")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Bridging Allied Health Professional Roles to Improve Patient Outcomes in Rural and Remote Australia: A Descriptive Qualitative Study
Authors Taylor SM , Culic A , Harris S, Senini R, Stephenson R, Glass BD
Received 31 January 2022
Accepted for publication 8 March 2022
Published 22 March 2022 Volume 2022:15 Pages 541—551
DOI https://doi.org/10.2147/JMDH.S360654
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Selina M Taylor,1,2 Aimee Culic,1 Sophie Harris,1 Rebecca Senini,1 Rebecca Stephenson,1 Beverley D Glass1
1Pharmacy, College of Medicine and Dentistry, James Cook University, Townsville, QLD, 4811, Australia; 2Murtupuni Centre for Rural and Remote Health, James Cook University, Mount Isa, QLD, 4825, Australia
Correspondence: Selina M Taylor, Murtupuni Centre for Rural and Remote Health, James Cook University, PO Box 2572, Mount Isa Hospital Campus, Joan/Deighton Street Entrance, Mount Isa, QLD, 4825, Australia, Tel +61 7 4745 4500, Email [email protected]
Purpose: Australia’s rural and remote populations experience inequality of access to healthcare, with demand exceeding capacity for delivery of health services, often due to a maldistribution of the health workforce. A strategy which may overcome barriers to accessing adequate healthcare includes implementation of interdisciplinary collaborative teams, identified as a successful method of healthcare delivery. This study thus aimed to explore interdisciplinary allied health collaborative practice in a rural community.
Methods: Role theory, as a philosophical perspective, was used to explore role perceptions and the potential for interdisciplinary collaboration between pharmacists and allied health professionals including dieticians/public health nutritionists, speech pathologists, occupational therapists, and physiotherapists, by conducting 29 interviews in a rural community. All interviews were transcribed verbatim, coded, and categorised into emerging themes.
Results: Five constructs of role theory were used to describe the data: role identity, role overload, role sufficiency, role conflict, and role ambiguity. Participants identified as rural generalists and health promoters, who work within innovative and adaptive healthcare settings. Role overload was reported as considerable due to high demand for services and a lack of resources in rural and remote regions, resulting in poor role sufficiency. Overall, there was a low level of role conflict, and participants were highly in favor of interprofessional collaboration; however, uncertainty of the pharmacist’s role (role ambiguity) was a major barrier identified. Health professionals with more years in practice provided few examples of how they would utilise a pharmacist in their practice, although these gave valuable insight into the potential integration of a pharmacist into an interdisciplinary health team, with allied health professionals.
Conclusion: This study has applied role theory providing a greater understanding of the enablers and barriers of pharmacists working within interdisciplinary allied health teams and highlighting opportunities to bridge interprofessional roles to improve patient outcomes, especially in rural and remote communities.
Keywords: interdisciplinary, pharmacist, dietician, occupational therapist, physiotherapist, speech pathologist
Introduction
Rural communities experience significant inequality within the Australian healthcare system due to declining populations, economic stagnation and shortages of healthcare professionals.1 Predisposition to healthcare deficits in rural communities has been shown to result in lower engagement with preventative healthcare services, decreased life expectancies and negative health outcomes.1 Due to lack of referral opportunities in rural communities, where demand does not satisfy the capacity to deliver specialised services, interdisciplinary collaboration and an increased skill set for all health professionals is often required to meet the need for generalist, rather than specialist care.2 Interdisciplinary collaboration may involve a range of healthcare professionals partaking in information sharing and team-based problem-solving to achieve shared goals.2,3 Within primary health, collaboration has been shown to greatly improve the quality of care delivered to patients.3
Workforce distribution is disproportionate for those in remote and very remote locations.4 It is widely recognised that health workforce density reduces, the further the distance from metropolitan cities.4 Pharmacist workforce density in urban areas is reported at 120 per 100,000 population, compared with 60 for remote and very remote areas.4 This reduction is also reflected in allied health professions with physiotherapists reporting 51/100,000 (remote) compared to 117/100,000 (urban) and occupational therapists even more sparse at 23/100,000 (remote) compared to 68/100,000 (urban).4 Comparatively, general practitioners (GP) have a greater population in remote and very remote areas 134/100,000 compared to urban 108/100 000.4 However, this is a reflection of the limited availability of secondary and tertiary medical practitioners available in more remote locations, and thus the GP workforce provides most of the medical services provided in these communities. These density profiles highlight the importance of collaborative healthcare models to ensure the valuable and limited health professionals in rural and remote locations are utilised most effectively.
On average, Australians visit their local pharmacy 12–14 times per year.5 Therefore, as one of the most accessible primary healthcare providers, pharmacists have an essential role in providing advice and onwards referrals.5 In rural communities, pharmacists are often expected to work to an expanded scope of practice to fill gaps consequential to poor workforce distribution.5 There is evidence to suggest that pharmacists and other allied health professionals, including dieticians, speech pathologists, occupational therapists and physiotherapists, can collaborate to address these gaps and alleviate workforce strain.3
Evidence of the potential for professional collaboration already exists between pharmacists and allied health professionals. Pharmacists liaise with dieticians to provide education to patients about medication, adherence and offer lifestyle advice with a focus on nutrition.6 Dieticians and pharmacists may collaborate in chronic disease management programs such as implementation of community-based diabetes clinics, which have the potential to improve glucose control, self-management, education and overall diabetes management.6 Diabetes in rural communities is highly prevalent and drastically undertreated,7 thus collaboration of dieticians and pharmacists may improve this major health burden.8
Speech pathologists and pharmacists may collaborate to reduce medication administration errors in patients who have dysphagia, as these patients are more than twice as likely to be involved in medication administration errors.9 Limited availability of varied dosage forms creates challenges when it comes to clinical decision making, therefore it has been suggested that collaboration between these two disciplines may target early intervention strategies to optimize medication management and prevent worsening conditions.10 Occupational therapists’ collaboration with pharmacists has the potential to improve home-health care services, evaluate patient medication-related skills and identify risks of non-adherence.11 This collaboration will allow recommendations for supportive aids to reduce medication misadventure, implementation of health literacy interventions, and additional support for palliative care services.11 Physiotherapist and pharmacist collaboration has the potential to combine diagnostic skills and physical therapy with expertise in pharmacology to provide optimal therapy.12 Information sharing between physiotherapists and pharmacists ensures that pharmacotherapy complements physical therapy to significantly improve patient outcomes, decrease recovery time for acute conditions and reduce the number of medication-related side effects experienced by patients.12,13
Collaboration between allied health professions and pharmacists in rural and remote Australia may be challenged by the sociological concepts of role theory: role identity, role overload, role sufficiency, role conflict and role ambiguity.14–16 These concepts have been explored to assess the attitudes of health professionals towards interdisciplinary collaboration to provide a potential solution to address disparities in access to health services in rural and remote communities. Studies have also been undertaken to assess poor workforce distribution in rural Australia and the benefits of interdisciplinary collaboration.1–3,6,10 However, this study has focused specifically on primary care dieticians’, speech pathologists’, occupational therapists’, and physiotherapists’ potential for collaboration with pharmacists in rural communities and aims to identify whether pharmacists can be utilised within a collaborative care model.
Materials and Methods
Study Design
An ethnographic lens for rural culture was applied to this phenomenological descriptive qualitative study. Rural dieticians, speech pathologists, occupational therapists and physiotherapists were interviewed using an in-depth semi structured interview process.
Setting, Participants and Recruitment
During February 2021, rural Australian allied health professionals were recruited through networks at the Murtupuni Centre for Rural and Remote Health in Mount Isa. Recruitment occurred via email and telephone. All except 4 invited participants agreed to be interviewed. The mode of the interview was dependent on participant preference and availability (eg face-to-face/telephone). To be eligible for inclusion in this study, health professionals needed to be working in a rural or remote location, as reported by the participant and be willing to participate.
Data Collection
Health professionals were contacted via direct communication, provided with an information sheet; and, if happy to participate, returned a written informed consent include consent for publication of anonymised responses. Interviews were conducted by all authors with varying levels of experience and novice interviewers were supported by senior authors. All interviews were audio recorded and transcribed verbatim; and data were de-identified in the transcription process. Demographic data collected included: age, gender, occupation, years of practice and practice setting. The interview guide was designed and piloted by three interviewees who were not included in the study, and aligned to the five constructs of role theory. Participants were also asked to describe their previous practice settings to gain a deeper understanding of their perceptions towards rural health and years of practice were documented to develop insight into the experience of each allied health professional.
Data Analysis
Framework analysis based on the work of Hardy and Conway 1988 was applied to collected data and all interview transcriptions were included in the analysis.14 The transcription process allowed researchers to become familiar with data to understand the context of research. Development of the framework involved confirmation of coding and development of themes informed by five constructs of role theory.14 Emergence of phenomenological descriptions in response to research questions allowed for interpretation of data. AC, SH, RS and RS conducted the coding independently and each transcription was revised by two authors, discrepancies were resolved by ST. ST and BG reviewed five randomly selected coded transcriptions. Assumed knowledge and bias were minimized and four participants were contacted via email for member checking in the validation process, to ensure that transcriptions were an accurate representation of their interview responses.
Ethics Approval
Ethical approval was granted by James Cook University Human Research Ethics Committee (H8278).
Results
Twenty-nine semi-structured interviews were conducted face-to-face (25), via telephone (2), and via video conference (2), with interview duration ranging from 14 to 46 minutes. Allied health professionals interviewed located in Mount Isa (28), and Weipa (1), included dieticians (4), a nutritionist (1), speech pathologists (6), occupational therapists (11) and physiotherapists (7). The mean age was 32.8 years, with a range from 22–65 years. Demographic data are summarised in Table 1. Direct quotes were annotated with each allied health professional’s primary occupation and numbered. Years of practice significantly influenced the responses from participants, where it was found that with increased clinical experience came an increased recognition of opportunity for pharmacist input in patient therapy, and increased potential for interdisciplinary collaboration.
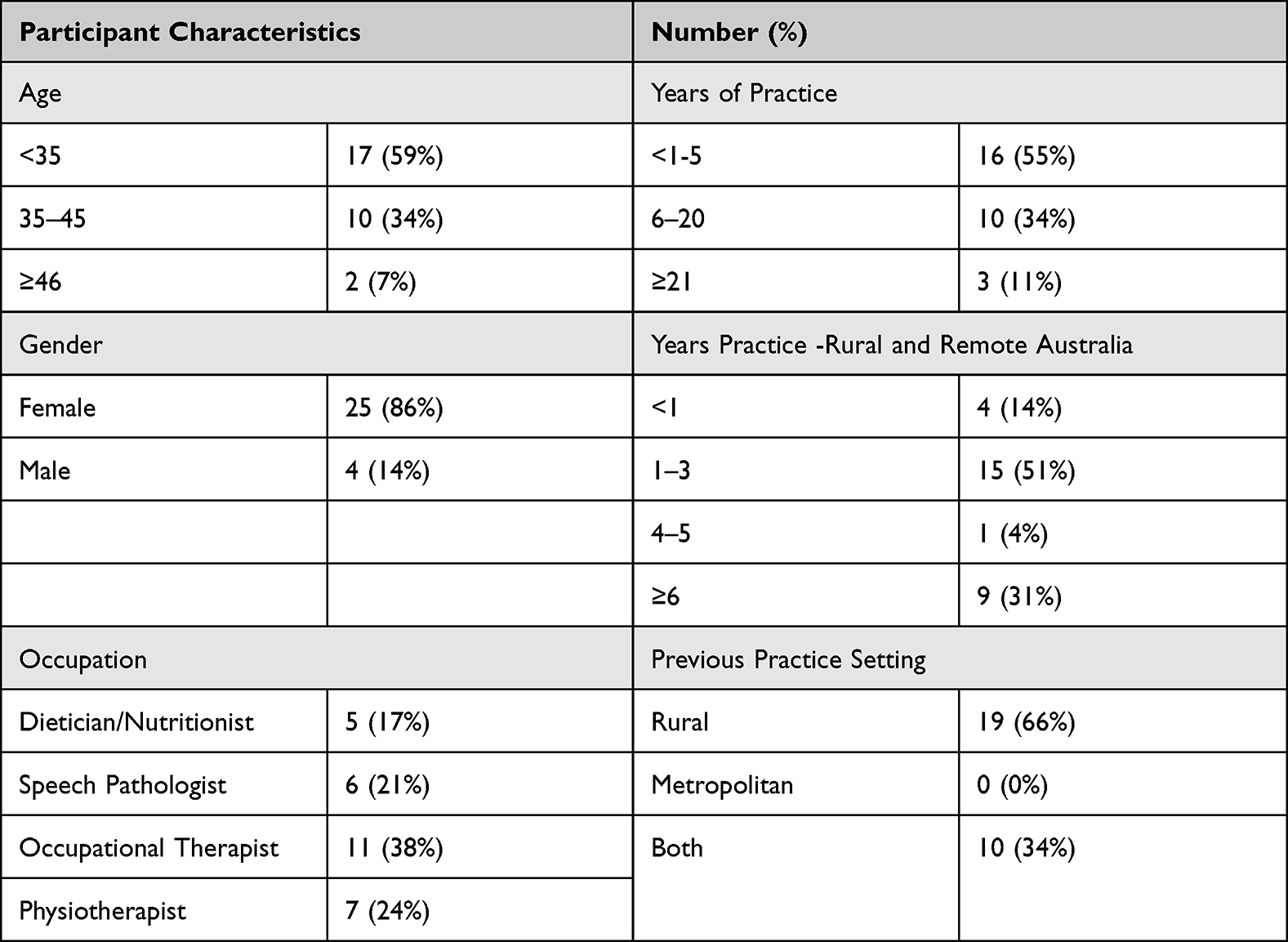 |
Table 1 Demographic Data for Participants (N = 29) |
Table 2 defines the role constructs investigated.14 These concepts describe a person’s role in society, outlining a set of rights, duties, expectations, norms, and behaviours.14
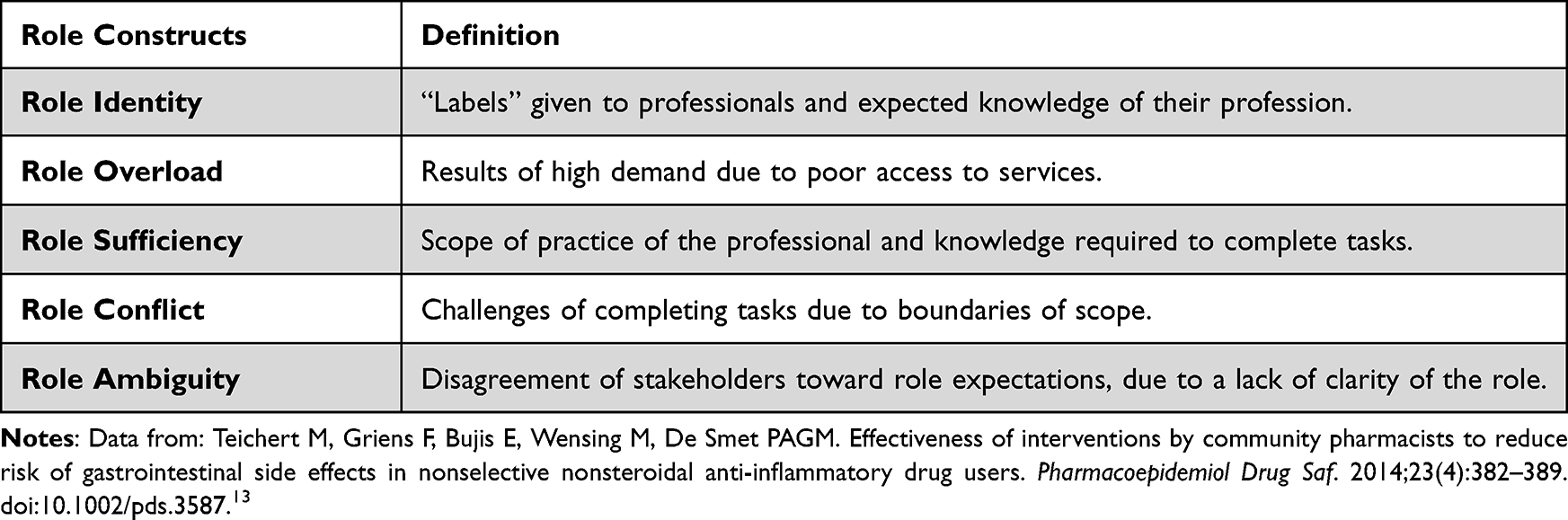 |
Table 2 Definitions of Role Theory Constructs |
Role Identity
Investigating role identity recognised recurrent themes regarding allied health professionals in rural communities operating in a generalist role; as well as implementing adaptive and innovative practices, and frequently participating in health promotion and community engagement. Professionals acknowledged that they enjoyed working with a variety of caseloads and experiencing a wide range of clinical presentations, unique to rural health settings. Participants mentioned that “no day is the same” and the broad range of clinical presentations they manage, covers the whole lifespan; some days are spent working in schools and other days are spent in patients’ homes. The majority of rural health professionals stated that they lacked access to referral pathways and to more specialised services. It was also popular opinion that the “problem-solving” aspect of the rural generalist role is a feature, which gave them great satisfaction.
“You do what you can because there’s no one else to do it.” (Physiotherapist 1)
The allied health professionals collectively agreed that the unpredictability of their job requires adaptability. With a lack of resources and a varied caseload, there was consensus that they are expected to “think outside the box” and must make do with what they have, to provide services for each individual patient. Participants agreed that outreach services require provision of basic patient education to ensure they have the adequate skills to manage their health, when professionals are unavailable. Participants who had previously worked in metropolitan locations reinforced the increased need for adaptiveness and innovation due to the need for greater flexibility in providing healthcare, compared to metropolitan practice.
We have to be creative about how our services can be delivered. My task involves exploring … how [patients] can be creative with the resources that we/they have to provide better services. (Occupational Therapist 1)
Participants also highlighted health promotion and community engagement as an important part of their role as health professionals in a rural community. This ranges from offering support in classrooms and “mums and bubs” groups, to engaging with the community in Cooking groups and meeting with councils and community organizations. Community involvement allows these professionals to establish rapport, which aids the provision of optimal healthcare to the entire community, inclusive of disengaged community members, patients with low health literacy and vulnerable children.
“It’s not just seeing the people referred to us; but I think we’ve also got to do a little bit more health promotion and community engagement work.” (Speech Pathologist 1)
Role Overload
Investigation into role overload demonstrated that many rural and remote based allied health professionals unsurprisingly have a significant workload. Participants acknowledged that they see many patients and experience a heavy caseload, which constantly expands due to growth and increased uptake of both local and outreach community services, with some practitioners seeing over 30 patients in each remote community.
Most agreed that in outreach communities they experience more pressure to see clients due to the lack of availability of permanent health services, however professionals are limited by time they spend in these communities, where chronic disease is highly prevalent. Participants agreed that they are required to prioritise their clients, enabling them to see more complex or “at risk” patients. Despite this, many patients are put on long wait lists, which may result in waiting several months or years to see desired practitioners.
“Dieticians have always got 100 plus [patients] on their waiting list but then in terms of identifying priorities, we triage the top 20.” (Dietician 1)
It was also noted that recruiting and retaining staff can be challenging in rural practice settings.15 There is limited attraction for health professionals to practice in rural communities due to the extent of isolation and lack of professional incentives,15,16 with many organizations reporting difficulty acquiring staff; therefore, contributing to the large workload.
“We’ve had the private practice out here, the speech pathology role there has been vacant for over 12 months now.” (Speech Pathologist 2)
In rural practice, building interprofessional relationships with other health professionals is crucial for patients and staff alike.15 It was highlighted that the inability to retain staff, for adequate durations, prevents the opportunity to develop strong professional relationships and build patient rapport. Furthermore, many clinicians agreed that it is demotivating to see people “come and go” over time and noted that the high staff turnover is counterproductive and time consuming, thus contributing to role overload. With a limited number of clinicians available there is “little support”, resulting in uneven distribution of workload, with participants identifying a high incidence of burnout. Professional support also becomes an issue, when staff are unable to cover for someone to take personal leave.
“If you’re not there … that person is unable to access care … because there are no other health professionals readily available to cover you on leave.” (Occupational Therapist 2)
Role Sufficiency
The scope of practice of health professionals in rural and remote communities is often expanded and therefore requires greater adaptability.15 All participating professionals expressed discontentment with both resources available to them and access to resources in the community, resulting in role insufficiency.
I think in remote and very remote areas, general resources are pretty poor. Sometimes there is more of a focus on the clinical space, which again is poorly resourced as well … so often, you are really working with nothing. (Dietician 2)
Most participants agreed that they were resourced with the bare minimum required to perform tasks and stated that enhancement of resources would significantly improve the wellbeing of the community. For example, occupational therapists require many physical resources to effectively treat patients, however access to such resources in rural settings is challenging. One occupational therapist stated that availability, transportation, and funding for equipment proved extremely difficult and that this was disadvantageous to the provision of care.
In the community, OT access to physical things like wheelchairs and equipment is near impossible, we have no trial options … there is a level of frustration but once you’ve been here long enough, you just accept it. (Occupational Therapist 3)
Overall participants agreed that they were able to access adequate resources to perform the baseline tasks for their profession. However, all agreed that with improved funding, resources and staffing, there would be a significant positive impact on the provision of healthcare to their community.
Role Conflict
Overall, all the participants agreed that there is a low level of role conflict between professions and that they all work to an expanded scope of practice in rural and remote settings to fill the gaps in healthcare. Most referred to working to their “full scope” in a generalist role, rather than specializing in a niche area of their profession, as they would in a metropolitan area. This was attributed to a large demand for care across a wide number of specialties; although not enough workload to substantiate the need for specialists within any of the professions.
“It is difficult to know where your scope ends in a rural setting … sometimes I feel like we end up being the whole multidisciplinary team.” (Occupational Therapist 4)
Each discipline collectively believed that there is no fear of “stepping on other professions’ toes” in rural practice. The consensus is that if professionals possess the skills and are “not putting their patient in harm’s way” then it is okay to provide services that expand the boundaries of their scope of practice. The lifestyle that comes with living in rural locations means that, over time, healthcare providers across the disciplines develop relationships on both a professional and social level. Therefore, due to improved rapport, rural allied health professionals tend to be happier to work together, rather than to maintain rigid borders between professions.
There will always naturally be a bit of blending, but as long as you’re within your typical scope of practice and you’re not putting anyone in danger you’re fine. (Physiotherapist 2)
Due to a high workload and lack of services to meet demands of the community, practitioners are more likely to collaborate for better patient outcomes rather than be protective of potential clientele. A lack of understanding around utilisation of pharmacists skills and knowledge prevented establishment of conclusive evidence as to whether dieticians, speech pathologists, occupational therapists or physiotherapists believe that a pharmacist would provide conflicting or mutually exclusive services. However, the allied health professionals were more likely to contact or refer a patient to their GP for medication related issues.
“We are always sending them to the doctor for [medication recommendations], so I think it’s kind of —- who do you send them to? The pharmacist or the doctor?” (Physiotherapist 3)
It is perceived that referral to a GP would be more beneficial for patients as the doctor is believed to have a more thorough understanding of the patient’s health conditions and would be more likely to provide solutions for medication related issues due to their prescribing rights. Furthermore, referrals to the GP are regarded as more important as “the GP should be coordinating” the patient’s healthcare overall.
Role Ambiguity
Investigations into the feasibility and acceptability of allied health interdisciplinary teams, revealed an overwhelmingly positive perception toward interdisciplinary collaboration. All participants believed that interdisciplinary collaboration is both feasible and beneficial to rural health practice. Regarding collaboration with pharmacists, a common theme, however was uncertainty of the pharmacist’s role, with many of the participants never having contacted a pharmacist and being unfamiliar with the pharmacist’s scope, outside that of traditional dispensing and retail duties. Of the 29 participants interviewed, nine stated that they had never had contact with a pharmacist during their career and 20 participants reported that contact with pharmacists, if any, was minimal and instances could be counted “on one hand”.
“It would be great to have pharmacists on board but I’m not sure to what capacity or how that would work.” (Dietician 1)
I have no idea about medications, so I [discuss with] the GP, not the pharmacist. There are probably a lot of things that the pharmacist can do, but we don’t utilise them. (Occupational Therapist 5)
Many of the health professionals interviewed were relatively new to practice, meaning that due to lack of professional exposure, they had no previous opportunities to work with pharmacists. Participants who had been registered for longer tended to have communicated with a pharmacist, however even then collaboration was minimal. The major barrier identified was the concern around available time and capacity of a pharmacist to be integrated into an allied health team.
Due to increased contact with pharmacists, professionals with greater years of experience had more ideas on the potential for collaboration opportunities. Dietician and pharmacist collaborative practice suggested by participants included chronic disease management such as diabetes services. Screening for dysphagia and swallowing-related medication misadventure was mentioned as potential collaboration between speech pathologists and pharmacists, initiating early interventions to prevent serious harms. Falls prevention was identified as a domain where occupational therapist and pharmacist collaboration would be beneficial, as some medications may increase falls risk and impact occupational therapist recommendations. Prophylactic pain management for physiotherapy sessions was identified as a potential area for collaboration between physiotherapists and pharmacists, where interprofessional education plays a vital role.
Particularly around diabetes medication and insulin, learning more about [diabetes medications] and how we can work with pharmacists to understand how side effects may affect someone’s nutrition, medications that cause deficiencies or side effects that increase appetite. (Dietician 1)
Having pharmacists know a little bit more about dysphagia … screening for dysphagia and being able to give some immediate advice – that would be really helpful. (Speech Pathologist 2)
I only have basic knowledge on [medications which increase falls risk]. It would change the way I treat patients because if they are at a higher risk of falls, you really need to work on home safety. (Occupational Therapist 4)
… maybe we could coordinate with a pharmacist to understand dosing when medications are administered at what time and at what times their medication covers their pain the most. Because then we might know when to provide our therapy, we will know if the true pain level is low or if they are just covered by their meds at that time. (Physiotherapist 4)
Discussion
Positive perceptions towards potential collaboration with pharmacists were identified by allied health professionals, however the lack of knowledge of the pharmacists’ role limited clarity of how pharmacist’s skills could be utilized in these collaborations. Allied health professionals believed that the role of the pharmacist is not widely known beyond the traditional supply of medications. Themes guided by the constructs of role theory have informed an opportunity to bridge the roles with interdisciplinary teams, consisting of pharmacists and allied health professionals, to deliver better access and therefore health outcomes in rural and remote communities.
Role identity refers to the expected roles of a profession and the “labels” assigned to them.17 The scope of rural health professionals’ is highlighted as being broad as they are accustomed to dealing with a variety of clinical presentations in their daily practice.20,21 The term “rural generalist” is often used to describe rural and remote healthcare providers, who have the required skills to deliver a broad scope of services.20 This rural generalist role exists in recognition of the scarcity of health professionals and the limited options for referrals, resulting in expanded practice, as a solution to address this demand for services.20 The benefits of expanded healthcare services in rural communities have been mentioned in previous studies as the most effective way to serve the needs of the community.2,3 Role identity in rural Australia may also be linked to high levels of community engagement, with increased health professional involvement in their community, targeting health promotion towards community members who are traditionally disengaged, those with a lower health literacy and vulnerable children. Community engagement is integral for building rapport between patients and professionals, and it has been shown that community involvement leads to better health outcomes for rural populations.22
Role overload explores how the demands of a particular role exceeds an individual’s capacity to perform that role and is particularly pertinent in rural and remote locations.17 On average, health professionals in rural regions have larger workloads due to increased demand for healthcare, higher prevalence of chronic disease and an imbalanced workforce distribution.23 The Australian Institute of Health and Welfare 2017 report outlines the increase in workload, demonstrated as more hours worked per week for those in rural locations compared to metropolitan Australia.22 This study reports high staff turnover due to work overload, which is encouraged by identified burnout as a key barrier to staff retention.18 As a result, tools are being utilized to prevent burnout in an effort to reduce staff turnover and improve patient outcomes through continuity of care.18,19 Although minor staff incentives such as higher salaries and rural funding for continued professional development are in place to attract professionals to rural locations,21,24 it was found that two to three years of practice is the average retention time for staff in the region. Two thirds of participants in this study had been practicing in rural Australia for three years or less, demonstrating the lack of longevity in the rural allied health workforce.
Role sufficiency examines the ability to fulfil role expectation, obligations or goals;17 challenged by the ability for professionals to complete their role with the resources that are available in rural practice. The uneven distribution of the health workforce in rural Australia and the availability of both physical resources and health professionals were identified as a major issue.1,18 Key resources for the provision of healthcare include skilled professionals, funding, availability of technology and physical resources required to provide such services.25 Poor access to physical resources, adequate workforce and professional support were identified as limitations to role sufficiency; these results were supported by findings confirming access to resources as a key facilitator to successful provision of care.1,3,4,18,20,27 The attitudes of health professionals in the study included a willingness to embrace innovation and adaptability to overcome this lack of access and prioritise provision of care.
Role conflict identifies role expectations that may be contradictory or mutually exclusive.17 Allied health professionals in this study were happy to share mutually exclusive services with other professionals and overall have a low level of role conflict, acknowledging that they were at an advantage with the strong professional relationships they are able to maintain in their community. Perception toward role conflict with pharmacists was not assessed, due to a lack of understanding of the scope of pharmacy practice. Studies which examined metropolitan practice reported health professionals’ enthusiasm towards collaboration with pharmacists, so long as there are borders to the jurisdiction of each stakeholder; demonstrating a potential for role conflict.26 However, challenges to providing healthcare in rural communities has resulted in a culture where sharing the work and scope overlap between professionals are common practice.1,3,18,23
Role ambiguity assesses the disagreement of stakeholders towards role expectations, due to a lack of clarity.17 Participants’ perceptions were overwhelmingly positive toward future collaboration with pharmacists, despite most lacking insight into the pharmacists’ scope of practice, which limited suggestions for potential collaborative opportunities. This is confirmed in the literature, where lack of knowledge around scope of practice of a pharmacist has been identified as a key barrier to collaboration.27,28
Allied health professionals in the study who had less professional experience lacked previous interactions with pharmacists and displayed poor understanding of the pharmacist’s role. As a result, they were unable to provide examples of potential interdisciplinary collaboration. In contrast, those health professionals who had more years’ experience in their role had more ideas for how to collaborate with pharmacists. Dieticians proposed that interdisciplinary collaboration with pharmacists would be beneficial in diabetes management. It was suggested by a speech pathologist that by improving interdisciplinary collaboration, pharmacists may be able to screen patients for dysphagia and give on-the-spot advice. With pharmacists performing dysphagia screening in the community setting, this could open a referral pathway to the speech pathologist for thorough assessment and advice; and would allow pharmacists to identify and prevent potentially serious medication misadventure.9,10 The value of having pharmacist input to assess patients who are taking medications which increase falls risk, was highlighted by an occupational therapist to tailor their implementation of home safety measures. This would be significant because there are many medications which increase drowsiness, dizziness, decrease bone mineral density and overall falls risk, especially in elderly patients.29 Working collaboratively with a pharmacist would also be of value to physiotherapist as this would inform the physiotherapy session for example, on assessment of pain levels.
This study has provided insight into the perceptions of allied health professionals towards pharmacist integration with interdisciplinary teams and the potential to bridge the gaps in healthcare in rural Australia. The positive response from participating rural allied health professionals demonstrates their willingness to incorporate a pharmacist into their interdisciplinary team, despite limited understanding of the pharmacists’ role. This justifies the recommendation for increased interprofessional education, where the role of the pharmacist is clarified and bridging opportunities are reviewed.15,27,28 University training would be beneficial as it will equip students with the skills for collaboration to address issues of role ambiguity in the workplace as supported by literature.15 It is recommended to develop a designated pharmacist role outside that of traditional dispensary duties to address the issue of accessibility and capacity of pharmacists for increased input in patient care.14 This role would allow pharmacists to be embedded in primary healthcare practices and community engagement programs. Expanded practice requires redefining traditional pharmacist roles and creating a new interdisciplinary pharmacist identity with the aim to break down the preconceived “shop keeper” stereotype which currently defines pharmacist role identity.27,28
This study has highlighted known deficits in rural healthcare, but also proposes the benefits of interdisciplinary health teams in these rural and remote settings. Implementation of a referral pathway between allied health and pharmacy should be established so that medication-related issues may also be directed towards the pharmacist, reducing some of this burden for the GP. Pharmacists are experts in pharmacotherapy and can alleviate workload pressures of other health professionals especially GPs.30 Further research should seek to explore specific areas where pharmacists can contribute and the resulting benefits to rural interdisciplinary practices of incorporating a pharmacist into interdisciplinary teams.
Limitations of this study include but are not limited to the sample size and geographical distribution of health professionals interviewed; interviews were conducted on a voluntary basis, hence only the participants who responded to the email invitation were included in the study and therefore may have excluded professionals, who were unaware of the study or those who might be less engaged with the topic. Interviews were conducted face-to-face, where the participants could discuss their lived experiences of healthcare practice. However, the fact that slightly more than half of the participants had 5 or less years’ experience in the practice, may have influenced the results. This limited professional experience resulting in fewer interactions with pharmacists, poorer understanding of the pharmacist’s role could result in them being able to make a lesser contribution to the potential for interdisciplinary collaboration between pharmacists and allied health professionals.
Conclusions
Interdisciplinary allied health teams may overcome barriers of access to adequate healthcare in rural Australia, with several areas for allied health and pharmacist collaboration identified. Despite limited interaction and lack of understanding of the pharmacists’ role, it is the positivity of allied health professionals towards working collaboratively with pharmacists that must be harnessed. This gap in rural healthcare highlighted by high workloads and insufficient resourcing, increasing demand for services could be plugged by this initiative. The rural culture of work sharing and positive perceptions toward collaborative practice make rural interdisciplinary teams a viable option to bridge gaps in health care to improve health outcomes for rural and remote communities. Future studies to examine general practitioners’ role in interdisciplinary teams would provide additional valuable evidence to support this area of healthcare delivery. Pharmacists are underutilized in traditional collaborative care models and thus collaboration with pharmacists in rural communities presents a real opportunity to integrate the profession into interdisciplinary care models and improve rural health outcomes. Further work in this area will surface important considerations for the role of pharmacists working within integrated models of care with a focus on interdisciplinary team care for improved patient outcomes, which may also improve rural health workforce shortages.
Acknowledgments
We acknowledge the rural and remote allied health professionals including dieticians/public health nutritionists, speech pathologists, occupational therapists, and physiotherapists who generously gave up their time to participate in this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Weisgrau S. Issues in rural health: access, hospitals, and reform. Health Care Financ Rev. 1995;17(1):1–14.
2. Supper I, Catala O, Lustman M, et al. Interprofessional collaboration in primary health care: a review of facilitators and barriers perceived by involved actors. J Pub Health. 2014;37(4):716–727. doi:10.1093/pubmed/fdu102
3. Saint-Pierre C, Herskovic V, Sepulveda M. Multidisciplinary collaboration in primary care: a systematic review. Fam Pract. 2017;35(2):132–141. doi:10.1093/fampra/cmx085
4. Australian Institute of Health and Welfare 2013. Health workforce 2012. National health workforce series. Canberra: AIHW. Available from: https://www.aihw.gov.au/reports-data/health-welfare-services/workforce/reports.
5. Taylor S, Cairns A, Glass B. Systematic review of expanded practice in rural community pharmacy. JPPR. 2019;49(6):585–600. doi:10.1002/jppr.1619
6. West D, Blevins MA, Brech D, et al. A multidisciplinary approach in a community pharmacy can improve outcomes for diabetes patients. Diabetes Educ. 2003;29(6):962–968. doi:10.1177/014572170302900606
7. Australian Government. Diabetes. Australian Institute of Health and Welfare; 2020. Available from: www.aihw.gov.au/reports-data/health-conditions-disability-deaths/diabetes/overview.
8. King DE, Petrone AB, Alcantara FM, et al. Outcomes in an interdisciplinary diabetes clinic in rural primary care. South Med J. 2019;112(4):205–209. doi:10.14423/SMJ.0000000000000960.
9. Serrano Santos JM, Poland F, Wright D, Longmore T. Medicines administration for residents with dysphagia in care homes: a small scale observational study to improve practice. Int J Pharm. 2016;512(2):416–421. doi:10.1016/j.ijpharm.2016.02.036
10. McFarlane M, Miles A, Atwal P, Parmar P. Interdisciplinary management of dysphagia following stroke. BJNN. 2014;10(1):13–20. doi:10.12968/bjnn.2014.10.1.13
11. Schwartz JK, Smith RO. Integration of Medication Management into Occupational Therapy Practice. AJOT. 2017;71(4):1–7. doi:10.5014/ajot.2017.015032
12. McDermott M, et al. The use of medication for chronic pain in primary care, and the potential for intervention by a practice-based pharmacist. Fam Pract. 2006;23(1):46–52. doi:10.1093/fampra/cmi068
13. Teichert M, Griens F, Buijs E, et al. Effectiveness of interventions by community pharmacists to reduce risk of gastrointestinal side effects in nonselective nonsteroidal anti-inflammatory drug users. Pharmacoepidem DRS. 2014;23(4):382–389. doi:10.1002/pds.3587
14. Conway M. Theoretical Approaches to the Study of Roles.
15. Cairns A, Glass B, Taylor S. Health professional perspectives of expanded practice in rural community pharmacy in Australia. Int J Pharm Pract. 2020;28(5):485. doi:10.1111/ijpp.12648
16. Yong F, Garcia-Cardenas V, Williams K, et al. Factors affecting community pharmacist work: a scoping review and thematic synthesis using role theory. RASP. 2020;16(2):123–141. doi:10.1016/j.sapharm.2019.05.001
17. Cairns A, Glass B, Taylor S. Role theory: a framework to explore health professional perceptions of expanding rural community pharmacists’ role. Pharmacy. 2020;8(3):161. doi:10.3390/pharmacy8030161
18. Wakerman J, Humphreys J, Russell D, et al. Remote health workforce turnover and retention: what are the policy and practice priorities? Hum Resour Health. 2019;17(99). doi:10.1186/s12960-019-0432-y
19. Institute of Medicine Committee on the Health Professionals Summit. Core competencies needed for healthcare professionals. In: Geiner A, Knebel E, editors. Health Professions Education: A Bridge to Quality. Washington (DC): National Academies Press (US); 2003. www.ncbi.nlm.nih.gov/books/NBK221519/.
20. Australian Government National Rural Health Commissioner. National rural generalist taskforce advice to the national rural health commissioner on the development of the national rural generalist pathway. Australian Government; 2018. Available from: www1.health.gov.au/internet/main/publishing.nsf/Content/2922D6D8BBCE122FCA2581D30076D09A/$File/Advice-to-the-National-Rural-Health-Commissioner-on-the-Development-of-the-National-Rural-Generalist-Pathway.pdf.
21. O’Toole K, Schoo A, Hernan A. Why did they leave and what did they tell us? Allied health professionals leaving rural settings. Australian Health Review. 2010;34(1):66–72. doi:10.1071/AH09711
22. Kilpatrick S. Multi-level rural community engagement in health. Aust J Rural Health. 2009;17(1):39–44. doi:10.1111/j.1440-1584.2008.01035.x
23. National Rural Health Alliance. Determinants of health. National Rural Health Alliance; 2017. Available from: www.ruralhealth.org.au/book/determinants-health.
24. Australian Institute of Health and Welfare. Allied health workforce 2012. Australian Institute of Health and Welfare; 2013. Available from: www.aihw.gov.au/reports/workforce/allied-health-workforce-2012/contents/table-of-contents.
25. Street T. Continuity of care for patients with chronic conditions from rural or remote Australia: a systematic review. Aust J Rural Health. 2019;27(3):196–202. doi:10.1111/ajr.12511
26. Wilbur K, Kur J. Multidisciplinary members’ perspectives on a pharmacist joining a rheumatology practice team. CPJ. 2015;148(4):200–2008. doi:10.1177/1715163515587742
27. Pettigrew S, Rieck A. How physician and community pharmacist perceptions of the community pharmacist role in Australia primary care influence the quality of collaborative chronic disease management. Qual Prim Care. 2013;21:105–111.
28. 2019 American Geriatrics Society Beers Criteria® Update Expert Panel. American geriatrics society 2019 updated AGS beers criteria® for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2019;67(4):647–694. doi: 10.1111/jgs.15767
29. Tumosa N, Lach H, Orr L, Barney KF. Intradisciplinary and interdisciplinary processes in gerontological care. In: Barney KF, Emerita C, Perkinson MA, editors. Occupational Therapy with Aging Adults. Amsterdam, Netherlands: Elsevier; 2016:428–443. doi:10.1016/B978-0-323-06776-8.00036-0
30. Dalton K, Byrne S. Role of the pharmacist in reducing healthcare costs: current insights. Integr Pharm Res Pract. 2017;6:37–46. doi:10.2147/IPRP.S108047
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.