Back to Journals » Journal of Hepatocellular Carcinoma » Volume 7
Can Immediately Treating Subcentimeter Hepatocellular Carcinoma Improve the Survival of Patients?
Authors Sun X, Hu D, Zhang Y ![]() , Lyu N
, Lyu N ![]() , Xu L
, Xu L ![]() , Chen Q, Lai J, Chen M, Zhao M
, Chen Q, Lai J, Chen M, Zhao M ![]()
Received 24 October 2020
Accepted for publication 3 December 2020
Published 16 December 2020 Volume 2020:7 Pages 377—384
DOI https://doi.org/10.2147/JHC.S287641
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Ahmed Kaseb
Xuqi Sun,1– 3 Dandan Hu,1,2 Yaojun Zhang,1,2 Ning Lyu,1,4 Li Xu,1,2 Qifeng Chen,1,4 Jinfa Lai,1,4 Minshan Chen,1,2 Ming Zhao1,4
1State Key Laboratory of Oncology in South China, Collaborative Innovation Center for Cancer Medicine, Sun Yat-Sen University Cancer Center, Guangzhou 510060, People’s Republic of China; 2Department of Liver Surgery, Sun Yat-Sen University Cancer Center, Guangzhou 510060, People’s Republic of China; 3Zhongshan School of Medicine, Sun Yat-Sen University, Guangzhou 510060, People’s Republic of China; 4Minimally Invasive Interventional Division, Liver Cancer Group, Sun Yat-Sen University Cancer Center, Guangzhou 510060, People’s Republic of China
Correspondence: Ming Zhao
Minimally Invasive Interventional Division, Liver Cancer Group, Sun Yat-Sen University Cancer Center, Guangzhou 510060, People’s Republic of China
Tel/Fax +86-20-87343272
Email [email protected]
Background: With the development of imaging technology, an increasing number of subcentimeter hepatocellular carcinoma (HCC) has been detected. How to manage these lesions remains controversial and lacks evidence. We aimed to explore whether timely treating subcentimeter HCC is necessary considering the risks of false-positives and treatment failure.
Methods: In this retrospective study, we reviewed HCC patients treated with hepatectomy or ablation in our institution. Then, we enrolled 439 HCC patients with solitary lesion measuring up to 2 cm from November 1, 2009 to June 30, 2019. The baseline and clinical characteristics of these patients were collected. The patients were classified into primary and recurrent groups. The Kaplan–Meier method with Log-rank test was performed to compare the overall survival (OS) and recurrence-free survival (RFS) between patients with subcentimeter HCC and those with HCC measuring 1– 2 cm. Univariate and multivariate analyses were adopted to identify prognostic factors for survival.
Results: The OS and RFS did not differ significantly between patients with subcentimeter HCC and those with HCC measuring 1– 2 cm in the primary group (p = 0.12 and 0.75). Similar results were found in the recurrent group. In multivariate analysis, the albumin-bilirubin (ALBI) grade and serum alpha fetoprotein (AFP) level were significantly associated with OS and RFS in the primary group. The serum AFP level was the only factor that correlated with OS and RFS in the recurrent group.
Conclusion: Routine screening for subcentimeter HCC is feasible. Considering uncertain diagnosis and treatment difficulties, it is more considerable to follow patients until lesions are larger than 1 cm and then provide curative treatments.
Keywords: carcinoma, hepatocellular, subcentimeter, disease management, survival
Introduction
Hepatocellular carcinoma (HCC) is the most common liver malignancy and ranks as the fourth leading cause of cancer-related mortality.1 Curative treatments can achieve a five-year survival rate of approximately 80% in patients with solitary HCC measuring up to 2 cm.2 This promising survival rates motivates wide surveillance programs for the population at risk for HCC.3 The introduction of magnetic resonance imaging (MRI) contrast agent gadoxetic acid increase the detection rate of small HCCs.4 Consequently, the proportion of newly diagnosed early-stage HCC has been increasing in recent years.5 Among these early lesions, how to manage subcentimeter hepatic nodules remains controversial.
Although multiphasic contrast-enhanced MRI and computed tomography (CT) can accurately diagnose HCC, their diagnostic performance is unsatisfactory for subcentimeter lesions; even with gadoxetic acid-enhanced MRI, the positive predictive value is only 48.3%.6–9 The diagnostic value of biopsy is also limited, with a false-negative rate of more than 30% due to sampling errors.10 Considering this diagnostic dilemma, both the American Association for the Study of Liver Diseases (AASLD) and the European Association for the Study of the Liver (EASL) propose routine screening for subcentimeter lesions.10,11 In contrast, the Japan Society of Hepatology (JSH) recommends imaging diagnosis for hypervascular subcentimeter hepatic lesions with washout in delayed phases and proposes hepatectomy or percutaneous ablation for these nodules.12 However, all of the aforementioned recommendations lack evidence.
In addition to primary subcentimeter lesions, these small nodules are more commonly detected with contrast-enhanced MRI or CT during the follow-up of HCC patients after curative treatments.13,14 Ablation is more suitable than resection for recurrent HCC due to the insufficient remnant liver and progressive hepatic dysfunction.15,16 Unfortunately, subcentimeter hepatic nodules are hard to visualize with ultrasound or CT, which limits the application of ablation.14,17 It is worth considering whether risking treatment failure to treat subcentimeter HCCs in a timely manner is necessary.
In this study, we aimed to compare the survival of patients with primary or recurrent subcentimeter HCCs and those with corresponding HCCs measuring 1–2 cm after curative treatments and to elucidate the optimal management for subcentimeter hepatic lesions.
Patients and Methods
Patients
We reviewed HCC patients treated with hepatectomy or ablation in Sun Yat-sen University Cancer Center from November 1, 2009 to June 30, 2019. A total of 7267 patients were enrolled. Patients were excluded according to the following criteria: 1) having HCC larger than 2 cm (n = 6109); 2) with multiple HCCs (n = 606); and 3) diagnosed with benign lesions, cholangiocarcinoma or combined hepatocellular-cholangiocarcinoma, or liver metastasis from other malignancies (n = 113). Eventually, we identified 45 solitary subcentimeter lesions and 394 solitary lesions measuring 1–2 cm in this study. All the hepatic nodules showed typical hypervascularity in the arterial phase and washout in the portal or delayed phases on MRI. The research flow chart is presented in Figure 1 in detail. Patients’ baseline and clinical characteristics were collected including gender, age at diagnosis, virus infection, albumin-bilirubin (ALBI) grade, alpha fetoprotein (AFP) level, cirrhosis, tumor size and treatment modalities. This study was performed in compliance with the ethical standards of the 1964 Helsinki declaration and was approved by the institutional review board of Sun Yat-sen University Cancer Center (approval number: B2020-104-01).
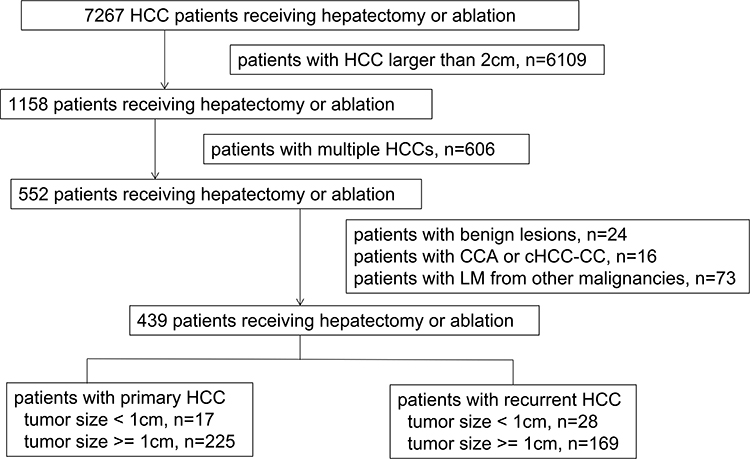 |
Figure 1 The flowchart of patients included in this study. |
Statistical Analyses
The oncological outcomes were compared between patients with subcentimeter HCC and those with HCC measuring 1–2 cm in the primary and recurrent groups, respectively. Chi-square or Fisher’s exact tests were adopted to compare baseline categorical variables. Two-sample independent t-tests were performed to compare continuous variables with a normal distribution. The Kaplan–Meier (K-M) method with Log rank test was adopted to compare overall survival (OS) and recurrence-free survival (RFS) between patients with subcentimeter HCC and those with HCC measuring 1–2 cm. The OS was measured from the date of curative treatments to the date of death or last follow-up. The RFS was defined as the period from the date of curative treatments to the date of recurrence or last follow-up. Univariate and multivariate Cox regression models were adopted to identify significant factors for the OS and RFS. A two-tailed P value of less than 0.05 was considered statistically significant.
Results
Characteristics of Patients with Subcentimeter HCC and Those with HCC Measuring 1–2 Cm
The entire cohort consisted of 242 patients with primary HCC (17 with subcentimeter HCC and 225 with HCC measuring 1–2 cm) and 197 patients with recurrent HCC (28 with subcentimeter HCC and 169 with HCC measuring 1–2 cm). No significant difference was found in gender, age at diagnosis, virus infection, ALBI grade, serum AFP level or cirrhosis between patients with subcentimeter HCC and those with HCC measuring 1–2 cm in both the primary and recurrent groups. The mean diameters of the subcentimeter HCC were 7.47 mm and 7.68 mm in the primary and recurrent groups, respectively. The mean diameter of the 1–2 cm HCCs was slightly smaller in the recurrent group than in the primary group. In the primary group, patients with subcentimeter HCC were more likely to undergo hepatectomy than those with HCC measuring 1–2 cm (p = 0.044). No significant difference was found in treatment modalities between patients with subcentimeter HCC and those with HCC measuring 1–2 cm. The detailed data are listed in Table 1. Supplementary Figure 1 shows the MRI and pathological images of an 8.6-mm HCC.
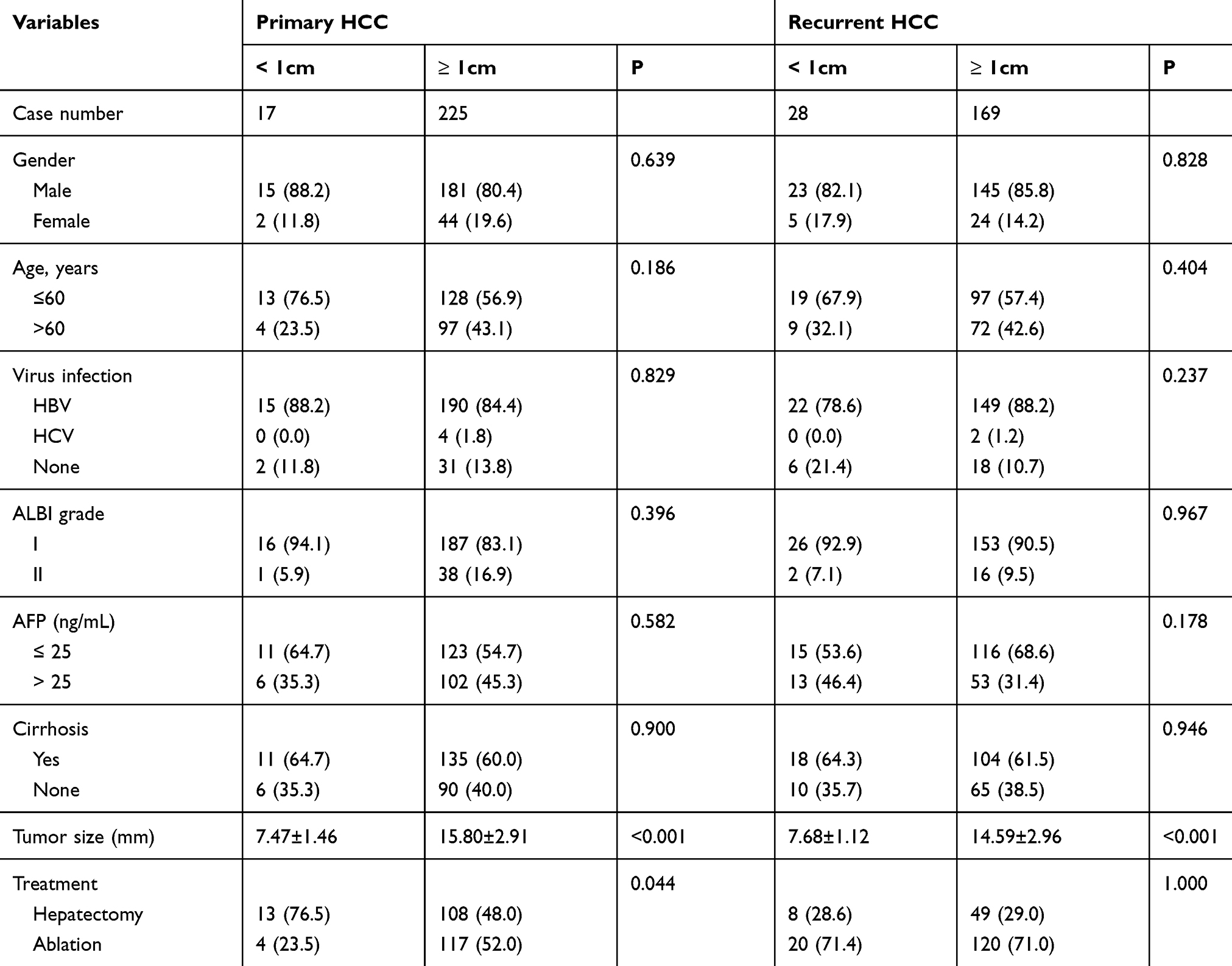 |
Table 1 Baseline Characteristics of Patients with Subcentimeter HCC and HCC Measuring 1–2 Cm |
Survival Outcomes
The median follow-up was 24.37 months. At the end of the study, 85 (35.1%) and 85 (43.1%) patients suffered from relapse in the primary and recurrent groups, respectively. The median RFS times were 14.27 months and 12.90 months in the primary and recurrent groups, respectively. The 1- and 2-year RFS rates were 73.3% and 66.7% in the primary group and 75.4% and 66.5% in the recurrent group, respectively. For the whole cohort, no significant difference was found in RFS or OS between patients with subcentimeter HCC and those with HCC measuring 1–2 cm (p = 0.51 and 0.08). The survival curves are shown in Figure 2A and D. For patients with primary HCC, the RFS and OS of patients with subcentimeter HCC did not significantly differ from those of patients with HCC measuring 1–2 cm (p = 0.75 and 0.12) (Figure 2B and E). Similar results were found in the recurrent group (p = 0.98 and 0.34) (Figure 2C and F).
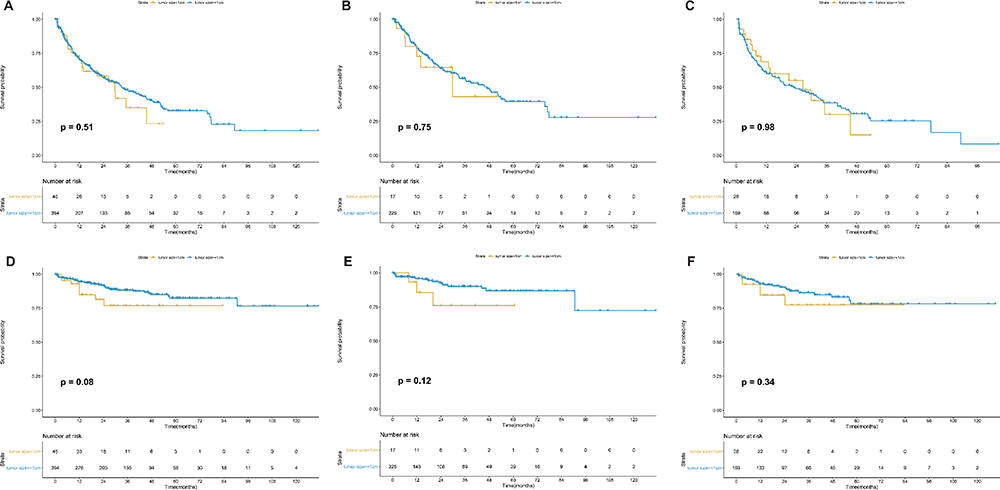 |
Figure 2 The survival curves of patients with subcentimeter HCC and those with HCC measuring 1–2 cm. There was no significant different in the recurrence-free survival (RFS) (A) or overall survival (OS) (D) between patients with subcentimeter HCC and those with HCC measuring 1–2 cm for the whole cohort (p = 0.51 and 0.08). In the primary group, the RFS (B) and OS (E) were similar between patients with subcentimeter HCC and those with HCC measuring 1–2 cm (p = 0.75 and 0.12). Similar tendency was found in the recurrent group for the RFS (C) and OS (F) (p = 0.98 and 0.34). |
In univariate analyses, the ALBI grade and serum AFP level were significantly associated with OS and RFS in the primary group. However, only the serum AFP level correlated with OS and RFS in the recurrent group. Detailed data are shown in Table 2.
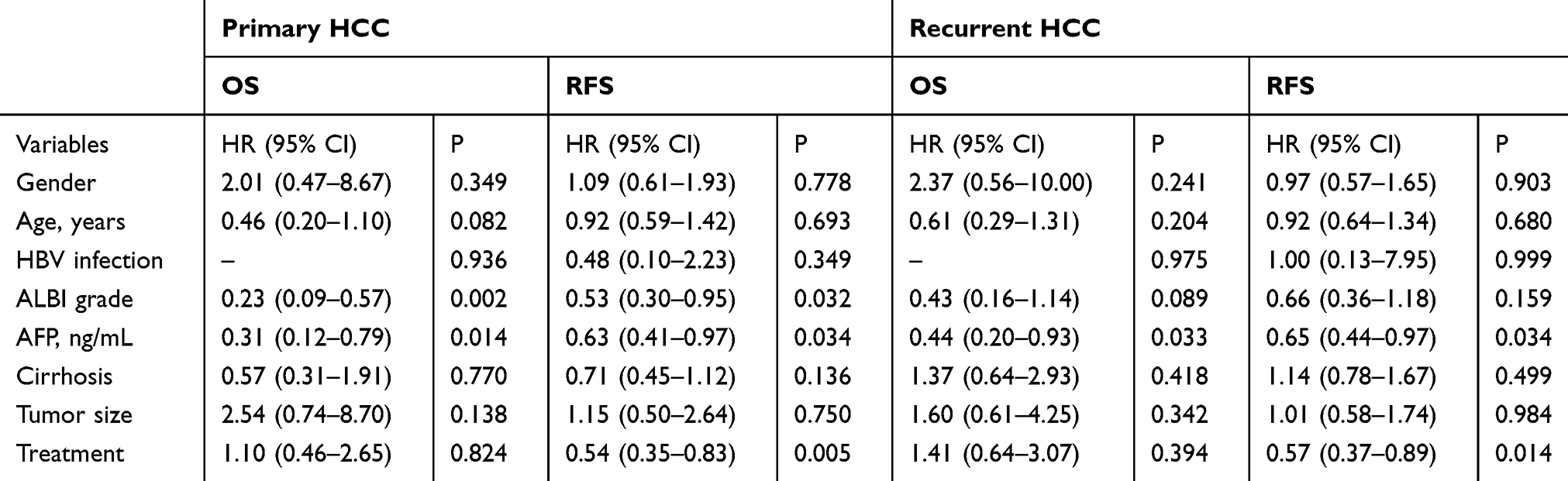 |
Table 2 Univariate Analyses for Prognostic Factors of OS and RFS in the Primary and Recurrent Groups |
Although treatment modalities showed a significant association with RFS in both the primary and recurrent groups, patients receiving ablation had worse liver function and a relatively larger tumor size (p<0.001 and = 0.044). After balancing these prognostic factors with propensity score matching (PSM), no significant association was found between treatment modalities and RFS in either the primary or recurrent groups (p = 0.056 and 0.052). Patients’ data after PSM are provided in data of the primary group after propensity score matching. In multivariate analyses, the ALBI grade and serum AFP level were significantly associated with OS and RFS in the primary group (p = 0.003 and 0.019; p = 0.024 and 0.027, respectively). In the recurrent group, only serum AFP was related with OS and RFS (p = 0.033 and 0.034, respectively). Detailed data are listed in Supplementary Table 1.
Discussion
To the best of our knowledge, this is the first real-world study evaluating the survival outcomes of patients with subcentimeter HCC and those with HCC measuring 1–2 cm after curative treatments. We found no significant difference in OS or RFS between patients with subcentimeter HCC and those with HCC measuring 1–2 cm. These results suggested that wait-and-see strategy is recommendable for patients with subcentimeter HCCs.
The Barcelona Clinic Liver Cancer (BCLC) system defines solitary HCC measuring up to 2 cm as very early stage in patients with preserved liver function.18 The five-year survival rate can reach approximately 80% in these patients.2 Even patients with early-stage recurrent HCC had comparable survival to those with primary HCCs after curative treatments.19 The promising survival improves people’s awareness of follow-up and motivates widely executed surveillance. In addition, advances in imaging technology allow for better detection and diagnosis of small hepatic lesions.13 Improvements in surveillance policy and technology have led to an increasing number of detected subcentimeter hepatic lesions. Although the diagnostic performance of multiphasic contrast-enhanced CT/MRI has developed in recent years, their diagnostic accuracy is still relatively poor for subcentimeter HCC. Though the diagnostic performance of contrast-enhanced US for small HCCs has been improving, it still remains uncertain for subcentimeter HCCs.20 In addition to imaging, biopsy is also limited in confirming subcentimeter HCCs due to sampling errors.10
Considering the current diagnostic difficulties, the management of subcentimeter HCC remains controversial at present. The AASLD and ESMO propose continued follow-up for subcentimeter hepatic nodules detected during surveillance, regardless of whether there are typical imaging features of HCC.10,11 The initial growth rate of subcentimeter HCC is usually low, so curative treatments are almost always available for HCCs measuring up to 2 cm at diagnosis.21 However, according to the JSH guidelines, hepatic nodules showing hypervascularity in the arterial phase and washout in the delayed phase can be diagnosed as HCC regardless of tumor size. Liver resection or percutaneous ablation is recommended for these patients.12 These aforementioned suggestions lack evidentiary support, and a multidisciplinary team is recommended for such tiny lesions. Our study evaluated the oncologic outcomes of patients with subcentimeter HCC and those with HCC measuring 1–2 cm, and the survival times of these two cohorts were comparable in both the primary and recurrent groups. Routine screening ought to be suitable for patients with subcentimeter hepatic lesions, even for those with subcentimeter HCC in terms of safety and cost efficiency.
Percutaneous ablation, a minimally invasive but efficient treatment, is recommended as the first-line therapy for patients with a solitary HCC lesion measuring up to 2 cm.10,11 However, technical difficulties exist in ablation for subcentimeter HCC. Ultrasound (US) or CT is usually adopted to guide ablation procedures, but the detection rate of subcentimeter HCC is relatively low with US and CT, which makes tumor localization difficult.17 Even with the US/MRI fusion-guided technique, the feasibility rate for subcentimeter HCCs was only 65.7%.14 Considering that the feasibility rate was unsatisfactory in academic institutions with MRI guidance, the feasibility of ablation for subcentimeter HCC with US/CT can be worse in other institutions. In addition to localization difficulties, percutaneous ablation can cause bleeding and tumor track seeding during treatment. With the coexistence of these risks, it may not be cost-effective to treat patients with subcentimeter HCC by ablation with a high risk of treatment failure.
Current studies of subcentimeter HCCs mainly focus on the diagnostic accuracy of imaging, and few studies have explored how to manage these tiny lesions. Woo et al reported that the RFS was similar between patients undergoing early treatments and those receiving watchful waiting for subcentimeter hepatic nodules with typical imaging features of HCC.22 The mean diameters of the lesions were 7.4 mm and 11.2 mm in the early-treatment and watchful-waiting groups, respectively. The RFS also did not differ significantly between patients with subcentimeter HCC and those with HCC measuring 1–2 cm in this study. However, the RFS in this study was better than that observed by Woo et al Only 25.9% (7/27) of patients received curative treatments at the subcentimeter stage in the early-treatment group, and 55.6% (20/36) of patients underwent curative treatments in the watchful-waiting group. The treatment modalities were quite different in their study. Though transarterial chemoembolization (TACE) can control the HCC progression with considerable cost-effectiveness, whether it can treat subcentimeter HCCs curatively remains uncertain.23 In addition, hepatectomy and ablation are first-line treatments for early-stage HCCs instead of TACE.11 All the patients in our study had a solitary HCC lesion up to 2 cm and received curative treatments, which is closer to clinical practice for the population at high risk for HCC. Previous study found that the OS was similar between patients with primary subcentimeter HCC and those with HCC measuring 1–2 cm based on the data from the Surveillance, Epidemiology and End Results database.24 The patients were mainly diagnosed with hepatitis C virus infection or non-alcoholic fatty liver disease in that study, and RFS was not evaluated.
Our results suggest that follow-up is suitable for patients with subcentimeter hepatic lesions, even for those with subcentimeter HCC. The follow-up protocol is rough for subcentimeter hepatic lesions currently. A precise protocol should be developed based on risk stratification. The subcentimeter hepatic lesions with typical imaging features are more progressive, so more intensive surveillance is suggested for patients with these nodules, such as examinations every two months. The growth rate of small HCC relates to cirrhosis, types of etiology and antiviral therapy.25,26 Patients with cirrhosis or high serum AFP levels should receive imaging examinations every 2–3 months. Biomolecules may also help identify those with more progressive HCCs and requiring more intensive surveillance for recurrence.27 To manage HCC patients after hepatectomy, combination of pathological and radiological characteristics can classify them into cohorts with different aggressiveness of HCCs, which can assist to develop individual follow-up protocol.28 Peri-hepatic-vein is a risk factor for recurrence, so lesions near hepatic veins may require more intensive follow-up during surveillance for recurrence.29 Future studies should focus on developing a surveillance protocol with an individualized optimal follow-up interval based on risk stratification. Liver stiffness, a non-invasive test, can also help to identify patients at high risk for HCCs either for primary or recurrent ones.30,31 An optimal follow-up schedule can not only confirm very early-stage HCC in a timely manner but also prevent the unnecessary waste of medical resources.
If patients with subcentimeter hepatic lesions insist on receiving biopsy, it is unnecessary for those with negative results first to receive a secondary biopsy. If subcentimeter lesions are confirmed to be HCC, curative treatments can be provided for anxious patients. However, false-negative rate can reach 30% for HCCs < 2 cm, which can be higher for subcentimeter HCCs.10 For patients with negative pathological diagnosis or rejection of biopsy, definite and precise diagnosis cannot be made if they are treated with ablation. Subsequent management on these patients may be difficult without precise diagnosis. Even if these patients received laparoscopic hepatectomy for accurate diagnosis, the costs may be high in terms of economy and physiology.
This study has several limitations in addition to its retrospective nature. First, not all patients were pathologically confirmed to have HCC. Of the patients with primary subcentimeter HCC, 76.5% of them received hepatectomy. Although the possibility existed that the ablated subcentimeter nodules were benign lesions, the survival of patients with subcentimeter HCC should be worse than that in this study, and the survival was even less likely to be significantly different between patients with subcentimeter HCC and those with HCC measuring 1–2 cm. Second, patients were mainly infected with hepatitis B virus in this study. Whether our results can be applied to HCCs with other etiologies should be further explored. Third, the sample size of patients with subcentimeter HCCs was relatively limited in this study. The tumor staging and microvascular invasion of primary HCCs can affect the survival of patients with recurrent HCCs.32 However, the present sample size is insufficient for further classifying recurrent patients into subgroups based on tumor staging and microvascular invasion. Subcentimeter HCC is relatively rare in clinical practice, so multicenter studies are needed to further explore this issue and provide high-level evidence.
In conclusion, the oncologic outcomes did not differ significantly between patients with subcentimeter HCC and those with HCC measuring 1–2 cm, in both the primary and recurrent cohorts. Routine screening is suitable for subcentimeter hepatic lesions detected during surveillance.
Abbreviations
HCC, hepatocellular carcinoma; MRI, magnetic resonance imaging; CT, computed tomography; AASLD, the American Association for the Study of Liver Diseases; EASL, the European Association for the Study of the Liver; ALBI, albumin-bilirubin; AFP, alpha fetoprotein; K-M, Kaplan–Meier; OS, overall survival; RFS, recurrence-free survival; PSM, propensity score matching; BCLC, the Barcelona Clinic Liver Cancer; US, ultrasound.
Data Sharing Statement
The datasets used during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the institutional review board of Sun Yat-Sen University Cancer Center as a retrospective study, and the requirement for informed consent was waived. All patients’ data assessed complied with relevant data protection and privacy regulations. All procedures performed in studies involving human participants were in accordance with the ethical standards of the1964 Helsinki declaration and its later amendments.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This study received no funding support.
Disclosure
The authors declare that they have no competing interests.
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424.
2. Yamamoto J, Okada S, Shimada K, et al. Treatment strategy for small hepatocellular carcinoma: comparison of long-term results after percutaneous ethanol injection therapy and surgical resection. Hepatology. 2001;34(4 Pt 1):707–713. doi:10.1053/jhep.2001.27950
3. Mittal S, Kanwal F, Ying J, et al. Effectiveness of surveillance for hepatocellular carcinoma in clinical practice: a United States cohort. J Hepatol. 2016;65(6):1148–1154. doi:10.1016/j.jhep.2016.07.025
4. Golfieri R, Garzillo G, Ascanio S, Renzulli M. Focal lesions in the cirrhotic liver: their pivotal role in gadoxetic acid-enhanced MRI and recognition by the Western guidelines. Dig Dis. 2014;32(6):696–704. doi:10.1159/000368002
5. De Toni EN, Schlesinger-Raab A, Fuchs M, et al. Age independent survival benefit for patients with hepatocellular carcinoma (HCC) without metastases at diagnosis: a population-based study. Gut. 2020;69(1):168–176. doi:10.1136/gutjnl-2018-318193
6. Yu MH, Kim JH, Yoon JH, et al. Small (</=1-cm) hepatocellular carcinoma: diagnostic performance and imaging features at gadoxetic acid-enhanced MR imaging. Radiology. 2014;271(3):748–760.
7. Horvat N, Monti S, Oliveira BC, Rocha CCT, Giancipoli RG, Mannelli L. State of the art in magnetic resonance imaging of hepatocellular carcinoma. Radiol Oncol. 2018;52(4):353–364. doi:10.2478/raon-2018-0044
8. Watanabe A, Ramalho M, AlObaidy M, Kim HJ, Velloni FG, Semelka RC. Magnetic resonance imaging of the cirrhotic liver: an update. World J Hepatol. 2015;7(3):468–487. doi:10.4254/wjh.v7.i3.468
9. Lee JM, Choi BI. Hepatocellular nodules in liver cirrhosis: MR evaluation. Abdom Imaging. 2011;36(3):282–289. doi:10.1007/s00261-011-9692-2
10. Heimbach JK, Kulik LM, Finn RS, et al. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology. 2018;67(1):358–380.
11. Galle PR, Forner A, Llovet JM, European Association for the Study of the Liver. Electronic address eee, European association for the study of the L. EASL clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2018;69(1):182–236. doi:10.1016/j.jhep.2018.03.019
12. Kokudo N, Hasegawa K, Akahane M, et al. Evidence-based clinical practice guidelines for hepatocellular carcinoma: the Japan society of hepatology 2013 update (3rd JSH-HCC guidelines). Hepatol Res. 2015;45(2). doi:10.1111/hepr.12464.
13. Park MJ, Kim YK, Lee MW, et al. Small hepatocellular carcinomas: improved sensitivity by combining gadoxetic acid-enhanced and diffusion-weighted MR imaging patterns. Radiology. 2012;264(3):761–770. doi:10.1148/radiol.12112517
14. Song KD, Lee MW, Rhim H, et al. Percutaneous US/MRI fusion-guided radiofrequency ablation for recurrent subcentimeter hepatocellular carcinoma: technical feasibility and therapeutic outcomes. Radiology. 2018;288(3):878–886. doi:10.1148/radiol.2018172743
15. Peng ZW, Lin XJ, Zhang YJ, et al. Radiofrequency ablation versus hepatic resection for the treatment of hepatocellular carcinomas 2 cm or smaller: a retrospective comparative study. Radiology. 2012;262(3):1022–1033. doi:10.1148/radiol.11110817
16. Shuto T, Kinoshita H, Hirohashi K, et al. Indications for, and effectiveness of, a second hepatic resection for recurrent hepatocellular carcinoma. Hepatogastroenterology. 1996;43(10):932–937.
17. Lee MW, Kim YJ, Park HS, et al. Targeted sonography for small hepatocellular carcinoma discovered by CT or MRI: factors affecting sonographic detection. AJR Am J Roentgenol. 2010;194(5):W396–400. doi:10.2214/AJR.09.3171
18. Bruix J, Reig M, Sherman M. Evidence-based diagnosis, staging, and treatment of patients with hepatocellular carcinoma. Gastroenterology. 2016;150(4):835–853. doi:10.1053/j.gastro.2015.12.041
19. Gavriilidis P, Askari A, Azoulay D. Survival following redo hepatectomy vs radiofrequency ablation for recurrent hepatocellular carcinoma: a systematic review and meta-analysis. HPB (Oxford). 2017;19(1):3–9. doi:10.1016/j.hpb.2016.10.003
20. Leoni S, Piscaglia F, Granito A, et al. Characterization of primary and recurrent nodules in liver cirrhosis using contrast-enhanced ultrasound: which vascular criteria should be adopted? Ultraschall Med. 2013;34(3):280–287. doi:10.1055/s-0033-1335024
21. Pecorelli A, Lenzi B, Gramenzi A, et al. Curative therapies are superior to standard of care (transarterial chemoembolization) for intermediate stage hepatocellular carcinoma. Liver Int. 2017;37(3):423–433. doi:10.1111/liv.13242
22. Woo JH, Song KD, Kim SH. Subcentimeter hypervascular nodules with typical imaging findings of hepatocellular carcinoma on gadoxetic acid-enhanced MRI: outcomes of early treatment and watchful waiting. Eur Radiol. 2017;27(10):4406–4414. doi:10.1007/s00330-017-4818-8
23. Cucchetti A, Trevisani F, Cappelli A, et al. Cost-effectiveness of doxorubicin-eluting beads versus conventional trans-arterial chemo-embolization for hepatocellular carcinoma. Dig Liver Dis. 2016;48(7):798–805. doi:10.1016/j.dld.2016.03.031
24. Sun X, Zhang Y, Lyu N, Li X, Chen M, Zhao M. The optimal management for sub-centimeter hepatocellular carcinoma: curative treatments or follow-up? Med Sci Monit. 2019;25:4941–4951. doi:10.12659/MSM.916451
25. An C, Choi YA, Choi D, et al. Growth rate of early-stage hepatocellular carcinoma in patients with chronic liver disease. Clin Mol Hepatol. 2015;21(3):279–286. doi:10.3350/cmh.2015.21.3.279
26. Taouli B, Goh JS, Lu Y, et al. Growth rate of hepatocellular carcinoma: evaluation with serial computed tomography or magnetic resonance imaging. J Comput Assist Tomogr. 2005;29(4):425–429. doi:10.1097/01.rct.0000164036.85327.05
27. Vasuri F, Golfieri R, Fiorentino M, et al. OATP 1B1/1B3 expression in hepatocellular carcinomas treated with orthotopic liver transplantation. Virchows Arch. 2011;459(2):141–146. doi:10.1007/s00428-011-1099-5
28. Vasuri F, Renzulli M, Fittipaldi S, et al. Pathobiological and radiological approach for hepatocellular carcinoma subclassification. Sci Rep. 2019;9(1):14749. doi:10.1038/s41598-019-51303-9
29. Chen J, Peng K, Hu D, et al. Tumor location influences oncologic outcomes of hepatocellular carcinoma patients undergoing radiofrequency ablation. Cancers (Basel). 2018;10(10):378. doi:10.3390/cancers10100378
30. Marasco G, Colecchia A, Colli A, et al. Role of liver and spleen stiffness in predicting the recurrence of hepatocellular carcinoma after resection. J Hepatol. 2019;70(3):440–448. doi:10.1016/j.jhep.2018.10.022
31. Marasco G, Colecchia A, Silva G, et al. Non-invasive tests for the prediction of primary hepatocellular carcinoma. World J Gastroenterol. 2020;26(24):3326–3343. doi:10.3748/wjg.v26.i24.3326
32. Xia Y, Li J, Liu G, et al. Long-term effects of repeat hepatectomy vs percutaneous radiofrequency ablation among patients with recurrent hepatocellular carcinoma: a randomized clinical trial. JAMA Oncol. 2020;6(2):255–263. doi:10.1001/jamaoncol.2019.4477
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.