Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Breathless and Blue in the Canadian Longitudinal Study on Aging: Incident and Recurrent Depression Among Older Adults with COPD During the COVID-19 Pandemic
Authors Taunque A ![]() , Li G, MacNeil A
, Li G, MacNeil A ![]() , Gulati I
, Gulati I ![]() , Jiang Y, de Groh M, Fuller-Thomson E
, Jiang Y, de Groh M, Fuller-Thomson E
Received 3 May 2023
Accepted for publication 24 July 2023
Published 13 September 2023 Volume 2023:18 Pages 1975—1993
DOI https://doi.org/10.2147/COPD.S417218
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Richard Russell
Aneisha Taunque,1 Grace Li,2 Andie MacNeil,1,3 Ishnaa Gulati,4 Ying Jiang,5 Margaret de Groh,5 Esme Fuller-Thomson1,3,6,7
1Institute for Life Course and Aging, University of Toronto, Toronto, ON, Canada; 2Department of Sociology, University of Victoria, Victoria, BC, Canada; 3Factor-Inwentash Faculty of Social Work, University of Toronto, Toronto, ON, Canada; 4Dalla Lana School of Public Health, University of Toronto, Toronto, ON, Canada; 5Applied Research Division, Center for Surveillance and Applied Research, Public Health Agency of Canada, Ottawa, ON, Canada; 6Department of Family and Community Medicine, Temerty Faculty of Medicine, University of Toronto, Toronto, ON, Canada; 7Bloomberg Faculty of Nursing, University of Toronto, Toronto, ON, Canada
Correspondence: Esme Fuller-Thomson, Institute for Life Course & Aging, Factor-Inwentash Faculty of Social Work, Cross-Appointed to Faculties of Medicine & Nursing, University of Toronto, 246 Bloor St. West, Toronto, ON, M5S 1V4, Canada, Tel +1 416 978-3269, Fax +1 416 978-7072, Email [email protected]
Background and Objectives: The COVID-19 pandemic and related public health measures intensified risk factors for depression and concurrently heightened numerous health-related stressors for individuals with Chronic Obstructive Pulmonary Disease (COPD). Utilizing a comprehensive longitudinal sample of Canadian older adults, this study examined the incidence and recurrence of depression among older adults with COPD, and identified factors that were associated with depression during the pandemic among this population.
Methods: Data came from four phases of the Canadian Longitudinal Study on Aging (CLSA) (n=875 with COPD). The primary outcome of interest was a positive screen for depression based on the CES-D-10, during autumn of 2020. Bivariate and multivariate logistic regression analyses were performed to identify factors that were associated with depression.
Results: Approximately 1 in 6 (17%) respondents with COPD and no lifetime history of depression developed depression for the first time during the early stages of the pandemic. Approximately 1 in 2 (52%) participants with COPD and a history of depression experienced a recurrence of depressive symptoms during this period. Loneliness, functional limitations, and family conflict were associated with a higher risk of both incident and recurrent depression. The risk of incident depression only was higher among those who had difficulty accessing healthcare resources. The risk of recurrent depression only was higher among women, those with a post-secondary education, and those with more adverse childhood experiences.
Conclusion: Screening and interventions aimed at individuals with COPD, both with and without a history of depression, are warranted to potentially mitigate the mental health impacts of the COVID-19 pandemic.
Keywords: depression, older adults, COVID-19, CLSA
Introduction
Since the beginning of the COVID-19 pandemic, there have been more than 6.9 million fatalities worldwide, with more than 1.1 million and 53,000 deaths occurring in the United States and Canada, respectively.1 In response to the pandemic, many governments introduced public health measures, such as physical distancing guidelines and shelter-in-place orders to help minimize the spread of COVID-19.2 Consequences of these measures included reduced social interaction, greater social isolation, and lower levels of physical activity.3–5 When considered in conjunction with unprecedented COVID-19 related stressors, such as economic insecurity, job loss, and increased caregiving responsibilities, it is unsurprising that there has been a marked increase in feelings of loneliness and the prevalence of depression among the general population.6,7
Chronic obstructive pulmonary disease (COPD) is a group of progressive lung diseases characterized by obstructed airflow from the lungs and persistent respiratory symptoms, such as difficulty breathing, wheezing, and mucus production.8 Other symptoms of COPD include functional limitations, poor lower extremity functioning, weak muscle strength, and reduced mobility.9 COPD is a pressing public health concern in Canada and ranks among the leading causes of disability and mortality.10 A recent Canadian study examined data from nine major urban centers and found that approximately 1 in 6 (16.6%) adults aged 40 and over had COPD.10
Although there is no cure for COPD, there are various treatment options to help control symptoms and slow the progression of the disease, such as pulmonary rehabilitation, which combines the use of education and behavioural intention with a central focus on exercise in order to improve muscle function and endurance.11 Regular exercise is extremely important for managing COPD. Many studies have found regular physical activity is associated with improved quality of life, increased respiratory muscle strength, lung function, and exercise capacity, and reduced shortness of breath among respondents with COPD,12–14 particularly among older adults.15 Increasing exercise capacity and reducing shortness of breath are important predictors of survival in COPD.16,17 In contrast, a sedentary lifestyle is associated with poorer long-term outcomes in COPD, including worsening quality of life, increased hospitalization, and mortality.18–21
Exercise is also important for supporting the mental well-being of people with COPD. Older adults with COPD have a higher risk of depression than their peers without COPD.22 Individuals with COPD who have comorbid depression have poorer disease prognosis, reduced exercise tolerance, increased functional limitations, more recurrent acute symptom exacerbations, and are at a greater risk for mortality when compared to their counterparts without depression23–25 particularly those individuals with persistent/recurrent episodes of depression.26 However, a recent systematic review and meta-analysis found that exercise improves depression symptoms among COPD patients,27 emphasizing the importance of promoting exercise-based interventions to support the mental well-being of individuals with COPD.
There is growing concern that the decline in physical activity during COVID-19 lockdowns may have contributed to the deterioration of physical and mental health among older adults with chronic health conditions, such as COPD. Moreover, individuals with COPD are more likely to experience severe symptoms and mortality from COVID-19 compared to their counterparts without COPD, further exacerbating the levels of stress among this population.28 When considering the high comorbidity between COPD and depression prior to the pandemic, combined with the well-established increased risk of adverse health outcomes among COPD patients with comorbid depression, and the unprecedented stressors introduced by the COVID-19 pandemic, it is evident that there is a need for longitudinal research to investigate the relationship between COPD and depression during this period. In addition, it is important to consider the mental health outcomes among people with COPD by differences in their lifetime history of depression, as risk factors may vary between these subpopulations. To address this gap in the literature, the present study uses a large sample from the Canadian Longitudinal Study on Aging (CLSA) to achieve the following objectives: (1) In a sample of participants with COPD and no history of depression at any previous point in their life, identify the prevalence of, and factors associated with, first onset depression (hereafter incident depression) during the COVID-19 pandemic; and (2) In a sample of participants with COPD and a history of depression at some point prior to the pandemic, identify the prevalence of, and factors associated with, the recurrence and/or continuation of depression (hereafter recurrent depression) during the pandemic.
Materials and Methods
Data Source
As has been described elsewhere,29,30 the CLSA is a large national study that recruited Canadian older adults aged 45 to 85 years.31,32 Participation in the CLSA cohort is voluntary and all individuals provided written informed consent.31 The baseline comprehensive cohort recruited 30,097 participants and 27,737 participants completed Follow-up 1. At baseline, respondents were excluded if they lived in one of Canada’s three territories, on an Aboriginal reserve, or in a long-term care facility. In addition, members of the armed forces, people who could not communicate in English or French, and people with severe cognitive impairment at baseline were excluded. In response to the COVID-19 pandemic, CLSA participants were invited to participate in the COVID Spring 2020 and COVID Autumn 2020 waves of data collection. We analyzed data from participants recruited in the Baseline wave (conducted between 2011 and 2015), Follow-up 1 wave (conducted between 2015 and 2018), COVID Spring 2020 wave (conducted between April 15 to May 30, 2020), and COVID Autumn 2020 wave (conducted between September 29 to December 29, 2020) of the comprehensive cohort of the CLSA. The detailed CLSA methodology are described elsewhere.31,32
All Canadian Longitudinal Study on Aging (CLSA) waves of data collection have been approved by research ethics boards at all collaborating Canadian institutions. The CLSA was conducted in accordance with the 1964 Helsinki declaration and its later amendments, and with the ethical standards of each institutional research committee. The current study was approved by the University of Toronto’s Research Ethics Board (Protocol #41167; approved June 4, 2021).
Sample
Our analysis was limited to CLSA respondents with chronic obstructive pulmonary disease (COPD) during the Baseline or Follow-up 1 waves prior to the COVID-19 pandemic (n = 875). Self-reported COPD was defined by the question, “Has a doctor told you that you have/had any of the following: emphysema, chronic bronchitis, chronic obstructive pulmonary disease (COPD), or chronic changes in lungs due to smoking?” (1 = yes; 0 = no). Among those with COPD, 506 respondents had no pre-pandemic history of depression and 369 had a history of depression. Respondents who did not participate in one or more of the four questionnaires or who were missing data on any of the measures utilized in the current study were excluded from the analyses.
Measures
The outcome of interest, depression, was measured using the Center for Epidemiologic Studies Short Scale of Depression (CES-D-10) during the Autumn 2020 questionnaire. This screening tool contains 10 items on depressive symptoms such as feelings of depression, loneliness, hope for the future, and restless sleep in the past 7 days. The total score ranges from 0 to 30, with higher scores indicating higher severity. A score of 10 or more (CES-D-10 total score ≥10) was used to identify those with depression. The CES-D-10 is a valid and reliable measure for screening depressive symptoms in older adults,33 and the cutoff point of 10 is widely used in this population.34
To identify a lifetime history of depression, four measures were used. The CES-D-10 scores from the Baseline and Follow-up 1 waves were used. Moreover, at Baseline and Follow-up 1, respondents were also asked: “Did your doctor ever tell you that that you had clinical depression?” Respondents were categorized as not having pre-pandemic depression if they had scores <10 on the CES-D-10 in both the Baseline and Follow-up 1 wave of data collection, and they reported at both waves that they had never been told by a doctor that they were clinically depressed. If at least one of the four outcomes above indicated depression at Baseline or Follow-up 1, the respondent was classified as having pre-pandemic depression.
We included the following sociodemographic variables: age at the COVID Autumn 2020 wave, sex (female; male), marital status (married/common-law; separated/divorced/widowed), immigrant status (yes; no), visible minority status (non-white; white), education (less than secondary school; some post-secondary school; post-secondary degree/diploma), household income (less than $50,000; $50,000 - $99,999; $100,000 or more; missing), home ownership (rent; own with mortgage; own without mortgage), total savings (less than $50,000; $50,000 - $99,999, $100,000 or more, missing), whether income satisfies needs (0 = with some difficulty / not very well / totally inadequate; 1 = very well / adequately).
Health-related variables included Body Mass Index (BMI), chronic pain, and multimorbidity. BMI was divided into three categories: underweight or normal weight (BMI < 25), overweight (BMI = 25.0–29.99), obese (BMI ≥30.0). Chronic pain was measured by the question: “Are you usually free of pain or discomfort?” (yes; no). Multimorbidity was defined as having multiple chronic conditions (0; 1; 2; 3 or more; missing), including (1) Diabetes, (2) Heart disease (3) Peripheral vascular disease or poor circulation in the extremities, (4) Dementia or Alzheimer’s disease, (5) Multiple sclerosis, (6) Epilepsy, (7) Migraine headache, (8) Intestinal or gastric ulcers, (9) Intestinal disorders, (10) Asthma, (11) Stroke or CVA (cerebrovascular accident), (12) Glaucoma, (13) Kidney disease, (14) Macular degeneration, (15) Mini-stroke or TIA (transient ischemic attack), and (16) Parkinson’s disease, and (17) Cancer.
Adverse childhood experiences were measured by childhood physical abuse, childhood sexual abuse, childhood exposure to intimate partner violence, and being neglected. Childhood physical abuse was present if respondents reported being kicked, bit or punched, or chocked, burned or physically attacked in some other way one or more times. Childhood sexual abuse was present if respondents reported that an adult forced them or attempted to force them into any unwanted sexual activity by threatening them, holding them down, or hurting them in some way one or more times. Childhood exposure to intimate partner violence was present if respondents reported seeing or hearing parents, step-parents or guardians hitting each other more than 10 times. Respondents were categorized as neglected during childhood if they reported their parents or guardians had ever not taken care of their basic needs such as keeping them clean or providing adequate food or clothing one.
Two measures of religiosity were used. The first measure was based on the question, “In the past 12 months, how often did you participate in church or religious activities, such as services, committees, or choirs?” The second measure was based on the question, “In the past 12 months, how often did you engage in religious or spiritual activities (including prayer, meditation) taking place at home or in any other location?” For each measure, respondents were coded as often (=1) if they participated in these activities at least once a month, and rare (=0) otherwise.
At the beginning of the COVID-19 pandemic, respondents were asked in the COVID Spring 2020 questionnaire if they had left home in the past month (yes; no). Respondents were also asked if they felt lonely (rarely or never/some of the time [0–2 days per week] vs occasionally/all of the time [3–7 days per week]). Respondents’ type of dwelling was categorized as house, apartment, and other. Respondents were also asked if they lived alone at the start of the COVID-19 pandemic.
The functional limitations scale consisted of three questions: “Do you have any difficulty standing up after sitting in a chair”, “Do you have any difficulty walking alone up and down a flight of stairs?”, and “Do you have any difficulty walking 2 to 3 neighborhood blocks?” (0 = all three questions answered no; 1 = otherwise).
Stressors associated with the COVID-19 were measured at the COVID Autumn 2020 wave, and they were categorized into five composite indicators. Experiences were categorized as yes if participants responded yes to at least one experience in a given category and were categorized as no if they responded no to all questions in that category. Health-related questions included: “You were ill”, “People close to you were ill”, and/or “Death of a person close to you”. Questions related to difficulties in accessing resources included: “Loss of income” and/or “Unable to access necessary supplies or food”. Questions related to family conflict included “Increased verbal or physical conflict” and/or “Breakdown of family/marital relationship”. Problems related to other family issues included “Separation from family”, “Increased time caregiving”, and/or “Unable to care for people who require assistance due to health condition or limitation”. Problems related to health care included “Unable to access to my usual health care”. Problems related to medication included “Unable to get my usual prescription drugs and treatments”.
Statistical Analyses
The analyses were conducted in several steps. First, descriptive statistics were presented in the form of frequencies and percentages for the two main COPD groups – those with or without pre-pandemic depression. We calculated the prevalence of incident and recurrent depression among these two COPD groups. Among respondents with COPD, but without a pre-pandemic history of depression and those with a pre-pandemic history of depression, we compared the distribution of independent variables among those who did not develop depression and those who did. Statistical differences at the bivariate level were tested using Chi-square tests and independent t-tests. Second, multivariate logistic regression analyses were used to examine the association between risk factors and depression during the COVID-19 pandemic. For all predictors, we reported adjusted odds ratios and 95% confidence intervals (CIs). We evaluated the goodness-of-fit of logistic models using the Nagelkerke R square and assessed multicollinearity through the variance inflation factor (VIF). All analyses were conducted using R version 4.1.3. All hypothesis tests were two-sided and p-values less than 0.05 were considered statistically significant.
Results
Table 1 presents the sample characteristics of participants with COPD characterized by pre-pandemic depression status. The results show respondents with a history of pre-pandemic depression were more likely than those without a depression history to be female, separated/divorced/widowed or single, to have a household income of less than $50,000, to have total savings of less than $50,000, to report insufficient income to meet needs, to be obese, to have chronic pain, to have more than three chronic health conditions, to have felt occasionally/always lonely during the first months of the pandemic, to live in an apartment, to have functional limitations, and to experience COVID-related stressors.
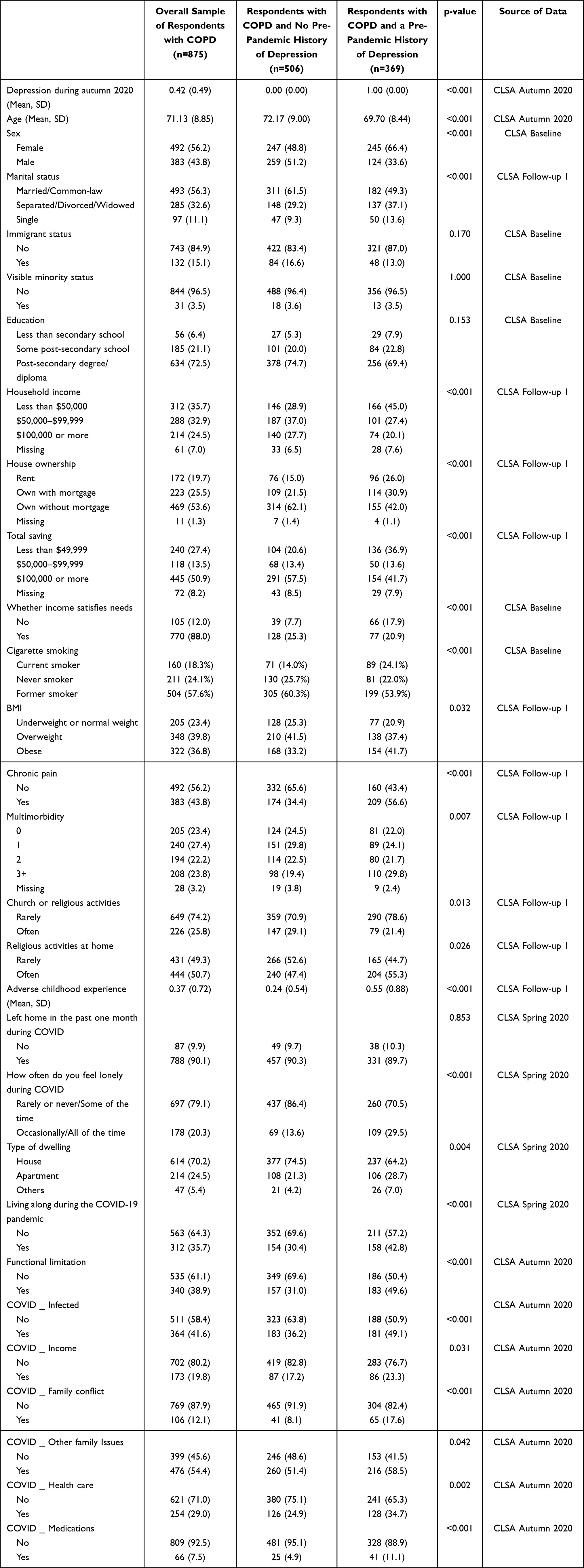 |
Table 1 Characteristics of CLSA Respondents with COPD (n=875) by Pre-Pandemic History of Depression |
Table 2 shows the characteristics of individuals with COPD broken down by pre-COVID depression status and depression status during Autumn 2020. Among COPD respondents without a pre-pandemic history of depression, 17% developed depression for the first time during the pandemic. Among those with a history of pre-pandemic depression, 52% were depression during the Autumn of 2020.
When incident and recurrent depression rates are compared to these rates during a non-COVID period (ie, between CLSA Baseline and Follow-up 1), the depression rates are higher during the COVID period (Analyses not shown). Specifically, for those with COPD and no history of depression, incident depression between the Baseline and Follow-up 1 wave was 6.5% compared to an incident depression rate between the follow-up 1 wave and Autumn 2020 of 17.0%. For recurrent depression among those with COPD, 44.4% of those with depression at baseline also had depression at the follow-up one wave, whereas 52.3% those with a history of depression pre-pandemic were also depressed during the COVID period. This sensitivity analysis suggests that there were higher incident and recurrent depression between the Follow-up 1 wave and Autumn 2020 than between the Baseline and Follow-up 1 wave.
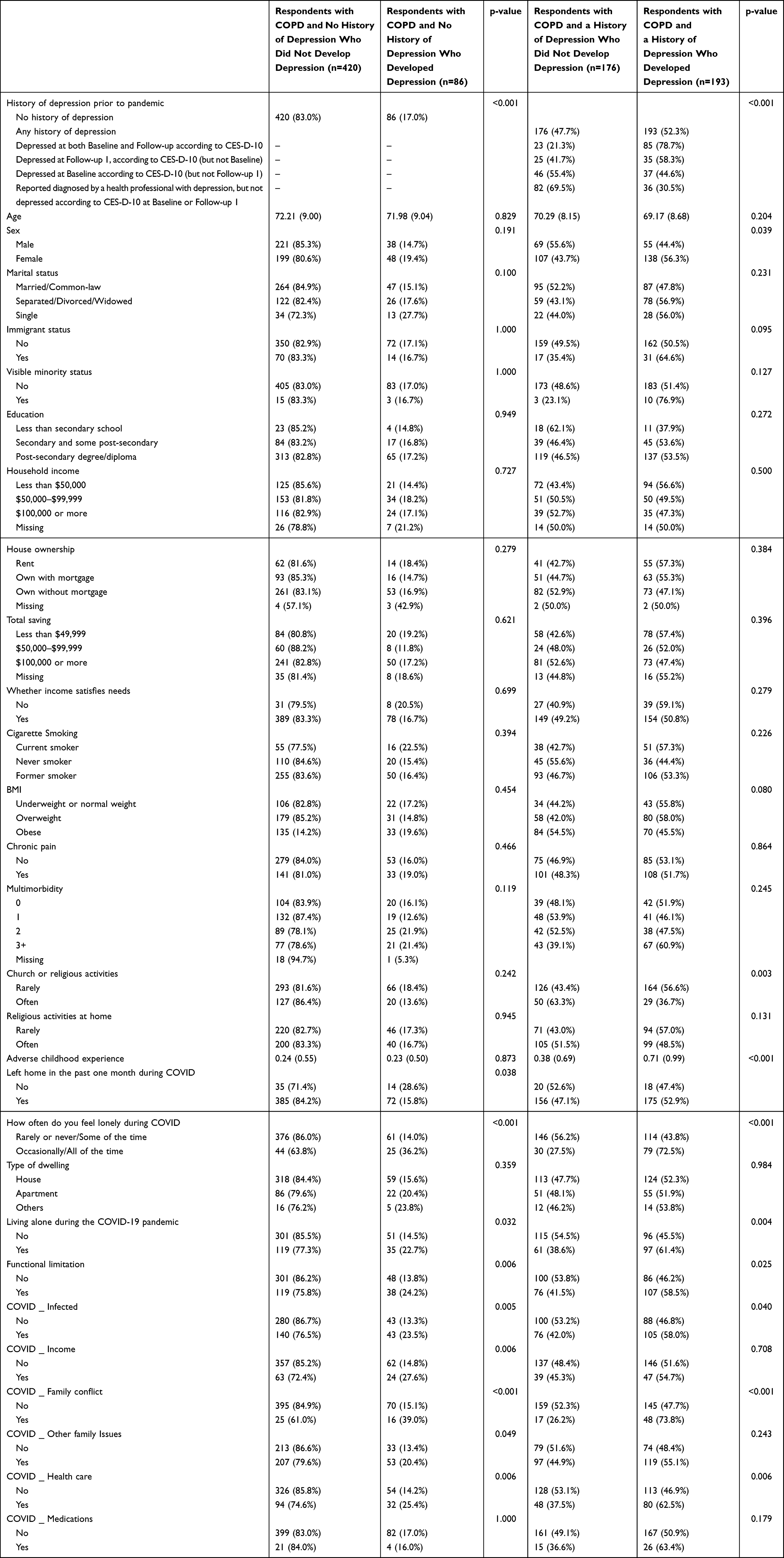 |
Table 2 Profile of CLSA Participants with COPD According to their Pre-Pandemic History of Depression and their Depression Status in Autumn 2020. |
When the recency and duration of depression was taken into account, there was a clear dose response during the COVID-19 pandemic: Those who had CES-D-10 scores indicative of depression at both Baseline and Follow-up 1 were most likely to be depressed during the pandemic (78.7%), followed by those whose CES-D-10 scores indicated depression at Follow-up 1 but not Baseline (58.3%), and those with CES-D-10 scores indicating depression at Baseline but not Follow-up 1 (44.6%). Among those who reported they had been diagnosed with depression by a health professional at some point in their life, but who had not been classified as depressed according to their CES-D-10 score at either Baseline or Follow-up 1, the percent who developed depression (30.5%) was much closer to their peers with no history of depression (17.0%).
Table 3 reports the association of depression status at the COVID Autumn 2020 wave and covariates among respondents with COPD with no pre-pandemic history of depression. Those with a household income between $50,000-$99,999 were more than twice as likely to report depression compared to those with a household income below $50,000, after adjusting for covariates (OR = 2.44, 95% CI [1.10; 5.41], p = 0.028). The same pattern was present for those with a household income greater than $99,999 when compared to those with a household income of less than $50,000 (OR = 2.65, 95% CI [1.03, 6.82], p=0.044). People who felt lonely occasionally or all of the time during the early months of the pandemic were at significantly higher risk for depression than those who rarely or never felt lonely during that period (OR = 3.38, 95% CI [1.70; 6.72], p <0.001). The odds of incident depression were higher among those who had functional limitations (OR = 2.24, 95% CI [1.22; 4.10], p=0.009), increased family conflict during the pandemic (OR = 2.68, 95% CI [1.17; 6.14], p =0.019), and had difficulties accessing healthcare during the pandemic (OR = 2.14, 95% CI [1.17; 3.89], p=0.013). The Nagelkerke R square for this model was 0.246.
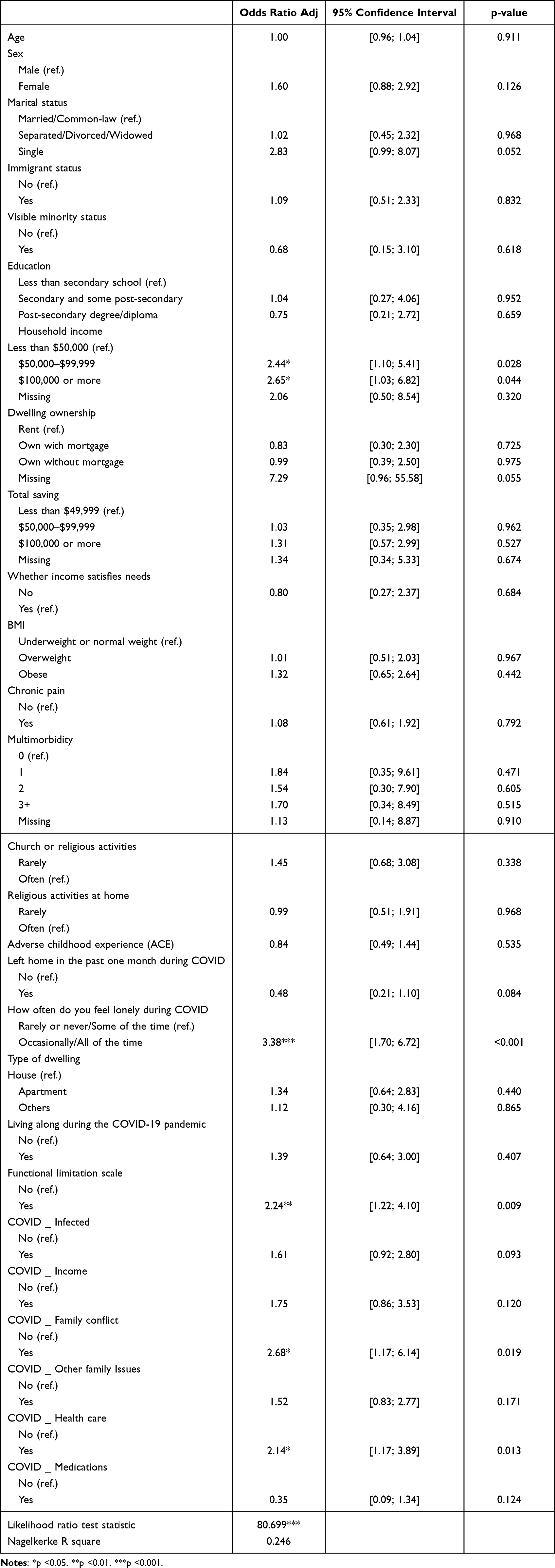 |
Table 3 Logistic Regression Results for Incident Depression During Autumn 2020 Among Respondents with COPD and No Pre-Pandemic History of Depression (n=506) |
Table 4 shows the association among covariates and depression status at the COVID Autumn 2020 wave among COPD respondents with a pre-pandemic history of depression. Women had a higher risk of recurrent depressive symptoms than men (OR = 1.88, 95% CI [1.06; 3.34], p = 0.030). Those who had post-secondary degree or diploma were more likely to be depressed than their counterparts with less than secondary school completion (OR = 3.00, 95% CI [1.12; 8.05], p = 0.029). Older respondents with higher adverse childhood experiences scores were more likely to report depression during the pandemic (OR = 1.44, 95% CI [1.03; 2.02], p = 0.033). Respondents who often felt lonely during the first few months of the COVID-19 pandemic were significantly more likely to have recurrent depressive symptoms (OR = 3.26, 95% CI [1.83; 5.83], p =<0.001). Older adults with functional limitations had a higher risk for depressive symptoms compared to their counterparts without such limitations (OR = 1.93, 95% CI [1.12; 3.33], p =0.018). Respondents who had increased family conflict during the pandemic had 2.52 times higher odds of depression during the pandemic (95% CI [1.23; 5.19], p=0.012). The Nagelkerke R square for this model was 0.321.
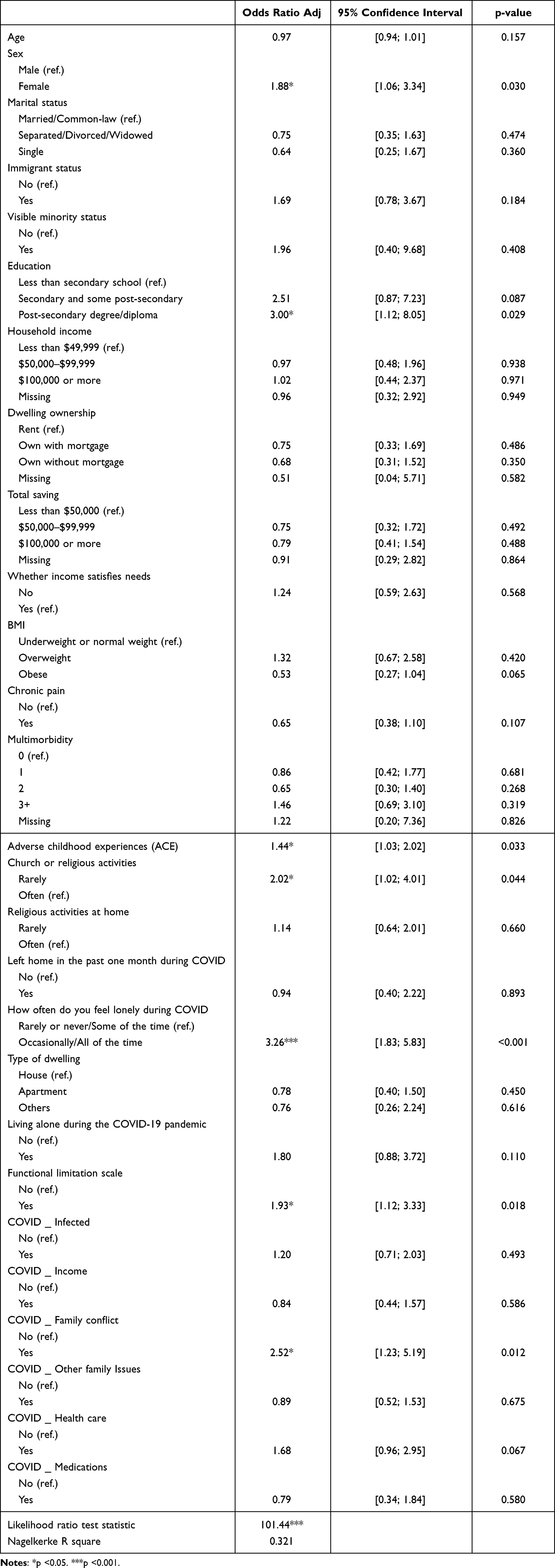 |
Table 4 Logistic Regression Results for Depression During Autumn 2020 Among Respondents with COPD and a Pre-Pandemic History of Depression (n=369) |
Discussion
This study examined the incidence and recurrence of depression during the COVID-19 pandemic among older adults with COPD using a large longitudinal study of Canadian older adults. Our findings indicate that 17% of older adults with COPD who had no pre-pandemic history of depression experienced incident depression during the pandemic. Among older adults with COPD who had a history of depression at some point in their lives, approximately 52% experienced a recurrence or persistence of depression during the pandemic. The findings of this study support emerging literature that has identified an increase in depression among older adults during the pandemic, and also highlights the vulnerability to depression among older adults with COPD who faced unprecedented health-related stressors during the pandemic.35–37 Our analyses identified several factors that were associated with a heightened risk of incident and recurrent depression in individuals with COPD.
Surprisingly, greater household income was not a protective factor against incident depression among older adults with COPD. In the logistic regression analysis, respondents with a household income greater than $50,000 were more likely to develop depression than those with an income less than $50,000. This contrasts with research conducted prior to the pandemic that has found low household income to be associated with an increased risk for developing depression.38 We hypothesize two possible explanations for our findings. First, the Canadian Emergency Response Benefit (CERB) provided many Canadians who lost employment during the COVID-19 pandemic with an income of $2000 per month. For many low-income individuals, this may have actually increased their monthly income, somewhat attenuating stress among this population during this stage of the pandemic. Second, the measure of incident depression focused solely on respondents with no lifetime history of depression. It is possible that older adults with COPD and low socioeconomic status who were free from depression before the pandemic had already developed coping mechanisms and had greater resilience to adversities in their daily life. In contrast, for individuals with higher household incomes, the pandemic may have introduced unfamiliar stressors, increasing first-onset depression among this subgroup of older adults.
Older adults with COPD who encountered challenges with accessing healthcare during the pandemic were found to be more likely to experience incident depression than those who did not report these difficulties. The COVID-19 pandemic greatly disrupted access to healthcare services, with particular challenges for COPD patients. For example, access to pulmonary rehabilitation, which has been found to alleviate depressive symptoms in older adults with COPD,27 was severely disrupted for many COPD patients during the pandemic.39 There were also significant reductions in COPD-related hospital admissions reported during the COVID-19 pandemic, which were likely impacted by a reluctance or inability to access medical care during the COVID-19 pandemic.40 As hospitals were overwhelmed with COVID-19 patients, many older adults with COPD also experienced appointment cancellations and/or shifts to telemedicine.41,42
Telemedicine, including virtual pulmonary rehabilitation, has been shown to have a positive impact on health outcomes on COPD patients, such as increased exercise capacity, reduced symptom exacerbation, and lower levels of depression and anxiety.43,44 Increasing access to telehealth pulmonary rehabilitation has been identified as a major priority to improve accessibility in care for people with COPD, even prior to the pandemic.45 However, it is important for clinicians to consider that there are still substantial barriers to using telemedicine for many people with COPD, such as older adults who may be less comfortable or familiar with using some forms of technology, those with sensory or cognitive impairments, those with low socioeconomic status who may have limited access to necessary equipment or reliable internet, and those with low English proficiency.46,47 As telemedicine continues to grow, it is important to improve its accessibility and reduce disparities in care for those who may struggle with this shift, which may include continuing in-person services for those individuals where telemedicine is not appropriate or accessible. Furthermore, future research should continue to examine ways to increase the accessibility of telemedicine for individuals who may need additional support, such as those with limited experience with technology.
Individuals with COPD who had functional limitations were found to be at a higher risk of incident and recurrent depression. This increased risk may partly stem from decreased physical activity levels. Significant variations in health attitudes have been observed among older adults diagnosed with COPD, and their participation in physical activity is notably low, particularly among those with higher levels of functional limitations.48 As previously established in the literature, regular exercise has been shown to help protect against the development of depressive symptoms in older adults with COPD.49 Hence, the inability to exercise due to functional limitations may contribute to the heightened likelihood of depression. This may contribute to a harmful cycle for COPD patients, in which individuals are hesitant to exercise due to their functional limitations, which in turn worsens their functional status and also negatively impacts their mental health. Clinicians supporting their patients with COPD should consider exercise interventions that are tailored to each individual’s capacity, and may also consider using psychoeducation to educate COPD patients with functional limitations on the benefits of appropriate physical activity.
We also found that that women were more likely to experience recurrent depression during the COVID-19 pandemic than men. This aligns with prior research that has found a higher prevalence of depression among women with COPD than men with COPD,26,50 as well as among women during the pandemic in comparison to men.51,52 One factor that may have contributed to this observed trend is the exacerbation of gendered roles during the pandemic and periods of lockdown, specifically related to caregiving and household labor.52,53
Limitations
The present study has some limitations to consider. First, the CES-D-10 is a self-report measure of depression. Although it is a well-validated and frequently utilized measure for screening depressive symptoms among older adults,33,34 future research should consider the assessment of depression by clinical interview. Second, the current study relied on a self-report measure of COPD. Although self-reported health measures are useful in large-scale epidemiological studies where clinical assessments may not be feasible for all participants, self-reported COPD may not be considered a definitive medical diagnosis. Additionally, we only have information on this self-report measure of COPD during the Follow-up 1 questionnaire, which means that any individuals who developed COPD after this point would be misclassified as without COPD. However, such an error would bias our findings towards the null. Third, the current study did not have information regarding COPD severity, which, in previous studies has been established as a predictor of comorbid depression.23 Fourth, we also did not have any information on treatments being utilized by the participants, such as oxygen, steroids, or other medications for COPD, which may influence depression status. Furthermore, we did not have information on depression treatments that may be utilized by the participants, such as medication or psychotherapy, which has a major impact on trajectories of depression and long-term outcomes among individuals with depression. Fifth, this study did not include older adults residing in long-term care facilities at baseline. This subpopulation of older adults was particularly vulnerable to extended periods of lockdown, and thus, their exclusion may result in a sampling bias and underrepresentation of depression among older adults with COPD. Lastly, this study only included individuals who were fluent in one of Canada’s official languages (ie, English or French).
Conclusions
Despite these limitations, this study provides novel information using a longitudinal sample of Canadian older adults with COPD to better understand the effects of the COVID-19 pandemic on the mental health of this population. The findings indicate a heightened risk for both incident and recurrent depression among older adults with COPD during the pandemic. Healthcare professionals should be aware of the mental health impacts of COVID-19 on individuals with COPD and continue to screen their COPD patients for depression to support their mental well-being.
Acknowledgments
This research was made possible using the data/biospecimens collected by the Canadian Longitudinal Study on Aging (CLSA). Funding for the Canadian Longitudinal Study on Aging (CLSA) is provided by the Government of Canada through the Canadian Institutes of Health Research (CIHR) under grant reference: LSA 94473 and the Canada Foundation for Innovation, as well as the following provinces, Newfoundland, Nova Scotia, Quebec, Ontario, Manitoba, Alberta, and British Columbia. This research has been conducted using the CLSA Baseline Comprehensive Dataset version 6.0, Follow-up 1 Comprehensive Dataset version 3.0, and COVID-19 Questionnaire Study Dataset version 1.0 under Application ID 2104024. The CLSA is led by Drs. Parminder Raina, Christina Wolfson and Susan Kirkland. The opinions expressed in this manuscript are the author’s own and do not reflect the views of the Canadian Longitudinal Study on Aging. The authors would like to thank James Cognata for his assistance with preparation of the tables. Andie MacNeil received funding from the Public Health Agency of Canada to support this research activity. This research was supported, in part, by the Canadian Institutes of Health Research (CIHR) grant #172862 (PI: EFT). We gratefully acknowledge the support of the Canadian Frailty Network. Data are available from the Canadian Longitudinal Study on Aging (www.clsa-elcv.ca) for researchers who meet the criteria for access to de-identified CLSA data.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. WHO coronavirus disease (COVID-19) dashboard. Available from: https://covid19.who.int/.
2. Canadian Public Health Association. Review of Canada’s initial response to the COVID-19 pandemic. Available from: https://www.cpha.ca/review-canadas-initial-response-covid-19-pandemic.
3. Ammar A, Brach M, Trabelsi K, et al. Effects of COVID-19 home confinement on eating behaviour and physical activity: results of the ECLB-COVID19 International Online Survey. Nutrients. 2020;12(6):1583. doi:10.3390/nu12061583
4. He M, Xian Y, Lv X, He J, Ren Y. Changes in body weight, physical activity, and lifestyle during the semi-lockdown period after the outbreak of COVID-19 in China: an online survey. Disaster Med Public Health Prep. 2021;15(2):e23–e28. doi:10.1017/dmp.2020.237
5. Yamada K, Yamaguchi S, Sato K, Fuji T, Ohe T. The COVID-19 outbreak limits physical activities and increases sedentary behavior: a possible secondary public health crisis for the elderly. J Orthop Sci. 2020;25(6):1093–1094. doi:10.1016/j.jos.2020.08.004
6. Dozois DJA. Anxiety and depression in Canada during the COVID-19 pandemic: a national survey. Can Psychol. 2021;62(1):136–142. doi:10.1037/cap0000251
7. Ettman CK, Abdalla SM, Cohen GH, Sampson L, Vivier PM, Galea S. Prevalence of depression symptoms in US adults before and during the COVID-19 pandemic. JAMA Netw Open. 2020;3(9):e2019686. doi:10.1001/jamanetworkopen.2020.19686
8. Devine JF. Chronic obstructive pulmonary disease: an overview. Am Health Drug Benefits. 2008;1(7):34–42.
9. Eisner MD, Blanc PD, Yelin EH, et al. COPD as a systemic disease: impact on physical functional limitations. Am J Med. 2008;121(9):789–796. doi:10.1016/j.amjmed.2008.04.030
10. Leung C, Bourbeau J, Sin DD, et al. The prevalence of Chronic Obstructive Pulmonary Disease (COPD) and the heterogeneity of risk factors in the Canadian population: results from the Canadian Obstructive Lung Disease (COLD) Study. Int J Chron Obstruct Pulmon Dis. 2021;16:305–320. doi:10.2147/COPD.S285338
11. Ries AL, Bauldoff GS, Carlin BW, et al. Pulmonary rehabilitation: joint ACCP/AACVPR evidence-based clinical practice guidelines. Chest. 2007;131(5):4S–42S. doi:10.1378/chest.06-2418
12. Neves LF, Reis MH, Plentz RDM, Matte DL, Coronel CC, Sbruzzi G. Expiratory and expiratory plus inspiratory muscle training improves respiratory muscle strength in subjects with COPD: systematic review. Respir Care. 2014;59(9):1381–1388. doi:10.4187/respcare.02793
13. Salcedo PA, Lindheimer JB, Klein-Adams J, Sotolongo AM, Falvo MJ. Effects of exercise training on pulmonary function in adults with chronic lung disease: a meta-analysis of randomized controlled trials. Arch Phys Med Rehabil. 2018;99(12):2561–2569.e7. doi:10.1016/j.apmr.2018.03.014
14. Wadell K, Webb KA, Preston ME, et al. Impact of pulmonary rehabilitation on the major dimensions of dyspnea in COPD. COPD. 2013;10(4):425–435. doi:10.3109/15412555.2012.758696
15. Li W, Pu Y, Meng A, Zhi X, Xu G. Effectiveness of pulmonary rehabilitation in elderly patients with COPD: a systematic review and meta‐analysis of randomized controlled trials. Int J Nurs Pract. 2019;25(5):e12745. doi:10.1111/ijn.12745
16. Nishimura K, Izumi T, Tsukino M, Oga T. Dyspnea is a better predictor of 5-year survival than airway obstruction in patients with COPD. Chest. 2002;121(5):1434–1440. doi:10.1378/chest.121.5.1434
17. Pinto-Plata V, Cote C, Cabral H, Taylor J, Celli BR. The 6-min walk distance: change over time and value as a predictor of survival in severe COPD. Eur Respir J. 2004;23(1):28–33. doi:10.1183/09031936.03.00034603
18. Esteban C, Quintana JM, Aburto M, et al. Impact of changes in physical activity on health-related quality of life among patients with COPD. Eur Respir J. 2010;36(2):292–300. doi:10.1183/09031936.00021409
19. Esteban C, Arostegui I, Aburto M, et al. Influence of changes in physical activity on frequency of hospitalization in chronic obstructive pulmonary disease. Respirology. 2014;19(3):330–338. doi:10.1111/resp.12239
20. Garcia-Aymerich J, Lange P, Benet M, Schnohr P, Antó JM. Regular physical activity reduces hospital admission and mortality in chronic obstructive pulmonary disease: a population based cohort study. Thorax. 2006;61(9):772–778. doi:10.1136/thx.2006.060145
21. Vaes AW, Garcia-Aymerich J, Marott JL, et al. Changes in physical activity and all-cause mortality in COPD. Eur Respir J. 2014;44(5):1199–1209. doi:10.1183/09031936.00023214
22. Schneider C, Jick SS, Bothner U, Meier CR. COPD and the risk of depression. Chest. 2010;137(2):341–347. doi:10.1378/chest.09-0614
23. Atlantis E, Fahey P, Cochrane B, Smith S. Bidirectional associations between clinically relevant depression or anxiety and COPD. Chest. 2013;144(3):766–777. doi:10.1378/chest.12-1911
24. Keating A, Lee A, Holland AE. What prevents people with chronic obstructive pulmonary disease from attending pulmonary rehabilitation? A systematic review. Chron Resp Dis. 2011;8(2):89–99. doi:10.1177/1479972310393756
25. Yohannes AM, Alexopoulos GS. Depression and anxiety in patients with COPD. Eur Respir Rev. 2014;23(133):345–349. doi:10.1183/09059180.00007813
26. Yohannes AM, Müllerová H, Hanania NA, et al. Long-term course of depression trajectories in patients with COPD: a 3-year follow-up analysis of the evaluation of COPD longitudinally to identify predictive surrogate endpoints cohort. Chest. 2016;149(4):916–926. doi:10.1016/j.chest.2015.10.081
27. Gordon CS, Waller JW, Cook RM, Cavalera SL, Lim WT, Osadnik CR. Effect of pulmonary rehabilitation on symptoms of anxiety and depression in COPD: a systematic review and meta-analysis. Chest. 2019;156(1):80–91. doi:10.1016/j.chest.2019.04.009
28. Gerayeli FV, Milne S, Cheung C, et al. COPD and the risk of poor outcomes in COVID-19: a systematic review and meta-analysis. EClinicalMedicine. 2021;33:100789. doi:10.1016/j.eclinm.2021.100789
29. MacNeil A, Li G, Jiang Y, de Groh M, Fuller-Thomson E. Incident and recurrent depression among older adults with asthma during the COVID-19 pandemic: findings from the Canadian Longitudinal Study on Aging. Respir Med. 2023;213:107003. doi:10.1016/j.rmed.2022.107003
30. MacNeil A, Birk S, Villeneuve PJ, Jiang Y, de Groh M, Fuller-Thomson E. Incident and recurrent depression among adults aged 50 years and older during the COVID-19 pandemic: a longitudinal analysis of the Canadian Longitudinal Study on aging. Int J Environ Res Public Health. 2022;19(22):15032. doi:10.3390/ijerph192215032
31. Raina PS, Wolfson C, Kirkland SA, et al. The Canadian longitudinal study on aging (CLSA). Can J Aging. 2009;28(3):221–229. doi:10.1017/S0714980809990055
32. Raina P, Wolfson C, Kirkland S, et al. Cohort profile: the Canadian Longitudinal Study on Aging (CLSA). Int J Epidemiol. 2019;48(6):1752–1753j. doi:10.1093/ije/dyz173
33. Mohebbi M, Nguyen V, McNeil JJ, et al. Psychometric properties of a short form of the Center for Epidemiologic Studies Depression (CES-D-10) scale for screening depressive symptoms in healthy community dwelling older adults. Gen Hosp Psychiatry. 2021;51:118–125. doi:10.1016/j.genhosppsych.2017.08.002
34. Andresen EM, Malmgren JA, Carter WB, Patrick DL. Screening for depression in well older adults: evaluation of a short form of the CES-D. Am J Prev Med. 1994;10(2):77–84.
35. Tyler CM, McKee GB, Alzueta E, et al. A study of older adults’ mental health across 33 countries during the COVID-19 pandemic. Int J Environ Health Res. 2021;18(10):5090. doi:10.3390/ijerph18105090
36. McAuley H, Hadley K, Elneima O, et al. COPD in the time of COVID-19: an analysis of acute exacerbations and reported behavioural changes in patients with COPD. ERJ Open Res. 2021;7(1):00718–2020. doi:10.1183/23120541.00718-2020
37. Krendl AC, Perry BL, Isaacowitz DM. The impact of sheltering in place during the COVID-19 pandemic on older adults’ social and mental well-being. J Gerontol. 2021;76(2):e53–e58. doi:10.1093/geronb/gbaa110
38. Sareen J, Afifi TO, McMillan KA, Asmundson GJG. Relationship between household income and mental disorders: findings from a population-based longitudinal study. Arch Gen Psychiatry. 2011;68(4):419–427. doi:10.1001/archgenpsychiatry.2011.15
39. Tsutsui M, Gerayeli F, Sin DD. Pulmonary rehabilitation in a post-COVID-19 world: telerehabilitation as a new standard in patients with COPD. Int J Chron Obstruct Pulmon Dis. 2021;16:379–391. doi:10.2147/COPD.S263031
40. Berghaus TM, Karschnia P, Haberl S, Schwaiblmair M. Disproportionate decline in admissions for exacerbated COPD during the COVID-19 pandemic. Respir Med. 2022;191:106120. doi:10.1016/j.rmed.2020.106120
41. Pleguezuelos E, Del Carmen A, Moreno E, et al. The experience of COPD patients in lockdown due to the COVID-19 pandemic. Int J Chron Obstruct Pulmon Dis. 2020;15:2621–2627. doi:10.2147/COPD.S268421
42. Rutkowski S. Management challenges in chronic obstructive pulmonary disease in the COVID-19 pandemic: telehealth and virtual reality. J Clin Med. 2021;10(6):1261. doi:10.3390/jcm10061261
43. Marquis N, Larivée P, Saey D, Dubois M, Tousignant M. In-home pulmonary telerehabilitation for patients with chronic obstructive pulmonary disease: a pre-experimental study on effectiveness, satisfaction, and adherence. Telemed J E Health. 2015;21(11):87–879. doi:10.1089/tmj.2014.0198
44. Barbosa MT, Sousa CS, Morais-Almeida M, Simões M, Mendes P. Telemedicine in COPD: an overview by topics. COPD. 2020;17(5):601–617. doi:10.1080/15412555.2020.1815182
45. Selzler AM, Wald J, Sedeno M, et al. Telehealth pulmonary rehabilitation: a review of the literature and an example of a nationwide initiative to improve the accessibility of pulmonary rehabilitation. Chron Respir Dis. 2018;15(1):41–47. doi:10.1177/1479972317724570
46. Paige SR, Bunnell BE, Bylund CL. Disparities in patient-centered communication via telemedicine. Telemed J E Health. 2022;28(2):212–218. doi:10.1089/tmj.2021.0001
47. Wang Y, Do DP, Wilson FA. Immigrants’ use of eHealth services in the United States, National Health Interview Survey, 2011–2015. Public Health Rep. 2018;133(6):677–684. doi:10.1177/0033354918795888
48. Chen M, Chen L, Chen YT, Gardenhire DS. The association of health-related factors with leisure-time physical activity among adults with COPD: a cross-sectional analysis. Healthcare. 2022;10(2):249. doi:10.3390/healthcare10020249
49. Yu T, ter Riet G, Puhan MA, Frei A. Physical activity and risk of comorbidities in patients with chronic obstructive pulmonary disease: a cohort study. NPJ Prim Care Respir Med. 2017;27(1):36. doi:10.1038/s41533-017-0034-x
50. Di Marco F, Verga M, Reggente M, et al. Anxiety and depression in COPD patients: the roles of gender and disease severity. Respir Med. 2006;100(10):1767–1774. doi:10.1016/j.rmed.2006.01.026
51. Herrera-Añazco P, Urrunaga-Pastor D, Benites-Zapata V, et al. Gender differences in depressive and anxiety symptoms during the first stage of the COVID-19 pandemic: a cross-sectional study in Latin America and the Caribbean. Front Psychiatry. 2022;13:727034. doi:10.3389/fpsyt.2022.727034
52. Seens H, Modarresi S, Fraser J, MacDermid JC, Walton DM, Grewal R. The role of sex and gender in the changing levels of anxiety and depression during the COVID-19 pandemic: a cross-sectional study. Womens Health. 2021;17:17455065211062964.
53. Lee SS, Chao MM, He H. When family interrupted work: the implications of gendered role perception in the face of COVID-19. J Soc Issues. 2022. doi:10.1111/josi.12504
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.