interpretation and utilisation of patient-reported outcome measures data to improve patient care. Health Serv Deliv Res. 2017;5(2):1–280.
3. Kwong E, Black N. Retrospectively collected patient reported outcomes show strong association and agreement with their contemporaneous reports. J Clin Epidemiol. 2017;81:22–32. doi:10.1016/j.jclinepi.2016.09.002
4. Kwong E, Neuburger J, Black N. Agreement between retrospectively and contemporaneously collected patient-reported outcome measures (PROMs) in hip and knee replacement patients. Qual Life Res. 2018;27:1845–1854. doi:10.1007/s11136-018-1823-6
5. Ameratunga SN, Norton RN, Connor JL, et al. A population-based cohort study of longer-term changes in health of car drivers involved in serious crashes. Ann Emerg Med. 2006;48(6):729–736. doi:10.1016/j.annemergmed.2006.07.001
6. Gabbe BJ, Cameron PA, Graves SE, Williamson OD, Edwards ER. Preinjury status: are orthopaedic trauma patients different than the general population? J Orthop Trauma. 2007;21(4):223–228. doi:10.1097/BOT.0b013e31803eb13c
7. Watson WL, Ozanne-Smith J, Richardson J. Retrospective baseline measurement of self-reported health status and health-related quality of life versus population norms in the evaluation of post-injury losses. Inj Prev. 2007;13(1):45–50. doi:10.1136/ip.2005.010157
8. Lange RT, Iverson GL, Rose A. Post-concussion symptom reporting and the “good-old-days” bias following mild traumatic brain injury. Arch Clin Neuropsychol. 2010;25(5):442–450. doi:10.1093/arclin/acq031
9. Lyons RA, Kendrick D, Towner EM, et al. Measuring the population burden of injuries–implications for global and national estimates: a multi-centre prospective UK longitudinal study. PLoS Med. 2011;8(12):e1001140. doi:10.1371/journal.pmed.1001140
10. Tøien K, Bredal IS, Skogstad L, Myhren H, Ekeberg O. Health related quality of life in trauma patients. Data from a one-year follow up study compared with the general population. Scand J Trauma Resusc Emerg Med. 2011;19(1):22. doi:10.1186/1757-7241-19-22
11. Wilson R, Derrett S, Hansen P, Langley J. Retrospective evaluation versus population norms for the measurement of baseline health status. Health Qual Life Outcomes. 2012;10(1):68. doi:10.1186/1477-7525-10-68
12. Mock C, MacKenzie E, Jurkovich G, et al. Determinants of disability after lower extremity fracture. J Trauma. 2000;49(6):1002–1011. doi:10.1097/00005373-200012000-00005
13. Michaels AJ, Madey SM, Krieg JC, Long WB. Traditional injury scoring underestimates the relative consequences of orthopedic injury. J Trauma. 2001;50(3):
14. Tidermark J, Zethraeus N, Svensson O, Törnkvist H, Ponzer S. Femoral neck fractures in the elderly: functional outcome and quality of life according to EuroQol. Qual Life Res. 2002;11(5):473–481. doi:10.1023/A:1015632114068
15. Gifford J, Husain N, Dinglas V, Colantuoni E, Needham DM. Baseline quality of life before intensive care: a comparison of patient versus proxy responses. Crit Care Med. 2010;38(3):855–860. doi:10.1097/CCM.0b013e3181cd10c7.Baseline
16. NHS England. GP patient survey. 2017. Available from: https://www.england.nhs.uk/statistics/2017/07/06/gp-patient-survey-2017/.
17. Campbell J, Smith P, Nissen S, Bower P, Elliott M, Roland M. The GP patient survey for use in primary care in the National Health Service in the UK – development and psychometric characteristics. BMC Fam Pract. 2009;10(1):57. doi:10.1186/1471-2296-10-57
18. NHS England. GPPS surveys and reports; 2017. Available from: www.gpatient.co.uk/download/Questionnaires/.
19. EuroQol Group. EuroQol – a new facility for the measurement of health-related quality of life. Health Policy (New York). 1990;16:199–208. doi:10.1016/0168-8510(90)90421-9
20. Dolan P, Roberts J. Modelling valuations for Eq-5d health states: an alternative model using differences in valuations. Med Care. 2002;40:442–446. doi:10.1097/00005650-200205000-00009
21. Kwong E, Black N. Feasibility of collecting retrospective patient reported outcome measures (PROMs) in emergency hospital admissions. J Patient Rep Outcomes. 2018;2(1):54. doi:10.1186/s41687-018-0077-y
22. Department for Communities and Local Government. English Indices of Deprivation. Crown Copyright; 2015.
23. Mujica-Mota RE, Roberts M, Abel G, et al. Common patterns of morbidity and multi-morbidity and their impact on health-related quality of life: evidence from a national survey. Qual Life Res. 2015;24(4):909–918. doi:10.1007/s11136-014-0820-7
24. Burt J, Lloyd C, Campbell J, Roland M, Abel G. Variations in GP–patient communication by ethnicity, age, and gender: evidence from a national primary care patient survey. Br J Gen Pract. 2016;66(642):e47–e52. doi:10.3399/bjgp15X687637
25. Groves RM, Peytcheva E. The impact of nonresponse rates on nonresponse bias: a meta-analysis. Public Opin Q. 2008;72(2):167–189. doi:10.1093/poq/nfn011
 © 2020 The Author(s). This work is published by Dove Medical Press Limited, and licensed under a
Creative Commons Attribution License.
The full terms of the License are available at http://creativecommons.org/licenses/by/4.0/.
The license permits unrestricted use, distribution, and reproduction in any medium, provided the
original author and source are credited.
© 2020 The Author(s). This work is published by Dove Medical Press Limited, and licensed under a
Creative Commons Attribution License.
The full terms of the License are available at http://creativecommons.org/licenses/by/4.0/.
The license permits unrestricted use, distribution, and reproduction in any medium, provided the
original author and source are credited.