Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Bridging the Gap Between Efficacy and Practice: A Systematic Review of Shared Decision-Making in Severe Mental Illness
Authors Dong J, Lu M ![]() , Chen Y, Zisman-Ilani Y, Feng Y, Zhang S
, Chen Y, Zisman-Ilani Y, Feng Y, Zhang S ![]() , Huang H, Zhou Y
, Huang H, Zhou Y
Received 20 March 2026
Accepted for publication 9 June 2026
Published 16 June 2026 Volume 2026:19 610845
DOI https://doi.org/10.2147/JMDH.S610845
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jagdish Khubchandani
Junhui Dong,1 Minle Lu,1 Yubin Chen,2 Yaara Zisman-Ilani,3 Yang Feng,1 Shuxin Zhang,1 Huizhen Huang,1 Yuqiu Zhou1,2
1Department of Nursing, College of Medical Science, Huzhou Normal University, Huzhou, Zhejiang, 313000, People’s Republic of China; 2Department of Nursing, Harbin Medical University, Harbin, Heilongjiang, 150081, People’s Republic of China; 3Department of Social and Behavioral Sciences, Temple University, Philadelphia, PA, 19122, USA
Correspondence: Yuqiu Zhou, Department of Nursing, College of Medical Science, Huzhou Normal University, No. 759, Erhuandong Road, Huzhou City, Zhejiang, 313000, People’s Republic of China, Tel +86 17858188203, Email [email protected]
Abstract: Shared decision-making (SDM) is recommended for preference-sensitive treatment decisions in severe mental illness, but its routine use in psychiatric services remains inconsistent. This systematic review synthesized evidence published between 2014 and 2024 and examined clinical, cultural, and organizational factors associated with SDM implementation. We searched PubMed, Embase, CINAHL, Cochrane Library, Web of Science, CNKI, Wanfang, and VIP for studies published from January 2014 to November 2024. Forty-two studies involving 8798 participants were included. Reporting followed PRISMA 2020 and SWiM guidance. Study quality was assessed with design-specific Joanna Briggs Institute tools, and certainty of key findings was appraised using a combined GRADE-CERQual approach. Because of heterogeneity in study design, interventions, outcomes, and settings, findings were synthesized narratively using Popay et al’s framework. Patient decision aids were generally associated with lower decisional conflict, greater readiness, satisfaction, involvement, or autonomy, with little evidence of meaningful consultation-time extension. Clinician training and SDM interventions improved short-term engagement and information sharing, but evidence for sustained improvements in adherence, decisional conflict, and clinician behavior was mixed or low certainty. Family-mediated or triadic decision-making was prominent in East and Southeast Asian studies and may support adherence and participation, although it can also create tension between patient autonomy and family preferences. Across studies, clinicians and patients often emphasized different treatment priorities, particularly symptom control versus side-effect tolerability. Evidence was concentrated in Europe and East Asia, with limited data from low-resource regions. SDM in psychiatric care appears most reliable for improving immediate decision processes rather than long-term outcomes. Future implementation should test culturally adapted triadic decision aids, workflow-integrated prompts, and interprofessional decision coaching while using cautious, context-sensitive outcome evaluation.
Keywords: patient participation, decision aids, implementation science, cross-cultural psychiatry, interprofessional collaboration
Introduction
Psychiatric treatments, particularly psychopharmacological interventions for severe mental illnesses (SMI) such as schizophrenia and bipolar disorder, frequently involve complex, preference-sensitive decisions.1 Because there is rarely a single universally superior treatment, clinicians and patients (also termed “service users” in some mental-health contexts; we use “patients” throughout for consistency) must navigate difficult trade-offs between clinical efficacy (eg., relapse prevention) and severe adverse effects (eg., metabolic syndrome, extrapyramidal symptoms). In such contexts of clinical uncertainty, shared decision-making (SDM) has emerged as the normative standard to ensure that medical choices align with patients’ underlying values and preferences.2,3 When operationalized through structured patient decision aids (PtDAs), SDM facilitates bidirectional information exchange, mitigates information asymmetry, and has been shown to reduce decisional conflict,4 improve patient satisfaction,5 and enhance overall treatment engagement.6
Yet evidence from implementation research indicates that improvements achieved under trial conditions are often difficult to sustain once structured support is withdrawn, with early gains in clinician behaviour and decisional outcomes commonly regressing toward baseline and routine adoption in everyday psychiatric practice remaining limited and uneven.7,8 Efficacy data alone do not predict practice-level adoption — a gap the present review aims to characterize. Despite strong theoretical rationale and empirical support, the routine implementation of SDM in psychiatric practice remains limited. Unlike many general medical settings, psychiatric decision-making is hindered by a unique combination of cognitive deficits, behavioral biases, and structural constraints. Two decision-science concepts frame this synthesis: choice architecture — features of the decision environment that determine which option is default or most salient9 — and heuristics, the mental shortcuts (anchoring, availability, status-quo bias) that can distort preference-sensitive decisions under time pressure.10 At the patient level, acute psychiatric episodes and inherent working memory deficits often result in fluctuating decisional capacity and vulnerability to cognitive overload during clinical consultations.11 Compounding these patient-level challenges are reported patterns of clinician heuristic behavior. Operating under severe time constraints, mental health professionals frequently default to fast, heuristic-driven decision-making. This pressure widens the gap between clinician and patient priorities: clinicians focus on symptom remission, whereas patients weigh side-effect tolerability.12 It also fosters overconfidence, leading clinicians to underestimate patients’ willingness and capacity to participate. Furthermore, the cognitive and temporal burden of SDM is frequently placed entirely on the prescribing psychiatrist, neglecting the critical potential of an interprofessional collaborative approach—involving clinical pharmacists, specialized nurses, and social workers—to distribute this decisional load.
Moreover, the implementation of SDM in global psychiatry is constrained by a mismatch between choice architecture and cultural norms. Prevailing SDM frameworks and decision support tools are predominantly built upon Western, individualistic paradigms of autonomy, assuming a dyadic (provider-patient) interaction. However, in collectivist cultures and resource-constrained healthcare systems, medical decision-making is often triadic, relying on family-substituted or surrogate decision-making models.13 In these contexts, Western-centric PtDAs—or tools not designed for varying health literacy—often fail to shift entrenched, physician-led patterns of care.
By 2014 the efficacy of patient decision aids was established in general medicine,14 but uptake of SDM in psychiatry lagged8—only 2 of 39 adoption studies were in mental health.15 Prior reviews, including a 2023 umbrella review, mainly catalogued interventions and outcomes;11 we instead apply a decision-science lens to 2014–2024 evidence and integrate East Asian triadic decision-making overlooked by Western-centric reviews. To address these critical gaps in the implementation science of mental health, this systematic review synthesizes global evidence from the past decade (2014–2024). Specifically, this study aims to: (1) evaluate the impact of SDM interventions and PtDAs on decision quality (eg., decisional conflict, choice concordance) and clinical outcomes in SMI; (2) systematically map the multi-level barriers—spanning cognitive heuristics, systemic constraints, and tool design flaws—that hinder SDM implementation; and (3) critically examine cross-cultural variations, particularly the tension between individual autonomy and triadic decision-making norms. By applying a decision-science lens to heterogeneous global data, this review aims to provide an evidence-based foundation for designing low-cognitive-load, culturally adaptive decision support architectures to overcome systemic inertia in psychiatric care.
Material and Methods
This study follows the PRISMA 2020 guidelines.16 The systematic review has been registered in the PROSPERO database under registration number: CRD42024614327. The review followed this registered protocol, with deviations introduced to strengthen methodological rigour: risk of bias was assessed with design-specific Joanna Briggs Institute tools rather than an unspecified point-based system; a hybrid GRADE-CERQual certainty assessment was added in response to peer review; and eligible designs were broadened beyond cross-sectional and cohort studies to include qualitative, randomized, quasi-experimental, and mixed-methods studies. The PROSPERO record has been updated accordingly.
Search Strategies
This study focuses on patients with mental illnesses. A systematic search was conducted by the two primary authors (JHD and MLL) across several databases, spanning from January 1, 2014, to November 12, 2024. The databases searched included English-language sources (PubMed, Embase, CINAHL [via EBSCO], Cochrane Library, and Web of Science) and Chinese-language databases (CNKI, Wanfang, and VIP). A systematic search strategy, incorporating keywords, free-text synonyms, and Boolean operators,17 was employed, with the final search strings determined through team consensus. Manual citation tracking of relevant literature was also performed to maximize study inclusion. Full search strategies are provided in Appendix 1 and Appendix 2.
Inclusion and Exclusion Criteria
Study eligibility was defined using the PICOS (Population, Intervention, Comparison, Outcomes, and Study design) framework to ensure methodological transparency. The detailed inclusion and exclusion criteria applied during the literature screening process are summarized in Table 1.
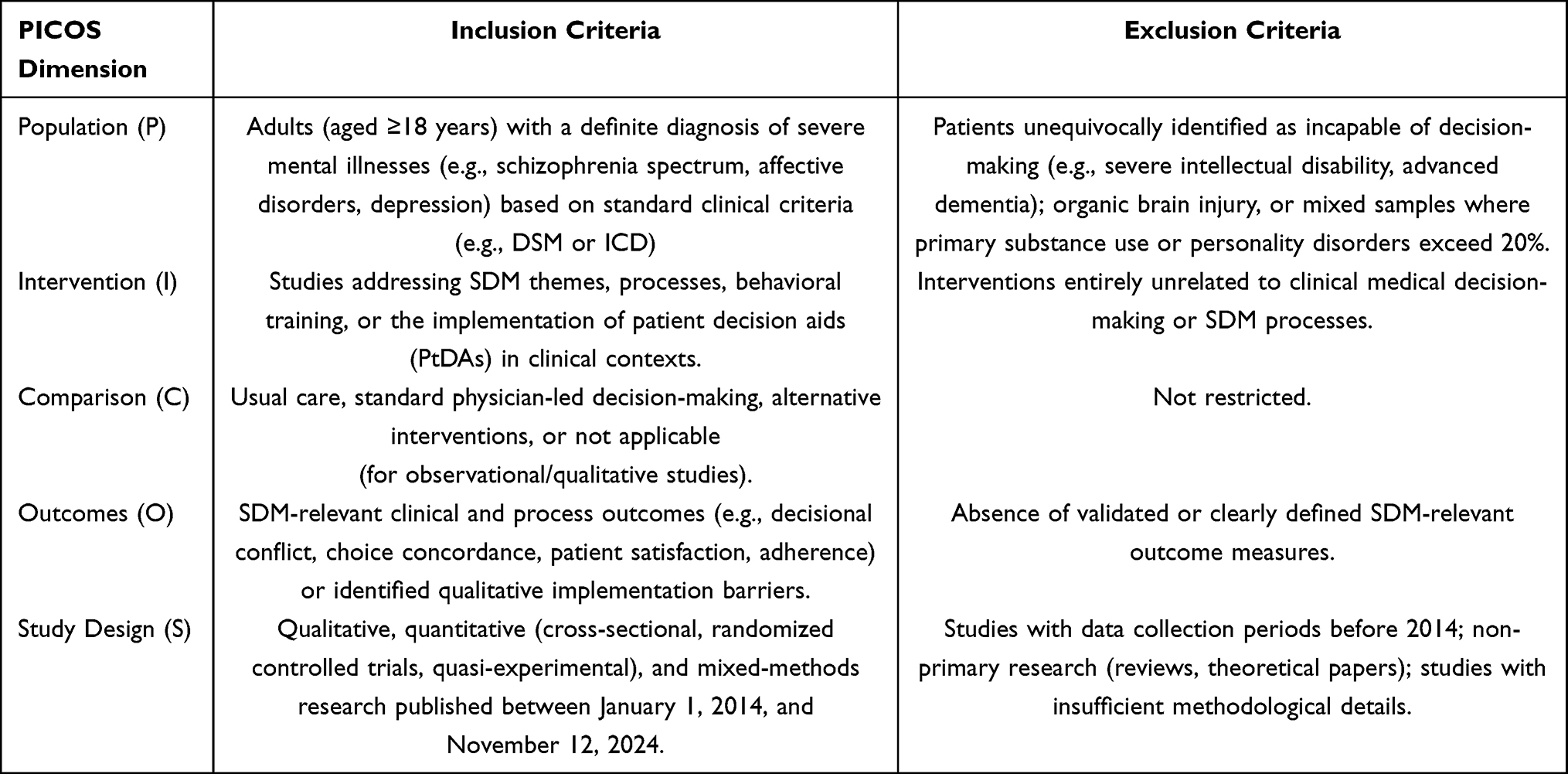 |
Table 1 PICOS Criteria for Study Inclusion and Exclusion |
Study Selection and Data Extraction
Literature search and screening were independently conducted by two authors (JHD and MLL) using Zotero 7.0, following PRISMA guidelines. Before formal screening, the two reviewers independently piloted the eligibility criteria on a random subset of records to calibrate their judgments and resolve interpretive differences; remaining discrepancies throughout screening and data extraction were resolved through consultation with a senior researcher (YQZ). Chinese database searches yielded nine records, none of which met the inclusion criteria due to methodological limitations (eg., lack of validated SDM measures or insufficient methodological details). The study selection procedure is detailed in Appendix 2. Data extraction utilized standardized coding forms capturing author details, publication year, country, diagnostic criteria, settings, sample characteristics, SDM practices, and intervention outcomes. All extracted data were documented in Appendix 3.
This study used the Joanna Briggs Institute (JBI) standardized appraisal tool to assess the risk of bias for the 42 included studies. Study-specific appraisal instruments from JBI were matched to research designs (Figure 1): ① analytical cross-sectional studies (8-item criteria), ② quasi-experimental studies (9-item criteria), ③ randomized controlled trials (13-item criteria), and ④ qualitative studies (10-item criteria). Mixed-methods studies underwent modular appraisal with independent scoring of qualitative and quantitative components. All instruments evaluated four core domains: bias control, methodological coherence, data reliability, and ethical compliance. A four-tier scoring system (yes=1, no=0, not applicable=0, unclear=0) was applied, with type-specific thresholds: cross-sectional (0–8), quasi-experimental (0–9), RCTs (0–13), and qualitative (0–10). Mixed-methods studies were scored by combining the qualitative module (0–10) and the quantitative module according to their respective design-specific criteria. Quality tiers were positively correlated with total scores. Complete appraisal results are detailed in Appendix 4.
 |
Figure 1 Risk of bias of included studies, by Joanna Briggs Institute (JBI) checklist: (A) qualitative (n = 24); (B) cross-sectional (n = 13); (C) randomized controlled trials (n = 7); (D) quasi-experimental (n = 2). Bars show the proportion of studies rated low (green), unclear (yellow), or high (red) risk. Mixed-methods studies were appraised under more than one checklist. For each panel, n is the number of studies appraised with that JBI checklist; the four mixed-methods studies were each appraised under two checklists, so the panel totals (46) exceed the 42 included studies. |
Classification of SDM Approaches
To address the conceptual heterogeneity in SDM research, included studies were classified by their primary SDM operationalization approach (Table 2). Studies were categorized into two domains: intervention studies (n=12) implementing specific SDM-enhancing strategies, and observational studies (n=30) examining SDM processes without targeted interventions. Intervention studies were further subcategorized by target: patient decision aids (n=5), provider training (n=3), patient empowerment programs (n=2), and combined patient-provider interventions (n=2). Observational studies comprised qualitative explorations (n=17) and cross-sectional surveys (n=13). This classification framework allowed a structured interpretation of findings while keeping the varied SDM conceptualizations transparent.
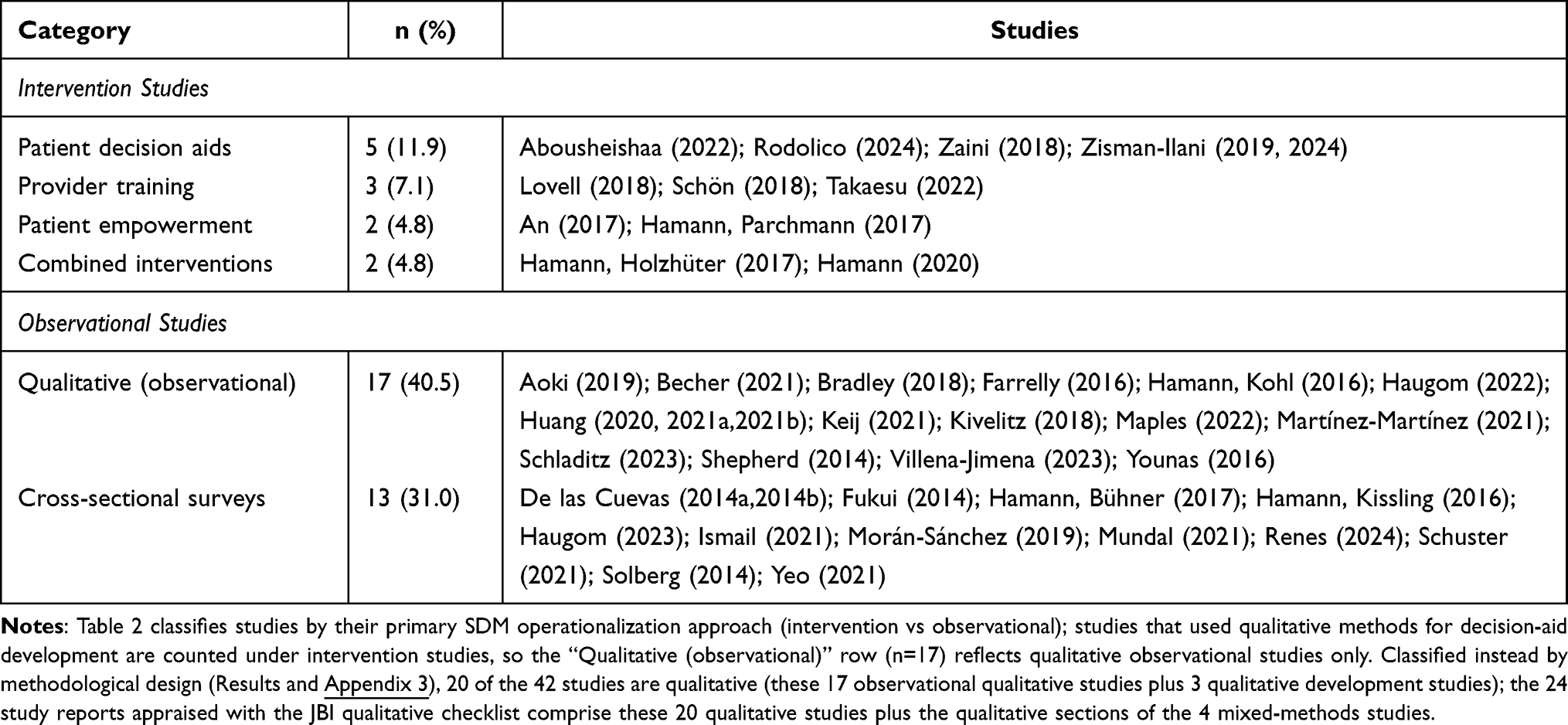 |
Table 2 Classification of Included Studies by SDM Approach (N=42) |
Data Synthesis
Due to substantial heterogeneity in study designs (qualitative 47.6%, cross-sectional 31.0%, RCT 9.5%), clinical populations, intervention types, and outcome measures, quantitative meta-analysis was not feasible. The synthesis followed SWiM guidelines18 and Popay et al19‘s four-element narrative-synthesis framework: (1) theoretical model — a decision-science lens (choice architecture, heuristics) was adopted a priori as an interpretive framework for organizing heterogeneous evidence, not as a tested causal model; (2) preliminary synthesis — studies were classified by SDM operationalization (Table 2) and tabulated by design, population, intervention, comparator, outcome, and effect direction; (3) exploring relationships — findings were cross-stratified by intervention vs. observational design, Western vs. non-Western context, and acute vs. community setting; (4) assessing robustness — methodological quality was appraised using design-specific JBI tools, and a hybrid GRADE-CERQual evidence-certainty assessment was applied to each major thematic claim. Findings were synthesized narratively with structured vote-counting where appropriate. To avoid overinterpreting heterogeneous evidence, we coded each study’s main SDM-related finding as favorable, mixed, null, or unfavorable according to the direction of its primary outcome or dominant qualitative theme. Vote-counting was used only to summarize the direction of evidence, not to estimate pooled effect size or infer causality. Mixed and null findings were retained in the synthesis and considered when judging the certainty of each thematic claim.
Evidence Certainty Assessment
For each major thematic finding, we conducted a hybrid evidence-certainty assessment. Qualitative findings were rated using the CERQual framework20 across four domains: methodological limitations, coherence, data adequacy, and relevance. Quantitative findings were rated using the GRADE approach21 across risk of bias, inconsistency, indirectness, imprecision, and publication bias. Two reviewers (JHD, MLL) independently rated each claim; disagreements were resolved by the senior author (YQZ). Final ratings (High, Moderate, Low, Very Low) appear alongside each claim in Table 3.
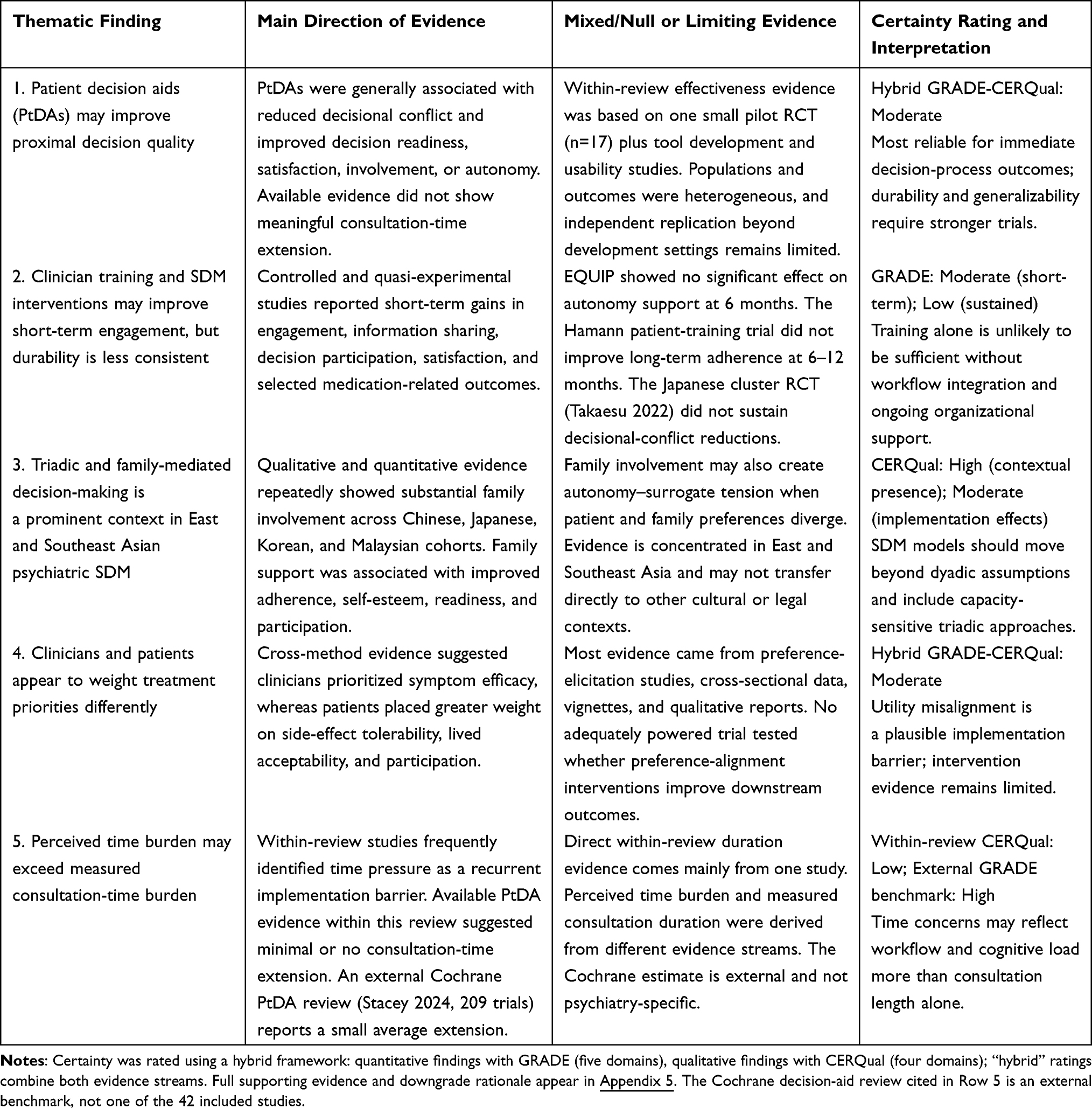 |
Table 3 Summary of Key Thematic Findings, Mixed/Null Evidence, and Evidence-Certainty Ratings (GRADE-CERQual) |
Rationale for Study Selection and Temporal Scope
The inclusion of diverse study designs was methodologically justified given SDM’s complexity as a context-dependent healthcare phenomenon. Qualitative studies illuminated implementation barriers and facilitators that intervention trials alone cannot capture22 while cross-sectional surveys provided population-level prevalence data across settings. Restricting to RCTs would have excluded 90.5% of available evidence. This approach aligns with Cochrane recommendations for complex intervention reviews.23,24 The search was restricted to January 2014 onward to capture the implementation era of SDM in psychiatry. By 2014, the field had shifted from establishing the efficacy of SDM to improving its real-world adoption; a landmark Cochrane review of this period identified only 2 of 39 adoption studies as situated in mental health, underscoring how far psychiatric implementation lagged.15 Evidence on SDM efficacy is already synthesized in earlier reviews of SDM in mental health, which the present review complements rather than duplicates; those reviews focused on intervention efficacy and had searches ending by January 2020.25,26
Results
Search Results and Study Characteristics
As detailed in the PRISMA flow diagram (Appendix 2), the systematic search yielded 4738 records. After removal of duplicates and screening, 42 studies published between 2014 and 2024 were included in the final synthesis; each represented an independent study sample, with no duplicate publications or overlapping cohorts identified. The geographic distribution spanned Europe (n=27), Asia (n=9), North America (n=4), the Middle East (n=1), and Oceania (n=1). The clinical populations predominantly comprised patients with schizophrenia spectrum disorders (78.6%), followed by bipolar disorder (35.7%) and major depressive disorder (35.7%).
To capture the contextual complexity of SDM implementation, the included studies utilized diverse methodological designs (Table 2 and Appendix 3): qualitative studies (n=20, 47.6%), cross-sectional surveys (n=13, 31.0%), randomized controlled trials (RCTs) (n=4, 9.5%), mixed-methods studies (n=4, 9.5%), and quasi-experimental designs (n=1, 2.4%). Quality appraisal using design-specific JBI Critical Appraisal Tools indicated high methodological quality; for instance, 80.0% of cross-sectional studies and 71.4% of RCTs met the highest quality thresholds (Appendix 4). Across the 24 qualitative studies appraised with the JBI qualitative checklist, all reported evidence of formal ethics approval (Appendix 4); the JBI checklists for quantitative, quasi-experimental, and randomized designs do not include a dedicated ethics-approval item, and conflict-of-interest disclosures were not systematically extracted.
Due to the substantial heterogeneity in intervention modalities (eg., decision aids vs. communication training), psychometric instruments (eg., Decisional Conflict Scale vs. SDM-Q-9), and clinical settings, a quantitative meta-analysis was precluded. Furthermore, even within ostensibly homogeneous subsets—for instance, randomized controlled trials measuring decisional conflict with the Decisional Conflict Scale—divergence in intervention components, comparator conditions, and follow-up intervals precluded the derivation of pooled standardized effect estimates. Following the Synthesis Without Meta-analysis (SWiM) guidelines, a narrative thematic synthesis was conducted. All statistical values (eg., coefficients, mean differences, P-values) reported below were extracted directly from the primary studies to indicate effect direction and magnitude, not pooled effects.
The four randomized controlled trials—the only designs supporting causal inference on SDM effects—are summarized in Table 4. All improved proximal decision-process outcomes but none sustained effects on adherence, autonomy support, or durable decisional-conflict reduction.
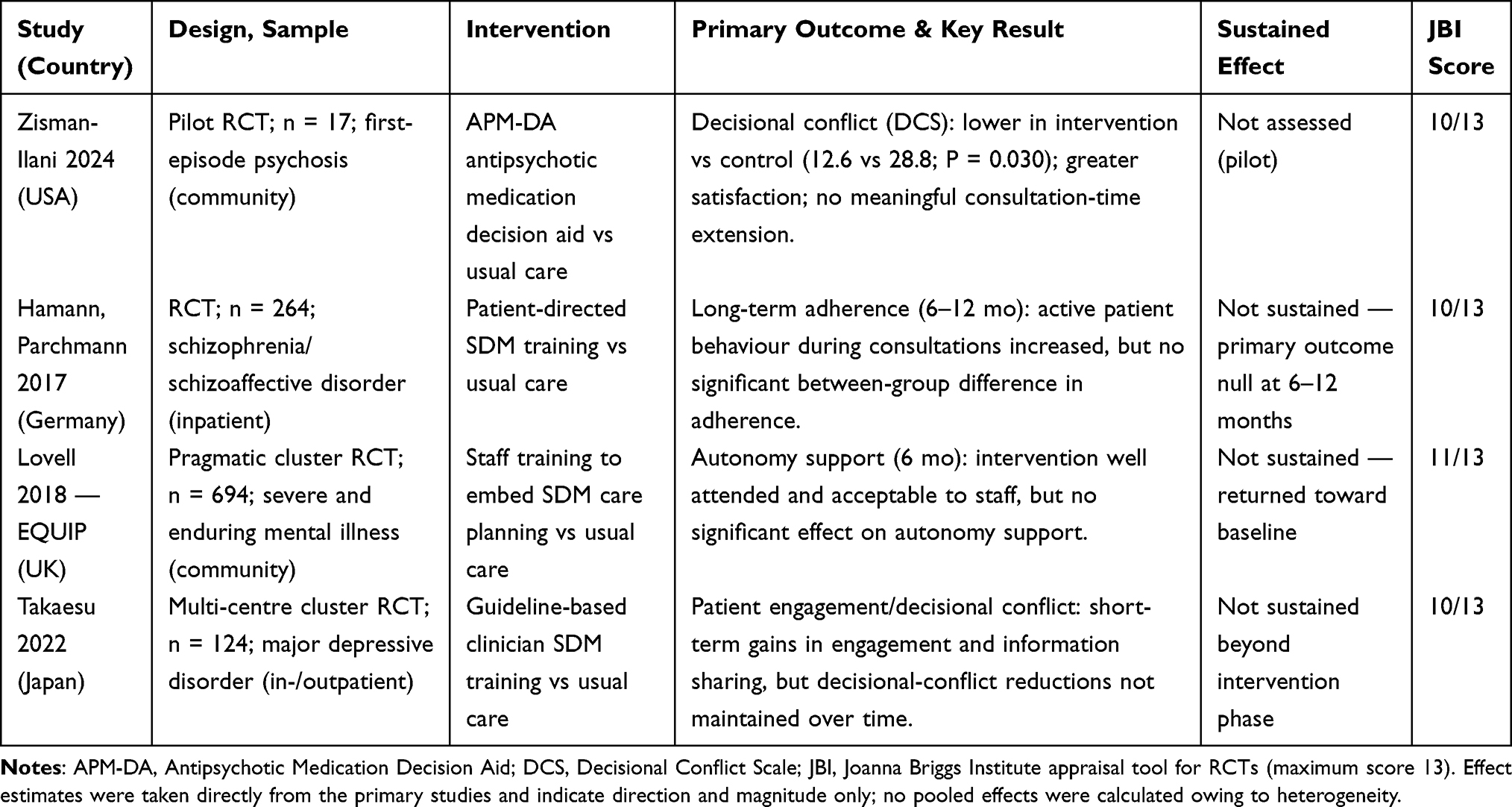 |
Table 4 Summary of Findings from Randomized Controlled Trials of SDM Interventions in Severe Mental Illness |
Thematic Synthesis of SDM Outcomes and Implementation Barriers
Impact on Decision Quality and Choice Concordance
Structured patient decision aids (PtDAs) consistently improved decision quality across the five PtDA studies in this synthesis (Abousheishaa 2022; Rodolico 2024; Zaini 2018; Zisman-Ilani 2019, 2024). In Zisman-Ilani et al 2024 specifically (pilot RCT, n=17), the APM-DA was associated with lower decisional conflict (intervention 12.59±8.21 vs control 28.75±19.86, P=0.030) and greater satisfaction without extending consultation time.27 Similarly, PtDAs improved decision readiness (84.10/100) and patient involvement scores (SDM-Q-9-Psy) in major depressive populations (Abousheishaa et al 2022 specifically).28 The clinical utility of these tools is supported by psychometric validation; for example, in Zisman-Ilani et al 2019 specifically, the application of the SDM-Q-9-PSY scale has been shown to capture and support patients’ sense of participation, remaining reliable during acute psychiatric hospitalization.29
Beyond static tools, behavioral training targeting the clinical dyad operationalized SDM. In Hamann, Parchmann et al 2017 specifically (n=264 RCT), patient-directed training increased active patient behavior in inpatient consultations, although the trial’s primary outcome (long-term adherence at 6–12 months) showed no significant group difference.30 Qualitative explorations helped explain the mechanisms behind these shifts, showing that interventions such as joint crisis plans reshape the therapeutic power dynamic (Farrelly et al 2016 specifically). They strengthened patients’ sense of empowerment and autonomy, supporting a more active role in their care.31 Conversely, clinician training disrupted heuristic biases: in Schön et al 2018 specifically (mixed-methods process evaluation), staff perceived the SDM tool as enhancing bidirectional negotiation and the integration of patient perspectives into clinical workflows; across the three provider-training studies in this synthesis (Lovell 2018; Schön 2018; Takaesu 2022), short-term increases in preference-elicitation behaviours were reported, with long-term maintenance inconsistent.32
These interventions were also associated with broader recovery and adherence outcomes. In An et al 2017 specifically (quasi-experimental study in schizophrenia), an SDM training program improved patients’ self-esteem, problem-solving skills, and quality of life.33 Qualitative findings supported these quantitative outcomes; in Shepherd et al 2014 specifically (qualitative interviews with UK consultant psychiatrists), a participant noted “If they feel they have some choice.that is helpful”.34 These localized benefits were echoed across large-scale, real-world observational cohorts. Large cross-sectional studies found that active SDM involvement aligned with positive medication attitudes and was associated with superior long-term treatment compliance and overall service satisfaction. This held across the three large cross-sectional cohorts in this synthesis (Renes 2024; Solberg 2014; De las Cuevas 2014): massive, diverse populations, including cohorts of patients with bipolar disorder (N=839),35 primary care depression (N=1168),36 and heterogeneous psychiatric outpatients (N=846).37 However, these observational findings should be interpreted as associations rather than evidence of long-term causal effects. Relatedly, in Hamann, Bühner et al 2017 specifically, lower self-stigma and shame were associated with more critical and participative patient communication, the behaviour that underpins shared rather than paternalistic decisions.38,39
Mixed and null findings were observed primarily for distal or sustained outcomes. In Hamann, Parchmann et al 2017, patient-directed training increased active patient behaviour during consultations, but the primary outcome—long-term adherence at 6–12 months—did not differ significantly between groups.30 Similarly, the UK EQUIP cluster RCT (Lovell et al 2018) was acceptable to staff and well attended, but did not demonstrate significant improvements in autonomy support at 6 months.40 In the Japanese multi-centre cluster RCT (Takaesu et al 2022), clinician SDM training was associated with short-term improvements in patient engagement and information sharing, although reductions in decisional conflict were not clearly maintained over time.41 Some PtDA evaluations also suggested possible ceiling effects in cohorts with relatively high baseline decisional self-efficacy.5,42 Taken together, these findings suggest that SDM interventions may produce more consistent effects on proximal decision-process outcomes than on longer-term adherence, sustained clinician behaviour, or durable reductions in decisional conflict.
Cultural Decision Contexts and Surrogate Decision-Making
A critical barrier identified across non-Western cohorts is the fundamental mismatch between the dyadic (provider-patient) assumptions of Western SDM models and local collectivist norms. In East Asian settings, medical decision-making operated as an inherently triadic or heavily surrogate-driven process. In Huang et al 2021 specifically (qualitative study of Chinese mental health professionals), psychiatric treatment decisions were frequently reported as executed by family members rather than patients.6 Mental health professionals attributed this to Confucian ethics prioritizing deference to authority and family consensus, which frequently overrides individual autonomy.13 However, framing familial involvement merely as an obstacle overlooks its clinical utility. Qualitative evidence examining caregiver and patient perspectives in China indicated that active family support serves as a crucial facilitator—significantly improving treatment adherence, preserving patient self-esteem, and promoting social reintegration.6,13 Similarly, in Japanese inpatient settings, formally integrating family members into the SDM process actively mitigated decisional conflicts and alleviated patient anxiety, rather than simply suppressing autonomy.43
This reliance on surrogate decision-making creates a preference-experience gap. In Ismail and Midin 2021 specifically (Malaysian cross-sectional survey of patients with schizophrenia), a 21-percentage-point discrepancy was observed between autonomous role preference (56%) and high SDM experience (35%).44
A comparable pattern was reported in Southern European cohorts (eg., Spain), where outpatients showed significant social desirability bias and tended to understate their participation preferences in line with more physician-led consultation norms.45
The demand for triadic SDM is not unique to collectivist cultures; it is increasingly recognized as a broader clinical need. Evidence from Western contexts reveals that patients and caregivers alike wanted an active role in treatment choices. In Germany, cross-sectional and qualitative findings highlighted a consensus among triads (patients, clinicians, and caregivers), with families advocating for a more integrated role.46,47 Yet, in these individualistic settings, triadic SDM is frequently paralyzed not by cultural deference but by structural barriers. As demonstrated in UK cohorts, stringent hospital privacy regulations, inadequate clinician-caregiver communication, and physician dominance marginalized family input, preventing their integration into the decision context.48
Provider Heuristics and Utility Misalignment
The synthesis highlighted a measurable misalignment in utility weighting between providers and patients regarding preference-sensitive psychopharmacological choices. In Yeo et al 2021 specifically (Australian discrete-choice experiment with 52 doctors and 49 patients), doctors and patients differed significantly in their treatment preferences (P<0.001): doctors were willing to accept a higher risk of side effects in exchange for greater efficacy, whereas patients placed relatively more weight on side-effect tolerability.12 Weight gain and metabolic side effects were the adverse effects of greatest concern to both groups. Qualitative inquiries directly attributed this misalignment to a “drug-led treatment” approach some clinicians reported; participants were described as limiting patient autonomy and the consideration of alternative, preference-sensitive options.49,50
Under time constraints, providers often defaulted to heuristic decision-making, sometimes reinforced through strategic clinical communication. In Hamann, Kohl et al 2016 specifically (qualitative study of patients and psychiatrists), participants described how clinicians implicitly manipulate decision context to maintain authority: by strategically delaying their medical recommendations until late in the consultation, psychiatrists used an anchoring effect: patients’ choices tended to follow the most recently presented option.51 When assessing preferences for long-acting injectable (LAI) antipsychotics, clinicians described overestimating patient resistance (Shepherd et al 2014 specifically, qualitative interviews with UK consultant psychiatrists), consistent with an availability heuristic in which recent or salient cases of non-adherence anchor risk perception, resulting in systematic under-presentation of evidence-based options.34 Under perceived time scarcity, providers frequently reduced SDM to information delivery rather than the harder task of preference elicitation and, in Fukui et al 2014 specifically (an analysis of 128 audio-recorded psychiatric visits), more complete discussion of patient preferences was the strongest predictor of clinician–patient agreement.28,52 This communication breakdown had tangible behavioral consequences: in Younas et al 2016 specifically (qualitative study of UK mental-health pharmacists), pharmacists reported that patient refusal of first-line antipsychotics appears closely associated with unaddressed fears of adverse effects.53
Cognitive Load, Tool Design, and Systemic Constraints
At the patient level, SDM relies heavily on cognitive resources, which are frequently compromised during severe mental illness. In Becher et al 2021 specifically (qualitative findings from the intervention group of an inpatient RCT), during acute psychotic exacerbations, impaired working memory and cognitive overload substantially restricted active SDM participation.5 This cognitive scarcity is multi-dimensional. Qualitative data revealed that beyond acute positive symptoms, environmental stressors and an internalized “mental burden” reduced patients’ motivation to engage in decisions.51,54 Furthermore, patients’ active engagement is often derailed by inconsistent personal preferences and distrust stemming from past negative treatment experiences.42 In Hamann, Bühner et al 2017 specifically, higher self-stigma and shame were associated with less critical and participative communication, with such patients more often deferring to physician recommendations.38
These vulnerabilities are exacerbated by limited human-factors engineering in some decision support tools. Complex visualizations and medical jargon in certain PtDAs contributed to information overload, with Rodolico 2024 and Zaini 2018 specifically reporting that some patients found tool graphics and complex information difficult to interpret.55,56 Moreover, standard tools frequently fail to account for varying levels of health literacy, diverse cultural backgrounds, and intense emotional distress. When information is not culturally tailored, communication often breaks down, making it harder to build the trust that collaborative care requires.57,58
Systemically, high clinician caseloads and the lack of institutional nudges created a hostile environment for SDM sustainability. Macro-environmental constraints strictly dictate the feasibility of patient involvement. Broad cross-sectional data indicated that SDM implementation was highly dependent on socioeconomic factors and care settings (Mundal 2021 specifically), with disparities in participation and positive medication attitudes observed between public and private psychiatric environments.59 In Haugom et al 2023 specifically (a Norwegian cross-sectional study of acute psychiatric care), mandatory care frameworks (eg., compulsory treatment orders) override patient autonomy and leave little room for SDM.60 In the UK EQUIP cluster RCT (Lovell et al 2018) specifically, the SDM intervention was well-attended and acceptable to staff but had no significant effect on the primary outcome (autonomy support) at 6 months, illustrating that absent EHR integration or alignment with organizational performance evaluations, implementation efforts can degrade into compliance-only exercises.40 Consequently, the long-term sustainability of behavioral interventions proved limited: in Hamann, Parchmann et al 2017 specifically, training had no significant effect on long-term adherence at 6–12 months; across the longitudinal evaluations in this synthesis, maintenance of training effects beyond the intervention phase was a consistent challenge attributed to systemic friction.30,32
Discussion
This systematic review of 42 global studies (n = 8798) confirms a central paradox in psychiatric care: while SDM interventions—particularly structured decision aids and behavioral training—consistently enhance immediate decision quality and choice concordance, their real-world implementation remains uneven. By synthesizing heterogeneous evidence through a decision-science lens, we move beyond the conventional narrative of “clinician reluctance” to identify the structural and behavioral mechanisms driving this implementation gap. Specifically, our findings highlight three mechanisms behind this gap: the poor fit of Western dyadic assumptions in non-Western, collectivist decision contexts which rely on family surrogates rather than the provider-patient dyad; a measurable misalignment in utility weighting between providers and patients; and systemic cognitive friction across acute care settings. The evidence, however, should not be interpreted as uniformly positive. The most consistent benefits were observed for proximal decision-process outcomes, including decisional conflict, involvement, satisfaction, and preference elicitation. Evidence was less consistent for distal outcomes such as medication adherence, sustained clinician behaviour, and long-term decisional conflict. This pattern indicates that SDM tools and training may improve the immediate quality of consultations, but their durability appears to depend on workflow integration, clinical setting, and continuing organizational support.
Triadic Decision Contexts vs. Dyadic Assumptions
A primary barrier to global SDM implementation is the structural incompatibility between Western-centric, individualistic decision aids and the cultural realities of collectivist settings. Our synthesis reveals that in East Asian contexts, medical decision-making is often triadic or surrogate-driven, with treatment decisions frequently made by family members, sometimes bypassing the patient entirely.6
Rather than framing this family involvement merely as a “cultural barrier” or a violation of individual autonomy, implementation science must recognize it as the prevailing local decision context. This paradigm shift aligns with emerging conceptual models in cross-cultural bioethics and triadic shared decision-making, which increasingly recognize family companions as essential epistemic partners rather than mere obstacles to individual autonomy.61 The persistent 21-percentage-point gap between patients’ participation preferences and actual experiences in Southeast Asia44 highlights the urgent need to redesign PtDAs from dyadic to triadic models, explicitly incorporating family surrogates as collaborative partners rather than marginalizing them as proxies. When patient and family preferences diverge (eg., a patient prefers Option A while the family surrogate insists on Option B), we propose a capacity-graded resolution: (1) with preserved decisional capacity, patient preference holds final authority and family input is documented; (2) in acute, capacity-limited phases, decisions are deferred or staged to preserve future autonomy; (3) culturally-informed mediators (decision coaches, social workers) facilitate negotiation rather than impose resolution. This capacity-graded triadic model balances individual autonomy with relational accountability and draws on qualitative evidence from East Asian and Southern European studies in our review.
The null yield from Chinese databases (9 records retrieved, 0 eligible) is itself a substantive finding. It may reflect three patterns: (a) limited Mandarin psychometric validation of standard SDM tools (eg., SDM-Q-9) in Chinese psychiatric populations; (b) a research culture oriented toward symptom-outcome trials rather than preference-sensitive implementation studies; and (c) the prevailing triadic decision norm, which renders dyadic SDM frameworks methodologically misaligned with local practice. This gap reinforces our case for culturally-adapted, triadic decision architectures.
Provider Heuristics, Utility Misalignment, and the “Time Illusion”
Our findings reframe provider resistance not as a lack of motivation but as a consequence of heuristic-driven behaviour under systemic pressure. As systematically recognized in contemporary medical decision-making research, cognitive heuristics and diagnostic noise frequently distort clinical judgments in high-uncertainty environments.62 The data reveal a misalignment in how physicians and patients weigh treatment attributes: physicians weigh clinical efficacy (eg., symptom remission) more heavily, whereas patients place relatively greater weight on side-effect tolerability.12 This asymmetry may contribute to clinicians overestimating patients’ resistance to certain treatments34 and preemptively dismissing patients’ decisional capacity to expedite guideline-concordant choices.
Furthermore, this heuristic behavior is perpetuated by a “time illusion.” While clinicians consistently cite time constraints (eg., 15-minute consultations) as the primary barrier to SDM,28 the latest Cochrane systematic review of 209 trials demonstrates that PtDA integration typically extends consultations by a clinically negligible margin (average of 1.5 minutes).14 The perceived time pressure is largely an artifact of administrative burden and cognitive overload, indicating that time barriers must be resolved through systemic workflow redesign rather than individual time-management strategies.
To de-bias this perception, three system-level nudges have shown promise in adjacent literatures and warrant evaluation in psychiatric settings: (1) audit-and-feedback dashboards that display each clinician’s actual versus perceived consultation duration (drawing on the EHR-nudge evidence base63,64); (2) pre-consultation patient priming via tablet-based decision pre-work that redistributes cognitive load away from the consultation window; and (3) institutional reframing of SDM as “time-displacing” rather than “time-adding” — the small upfront investment offsets downstream non-adherence visits and emergency presentations.
Cognitive Friction and Flawed Tool Design
Patient-level barriers must be reframed through the lens of cognitive scarcity. Severe mental illness can compromise the working memory required for decision-making, which may help explain why, even within the intervention arm of a successful SDM trial among acutely ill inpatients, genuine shared decision-making was achieved in only 29% of treatment decisions.5
However, current decision aids frequently fail to accommodate this cognitive vulnerability. Reported difficulty interpreting tool graphics and complex information in some PtDAs exposes a deficit in human-factors engineering,56 failing to meet updated evidence-based standards for cognitive accessibility reaffirmed in the 2024 Cochrane guidelines.14 Presenting complex medical jargon without low-cognitive-load visual risk communication creates cognitive overload, turning a decision aid into a barrier. Furthermore, the association between high self-stigma and reduced participative decision-making behaviour38 reflects internalized assumptions of decisional incapacity, necessitating tools that rebuild decisional self-efficacy rather than merely providing medical information.
Institutional Inertia and the Need for Systemic Nudges
The mixed durability of SDM training effects suggests that short-term educational interventions alone may be insufficient without workflow-level support. Across studies, initial training increased preference-elicitation behaviour, but sustained use was often not maintained; for example, in a Swedish process evaluation, staff enthusiasm after training gave way to routine practice and use of the decision tool remained low across all participating units.32 For example, the Japanese multi-center cluster RCT reported short-term improvements in engagement and information sharing, but did not maintain long-term reductions in decisional conflict without ongoing structural support.41
Similarly, SDM-PLUS appeared more feasible within structured acute inpatient settings,65 yet the same gains were less evident post-discharge, suggesting setting-dependent effects, with such gains gradually reverting into institutional inertia and baseline levels.66
Without integrating SDM metrics into electronic health records (EHR) as mandatory behavioral nudges, or linking decisional quality to value-based reimbursement (Pay-for-Performance), behavioral interventions may succumb to institutional inertia. Drawing on recent implementation science breakthroughs evaluating EHR-embedded nudges in clinical care,63,64 it is evident that in efficiency-driven healthcare systems, training outcomes dissipate unless the choice environment is structurally redesigned to make shared decision-making the default “path of least resistance.”
Task-shifting offers a concrete pathway to address provider cognitive load. Specifically: clinical pharmacists can conduct metabolic-risk and side-effect counseling — the domain where utility misalignment is largest; psychiatric nurses can act as “decision coaches,” guiding patients through preference clarification before and after the consultation; clinical social workers can navigate triadic family dynamics in culturally appropriate ways; and digital-health coordinators can maintain EHR-embedded SDM documentation as the structural nudge. This redistribution directly addresses the cognitive-load problem by sequencing decision work across multiple, less-pressured contact points rather than concentrating it within a 15-minute psychiatric consultation.
Strengths and Limitations
The methodological heterogeneity of the included studies (ranging from qualitative explorations to RCTs) is a core strength of this review, as complex healthcare phenomena like SDM cannot be adequately captured through intervention trials alone.22 However, several limitations warrant acknowledgment. First, the evidence base is predominantly derived from Western and East Asian contexts, with low-resource settings—notably sub-Saharan Africa, Latin America, and the Middle East—markedly underrepresented; differing cultural architectures and health-system structures in these regions may limit the transferability of existing SDM tools. Second, the validity of many decision aids relies heavily on developer-reported data without independent replication. Third, the high heterogeneity in metrics (eg., mean differences, coefficients) precluded a quantitative meta-analysis, necessitating a narrative SWiM approach. Future priorities must include the cross-cultural validation of triadic PtDAs and the longitudinal evaluation of EHR-integrated systemic nudges, evaluated against decisional conflict, choice concordance, medication adherence, and sustained clinician behaviour at 6–12 months.
Conclusion
This systematic review suggests that SDM may improve proximal decision quality and patient involvement in psychiatric care, but evidence for sustained effects on adherence, decisional conflict, and routine implementation remains mixed. This efficacy-to-practice gap appears closely associated with structural constraints in the decision context, alongside cognitive and cultural factors, rather than mere stakeholder reluctance. Specifically, implementation is impeded by a cultural mismatch between Western dyadic models and triadic, surrogate-driven norms in collectivist settings; a measurable misalignment in utility weighting where provider heuristics prioritize symptom remission over patient-weighted side-effect tolerability; and cognitive scarcity exacerbated by poorly designed tools during acute psychiatric episodes.
Bridging this gap requires a strategic shift from the solitary physician-patient dyad to a multidisciplinary systemic redesign. Future clinical workflows must embrace culturally adaptive, triadic decision aids that formally incorporate family companions and utilize human-factors engineering to minimize patient cognitive load. The temporal and cognitive burden of SDM should be distributed across an interprofessional collaborative team—utilizing clinical pharmacists to counsel on metabolic risks, social workers to navigate triadic dynamics, and specialized nurses to assess psychosocial readiness as “decision coaches.” Ultimately, integrating SDM metrics into EHR as mandatory behavioral nudges may be important to disrupt institutional inertia and establish multidisciplinary, collaborative care as the clinical default in global psychiatry. The durability and generalizability of EHR-embedded SDM prompts in psychiatric settings, however, require further prospective evaluation.
Funding
This work was supported by the National Natural Science Foundation of China [grant number:72574066]. The funders were not involved in study design, analysis, or interpretation. They also had no part in manuscript preparation, review, or approval, and did not influence the decision to publish.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Faiman B, Tariman JD. Shared Decision Making: improving patient outcomes by understanding the benefits of and barriers to effective communication. Clinical Journal of Oncology Nursing. 2019;23(5):540–15. doi:10.1188/19.CJON.540-542
2. Charles C, Gafni A, Whelan T. Shared decision-making in the medical encounter: what does it mean? (or it takes at least two to tango). Social Science & Medicine. 1997;44(5):681–692. doi:10.1016/S0277-9536(96)00221-3
3. Zisman-Ilani Y, Roth RM, Mistler LA. Time to support extensive implementation of shared decision making in psychiatry. JAMA Psychiatry. 2021;78(11):1183–1184. doi:10.1001/jamapsychiatry.2021.2247
4. Leucht S, Siafis S, Rodolico A, et al. Shared Decision Making Assistant (SDMA) and other digital tools for choosing antipsychotics in schizophrenia treatment. European Archives of Psychiatry and Clinical Neuroscience. 2023;273(8):1629–1631. doi:10.1007/s00406-023-01712-9
5. Becher S, Holzhüter F, Heres S, Hamann J. Barriers and facilitators of shared decision making in acutely ill inpatients with schizophrenia—Qualitative findings from the intervention group of a randomised-controlled trial. Health Expectations. 2021;24(5):1737–1746. doi:10.1111/hex.13313
6. Huang C, Lam L, Zhong Y, Plummer V, Cross W. Chinese mental health professionals’ perceptions of shared decision-making regarding people diagnosed with schizophrenia: a qualitative study. International Journal of Mental Health Nursing. 2021;30(1):189–199. doi:10.1111/inm.12771_1
7. Joseph-Williams N, Lloyd A, Edwards A, et al. Implementing shared decision making in the NHS: lessons from the MAGIC programme. BMJ. 2017;357:j1744. doi:10.1136/bmj.j1744
8. Slade M. Implementing shared decision making in routine mental health care. World Psychiatry. 2017;16(2):146–153. doi:10.1002/wps.20412
9. Last BA, Timon CE, Timon CE, et al. Systematic review of clinician-directed nudges in healthcare contexts. BMJ Open. 2021;11(7):e048801. doi:10.1136/bmjopen-2021-048801
10. Yoong HA, Stacey F, Grady A, et al. Nudge strategies to improve healthcare providers’ implementation of evidence-based guidelines, policies and practices: a systematic review of trials included within Cochrane systematic reviews. Implement Sci. 2020;15(1). doi:10.1186/s13012-020-01011-0
11. Chmielowska M, Zisman-Ilani Y, Saunders R, Pilling S. Trends, challenges, and priorities for shared decision making in mental health: the first umbrella review. International Journal of Social Psychiatry. 2023;69(4):823–840. doi:10.1177/00207640221140291
12. Yeo V, Dowsey M, Alguera-Lara V, Ride J, Lancsar E, Castle DJ. Antipsychotic choice: understanding shared decision-making among doctors and patients. Journal of Mental Health. 2021;30(1):66–73. doi:10.1080/09638237.2019.1630719
13. Huang C, Plummer V, Wang Y, Lam L, Cross W. I am the person who knows myself best: perception on shared decision-making among hospitalized people diagnosed with schizophrenia in China. International Journal of Mental Health Nursing. 2020;29(5):846–855. doi:10.1111/inm.12718
14. Stacey D, Légaré F, Lewis K, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database of Systematic Reviews. 2014;1:CD001431.
15. Légaré F, Adekpedjou R, Stacey D, et al. Interventions for increasing the use of shared decision making by healthcare professionals. Cochrane Database of Systematic Reviews. 2014;9:CD006732.
16. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. THE BMJ. 2021;372:n71. doi:10.1136/bmj.n71
17. Bramer WM, De Jonge GB, Rethlefsen ML, Mast F, Kleijnen J. A systematic approach to searching: an efficient and complete method to develop literature searches. Journal of the Medical Library Association: JMLA. 2018;106(4):531–541. doi:10.5195/jmla.2018.283
18. Campbell M, McKenzie JE, Sowden A, et al. Synthesis without meta-analysis (SWiM) in systematic reviews: reporting guideline. BMJ. 2020;368:l6890. doi:10.1136/bmj.l6890
19. Popay J, Roberts H, Sowden A, et al. Guidance on the Conduct of Narrative Synthesis in Systematic Reviews: A Product From the ESRC Methods Programme. Vol. 1. 2006:92.
20. Lewin S, Booth A, Glenton C, et al. Applying GRADE-CERQual to qualitative evidence synthesis findings: introduction to the series. Implementation Science. 2018;13(Suppl 1):2. doi:10.1186/s13012-017-0688-3
21. Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. THE BMJ. 2008;336(7650):924–926. doi:10.1136/bmj.39489.470347.AD
22. Légaré F, Thompson-Leduc P. Twelve myths about shared decision making. Patient Education and Counseling. 2014;96(3):281–286. doi:10.1016/j.pec.2014.06.014
23. Noyes J, Booth A, Flemming K, et al. Cochrane Qualitative and Implementation Methods Group guidance series—paper 3: methods for assessing methodological limitations, data extraction and synthesis, and confidence in synthesized qualitative findings. Journal of Clinical Epidemiology. 2018;97:49–58. doi:10.1016/j.jclinepi.2017.06.020
24. Petticrew M, Anderson L, Elder R, et al. Complex interventions and their implications for systematic reviews: a pragmatic approach. Journal of Clinical Epidemiology. 2013;66(11):1209–1214. doi:10.1016/j.jclinepi.2013.06.004
25. Duncan E, Best C, Hagen S. Shared decision making interventions for people with mental health conditions. Cochrane Database of Systematic Reviews. 2010;1:CD007297.
26. Zisman-Ilani Y, Barnett E, Harik J, Pavlo A, O’Connell M. Expanding the concept of shared decision making for mental health: systematic search and scoping review of interventions. Mental Health Review Journal. 2017;22(3):191–213. doi:10.1108/MHRJ-01-2017-0002
27. Zisman-Ilani Y, Parker M, Thomas EC, et al. Usability and feasibility of the antipsychotic medication decision aid in a community program for first-episode psychosis. Psychiatric Services. 2024;75(8):807–811. doi:10.1176/appi.ps.20230230
28. Abousheishaa AA, Lazim NHM, Tang SL, Sulaiman AH, Huri HZ, Guan NC. Antidepressant decision aid for major depressive disorder patients (ADAM): development and pilot testing. Patient Education and Counseling. 2022;105(7):2466–2474. doi:10.1016/j.pec.2021.11.007
29. Zisman-Ilani Y, Roe D, Elwyn G, et al. Shared decision making for psychiatric rehabilitation services before discharge from psychiatric hospitals. Health Communication. 2019;34(6):631–637. doi:10.1080/10410236.2018.1431018
30. Hamann J, Parchmann A, Sassenberg N, et al. Training patients with schizophrenia to share decisions with their psychiatrists: a randomized-controlled trial. Social Psychiatry and Psychiatric Epidemiology. 2017;52(2):175–182. doi:10.1007/s00127-016-1327-z
31. Farrelly S, Lester H, Rose D, et al. Barriers to shared decision making in mental health care: qualitative study of the Joint Crisis Plan for psychosis. Health Expectations. 2016;19(2):448–458. doi:10.1111/hex.12368
32. Schön U-K, Grim K, Wallin L, Rosenberg D, Svedberg P. Psychiatric service staff perceptions of implementing a shared decision-making tool: a process evaluation study. International Journal of Qualitative Studies on Health and Well-Being. 2018;13(1):1421352. doi:10.1080/17482631.2017.1421352
33. An SY, Kim GH, Kim JY. Effectiveness of Shared Decision-Making Training Program in People With Schizophrenia in South Korea. Perspectives in Psychiatric Care. 2017;53(2):111–118. doi:10.1111/ppc.12144
34. Shepherd A, Shorthouse O, Gask L. Consultant psychiatrists’ experiences of and attitudes towards shared decision making in antipsychotic prescribing, a qualitative study. BMC Psychiatry. 2014;14(1):127. doi:10.1186/1471-244X-14-127
35. Renes JW, Metz MJ, Nolen WA, Hoogendoorn AW, Kupka RW, Regeer EJ. Shared decision-making in the treatment of bipolar disorder: findings from a nationwide naturalistic cohort study in everyday clinical practice. Social Psychiatry and Psychiatric Epidemiology. 2024;60(6):1489–1497. doi:10.1007/s00127-024-02761-8
36. Solberg LI, Crain AL, Rubenstein L, Unützer J, Whitebird RR, Beck A. How much shared decision making occurs in usual primary care of depression? The Journal of the American Board of Family Medicine. 2014;27(2):199–208. doi:10.3122/jabfm.2014.02.130164
37. De Las Cuevas C, Peñate W, de Rivera L. To what extent is treatment adherence of psychiatric patients influenced by their participation in shared decision making? Patient Preference and Adherence. 2014;8:1547–1553. doi:10.2147/PPA.S73029
38. Hamann J, Bühner M, Rüsch N. Self-stigma and consumer participation in shared decision making in mental health services. Psychiatric Services. 2017;68(8):783–788. doi:10.1176/appi.ps.201600282
39. De Las Cuevas C, Peñate W. To what extent psychiatric patients feel involved in decision making about their mental health care? Relationships with socio-demographic, clinical, and psychological variables. Acta Neuropsychiatrica. 2014;26(6):372–381. doi:10.1017/neu.2014.21
40. Lovell K, Bee P, Brooks H, et al. Embedding shared decision-making in the care of patients with severe and enduring mental health problems: the EQUIP pragmatic cluster randomised trial. PLoS One. 2018;13(8):e0201533. doi:10.1371/journal.pone.0201533
41. Takaesu Y, Aoki Y, Tomo Y, et al. Implementation of a shared decision-making training program for clinicians based on the major depressive disorder guidelines in Japan: a multi-center cluster randomized trial. Frontiers in Psychiatry. 2022;13:967750. doi:10.3389/fpsyt.2022.967750
42. Maples NJ, Velligan DI, Jones EC, Espinosa EM, Morgan RO, Valerio-Shewmaker MA. Perspectives of patients and providers in using shared decision making in psychiatry. Community Mental Health Journal. 2022;58(3):578–588. doi:10.1007/s10597-021-00856-z
43. Aoki Y, Furuno T, Watanabe K, Kayama M. Psychiatric outpatients’ experiences with shared decision-making: a qualitative descriptive study. Journal of Communication in Healthcare. 2019;12(2):102–111. doi:10.1080/17538068.2019.1612212
44. Ismail MA, Midin M. Shared decision-making and role preference among patients with schizophrenia in Malaysia: a cross-sectional study. Frontiers in Psychiatry. 2021;12:680800. doi:10.3389/fpsyt.2021.680800
45. Morán-Sánchez I, Gómez-Vallés P, Bernal-López MÁ, Pérez-Cárceles MD. Shared decision-making in outpatients with mental disorders: patients´ preferences and associated factors. Journal of Evaluation in Clinical Practice. 2019;25(6):1200–1209. doi:10.1111/jep.13246
46. Schladitz K, Weitzel EC, Löbner M, et al. Experiencing (shared) decision making: results from a qualitative study of people with mental illness and their family members. Healthcare. 2023;11(16):2237. doi:10.3390/healthcare11162237
47. Schuster F, Holzhüter F, Heres S, Hamann J. ‘Triadic’ shared decision making in mental health: experiences and expectations of service users, caregivers and clinicians in Germany. Health Expectations. 2021;24(2):507–515. doi:10.1111/hex.13192
48. Bradley E, Green D. Involved, inputting or informing: “Shared” decision making in adult mental health care. Health Expectations. 2018;21(1):192–200. doi:10.1111/hex.12601
49. Martínez-Martínez C, Sánchez-Martínez V, Ballester-Martínez J, Richart-Martínez M, Ramos-Pichardo JD. A qualitative emancipatory inquiry into relationships between people with mental disorders and health professionals. Journal of Psychiatric and Mental Health Nursing. 2021;28(4):721–737. doi:10.1111/jpm.12727
50. Villena-Jimena A, Morales-Asencio JM, Quemada C, Hurtado MM. “It’s That They Treated Me Like an Object”: a qualitative study on the participation of people diagnosed with psychotic disorders in their health care. International Journal of Environmental Research and Public Health. 2023;20(5):4614. doi:10.3390/ijerph20054614
51. Hamann J, Kohl S, McCabe R, et al. What can patients do to facilitate shared decision making? A qualitative study of patients with depression or schizophrenia and psychiatrists. Social Psychiatry and Psychiatric Epidemiology. 2016;51(4):617–625. doi:10.1007/s00127-015-1089-z
52. Fukui S, Salyers MP, Matthias MS, et al. Predictors of shared decision making and level of agreement between consumers and providers in psychiatric care. Community Mental Health Journal. 2014;50(4):375–382. doi:10.1007/s10597-012-9584-0
53. Younas M, Bradley E, Holmes N, Sud D, Maidment ID. Mental health pharmacists views on shared decision-making for antipsychotics in serious mental illness. International Journal of Clinical Pharmacy. 2016;38(5):1191–1199. doi:10.1007/s11096-016-0352-z
54. Kivelitz L, Härter M, Mohr J, et al. Choosing the appropriate treatment setting: which information and decision-making needs do adult inpatients with mental disorders have? A qualitative interview study. Patient Preference and Adherence. 2018;12:823–833. doi:10.2147/PPA.S164160
55. Rodolico A, Di Francesco A, Cutrufelli P, et al. Developing STEP-SE: a Qualitative Usability Study of a Novel Patient-Reported Outcomes Tool for Managing Side Effects in Shared Decision-Making for Schizophrenia Spectrum Disorder Care. Health Expectations. 2024;27(6):e70019. doi:10.1111/hex.70019
56. Zaini S, Manivanna Bharathy HA, Sulaiman AH, et al. Development of a strategic tool for shared decision-making in the use of antidepressants among patients with major depressive disorder: a focus group study. International Journal of Environmental Research and Public Health. 2018;15(7):1402. doi:10.3390/ijerph15071402
57. Haugom EW, Stensrud B, Beston G, Ruud T, Landheim AS. Experiences of shared decision making among patients with psychotic disorders in Norway: a qualitative study. BMC Psychiatry. 2022;22(1):192. doi:10.1186/s12888-022-03849-8
58. Keij SM, van Duijn-Bakker N, Stiggelbout AM, Pieterse AH. What makes a patient ready for shared decision making? A qualitative study. Patient Education and Counseling. 2021;104(3):571–577. doi:10.1016/j.pec.2020.08.031
59. Mundal I, Lara-Cabrera ML, Betancort M, De Las Cuevas C. Exploring patterns in psychiatric outpatients’ preferences for involvement in decision-making: a latent class analysis approach. BMC Psychiatry. 2021;21(1):133. doi:10.1186/s12888-021-03137-x
60. Haugom EW, Benth JŠ, Stensrud B, Ruud T, Clausen T, Landheim AS. Shared decision making and associated factors among patients with psychotic disorders: a cross-sectional study. BMC Psychiatry. 2023;23(1):747. doi:10.1186/s12888-023-05257-y
61. Laidsaar-Powell RC, Butow PN, Bu S, et al. Physician–patient–companion communication and decision-making: a systematic review of triadic medical consultations. Patient Education and Counseling. 2013;91(1):3–13. doi:10.1016/j.pec.2012.11.007
62. Blumenthal-Barby JS, Krieger H. Cognitive biases and heuristics in medical decision making: a critical review using a systematic search strategy. Medical Decision Making. 2015;35(4):539–557. doi:10.1177/0272989X14547740
63. Nguyen OT, Kunta AR, Katoju SV, et al. Electronic health record nudges and health care quality and outcomes in primary care: a systematic review. JAMA Network Open. 2024;7(9):e2432760. doi:10.1001/jamanetworkopen.2024.32760
64. Trinkley KE, Maestas Duran D, Zhang S, et al. Application of nudges to design clinical decision support tools: systematic approach guided by implementation science. Journal of Medical Internet Research. 2025;27:e73189. doi:10.2196/73189
65. Hamann J, Holzhüter F, Stecher L, Heres S. Shared decision making PLUS–a cluster-randomized trial with inpatients suffering from schizophrenia (SDM-PLUS). BMC Psychiatry. 2017;17(1):78. doi:10.1186/s12888-017-1240-3
66. Hamann J, John M, Holzhüter F, Siafis S, Brieger P, Heres S. Shared decision making, aggression, and coercion in inpatients with schizophrenia. European Psychiatry. 2020;63(1):e90. doi:10.1192/j.eurpsy.2020.88
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
What It Takes to Manage Change: A Qualitative Study of Healthcare Managers’ Role Perceptions in Supporting and Sustaining TeamSTEPPS Implementation
Lüchinger R, Blondon K, Junod Perron N, Audétat MC
Journal of Healthcare Leadership 2026, 18:584769
Published Date: 30 April 2026