")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Burnout Syndrome Among Critical Care Health Providers in Saudi Arabia
Authors Alshurtan KS, Aldhaifi SY , Alshammari KA, Alodayli OM , Alqahtani KF, Aldhaifi SY
Received 28 November 2023
Accepted for publication 20 February 2024
Published 27 February 2024 Volume 2024:17 Pages 843—854
DOI https://doi.org/10.2147/JMDH.S452294
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Kareemah Salem Alshurtan, Saad Yousef Aldhaifi, Khalid Abdulkarim Alshammari, Othman Mohammed Alodayli, Khalid Falah Alqahtani, Sarah Yousef Aldhaifi
Department of Internal Medicine and Adult Critical Care, College of Medicine, University of Ha’il, Ha’il, Saudi Arabia
Correspondence: Kareemah Salem Alshurtan, Department of Internal Medicine and Adult Critical Care, College of Medicine, University of Ha’il, Ha’il, Saudi Arabia, Email [email protected]
Background: Burnout Syndrome constitutes a critical concern in healthcare, particularly among practitioners operating in high-stress, critical care settings. Understanding the multifaceted factors contributing to burnout in this context is pivotal for devising effective interventions and promoting the well-being of critical care professionals.
Objective: To investigate the prevalence, contributing factors, and potential interventions related to Burnout Syndrome among critical care health providers in Saudi Arabia.
Methods: A cross-sectional research design was employed, gathering data from a sample of critical care health providers, including medical practitioners. A self-administered structured electronic questionnaire was used, incorporating the Maslach Burnout Inventory (MBI) with its three subscales: emotional exhaustion, depersonalization, and personal accomplishment. The target population was male and female critical care health providers over 18 years age, most participants lies between 25 years to 34 years.
Results: Statistical analysis shows significant disparities in response distribution (p< 0.05), highlighting the importance of understanding encounters with emotional exhaustion, personal accomplishment, and depersonalization. The Durbin-Watson statistic indicated limited autocorrelation, and collinearity tolerance values suggested nominal intercorrelations among predictors. A significant positive correlation was found between the “Depersonalization Loss of Empathy MBI” factor and the outcome variables, indicating complex relationships between emotional exhaustion, personal accomplishment, and depersonalization.
Conclusion: The study highlights the multifaceted nature of burnout, revealing intricate relationships between emotional exhaustion, personal accomplishment, and depersonalization. These findings collectively form an important foundation for future guidelines and interventions to enhance the well-being of healthcare professionals.
Keywords: maslach burnout inventory, MBI, emotional exhaustion, depersonalization, personal accomplishment, high-stress environments, healthcare professionals, work-related stress, occupational burnout
A Letter to the Editor has been published for this article.
Introduction
Burnout syndrome is a psychological syndrome arising from a continued response to chronic interpersonal stressors.1 A generic description of burnout defines it as physical and mental exhaustion related to caregiving activities or work.2 Over the preceding decade, there has been a discernible and continuous recognition of burnout syndrome as a substantive concern afflicting individuals within healthcare professions.3 Characterized by its multifaceted nature, burnout syndrome is commonly delineated by heightened emotional exhaustion, elevated depersonalization, and a diminished sense of personal accomplishment.4 Emotional exhaustion is equivalently characterized as experiencing profound weariness, a dissipation of energy reserves, a state of depletion, and perceptible fatigue. Depersonalization manifests as adverse or inappropriate attitudes toward patients, coupled with irritability and social withdrawal. Diminished personal accomplishment entails reduced efficacy and an impaired ability to manage challenges effectively.5
Work-related stress among healthcare professionals has become a severe health problem for workers and the world economy. Meanwhile, the syndrome among both physicians in practice and in training has reached epidemic levels, with a prevalence near or exceeding 50%.2 Moreover, burnout poses an emerging critical issue confronting specialists and trainees in all disciplines. Physicians experiencing burnout show associations with severe adverse patient outcomes, characterized by elevated rates of medical errors and diminished quality of care.6 Furthermore, burnout correlates with negative consequences for physicians, such as substance abuse and suicide.7
The challenges of working during the COVID-19 pandemic have significantly impacted the mental health of healthcare workers, particularly frontline nurses managing COVID-19 patients, who have reported heightened levels of psychological distress, fear, and anxiety. Notably, participants lacking COVID-19 management training experienced more severe psychological difficulties. These findings underline the need for targeted training for frontline nurses to address specific challenges during variant outbreaks.8 Additionally, the nursing profession became more stressful and demanding because of the high patient load and job intensity, as well as the rapid protocol and management changes. Due to job demand and resource limits, including limited personal protective gear and disinfection supplies, stress and health decline worsen to address life-threatening conditions.9
Also, it has a significant impact on nursing undergraduates’ mental health and well-being, resulting in increased fatigue, anxiety, and depression. The transition to virtual learning, home or hostel confinement, and decreased physical activity have exacerbated these psychological issues. Lockdown-related fatigue was discovered to be widespread among nursing undergraduates, with junior students, those who tested positive, and those hospitalized during the pandemic experiencing higher levels of exhaustion. The study emphasizes the importance of individual resilience and structured coping techniques in reducing the pandemic’s detrimental impact on nursing students’ mental health. It advises that nursing educators prioritize ways to reduce pandemic-induced weariness and increase students’ personal resilience. Resilience-promoting practices and positive coping mechanisms can improve nursing students’ mental health and well-being during stressful circumstances.10
Several studies have been conducted to examine burnout among healthcare providers; Al-Youbi and Jan,11 conducted a pioneering assessment of Burnout Syndrome among healthcare providers in Saudi Arabia and concluded that at least one-third of practicing pediatricians experience Burnout Syndrome. Furthermore, Alwashmi and Alkhamees,12 assessed burnout, depression, anxiety, and stress among psychiatrists during the ongoing COVID-19 pandemic crisis in Saudi Arabia and demonstrated that burnout exists among more than two-thirds of practising physiatrists in physical medicine and rehabilitation (PM&R), and this phenomenon did not demonstrate a statistically significant impact on stress, anxiety, or depression. Moreover, in 2020, there was a noteworthy incidence of burnout within the cohort of physicians practising within primary health care centers (PHCCs). Furthermore, an observable correlation between elevated levels of burnout and specific risk factors was discerned.13
Additionally, the Baghdadi literature review investigated the frequency of burnout, job satisfaction, and ethics within hospital settings in Makkah, Saudi Arabia, among physicians with varied levels of experience and seniority. The findings suggested that burnout and career-choice regret manifest as widespread phenomena among physicians.14 Concurrently, an investigation has also been undertaken to ascertain the extent of burnout within the cohort of healthcare workers (HCWs) fulfilling their duties in Saudi Arabia amid the difficulties of the COVID-19 pandemic. This study endeavored to elucidate the nuanced interplay of individual and occupational determinants concomitant with the phenomenon of burnout in this specific demographic. The analysis has revealed that several salient variables exhibit a statistically significant correlation with burnout, including but not limited to chronological age, professional designation, cumulative years of experience, augmented temporal engagement in professional responsibilities during the pandemic, mean daily duration of sleep, direct contact with COVID-19-afflicted patients, frequency of COVID-19 screening, and perceived sense of obligation to manage cases involving COVID-19 patients.15
Moreover, researchers assessed burnout prevalence among Saudi Plastic Surgery Residency Program residents. The findings revealed that approximately 50% of the respondents had signs of professional burnout.16 Furthermore, Burnout Syndrome is high among middle-grade physicians at their medical facility in Saudi Arabia.17 Concurrently, a series of empirical investigations carried out within the confines of Saudi Arabia from 2010 to 2020, targeting the cohort of nursing professionals gainfully employed therein, collectively ascertained that the incidence of burnout manifested a discernibly moderate to elevated spectrum of prevalence within the demographic mentioned above.18–21 Nevertheless, an insufficiency of comprehensive data on the incidence of severe burnout among alternate healthcare providers such as physiotherapists and respiratory or speech therapists was evident in the literature.22 Nevertheless, an insufficiency of comprehensive data on the incidence of severe burnout among alternate healthcare providers such as physiotherapists and respiratory or speech therapists was evident in the literature.22
Despite the extensive body of research focused on gauging the frequency of burnout within the cohort of healthcare practitioners, more inquiries need to elucidate prescriptive measures. The current investigation endeavors to appraise the incidence of burnout among a subset of healthcare providers specializing in critical care, namely emergency physicians, anesthesiologists, and intensivists, within the context of Saudi Arabia. Moreover, the study seeks to undertake an evaluative inquiry into recommendations tendered by these physicians. The overarching objective of this inquiry is to contribute to delineating innovative directives aimed at mitigating burnout and alleviating work-related stress, thereby fostering enhanced occupational well-being within this cadre.
The rationale behind investigating burnout syndrome among critical care health providers, including emergency physicians, anesthesiologists, intensivists and nurses in Saudi Arabia lies in its potential impact on patient care, healthcare systems, and the overall well-being of healthcare professionals. Burnout affects the mental health and job satisfaction of healthcare providers and can lead to reduced productivity, increased medical errors, and compromised patient safety. Given the critical nature of their work, any decline in the well-being of these providers can have severe consequences on patient outcomes and quality of care. Additionally, understanding the factors contributing to burnout among critical care health providers in Saudi Arabia is essential for developing effective intervention strategies.
Cultural norms, work-related stressors, organizational support, and individual coping mechanisms may differ across countries and healthcare systems. Tailored and targeted interventions can be designed to alleviate burnout and improve the overall work environment for critical care providers by pinpointing the specific factors that contribute to burnout in this context. Thus, comprehensively investigate the prevalence, contributing factors, and potential interventions related to Burnout Syndrome among critical care health providers in Saudi Arabia.
Materials and Methods
Study Design
A cross-sectional research design was employed to gather data from critical care health providers in Saudi Arabia. The cross-sectional approach allows for data collection at a single point in time, enabling an analysis of the prevalence of burnout and associated factors. Where IRB were taken from all the participants; this study followed the Helsinki Declaration of 1975 and Ha’il University’s human experimentation committee’s ethical guidelines. We are pleased to announce that the University of Ha’il College of Medicine’s Committee of Scientific Research and Conferences (H-2022-384) has approved the study “Burnout Syndrome among Critical Care Health Providers in Saudi Arabia”. The research aims were explained to participants, who consented to the study.
Study Population
The target population comprises males and females above 18 years, critical care health providers, including physicians, nurses, Emergency physicians, anesthesiologists, intensivists, and allied healthcare professionals working in various critical care settings across Saudi Arabia. A stratified random sampling technique was used to ensure representation from different healthcare facilities.
Sample Collection
Data was collected through a self-administrated structured electronic questionnaire.23 The questionnaire includes demographic information and items related to work conditions, workload, support systems, and coping strategies.
Sample Collection and Processing
A validated electronic questionnaire, which had been employed in prior investigations, in conjunction with a demographic data questionnaire, was utilized for data collection. The self-administered electronic questionnaire comprises 22 items, each rated on a Likert-type scale with five response options. The instrument incorporates the Maslach Burnout Inventory (MBI).24 encompassing three distinct sub-scales—namely, emotional exhaustion, depersonalization, and personal accomplishment—to gauge the propensity for experiencing burnout. The participant sample encompassed 1000 individuals, determined by applying the Raosoft sample size calculator.25 This calculation was based on the total population, with a confidence level of 95% and a margin of error of 5%.
Item 1: Psychiatric psychological counselling; Item 2: Mandatory vacation; Item 3: Off-duty activities; Item 4: Temporary transfer to low-load work; Item 5: Decreased number of patients; Item 6: Increased overtime salary; Item 7: Decreased number of monthly duties; Item 8: Decreased number of daily duty hours; Item 9: Implementation of ward and employee of the month systems; Item 10: Periodic burnout assessment by a specialist; Item 11: Training programs directed towards increasing ability.
Statistical Analysis
Descriptive statistics was used to characterize the demographic and professional profiles of the participants. The prevalence of burnout was calculated based on the MBI scores. Inferential statistics, such as chi-square tests and regression analysis, explored relationships between burnout and various factors, including work environment, workload, and support systems. The statistical analysis was processed using the Statistical Package for Social Sciences (SPSS) software version 23 (SPSS Inc., Chicago, IL, USA).
Results
Demographic Characteristics
The data depicts a gender distribution of 251 males (49.5%) and 255 females (50.4%), with a dominant age group of 25–34 years (407 individuals, 80.4%). Marital status shows 199 unmarried (39.3%), 272 married (53.8%), 14 divorced (2.8%), and 18 separated (3.6%) respondents. Saudi nationals account for 411 (81.2%), while non-Saudis comprise 95 (18.8%) of the sample. Occupations include nurses (203, 40.1%), consultants (43, 8.5%), residents (142, 28.1%), and specialists (89, 17.6%). The dataset represents different departments, primarily the Intensive care units (ICU) (117, 23.1%) and the ED (337, 66.6%). Monthly income ranges include less than 5000 SR (49, 9.7%), 5000–10,000 SR (164, 32.4%), 10,000–15,000 SR (106, 20.9%), 15,000–20,000 SR (106, 20.9%), and more than 20,000 SR (81, 16%). Place of residency encompasses multiple provinces, with Riyadh (151, 29.8%) and Hail (69, 13.6%) being the most prevalent. Respondents’ years in service span less than 2 years (178, 35.2%), 2–5 years (185, 36.6%), 5–10 years (84, 16.6%), and more than 10 years (59, 11.7%). Duty hours include less than 8 hours (36, 7.1%), 8 hours shifts (291, 57.5%), 12 hours shifts (131, 25.9%), and 8–16 hours shifts (42, 8.3%). Duty days per month consist of less than 10 days (52, 10.3%), 10–20 days (270, 53.4%), and more than 20 days (184, 36.4%). Back-to-back off days per week exhibit varying frequencies, with 2 days off (202, 39.9%) being the most common (Figure 1A–E).
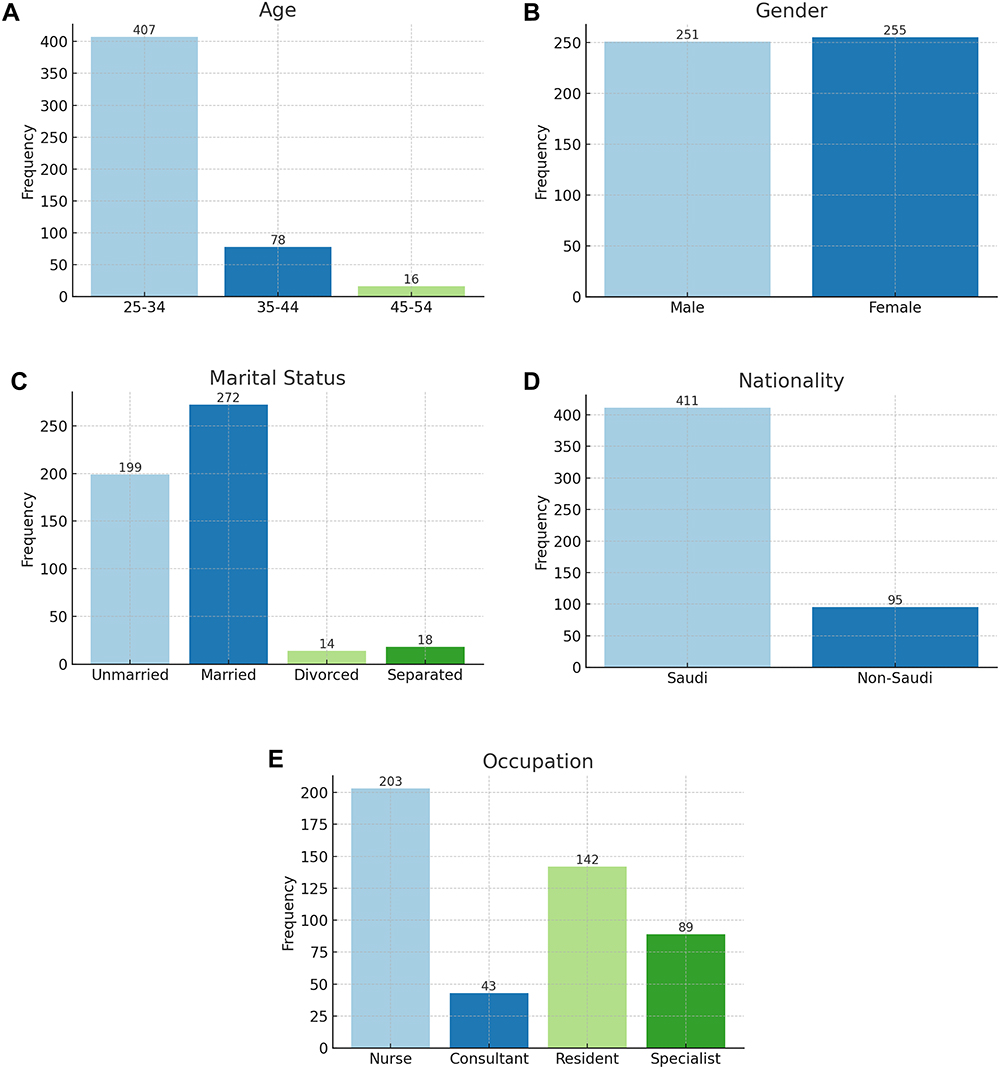 |
Figure 1 Demographic characteristics; where; (A) Age. (B): Gender. (C) Martial status. (D) Nationality. (E) Occupation. |
Burnout Response
The survey provided results on the prevalence of emotional exhaustion, personal accomplishment, and depersonalization (loss of empathy) among respondents (Table 1). In the survey, a Likert scale was utilized to assess the frequency of these experiences, ranging from “Never” to “Every day”. A specific item/question related to emotional exhaustion, personal accomplishment, or depersonalization, and the different response options and their respective counts (n) and % were presented. Notably, emotional exhaustion was the most frequently reported at higher frequencies (eg, “A few times a month” to “Every day”) as evidenced by higher counts and percentages for corresponding items.
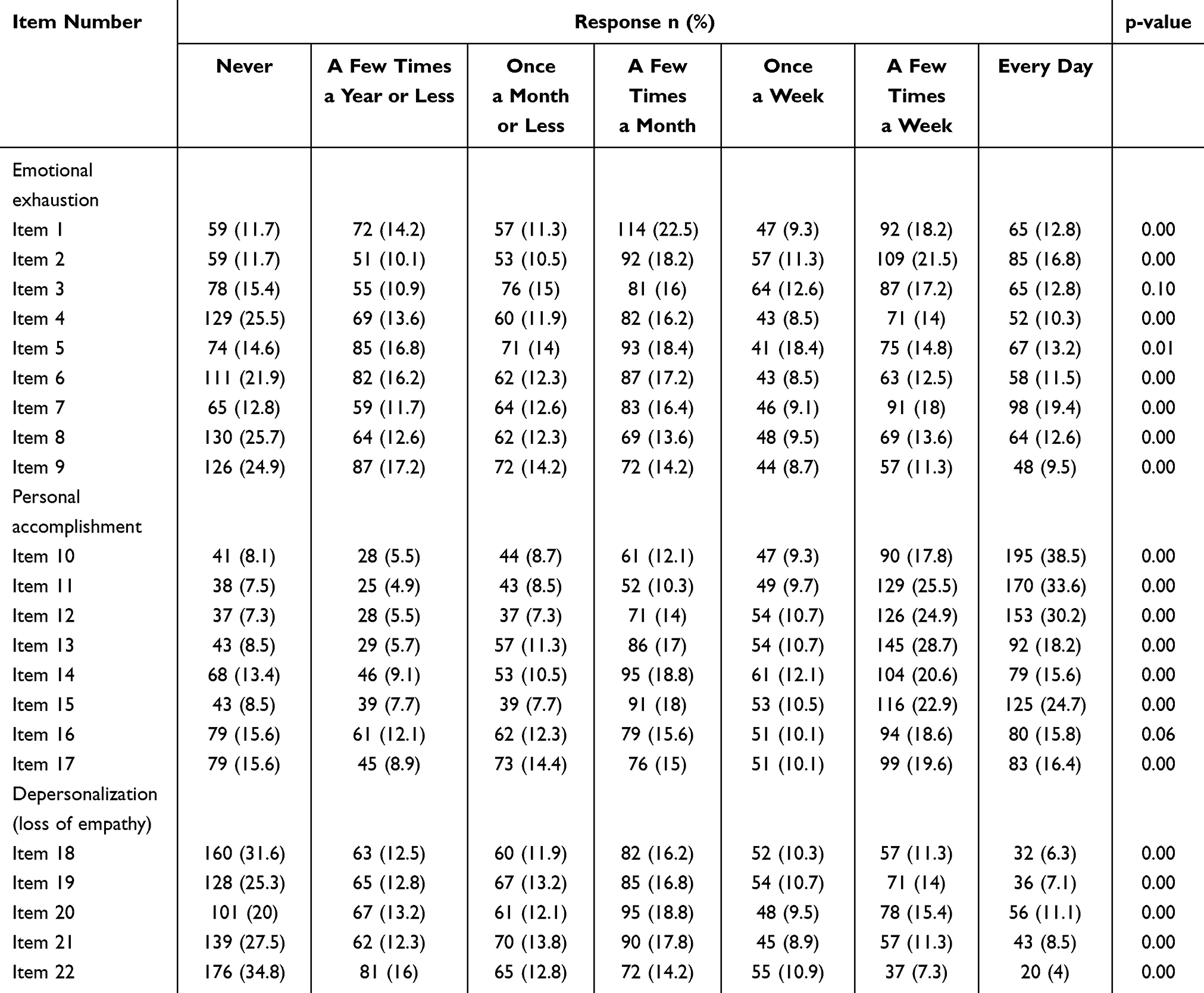 |
Table 1 Questions Related to Burnout |
Conversely, personal accomplishment tends to be reported more frequently at the positive end of the scale (eg, “Every day”), with the highest counts and percentages in those categories. Depersonalization exhibits similar patterns to emotional exhaustion, with notable prevalence reported at higher response frequencies. The low p-values (p<0.05) suggest that the observed response distribution differences are statistically significant, underscoring the importance of the findings in understanding the respondents’ experiences of emotional exhaustion, personal accomplishment, and depersonalization.
Model Summary
Statistical results from a regression analysis presented in (Table 2). The model’s goodness of fit was assessed using several metrics: the coefficient of determination (R) indicates the proportion of the variance in the dependent variable explained by the independent variables, with R values of 0.420 and 0.116. The adjusted R2 accounts for the number of predictors in the model, yielding values of 0.173 and 0.009, respectively, for both predictors (Depersonalization Loss of Empathy, Personal Accomplishment MBI Factor and Emotional Exhaustion MBI Factor, Depersonalization Loss of Empathy). The SE measures the average distance between the observed and predicted values, with values of 1.45 and 1.44 in the table The Durbin-Watson statistic detects the presence of autocorrelation in the residuals (unexplained variation), with values close to 2 suggesting no significant autocorrelation; the values of 1.86 and 1.83 indicate relatively low levels of autocorrelation. These results collectively provide insights into the model’s explanatory power, precision of predictions, and potential issues related to the independence of residuals.
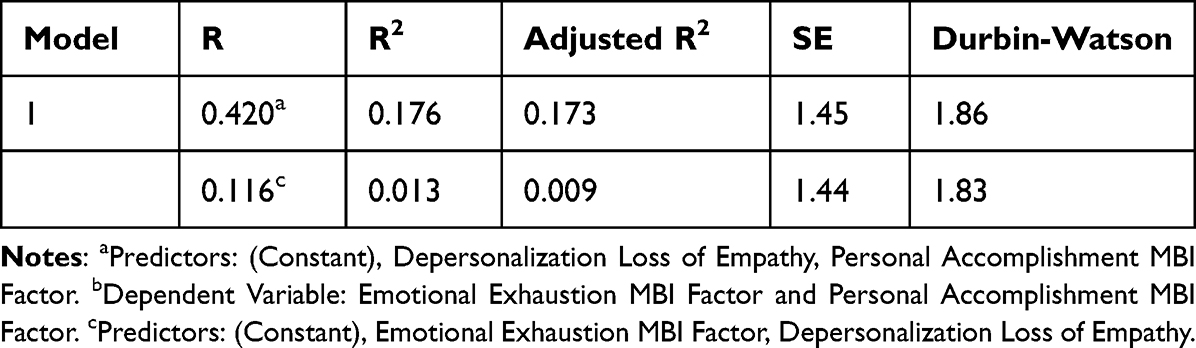 |
Table 2 Model Summary b |
Regression Analysis
To better elucidate the relationships between burnout-related factors, as measured by the MBI scale, and the outcome variables, the presented table exhibits the results of multiple linear regression analyses (Model 1a) examining the relationships between burnout-related factors (as measured by the MBI scale) and outcome variables. In Model 1, the unstandardized and standardized coefficients (β) along with SE are provided for the “Personal Accomplishment MBI factor” and “Depersonalization Loss of Empathy MBI factor” predictors. The t values indicate the significance of the coefficients, with higher t values suggesting stronger relationships. The sig. values indicate the statistical significance of the coefficients, where lower values (p < 0.05) indicate significant relationships. Collinearity tolerance values provide information about the multi-collinearity among predictors; values closer to 1 indicate low multicollinearity. Model 1b presents a similar analysis, emphasizing the predictors “Depersonalization Loss of Empathy MBI factor” and “Emotional Exhaustion MBI factor. Table 3 offers insights into how the different factors relate to the outcome variables, their significance, and potential multicollinearity issues. The presented results suggest that the Depersonalization Loss of Empathy MBI” factor appears to have a substantial positive relationship with the outcome variables (emotional exhaustion and personal accomplishment) in the model.
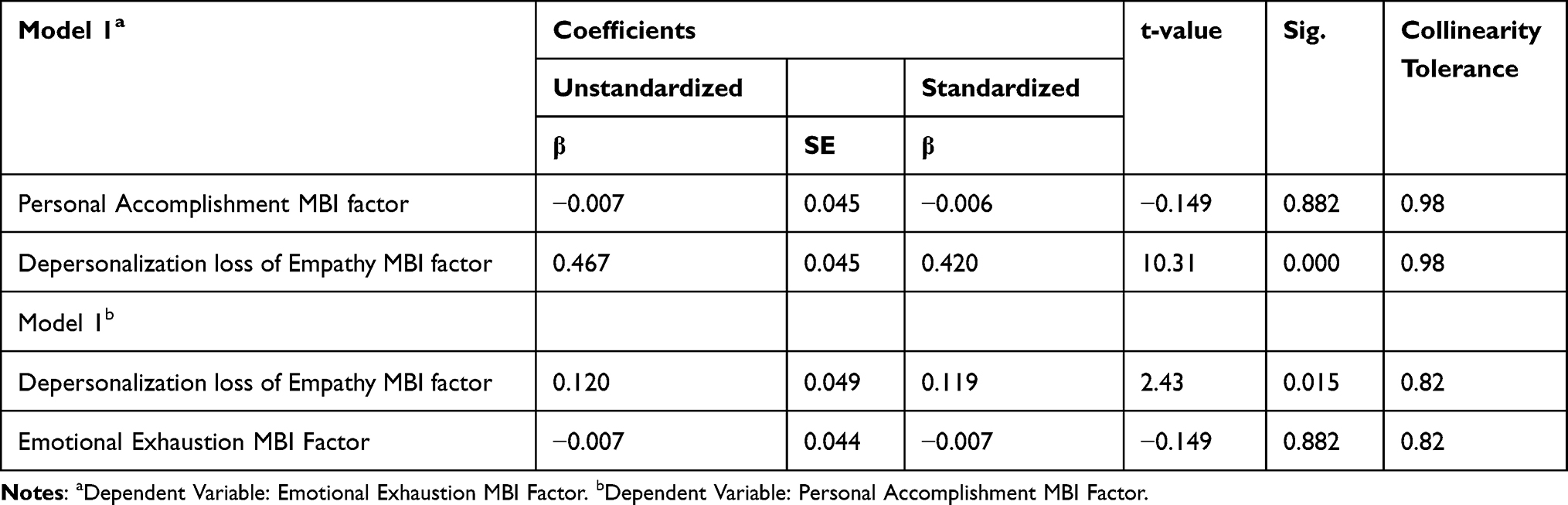 |
Table 3 Regression Analysis of MBI for Continuous Variables |
Precision Bandwidth
In the context of our analysis, it is essential to consider the distribution of the “Emotional Exhaustion for MBI” factor, as it plays a pivotal role in subsequent statistical analyses aimed at testing our research hypotheses and achieving our research objectives. The “Emotional Exhaustion for MBI” factor exhibits a near-normal distribution, indicating its suitability for subsequent statistical analyses to test research hypotheses and achieve research objectives. The mean value of approximately ‘4’ signifies that, on average, respondents assess the “emotional exhaustion for MBI” factor a few times within a given month. This is accompanied by a relatively minor standard deviation, indicative of reduced variability around the mean. Similarly, the “personal accomplishment for MBI” also displays a distribution close to normal, implying the feasibility of further statistical computations for hypothesis testing and research objective assessment. With a mean value of roughly ‘5’, this indicates that, on average, respondents evaluate the “Personal Accomplishment for MBI” factor about once weekly. The comparatively diminished standard deviation underscores the limited variance around the mean.
Similarly, the “Personal Accomplishment for MBI” also displays a distribution close to normal, implying the feasibility of further statistical computations for hypothesis testing and research objective assessment. With a mean value of roughly ‘5’, this indicates that, on average, respondents evaluate the “Personal Accomplishment for MBI” factor about once weekly. The comparatively diminished standard deviation underscores the limited variance around the mean.
Furthermore, the factor denoted as “Depersonalization (loss of empathy) for MBI” showcases a distribution nearly conforming to normality, substantiating its suitability for subsequent statistical analyses to test research hypotheses and evaluate research objectives. The mean value of around ‘3’ suggests that, on average, respondents assess the “Depersonalization for MBI” factor approximately once a month or less. The minor standard deviation underscores the reduced variability surrounding the mean value (Figure 2).
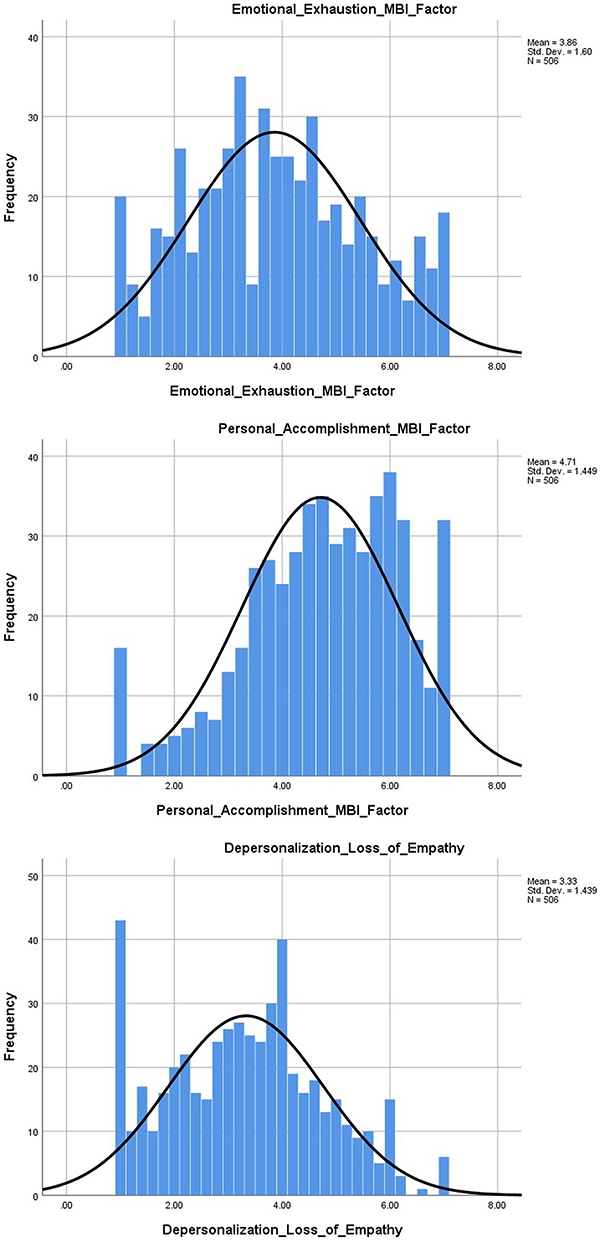 |
Figure 2 Emotional Exhaustion, Depersonalization, and Personal Accomplishment MBI-scales with mean and SD distribution. |
Suggested Factors
The results of a Likert scale-based survey to assess participants’ opinions or attitudes towards a set of eleven items Presented in (Table 4). Each item was rated on a five-point Likert scale ranging from “Strongly disagree” to “Strongly agree”. The table provides the distribution of responses in terms of percentage frequencies for each Likert scale option across the surveyed items. For instance, for “Item 1”, 36 individuals (7.1%) strongly disagreed, 42 individuals (8.3%) disagreed, 138 individuals (27.3%) chose the neutral option, 157 individuals (31%) agreed, and 133 individuals (26.3%) strongly agreed. The same pattern is applied to the remaining items as indicated in Table 3, illustrating the varying degrees of agreement or disagreement among participants for each statement. This information offers insight into the participants’ collective sentiment towards the presented items, enabling researchers to analyze trends and draw conclusions about the participants’ attitudes.
 |
Table 4 Suggested Factors to Reduce Burnout Among the Healthcare Providers |
Clearly, most respondents provided positive and strongly agreed responses regarding the factors that are most effective in preventing Burnout Syndrome. According to their opinions, reducing certain duty-related factors, such as timing and workdays, while implementing reward systems for healthcare workers, emerges as a prominent strategy. The aim of this study, which seeks to identify practical measures to mitigate Burnout Syndrome among critical care providers, and highlighting the importance of addressing work-related factors and introducing incentives to enhance their well-being.
Discussion
Critical care demands unwavering dedication and resilience from healthcare providers. In the pursuit of delivering life-saving interventions, these professionals often navigate an environment fraught with intense emotional demands, prolonged working hours, and intricate medical complexities.26 Burnout Syndrome is pervasive across various cadres of healthcare professionals and is notably prevalent among those who attend to patients in critical condition.22 In this discussion, we delve into the multifaceted dimensions of Burnout Syndrome among critical care health providers, unraveling its origins, impact, and potential interventions. By shedding light on this pressing issue, we strive to acknowledge the challenges these providers face and seek to illuminate pathways towards fostering their resilience and preserving the vitality of our healthcare systems. Thus, the present study is focused on the prevalence, contributing factors, and potential interventions related to Burnout Syndrome among critical care health providers in Saudi Arabia.
In the present study, the low p values (p<0.05) suggest that the observed response distribution differences are statistically significant, underscoring the importance of the findings in understanding the respondents’ experiences of emotional exhaustion, personal accomplishment, and depersonalization. An inverse relationship between burnout and work engagement was observed, indicating a negative correlation between these two constructs.27 The elevated incidence of burnout, particularly in instances linked to emotional exhaustion and depersonalization, may imply a pronounced workload and a disproportion between adept technical skills and interpersonal relationships.28,29 Several investigations have demonstrated that not only individual variables but also factors inherent in structuring work processes augment susceptibility to burnout.30
Furthermore, four distinct domains exhibited associations with severe Burnout Syndrome, encompassing: (1) individual attributes, including age [OR] 0.97 per year increase, a CI=0.96–0.99, and p=0.0008); (2) organizational elements, such as the capacity to select rest days (OR 0.69, CI of 0.52–0.91, p = 0.009) or engagement in an ICU research consortium (OR 0.74, CI of 0.56–0.97, p = 0.03); (3) calibre of interpersonal relationships assessed on a scale of 1 to 10, encompassing conflicts with patients (OR of 1.96, CI of 1.16–1.30, p = 0.01), association with the head nurse (OR 0.92, CI of 0.86–0.98, p = 0.02), and relationships with physicians (OR 0.81, CI of 0.74–0.87, p = 0.0001); and (4) considerations pertaining to end-of-life scenarios, comprising care provision for terminally ill patients (OR 1.39, CI of 1.04–1.85, p = 0.02) and the number of decisions to withhold life-sustaining interventions within the preceding week (OR 1.14, CI of 1.01–1.29, p = 0.04).28 Moreover, individuals exhibiting a heightened perfectionistic disposition, coupled with intense apprehension regarding the outcome of their endeavours, are notably predisposed to experiencing burnout.31
The results of the present study indicated the overall significance of the model. Tests assessing collinearity and autocorrelations revealed the absence of assumption-related issues. Furthermore, the regression analysis underscored the significance of the multiple linear regression, establishing a strong positive coefficient between the predictor “depersonalization” and “personal accomplishment”. Notably, the “Emotional Exhaustion” distribution within the MBI framework approaches normality, facilitating subsequent statistical computations for hypothesis testing and objective assessment. Questions can arise as to why participants showed high burnout, which may be due to the department as the participants were working in critical healthcare units. This assumption is supported by different studies, such as Elshaer, Moustafa.32 In another study conducted in Saudi Arabia among ICU staff, a heightened susceptibility existed to emotional exhaustion, depersonalization, and reduced personal accomplishment, with prevalence rates of 36%, 28%, and 47%, respectively. The primary instigator of burnout was identified to be the excessive workload. Notably, the predominant strategy cited by respondents for mitigating occupational burnout was using vacation as a coping mechanism.33 Moreover, Azoulay, Timsit,34 documented a prevalence of perceived conflicts in a considerable portion, approximately 70%, of ICU personnel. In instances where these conflicts were manifest, they were appraised as notably severe in over fifty percent of the cases, concurrently demonstrating an association with heightened job strain levels. In contrast to preceding investigations, no discernible distinctions emerged about the prevalence of profound Burnout Syndrome when considering diverse clinical settings or distinct professional cohorts.22,35 Prior suppositions posited that ICU/critical healthcare unit physicians and nurses faced a susceptibility to developing severe Burnout Syndrome that was comparable to that of their counterparts in other healthcare domains. A plausible elucidation for our research findings could be traced to the routine practices of critical health care clinical deliberations, which entailed the collective participation of all critical care providers, thereby fostering the equitable dispersion of decisions and responsibilities amidst the entire spectrum of professionals entrusted with patient care.
In the present study, different suggestions were also proposed, such as timing, days, etc., which should be reduced, and some rewards should be given to workers to help establish future guidelines that could reduce Burnout Syndrome among critical care providers. Rewards are crucial in mitigating Burnout Syndrome by providing recognition, intrinsic satisfaction, and a sense of accomplishment to individuals within their professional roles.36 These rewards can encompass various dimensions, such as financial compensation, career advancement opportunities, acknowledgement of achievements, and opportunities for skill development. When healthcare providers receive tangible rewards for their efforts and dedication, their motivation is bolstered, self-worth is enhanced, and contributions are validated, all of which serve to counter the emotional exhaustion and cynicism often associated with burnout. Additionally, rewards can signify that an individual’s contributions are valued by their organization, fostering a positive work environment and promoting a greater alignment between personal and professional aspirations.
Conclusion
This study finds a critical correlation between workplace factors and the personal accomplishment of critical care practitioners in Saudi Arabia, as measured by the Maslach Burnout Inventory (MBI). Our findings underscore the necessity of implementing targeted interventions to ameliorate burnout syndrome by enhancing job satisfaction, improving work conditions, and strengthening support systems. These insights not only contribute to the existing body of research but also pave the way for future investigations aimed at developing and accessing strategies to bolster the well-being of healthcare professionals in high-stress environments.
Data Sharing Statement
The data used to support the findings of this study are included in the article.
Funding
This research received no external funding.
Disclosure
The authors declare no conflict of interest.
References
1. Montero-Marín J, García-Campayo J, Mosquera Mera D, López Del Hoyo Y. A new definition of burnout syndrome based on Farber’s proposal. J Occup Med Toxicol. 2009;4:31. doi:10.1186/1745-6673-4-31
2. Rodrigues H, Cobucci R, Oliveira A, et al. Burnout syndrome among medical residents: a systematic review and meta-analysis. PLoS One. 2018;13(11):e0206840. doi:10.1371/journal.pone.0206840
3. de Paiva LC, Canário ACG, De paiva china ELC, Gonçalves AK. Burnout syndrome in health-care professionals in a university hospital. Clinics. 2017;72(5):305–309. doi:10.6061/clinics/2017(05)08
4. Schaufeli WB, Maslach C, Marek T. Professional Burnout: Recent Developments in Theory and Research. London, UK: Routledge; 2017.
5. Maslach C, Leiter MP. Understanding the burnout experience: recent research and its implications for psychiatry. World Psychiatry. 2016;15(2):103–111. doi:10.1002/wps.20311
6. Patel RS, Bachu R, Adikey A, Malik M, Shah M. Factors related to physician burnout and its consequences: a review. Behav Sci. 2018;8(11). doi:10.3390/bs8110098
7. Bateman EA, Viana R. Burnout among specialists and trainees in physical medicine and rehabilitation: a systematic review. J Rehabil Med. 2019;51(11):869–874. doi:10.2340/16501977-2614
8. Dahiya H, Goswami H, Bhati C, et al. Severe acute respiratory syndrome coronavirus 2 omicron variant and psychological distress among frontline nurses in a major COVID-19 center: implications for supporting psychological well-being. J Prim Care Special. 2023;4(1):10–16. doi:10.4103/jopcs.jopcs_22_22
9. Chaudhary P, PayalNain P, Pooja Rana P, et al. Perceived risk of infection, ethical challenges and motivational factors among frontline nurses in Covid-19 pandemic: prerequisites and lessons for future pandemic. BMC Nurs. 2024;23(1):5. doi:10.1186/s12912-023-01653-7
10. Kumar R, Beniwal K, Bahurupi Y. Pandemic fatigue in nursing undergraduates: role of individual resilience and coping styles in health promotion. Frontiers in Psychology. 2022;13:940544. doi:10.3389/fpsyg.2022.940544
11. Al-Youbi RA, Jan MM. Burnout syndrome in pediatric practice. Oman Med J. 2013;28(4):252–254. doi:10.5001/omj.2013.71
12. Alwashmi AH, Alkhamees AA. Burnout and the psychological impact among physiatrists in Saudi Arabia during COVID-19. Int J Environ Res Public Health. 2021;18(18). doi:10.3390/ijerph18189621
13. Al-Haddad A, Al-Omar F, Al-Khaleel A, Al-Khalaf A. Prevalence of burnout syndrome and its related risk factors among physicians working in primary health care centers of the Ministry of Health, Al Ahsa region, Saudi Arabia, 2018–2019. J Family Med Prim Care. 2020;9(2):571–579. doi:10.4103/jfmpc.jfmpc_743_19
14. Baghdadi LR, Baghdadi RR, Kamal RS, et al. Physicians’ job satisfaction, ethics and burnout in Makkah, Saudi Arabia. J Pak Med Assoc. 2020;70(12):2383–2389. doi:10.47391/jpma.401
15. Alsulimani LK, Farhat AM, Borah RA, et al. Health care worker burnout during the COVID-19 pandemic: a cross-sectional survey study in Saudi Arabia. Saudi Med J. 2021;42(3):306–314. doi:10.15537/smj.2021.42.3.20200812
16. Aldrees T, Hassouneh B, Alabdulkarim A, et al. Burnout among plastic surgery residents. National survey in Saudi Arabia. Saudi Med J. 2017;38(8):832–836. doi:10.15537/smj.2017.8.18346
17. Agha A, Mordy A, Anwar E, Saleh N, Rashid I, Saeed M. Burnout among middle-grade doctors of tertiary care hospital in Saudi Arabia. Work. 2015;51(4):839–847. doi:10.3233/wor-141898
18. Alharbi J, Wilson R, Woods C, Usher K. The factors influencing burnout and job satisfaction among critical care nurses: a study of Saudi critical care nurses. J Nurs Manag. 2016;24(6):708–717. doi:10.1111/jonm.12386
19. Almodibeg BA, Smith H. A cross-sectional survey to explore the prevalence and causes of occupational burnout syndrome among perioperative nurses in Saudi Arabia. Nurs Open. 2021;8(1):364–371. doi:10.1002/nop2.637
20. Alqahtani AM, Awadalla NJ, Alsaleem SA, Alsamghan AS, Alsaleem MA. Burnout syndrome among emergency physicians and nurses in Abha and Khamis Mushait Cities, Aseer Region, Southwestern Saudi Arabia. Sci World J. 2019;2019:4515972. doi:10.1155/2019/4515972
21. Al-Turki HA, Al-Turki RA, Al-Dardas HA, et al. Burnout syndrome among multinational nurses working in Saudi Arabia. Ann Afr Med. 2010;9(4):226–229. doi:10.4103/1596-3519.70960
22. Moss M, Good VS, Gozal D, Kleinpell R, Sessler CN. A critical care societies collaborative statement: burnout syndrome in critical care health-care professionals. A call for action. Am J Respir Crit Care Med. 2016;194(1):106–113. doi:10.1164/rccm.201604-0708ST
23. Alwhaibi M, Alhawassi TM, Balkhi B, et al. Burnout and depressive symptoms in healthcare professionals: a cross-sectional study in Saudi Arabia. Healthcare. 2022;10(12). doi:10.3390/healthcare10122447
24. Williamson K, Lank PM, Cheema N, Hartman N, Lovell EO. Comparing the maslach burnout inventory to other well-being instruments in emergency medicine residents. J Grad Med Educ. 2018;10(5):532–536. doi:10.4300/jgme-d-18-00155.1
25. Raosoft. Sample size calculator by Raosoft; 2020.
26. Moreno-Jiménez JE, Demerouti E, Blanco-Donoso LM, Chico-Fernández M, Iglesias-Bouzas MI, Garrosa E. Passionate healthcare workers in demanding intensive care units: its relationship with daily exhaustion, secondary traumatic stress, empathy, and self-compassion. Curr Psychol. 2022;1–16. doi:10.1007/s12144-022-03986-z
27. Castro C, Timenetsky KT, Katz M, et al. Burnout syndrome and engagement among critical care providers: a cross-sectional study. Rev Bras Ter Intensiva. 2020;32(3):381–390. doi:10.5935/0103-507x.20200066
28. Poncet MC, Toullic P, Papazian L, et al. Burnout syndrome in critical care nursing staff. Am J Respir Crit Care Med. 2007;175(7):698–704. doi:10.1164/rccm.200606-806OC
29. Merlani P, Verdon M, Businger A, Domenighetti G, Pargger H, Ricou B. Burnout in ICU caregivers: a multicenter study of factors associated to centers. Am J Respir Crit Care Med. 2011;184(10):1140–1146. doi:10.1164/rccm.201101-0068OC
30. Ramos TT, Tung TC, Cecílio HJE. Síndrome de burnout ou estafa profissional e os transtornos psiquiátricos. Archiv Clin Psych. 2007;34:223–233. doi:10.1590/S0101-60832007000500004
31. Hill AP, Curran T. Multidimensional perfectionism and burnout: a meta-analysis. Pers Soc Psychol Rev. 2016;20(3):269–288. doi:10.1177/1088868315596286
32. Elshaer NSM, Moustafa MSA, Aiad MWM, Ramadan MIE. Job stress and burnout syndrome among critical care healthcare workers. Alexandria J Med. 2018;54(3):273–277. doi:10.1016/j.ajme.2017.06.004
33. Abdullah S, Mohammed A. Assessment of occupational burnout among intensive care unit staff in Jazan, Saudi Arabia, using the maslach burnout inventory. Critical Care Res Pract. 2022;2022:1298887.
34. Azoulay É, Timsit J-F, Sprung CL, et al. Prevalence and factors of intensive care unit conflicts: the conflicus study. Am J Respir Crit Care Med. 2009;180(9):853–860. doi:10.1164/rccm.200810-1614OC
35. Fumis RRL, Junqueira Amarante GA, de Fátima Nascimento A, Vieira Junior JM. Moral distress and its contribution to the development of burnout syndrome among critical care providers. Ann Intensive Care. 2017;7(1):71. doi:10.1186/s13613-017-0293-2
36. Alvarado LE, Bretones FD, Rodríguez JA. The effort-reward model and its effect on burnout among nurses in Ecuador. Front Psychol. 2021;12:760570. doi:10.3389/fpsyg.2021.760570
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.