Back to Journals » Advances in Medical Education and Practice » Volume 17
Cadaver Dissections in Medical School Based on Functional Neuroanatomy Improve Results: A Double Blind Prospective Randomized Controlled Study
Authors Ternerot J, Vigren P ![]()
Received 9 July 2025
Accepted for publication 19 December 2025
Published 24 February 2026 Volume 2026:17 552551
DOI https://doi.org/10.2147/AMEP.S552551
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Balakrishnan Nair
Jens Ternerot,1 Patrick Vigren1– 5
1Department of Biomedical and Clinical Sciences, Linköping University, Lnköping, Sweden; 2Department of Neurology, Region Östergötland, Linköping, Sweden; 3Department of Neurosurgery, Region Östergötland, Linköping, Sweden; 4Department of Neurosurgery, Örebro University Hospital, Örebro, Sweden; 5Faculty of Medicine and Health, Örebro University, Örebro, Sweden
Correspondence: Patrick Vigren, Email [email protected]
Background: Cadaver dissection is a well-established method to teach neuroanatomy in medical school. However, the outcome on functional anatomical understanding and student experience has not been studied. The aim of this study was to compare traditional topographically based brain cadaver dissections with dissections based on functional white matter dissections with regard to functional-anatomical knowledge and student experience.
Methods: Pre-clinical medical students were randomly assigned to a control group with traditional two dimensional topographical cadaver dissections and to study groups with functionally based white matter dissections. The control dissections were performed as formerly planned by non-clinical anatomy tutors and the study dissections were planned and overseen by an experienced neurosurgeon. After the dissections, the students underwent a web-based questionnaire including four questions on topographical and functional neuroanatomy, and three questions on experience and self-evaluation of neuroanatomical knowledge.
Results: A total of 130 students were included, (n=33 in the control group and n=97 in the study group). Students in the study group scored higher on knowledge-based multiple-choice questions regarding speech and language, motor functions and the ventricular system; however, statistical significance was observed only for speech and language. They also scored higher in self-perceived knowledge after the dissections, although not statistically significant.
Discussion: Including functional and clinical aspects in brain cadaver improves anatomy teaching in pre-clinical medical students. The authors argue that it is of importance to integrate clinicians in the pre-clinical anatomy teaching.
Keywords: anatomy, neuroanatomy, cadaver dissections, preclinical education, medical school
Introduction
Teaching anatomy has been an integral part of medical education for many centuries and the methods for doing so have remained relatively unchanged until recently.1 The use of human cadavers for gaining medical knowledge is widely thought to have originated in ancient Greece, later revived in medieval Italy and subsequently modernized in the US and Europe the following centuries.2
Neuroanatomy and neural sciences have been described as fields that are perceived as complicated subjects by students,3 most famously by Jozefowicz who coined the term “neurophobia”.4 He defined it as “fear of the neural sciences and clinical neurology that is due to the students’ inability to apply their knowledge of basic sciences to clinical situations” and stated that around 50% of alla medical students experienced this phenomenon during the course of their undergraduate studies. Later authors have developed the concept further. Rodriguez et al performed a cross-sectional study covering four medical schools and different stages of education (pre-clinical, clinical and internship) – finding that 63.3% expressed neurophobia, with the incidence increasing the further the training proceeded. The students stressed that the need to understand neuroanatomy and neurophysiology were the most important reasons for neurophobia, whereas more and better bedside teaching was proposed as to improve education.5 An updated review in 2024 found 119 publications on this phenomenon during a 30-year period. However, most studies identified anxiety (81%) rather than fear (42%) as the dominating emotion.6
Appropriate and well-directed teaching methods in neuroanatomy are therefore of great interest for the educational community. Neuroanatomy is mainly being studied in 2D during the course of a medical curriculum, with anatomy atlases and text books as the primary source of material. Historically, this method of learning has been complemented by cadaver dissections of the central nervous system.1 However, several new approaches have been proposed, not least utilizing new technologies. Hortsch et al (2025) reviewed the trends in anatomical teaching over time and from a world-wide perspective. Regarding neuroanatomy, they observed that, in US, there had been a clear shift from laboratory hours to classroom hours the last 50 years. The actual content and methods included in each category were not further specified. They also conclude that literature on neuroanatomy teaching is sparse.7 On the other hand, there are a lot of studies emphasizing new technologies of neuroanatomy teaching. One of the latest technologies is virtual reality. In a single-blind randomized controlled study, Garcia-Robles et al compared the effects of immersive virtual reality as a tool to teach neuroanatomy to physiotherapy students. Their study group used a virtual reality tool with the MetaQuest 2 IVR device and the control group followed a “traditional learning approach” using textbooks and atlases. There was an obvious statistical difference, favouring the virtual reality group regarding anatomical knowledge retention. Telecan et al (2025) compared results of studies evaluating differences between virtual tables and cadaver dissections, concluding that these methods are best if used in combination – being complimenting rather than competing.8 A group at Stanford University made similar conclusions: integrating case-based virtual reality and cadaver dissections is well received in neuroanatomy teaching.9 Despite the vast number of studies comparing different technologies for neuroanatomy teaching, we have found no studies comparing the effects of different approaches in neuroanatomy cadaver dissections in medical school.
Traditionally, the cadaver dissections at the Faculty of Medicine at Linköping University in Sweden were focused on teaching neuroanatomy with the support of cross-sectional slices of the brain in coronal, sagittal and transversal planes. In contrast to this setup, the Klingler’s fibre dissection method, where the brain is prepared and dissected in 3D with focus on white matter tracts, topography and spatial organisation, focuses on demonstrating the white matter connectome.10,11 This technique is being used both by anatomists and clinically oriented neuroscientists, and examples of its utilization can be found in the field of neurosurgery (13) and neuroimaging.10 Studies in other fields have shown that 3D-visualisation has a complimentary potential to 2D-visualisation.12,13
The objective of this randomized controlled prospective study was to compare traditional cross-sectional cadaver dissections with functionally based dissections of the brain, using the Klingler method.
Materials and Methods
Pre-clinical medical students, partaking in neuroanatomy classes, were all given the same theoretical training: 90 minutes of interactive group seminar on functional neuroanatomy focusing on speech and motor functions including cortical organization, subcortical white matter pathways and spine white matter pathways. For this session, students were not assigned to any group related to subsequent randomisation, and the teacher did not know which students would be in which cadaver dissection group. “Pre-clinical” was defined as being part of the fifth semester, not starting clinical rotations.
Students were thereafter blindly and randomly assigned to either a study group or a control group, through scheduling by an independent and blinded scheduler. There was no prior information to the students about the teaching sessions being different. The anatomy tutors (senior medical students) were not informed that there were different groups with different cadaver preparations. The group sizes were restricted by practical considerations, such as availability of trained tutors for the different settings. For both groups, cadaver dissection sessions lasted for approximately 60 minutes.
For the study group, the fibre dissection was overseen by an experienced neurosurgeon experienced in functional neuroanatomy, awake functional mapping and white tract fiber dissection.14,15
For the control group, non-clinical anatomy tutors prepared the brains using cross-sectional dissection.
In the study group, the Klingler method of three-dimensional fibre dissection was used.11 The teaching session was divided into four different stations. At the speech/language station, the cadaver was prepared with exposure of the arcuate fascicle (FA), the inferior fronto-occipital fascicle (IFOF) and the inferior longitudinal fascicle (ILF). At the motor function station, the brain was prepared with dissection of the cortico-spinal tract (CST) from the precentral gyrus, exposing the internal and external capsules by splitting the putamen and following the latter through the cerebral peduncle and to the medulla oblongata. The hydrocephalus station exposed the frontal horn, cella media, trigonum and temporal horn of the lateral ventricle and the third ventricle through a staged 3d dissection. The fourth station, cerebrovascular anatomy, exposed the Circle of Willis.
The control group underwent teaching using cadavers with cross-sectional slices of the brain divided into four stations: axial 10 mm slices of the brain, coronal 10 mm sections of the brain, hydrocephalus and vascular anatomy, the latter two being the same preparations as in the study group.
After the cadaver teaching sessions, all students were asked to answer a web-based questionnaire on the way out of the lecture hall. The questionnaire consisted of four questions on topographical and functional anatomy, of which the answers to the questions had been mentioned during the teaching moment in both groups. An example of questions is “What structures are involved in speech function?” with four alternatives including three structures each. Furthermore, the questionnaire also included three questions on experience and self-evaluation of neuroanatomical knowledge. The results were exported to Excel and compiled.
The students in the control group were offered to join a separate session with the same set up as the study group, after the study was completed. This did not differ from other offers of teaching at the university, since there are several “resource sessions” that are offered to student, without being compulsory.
Statistical analysis was made in house using Excel t-test.
Results
A total of 130 students were included in three groups (n=33 in the control group and total n=97 in the study group). The group sizes were, as previously mentioned, defined by practical considerations rather than statistical, due to restrictions in tutor availability.
Knowledge Based Questions
Students in the study group answered correctly to a greater extent (38%) than students in the control group (12%) regarding speech function (p=0.0052). Regarding motor function, there was a difference in correct answers with 73% of the students in the study group stating correct answers as compared to 58% in the control group, however not statistically significant (p=0.0945). Regarding hydrocephalus, there was no statistically significant difference (p=0.1481) (Table 1).
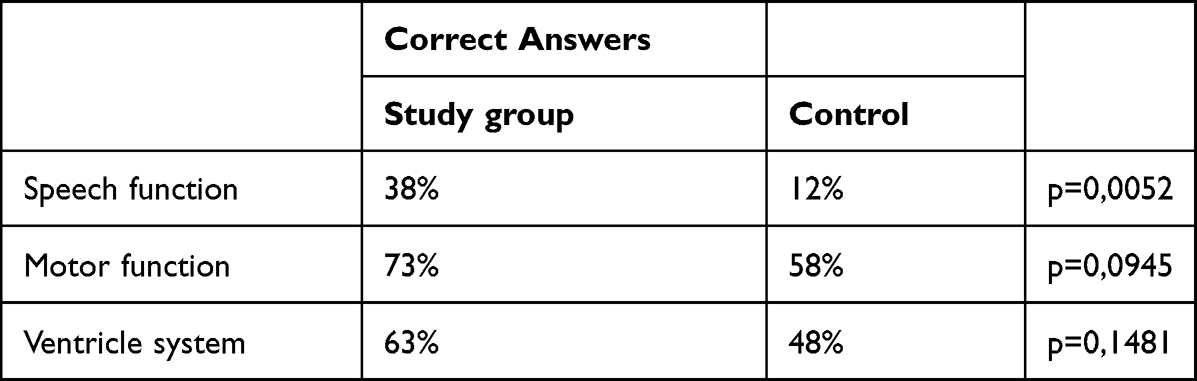 |
Table 1 Knowledge Results |
Self-Evaluated Knowledge
Regarding self-evaluated knowledge, there were no statistical differences between the groups, although the change from before and after the cadaver sessions was higher in the study group than in the control group (Table 2).
 |
Table 2 Self-Evaluated Knowledge |
Teaching Experience
Both groups scored high on experience of the session. The scale was 1–5 (lowest to highest general experience of the teaching session) and there was no significant difference between the groups (Table 3).
 |
Table 3 Experience of the Session |
Discussion
The present study compared acquired knowledge and experienced knowledge between two different teaching approaches within the realm of brain cadaver dissection. Using the Klingler method5 of white matter dissection, combined with neuro-functional teaching on the dissection session, improves knowledge about speech and language networks of the brain, as compared to the traditional axial/coronal/sagittal slice dissection method. The students in the former group also score higher for motor function and hydrocephalus, but this was not statistically significant.
As all students underwent the same theoretical training on neuro-functional anatomy, specifically emphasising the speech/language networks and motor function, we strongly suggest that the effect can be attributed to the dissection setup itself. Additionally, with the differences in correct answers for motor function and hydrocephalus, there is a possibility that these would be statistically significant if larger groups were studied. This, however, needs to be studied further.
The fact that both groups had a high level of perceived level of experience in the cadaver teaching sessions shows that the results are not due to tutors being more engaging in the study group, further supporting that there is an actual causality between the dissection set-up and better results in the study group, not related to subjective experience. We interpret this as the tutors as support that the study is really isolating the causality of the method, and neutralizing teaching bias.
It has previously been demonstrated that cadaver dissections are superior to theoretical teaching alone in the realm of neuro-anatomy, also when looking at knowledge retention.16 It has also been shown that students do not experience the same teaching effect with online anatomy labs as they do in “face-to-face” dissections in neuroanatomy.11
Recent studies support that a combination of cadaver dissections and other anatomical teaching modalities, such as 3d-models, can give better results than cadaver dissection alone. Some authors refer to cadaver dissection as the golden standard in teaching neuroanatomy, whilst others dispute this view.13,17–20
The strength of this study is that it is a prospective, blind, randomized study. It can be argued that it selectively investigates the difference between pure topographical brain cadaver dissection and 3d dissections based on functional networks, with the latter being supposedly superior. Although not comparing with other model-based teaching methods, the difference between the two groups at least shows that dissection methodology influences knowledge on specific topics, in this case speech function networks of the brain. Certainly, it can be argued that the groups are not equally large. This was, however, the due to the reality of resources and not approachable by scientific considerations.
Further studies could compare 3d printed models of the subcortical white matter networks with comparable cadaver dissections to evaluate if one of these set ups is more effective.
Conclusion
The present study compared two methods of teaching neuroanatomy with cadaver dissections. It showed some favourability of function based, white matter dissections when compared to a traditional topographical method.
Ethical Statement
The study does not fall under the Swedish Ethical Review Act (2003:460) as no personal information was collected from the study objects (students). The cadaver management was in accordance with laws regulating medical teaching and body donations (SFS 1995:831 and SFS 2008:286), where medical institutions accept donations through an official programme. The brain cadaver specimens at Linköping University Faculty of Medicine were obtained through Karolinska Institutet’s donation programme.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sugand K, Abrahams P, Khurana A. The anatomy of anatomy: a review for its modernization. Anat Sci Educ. 2010;3(2):83–5. doi:10.1002/ase.139
2. Ghosh SK. Human cadaveric dissection: a historical account from ancient Greece to the modern era. Anatomy Cell Biology. 2015;48(3):153–169. doi:10.5115/acb.2015.48.3.153
3. Burford C, Pasha T, Iyer P, Rupawala H, Andreica EC, Huett M. Initiatives to reduce neurophobia in medical students: a novel neuroscience conference model. J Neurol Sci. 2019;398:119–120. doi:10.1016/j.jns.2019.01.042
4. Jozefowicz RF. Neurophobia: the fear of neurology among medical students. Arch Neurol. 1994;51(4):328–329. doi:10.1001/archneur.1994.00540160018003
5. Rodrigues AN, Sousa TS, Marvão MCR, et al. Education research: monitoring and tracking neurophobia: evidence from a temporal analysis of Brazilian medical schools. Neurol Educ. 2023;2(3):e200076. doi:10.1212/NE9.0000000000200076
6. Tan Y, Lin SZZ, Tan Z. From neurophobia to neuroanxiety: an opportune review of its definition and impact on neurology educators and learners. Neurol Educ. 2025;4(3):e200247. doi:10.1212/NE9.0000000000200247
7. Hortsch M, Girão-Carmona VCC, Leite ACRM, et al. A global overview of anatomical science education and its present and future role in biomedical curricula. Anat Sci Educ. 2025;19(1):5–45. doi:10.1002/ase.70137
8. García‐Robles P, Obrero‐Gaitán E, Cortés‐Pérez I, Ibancos‐Losada MDR, Díaz‐Fernández Á, Osuna‐Pérez MC. The effectiveness of immersive virtual reality as a student-centered tool for learning neuroanatomy: a single-blind randomized controlled trial with physiotherapy students. Anat Sci Educ. 2025;18(10):1083–1094. doi:10.1002/ase.70068
9. Savchuk S, Vigo V, Chidambaram S, et al. Early neurosurgical education in the era of distance learning: incorporating virtual reality and cadaveric specimen demonstrations. World Neurosurg. 2025;193:706–714. doi:10.1016/j.wneu.2024.09.132
10. Agrawal A, Kapfhammer JP, Kress A, et al. Josef Klingler’s models of white matter tracts: influences on neuroanatomy, neurosurgery, and neuroimaging. Neurosurgery. 2011;69(2):238–254;discussion52–4. doi:10.1227/NEU.0b013e318214ab79
11. Wysiadecki G, Clarke E, Polguj M, Haladaj R, Zytkowski A, Topol M. Klingler’s method of brain dissection: review of the technique including its usefulness in practical neuroanatomy teaching, neurosurgery and neuroimaging. Folia Morphol. 2019;78(3):455–466. doi:10.5603/FM.a2018.0113
12. Estevez ME, Lindgren KA, Bergethon PR. A Novel three-dimensional tool for teaching human neuroanatomy. Anat Sci Educ. 2010;3(6):309–317.
13. Ye Z, Dun A, Jiang H, et al. The role of 3D printed models in the teaching of human anatomy: a systematic review and meta-analysis. BMC Med Educ. 2020;20(1):335. doi:10.1186/s12909-020-02242-x
14. Vigren P, Eriksson M, Gauffin H, et al. Awake craniotomy in epilepsy surgery includes previously inoperable patients with preserved efficiency and safety. Int J Neurosci. 2024;134(12):1624–1629. doi:10.1080/00207454.2023.2279498
15. Milos P, Metcalf K, Vigren P, Lindehammar H, Nilsson M, Boström S. Awake craniotomy for brain tumours. Lakartidningen. 2016;113:D4FI.
16. Antonopoulos I, Pechlivanidou E, Piagkou M, et al. Students’ perspective on the interactive online anatomy labs during the COVID-19 pandemic. Surg Radiol Anat. 2022;44(8):1193–1199. doi:10.1007/s00276-022-02974-z
17. Baskaran V, Strkalj G, Strkalj M, Di Ieva A. Current applications and future perspectives of the use of 3D printing in anatomical training and neurosurgery. Front Neuroanat. 2016;10:69. doi:10.3389/fnana.2016.00069
18. Chytas D, Piagkou M, Salmas M, Johnson EO. Is cadaveric dissection the “gold standard” for neuroanatomy education? Anat Sci Educ. 2020;13(6):804–805. doi:10.1002/ase.1957
19. De Benedictis A, Duffau H, Paradiso B, et al. Anatomo-functional study of the temporo-parieto-occipital region: dissection, tractographic and brain mapping evidence from a neurosurgical perspective. J Anat. 2014;225(2):132–151. doi:10.1111/joa.12204
20. Pitts LL, Majewski-Schrage T, Schieltz EK, Harpenau LA, Radunzel J. A know-brainer: the power of cadaver-based instruction to teach clinical neuroanatomy. Am J Speech Lang Pathol. 2023;1–15.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.