")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Burdens and Difficulties Experienced by Parental Caregivers of Children and Adolescents with Idiopathic Nephrotic Syndrome in Mainland China: A Qualitative Study
Authors Hu X , Wu Q, Lu Q, Zhang J, Yang X, Chen W, Wang P, Yu Q, Dong J, Sang Y
Received 22 March 2023
Accepted for publication 21 November 2023
Published 2 December 2023 Volume 2023:16 Pages 3749—3759
DOI https://doi.org/10.2147/JMDH.S413677
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Xinmiao Hu,1– 3,* Qian Wu,1,2,* Qunfeng Lu,4,5,* Jiangao Zhang,6 Xiaowei Yang,7 Wenjian Chen,3 Ping Wang,3 Qinglin Yu,3 Jingan Dong,3 Yan Sang8
1School of Medicine, Tong University, Shanghai, People’s Republic of China; 2Department of Nursing, Shanghai Tenth People’s Hospital Affiliated to Tongji University, Shanghai, People’s Republic of China; 3Department of Nephrology and Rheumatology, Shanghai Children’s Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, People’s Republic of China; 4Department of Nursing, Shanghai Sixth People’s Hospital Affiliated to Shanghai Jiao Tong University, Shanghai, People’s Republic of China; 5School of Medicine, Shanghai Jiao Tong University, Shanghai, People’s Republic of China; 6Nantong Visionland Eye Hospital, Jiangsu, People’s Republic of China; 7School of Medicine, Nantong University, Jiangsu, People’s Republic of China; 8Department of Nursing, Department of Computer Technology, Affiliated Hospital of Nantong University, Nantong, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yan Sang, Department of Computer Technology, Affiliated Hospital of Nantong University, No. 20 Xisi Road, Nantong, Jiangsu, 226001, People’s Republic of China, Tel +86 13862915051, Email [email protected]
Purpose: To identify the difficulties and burdens related to the experience of caring for children.
Methods: A phenomenological approach was used in this qualitative study. Semi-structured and adolescents with idiopathic nephrotic syndrome (INS) in mainland China. Interviews lasting 35– 90 minutes were conducted with 13 parental caregivers of youth with INS. The Colaizzi’s analysis was used in data analysis.
Results: The mean age of parental caregivers was 40.3 ± 6.1 years, and the average caregiving year of 3.2 ± 3.3 years. Most INS patients were male (69.2%), had a mean age of 7.6 ± 4.2 years. Based on the analysis of the data, five major themes emerged. These were: persistent emotional burden; neglected physical burden; overwhelming financial burden; absence of social support system and burden related to loss of normal life.
Conclusion: Health professionals must develop strategies to provide stage-by-stage, targeted health education and psychological support services to parental caregivers of INS youth in China. The government must subsidize routine medications and frequent hospitalizations to minimize the financial burden on parental caregivers of INS youth. Moreover, anti-discrimination policies must be established to protect caregivers from explicit discrimination in public places.
Keywords: caregiver, burden, idiopathic nephrotic syndrome, youth
A Letter to the Editor has been published for this article.
Introduction
Nephrotic syndrome (NS) in children is characterized by the triad of hypoalbuminaemia, oedema, and proteinuria.1 Idiopathic nephrotic syndrome (INS) accounts for about 90% of childhood NS, which is one of the most common chronic glomerular diseases affecting 1.15 to 16.9 per 100000 children.2,3 Based on data from 37 collaborating hospitals in China, INS accounted for approximately 20% of all youth hospitalized for urological diseases during the same period.4 Many youth with INS will achieve complete remission with an initial course of steroid therapy, but over 80% will relapse.5 These patients usually require immunosuppressive agents or steroid-sparing agents to minimize relapses.6 Complications, either of treatment or secondary to the disease, are extremely common.7 Previous studies have shown that INS negatively affects the psychological well-being, personal and social growth of youth, as well as reduces the quality of life of youth and their families.8–10
Caregivers play a crucial role in the long-term care of youth with INS. Most youth with INS are unable to self-manage their disease, and depend heavily on their parental caregivers for disease management.11,12 Continuous proteinuria monitoring, supervising medication, and critical treatment-related decisions are frequently performed by parental caregivers.13 Meanwhile, parents are required to deal with frequent follow-up visits to the hospital, school challenges, and dietary restrictions.14,15 These responsibilities are challenging as well as stressful for parental caregivers.
Being a parental caregiver of INS is mentally stressful due to fears of relapse. A cross-sectional study in China on parental caregivers showed that parental caregivers of youth with NS were anxious in 67.37% of cases and depressed in 68.42% of cases,16 which is similar to the prevalence of parental depression in youth with NS (67.82%) reported by Zhang et al.17 Moreover, NS is a chronic disease that requires long-term treatment, and the high medical costs aggravate the psychological pressure on parental caregivers, and even more so the financial burden on them.18 The negative effects experienced by parental caregivers can accumulate over time and adversely affect their quality of life and well-being, leading to caregiving stress. Dong et al found that parents of NS youth have a lower health-related quality of life (HRQOL) compared with controls.19 The parents’ health status influences the progression and recovery of the disease.20 Understanding the burdens experienced by parental caregivers of INS youth may greatly help parents adapt to the role of caregivers, and achieve optimal health outcomes for patients with INS.
Despite the recent increase in research investigating caregiver burdens for youth with chronic diseases, the nature of the burden experienced by parental caregivers of INS youth remains largely unexplored. Most current research in China focuses primarily on quantitative studies of the HRQOL,21 coping style,22 and psychosocial state of INS patients and their parents.23 Qualitative research defines people and cultures deeply and attempts to uncover the meaning, events, processes, understandings, and understandings that individuals attribute to reality.24 As a result, this study sought to explore the burdens and difficulties faced by parental caregivers of youth with INS and to present in-depth data on their thoughts and feelings on this issue. In turn, these insights may guide service development towards a less burdensome and more family-friendly model of care for children and adolescents with INS.
Methodology
Study Design
The purpose of this study was to investigate the lived experiences of parental caregivers of INS youth and to understand their difficulties and burdens by utilizing a qualitative phenomenological design. A semi-structured, telephone or face-to-face interview was conducted with parental caregivers in mainland China.
Study Participants
A purposive sampling approach was used to recruit participants in this study, through the deliberate selection of participants based on inclusion criteria, until saturation of themes had occurred. As a phenomenology study involved a small number of subjects, the recruitment aim was to recruit 10–15 participants for one-to-one interviews.25 The participants were recruited from caregivers attending visits with INS patients assessed or hospitalized in the Nephrology Department of Shanghai Children’s Hospital, Shanghai Jiao Tong University from May 2022 to November 2022.
To be eligible for participation in the study interview, INS parental caregivers were required to (i) be the father or mother of a child 18 years of age or younger with diagnosed INS,26 and (ii) be a primary caregiver during at least 3 months of continuous care for a child being treated for INS during this period. INS parental caregivers were considered ineligible to participate in interviews if (i) the child with INS also experienced chronic diseases or other significant comorbidities; (ii) the child with INS was considered to require immediate treatment or medical care and the study could pose an undue burden on the patient or caregiver; (iii) the INS parental caregiver was unable to communicate fluently with the researcher in the Chinese language.
Data Collection
Prior to the interviews, demographic data were collected, including the length of care, which was defined as the total number of months that parental caregivers devoted to caring for INS youth.
Pilot interviews were carried out among three parental caregivers to check interview questions. The interview questions were not modified. As part of our interviewing process, we encouraged interviewees to provide more clarifications and clear interpretations in the event of any ambiguity. Participants’ willingness and preparedness determined the duration of each interview. Each interview lasted between 35 and 90 minutes, and the sessions were recorded using a voice recorder. We conducted the interview in Chinese using semi-structured questions, and the interview guide was shown in Box 1.
 |
Box 1 Interview Questions |
Data Analysis
The audio recordings of the interviews were transcribed into text within 24 hours of the end of the interviews without any modification or deletion of the recorded content to ensure the authenticity of the data and were imported into NVivo 11.0 software for collation and analysis. Colaizzi’s 7-step phenomenological analysis method was used to analyze the data.27 In order to avoid errors, data was analyzed independently by three researchers. The researcher transcribed the audio recordings of the interviews and reviewed each transcript repeatedly to gain a comprehensive sense and understanding of the entire transcript. All researchers extracted important and meaningful statements respecting the phenomenon from the transcripts. Relying on differences and similarities, categories and subcategories were then identified through mutual discussion and shared views. All emerging categories were defined in an integrated context. Discrepancies in categories and subcategories, as well as overestimated or misused categories, were resolved by consensus. The final structure of the study was based on the agreement categories. Using member checking, the findings of the study were validated. The researchers sent the descriptive results to the participants for verification.
Ethical Considerations
In accordance with the requirements of the Declaration of Helsinki, this study was conducted. The study was approved by the Ethics Committee of Shanghai Children’s Hospital, Shanghai Jiao Tong University. The approval number was 2022R133. Participants in the study provided written informed consent. The informed consent of participants included the publication of anonymized responses. All participants agreed to the use of their data for academic and analytical purposes.
Results
Demographic Characteristics
Saturation was reached when 13 INS parental caregivers completed interviews. Tables 1 and 2 present the demographic data of the 13 parental caregivers and their children with INS who took part in the study. As shown in Table 1, the majority of caregivers were female (11, 84.6%), employed (7, 53.8%), living in rural areas (10, 76.9%), married (13, 100%) and educated to college or above (5, 38.5%). The mean age of parental caregivers was 40.3 ± 6.1 years, with monthly incomes of between CNY (Chinese Yuan) 5000 and CNY 10000 per capita, and the average caregiving year of 3.2 ± 3.3 years. INS patients were mostly male (9, 69.2%), had a mean age of 7.6 ± 4.2 years, had health insurance (10, 76.9%), and the age of INS onset was 10.9 ± 3.9 years. The majority of the pathological type of INS patients had minimal change nephrotic syndrome (7, 53.8%), and most of them took prednisone (12, 92.3%).
 |
Table 1 Demographic Characteristics of the Parental Caregivers of INS Youth Interviewed |
 |
Table 2 Demographic Characteristics of Children and Adolescents with INS |
Based on the analysis of the transcripts of interviews, five major emergent themes were identified consistently throughout the interview data. Table 3 summarizes all 12 minor sub-themes within these five themes. The themes/sub-themes are further characterized below.
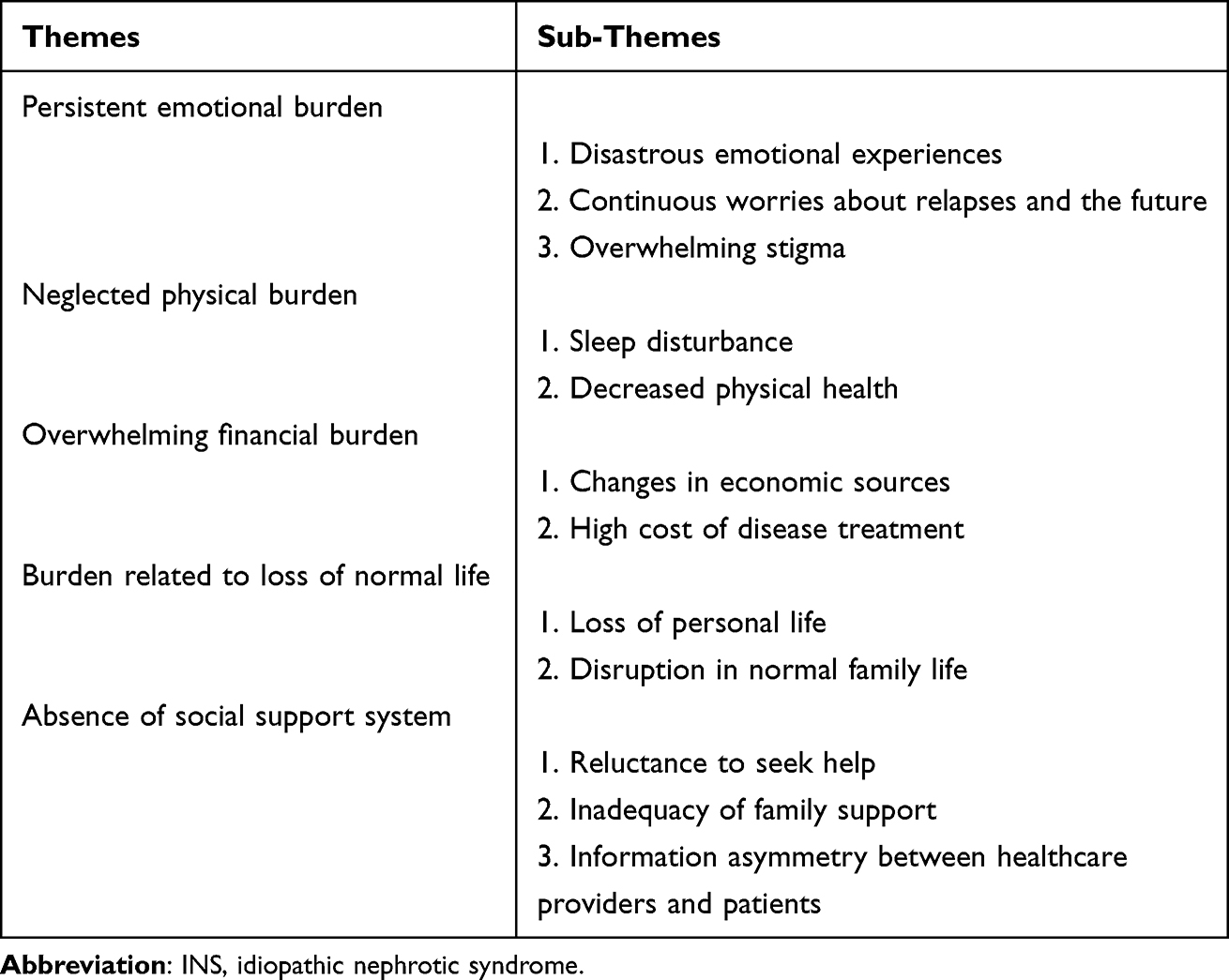 |
Table 3 Themes and Sub-Themes Emerging from Interviews with Parental Caregivers of INS Youth |
Persistent Emotional Burden
Disastrous Emotional Experiences
After a child’s diagnosis, many parental caregivers frequently experience overwhelming emotions, such as hopelessness, fearfulness, shock, guilt, sadness, frustration, and a sense of impending disaster.
When the doctor took a look at my child’s lab report, he said it would be a lot of trouble to cure this disease, and I was feeling as if people were just sentenced to death. (Participant 3)
At the time, we were scared by the diagnosis of idiopathic nephrotic syndrome and in a hopeless dilemma. (Participant 12)
Continuous Worries About Relapses and the Future
All caregivers expressed anxiety about the repeated infections and relapses of INS. Worry and fear were mentioned many times and most parental caregivers lived with uncertainty and anxiety for years. They maintained a high level of mental stress over the child’s urine tests and affected the child’s daily activities. Moreover, they were concerned that patients would not be able to adapt to adult life.
He cannot strain himself and needs to rest. So I’m scared that she wouldn’t be able to find a job to support herself in the future. (Participant 4)
Whenever he had a cold or cough, I was nervous about the appearance of proteinuria. (Participant 6)
Overwhelming Stigmatization
When we evaluated the parents’ feelings of having a child diagnosed with INS, we found that the majority of them experienced self-stigma due to the effects of the disease. They were often treated discriminatorily in public places, and feared being judged by others.
Whenever I take my child to a public place, I always sterilize his hands before touching anything. But this action often draws strange looks from others. (Participant 3)
Neglected Physical Burden
Sleep Disturbance
Children and adolescents with INS require frequent and prolonged care, which results in a loss of rest for parental caregivers. Parental caregivers also reported a lack of quality rest, as they were often concerned about relapses in their children. Moreover, as most parents described their caring responsibilities as a “24-hour job”2, rest was not seen as a privilege. The emotional and physical health of parental caregivers would be adversely affected by long-term sleep deficiency.
I doze off a lot on night shifts. I could only sleep 1–2 hours during the day before working night shift, I couldn’t sleep during the day and rarely fall asleep. Can’t have anything, can’t sleep if I have something, I’m a terrible daytime sleeper. (Participant 2)
Decreased Physical Health
Parental caregivers were already facing a decline in health as they age. They face challenges such as headaches, back pain, weight loss, menstrual disorders and fever. Due to their involvement in the patient’s care, caregivers were unable to take care of themselves and attend to their own medical concerns.
I have frequent headaches, but I’ve been putting up with the pain and not going to the hospital. I don’t care about myself. (Participant 4)
Since he has been ill, my periods have been a bit disrupted. (Participant 5)
Overwhelming Financial Burden
Changes in Economic Sources
Caring for a child with INS usually requires round-The-clock care. Some parental caregivers reported that one parent gave up work and reduced working hours in order to provide adequate care for their children, which tends to reduce family income and further increase the financial strain on low-income and middle-income families.
It’s a chronic condition and his dad told me I couldn’t work anymore and had to stay home all the time to take care of him. So I’m quitting my job and staying home now, with all my thoughts on him. (Participant 3)
High Cost of Disease Treatment
As expressed by most parents, caring for a child with a chronic disease is financially draining. A large part of caregivers’ financial burden is attributed to frequent hospitalisations and the cost of medications. Additionally, some high-cost medications are not covered by insurance. Parental caregivers stressed that they sacrificed their expenses and went to different doctors in order to take care of the patients.
We spent over 600,000 RMB on him. (Participant 1)
Most of their medications contain immunosuppressants, such as tacrolimus or cyclosporin. They are not covered by insurance. (Participant 11)
Absence of Social Support System
Reluctance to Seek Help
The tendency for parental caregivers to ask for assistance was low. Fearing ridicule and gossip from others, parental caregivers often hide their child’s condition from others. When faced with challenges, doing it all on their own was considered more effective than dealing with unwanted rejection from others.
When the neighbours saw him, they would ask why the boy was lying there and said that the boy didn’t look good either, so they wondered if our boy was as sick as if he was very sick. (Participant 3)
Inadequacy of Family Support
Kids are the hope of the entire family, particularly those who have only one child in China. It is devastating for a family when a child is diagnosed with INS. Family support is one of the most critical factors influencing caregiver stress, but inadequate family support systems are a common problem for parents of youth with INS. Parental caregivers took on most of the roles in caring for INS, yet some family members were not only uninvolved, but also unsupportive of the child’s parents’ caring behaviour.
My family didn’t understand, and there were a lot of family conflicts. In those six months, the child was hospitalised every month, so how could it not be tiring? I stayed at home for two days and still quarrelled every day. (Participant 10)
Information Asymmetry Between Healthcare Professionals and Patients
Parental caregivers of youth with INS wanted to know details about medication, treatment effects, diet, and prognosis from healthcare professionals, but when they sought support or help from the healthcare professionals, the healthcare professionals did not have time to explain or rarely do.
I would love to ask the doctors and the nurses, but you guys are busy and I don’t know where to start. (Participant 4)
Less salt, and I’m not sure if less salt means you can’t have any salt at all, or if you can set aside a little bit. (Participant 7)
Burden Related to Loss of Normal Life
Loss of Personal Life
Caregiver’s personal life limited by multitasking, time-consuming care processes, and excessive dependence on patients. After the illness, most parental caregivers stated that they were unable to participate in many activities that they performed prior to the illness.
I couldn’t go out, I couldn’t do anything else, I just stay at home with him every day. (Participant 3)
Disruption in Normal Family Life
After the diagnosis of INS, the pattern of daily life in the child’s family changes. As a result of their child’s unpredictable physical condition, parental caregivers reported difficulty attending “normal” activities outside the home. They often canceled family vacations due to concerns that their children may be infected. Moreover, parents of INS patients usually canceled family activities and went out less for fear of relapse.
As we were worried about our child getting infected during the trip, we decided not to travel until she was well enough. (Participant 8)
Discussion
Parental caregivers of youth with INS are faced with a variety of challenges and difficulties when caring for a child with INS. In this study, the burden faced by parental caregivers in caring for their youth with INS generated five major themes, which included persistent emotional burden, neglected physical burden, overwhelming financial burden, absence of social support system and burden related to loss of normal life. The analysis of burdens from the parental caregiver’s perspective can assist in consolidating family caregiving support systems and provide a basis for the development of public health policies and rational treatment measures.
As a result of our study, we found that parental caregivers of youth with INS were particularly vulnerable to emotional burden after the diagnosis of their child. These stressors manifested themselves as memories of negative emotions that led to emotional distress, including hopelessness, shock, guilt, sadness, frustration. These findings are similar to other chronic disease studies showing symptoms of post-traumatic stress disorder in caregivers.28,29 Besides, the main emotional burden experienced by parental caregivers of INS youth was worry, which was related to the frequent relapses of the disease. Frequent relapses led to a strong sense of uncertainty among the parents of INS youth, and increase the risk of complications such as thrombosis, infections, malnutrition and dyslipidaemia.6 This observation in agreement with previous studies, which may adversely affect the health and physical and psychological well-being of parent caregivers and the INS youth they care for.30,31 Therefore, healthcare professionals should provide parental caregivers with stage-by-stage, targeted health education based on the actual condition of the child, and encourage parental caregivers to actively participate in treatment and care, so as to reduce the emotional and physical burden.
Regardless of their income levels, parental caregivers experienced heavy financial burden due to frequent hospitalizations and high medication costs. Although most patients had valid health insurance, many immunosuppressive agents and biologic agents were not covered by medical insurance. Moreover, even though parental caregivers of youth with INS face financial hardship, our study revealed that most families only had one income-earning member who was working. It has been shown in similar studies that parental caregivers and their families suffer greater financial losses and burdens as a result.32 The burdensome financial stress has a significant impact not only on the functioning of the family, but also on the quality of life of the parental caregivers, ultimately resulting in a reduction in the caregiver’s ability to care. Most parental caregivers stated that INS should be recognized as a disease of public health concern and the government should provide subsidies for routine medication and frequent hospitalizations. Similar findings have been reported in other studies.18,33 Liu et al stated that the government should help the disadvantaged groups to overcome their difficulties by establishing relevant laws and regulations.34
The absence of social support and relative social isolation of parental caregivers, particularly those who left jobs to serve as primary caregivers, was also reported in this study. In agreement with findings in other chronic diseases,35 our study demonstrated that stigmatization led parental caregivers to avoid social activities and social contact. Family stigma is prevalent in Chinese culture, which makes it even more difficult for parental caregivers of chronic diseases.36 In order to avoid feeling shameful and embarrassed, parental caregivers of INS youth avoid seeking assistance, further compounding the social burden on caregivers. The government should implement anti-discrimination policies and raise the level of public awareness through social media to ensure that patients and their parental caregivers are protected from explicit discrimination in public places. Moreover, limited family social activities and the absence of support systems increased the stress of parental caregivers caring for youth with INS. The stress of caring is exacerbated when the caregiver was in conflict with a spouse or other family member. As the care responsibilities are concentrated on a few family members or one primary caregiver, broken families or families with fewer members would encounter greater stress and burden. Meanwhile, in comparison with other developed regions, China lacks nephrology nurses in kindergartens, primary schools, and secondary schools.37 Thus, to improve the social support system for youth with INS, we propose, as a healthcare system, to selectively learn from the successful experiences of other countries, and to gradually implement training for school personnel and other personnel who interact with youth with INS.
Our study showed that there was an information asymmetry between healthcare providers and patients. Some participants expressed little confidence with their INS management and did not understand the disease. Cao et al have reported similar findings.38 As a consequence of inadequate parental knowledge on the disease course, early detection of relapse in youth may be delayed, leading to a delay in treatment.39 In the early stages of a diagnosis, it is critical to provide adequate information to parental caregivers and maintain good communication with them. It helps parental caregivers recognize potential problems in the future and reduce their burden of care.40 Consequently, medical staff should regularly conduct educational lectures and distribute knowledge brochures to raise parents’ awareness of the disease. When youth are discharged from the hospital, medical staff should patiently explain the precautions to be taken in activities, rest and medication, and give parental caregivers as much psychological support as possible to improve their confidence and provide a guarantee for long-term efficacy and prognosis.
Limitations
There are also limitations to this study. First, it should be noted that our results reflect only the perspective of the parental caregiver and are not accompanied by that of the patient. Perhaps independence does not reduce the overall burden of care, but rather transfers it to the patient. Second, most of the parental caregivers included in our study were female. Therefore, it is important to interpret the findings with caution. Third, in the process of translating Chinese to English, two bilingual experts who participated in the data analysis performed multiple checks to ensure that the translations were accurate. Due to cultural and linguistic differences, however, there is a possibility that subtle differences in the original linguistic expressions may have been lost.
Conclusion
Parental caregivers of INS youth encounter difficulties and burdens in caring for their children, such as persistent emotional burdens, heavy financial burdens and lack of social support. These hardships are linked with social isolation, high cost of disease treatment, information asymmetry, changes in economic sources, and disruption in normal family life. In spite of these burdens, there is no targeted intervention available to assist parental caregivers of youth with INS in China. By characterizing these common experiences, we can better prepare medical staff to support parental caregivers of INS youth as they adjust to medical management of INS at different stages, thereby improving their disease management capabilities.
Acknowledgments
The authors would like to thank the parents who participated in this study and completed the interviews.
Funding
This work was supported by Nantong University Natural Science Cross-disciplinary Project (Grant No.23ZH313), Shanghai Jiao Tong University Medical School Science and Technology Fund Project (Grant No. Jyh2106), Research Project of Nantong Municipal Health Commission (Grant No. MS2022009), 2023 Shanghai Children’s Hospital Hospital-level Project Nursing special (Grant No.2023HLZX06). Study sponsors were not involved in the design, collection, analysis, or interpretation of data, writing of the manuscript, or submission of the manuscript for publication of the study.
Disclosure
There are no conflicts of interest reported by the authors.
References
1. Eddy AA, Symons JM. Nephrotic syndrome in childhood. Lancet. 2003;362(9384):629–639. doi:10.1016/S0140-6736(03)14184-0
2. Noone DG, Iijima K, Parekh R. Idiopathic nephrotic syndrome in children. Lancet. 2018;392(10141):61–74. doi:10.1016/S0140-6736(18)30536-1
3. Chanchlani R, Parekh RS. Ethnic differences in childhood nephrotic syndrome. Front Pediatr. 2016;4:39. doi:10.3389/fped.2016.00039
4. Xiaoyun J. Multicenter survey of diagnostic and therapeutic status in Chinese childhood patients with steroid-sensitive, relaping/steroid-dependent nephrotic syndrome. Chin J Paediatr. 2014;52(03):194–200.
5. Zotta F, Vivarelli M, Emma F. Update on the treatment of steroid-sensitive nephrotic syndrome. Pediatr Nephrol. 2022;37(2):303–314. doi:10.1007/s00467-021-04983-3
6. Mattoo TK, Sanjad S. Current understanding of nephrotic syndrome in children. Pediatr Clin North Am. 2022;69(6):1079–1098. doi:10.1016/j.pcl.2022.08.002
7. Hahn D, Hodson EM, Willis NS, Craig JC. Corticosteroid therapy for nephrotic syndrome in children. Cochrane Database Syst Rev. 2015;2015(3):D1533.
8. Guha P, De A, Ghosal M. Behavior profile of children with nephrotic syndrome. Indian J Psychiat. 2009;51(2):122–126. doi:10.4103/0019-5545.49452
9. Prakash CT, Prakash CT, Shobha S, Kuldip K. Behavioral problems in children with steroid-sensitive nephrotic syndrome: an ignored aspect! Indian J Child Health. 2018;5(12):724–729. doi:10.32677/IJCH.2018.v05.i12.005
10. Hong L, Ji Z, Tao W, Yuting Y, Juan W. Progress in the study of psychological problems in children with nephrotic syndrome. J Nurse Train. 2011;26(17):1549–1551.
11. Selewski DT, Troost JP, Massengill SF, et al. The impact of disease duration on quality of life in children with nephrotic syndrome: a midwest pediatric nephrology consortium study. Pediatr Nephrol. 2015;30(9):1467–1476. doi:10.1007/s00467-015-3074-x
12. Rüth EM, Landolt MA, Neuhaus TJ, Kemper MJ. Health-related quality of life and psychosocial adjustment in steroid-sensitive nephrotic syndrome. J Pediatr. 2004;145(6):778–783. doi:10.1016/j.jpeds.2004.08.022
13. Juanjuan Y, Ying C, Jinrui C. Relationship between quality of life and family management status among children with nephrotic syndrome. J Nurs Sci. 2017;32(09):20–22.
14. Lo CE, Amir N, McKay A, Durkan AM. Parental understanding of relapsing idiopathic nephrotic syndrome-Where are the knowledge gaps? Acta Paediatr. 2020;109(7):1465–1472. doi:10.1111/apa.15111
15. Zhuo W, Yanhui L, Lei Z, Jiangbing M. Analysis of the correlation between the quality of life of children with nephrotic syndrome and their family factors. J Med Colle People Liber Army. 2014;35(02):153–156.
16. Liu Y, Yuming L, Xiaodan Z. Survey and analysis of psychological characteristics and stress coping ability of parents of children with nephrotic syndrome. Health Professions Educ. 2018;36(05):107–108.
17. Wenli Z, Yongai Z, Lu Z. Parents of children with nephrotic syndrome investigation and analysis of psychological characteristics and stress coping ability. China Mater Child Health Res. 2017;28(10):1174–1176.
18. Yeqing D, Wanhua X. Qualitative study on true experience of caregivers of pre-school children with nephrotic syndrome. Nurs Res. 2013;27(14):1307–1309.
19. Ling D, Shenghua W, Lanzheng B, Shengying G. Behavior problem, family environment and quality of parents’ life in children with nephrotic syndrome. Chin Ment Health J. 2004;10:702–704.
20. Li N, Hao J, Fu T, Du Y. Evaluating the quality of life of 231 children with primary nephrotic syndrome and assessing parental awareness of the disease. Front Pediatr. 2021;9:745444. doi:10.3389/fped.2021.745444
21. Zeng Y, Du Y. Analysis of health-related quality of life in children with primary nephrotic syndrome. Chin General Med. 2022;25(27):3379–3383.
22. Feng S, Abulaiti GK, Ying L, Abbas AG. Mediating effect of coping style on parental resilience and caregiving ability in children with nephrotic syndrome. Zhejiang Med J. 2023;45(09):939–944.
23. Jinrong W, Meiyu Z, Yunxia L, Ming’E L, Junfang G. Analysis of parenting stress among parents of children with nephrotic syndrome and its influencing factors. General Pract Nurs. 2022;20(26):3705–3710.
24. Vishnevsky T, Beanlands H. Qualitative research. Nephrol Nurs J. 2004;31(2):234–238.
25. Green CA, Duan N, Gibbons RD, Hoagwood KE, Palinkas LA, Wisdom JP. Approaches to mixed methods dissemination and implementation research: methods, strengths, caveats, and opportunities. Adm Policy Ment Health. 2015;42(5):508–523. doi:10.1007/s10488-014-0552-6
26. Rovin BH, Adler SG, Barratt J, et al. Executive summary of the KDIGO 2021 guideline for the management of glomerular diseases. Kidney Int. 2021;100(4):753–779. doi:10.1016/j.kint.2021.05.015
27. Ming L. Application of colaizzi’s seven steps in analysing data for phenomenological research. J Nur. 2019;34(11):90–92.
28. Zimmerman K, May B, Barnes K, et al. Post-traumatic stress symptoms in caregivers and children with hydrocephalus. World Neurosurg. 2021;148:e66–e73. doi:10.1016/j.wneu.2020.12.008
29. Beaudoin W, Moore H, Bliss L, Souster J, Mehta V. Prevalence of post-traumatic stress disorder in caregivers of pediatric neurosurgical patients. Childs Nerv Syst. 2021;37(3):959–967. doi:10.1007/s00381-020-04938-3
30. Li W, Yan C. A study of the correlation between illness uncertainty and coping styles of parents of children with nephrotic syndrome. Nurs Pract Res. 2017;14(16):98–99.
31. Weihong Y, Li Z, He Z. Analysis of the correlation between disease uncertainty and psychological symptoms in parents of children with primary nephrotic syndrome. J Nurs Sci. 2017;24(01):53–56.
32. Jinrong W, Min Z, Junfang G, Ming’E L. A study to investigate the current status of parenting stress among parents of children with nephrotic syndrome. J Binzhou Med Colle. 2019;42(01):33–35.
33. Mei Z. Impact of hospital-acquired infections in nephrotic syndrome on patients’ hospitalisation costs, medication costs and length of hospital stay. Chin J Hosp Infect. 2009;19(15):2003.
34. Mei W. Anxiety status and influencing factors of primary caregivers of children with frequently recurrent nephrotic syndrome. Nurs Integr Trad Chin West Med. 2018;4(12):46–51.
35. Ng C, Ng S. A qualitative study on the experience of stigma for Chinese parents of children with autism spectrum disorder. Sci Rep. 2022;12(1):19550. doi:10.1038/s41598-022-23978-0
36. Hsiao CY, Tsai YF. Factors of caregiver burden and family functioning among Taiwanese family caregivers living with schizophrenia. J Clin Nurs. 2015;24(11–12):1546–1556. doi:10.1111/jocn.12745
37. Chunmei Z. Focusing on the challenge of the shortage of paediatric nurses. Beiji Observa. 2019;8:38.
38. Xuehong C, Shuanchun W, Ru J, Jieqiong J, Xiaobi R. Analysis of the cognitive status of disease-related knowledge of parents of children with recurrent nephrotic syndrome and the factors affecting it. J Nurs Sci. 2010;17(01):13–15.
39. Diong SC, Syed ZS, Rasat R, Wan IW. Parental knowledge on nephrotic syndrome and disease relapse in children. Med J Malaysia. 2019;74(4):288–295.
40. Hang P. Survey analysis on health knowledge perception and needs of outpatients with primary nephrotic syndrome. Contempor Nurse. 2012;1:106–107.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.