Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Bullous Pemphigoid Possibly Induced by Deucravacitinib in a Patient with Psoriasis
Authors Lu X, Zhang Y, Zhang H ![]() , Tang K, Jin H
, Tang K, Jin H
Received 6 March 2026
Accepted for publication 30 April 2026
Published 26 May 2026 Volume 2026:19 606758
DOI https://doi.org/10.2147/CCID.S606758
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Michela Starace
Xinyi Lu,* Yuqiao Zhang,* Hanlin Zhang, Keyun Tang, Hongzhong Jin
Department of Dermatology, State Key Laboratory of Complex Severe and Rare Diseases, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hongzhong Jin, Department of Dermatology, State Key Laboratory of Complex Severe and Rare Diseases, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing, People’s Republic of China, Email [email protected]
Abstract: While bullous pemphigoid (BP) can be induced by various drugs, cases involving small-molecule inhibitors remain rare. We report the first case of BP occurring in a patient with psoriasis shortly after receiving deucravacitinib, a TYK2 inhibitor. Following treatment with methylprednisolone, minocycline, and ixekizumab, the lesions resolved within one month. Although the precise mechanism remains unclear, it may involve immunological drift and remodeling of skin immune microenvironment, which raises the need for clinical awareness regarding such reactions when using novel targeted immunomodulators.
Keywords: bullous pemphigoid, deucravacitinib, psoriasis, TYK2 inhibitor
Introduction
Bullous pemphigoid (BP) is an autoimmune blistering disorder that can be triggered by various medications, such as immune checkpoint inhibitors and dipeptidyl peptidase-4 (DPP-4) inhibitors.1 Certain biologics used in psoriasis treatment, including adalimumab and ustekinumab, have also been reported to be potential triggers of BP.2 We present the first case of BP possibly induced by deucravacitinib in a patient with psoriasis.
Case Report
A 35-year-old male presented to our outpatient clinic with newly developed blisters and bullae on the trunk and upper limbs. He had a history of psoriasis for over ten years and intermittently received traditional Chinese medicines for treatment, but the lesions relapsed repeatedly. The patient denied any medication use in the past six months. In September 2025, he initiated deucravacitinib treatment at a local hospital. One week later, while the pre-existing lesions showed no significant improvement, he developed pruritic blisters on the trunk and upper limbs. The patient subsequently discontinued deucravacitinib, but the blisters progressed continuously, leading to his visit to our center.
The patient weighed 100 kg (BMI 29.2 kg/m2). Physical examination revealed tense blisters on an erythematous base over the chest, abdomen, waist, and bilateral upper extremities (Figure 1). Erosions, crusts, and hemorrhagic bullae were observed. BP Disease Area Index (BPDAI) activity score was 27. Some erythematous plaques were covered with scale. Psoriatic plaques were present on scalp, elbows, back, waist, and lower limbs, with a psoriasis area and severity index (PASI) score of 13.6. No joint involvement was identified.
 |
Figure 1 Skin lesions in the patient treated with deucravacitinib for psoriasis. Multiple blisters and bullae on an erythematous base over the chest (A), back (B) and waist (C), accompanied by scattered psoriatic lesions (D). |
Laboratory tests, including complete blood count and biochemistry, were within normal limits. Histopathological examination demonstrated a subepidermal blister and infiltration of eosinophils within the blister cavity and surrounding blood vessels in the superficial dermis (Figure 2A). Direct immunofluorescence of perilesional erythematous skin showed linear deposition of C3 along the basement membrane zone, while IgG/IgA/IgM were negative (Figure 2B). Indirect immunofluorescence revealed a linear deposition pattern with a titer of ≥1:320. Autoantibody tests revealed elevated anti-BP180 and anti-BP230 antibodies. Anti-p200 antibody test was negative. These findings confirmed the diagnosis of BP.
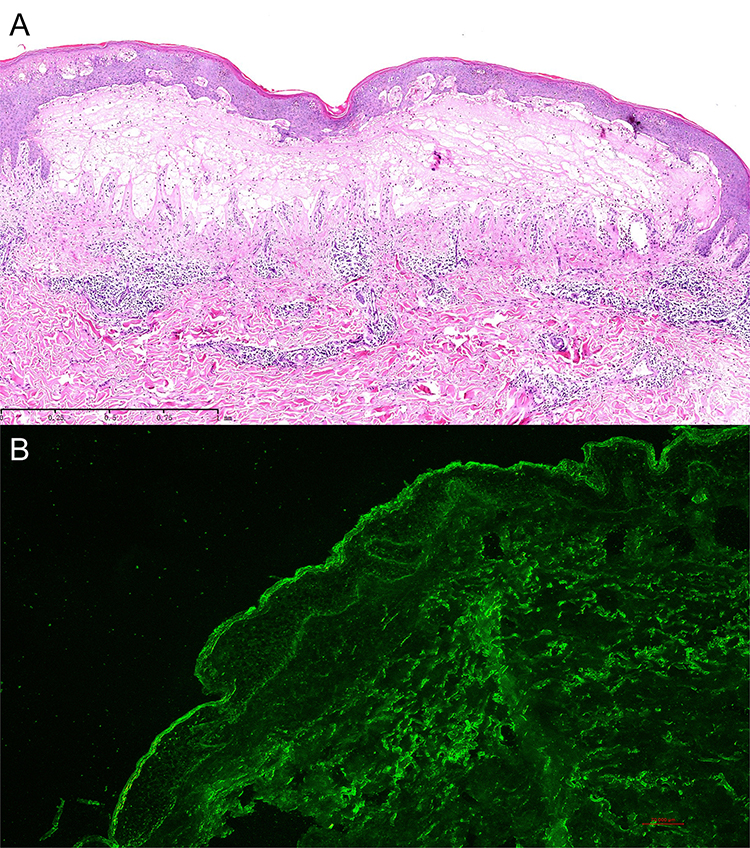 |
Figure 2 Histopathological and direct immunofluorescence findings. (A) Hematoxylin and eosin staining of a skin biopsy showed subepidermal blister formation with eosinophils infiltrates in the superficial dermis. (B) Direct immunofluorescence demonstrated linear C3 deposition along the basement membrane zone. |
The patient received methylprednisolone (32 mg daily), minocycline, and nicotinamide for BP, combined with ixekizumab for psoriasis. At the one-month follow-up, methylprednisolone was tapered to 8 mg daily, and other therapies were continued. Physical examination showed that blisters had dried and resolved without new lesions (Figure 3).
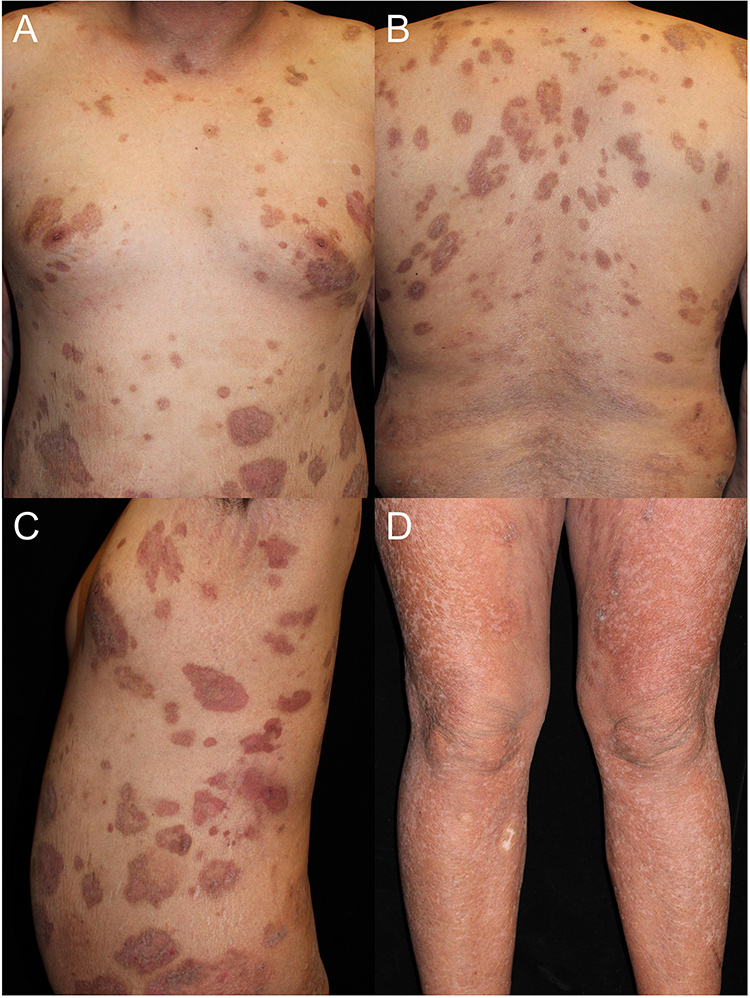 |
Figure 3 Post-treatment follow-up at one month. Resolution of blisters with residual hyperpigmentation on chest (A), back (B) and waist (C). Psoriasis was also improved (D). |
Discussion
To our knowledge, this is the first reported case of BP possibly triggered by deucravacitinib in a patient with psoriasis. In this case, the Naranjo score was calculated as 3, suggesting a possible association between deucravacitinib and BP. Deucravacitinib, a selective tyrosine kinase 2 (TYK2) inhibitor, acts by inhibiting the JAK-STAT pathways involved in psoriasis pathogenesis.3 Interestingly, recent studies suggest that JAK inhibitors are emerging as potential therapies for BP.4,5 This presents a paradoxical phenomenon where the medication may both induce and treat BP, complicating the exploration of underlying mechanism.
Certain biologics, including TNF-α inhibitors, IL-12/23 antagonists, and IL-17 antagonists, exhibit this dual potential.2 While they are used to treat refractory BP, particularly in patients with comorbid psoriasis, they have also been reported to trigger new-onset BP. Notably, many patients who develop drug-induced BP were younger than the typical onset age of spontaneous BP.2 Our patient also aligns with this clinical profile, suggesting that age might be a potential risk factor.
TYK2 mainly mediates signaling for cytokines such as IL-23, IL-12, and type I interferons.6 Therefore, one hypothesis is that the inhibition of TYK2 by deucravacitinib may disrupt the Th1/Th17-Th2 balance, potentially leading to relative Th2 predominance and contributing to the development of BP.7 However, TYK2 is also involved in IL-4/IL-13-related signaling pathways and can partially inhibit Th2 responses as well.8 Therefore, a simple Th1/Th2 immune drift is insufficient to fully explain the development of BP in this case. We speculate that the long-term uncontrolled psoriasis and persistent cutaneous inflammation may have promoted the exposure of autoantigens such as BP180 and BP230, predisposing the patient to BP.9 Deucravacitinib may then have further altered the immune microenvironment through broader cytokine network remodeling, ultimately triggering the disease onset.
In this case, Ixekizumab was selected for the treatment of psoriasis for several reasons. First, it can provide rapid disease control.10 Second, compared with other biologics used for psoriasis, IL-17 inhibitors have been associated with fewer reported cases of BP, suggesting a relatively lower risk of BP induction.2 In addition, systemic corticosteroids were simultaneously administered to suppress the inflammatory response and reduce the disease activity of BP.
Conclusion
Our case highlights the need for monitoring paradoxical autoimmune reactions during treatment with novel targeted immunomodulators. Individualized risk-benefit assessment could be made in patients with chronic psoriatic lesions before initiating TYK2 inhibitors. However, as a single case report, the causal relationship between deucravacitinib and BP cannot be firmly established, and our observation does not alter the overall safety and therapeutic benefit of deucravacitinib. Future large-scale studies could investigate the incidence and precise mechanisms of such paradoxical immune reactions.
Abbreviations
BP, bullous pemphigoid; DPP-4, dipeptidyl peptidase-4; BPDAI, Bullous Pemphigoid Disease Area Index; PASI, psoriasis area and severity index; TYK2, tyrosine kinase 2.
Data Sharing Statement
The data are not publicly available due to ethical restrictions. Further inquiries can be directed to the corresponding author.
Ethics Approval and Informed Consent
The patient in this manuscript has given written informed consent to the publication of the case details, including the images. Additional institutional approval of Peking Union Medical College Hospital was not required to publish the case details.
Funding
This study was supported by National High Level Hospital Clinical Research Funding (2022-PUMCH-B-092), Beijing Key Clinical Specialty Construction Project, and National Key Clinical Specialty Project of China.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ujiie H. What’s new in the pathogeneses and triggering factors of bullous pemphigoid. J Dermatol. 2023;50(2):140–5. doi:10.1111/1346-8138.16654
2. Husein-ElAhmed H, Steinhoff M. Bullous pemphigoid induced by biologic drugs in psoriasis: a systematic review. J Dermatolog Treat. 2022;33(7):2886–2893. doi:10.1080/09546634.2022.2089331
3. Armstrong AW, Lebwohl M, Warren RB, et al. Safety and efficacy of deucravacitinib in moderate to severe plaque psoriasis for up to 3 years: an open-label extension of randomized clinical trials. JAMA Dermatol. 2025;161(1):56–66. doi:10.1001/jamadermatol.2024.4688
4. Jiang W, Ma X, Guo T, Song M, Zhang J. Abrocitinib-A promising option for patients with refractory bullous pemphigoid. J Eur Acad Dermatol Venereol. 2024;38(1):e119–e121. doi:10.1111/jdv.19475
5. Hu YQ, Zhang JZ, Zhao Y. Successful treatment of concurrent bullous pemphigoid and psoriasis vulgaris with abrocitinib: a case report and literature review. Clin Cosmet Investig Dermatol. 2026;19:566664. doi:10.2147/CCID.S566664
6. Estevinho T, Lé AM, Torres T. Deucravacitinib in the treatment of psoriasis. J Dermatolog Treat. 2023;34(1):2154122. doi:10.1080/09546634.2022.2154122
7. Takamura S, Teraki Y. Treatment of bullous pemphigoid with dupilumab: dupilumab exerts its effect by primarily suppressing T-helper 2 cytokines. J Dermatol. 2022;49(9):845–850. doi:10.1111/1346-8138.16428
8. Jensen LT, Attfield KE, Feldmann M, Fugger L. Allosteric TYK2 inhibition: redefining autoimmune disease therapy beyond JAK1-3 inhibitors. EBioMedicine. 2023;97:104840. doi:10.1016/j.ebiom.2023.104840
9. Maronese CA, Cassano N, Genovese G, Foti C, Vena GA, Marzano AV. The Intriguing Links between Psoriasis and Bullous Pemphigoid. J Clin Med. 2022;12(1):328. doi:10.3390/jcm12010328
10. Egeberg A, Andersen YMF, Halling-Overgaard AS, et al. Systematic review on rapidity of onset of action for interleukin-17 and interleukin-23 inhibitors for psoriasis. J Eur Acad Dermatol Venereol. 2020;34(1):39–46. doi:10.1111/jdv.15920
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effectiveness and Safety of Deucravacitinib for the Management of Psoriasis: A Review of the Current Literature
Potestio L, Ruggiero A, Fabbrocini G, Martora F, Megna M
Psoriasis: Targets and Therapy 2023, 13:19-26
Published Date: 4 May 2023
Adverse Events Associated with Apremilast and Deucravacitinib for Psoriasis: A Pharmacovigilance Study Based on the FAERS Database
Xu Y, Liu X, Guo L, Jiang X
Clinical, Cosmetic and Investigational Dermatology 2025, 18:1121-1135
Published Date: 5 May 2025
Successful Treatment of Concurrent Bullous Pemphigoid and Psoriasis Vulgaris with Abrocitinib: A Case Report and Literature Review
Hu YQ, Zhang JZ, Zhao Y
Clinical, Cosmetic and Investigational Dermatology 2026, 19:566664
Published Date: 27 January 2026
The Impact of Targeted Therapies on the Bone-Vascular Axis in Psoriasis: A Narrative Review
Zeng H, Chen Y, Yang L
Clinical, Cosmetic and Investigational Dermatology 2026, 19:595065
Published Date: 1 April 2026