Back to Journals » Infection and Drug Resistance » Volume 15
Brucellar Knee Arthritis with Knee Joint Tuberculosis: A Case Report and Review of the Literature
Authors Wang J ![]() , Li S
, Li S ![]() , Zhang Q
, Zhang Q
Received 24 January 2022
Accepted for publication 26 March 2022
Published 8 April 2022 Volume 2022:15 Pages 1659—1665
DOI https://doi.org/10.2147/IDR.S359693
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Jie Wang, Shuguang Li, Qiang Zhang
Department of Orthopedics, Beijing Ditan Hospital, Capital Medical University, Beijing, 100015, People’s Republic of China
Correspondence: Qiang Zhang, Email [email protected]
Abstract: Brucella and Mycobacterium tuberculosis (MTB) primarily affect the spine and only rarely the knee joint in osteoarticular disease in adults. We present an unusual instance of brucellar knee arthritis combined with knee joint tuberculosis. A 59-year-old man was initially diagnosed with brucellar knee arthritis in the orthopedics department of our hospital, while two weeks of standardized treatment did not improve the joint discomfort and inflammation indexes. Subsequent evaluation of serum tuberculosis interferon-gamma release assays (TB-IGRAs) and the effectiveness of empirical anti-tuberculosis therapy confirmed the mixed infection of tuberculosis. This case report demonstrates that clinical signs and imaging for brucellar knee arthritis and knee joint tuberculosis are similar. Patients with both disorders are more likely to be misdiagnosed or have their diagnosis delayed; clinicians should be aware of this uncommon combination of mixed infections.
Keywords: brucellar knee arthritis, knee joint tuberculosis, mixed infections, case report
Introduction
Brucellosis is endemic to Australia, India, the Mediterranean region, and northern China, a zoonosis transmitted predominantly by sheep and through cattle and pigs.1 As an intracellular parasite, Brucella is ingested by phagocytes and reproduces continuously after entering the organism; when the human immunity is low, the bacteria can be released into the bloodstream and cause brucellosis.1 Patients with brucellosis have a rate of osteoarticular system involvement ranging from 10% to 85%, and the spine is usually infected with infection of the knee joint unusual in adults.2 Globally, tuberculosis is the leading cause of health problem, particularly in developing countries; inflammation, bacterial toxicity, immune damage, and bacterial proliferation are possible causes of tuberculosis caused by MTB.3 MTB causes tuberculosis, which primarily affects the respiratory system; extrapulmonary tuberculosis is less common; again, the spine is the most prevalent location for osteoarticular tuberculosis in adults, followed by the knee joint.4 Here, we present an unusual adult case of concomitant brucellar and tubercular knee joint septic arthritis.
Case Presentation
A 59-year-old male patient presented to the orthopaedic department of our institution with a 5-month history of left-knee pain and more recent activity restrictions for 10 days. This patient, an electrician, had worked around the sheepfold 10 months before, developing transient fever and fatigue with subsequent symptoms improvement after taking anti-inflammatory medication. The patient then developed knee pain, which worsened progressively. Serum agglutination test (SAT) was positive (1:160) in the local hospital, and he was transferred to our institution for further treatment.
The patient’s core temperature was 38.3°C on admission. Physical examination showed a left knee joint that was obviously swollen with a positive floating patella test, active flexion and extension of left-knee joint were limited. Blood parameters revealed white blood count (WBC) 8.47×109/L with lymphocytosis, erythrocyte sedimentation rate (ESR) 72 mm/hr and C-reactive protein (CRP) 66.2 mg/L. The biochemical tests were all normal. Immunological tests showed that Rose Bengal Plate Agglutination Test (RBPT) and SAT (1:200) were positive and serum anti-tuberculosis antibody test was negative. X-ray film of the left-knee joint showed patchy osteopaenia of the distal femur and proximal tibia without obvious joint space narrowing (Figure 1A and B). Magnetic resonance imaging (MRI) showed associated bone marrow with diffuse patchy abnormal signal on T2-weighted imaging (T2WI), local full-thickness defect of patellar cartilage and knee joint synovitis (Figure 1C–E). X-ray and computerized tomography (CT) of the chest showed no evidence of pulmonary involvement or enlarged mediastinal lymph nodes. A presumed diagnosis of brucellar knee arthritis was made. The left knee joint underwent arthrotomy, sampling of discoloured joint fluid and irrigation. Aspirate was culture-negative; however, Brucella melitensis (B. melitensis) was detected by real-time polymerase chain reaction (Figure 2). HE staining of knee joint effusion and inflammatory tissue revealed inflammatory cell infiltration, while acid-fast staining was negative (Figure 3A and B). Combination therapy with rifampicin (0.6 g po qd; Guangdong Hengjian Pharmaceuticals), doxycycline (0.1 g po bid; Jiangsu Lianhuan Pharmaceuticals) and cefotaxime-sulbactam (2.25 g ivgtt q8h; Xiangbei Weierman Pharmaceuticals) were administered post-operatively.
 |
Figure 1 On admission to the hospital, X-ray and MRI images were taken of the left knee joint. (A and B) An X-ray of the distal femur and the proximal tibia revealed patches of osteopenia (blue circle). (C–E) There was a synovial infection in the knee joint, a localized full-thickness defect in the patellar cartilage (red arrow), and a diffuse patchy signal in the bone marrow on T2-weighted imaging (red circle). |
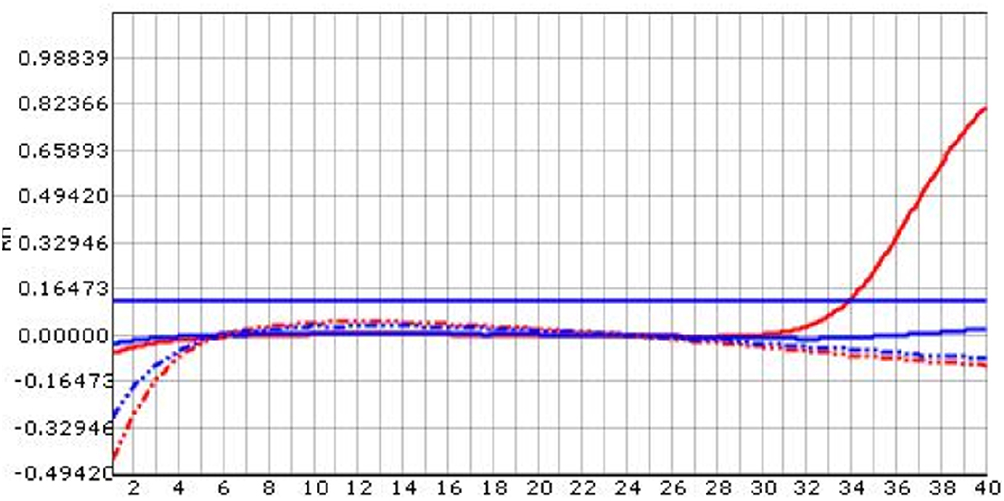 |
Figure 2 Brucella melitensis was detected by real-time PCR, real-time PCR showed that the DNA content of Brucella melitensis (Solid red line) increased in 32 cycles. |
 |
Figure 3 Pathological staining of knee joint effusion and inflammatory tissue. (A) Inflammatory cell infiltration was seen by HE staining. (B) Acid-fast staining was negative. |
Left knee joint symptoms did not improve after two weeks of anti-brucellosis treatment. Inflammatory indexes did not diminish significantly (ESR 68mm/hr, CRP 66.1mg/L). Subsequently, knee joint tuberculosis was considered when serum TB-IGRAs were positive. Empirical anti-tuberculosis medications with isoniazid (0.3 g po qd; Shenyang Hongqi Pharmaceuticals), ethambutol (1 g po qd; Guangzhou Baiyunshan Pharmaceuticals) and pyrazinamide (0.5 g po tid; Chongqing Huabang Pharmaceuticals) were added.
Within three days, the pain in the left knee improved, CRP fell to 29.40 mg/L and ESR to 60mm/hr. Symptoms continued to settle and the patient was discharged from hospital 10 days later. Anti-brucellosis therapy was maintained for 5 months after discharge: rifampicin (0.6 g po qd; Guangdong Hengjian Pharmaceuticals) and doxycycline (0.1 g po bid; Jiangsu Lianhuan Pharmaceuticals). Anti-tuberculosis therapy was maintained for 9 months in all: 3-month intensive therapy and 6-month consolidation therapy), 3-month intensive therapy includes rifampicin (0.6 g po qd; Guangdong Hengjian Pharmaceuticals), isoniazid (0.3 g po qd; Shenyang Hongqi Pharmaceuticals), ethambutol (1 g po qd; Guangzhou Baiyunshan Pharmaceuticals), pyrazinamide (0.5 g po tid; Chongqing Huabang Pharmaceuticals) and 6-month consolidation therapy includes rifampicin (0.6 g po qd; Guangdong Hengjian Pharmaceuticals), isoniazid (0.3 g po qd; Shenyang Hongqi Pharmaceuticals). Symptoms were completely resolved and inflammatory indexes were normal at the end of treatment.
At last follow-up five years later, the patient had no discomforts in the left knee. X-ray showed resolution of previous abnormal X-ray appearances of the distal femur and proximal tibia (Figure 4A and B). MRI changes were also largely resolved (Figure 4C–E). Blood tests showed WBC of 6.28× 109/L with no lymphocytosis, CRP 3.9mg/L, ESR 7mm/hr. The results of all the biochemical tests were normal. Immunological tests including serum anti-tuberculosis antibody, TB-IGRA, RBPT and SAT were all negative.
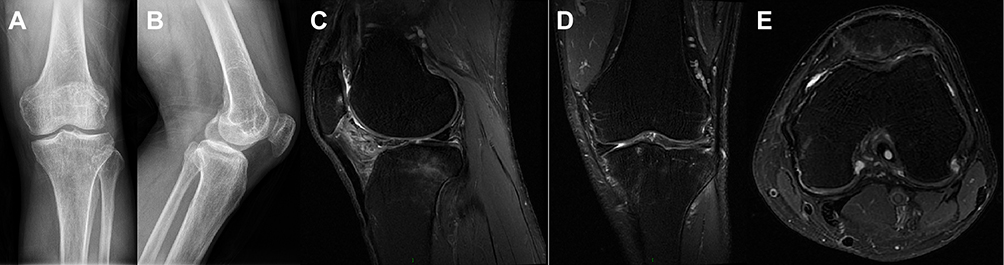 |
Figure 4 After five years, X-rays and MRI scans of the left knee joint were taken. (A and B) The X-rays showed that the distal femur and proximal tibia had resolved from the previous abnormal X-ray appearances. (C–E) It was also noted that the MRI changes were largely resolved. |
Discussion
Concomitant infection with Brucella and MTB has only been recorded in one instance: a patient with brucellar spondylitis and spinal tuberculosis;5 however, no case of brucellosis with tuberculosis of the knee joint has been described. There are only four cases of mixed infections of knee joint tuberculosis to date (Table 1). Most cases of Brucella infection are caused by skin and mucous membrane injury followed by the consumption of contaminated meat or dairy products; Brucella may also spread via the respiratory tract, blood transfusion, and placental transmission.10–12 The patient in our report had no direct contact with a zoonotic source of infection and was presumably infected with Brucella via the respiratory system. The rarity of mixed infections, unusual infectious sites, and unusual transmission methods are features of this case.
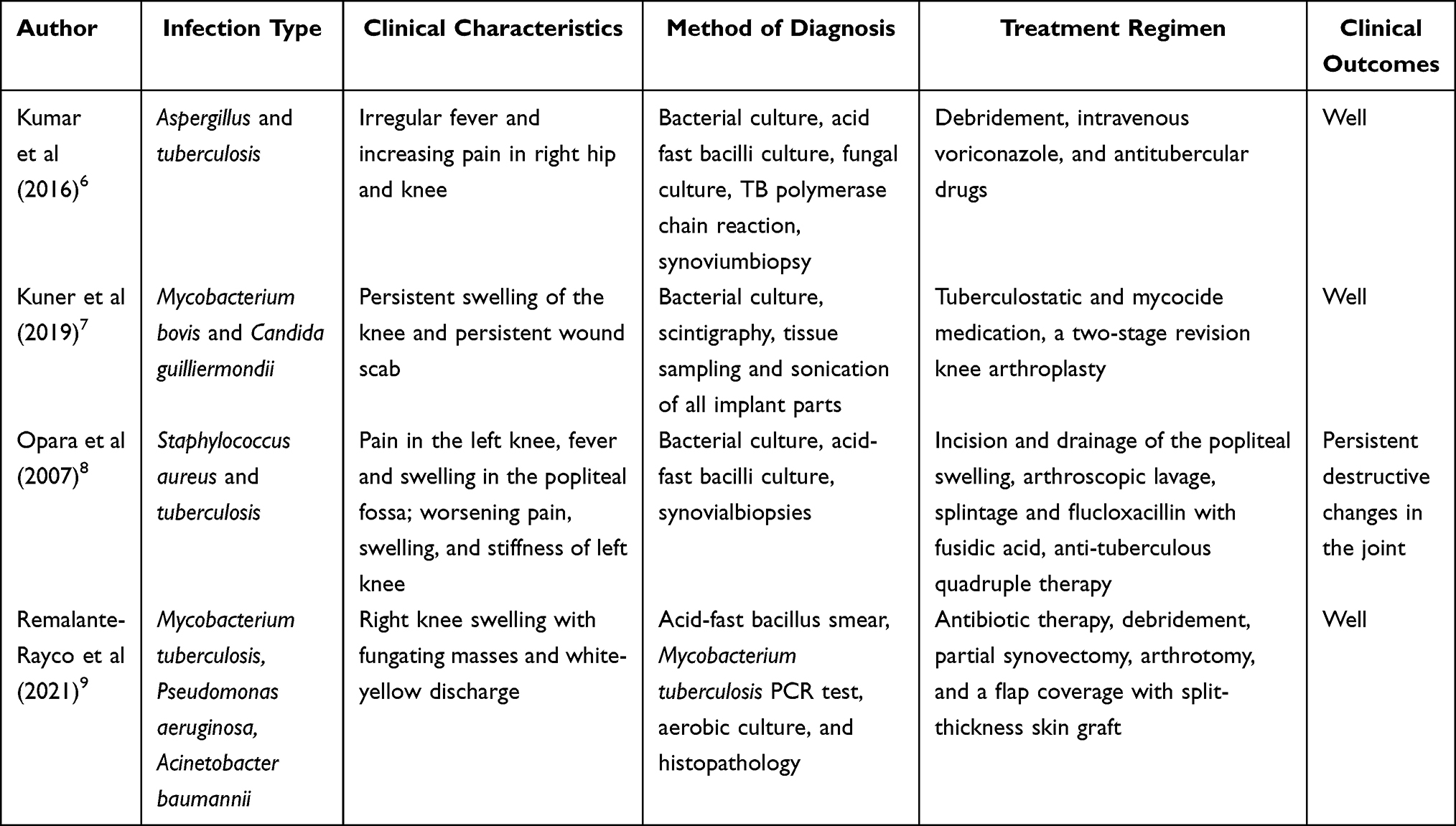 |
Table 1 Literature Review of Knee Joint Tuberculosis with Mixed Infections |
Bacterial isolates from blood, bone marrow, synovial fluid, and other tissues are the gold standards in diagnosing brucellosis, but positive bacterial culture is challenging to achieve in chronic disease, so real-time polymerase chain reaction (real-time PCR) is the usual detection method.13,14 The WBC count is often average or low, and lymphocyte count is increased in most patients; ESR is increased in the acute phase of the disease, yet is generally normal in the chronic phase.15,16 Immunological tests such as RBPT and SAT have significant diagnostic value, SAT titer ≥1:160 is highly suggestive of Brucella infection.13
Rifampicin and doxycycline are the most often-utilized drugs in the acute phase of brucellosis, whereas rifampicin, doxycycline, and fluoroquinolones/third-generation cephalosporins are more commonly used in chronic or refractory infections.17,18 It is possible to lower the risk of recurrence by continuing the course of medication beyond three months in patients with bone and joint system involvement.19 During the 5-year follow-up period, no recurrence of the infection was seen in our patient treated with a triple regimen of rifampicin, doxycycline, and cefotaxime-sulbactam for half a year.
Research on extrapulmonary tuberculosis is mostly reported in developed countries, with fewer studies conducted in developing and undeveloped nations.20,21 Recent studies indicate that extrapulmonary tuberculosis may be rising in China, a phenomenon that should be noted by physicians treating infectious diseases.4,22,23
The local symptoms (pain, swelling, joint dysfunction) and systemic symptoms (fever, fatigue, hyperhidrosis) in patients with osteoarticular tuberculosis are similar to those of brucellosis when the osteoarticular system is involved, and there are no specific differences in imaging findings; thus, misdiagnosis or delayed diagnosis is common.5 TB-IGRA is represented by T-SPOT. TB assay (T-SPOT) and GeneXpert MTB/RIF (Xpert) have a higher detective efficiency for extrapulmonary tuberculosis, T-SPOT has higher sensitivity, and Xpert has higher specificity. However, T-SPOT cannot distinguish between active tuberculosis, latent infection, and previous infection, the World Health Organisation (WHO) recommends the application of Xpert in the diagnosis of extrapulmonary tuberculosis.24,25 The accuracy of Xpert and T-SPOT in early diagnosis of osteoarticular tuberculosis is higher than other tests, such as serum anti-tuberculosis antibody test.26,27 A negative result of serum anti-tuberculosis antibody test led to an early missed diagnosis of knee joint tuberculosis in this case. Two weeks of anti-brucellosis medications did not relieve knee joint symptoms, and only a positive T-SPOT, a negative chest CT, and the effectiveness of empirical anti-tuberculosis therapy confirmed left-knee joint tuberculosis. A high index of suspicion, in conjunction with wide-ranging diagnostic methods, should be combined to reduce the occurrence of misdiagnosis and delayed diagnosis in practical work.
The chemotherapy regimen for bone and joint tuberculosis is divided into short-term chemotherapy (6 months) and long-term chemotherapy (≥9 months). There is no consensus on the time required for chemotherapy in bone and joint tuberculosis patients due to the lack of large-scale and multicenter studies in developing countries. However, most centers continue to use long-term chemotherapy regimens.28,29 Aryal et al29 compared the efficacy of short-term treatment and long-term treatment in patients with spinal tuberculosis; the results showed no significant difference in curative rates of relapse between the two regimens. In this article, the patient was treated with a 9-month chemotherapy regimen: 3-month intensive therapy (isoniazid, rifampicin, pyrazinamide, ethambutol) and 6-month consolidation therapy (isoniazid, rifampicin). There were no adverse drug reactions during chemotherapy and no recurrence during follow-up for five years.
Extrapulmonary tuberculosis tests have a high false-negative rate.30 Even if tuberculosis-related tests are negative, knee joint tuberculosis should be considered if long-term anti-brucellosis medications are ineffective in individuals with brucellar knee arthritis. Brucellar knee arthritis and knee joint tuberculosis overlap in the use of rifampicin treatment, but the use of an anti-brucellar regime cannot achieve a cure for tuberculosis.17,29 Delayed diagnosis and treatment will not arrest the progression of knee joint tuberculosis.
Conclusion
In conclusion, brucellar knee arthritis with knee joint tuberculosis is unusual in clinical practice. The symptoms, signs, and imaging examinations of these two diseases are very similar. Clinicians should be aware of the potential for this uncommon combination of infections so that they can avoid misdiagnosis or delayed diagnosis.
Statement
The patient provided informed consent for publication of the case. No ethics committee approval was required for this study as the data had been analyzed in a retrospective manner.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work received no funding.
Disclosure
The authors have no conflicts of interest to declare in this work.
References
1. Głowacka P, Żakowska D, Naylor K, Niemcewicz M, Bielawska-Drózd A. Brucella - virulence factors, pathogenesis and treatment. Pol J Microbiol. 2018;67(2):151–161. doi:10.21307/pjm-2018-029
2. Alp E, Doganay M. Current therapeutic strategy in spinal brucellosis. Int J Infect Dis. 2008;12(6):573–577. doi:10.1016/j.ijid.2008.03.014
3. Rowland JL, Niederweis M. Resistance mechanisms of Mycobacterium tuberculosis against phagosomal copper overload. Tuberculosis. 2012;92(3):202–210. doi:10.1016/j.tube.2011.12.006
4. Fan J, An J, Shu W, et al. Epidemiology of skeletal tuberculosis in Beijing, China: a 10-year retrospective analysis of data. Eur J Clin Microbiol Infect Dis. 2020;39(11):2019–2025. doi:10.1007/s10096-020-03924-6
5. Zou D, Zhou J, Jiang X. Diagnosis and management of spinal tuberculosis combined with brucellosis: a case report and literature review. Exp Ther Med. 2018;15(4):3455–3458. doi:10.3892/etm.2018.5812
6. Kumar M, Thilak J, Zahoor A, Jyothi A. Septic arthritis due to tubercular and Aspergillus co-infection. Indian J Orthop. 2016;50(3):327–330. doi:10.4103/0019-5413.181783
7. Kuner E, Jöckel JA, Orler R, Nüesch R. Periprosthetic knee infection by Mycobacterium bovis and Candida guilliermondii in the context of a zoonosis: a case report and review of the literature. J Med Case Rep. 2019;13(1):54. doi:10.1186/s13256-019-2009-8
8. Opara TN, Gupte CM, Liyanage SH, Poole S, Beverly MC. Tuberculous arthritis of the knee with Staphylococcus superinfection. J Bone Joint Surg Br. 2007;89(5):664–666. doi:10.1302/0301-620X.89B5.18462
9. Remalante-Rayco PP, Dumlao PIE, Santiago AT. Great imitator: an unusual presentation of osteoarticular tuberculosis of the knee with gram-negative bacterial arthritis. BMJ Case Rep. 2021;14(11):e245583. doi:10.1136/bcr-2021-245583.112-4
10. Zheng R, Xie S, Lu X, et al. A systematic review and meta-analysis of epidemiology and clinical manifestations of human brucellosis in China. Biomed Res Int. 2018;2018:5712920. doi:10.1155/2018/5712920
11. Tuon FF, Gondolfo RB, Cerchiari N. Human-to-human transmission of brucella - a systematic review. Trop Med Int Health. 2017;22(5):539–546. doi:10.1111/tmi.12856
12. Xu D, Li X, Cheng B, et al. Congenital brucellosis: a case report. Vector Borne Zoonotic Dis. 2021;21(9):727–730. doi:10.1089/vbz.2021.0015
13. Alişkan H. Kültür ve serolojik yöntemlerin insan brusellozu tanisindaki değeri [The value of culture and serological methods in the diagnosis of human brucellosis]. Mikrobiyol Bul. 2008;42(1):185–195.
14. Hekmatimoghaddam S, Sadeh M, Khalili MB, Mollaabedin M, Sazmand A. Comparison of PCR, Wright agglutination test and blood culture for diagnosis of brucellosis in suspected patients. Pak J Biol Sci. 2013;16(22):1589–1592. doi:10.3923/pjbs.2013.1589.1592
15. Akya A, Bozorgomid A, Ghadiri K, et al. Usefulness of blood parameters for preliminary diagnosis of brucellosis. J Blood Med. 2020;11:107–113. doi:10.2147/JBM.S245513
16. Xu N, Dong X, Yao Y, et al. Improved early detection of focal brucellosis complications with anti-brucella IgG. J Clin Microbiol. 2020;58(10):e00903–20. doi:10.1128/JCM.00903-20
17. Shakir R. Brucellosis. J Neurol Sci. 2021;420:117280. doi:10.1016/j.jns.2020.117280
18. Vollmar P, Zange S, Zöller L, Erkel J, Robert Thoma B. Brucellose [Brucellosis, an overview and current aspects]. Dtsch Med Wochenschr. 2016;141(14):1014–1018. German. doi:10.1055/s-0042-101723
19. Franco MP, Mulder M, Gilman RH, Smits HL. Human brucellosis. Lancet Infect Dis. 2007;7(12):775–786. doi:10.1016/S1473-3099(07)70286-4
20. Rodriguez-Takeuchi SY, Renjifo ME, Medina FJ. Extrapulmonary tuberculosis: pathophysiology and imaging findings. Radiographics. 2019;39(7):2023–2037. doi:10.1148/rg.2019190109
21. Park M, Kon OM. Use of Xpert MTB/RIF and Xpert Ultra in extrapulmonary tuberculosis. Expert Rev Anti Infect Ther. 2021;19(1):65–77. doi:10.1080/14787210.2020.1810565
22. Wang X, Yang Z, Fu Y, et al. Insight to the epidemiology and risk factors of extrapulmonary tuberculosis in Tianjin, China during 2006–2011. PLoS One. 2014;9(12):e112213. doi:10.1371/journal.pone.0112213
23. Pang Y, An J, Shu W, et al. Epidemiology of extrapulmonary tuberculosis among inpatients, China, 2008–2017. Emerg Infect Dis. 2019;25(3):457–464. doi:10.3201/eid2503.180572
24. World Health Organization. Automated real-time nucleic acid amplification technology for rapid and simultaneous detection of tuberculosis and rifampicin resistance: xpert MTB/RIF assay for the diagnosis of pulmonary and extrapulmonary TB in adults and children: policy update. Geneva: World Health Organization; 2013.
25. Zhou Z, Zheng Y, Wang L. A comparative study on the value of Xpert MTB/RIF and T-SPOT.TB tests in the diagnosis of bone and joint tuberculosis. Clin Chim Acta. 2020;500:115–119. doi:10.1016/j.cca.2019.09.026
26. Zhu F, Ou Q, Zheng J. Application values of T-SPOT.TB in clinical rapid diagnosis of tuberculosis. Iran J Public Health. 2018;47(1):18–23.
27. Liu Q, Chen X, Dai X, Liu X, Xu F, Peng P. Comparative analysis of five inspection techniques for the application in the diagnosis and treatment of osteoarticular tuberculosis. Int J Infect Dis. 2021;112:258–263. doi:10.1016/j.ijid.2021.09.019
28. Lin L, Ke Z, Cheng S. Efficacy and safety of short-term chemotherapy for patients with spinal tuberculosis undergoing surgery in Chinese population: a meta-analysis. J Orthop Surg Res. 2021;16(1):229. doi:10.1186/s13018-021-02375-9
29. Aryal A, Garg B, Mehta N, Shekhar S, Gupta V. Is 6 months of antitubercular chemotherapy as effective as more than 6 months regimen in spinal tuberculosis? A systematic review and meta-analysis. Asian Spine J. 2021. doi:10.31616/asj.2021.0104
30. Norbis L, Alagna R, Tortoli E, Codecasa LR, Migliori GB, Cirillo DM. Challenges and perspectives in the diagnosis of extrapulmonary tuberculosis. Expert Rev Anti Infect Ther. 2014;12(5):633–647. doi:10.1586/14787210.2014.899900
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.