")
Back to Journals » Infection and Drug Resistance » Volume 16
Burkholderia cepacia Induced Occipital Subcutaneous Abscess and Fracture in a Brain-Dead Woman
Authors Yang W, Liu T, Zhan C, Jiang H, Zhang W, Yang Q , Zheng X
Received 17 May 2023
Accepted for publication 27 June 2023
Published 11 July 2023 Volume 2023:16 Pages 4535—4538
DOI https://doi.org/10.2147/IDR.S418967
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Wu Yang,1,* Tingting Liu,1,* Chun Zhan,2 Hui Jiang,1 Wang Zhang,3 Qing Yang,4 Xia Zheng1
1Department of Critical Care Medicine, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, 310000, People’s Republic of China; 2Department of Critical Care Medicine, Hang Zhou Integrative Medicine Hospital, Hangzhou, Zhejiang, 310000, People’s Republic of China; 3Department of Infectious Diseases, Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, 310000, People’s Republic of China; 4Department of Laboratory Medicine, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, 310000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xia Zheng, Department of Critical Care Medicine, The First Affiliated Hospital, Zhejiang University School of Medicine, No. 79, Qingchun Road, Shangcheng District, Hangzhou, Zhejiang, People’s Republic of China, Tel +86-13958174689, Fax +86-571-87236838, Email [email protected]
Abstract: Burkholderia cepacia is an aerobic opportunistic Gram-negative pathogen that mainly infects immunodeficiency patients. However, soft tissue infections with fractures due to Burkholderia cepacia are rare with no cases reported. Here, we report a rare case of 3 years of brain death in a 43-year-old woman with Burkholderia cepacia resulting in an occipital subcutaneous abscess and fracture. Through the second-generation sequencing of the whole genome of this strain, it was found that there were no high virulence genes and virulence factors. The patient received targeted antibiotic therapy and showed improvement in clinical symptoms and radiological signs. Bone destruction because of Burkholderia cepacia is easily overlooked due to the lack of characteristic symptoms and limited clinical examination. This case reminds us that Burkholderia cepacia without major virulence factors could damage the bone in immune-compromised patients.
Keywords: brain death, Burkholderia cepacia, subcutaneous abscess, generation sequencing, case report
Introduction
Burkholderia cepacia (B. cepacia), a Gram-negative aerobic bacillus, is a well-known opportunistic pathogen of immune-compromised patients including cystic fibrosis, chronic granulomatous disease, and lung transplantation patients.1 Several cases report that B. cepacia could induce extrapulmonary-tissue abscesses, such as brain, bilateral psoas, chest intra-abdominal, and deep neck.2–8 However, soft tissue infections with fractures caused by B. cepacia are extremely rare with no instances reported. We report a middle-aged female with a medical history of 3-year brain dead who developed a subcutaneous abscess with a bone fracture in her right occipital region.
Case Report
A 40-year-old female was diagnosed with viral encephalitis-induced secondary brain death on September 11, 2019, based on the American Academy of Neurology (AAN) criteria for the determination of brain death in adults.2 Her clinical manifestations presented as comatose, lack of brainstem reflexes, and cannot breathe spontaneously. The head CT showed diffuse edema of brain tissue and gray matter with white matter structure blurred (Figure 1A). The electroencephalogram (EEG) indicated resting-state brain electrical activity. Her family finally decided to transfer to the Hang Zhou Integrative Medicine Hospital. She received mechanical ventilation and rehabilitation exercise during hospitalization lasting for almost 3 years. The patient had a high fever on September 12, 2022. Physical examination revealed intense swelling of her right occipital region and the abscess was approximately four centimeters in diameter. The brain computed tomography (CT) imaging showed the right temporoparietal cerebral hemorrhage and occipital defect with a subcutaneous abscess in Figure 1B, and laboratory workup showed white blood cell, 9.0×109/L; neutrophils, 87.8%; lymphocytes, 9.1%; red blood cell, 2.84×1012/L; hemoglobin, 86 g/L; platelet, 183×109/L; C-reactive protein, 100.2 mg/L; procalcitonin, <0.25 ug/L. The sampling of abscess fluid was conducted, and bloody pus was obtained (Figure 2). The pus’s direct smear examination and culture showed B. cepacia. The colony was susceptible to cefoperazone-sulbactam, meropenem, ceftazidime, minocycline, and TMP-SMX (Table 1). To confirm the result, we further conducted metagenomic next-generation sequencing (NGS) of the abscess aspiration and revealed B. cepacia (Table 2). We analyzed its virulence genes and the major virulence factors focusing on the function of motility, such as fliM, flhA, motA, fliA, flgG, and flgI. We further found that the drug-resistant genes of this strain were mphL, satA_Ba, BcII, and bla1 via the second-generation sequencing of the whole genome.3
 |
Table 1 Burkholderia cepacia Susceptibility Results by the MIC Test |
 |
Table 2 Pathogenic Microorganisms Identified in a Subcutaneous Abscess Sample |
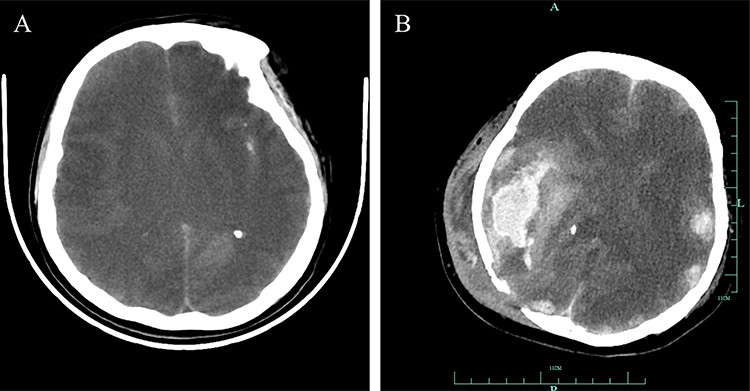 |
Figure 1 Brain CT images of the patient. (A) Brain CT imaging on October 15, 2019. The head CT imaging was showed diffuse edema of brain tissue, gray matter and white matter structure blurred. (B) Brain CT on September 14, 2022. The brain CT imaging was showed the right temporo-parietal cerebral hemorrhage and occipital defect with subcutaneous abscess. |
 |
Figure 2 The sampling of bloody pus. |
The cerebrospinal fluid examination (CSF) was performed to rule out intracranial infection, and no positive results were seen in the CSF, including CSF routine, culture, Cryptococcus neoformans, Mycobacterium tuberculosis and NGS. She was then treated with Cefoperazone-sulbactam 2.0g q8h for 5 days depending on the result of the antimicrobial susceptibility testing for B. cepacia. By this series of treatments, she had no fever, and the inflammation presented white blood cells, 5.5×109/L; neutrophils, 79.6%; lymphocytes, 17.4%; red blood cells, 3.0×1012/L; hemoglobin, 89 g/L; platelet, 135×109/L; C-reactive protein, 40 mg/L; procalcitonin, <0.25 ug/L. The inflammatory markers were significantly lower than before with no apparent swollen sign of the right occipital area in several days. Worth mentioning is that the patient neither reviewed for the CT nor got enough treatment courses to objectively evaluate the therapeutic effect of the soft tissue abscess with a bone fracture because family members decided to abandon treatments.
Discussion
Extrapulmonary infection caused by B. cepacia is a rare, life-threatening disease usually found in immunocompromised patients.1,3 B. cepacia-induced infections are difficult to treat because the pathogen is resistant to multiple antibiotics inherently.3
Several cases report that B. cepacia could cause abscesses in the brain, bilateral primary psoas, chest intra-abdominal, and even deep neck.3–8 One report of a case of septic arthritis of the knee caused by B. cepacia complex in a patient and his X-ray showed soft tissue swelling but no discrete fracture.9 However, the histopathological examination of the tissue from another case of B. cepacia causing frontal mucopyocele with anterior cranial fossa extension showed the surrounding bone destruction despite brain images with no bone fracture.10 We encountered an uncommon case of subcutaneous abscess in the right occipital region of a brain-dead woman due to a B. cepacia infection with no special virulence factors. We originally suspected a secondary subcutaneous abscess following an intracranial infection, yet a couple of rounds of CSF examinations showed negative, we then finally confirmed that the abscess with bony destruction was directly caused by B. cepacia. This case demonstrates that B. cepacia without major virulence factors could cause bone injury in immune-compromised patients.
Conclusion
Immunocompromised patients, such as those with AIDS, organ transplantation, long-term hormone treatment, malignant tumors, or diabetes, are at high risks for intracranial infection. Intracranial infection caused by Bacillus cepacia, especially bone destruction, is a rare infection. Early diagnosis and adequate antibiotic therapy could reduce the morbidity of immunocompromised patients suffering from disseminated B. cepacia.
Consent Statement
The patient’s husband provided written informed consent to allow the case details and any accompanying images to be published.
Clinical research ethics committee of The First Affiliated Hospital, Zhejiang University School of Medicine approved this study (IIT20221198A).
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Pareek P, Gupta B, Chetan C, et al. Burkholderia cepacia brain abscess in a term neonate. Indian J Pediatr. 2020;87(6):478–479. doi:10.1007/s12098-019-03156-3
2. Greer DM, Shemie SD, Lewis A, et al. Determination of brain death/death by neurologic criteria: the world brain death project. JAMA. 2020;324(11):1078–1097. doi:10.1001/jama.2020.11586
3. Rohit A, Rani MS, Anand NS, et al. Burkholderia vietnamiensis causing a non-lactational breast abscess in a non-cystic fibrosis patient in Tamil Nadu, India. Indian J Med Microbiol. 2020;38(3 and 4):496–499. doi:10.4103/ijmm.IJMM_20_329
4. Agrawal S, Kapil A, Dhawan B, et al. Burkholderia cepacia: an uncommon cause of bilateral primary psoas abscesses in a patient with a pott spine that cannot be ignored. Natl Med J India. 2018;31(2):124–125. doi:10.4103/0970-258X.253158
5. Fadini GP, Tiengo A, Avogaro A, et al. First isolation of Burkholderia cepacia from a deep neck abscess in a diabetic patient successfully treated with hyperbaric oxygen. J Clin Microbiol. 2005;43(1):529. doi:10.1128/JCM.43.1.529.2005
6. Mukhopadhyay C, Bhargava A, Ayyagari A. Two novel clinical presentations of Burkholderia cepacia infection. J Clin Microbiol. 2004;42(8):3904–3905. doi:10.1128/JCM.42.8.3904-3905.2004
7. Hobson R, Gould I, Govan J. Burkholderia (Pseudomonas) cepacia as a cause of brain abscesses secondary to chronic suppurative otitis media. Eur J Clin Microbiol Infect Dis. 1995;14(10):908–911. doi:10.1007/BF01691499
8. Simmonds NJ, Gyi KM. Cystic fibrosis, a Burkholderia cenocepacia chest wall abscess and rapid clinical deterioration. J R Soc Med. 2008;Suppl 1(suppl 1):S46–S50. doi:10.1258/jrsm.2008.s18011
9. Koo J, Deans GD. A rare case of Burkholderia cepacia complex septic arthritis. Case Rep Infect Dis. 2018;2018:6232760. doi:10.1155/2018/6232760
10. Saratziotis A, Zanotti C, Baldovin M, et al. Burkholderia cepacia causes frontal mucopyocele with anterior cranial fossa extension: a novel case report. Iran J Otorhinolaryngol. 2021;33(118):327–332. doi:10.22038/ijorl.2021.51654.2753
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.