")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
CACNA1C Gene rs1006737 Polymorphism Affects Cognitive Performance in Chinese Han Schizophrenia
Authors Chen M , Jiang Q, Zhang L
Received 12 May 2022
Accepted for publication 27 July 2022
Published 10 August 2022 Volume 2022:18 Pages 1697—1704
DOI https://doi.org/10.2147/NDT.S373492
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yuping Ning
Mengyi Chen, Qi Jiang, Lei Zhang
Department of Geriatric, Shanghai Pudong New Area Mental Health Center, Tongji University School of Medicine, Shanghai, People’s Republic of China
Correspondence: Mengyi Chen, Department of Geriatric, Shanghai Pudong New Area Mental Health Center, Tongji University School of Medicine, Shanghai, People’s Republic of China, Tel/Fax +8602168306699, Email [email protected]
Objective: To investigate the relationship between L-type calcium channel α 1C subunit (CACNA1C) gene polymorphism and schizophrenia (SCZ) and cognitive function in the Han nationality, the main nationality in China.
Methods: Genotyping of CACNA1C SNP (rs1006737, rs1024582, rs2007044) in SCZ patients (n = 312) and healthy controls (n = 305) was performed. Cognitive function was assessed in the SCZ patients using Repeatable Battery for the Assessment of Neuropsychological Status (RBANS). Then, the correlation between SNP and SCZ, as well as cognition, was calculated.
Results: There was no significant difference in allele frequency and genotype distribution frequency of the three polymorphic loci of CACNA1C gene between the two groups. In cognitive tests, delayed memory scores in RBANS were significantly lower in rs1006737 “A” risk allele carriers than in non-carriers.
Conclusion: There is no significant difference in allele and genotype frequency of CANCA1C Gene rs1006737, rs1024582 and rs2007044 between the schizophrenia patients and healthy controls. The cognitive function of schizophrenia patients is correlated with the rs1006737, and the delayed memory of “A” allele carriers is significantly reduced.
Keywords: schizophrenia, SNP, cognition, CACNA1C
Introduction
Schizophrenia is a lifelong mental disorder with unknown etiology and severe disability risk.1 Due to the prolonged course of the disease, easy recurrence and often accompanied by cognitive impairment, patients often have varying degrees of social function loss, coupled with poor treatment compliance, poor family and social support, suicide and accidents and other factors, the average life expectancy of patients with schizophrenia is significantly shorter than the general population.2–4 Based on the year lived with Disability (YLD) index of the Global Burden of Disease Study, schizophrenia ranks 20th among all diseases and third among mental disorders. It ranks 17th among all diseases in China and 3rd among mental disorders.5 Studies have shown that genetic factors play an important role in the occurrence of this disease.6,7
Calcium channels are an important hub for converting electrical activity into biochemical events in the central nervous system. Since nerve cells containing L-type calcium channels α1C (voltage-dependent, L-type, alpha1C, CACNA1C) account for more than 80% of mammalian brains,8 CACNA1C becomes the primary target for ion channel hypothesis of schizophrenia. CACNA1C gene is located on the short arm of chromosome 12P13.3, spanning a genomic region of about 6.45 MB.9 It mediates calcium influx into cells by regulating L-type voltage-gated calcium channels (LTCC), which play an important role in regulating dendrite development, neuronal survival, synaptic plasticity, memory and cognition.10,11 Recent molecular genetics studies have found that the polymorphism of CACNA1C and abnormal expression were significantly associated with schizophrenia. It also involves multiple single nucleotide polymorphism (SNP).12 However, studies on the association between specific genetic loci and schizophrenia have been mixed. Recent meta-analyses have shown that CACNA1C associated rs1006737 is a susceptibility gene for schizophrenia in European and East Asian populations.13,14 However, another study showed that the influence of rs1006737 genotype on susceptibility to schizophrenia was ethnically different.15,16 This feature is also reflected in other CACNA1C-related gene segments.
Because schizophrenia patients are accompanied by cognitive abnormalities during the course of disease or even before the onset,17 it is difficult to ignore the influence of CACNA1C-related genes on cognition. Previous studies have shown that CANCA1C gene rs2007044 polymorphism affects Positive and Negative Syndrome Scale (PANSS) score of schizophrenia patients.18 Therefore, we based on the CHB (Chinese Han Origin in Beijing) data from dbSNF and HapMap database, combined with the meta-analysis results of Zheng et al on schizophrenia-related CACNA1C SNP in the Han nationality, the main nationality in China,19 then selected rs1006737, rs1024582 and rs2007044 as target loci. We intended to determine the SNP of rs1006737, rs1024582 and rs2007044 in the patient group and the control group, respectively, to explore whether specific CACNA1C SNP is correlated with schizophrenia, and measuring the cognitive level of the patient group to discuss the influence of different genotypes on the cognitive function of schizophrenia patients.
Methods
Subjects
This study was a case–control study, and a total of 312 patients with SCZ and 305 healthy controls were enrolled. The study subjects were all Han Chinese and were recruited from inpatients at Pudong New Area Mental Health Center from March 2021 to March 2022, aged 20 to 65 years. All patients were in a stable phase with antipsychotic medications for more than 4 weeks, meeting the ICD-10 (International Classification of Diseases, 10th Revision) diagnostic criteria for schizophrenia, and were diagnosed by two experienced psychiatrists. Exclusion criteria included a history of other mental illness, a history of severe head injury (including any closed or open head injury that may be related to current symptoms or affect cognition), current acute psychotic episode, substance abuse, and failure to coordinate cognitive test during the period.
After excluding patients who did not meet the experimental criteria, the study was explained to the patients by the clinician and psychotherapist, including blood drawing and cognitive tests, and all questions were answered. After the subjects signed the informed consent, blood was drawn, and psychotherapist interviewed the patients to complete cognitive tests. PANSS was used to assess the severity of the illness in each schizophrenic patient.
The control group was socially recruited from the same area and matched for age and education. They were screened by experienced psychiatrists to exclude anyone with a family history of mental illness. Demographic information of patients and healthy controls is shown in Table 1. This study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Shanghai Pudong New Area Mental Health Center. All participants completed written informed consent.
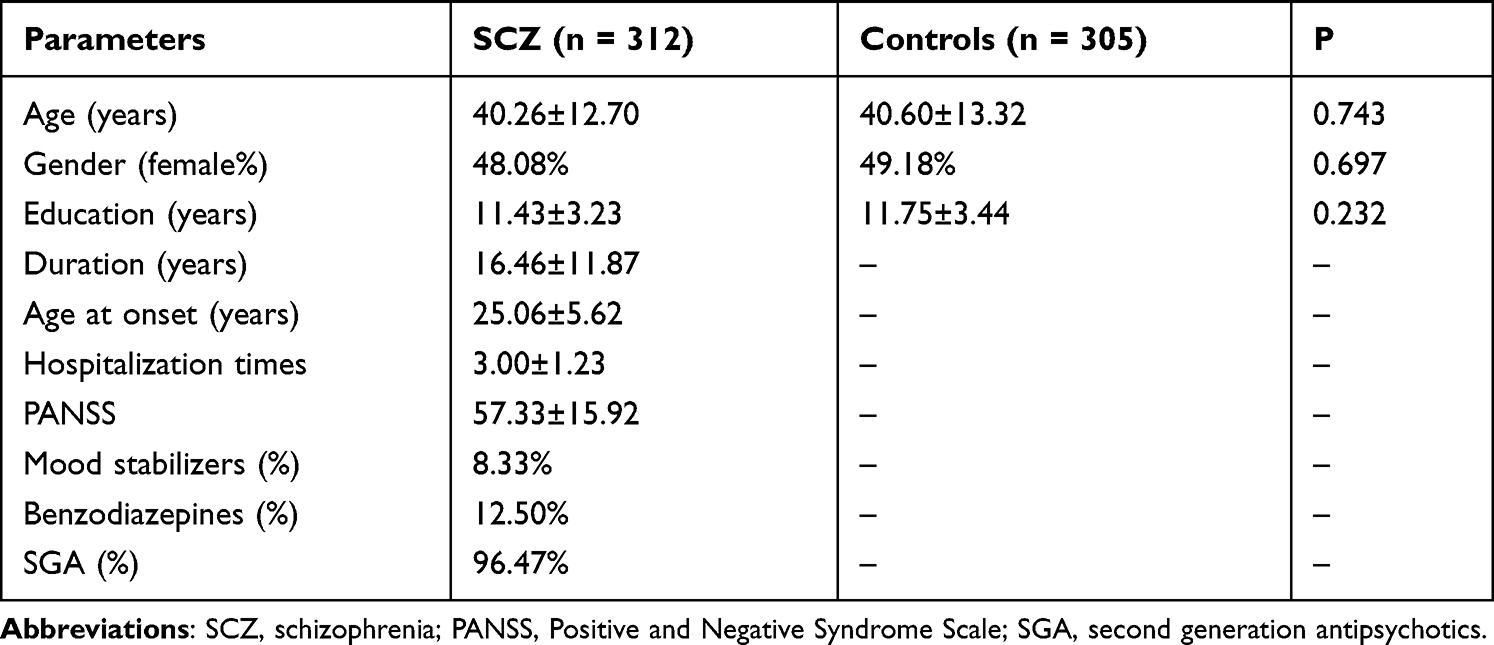 |
Table 1 Characteristics of SCZ Patients and Healthy Controls |
SNP Selection and Genotyping
Five milliliters of fasting peripheral venous blood was extracted from the patient group, and DNA was extracted according to the standard protocol of DNA separation kit (Genesky Biotechnologies, Shanghai, China). Three SNP loci rs1006737, rs1024582 and rs2007044 were selected for polymorphism detection. The target gene was amplified by PCR. DNA was extracted according to the standard protocol of DNA isolation kit (Genesky Biotechnologies, Shanghai, China). In order to ensure the accuracy of genotyping, blind quality control was used during genotyping. In addition, 5% of the samples were randomly selected for retesting and the results were 100% consistent.
Cognitive Experiment
Cognitive function was assessed in 312 SCZ patients using Repeatable Battery for the Assessment of Neuropsychological Status (RBANS). RBANS consists of vocabulary learning, story retelling, graphics copy, picture naming, line orientation, sumantio fluency, digit span, coding, vocabulary memory, vocabulary recognition, stories memory and graphics memory of 12 sub-tests, and evaluates cognitive function from 5 dimensions (Immediate Memory, Visuospatical/Constructional, Language, Attention and Delayed Memory). Finally, the original score of each test was converted into scale score according to the conversion norm.
Statistical Analysis
Hardy-Weinberg Equilibrium (HWE) testing for SNP was done using the SHEsis software (http://analysis.bio-x.cn/SHEsisMain.htm). SPSS 23.0 version and Graphpad Prism 9.0 version were used for other analyses. The measurement data was expressed as Mean ± Standard Deviation (X ± S), t-test was adopted, and the chi-square test was used for counting data. Because the number of homozygous for some risk genes was small, we considered the risk gene carriers as one group and the non-carriers as another. Pearson correlation analysis was used for correlation analysis. Significance was set at p < 0.05, two tailed.
Results
Sample Characteristics
There were no significant differences in average age, sex ratio and education level between the SCZ group and the control group (P > 0.05), as shown in Table 1.
Comparison of Genotype and Allele Distribution Frequency
The results of HWE test of genotype distribution frequency of 3 SNP loci in SCZ group and control group showed that rs1006737, rs1024582 and rs2007044 all matched HWE. All 3 SNP loci in this study were included in the subsequent analysis. Comparison of genotype and allele distribution frequency between the two groups showed that there was no significant difference in allele and genotype frequency of rs1006737, rs1024582 and rs2007044 between the SCZ group and the control group (P > 0.05), as shown in Table 2.
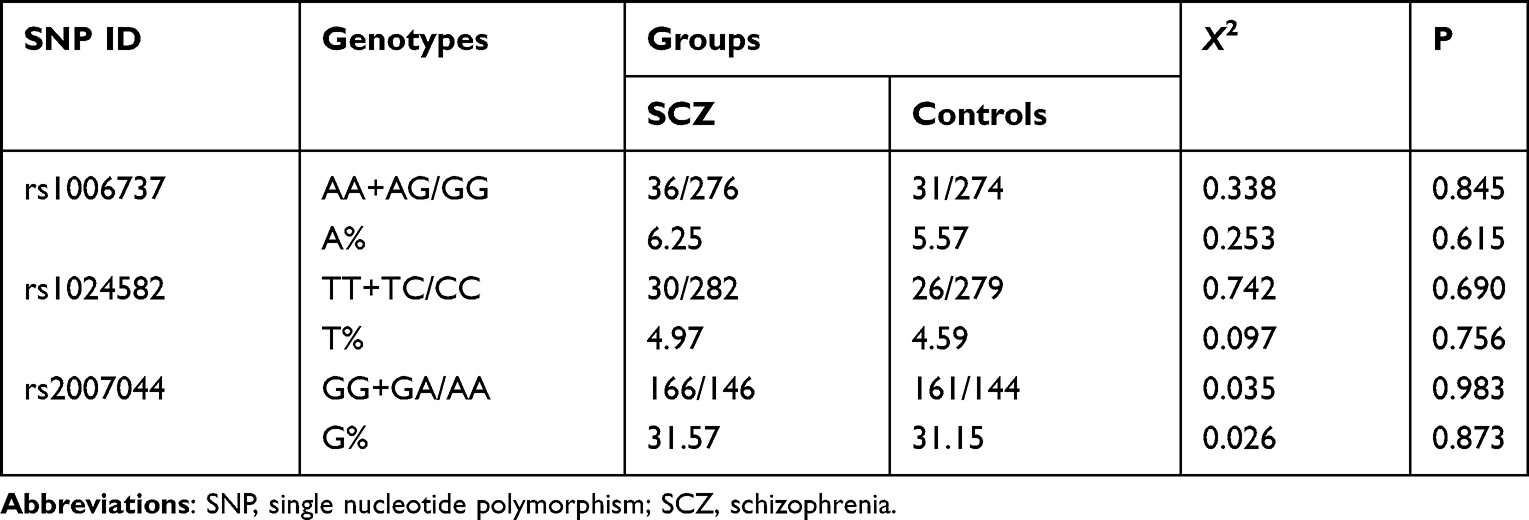 |
Table 2 Genotype and Allele Distribution Frequency in rs1006737, rs1024582, rs2007044 |
Comparison of Cognitive Function with Different Genotypes
The cognitive function in SCZ group was different among different genotypes in rs1006737, that is, the delayed memory score of “A” risk allele carriers was significantly lower that non-carriers (F=0.629, P=0.045). However, there were no significant differences in Immediate Memory, Visuospatical/Constructional, Language, Attention and total scores. Furthermore, no significant differences were found in RBANS total score and sub-item score among different genotypes in rs1024582 and rs2007044 (Table 3 and Figure 1). Pearson correlation analysis showed that RBANS total score was negatively correlated with age, disease course and PANSS score (Figure 2).
 |
Table 3 Comparison of RBANS Scores Between Risk Allele Carriers and Non-Carriers in SCZ Group |
 |
Figure 1 Comparison of RBANS scores between risk allele carriers and non-carriers in the SCZ group. *P-value <0.05. In rs1006737, the risk allele carriers had significantly lower scores than non-carriers, while in rs1024582 and rs2007044, there was no significant difference between the risk allele carriers and non-carriers.Abbreviations: RBANS, Repeatable Battery for the Assessment of Neuropsychological Status; SCZ, schizophrenia. |
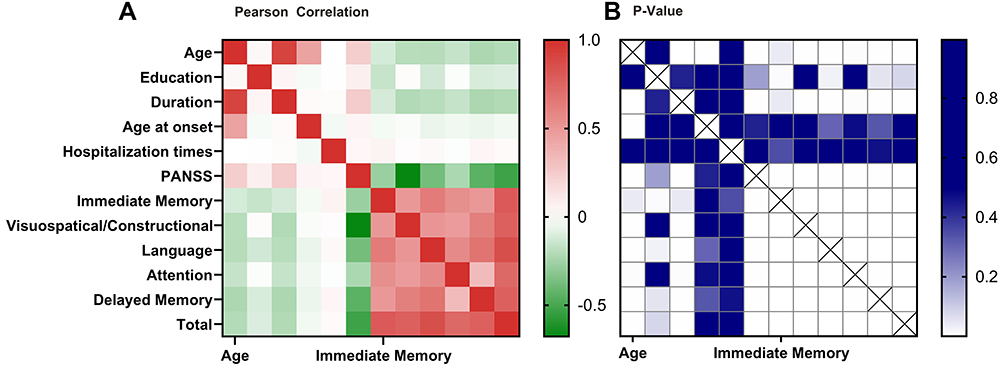 |
Figure 2 Heat map of correlation between characteristics and cognitive score in SCZ group. The RBANS total score of SCZ patients were negatively correlated with age, duration, and PANSS, but had no significant correlation with age of onset, education level, and hospitalization times.Abbreviations: SCZ, schizophrenia; PANSS, Positive and Negative Syndrome Scale; RBANS, Repeatable Battery for the Assessment of Neuropsychological Status. |
Discussion
In this study, genotypes and allele frequencies of 3 SNP loci (rs1006737, rs1024582, rs2007044) were compared between SCZ patients and healthy controls. It was found that there were no significant differences in genotypes and allele frequencies of each locus between SCZ patients and healthy controls. This result seems to suggest that the CACNA1C SNP rs1006737, rs1024582 and rs2007044 are not associated with SCZ susceptibility, which is contrary to the results of previous studies. However, by observing other similar studies, we found that the frequency of rs1006737 “A” allele in Chinese Han population ranged from 5.0% to 13.8%, and the SCZ group was 0.5 to 2 percentage points higher than the healthy control group,19–22 which was similar to this study. Besides, many previous studies with statistically significant differences had a sample size of more than 3000.19–22 Therefore, if the study continues to expand the sample size, more accurate results will be obtained.
In this study, we found that the “A” risk allele carriers of rs1006737 gene in SCZ patients had delayed memory loss, reflecting cognitive dysfunction. This is consistent with the results of previous studies. Previous studies have shown that rs1006737 risk allele “A” was associated with impaired spatial working memory in both SCZ patients and healthy people.20 Some studies on healthy people have further demonstrated the impact of risk alleles on cognition. So far, studies have shown that carriers of the “A” allele of rs1006737 are more likely to show negative cognitive bias,23 attention deficit,24 and slow response to reward.25 With the development of magnetic resonance technology, we can observe morphological changes in the brain more directly. For example, Wang’s study showed that SCZ patients carrying rs1006737 risk allele “A” had decreased gray matter volume of thalamus, surface area of isthmus of cingulate cortex, and thickness of cortex of transtemporal sulcus and superior temporal sulcus.26 Wolf’s study showed that there was also a significant difference in the volume of the left and right amygdala in this group.27 Mallas’s study showed that diffusion tensor imaging (DTI) of such patients showed decreased white matter integrity in several parts of the brain.28 Functional magnetic resonance imaging (FMRI) experiments on first-degree relatives of SCZ patients and healthy people also found some hemodynamic abnormalities in the brain.29–31 Unfortunately, such studies differed greatly in the location of abnormal regions, so more accurate studies could not be carried out. Researchers had targeted the gene by tracking the messenger RNA, but found that the “A” allele carriers had abnormal expression of CACNA1C messenger RNA in several different brain regions. Later, other researchers attached importance to gender differences and finally found that such cognitive and brain functional activity abnormalities accompanied by risk alleles have slight gender differences, that is, anxiety is more common in males, while hostility is more common in females.23,32 In general, carriers of risk alleles exhibit a different neurological phenotype from non-carriers at a macro level, which is the key to such studies in clinical psychiatry today.
Correlation analysis showed that RBANS scores of SCZ patients were negatively correlated with age, course of disease, and PANSS, but had no significant correlation with age of onset, education level, and hospitalization times. However, previous studies generally believed that education level was positively proportional to patients’ cognition.33 After further study of the experiment in the population, we got the answer. This study was conducted in Shanghai, where SCZ patients ranged in age from 20 to 65 years. In recent decades, Shanghai has witnessed rapid economic development, and people have increasingly attached importance to education. Therefore, for young patients and elderly patients with the same education years, their actual educational level may be far apart. So using years of schooling as a parameter is not so accurate.
Due to the special significance of calcium channel in schizophrenia, it is not difficult to imagine whether calcium channel antagonists (CCB) can be used in the treatment of schizophrenia. In fact, as early as the 1980s, some clinicians tried to use CCB as an adjunctive treatment for patients with refractory schizophrenia. In randomized controlled trials, CCB was found to enhance learning and memory in schizophrenics with tardive dyskinesia.34 Dyke’s team found that the group treated with antipsychotic drugs in combination with CCB had significantly better Clinical Global Impression (CGI) scores at multiple time points than the group treated with normal therapy.35 However, a study on the Korean schizophrenia population found that in the same group of hospitalized patients, the CACNA1C SNP rs723672 and rs1034936 were significantly correlated with the improvement of PANSS positive score, which is suggested that different genotypes may influence antipsychotic effects.36 Other studies showed that the mechanism of action of some atypical antipsychotics might be related to calcium channels.37 For instance, papperidone could effectively prevent calcium influx by inhibiting voltage-gated calcium channels, thus effectively delay nerve cell death.38 In the latest study, the researchers used mice to simulate perinatal fetal central nervous system development and showed that the failure of LTCC in prematurity neurons might lead to errors in nerve growth and cortical migration. Interestingly, a range of symptoms caused by such errors could be revised by postnatal correction of LTCC signal aberrations. This study suggested that CACNA1C, as an important component of LTCC, might be a perinatal therapeutic target for neurodevelopmentally related psychiatric disorder.39
This study also has some limitations. On the one hand, due to the limitations of experimental conditions, we failed to conduct RBANS in healthy controls, which to some extent affected the persuasion of the experiment. If cognitive abnormalities were also found in carriers of the rs1006737 “A” allele in healthy controls, it would be strong evidence that CACNA1C gene polymorphisms affect cognitive function. On the other hand, there are also differences in CACNA1C-related gene polymorphisms in other psychiatric diseases, such as rs1006737 polymorphism is associated with bipolar disorder,40 rs1034936 polymorphism is associated with alcohol dependence and cocaine abuse.37 Poor specificity is a common flaw in studies of SNP of mental disease.
Conclusions
There is no significant difference in allele and genotype frequency of CANCA1C Gene rs1006737, rs1024582 and rs2007044 between the schizophrenia patients and healthy controls. The cognitive function of schizophrenia patients is correlated with the rs1006737, and the delayed memory of “A” allele carriers is significantly reduced.
Abbreviations
CACNA1C, L-type calcium channel α1C subunit; SCZ, schizophrenia; SNP, Single nucleotide polymorphism; RBANS, Repeatable Battery for the Assessment of Neuropsychological Status; YLD, year lived with disability; LTCC, L-type voltage-gated calcium channels; CHB, Chinese Han Origin in Beijing; ICD-10, international Classification of Diseases, 10th Revision; PANSS, Positive and Negative Syndrome Scale; HWE, Hardy-Weinberg Equilibrium; SGA, second-generation antipsychotics; DTI, diffusion tensor imaging; FMRI, Functional magnetic resonance imaging; CCB, calcium channel antagonists.
Ethics Approval and Informed Consent
The study was approved by the Ethics Committee of Shanghai Pudong New Area Mental Health Center (reference number: PDJWLL2020012)
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the Special Fund for Livelihood Research (Medical and Health Care) of the Science and Technology Development Fund of Pudong New Area 2020 (PKJ2020-Y33).
Disclosure
The authors report no conflicts of interest in this work.
References
1. McGrath J, Saha S, Chant D, et al. Schizophrenia: a concise overview of incidence, prevalence, and mortality. Epidemiol Rev. 2008;30:67–76. doi:10.1093/epirev/mxn001
2. Howes OD, Murray RM. Schizophrenia: an integrated sociodevelopmental-cogniti- ve model. Lancet. 2014;10(9929):1677–1687. doi:10.1016/S0140-6736(13)62036-X
3. Olfson M, Stroup TS, Huang C, et al. Suicide risk in medicare patients with schizophrenia across the life span. JAMA Psychiatry. 2021;78(8):876–885. doi:10.1001/jamapsychiatry.2021.0841
4. Charlson FJ, Ferrari AJ, Santomauro DF, et al. Global epidemiology and burden of schizophrenia: findings from the global burden of disease study 2016. Schizophr Bull. 2018;44(6):1195–1203. doi:10.1093/schbul/sby058
5. GBD 2019 Mental Disorders Collaborators. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990–2019: a systematic analysis from the global burden of disease study 2019. Lancet Psychiatry. 2022;9(2):137–150. doi:10.1016/S2215-0366(21)00395-3
6. Jauhar S, Johnstone M, McKenna PJ. Schizophrenia. Lancet. 2022;399(10323):473–486. doi:10.1016/S0140-6736(21)01730-X
7. Schizophrenia Psychiatric Genome-Wide Association Study (GWAS) Consortium. Genome-wide association study identifies five new Schizophrenia loci. Nat Genet. 2011;43(10):969–976. doi:10.1038/ng.940
8. De Jesús-Cortés H, Rajadhyaksha AM, Pieper AA. Cacna1c: protecting young hippocampal neurons in the adult brain. Neurogenesis. 2016;3(1):e1231160. doi:10.1080/23262133.2016.1231160
9. Jiang M, Swann JW. A role for L-type calcium channels in the maturation of parvalbumin-containing hippocampal interneurons. Neuroscience. 2005;135(3):839–850. doi:10.1016/j.neuroscience.2005.06.073
10. Bigos KL, Mattay VS, Callicott JH, et al. Genetic variation in CACNA1C affects brain circuitries related to mental illness. Arch Gen Psychiatry. 2010;67(9):939–945. doi:10.1001/archgenpsychiatry.2010.96
11. Bhat S, Dao DT, Terrillion CE, et al. CACNA1C (Cav1.2) in the pathophysiology of psychiatric disease. Prog Neurobiol. 2012;99(1):1–14. doi:10.1016/j.pneurobio.2012.06.001
12. Takahashi S, Glatt SJ, Uchiyama M, et al. Meta-analysis of data from the psychiatric genomics consortium and additional samples supports association of CACNA1C with risk for schizophrenia. Schizophr Res. 2015;168(1–2):429–433. doi:10.1016/j.schres.2015.07.033
13. Zhu D, Yin J, Liang C, et al. CACNA1C (rs1006737) may be a susceptibility gene for schizophrenia: an updated meta-analysis. Brain Behav. 2019;9(6):e01292. doi:10.1002/brb3.1292
14. Jiang H, Qiao F, Li Z, et al. Evaluating the association between CACNA1C rs1006737 and schizophrenia risk: a meta-analysis. Asia Pac Psychiatry. 2015;7(3):260–267. doi:10.1111/appy.12173
15. Liu YP, Wu X, Xia X, et al. The genome-wide supported CACNA1C gene polymorphisms and the risk of schizophrenia: an updated meta-analysis. BMC Med Genet. 2020;21(2):159. doi:10.1186/s12881-020-01084-0
16. Yang L, Zhou C, Fang L, et al. Meta-analysis of l-type calcium channel α1C gene polymorphism and schizophrenia. J China Med Univ. 2014;39(6):858–863. doi:10.13406/j.cnki.cyxb.000119
17. Kowalec K, Lu Y, Sariaslan A, et al. Increased schizophrenia family history burden and reduced premorbid IQ in treatment-resistant schizophrenia: a Swedish national register and genomic study. Mol Psychiatry. 2021;26(8):4487–4495. doi:10.1038/s41380-019-0575-1
18. Zheng F, Cui Y, Yan H, et al. The effects of a genome-wide supported variant in the CACNA1C gene on cortical morphology in schizophrenia patients and healthy subjects. Sci Rep. 2016;09–29(6):34298. doi:10.1038/srep34298
19. Zheng F, Zhang Y, Xie W, et al. Further evidence for genetic association of CACNA1C and schizophrenia: new risk loci in a Han Chinese population and a meta-analysis. Schizophr Res. 2014;52(1):105–110. doi:10.1016/j.schres.2013.12.003
20. Zhang Q, Shen Q, Xu Z, et al. The effects of CACNA1C gene polymorphism on spatial working memory in both healthy controls and patients with schizophrenia or bipolar disorder. Neuropsychopharmacology. 2012;37(3):677–684. doi:10.1038/npp.2011.242
21. He K, An Z, Wang Q, et al. CACNA1C, schizophrenia and major depressive disorder in the Han Chinese population. Br J Psychiatry. 2014;204(1):36–39. doi:10.1192/bjp.bp.113.126979
22. Guan F, Zhang B, Yan T, et al. MIR137 gene and target gene CACNA1C of miR-137 contribute to schizophrenia susceptibility in Han Chinese. Schizophr Res. 2013;152(1):97–104. doi:10.1016/j.schres.2013.11.004
23. Pasparakis E, Koiliari E, Zouraraki C, et al. The effects of the CACNA1C rs1006737 A/G on affective startle modulation in healthy males. Eur Psychiatry. 2015;30(4):492–498. doi:10.1016/j.eurpsy.2015.03.004
24. Meller T, Schmitt S, Stein F, et al. Associations of schizophrenia risk genes ZNF804A and CACNA1C with schizotypy and modulation of attention in healthy subjects. Schizophr Res. 2019;208:67–75. doi:10.1016/j.schres.2019.04.018
25. Lancaster TM, Heerey EA, Mantripragada K, et al. CACNA1C risk variant affects reward responsiveness in healthy individuals. Transl Psychiatry. 2014;4:e461. doi:10.1038/tp.2014.100
26. Wang Z, Chen W, Cao Y, et al. An independent, replicable, functional and significant risk variant block at intron 3 of CACNA1C for schizophrenia. Aust N Z J Psychiatry. 2022;56(4):385–397. doi:10.1177/00048674211009595
27. Wolf C, Mohr H, Schneider-Axmann T, et al. CACNA1C genotype explains interindividual differences in amygdala volume among patients with schizophrenia. Eur Arch Psychiatry Clin Neurosci. 2014;264(2):93–102. doi:10.1007/s00406-013-0427-y
28. Mallas E, Carletti F, Chaddock CA, et al. The impact of CACNA1C gene, and its epistasis with ZNF804A, on white matter microstructure in health, schizophrenia and bipolar disorder1. Genes Brain Behav. 2017;16(4):479–488. doi:10.1111/gbb.12355
29. Erk S, Meyer-Lindenberg A, Schmierer P, et al. Hippocampal and frontolimbic function as intermediate phenotype for psychosis: evidence from healthy relatives and a common risk variant in CACNA1C. Biol Psychiatry. 2014;76(6):466–475. doi:10.1016/j.biopsych.2013.11.025
30. Paulus FM, Bedenbender J, Krach S, et al. Association of rs1006737 in CACNA1C with alterations in prefrontal activation and fronto-hippocampal connectivity. Hum Brain Mapp. 2014;35(4):1190–1200. doi:10.1002/hbm.22244
31. Lancaster TM, Foley S, Tansey KE, et al. CACNA1C risk variant is associated with increased amygdala volume. Eur Arch Psychiatry Clin Neurosci. 2016;266(3):269–275. doi:10.1007/s00406-015-0609-x
32. Takeuchi H, Tomita H, Taki Y, et al. A common CACNA1C gene risk variant has sex-dependent effects on behavioral traits and brain functional activity. Cereb Cortex. 2019;29(8):3211–3219. doi:10.1093/cercor/bhy189
33. Merinder LB. Patient education in schizophrenia: a review. Acta Psychiatr Scand. 2000;102(2):98–106. doi:10.1034/j.1600-0447.2000.102002098.x
34. Schwartz BL, Fay MM, Kendrick K, et al. Effects of nifedipine, a calcium channel antagonist, on cognitive function in schizophrenic patients with tardive dyskinesia. Clin Neuropharmacol. 1997;20(4):364–370. doi:10.1097/00002826-199708000-00009
35. Van DP, Thomas KL. Concomitant calcium channel blocker and antipsychotic therapy in patients with schizophrenia: efficacy analysis of the CATIE-Sz Phase 1 data. Ann Clin Psychiatry. 2018;30(1):6–16.
36. Porcelli S, Lee SJ, Han C, et al. CACNA1C gene and schizophrenia: a case–control and pharmacogenetic study. Psychiatr Genet. 2015;25(4):163–167. doi:10.1097/YPG.0000000000000092
37. Mosheva M, Serretti A, Stukalin Y, et al. Association between CANCA1C Gene rs1034936 polymorphism and alcohol dependence in bipolar disorder. J Affect Disord. 2020;261:181–186. doi:10.1016/j.jad.2019.10.015
38. Zhu D, Zhang J, Wu J, et al. Paliperidone Protects SH-SY5Y cells against MK- 801-induced neuronal damage through inhibition of Ca(2+) influx and regulation of SIRT1/miR-134 signal pathway. Mol Neurobiol. 2016;53(4):2498–2509. doi:10.1007/s12035-015-9217-z
39. Kamijo S, Ishii Y, Horigane SI, et al. A critical neurodevelopmental role for L-type voltage-gated calcium channels in neurite extension and radial migration. J Neurosci. 2018;38(24):5551–5566. doi:10.1523/JNEUROSCI.2357-17.2018
40. Khalid M, Driessen TM, Lee JS, et al. Association of CACNA1C with bipolar disorder among the Pakistani population. Gene. 2018;664:119–126. doi:10.1016/j.gene.2018.04.061
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.