Back to Journals » Advances in Medical Education and Practice » Volume 17
Bridging the Gap Between Learning and Practice: Final-Year Physiotherapy Students’ Perceptions of Enablers and Barriers to Interprofessional Collaboration in the UAE – A Qualitative Focus Group Study
Authors Ramakrishnan S ![]() , Elhanbali IGHH, McIsaac J
, Elhanbali IGHH, McIsaac J
Received 19 February 2026
Accepted for publication 8 May 2026
Published 19 May 2026 Volume 2026:17 604221
DOI https://doi.org/10.2147/AMEP.S604221
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sateesh Arja
Sivapriya Ramakrishnan,1 Israa Gamal Hamed Hamed Elhanbali,2 Jaye McIsaac3,4
1Department of Physiotherapy, College of Health Sciences, University of Sharjah, Sharjah, United Arab Emirates; 2Research Institute for Medical and Health Sciences, University of Sharjah, Sharjah, United Arab Emirates; 3Te Whare Wānanga o Awanuiārangi, Whakatane, Bay of Plenty, New Zealand; 4University of Liverpool, Liverpool, UK
Correspondence: Sivapriya Ramakrishnan, Department of Physiotherapy, College of Health Sciences, University of Sharjah, Sharjah, United Arab Emirates, Email [email protected]
Background: Interprofessional collaboration (IPC) is a key component of effective, patient-centered healthcare. Despite growing emphasis on interprofessional education, there is limited qualitative evidence exploring how physiotherapy students in the United Arab Emirates (UAE) perceive and interpret IPC within clinical training environments.
Objective: To explore final-year physiotherapy students’ perceptions of interprofessional collaboration, including perceived enablers and barriers within clinical settings in a university in the UAE.
Methods: A qualitative methodology was employed using Focus Group Discussions (FGDs). Two focus groups were conducted with final-year physiotherapy students (n = 19) at the University of Sharjah, United Arab Emirates. The focus groups were gender-segregated to align with local cultural norms. The discussions were audio recorded and transcribed verbatim. Thematic analysis was undertaken using Braun and Clarke’s six-phase approach to generate key themes and subthemes.
Results: Analysis generated five overarching themes and 11 subthemes, broadly reflecting: (1) understanding of interprofessional collaboration, (2) learning experiences, (3) influencing factors (including enablers and barriers), (4) application to practice, and (5) the need for structured interprofessional education. Students recognized IPC as essential for improving patient outcomes, particularly through effective communication, shared decision-making, and role clarity. However, readiness for collaborative practice appeared variable and was largely shaped by clinical exposure rather than structured training. Key barriers included hierarchical clinical structures, limited interprofessional engagement, and communication challenges across disciplines.
Conclusion: Final-year physiotherapy students demonstrate a strong conceptual understanding of IPC but face contextual and educational barriers to its effective implementation. These findings highlight a gap between theoretical preparation and clinical practice. Integrating structured interprofessional education within physiotherapy curricula, alongside addressing hierarchical and organizational constraints in clinical environments, may enhance students’ readiness for collaborative practice in multidisciplinary healthcare settings.
Keywords: physiotherapy education, interprofessional collaboration, interprofessional education, qualitative research, United Arab Emirates
Introduction
Interprofessional collaboration (IPC) is widely recognized as a cornerstone of effective, safe, and patient-centered healthcare delivery. As healthcare systems become increasingly complex, the ability of professionals to work collaboratively across disciplines is no longer optional but essential. In this context, physiotherapy education must evolve to equip students with the competencies required for collaborative practice.1 Interprofessional Education (IPE) has emerged as a critical pedagogical approach to foster these competencies, aiming to break down professional silos and prepare students for real-world interdisciplinary teamwork.2,3
Evidence suggests that physiotherapy students, both globally and within the United Arab Emirates (UAE), generally demonstrate positive attitudes toward IPE and collaborative learning.4 Students recognize the value of learning about the roles and contributions of other healthcare professionals and acknowledge that interprofessional learning enhances communication, mutual respect, and preparedness for collaborative practice. Participation in IPE activities, such as team-based learning and case-based discussions, has been shown to improve clinical reasoning and increase confidence in managing complex patient care scenarios through shared decision-making.5–8
However, despite these positive perceptions, challenges persist in translating interprofessional learning into effective collaborative practice. Existing literature highlights several barriers, including logistical constraints such as scheduling conflicts and limited resources, educational challenges such as role ambiguity and lack of structured IPE, and cultural factors such as hierarchical norms and professional boundaries.9–11 Importantly, while global studies consistently report favorable attitudes toward IPE, emerging evidence suggests that these attitudes do not always translate into meaningful interprofessional collaboration in clinical environments due to structural and contextual limitations.
The UAE healthcare system presents a unique context for examining interprofessional collaboration. It is characterized by a highly multicultural workforce, where healthcare professionals from diverse educational and cultural backgrounds interact within multidisciplinary teams. While this diversity enhances the potential for comprehensive patient care, it may also introduce challenges related to communication, role clarity, and hierarchical structures in clinical practice.12 Furthermore, interprofessional education within health professional programs in the UAE is still evolving, with limited structured opportunities for students to engage in collaborative learning during clinical training.8,13 These contextual factors highlight the importance of exploring how students perceive interprofessional collaboration within this setting.
Despite growing evidence on students’ readiness for interprofessional education, there remains limited qualitative research exploring how physiotherapy students in the UAE context perceive interprofessional collaboration during clinical training. Studies indicate that students demonstrate positive attitudes toward interprofessional learning; however, evidence exploring their perceptions within clinical settings remains limited.8,12–26
Final-year physiotherapy students were selected for this study as they represent the transition point between education and professional practice. Unlike early-stage students, who may primarily report expectations or initial challenges during clinical exposure, final-year students have completed substantial clinical rotations and are more likely to have experienced interprofessional collaboration within real healthcare settings. Previous research has highlighted that students in early clinical phases often experience stress, role uncertainty, and limited preparedness during the transition to clinical training, with competencies developing progressively through exposure. Therefore, final-year students are uniquely positioned to provide informed reflections on the enablers and barriers to interprofessional collaboration, as well as the extent to which educational preparation aligns with clinical practice.27,28
While IPE aims to prepare students for collaborative practice, the extent to which these competencies are translated into actual interprofessional collaboration (IPC) within clinical settings remains unclear. To better understand this transition, this study is guided by the Canadian Interprofessional Health Collaborative (CIHC) framework, which provides a comprehensive structure for examining IPC competencies, including communication, role clarification, team functioning, leadership, conflict resolution, and patient-centered care. This framework supports a structured interpretation of students’ perceptions within clinical environments.
Therefore, this study aims to explore final-year physiotherapy students’ perceptions of interprofessional collaboration within a university in the UAE, with a particular focus on identifying key enablers and barriers within clinical training settings.
Research Question
How do final-year physiotherapy students in a UAE university perceive the enablers and barriers to interprofessional collaboration in clinical settings?
Methods
Study Design
This study employed a descriptive qualitative design underpinned by an interpretivist paradigm. Interpretivism assumes that reality is socially constructed and that participants’ perceptions are best understood through the meanings they assign to those experiences.29 This approach was appropriate for exploring final-year physiotherapy students’ perception of interprofessional collaboration within clinical training contexts.
A descriptive qualitative design was selected because the study aimed to explore students’ perceptions including perceived enablers, and barriers rather than to conduct a phenomenological analysis. FGDs were used to encourage interaction, collective reflection, and the sharing of diverse viewpoints on interprofessional collaborative practice.30 This approach is suitable for examining complex educational and clinical experiences, particularly in multicultural healthcare education settings. This study is reported in accordance with the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist. A completed COREQ checklist is provided as supplementary material.31
Setting and Participants
The study was conducted in the Department of Physiotherapy at the University of Sharjah, UAE. FGDs were held in a pre-booked meeting room within the department to provide a comfortable, private, and supportive environment for discussion.
The target population was final-year physiotherapy students who had completed substantial clinical rotations. A purposive sampling strategy was used to recruit participants. Students were eligible if they were final-year physiotherapy students and had completed at least one clinical rotations in healthcare settings such as hospitals, rehabilitation centers, and outpatient/private clinical facilities. No exclusions were made based on gender, ethnicity, or health status.
A total of 19 final-year physiotherapy students participated in the study. Participants represented diverse cultural and educational backgrounds, reflecting the multicultural student population in the UAE. Participant characteristics, including gender, age, country of origin, number of clinical rotations completed, emirate of clinical placement, and type of clinical setting, are presented in Table 1.
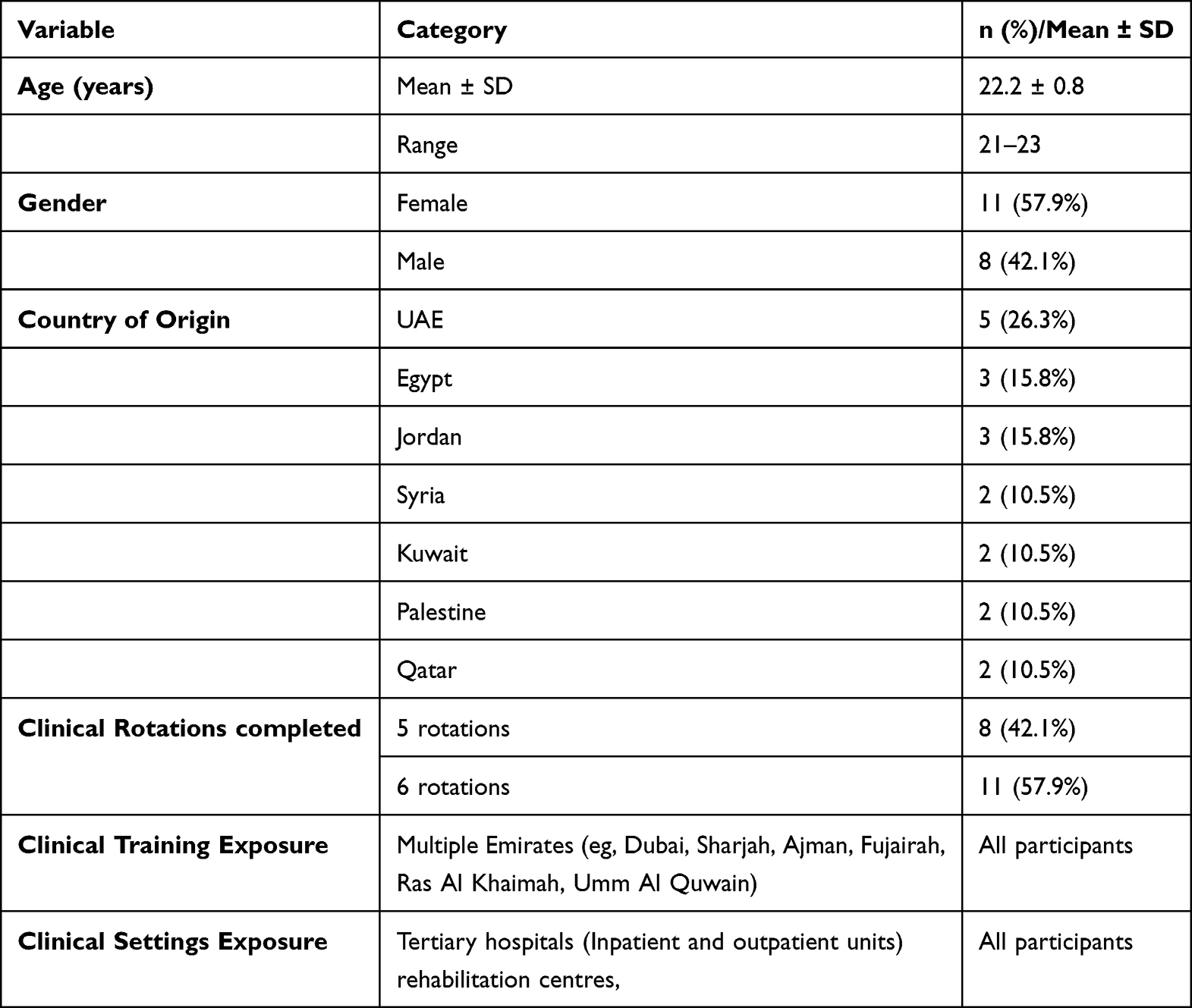 |
Table 1 Demographic Characteristics of the Participants |
Participant Recruitment and Flow
Eligible students were invited to participate through institutional Email approximately three weeks before the scheduled FGDs. The invitation included information about the study purpose, voluntary participation, confidentiality, and the right to withdraw at any time without academic consequences.
Students who agreed to participate provided written informed consent before data collection. All consenting participants were included in the study. No incentives were provided for participation. The participant recruitment and inclusion process is presented in Figure 1.
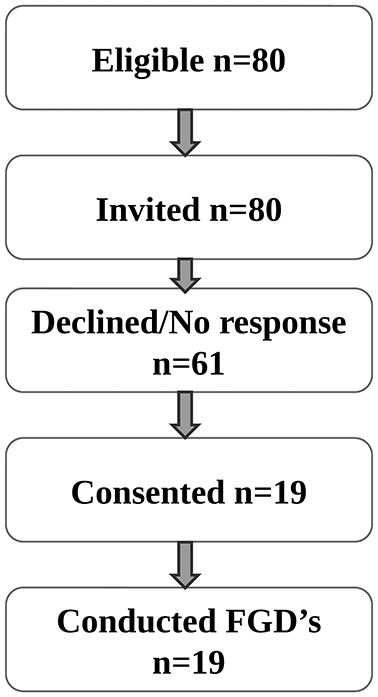 |
Figure 1 Participant Recruitment. |
Data Collection
Data were collected using gender-segregated FGDs to align with local cultural norms and to encourage open participation. Two focus groups were conducted, with approximately 9–10 participants per group. Each discussion lasted for up to 45 minutes to 60 minutes was guided by a semi-structured moderator guide developed for this study.
The moderator guide included demographic questions and content-related questions exploring students’ understanding of interprofessional collaboration, their clinical experiences, perceived enablers and barriers, communication across disciplines, professional roles, and suggestions for improving interprofessional education.
A semi-structured moderator guide was developed by the research team based on the study objectives and relevant literature. The guide was reviewed by experts in qualitative research and interprofessional health education to ensure clarity, relevance, and alignment with the study aims. Although the guide was not explicitly structured around the Canadian Interprofessional Health Collaborative (CIHC) competency domains, it addressed key components of interprofessional collaboration and was subsequently mapped to the CIHC framework during analysis.
The moderator guide used during data collection is presented in Figure 2. For clarity in reporting, the guide has been organized into thematic domains; however, the content and sequence of questions reflect those used during the focus group discussions. The guide was not formally pilot tested, although minor refinements were made following initial discussions within the research team.
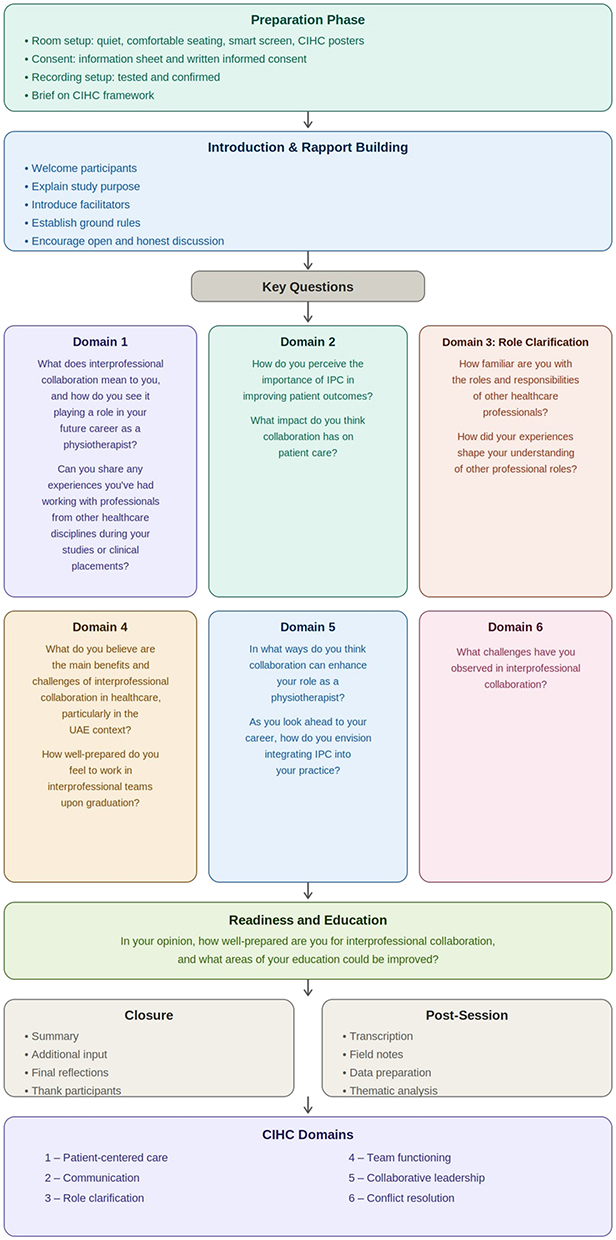 |
Figure 2 FGDs Process and Moderator guide. |
The focus groups were facilitated by two female faculty members [SR,JM]. One facilitator had experience in qualitative research and focus group methods among healthcare students, while the other had expertise in interprofessional health education and final-year physiotherapy mentoring. To reduce the possibility of power imbalance, participants were informed that their participation was voluntary, that there were no right or wrong answers, and that their responses would not affect their academic standing.
Reflexive memoing was undertaken throughout the data analysis process to enhance analytical transparency and minimize the influence of pre-existing assumptions. Themes were iteratively refined through constant comparison across transcripts to ensure consistency and depth of interpretation. An audit trail was maintained to document analytical decisions and support methodological transparency.
In addition, all members of the research team reviewed the data and emerging themes to ensure coherence and alignment between the raw data, coding framework, and final thematic structure. Transcripts were not returned to participants for comment or correction, as the focus of the analysis was on collective thematic patterns rather than individual transcript validation.
With participants’ consent, FGDs were audio-recorded. Recordings were transcribed verbatim and checked for accuracy against the original recordings. Transcripts were anonymized by removing identifying details and assigning participant codes.
Participant quotations were labelled using both focus group and participant identifiers, for example, FG1, P2 or FG2, P6, to improve transparency while maintaining confidentiality. Data is stored securely and accessed only by the research team. The informed consent process included permission to use anonymized participant quotations in publications.
Research Team
The research team comprised members with expertise in physiotherapy, medical education, and qualitative research, with roles ranging from lecturer to senior academic. This multidisciplinary composition facilitated a nuanced interpretation of the data and supported reflexivity throughout the research process. Team members engaged in ongoing discussions to acknowledge and reflect on their professional backgrounds, assumptions, and potential influences on data collection and analysis, which were considered during coding and theme development to enhance analytical rigor and transparency.
A pre-existing academic relationship existed between one member of the research team (SR) and the participants, as SR was involved in teaching within the physiotherapy program. The other facilitators (JM and IGE) had no prior teaching or supervisory relationship with the participants. To minimize potential influence on participant responses, students were informed that participation was voluntary, responses would remain confidential, and involvement would not affect their course grades or academic evaluation.
Data Analysis
Audio-recorded focus group discussions were transcribed verbatim and analysed using Braun and Clarke’s six-phase thematic analysis approach.32 The analysis began with familiarization through repeated reading of the transcripts, followed by the inductive generation of initial codes, allowing patterns to emerge directly from the data. Themes were not identified in advance but were derived inductively from the data. Two researchers (SR and IGE) independently reviewed the transcripts and identified meaningful units of text to generate initial codes. These codes were compared and refined through discussion to ensure consistency.
The codes were then organized into a coding framework and grouped into subthemes, which were subsequently refined into overarching themes through an iterative process of constant comparison and team discussion. Discrepancies in coding were resolved through consensus, with the involvement of a third researcher (JM) where necessary. The research team engaged in regular discussions throughout the analysis process to enhance credibility and ensure consistency in theme development. The final stages involved defining and naming the themes and producing the report, ensuring coherence and consistency across the dataset. Data analysis was conducted manually by the research team without the use of qualitative data analysis software.
Results
Thematic analysis, conducted using Braun and Clarke’s six-phase approach, generated five overarching themes and eleven sub themes reflecting final-year physiotherapy students’ perceptions of interprofessional collaboration (IPC) within clinical settings in Table 2. These themes were iteratively developed through coding and refinement and were interpreted in alignment with the Canadian Interprofessional Health Collaborative (CIHC) competency framework.
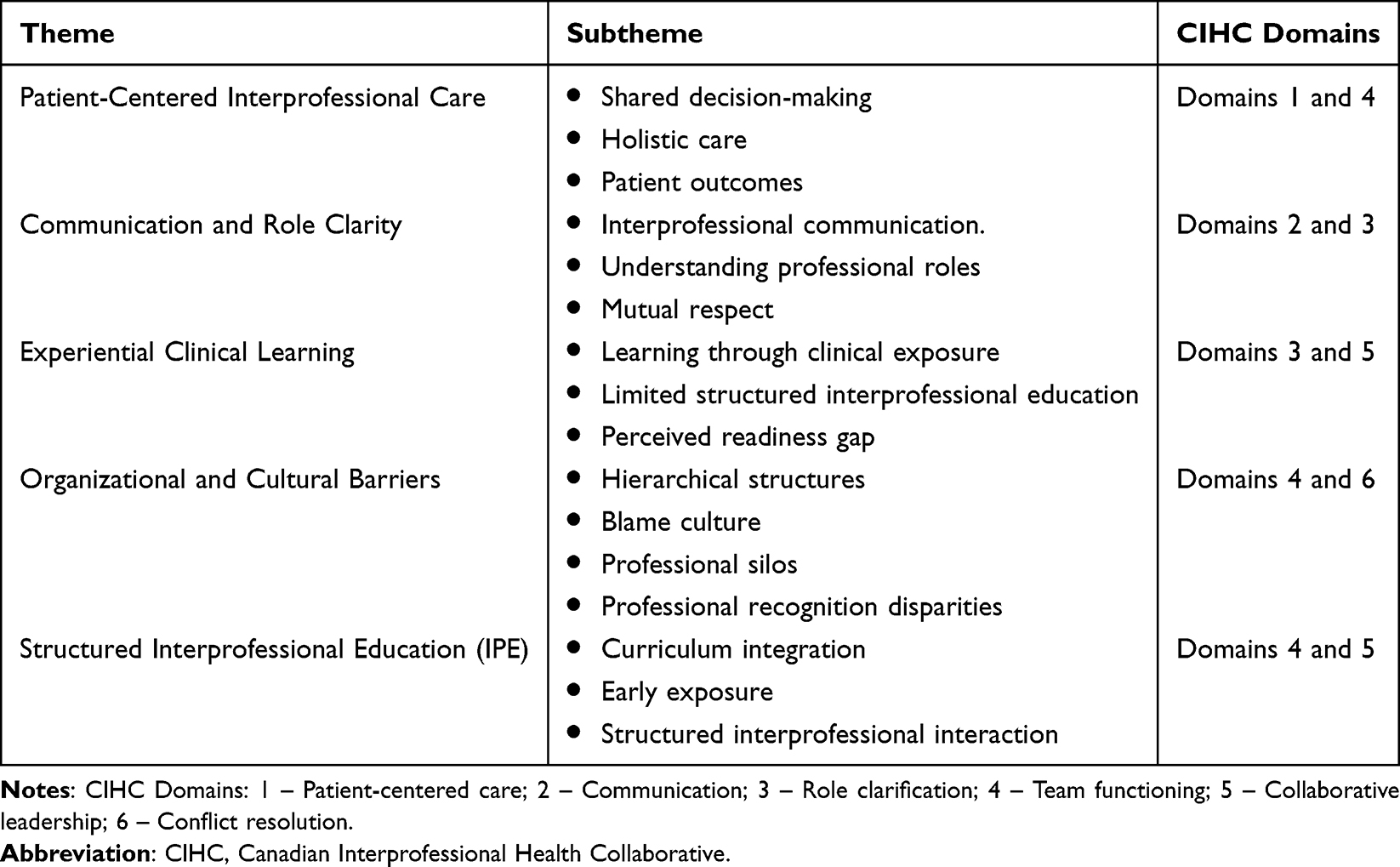 |
Table 2 Themes and Subthemes |
Through discussions, participants consistently endorsed IPC as an essential model of care while highlighting a clear tension between its perceived value and its implementation in practice. The five themes identified were: (1) Patient-centered interprofessional care, (2) Communication and role clarity, (3) Experiential clinical learning, (4) Organizational and cultural barriers, and (5) Need for structured interprofessional education. The relationships between these themes are illustrated in Figure 3.
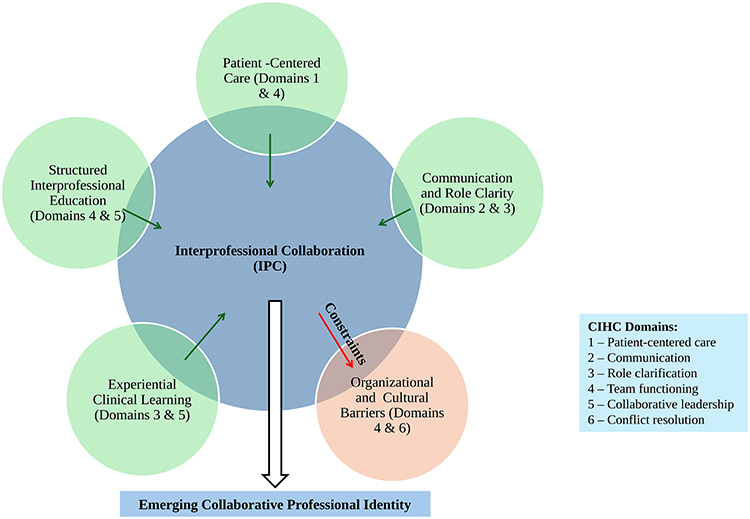 |
Figure 3 Thematic map illustrating relationships between themes influencing interprofessional collaboration among physiotherapy students. |
Theme 1: Patient-Centered Interprofessional Care (CIHC Domains 1 and 4: Patient-Centered Care; Team Functioning)
This theme comprised three subthemes: shared decision-making, holistic care, and patient outcomes.
Participants consistently conceptualized IPC as fundamental to achieving optimal patient outcomes. Collaboration was not viewed as optional but as a necessary condition for effective, coordinated care. Students emphasized that patient care is a shared responsibility, requiring the integration of expertise across disciplines.
We’re a team aiming for the same goal… every profession has their own way to reach that goal. (FG1, P2)
I alone can’t reach it alone. (FG1, P1)
This perspective reflects an emerging understanding of patient-centered care as a collective process rather than individual responsibility. Participants further associate collaboration with improved efficiency and timely intervention, suggesting that coordinated teamwork enhances both care quality and clinical outcomes.
Importantly, patient-centeredness was grounded in real clinical experiences rather than abstract concepts, indicating that students are beginning to internalize IPC as a practical and outcome-oriented approach.
Theme 2: Communication and Role Clarity (CIHC Domains 2 and 3: Communication; Role Clarification)
This theme included three subthemes: interprofessional communication, understanding professional roles, and mutual respect.
Effective communication and understanding of professional roles were identified as central enablers of interprofessional collaboration. Participants described how interactions with other healthcare professionals enhanced their clinical reasoning and broadened their understanding of patient management.
The physician showed me MRI and X-rays… this helped me understand the case much better. (FG2, P4)
It’s like a puzzle where each profession provides a piece. (FG1, P3)
These accounts illustrate how communication facilitates shared understanding and collaborative decision-making. However, participants also highlighted gaps in role clarity, noting that limited awareness of other professionals’ responsibilities can hinder effective collaboration.
If I don’t know what another specialist does, I won’t know how to involve them. (FG1, P1)
Overall, communication and role clarity were viewed as interdependent competencies that directly influence the effectiveness of team-based care.
Theme 3: Experiential Clinical Learning (CIHC Domains 3 and 5: Role Clarification; Collaborative Leadership)
This theme consisted of three subthemes: learning through clinical exposure, limited structured interprofessional education, and perceived readiness gaps.
Participants emphasized that their understanding and development of IPC competencies were largely shaped by clinical exposure rather than formal education. Experiential learning within clinical placements was described as the primary context in which collaborative skills were observed and developed.
I was prepared from the clinical sites, not from here. (FG1, P2)
The clinic is the main step that helped me. (FG2, P3)
This reliance on clinical experience highlights a gap between academic preparation and practical competency development. While students demonstrated awareness of IPC principles, many expressed uncertainties about their readiness to independently engage in collaborative practice.
Participants described their preparedness as partial and evolving, indicating that experiential learning alone may not be sufficient to fully develop interprofessional competencies.
Theme 4: Organizational and Cultural Barriers (CIHC Domains 4 and 6: Team Functioning; Conflict Resolution)
This theme comprised four subthemes: hierarchical structures, blame culture, professional silos, and disparities in professional recognition.
Despite strong endorsement of IPC, participants identified multiple systemic and relational barriers that constrain its implementation in clinical settings. These barriers were described as both organizational (structural hierarchies, lack of coordination) and cultural (professional dominance, communication challenges).
A prominent barrier was the presence of hierarchical structures, particularly physician dominance, which limited open communication and collaborative decision-making:
Doctors feel superior… their ego stops them from working as a team. (FG1, P1)
Participants also highlighted issues related to professional recognition, particularly for physiotherapists:
Doctors are highly glorified… physiotherapists don’t get similar recognition. (FG2, P5)
In addition, a blame-oriented culture was identified as a significant barrier:
When something goes wrong, people start blaming each other. (FG1, P1)
This environment was perceived to discourage accountability and reduce trust within teams, ultimately affecting collaboration and patient care.
Participants further described fragmented practice environments:
Hospitals do not prefer to work with each other… each person is on their own. (FG2, P8)
These findings suggest that barriers to IPC are deeply embedded within organizational systems and professional cultures, requiring system-level interventions.
Theme 5: Need for Structured Interprofessional Education (IPE) (CIHC Domains 4 and 5: Team Functioning; Collaborative Leadership)
This theme included three subthemes: curriculum integration, early exposure, and structured interprofessional interaction.
Participants expressed a strong need for structured and formalized interprofessional education to support the development of collaborative competencies. While IPC was recognized as important, students reported limited opportunities for structured learning within the curriculum.
Suggestions for improvement included early integration of IPC concepts, structured interdisciplinary activities, and increased opportunities for shared learning.
Hospitals should set one hour daily for all specialties to meet. (FG2, P6)
Awareness should start from universities. (FG1, P1)
Participants emphasized that structured educational interventions are essential to bridge the gap between theoretical knowledge and clinical practice. These recommendations reflect an understanding that collaborative competencies must be intentionally developed through both educational and clinical systems.
Positive drivers such as patient-centred care, communication, experiential clinical learning, and structured interprofessional education enhance IPC, while organizational and cultural barriers constrain its implementation. These interactions collectively shape the development of a collaborative professional identity.
Emerging Collaborative Professional Identity
Across all themes, participants demonstrated an emerging professional identity characterized by openness, humility, and a willingness to engage with other healthcare professionals. This identity was shaped through both experiential learning and exposure to interprofessional interactions within clinical settings. This cross-cutting insight is reflected in Figure 3 as the outcome of interactions between the identified themes.
Even if I’m super smart, I don’t know everything. (FG1, P1)
I’m prepared like 50–60%… there’s still more to learn. (FG2, P4)
This finding suggests that interprofessional collaboration extends beyond the acquisition of discrete competencies, encompassing the development of professional values, attitudes, and self-awareness. The emergence of this collaborative professional identity represents a critical dimension of readiness for interprofessional practice.
Discussion
This study explored final-year physiotherapy students’ perceptions of interprofessional collaboration (IPC) within a UAE university context, interpreting findings through the Canadian Interprofessional Health Collaborative (CIHC) framework. The results demonstrate that while students strongly endorse IPC as essential for patient-centered care, their readiness for collaborative practice is shaped by experiential learning gaps and constrained by organizational and cultural barriers. These findings highlight a clear distinction between the conceptual understanding of IPC and its consistent enactment in practice.
Patient-Centered Interprofessional Care – IPC as a Shared Responsibility
Participants consistently conceptualized IPC as fundamental to achieving optimal patient outcomes, emphasizing shared responsibility and holistic care. This aligns with global evidence demonstrating that collaborative practice enhances care quality and safety.33,34
However, rather than merely confirming existing findings, this study extends the literature by illustrating how students operationalize patient-centered care as an interdependent process requiring contributions from multiple professions rather than an individual responsibility.35 Importantly, these experiences were grounded in clinical exposure rather than structured instruction, suggesting that experiential learning plays a critical role in shaping students’ understanding of IPC.36
In contrast to settings where IPC is systematically embedded within curricula, students in this study appeared to develop this understanding informally. This indicates that while the value of IPC is well recognized, its consistent application may be context-dependent, particularly in environments where interprofessional education (IPE) is still evolving.37 From a CIHC perspective, this reflects early development of competencies related to patient-centered care and team functioning, but highlights the need for structured reinforcement.38
Communication and Role Clarity – Learning Through Practice Rather Than Curriculum
Communication and role clarity emerged as central enablers of IPC, consistent with prior research identifying communication as a cornerstone of effective teamwork and patient safety11 Participants described how interdisciplinary interactions enhanced their understanding of patient management, supporting findings from Nygren-Bonnier et al.9
However, a key contribution of this study is the finding that communication skills and role understanding were primarily developed through informal clinical interactions rather than structured educational experiences. This aligns with earlier work39 which highlights persistent gaps in role clarity among healthcare students.
This reveals a significant curriculum–practice gap: while communication may develop opportunistically, role clarification requires intentional educational design. Within the CIHC framework, this reinforces the interdependence of communication and role clarification competencies and underscores the need for structured learning opportunities that enable students to move beyond observation toward active participation.
Experiential Clinical Learning – Exposure without Full Competence
Participants consistently reported that their preparation for IPC was shaped primarily through clinical placements rather than formal academic training. This aligns with literature emphasizing the importance of experiential learning in developing interprofessional competencies.5,6
However, in contrast to studies conducted in institutions with established IPE frameworks, where students report higher confidence and readiness, participants in this study described only partial preparedness.11,40 This finding is critical, as it highlights a gap between exposure and competence.
Importantly, this study does not claim that IPC competencies are fully developed through clinical experience. Instead, it demonstrates that students perceive IPC as important yet feel insufficiently prepared to independently engage in collaborative practice.13 From a CIHC perspective, this reflects emerging competencies in role clarification and collaborative leadership but indicates the need for structured educational scaffolding to support competency consolidation.
Organizational and Cultural Barriers – Hierarchy, Blame Culture, and Power Dynamics
One of the most significant and context-specific findings of this study is the identification of organizational and cultural barriers, particularly hierarchy, professional silos, and blame culture, as constraints to IPC. These findings are consistent with global literature highlighting structural barriers to collaboration.11,18,22,41,42
However, this study extends existing evidence by providing deeper insight into how these barriers are perceived by students within the UAE healthcare context. Participants described physician dominance as limiting communication and shared decision-making,43 but also illustrating how such hierarchies influence students’ experiences of professional identity and participation.
The presence of a blame-oriented culture emerged as a particularly important barrier. While hierarchy is widely reported, fewer studies explicitly identify blame culture as a constraint to IPC. In this study, blame culture was perceived to reduce psychological safety, discourage open communication, and limit shared accountability. This suggests that organizational culture plays a critical role in shaping interprofessional interactions.
Furthermore, the UAE’s multicultural healthcare environment may amplify these challenges, as variations in professional training, cultural norms, and communication styles can influence collaboration. These findings directly address reviewer concerns regarding insufficient contextualization and align with CIHC domains related to team functioning and conflict resolution.
Need for Structured Interprofessional Education – Bridging the Gap
Participants strongly advocated for structured interprofessional education, including early exposure, interdisciplinary learning opportunities, and formal integration within curricula. This aligns with global evidence demonstrating that structured IPE improves collaborative competencies.33,40
In contrast to settings where IPE is longitudinally embedded, students in this study reported limited structured opportunities, relying instead on variable clinical exposure. This highlights a critical opportunity for curriculum development within the UAE context.
Embedding IPC longitudinally across academic and clinical training may help bridge the gap between theoretical understanding and practical application. From a CIHC perspective, this supports the development of competencies related to team functioning and collaborative leadership, emphasizing the need for intentional and sustained educational strategies.
Emerging Collaborative Professional Identity
An important contribution of this study is the identification of an emerging collaborative professional identity among students. Participants demonstrated openness, humility, and awareness of their professional limitations3 which emphasize identity formation as a key component of interprofessional competence.
However, unlike contexts where identity development is supported through structured IPE,44 students in this study appeared to develop this identity informally through clinical exposure. This suggests that while collaborative identity is emerging, it may benefit from more intentional educational support to strengthen interprofessional values and attitudes.
Final-year physiotherapy students demonstrate a strong conceptual understanding of IPC but face challenges in translating this into practice due to educational gaps and systemic barriers. Strengthening structured interprofessional education and addressing organizational constraints may support the development of collaborative competencies and professional identity within the UAE healthcare context.
Implications for Practice and Education
The findings of this study highlight the need for a more structured and contextually responsive integration of interprofessional collaboration (IPC) within physiotherapy education and clinical practice. While students demonstrated a strong conceptual understanding of IPC, their readiness to enact collaborative competencies appeared inconsistent, underscoring the need for targeted educational and system-level interventions as explained in Table 3.
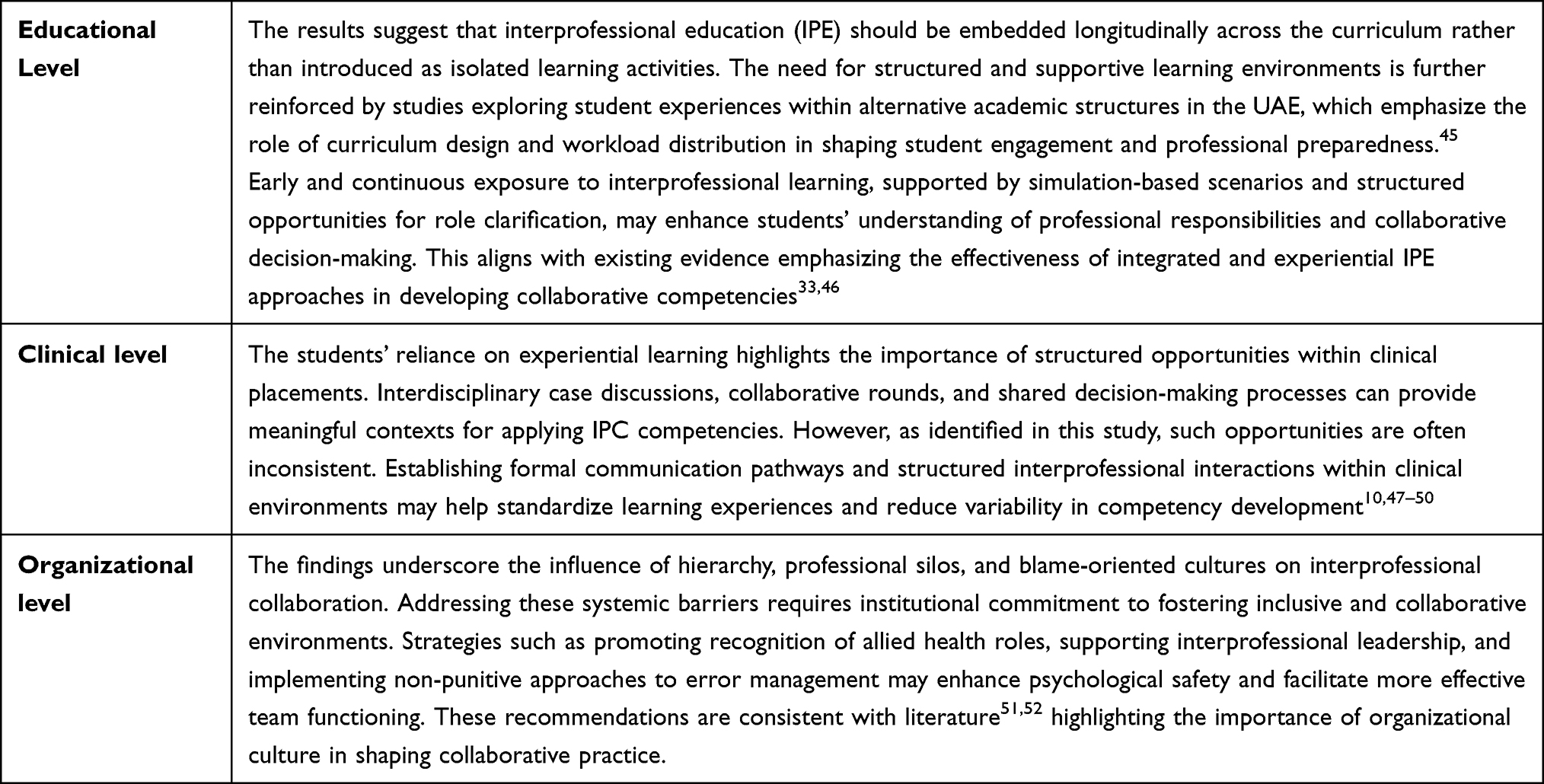 |
Table 3 System-Level Interventions |
Taken together, these implications emphasize that developing IPC competencies requires coordinated efforts across educational, clinical, and organizational systems, rather than relying solely on individual learning experiences.
Key Contribution of the Study
This study makes several important contributions to the existing literature on interprofessional collaboration in healthcare education. It provides context-specific qualitative insights from the UAE, addressing a notable gap in regional evidence where interprofessional education is still evolving. By situating the findings within a multicultural healthcare context, the study highlights how cultural and systemic factors influence students’ perceptions of collaboration. It highlights the impact of hierarchy and blame culture as key barriers to IPC, extending existing literature by illustrating how these factors influence not only team functioning but also students’ perceptions of professional identity and participation.
This study also identifies a curriculum–practice gap in IPC readiness, demonstrating that while students value collaboration, their competencies are primarily developed through variable clinical exposure rather than structured educational design. It demonstrates that IPC competency development is not solely skill-based but also experiential, identity-driven, and system-dependent. This finding reinforces the importance of integrating educational strategies with supportive clinical and organizational environments to enable meaningful and sustained interprofessional practice.
Limitations
The findings of this study should be interpreted considering several considerations. The sample was drawn from final-year physiotherapy students within a single institution, which may limit the transferability of insights to other educational or healthcare contexts. As with qualitative research, the applicability of findings depends on the similarity of context, and readers are encouraged to interpret the findings accordingly.
The voluntary nature of participation may have resulted in the inclusion of students with more favorable views toward interprofessional collaboration, potentially influencing the overall tone of the findings. In addition, the use of faculty moderators may have introduced response bias due to perceived power dynamics, which could have influenced the extent to which participants shared critical experiences.
The use of FGDs as the sole data collection method may have also influenced the findings. Group dynamics, including dominant participants or peer influence, may have shaped the responses and potentially limited the expression of dissenting views.
Furthermore, the study focused on a single professional group, which restricts the ability to capture broader interprofessional dynamics that may emerge when multiple healthcare disciplines are included. The absence of methodological triangulation, such as incorporating individual interviews or observational data, may also limit the depth and diversity of experiences captured.
Finally, as a cross-sectional study, the findings reflect students’ perceptions at a single point in time and do not account for how interprofessional competencies may evolve throughout training or into professional practice.
Recommendations
Building on these findings, future research should extend beyond single-institution studies to include larger, multi-institutional and multi-disciplinary samples, enabling comparative exploration of interprofessional collaboration (IPC) competencies across different healthcare education contexts. Including students from multiple health professions would provide a more comprehensive understanding of interprofessional dynamics and shared learning experiences.
Longitudinal research designs are particularly warranted to examine how IPC competencies develop over time, from undergraduate education into early professional practice. Such approaches would provide deeper insight into the transition from conceptual understanding to sustained collaborative behavior, addressing the readiness gap identified in this study.
Further research should also evaluate the effectiveness of structured interprofessional education (IPE) interventions, including simulation-based learning, interdisciplinary case discussions, and collaborative clinical placements. Investigating how these approaches influence competencies related to communication, role clarification, and team functioning would provide evidence to inform curriculum design and implementation.
In addition, incorporating perspectives from faculty members, clinical educators, and supervisors would enhance understanding of the educational and organizational factors that shape IPC. This multi-level perspective is essential to identify barriers and facilitators across both academic and clinical environments.
Finally, given the contextual findings of this study, further research is needed to examine how cultural and institutional factors within the UAE influence professional hierarchies, communication patterns, and team dynamics. Such work would support the development of contextually relevant and culturally responsive interprofessional education strategies, ensuring that IPC interventions are aligned with local healthcare systems and practices.
Conclusion
This study explored final-year physiotherapy students’ perceptions of interprofessional collaboration within a UAE university context, interpreted through the Canadian Interprofessional Health Collaborative (CIHC) framework. The findings identified five key dimensions—patient-centered care, communication and role clarity, experiential clinical learning, organizational and cultural barriers, and the need for structured interprofessional education—that collectively shape students’ perceptions and readiness for collaborative practice.
Students demonstrated a strong conceptual understanding of IPC and its importance for patient-centered care and shared decision-making. However, their readiness to engage in collaborative practice was uneven and largely dependent on variable clinical exposure rather than structured educational preparation. The findings also highlight the influence of contextual factors within the UAE healthcare system, including hierarchical professional structures, limited recognition of allied health roles, and blame-oriented cultures, which constrain the consistent enactment of IPC.
Together, these findings reveal a disconnect between the theoretical understanding of interprofessional collaboration and its practical implementation. Bridging this gap requires embedding structured, longitudinal interprofessional education within physiotherapy curricula, supported by meaningful interdisciplinary engagement during clinical training. In parallel, fostering organizational cultures that promote equitable team functioning, open communication, and reflective approaches to practice will be essential to support sustainable interprofessional collaboration.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available due to ethical and confidentiality restrictions. Anonymized data may be made available from the corresponding author upon reasonable request, subject to institutional ethical approval.
Ethical Approval
Ethical approval for this study was obtained from the Research Ethics Committee of the University of Sharjah (REC-24-09-30-02-F) and the Research Ethics and Integrity Office at the University of Liverpool (ETH-200050112). The study was conducted in accordance with the principles of the Declaration of Helsinki. All participants provided informed consent prior to participation. Consent included permission for the use of anonymized data and direct quotations for research and publication purposes.
Acknowledgments
The authors would like to extend their gratitude to all the physical therapy students who participated in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Davies K, Harrison K, Clouder DL, Gilchrist M, McFarland L, Earland J. Making the transition from physiotherapy student to interprofessional team member. Physiotherapy. 2011;97(2):139–16.
2. Carlisle C, Cooper H, Watkins C. “Do none of you talk to each other?”: the challenges facing the implementation of interprofessional education. Med Teach. 2004;26(6):545–552. doi:10.1080/61421590410001711616
3. Thistlethwaite J. Interprofessional education: a review of context, learning and the research agenda. Med Educ. 2012;46(1):58–70. doi:10.1111/j.1365-2923.2011.04143.x
4. Ntinga M, Van Aswegen H. Physiotherapists’ perceptions of collaborations with inter-professional team members in an ICU setting. South Afr J Crit Care. 2020;36(2):86–91. doi:10.7196/SAJCC.2020.v36i2.431
5. Frenk J, Chen L, Bhutta ZA, et al. Health professionals for a new century: transforming education to strengthen health systems in an interdependent world. Lancet. 2010;376(9756):1923–1958. doi:10.1016/S0140-6736(10)61854-5
6. McLaney E, Morassaei S, Hughes L, Davies R, Campbell M, Di Prospero L. A framework for interprofessional team collaboration in a hospital setting: advancing team competencies and behaviours. Healthc Manage Forum. 2022;35(2):112–117. doi:10.1177/08404704211063584
7. Robson M, Kitchen SS. Exploring physiotherapy students’ experiences of interprofessional collaboration in the clinical setting: a critical incident study. J Interprof Care. 2007;21(1):95–109. doi:10.1080/13561820601076560
8. Sulaiman N, Rishmawy Y, Hussein A, et al. A mixed methods approach to determine the climate of interprofessional education among medical and health sciences students. BMC Med Educ. 2021;21(1). doi:10.1186/s12909-021-02645-4
9. Nygren-Bonnier M, Högstedt K, Laurell A, Boström C. First and final year physiotherapy students’ expectations of their future profession. Physiother Theory Pract. 2023;39(11):2366–2376.
10. Rojas JG, Fuster-Guillén D, Flores JRC, Hernandez RM. Successful Practices in the Teaching-Learning of Physical Therapy. Health Edu Health Promotion. 2024;12(1):91–104.
11. Reeves S, Fletcher S, Barr H, et al. A BEME systematic review of the effects of interprofessional education: BEME Guide No. 39. Med Teach. 2016;38(7):656–668. doi:10.3109/0142159X.2016.1173663
12. Ahmed FR, Khaiwa L, Mustafaalsaafin H, et al. Multicultural Nursing Team in ICU: intraprofessional Collaboration and Job Performance. Nurs Forum. 2025;2025(1). doi:10.1155/nuf/2541827
13. Yasin H, Palaian S, Shankar PR, Nallamilli S. Readiness for interprofessional education among health profession students in a university in the United Arab Emirates. J Multidiscip Healthc. 2023;16:1141–1149. doi:10.2147/JMDH.S395320
14. El-Awaisi A, Joseph S, El Hajj MS, Diack L. Pharmacy academics’ perspectives toward interprofessional Education prior to its implementation in Qatar: a qualitative study. BMC Med Educ. 2019;19(1):278. doi:10.1186/s12909-019-1689-5
15. Homeyer S, Hoffmann W, Hingst P, Oppermann RF, Dreier-Wolfgramm A. Effects of interprofessional education for medical and nursing students: enablers, barriers and expectations for optimizing future interprofessional collaboration - a qualitative study. BMC Nurs. 2018;17(1). doi:10.1186/s12912-018-0279-x
16. Johnson K, Martin P, McGrail M. Interprofessional education and collaborative practice in diagnostic radiography: insights from an Australian interview study. Radiography. 2026;32(2):103285. doi:10.1016/j.radi.2025.103285
17. Lackie K, Hayward K, Ayn C, et al. Creating psychological safety in interprofessional simulation for health professional learners: a scoping review of the barriers and enablers. J Interprof Care. 2023;37(2):187–202. doi:10.1080/13561820.2022.2052269
18. Lee CS, Poon Z, He JCE, et al. Qualitative study on the perceived enablers and barriers to interprofessional education in primary care in Singapore. BMC Prim Care. 2025;26(1). doi:10.1186/s12875-025-02769-2
19. Mattiazzi S, Cottrell N, Ng N, Beckman E. Behavioural outcomes of interprofessional education within clinical settings for health professional students: a systematic literature review. J Interprof Care. 2024;38(2):294–307. doi:10.1080/13561820.2023.2170994
20. Mohamed N, Peck CW, Senekal J. Perceptions of interprofessional collaborative practice in South Africa: a systematic review. Health SA. 2024;29. doi:10.4102/hsag.v29i0.2413
21. Nandakumaran N, Nihardeen A, Lizarondo L, et al. A mixed methods systematic review of interprofessional education and collaborative practice in rural healthcare settings. J Interprof Care. 2026;40(1):127–144. doi:10.1080/13561820.2025.2538083
22. Perron D, Parent K, Gaboury I, Bergeron DA. Characteristics, barriers and facilitators of initiatives to develop interprofessional collaboration in rural and remote primary healthcare facilities: a scoping review. Rural Remote Health. 2022;22(4). doi:10.22605/RRH7566
23. Thomas J, Kumar K, Chur-Hansen A. How pharmacy and medicine students experience the power differential between professions: “Even if the pharmacist knows better, the doctor’s decision goes”. PLoS One. 2021;16:e0256776. doi:10.1371/journal.pone.0256776
24. Whitehead C. The doctor dilemma in interprofessional education and care: how and why will physicians collaborate? Med Educ. 2007;41(10):1010–1016. doi:10.1111/j.1365-2923.2007.02893.x
25. Wong PS, Chen YS, Saw PS. Influencing factors and processes of interprofessional professional education (IPE) implementation. Med Teach. 2021;43(S1):S39–S45. doi:10.1080/0142159X.2019.1672864
26. Zwaan E, Zipfel N, Kuijer-Siebelink W, Oomens S, van der Burg-Vermeulen SJ. Barriers and facilitators for interprofessional education in work-focused healthcare: an integrative review. J Occup Rehabil. 2026;36(1):97–116. doi:10.1007/s10926-025-10278-3
27. Brar G, Harney S, McGarr O, McFarland J. Mentoring & support practices for final year medical students during a pandemic – ‘The covid doctors’. BMC Med Educ. 2023;23(1). doi:10.1186/s12909-023-04513-9
28. Abdalla ME, Shorbagi S. Challenges faced by medical students during their first clerkship training: a cross-sectional study from a medical school in the Middle East. J Taibah Univ Sci. 2018;13(4):390–394. doi:10.1016/j.jtumed.2018.03.008
29. The Interpretive Paradigm. Understanding Communication Research Methods: A Theoretical and Practical Approach.
30. Villamin P, Lopez V, Thapa DK, Cleary M. A worked example of qualitative descriptive design: a step-by-step guide for novice and early career researchers. J Adv Nurs. 2025;81(8):5181–5195. doi:10.1111/jan.16481
31. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
32. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
33. Reeves S, Pelone F, Harrison R, Goldman J, Zwarenstein M. Interprofessional collaboration to improve professional practice and healthcare outcomes. Cochrane Database Syst Rev. 2017;6(6):Cd000072. doi:10.1002/14651858.CD000072.pub3
34. Collaborative CIH. A National Interprofessional Competency Framework. University of British Columbia; 2010.
35. Campagna V, Lee-Riley L. Interprofessional Collaboration as a Best Practice Across the Care Continuum. Prof Case Manag. 2025;30(3):100–106. doi:10.1097/NCM.0000000000000793
36. Bianchi M, Bagnasco A, Ghirotto L, et al. The point of view of undergraduate health students on interprofessional collaboration: a thematic analysis. Sage Open Nurs. 2019;5. doi:10.1177/2377960819835735
37. North SE, Lafky R, Porta C, Sick B. Interprofessional students’ insights into the experiential learning environment: values, impacts, and alignment with interprofessional collaborative practice competencies and the triple aim. J Interprof Educ Pract. 2023;32:100639. doi:10.1016/j.xjep.2023.100639
38. Hepp SL, Suter E, Jackson K, et al. Using an interprofessional competency framework to examine collaborative practice. J Interprof Care. 2015;29(2):131–137. doi:10.3109/13561820.2014.955910
39. Hammick M, Freeth D, Koppel I, Reeves S, Barr H. A best evidence systematic review of interprofessional education: BEME Guide no. 9. Med Teach. 2007;29(8):735–751. doi:10.1080/01421590701682576
40. World Health Organization. Framework for action on interprofessional education and collaborative practice. 2010.
41. Jung H, Ro E. Validating common experiences through focus group interaction. J Pragmatics. 2019;143:169–184. doi:10.1016/j.pragma.2019.02.019
42. Gallegos PJ, Peeters JM. A measure of teamwork perceptions for team-based learning. Curr Pharm Teach Learn. 2011;3(1):30–35. doi:10.1016/j.cptl.2010.10.004
43. Baxter S, Johnson M, Chambers D, Sutton A, Goyder E, Booth A. The effects of integrated care: a systematic review of UK and international evidence. BMC Health Serv Res. 2018;18(1):350.
44. Africa L, Jaffer L, Filies G, et al. Navigating an interprofessional curriculum: the interprofessional education passport and the quest for an interprofessional identity. J Interprof Care. 2026;40(2):261–271.
45. Arumugam A, Dias JM, Narasimhan S, et al. Balancing academics and life: qualitative study of health professions students’ perceptions of a four-day academic week in the United Arab Emirates. JMIR Med Educ. 2025;11(1):e67775. doi:10.2196/67775
46. Bridges DR, Davidson RA, Odegard PS, Maki IV, Tomkowiak J. Interprofessional collaboration: three best practice models of interprofessional education. Med Educ Online. 2011;16(1).
47. Shi Y, Miao S, Fu Y, Sun C, Wang H, Zhai X. TeamSTEPPS improves patient safety. BMJ Open Qual. 2024;13(2):e002669. doi:10.1136/bmjoq-2023-002669
48. Poole G, Simmons N. Contributions of the scholarship of teaching and learning to quality enhancement in Canada. In: Enhancing Quality in Higher Education: International Perspectives. Routledge; 2013:118–128.
49. Szczyrba B. Teaching guided by science—with scholarship of teaching and learning. In: Applied Higher Education Yearbook 2019: German-Chinese Perspectives and Discourses. Springer; 2023:245–256.
50. Wei H, Corbett RW, Ray J, Wei TL. A culture of caring: the essence of healthcare interprofessional collaboration. J Interprof Care. 2020;34(3):324–331. doi:10.1080/13561820.2019.1641476
51. Muller-Schoof IJM, Snoeren M, Verbiest MEA, Luijkx KG. Evaluation of an interprofessional educational program in nursing home practice: a mixed methods multiple-case study. J Interprof Care. 2024;38(6):1081–1091. doi:10.1080/13561820.2024.2395966
52. Shrader S, Hodgkins R, Bhattacharya S, Laverentz D, Johnston K, Jernigan S. Evaluating the impact of an interprofessional education program on workforce: recruitment, collaborative practice, and culture. J Interprof Educ Pract. 2022;28:100495. doi:10.1016/j.xjep.2022.100495
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.