")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
Breathing Exercises in the Treatment of COPD: An Overview of Systematic Reviews
Authors Li Y , Ji Z, Wang Y, Li X, Xie Y
Received 11 August 2022
Accepted for publication 24 November 2022
Published 7 December 2022 Volume 2022:17 Pages 3075—3085
DOI https://doi.org/10.2147/COPD.S385855
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Richard Russell
Yiting Li,1 Zile Ji,1 Yan Wang,1 Xuanlin Li,1 Yang Xie2– 4
1The First Clinical Medical College, Henan University of Chinese Medicine, Zhengzhou, Henan, People’s Republic of China; 2Department of Respiratory Diseases, The First Affiliated Hospital of Henan University of Chinese Medicine, Zhengzhou, Henan, People’s Republic of China; 3Collaborative Innovation Center for Chinese Medicine and Respiratory Diseases Co-Construction by Henan Province & Education Ministry of P.R. China, Henan University of Chinese Medicine, Zhengzhou, People’s Republic of China; 4Henan Key Laboratory of Chinese Medicine for Respiratory Disease, Henan University of Chinese Medicine, Zhengzhou, People’s Republic of China
Correspondence: Yang Xie, Department of Respiratory Medicine, The First Affiliated Hospital of Henan University of Chinese Medicine, No. 19 Renmin Road, Zhengzhou, Henan, 450046, People’s Republic of China, Email [email protected]
Background: The effectiveness of breathing exercises in the treatment of chronic obstructive pulmonary disease (COPD) has been demonstrated in several systematic reviews (SRs), but a comprehensive review is still lacking. The aim of this study was to synthesize evidence from SRs, to summarise the effects of breathing exercises interventions for COPD patients.
Methods: We conducted an overview of the SRs of breathing exercises in the treatment of COPD. We include Systematic Reviews of randomized-controlled clinical trials. In the included COPD, control of breathing exercises alone was the only variable and no restriction was placed on relevant outcome measures. The SRs were screened by computer retrieval from the Chinese National Knowledge Infrastructure (CNKI), WanFang database, Chinese Science and Technology Journal Database (CSTJ), Chinese Biological Medicine (CBM), MEDLINE (PubMed), Embase, Cochrane library, and Web of Science. The Risk of Bias in Systematic reviews (ROBIS) tool, the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) statement, a Measure Tool to Assess Systematic Reviews (AMSTAR) 2, and the Grades of Recommendations, Assessment, Development and Evaluation (GRADE) were used to evaluate the risk of bias, reporting quality, methodology quality, and evidence quality.
Results: Nine SRs met the inclusion criteria and were included in the overview, 4 SRs in Chinese, and 3 SRs in English. All the SRs were published between 2015– 2021. According to the ROBIS tool, 4 SRs (57.14%) were rated as low risk of bias. The PRISMA scale showed that 5 SRs had some defects, and 2 SRs were relatively complete. Reporting deficiencies exist primarily in protocol and registration (28.6%), search (42.9%), risk of bias across studies (0%), additional analyses (42.9%), and funding (28.6%). Based on the AMSTAR-2 scale, 3 SRs were low quality, and the other 4 SRs were very low. The result of evidence quality assessment showed that among the 34 outcomes involved in the 7 studies, 19 were low-level outcomes, 15 were very low-level outcomes, and there were no moderate and high-level quality outcomes. Limitations and publication bias were two major factors that reduced the quality of evidence.
Conclusion: Breathing exercises in certain can improve pulmonary function, exercise endurance, dyspnea, quality of life, and respiratory muscle strength of COPD patients. However, there is an urgent need for high-quality studies to guide clinical practice due to certain deficiencies in reporting quality and the low quality of methodology and outcomes.
Keywords: breathing exercises, chronic obstructive pulmonary disease, overview, systematic reviews
Introduction
Chronic obstructive pulmonary disease (COPD) is a preventable and treatable disease characterized by persistent respiratory symptoms and restricted airflow.1,2 As a common multiple respiratory disease, COPD has a high prevalence and mortality rate and is expected to become the 5th-largest burden disease in the world by 2030.3 The treatment methods for COPD include pharmacotherapies and non-pharmacotherapies. The standard treatments of COPD include bronchodilators, inhaled glucocorticoids, and theophylline drugs. However, due to physical factors or other reasons, several patients have developed certain adverse effects to these pharmacotherapies,4 such as increased heart rate, dizziness, headache, dysuria, nausea, and vomiting. Therefore, more and more attention was paid to nonpharmacological treatments.
Pulmonary rehabilitation (PR), as a comprehensive treatment program, is to formulate an individualized treatment scheme for patients based on a comprehensive evaluation of patients’ overall condition to improve the physical and mental condition of patients with chronic respiratory diseases.5 Its application in clinical treatment is receiving more and more attention. Breathing exercise is an important part of the global lung rehabilitation program for COPD patients,6 including training in breathing patterns (pursed-lip breathing, diaphragmatic breathing, whole-body breathing exercises, etc.) and exercise of breathing muscles (inspiratory muscle training and expiratory muscle training). Compared with other treatment methods, breathing exercises are simple to operate, have no site restrictions, and do not require excessive capital investment, which can greatly improve patients’ initiative and compliance.
In recent years, a growing number of studies have proved that breathing exercises can significantly improve lung function and dyspnea, increase exercise endurance and improve the quality of life of patients with COPD.7–11 With the development of evidence-based medicine, the systematic reviews (SRs) of breathing exercises of COPD patients are also increasing year by year, but the quality of the reports is uneven, which brings great challenges to researchers’ clinical decision-making. For example, Langer et al12 and Basso-Vanelli et al13 found inspiratory muscle training (IMT) improved respiratory muscle strength and endurance, dyspnea, and exercise tolerance in patients with COPD. However, Figueiredo et al14 found IMT improved inspiratory muscle strength, functional capacity, and pulmonary function, without changing dyspnea and quality of life.
This is the first overview that comprehensively assessed SRs of breathing exercises for COPD patients. The aim of this overview is to critically assess the quality of relevant SRs and present an objective and comprehensive evaluation on effectiveness of breathing exercises for COPD, which can provide a scientific basis for clinical decision-making.
Materials and Methods
The overview protocol was registered in the PROSPERO (International prospective register of systematic overview) database (No. CRD42022329999).
Search Strategy
Relevant literature was searched from the Chinese National Knowledge Infrastructure (CNKI), WanFang database, Chinese Science and Technology Journal Database (CSTJ), Chinese Biological Medicine (CBM), MEDLINE (PubMed), Embase, Cochrane Library, and Web of Science up to March 30, 2022. The retrieval words are the combination of subject words and free words. The keywords include chronic obstructive pulmonary disease, COPD Chronic obstructive airway disease, COAD, chronic obstructive lung disease, respiratory muscle training, inspiratory muscle training, ventilation muscle training, breathing exercise, respiratory exercise, respiratory training, meta-analysis, systematic review, etc. The search strategy is shown in Table S1.
Inclusion Criteria
The inclusion criteria are described below.
Types of Studies
SRs of breathing exercises for COPD, in Chinese and English.
Types of Participants
Patients with a definite diagnosis of COPD, meeting any diagnostic standard at home and abroad, regardless of clinical stage and severity rating.
Types of Interventions
The experimental group received at least one form of breathing exercise (inspiratory muscle training, expiratory muscle training, diaphragmatic breathing, pursed-lip breathing, yoga breathing, respiratory gymnastics, etc.), and the control group received routine treatment (such as vital sign testing and dietary care), placebo, blank control (no interventions), or other treatments (conventional Western medical treatments).
Types of Outcome Measures
The outcome measures are as follows:
- Pulmonary function: forced expiratory volume in the first second (FEV1), forced vital capacity (FVC), the percentage of forced expiratory volume in the first second to the expected value (FEV1%), the ratio of forced expiratory volume to forced vital capacity in the first second (FEV1/FVC).
- Exercise capacity: six-minute walking distance (6MWD).
- Quality of life: St. George’s Respiratory Questionnaire (SGRQ).
- Dyspnea: modified Medical Research Council (mMRC) scale or other related scales.
- Respiratory muscle strength: maximum inspiratory pressures (PImax), maximum expiratory pressures (PEmax).
Exclusion Criteria
The SRs were excluded if one of the following criteria was met: duplicated publications; updated SRs; network meta-analysis; conference abstracts or systematic reviews’ protocols.
Screening and Data Extraction
According to the inclusion and exclusion criteria, two researchers independently conducted literature retrieval, screening and data extraction, and cross-checking. If there is a dispute, the third researcher will be asked to assist in the judgment. Use EndNoteX9 to check duplicates, delete duplicate documents, and then use Excel to record and extract the data. Extracted data include title, first author, year of publication, relevant data of the original research included (research type, sample size, intervention measures, outcome indicators, etc.), quality evaluation methods, main conclusions, etc. When necessary, complete information can be obtained by tracing and searching the included original research or attempting to contact the corresponding author for as complete information as possible.
Assessment of Included SRs
The quality of the final included literature and conducted cross-checking was independently evaluated by two researchers. If the evaluation is inconsistent, discuss or ask a third researcher to intervene.
Risk of Bias Evaluation
The ROBIS tool was used to evaluate the level of bias presented in the included SRs. The process includes three phases: (1) assess the relevance (optional) to evaluate the degree of coincidence between the target problem and the problem to be solved in the review; (2) identify concerns with the review process, including 4 domains (study eligibility criteria, identification and selection of studies, data collection and study appraisal, synthesis and findings); (3) judge risk of bias in the review. Each domain has signaled questions and a judgment of concerns about the risk of bias in the domain, and the results are rated as “high risk”, “low risk”, or “unclear risk”.15
Report Quality Evaluation
PRISMA statement16 was used to assess the report quality of the included SRs. It consists of 27 statements, of which 1 point is for a standardized and complete report, 0.5 points for a partial report, and 0 points for a non-report. A score of ≤15 was considered to be a relatively serious information c, >15–21 was considered to be a report with some deficiencies, and >21–27 was considered to be a relatively complete report.
Methodological Quality Evaluation
AMSTAR-2 scale17 was used to assess the methodological quality of the included SRs. AMSTAR-2 scale contains 16 items, and the grade of literature quality is mainly based on 7 critical items: items 2, 4, 7, 9, 11, 13, and 15. According to the compliance of critical items and non-critical items, it is divided into four quality levels: high, medium, low, and critically low. 0–1 non-critical item do not meet the requirements is considered high quality; more than one non-critical item is not met (when multiple non-critical items fail to meet the requirements, the confidence of the systematic review can be reduced from intermediate to low level), as medium quality; one critical item does not meet with or without non-critical items non-compliance is considered low quality; more than one critical item does not meet the requirements, with or without non-critical items non-compliance, is considered critically low quality.
Evidence Quality Evaluation
The quality of outcomes of included SRs was evaluated by the GRADE system.18 The GRADE system divides the evidence into four levels: high, moderate, low, and very low, based on five degrading factors (risk of bias, inconsistency, indirection, imprecision, and publication bias). Randomized controlled trials (RCTs) are specified as high quality, downgrade 1 is moderate, downgrade 2 is low, and downgrade 3 is very low.
Results
Literature Search
According to the formulated search strategy, 801 related documents were preliminarily retrieved. We used EndNoteX9 to check the duplicates. After checking, 645 articles remained. 583 records were excluded through reading the title and abstract, and 55 were excluded after downloading the full text. The reasons for exclusion are presented in Table S2. Finally, 7 studies were included. The process of study selection is shown in Figure 1.
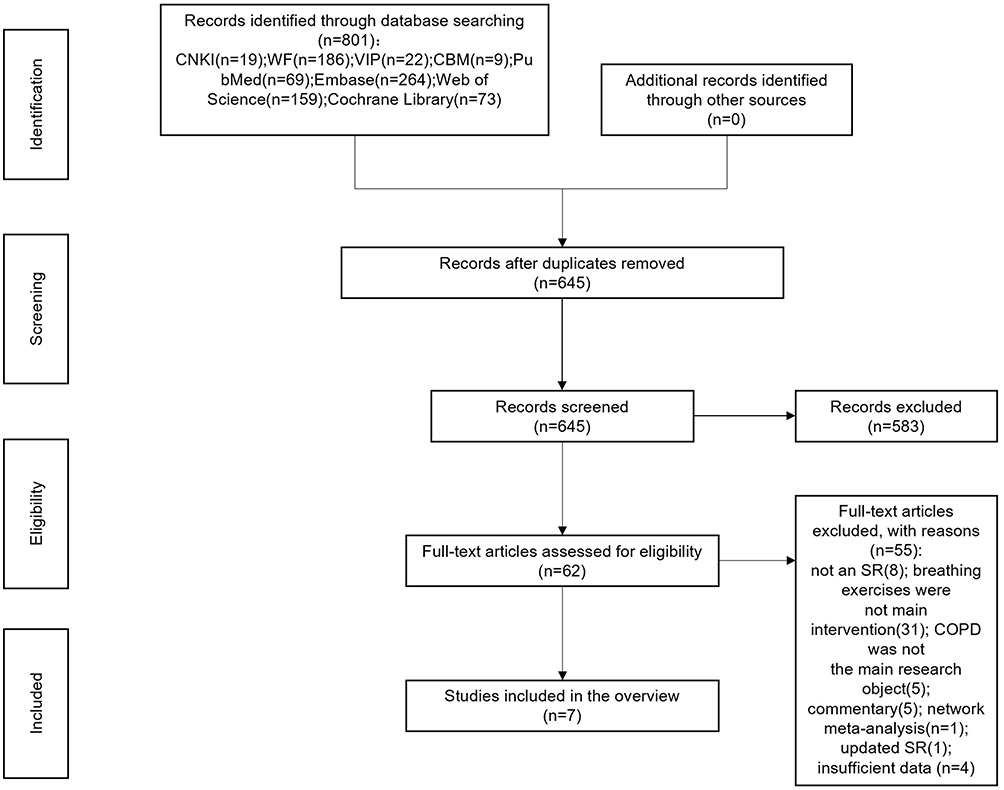 |
Figure 1 Flowchart of literature screening. |
Characteristics of Included SRs
A total of 719–25 SRs were included in this study, 419–22 SRs in Chinese, and 323–25 SRs in English, all of which were published in journals from 2015 to 2021. The number of original studies included ranged from 8 to 17, and the sample size ranged from 593 to 1098. The subjects were all patients with COPD, of which 419,20,22,23 were diagnosed as patients with stable COPD, and 519–21,23,25 described the diagnostic criteria. In terms of quality assessment tools, 119 SR used the Jadad scale, 420–22,24 SRs used the Cochrane risk of bias tool, 125 SR used both the Jadad scale and Cochrane risk of bias tool, and 123 SR used PEDro scale. The characteristics of included SRs are presented in Table S3.
Risk of Bias of Included SRs
The ROBIS tool evaluation results are shown in Table 1 and Figure S1. Phrase 1 which is optional was not performed in our study. Domain 1 assessed whether study eligibility criteria were prespecified, clear, and appropriate to the review question, and 7 SRs (100%) were at low risk of bias. Domain 2 assessed whether any original studies that meet the inclusion criteria have been omitted, and 2 SRs (28.57%) were rated as low risk of bias. Domain 3 assessed whether bias occurred during data extraction or quality evaluation of the original studies, and 7 SRs (100%) were at low risk of bias. Domain 4 assessed whether used appropriate methods to combine data from the primary studies, including qualitative and quantitative synthesis, and 4 SRs were at unclear risk of bias. The final phrase considered the overall risk of bias, and 4 SRs (57.14%) were rated as low risk of bias.
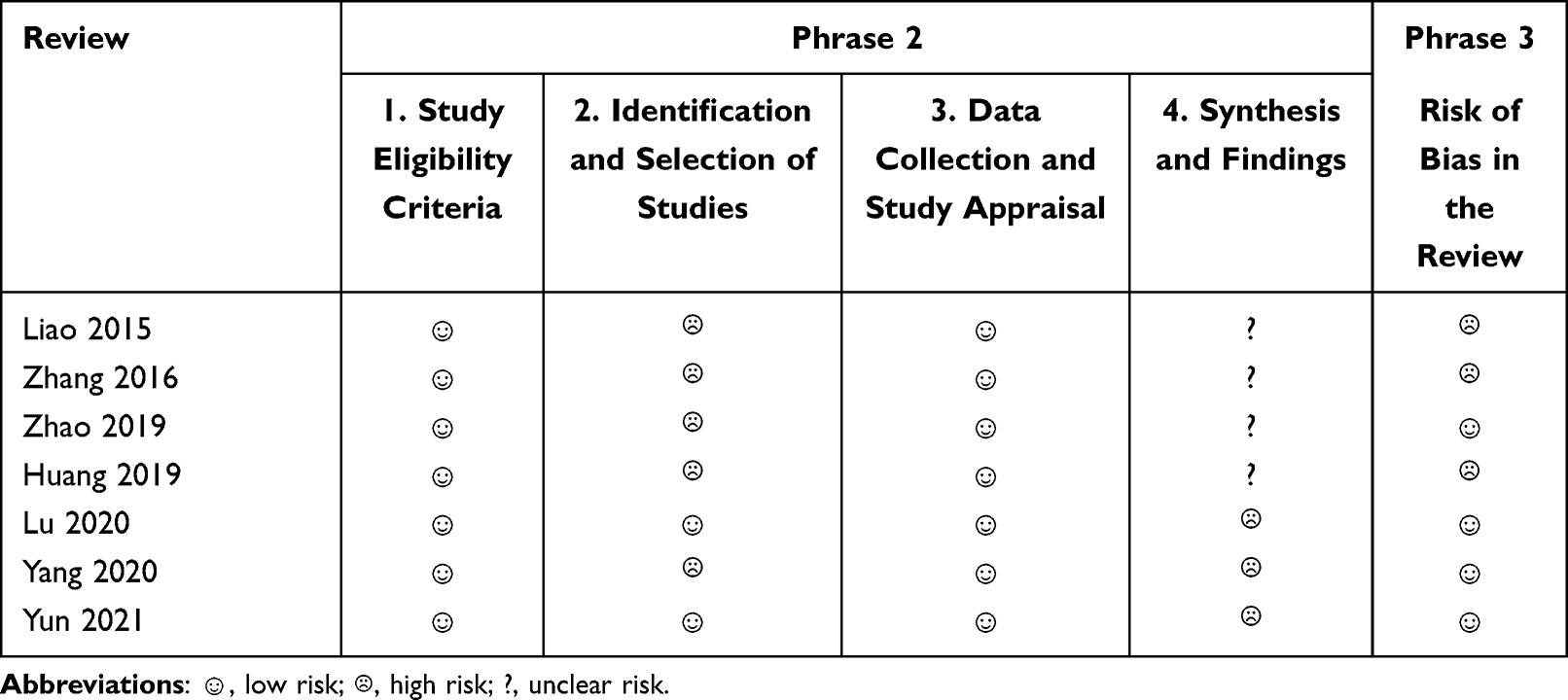 |
Table 1 Tabular Presentation of Risk of Bias of Included SRs |
Report Quality of Included SRs
The PRISMA scale report quality evaluation shows that the score of the included SRs ranged from 15.5 to 24. There were no SRs with a score of ≤15 points; 519,20,22–24 SRs with a score of 15–21 points; 221,25 SRs with a score of ≥21 points. All SRs completely reported the rationale, objectives, data collection process, risk of bias in individual studies, summary measures, synthesis of results, risk of bias within studies, results of individual studies, and conclusions. Reporting deficiencies mainly exist in the following items: protocol and registration (28.6%), search (42.9%), risk of bias across studies (0%), additional analyses (42.9), and funding (28.6%). The report quality of included SRs is shown in Table 2 and Figure S2.
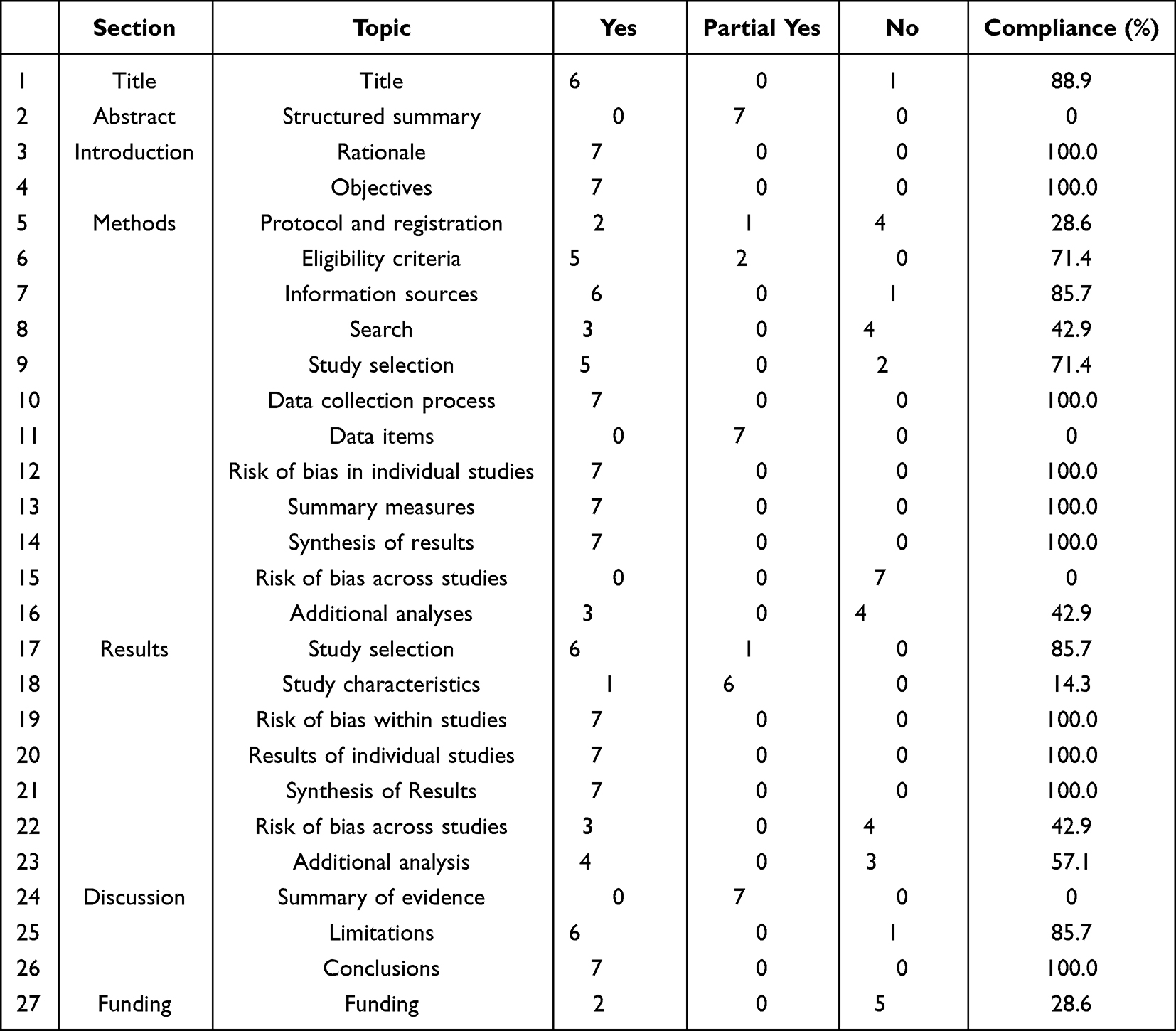 |
Table 2 Report Quality of Included SRs |
Methodological Quality of Included SRs
The results of the AMSTAR-2 assessment are presented in Table 3 and Figure S3. The overview shows that 320,23,25 were low quality, and 419,21,22,24 SRs were critically low quality. Focus on the evaluation results of critical items: 419–22 SRs did not state the review methods; 719–25 SRs did not search the relevant grey literature; 121 SR did not provide the exclusion list, and 619,20,22–25 SRs provided the exclusion list, but not detail enough; 719–25 SRs used a satisfactory tool to evaluate the risk of bias in individual studies, and selected appropriate statistical methods to merge the research results in meta-analysis; 219,24 SRs did not consider the risk of bias when interpreting or discussing the results of each study; only 220,21 SRs evaluated and discussed the publication bias.
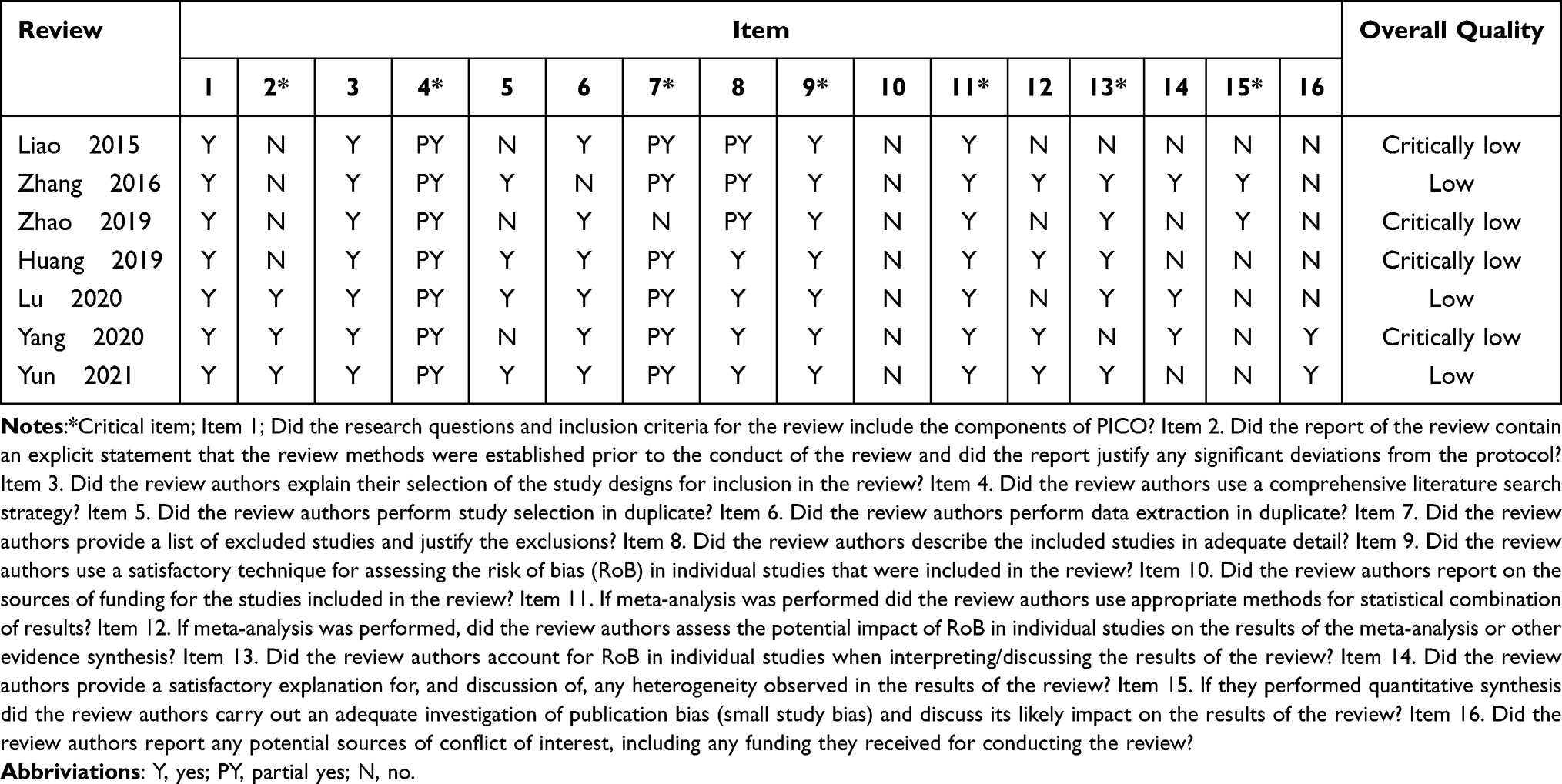 |
Table 3 Tabular Presentation of Methodological Quality of Included SRs |
Evidence Quality of Included SRs
34 outcomes were evaluated by the GRADE system. Further details can be seen in Table S4. The results showed that there were 19 low-level outcomes, 15 very low-level outcomes, and there were no moderate and high-level quality outcomes. Limitations and publication bias are two major factors that reduce the evaluation of evidence quality.
Pulmonary Function
The main outcomes of pulmonary function were FEV1, FVC, FEV1%, and FEV1/FVC. Six19–21,23–25 articles reported the effect of breathing exercises on pulmonary function of COPD patients. Except for one SR showed no significant difference, the other 519–21,23,24 SRs showed that breathing exercises could significantly improve the pulmonary function of COPD patients. Among them, 419–21,24 SRs used the outcome FEV1, 319,21,24 SRs had a low-quality level, and 120 SR had a very low-quality level; 319,21,24 SRs used the outcome FVC, 221,24 SRs had a low-quality level, and 119 SR had a very low-quality level; only 123 SR used the outcome FEV1%, and the quality level was very low; 619–21,23–25 SRs used the outcome FEV1/FVC. The quality grade of 321,23,25 SRs was low, and the other 319,20,24 SRs were very low.
6MWD
The included 719–25 SRs all reported the effect of breathing exercises on 6MWD in patients with COPD. The quality level of 323–25 SRs was low, and 419–22 SRs were very low. The results of the meta-analysis showed that: only 122 SRs showed no statistically significant difference, considering the possibility of the small sample size and/or irreversible pulmonary fibrosis structural changes in COPD patients; the remaining 619–21,23–25 SRs showed that breathing exercises can significantly improve the exercise endurance in COPD patients.
SGRQ
There are 421–23,25 SRs reporting the effect of breathing exercises on SGRQ in COPD patients. The quality level of 221,23 SRs is low, and 222,25 SRs are very low. 122 SR used descriptive analysis showed that after IMT intervention, the quality of life of patients was significantly improved; 321,23,25 SRs used meta-analysis: 125 showed that there was no significant difference between the experimental group and the control group, and 221,23 showed that breathing exercises could significantly improve the quality of life of patients.
Dyspnea
Four21–23,25 SRs reported the effect of breathing exercises on dyspnea in patients with COPD. The quality level of 222,23 SRs was low, and 221,25 SRs was very low. Two22,25 SRs used descriptive analysis, one showed that IMT could relieve dyspnea in COPD patients, and the other one showed that breathing exercises did not significantly improve dyspnea; 221,23 SRs used meta-analysis: one SR showed no statistically significant difference, another one showed that breathing exercises could significantly improve dyspnea in COPD patients.
Respiratory Muscle Strength
The outcomes of respiratory muscle strength are mainly PImax and PEmax. Three22,23,25 SRs reported PImax: 222,23 SRs have a low-quality level, and 125 SR have a very low-quality level. The meta-analysis results showed that breathing exercises can significantly improve the inspiratory muscle strength of patients. Two23,25 SRs reported PEmax: 123 SR was rated as low quality, the other one was rated as very low quality. One23 SR showed that breathing training could significantly improve the expiratory muscle strength of patients, and another one conducted a subgroup analysis based on different ethnic groups. The results showed that the expiratory muscle strength of Caucasian people was improved, but not increased in Asian people. Considering that this may be due to differences in interventions for patients of different races, as well as differences in the severity of COPD.
Discussion
This is the first overview of SRs to investigate the effectiveness of breathing exercises in COPD patients, with the aim of providing more scientific evidence for clinical decision-makers. We rigorously appraised the included SRs with the ROBIS tool, PRISMA statement, AMSTAR-2 scale, and GRADE system. Based on ROBIS tool, 4 SRs (57.14%) were rated as low risk of bias. With PRISMA checklist, we found that 5 SRs had some defects, and 2 SRs were relatively complete. The results of AMSTAR-2 suggested that 3 SRs were low quality, and the other 4 SRs were very low. GRADE evidence quality evaluation showed that among the 34 outcomes involved in the 7 studies, 19 were low-level outcomes, 15 were very low-level outcomes, and there were no moderate and high-level quality outcomes.
According to the ROBIS tool, we found a relatively high risk of bias in domain 2 and domain 4 of Phase 2. Domain 2 assessed whether omitted any original studies that meet the inclusion criteria. The results indicated that the researchers should involve appropriate databases and electronic sources to identify published reports, include methods additional to database searching, and use an appropriate and sensitive search strategy when conducting SRs/meta-analyses. In domain 4, the risk of bias in the synthesis of findings was high. Although all SRs synthesized data, we could not determine whether the data synthesis and analysis methods were appropriate for the research question posed, which may lead to the loss of some research results. The robustness of study results should be assessed by funnel plots or sensitivity analyses, and biases in primary studies should be taken into account.
The overview results of the PRISMA statement and AMSTAR-2 scale showed the included SRs had some reporting weaknesses and the overall methodological quality needed to be improved. This is mainly because although the included SRs followed the PICO principles, they did not design a reasonable study protocol and register before the start of the study; the grey literature was not searched when searching literature; the detailed list and reasons for the excluded SRs were not provided when screening literature; the analysis and discussion did not include an explanation for the risk of heterogeneity and bias; the source of funding and potential conflicts of interest were not disclosed. Therefore, it is suggested that researchers should strictly adhere to the PRISMA statement and AMSTAR-2 scale in future evaluation.
Although the conclusion of the SRs included in this study showed that breathing exercises have a certain effect on COPD patients, the GRADE systematic evaluation showed that the overall quality of evidence for the outcome indicators of the included SRs is low. Limitations and publication bias were the main factors for downgrading. The main reasons for the limitation were that the original study included in the literature did not completely and clearly report the randomization methods, blinding, allocation concealment, and loss of follow-up; the main reasons for publication bias were that the small number of included studies, all positive results and no assessment of publication bias. Therefore, in clinical research, we need to improve the quality of the original research as much as possible, and strictly standardize the research methods, so as to obtain more real and objective evidence support.
This overview suggests that although the quality of the available evidence is low, there is a certain role for breathing exercises in COPD patients. The specific modalities of breathing exercises in the included SRs were breathing gymnastics, IMT, EMT, PLB, DB, combined or not with other treatments (including usual care and medication). Regardless of the modality of breathing exercises, all of them have a certain positive effect on COPD. All seven included SRs reported on exercise endurance, with six showing that breathing exercises significantly improved patients’ exercise endurance; six reported on lung function, with five showing that patients’ lung function improved; and four reported on the quality of life, with three showing that patients’ quality of life could be improved. Breathing exercises can not only exercise the respiratory muscles of COPD patients, improve their dyspnea symptoms, increase tolerance to physical activity, enhance physical fitness, and enable them to establish an effective breathing pattern, but can also be associated with the prevention and reduction of pulmonary function impairment due to hypoxia, carbon dioxide retention, and other causes. Adhering to respiratory training on the basis of conventional drug therapy can delay the progress of slow obstructive pulmonary disease to a certain extent.
To improve the evidence base for breathing exercises, there are several concerns that need to be resolved, including the heterogeneity of the primary studies and the lack of systematic evaluation and interpretation of the overall quality of the evidence within SRs. First, there was generally clinical heterogeneity across studies included within SRs, in terms of participants (phase of COPD), interventions (type, intensity, and frequency) and outcomes. The results of heterogeneous studies were often pooled within meta-analyses, influencing the results and conclusions of SRs. Importantly, meta-analyses only combine the results of studies with sufficient homogeneity.26 Second, the quality of evidence includes consideration of within-study RoB (methodological quality), directness of evidence, heterogeneity, precision of effect estimates and risk of publication bias.27 Therefore, systematic evaluation of certainty of evidence generated in the overview is difficult to achieve for several different methodological reasons, including the lack of standard methods for overviews, the use of overall scores to summarize RoB assessment and the certainty assessment of evidence. While the GRADE approach provides a systematic method for assessing the certainty of evidence, there remains uncertainty about the best way to implement this within overviews.28
Implications for Future Practice and Research
Due to its superior availability and relatively low clinical side effects, breathing exercises have become an important supplementary and alternative therapy for COPD. We found some positive evidence supporting the use of breathing exercises for COPD, although the GRADE quality of evidence was assessed as low. Because of these issues, more rigorous larger-scale and well-designed RCTs are needed to provide higher-quality evidence and assess the efficacy of breathing exercises for COPD. First, RCTs should follow appropriate guidelines, such as AMSTAR-2 scale and CONSORT40 (Consolidated Standards of Reporting Trials). Second, many different types of breathing exercises are used in clinical practice to treat COPD. Therefore, future comparative studies of different breathing exercise interventions are needed to determine the most effective method of breathing exercises. Third, all SRs must be pre-registered to promote transparency of processing and to avoid the risk of methodological bias. In addition, a critical assessment of the safety of breathing exercises for COPD needs to be conducted in clinical trials.
Limitations
There are several limitations in this overview. First, this study only included the studies published in Chinese or English, which were manually searched by researchers, and the relevant gray literature was not searched, so there was a certain selective bias. Second, although some overlap of primary articles within the included SRs could be expected, we did not explore these overlaps systematically. As a result, this may lead to inaccurate reporting of data, such as the number of participants and primary studies. Third, due to the apparent clinical and statistical heterogeneity among the included systematic reviews and the complex categories of interventions, we only provide a narrative summary of the effectiveness of interventions rather than a quantitative analysis. Finally, although the researchers strictly follow the PRISMA statement, AMSTAR-2 scale, and GRADE system assessed the quality of included SRs, the interference of subjective factors cannot be avoided in the evaluation, which will also produce a certain bias.
Conclusions
What is the exact effect of breathing exercises in the treatment of COPD? In our study, the methodological quality of the included SRs was varied, as well as the quality of evidence underlying these outcomes, which made it difficult to draw firm conclusions on this question. Therefore, more high-quality and large sample randomized controlled trials are urgently needed in the future. At the same time, it is hoped that researchers can strictly follow the PRISMA statement and AMSTAR-2 scale to standardize the research protocols and improve the level of evidence when conducting SRs, in order to obtain more high-quality research and provide a scientific decision-making basis for clinicians.
Acknowledgments
The authors really appreciate the help of people from Henan University of Chinese Medicine.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was supported by the National key R & D Program (NO. 2018YFC1704806); Henan science and technology research project (NO. 212102311128); Henan Province Outstanding Youth Science Fund Project (NO.212300410056); Henan Province Second Batch of Top-notch Chinese Medicine Talent Projects (Yuwei Chinese Medicine Letter 2021 No. 15).
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Panel of Practice Standard for Clinical Diagnosis and Treatment of Chronic Obstructive Pulmonary Disease. Standards for clinical practice in diagnosis and treatment of chronic obstructive pulmonary disease. Int J Respir. 2022;42(6):401–409. doi:10.3760/cma.j.cn131368-20211223-00939
2. Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report. GOLD executive summary. Am J Respir Crit Care Med. 2017;195(5):557–582. doi:10.1164/rccm.201701-0218PP
3. World Health Organization. World Health Statistics 2008M. Geneva: World Health Organization; 2008.
4. Labaki WW, Rosenberg SR. Chronic obstructive pulmonary disease. Ann Intern Med. 2020;173(3):ITC17–ITC32. doi:10.7326/AITC202008040
5. Spruit MA, Singh SJ, Garvey C, et al. An official American Thoracic Society/European Respiratory Society statement: key concepts and advances in pulmonary rehabilitation. Am J Respir Crit Care Med. 2013;188(8):e13–e64. doi:10.1164/rccm.201309-1634ST
6. Ubolnuar N, Tantisuwat A, Thaveeratitham P, et al. Effects of breathing exercises in patients with chronic obstructive pulmonary disease: systematic review and meta-analysis. Ann Rehabil Med. 2019;43(4):509–523. doi:10.5535/arm.2019.43.4.509
7. Mehani SHM. Comparative study of two different respiratory training protocols in elderly patients with chronic obstructive pulmonary disease. Clin Interv Aging. 2017;12:1705–1715. doi:10.2147/CIA.S145688
8. Holland AE, Hill CJ, Jones AY, McDonald CF. Breathing exercises for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2012;10:CD008250. doi:10.1002/14651858.CD008250.pub2
9. Marotta N, Demeco A, Moggio L, et al. Comparative effectiveness of breathing exercises in patients with chronic obstructive pulmonary disease. Complement Ther Clin Pract. 2020;41:101260. doi:10.1016/j.ctcp.2020.101260
10. Beaumont M, Forget P, Couturaud F, Reychler G. Effects of inspiratory muscle training in COPD patients: a systematic review and meta-analysis. Clin Respir J. 2018;12(7):2178–2188. doi:10.1111/crj.12905
11. Xiao L, Duan H, Li P, Wu W, Shan C, Liu X. A systematic review and meta-analysis of Liuzijue in stable patients with chronic obstructive pulmonary disease. BMC Complement Med Ther. 2020;20(1):308. doi:10.1186/s12906-020-03104-1
12. Langer D, Ciavaglia C, Faisal A, et al. Inspiratory muscle training reduces diaphragm activation and dyspnea during exercise in COPD. J Appl Physiol. 2018;125(2):381–392. doi:10.1152/japplphysiol.01078.2017
13. Basso-Vanelli RP, Di Lorenzo VA, Labadessa IG, et al. Effects of inspiratory muscle training and calisthenics-and-breathing exercises in COPD with and without respiratory muscle weakness. Respir Care. 2016;61(1):50–60. doi:10.4187/respcare.03947
14. Figueiredo RIN, Azambuja AM, Cureau FV, et al. Inspiratory muscle training in COPD. Respir Care. 2020;65(8):1189–1201. doi:10.4187/respcare.07098
15. Whiting P, Savović J, Higgins JPT, et al. ROBIS: un nuovo strumento sviluppato per valutare i rischi di distorsione nelle revisioni sistematiche ROBIS: a new tool to assess risk of bias in systematic reviews was developed. Recenti Prog Med. 2018;109(9):421–431. doi:10.1701/2990.29928
16. Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097. doi:10.1371/journal.pmed.1000097
17. Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. doi:10.1136/bmj.j4008
18. Guyatt G, Oxman AD, Akl EA, et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J Clin Epidemiol. 2011;64(4):383–394. doi:10.1016/j.jclinepi.2010.04.026
19. Huang H, Qiu L, Chen P, et al. Systematic evaluation and meta-analysis of the effect of inspiratory muscle training on respiratory function in patients with stable COPD (in Chinese). China Med Herald. 2019;16(35):143–148.
20. Zhao Y, Hu H, Zhang L. Effect of breathing exercise on chronic obstructive pulmonary disease: a meta-analysis (in Chinese). Nurs J Chin Peoples Lib Army. 2019;36(01):32–37.
21. Zhang T, Zhang J, Zhang H. Aminophylline combined with respiratory function training for stable COPD: a meta-analysis (in Chinese). J HuBei Minzu Univ. 2016;33(3):36–40.
22. Liao L, Zhang P, Chen S. Meta-analysis of respiratory function training on pulmonary function and exercise endurance influence in patients with stable chronic obstructive pulmonary disease (in Chinese). Popul Sci Technol. 2015;17(12):79–82.
23. Lu Y, Li P, Li N, et al. Effects of home-based breathing exercises in subjects with COPD. Respir Care. 2020;65(3):377–387. doi:10.4187/respcare.07121
24. Yang Y, Wei L, Wang S, et al. The effects of pursed lip breathing combined with diaphragmatic breathing on pulmonary function and exercise capacity in patients with COPD: a systematic review and meta-analysis. Physiother Theory Pract. 2020;2020:1–11.
25. Yun R, Bai Y, Lu Y, et al. How breathing exercises influence on respiratory muscles and quality of life among patients with COPD? A systematic review and meta-analysis. Can Respir J. 2021;2021:1904231. doi:10.1155/2021/1904231
26. Murad MH, Montori VM, Ioannidis JP, et al. How to read a systematic review and meta-analysis and apply the results to patient care: users’ guides to the medical literature. JAMA. 2014;312(2):171–179. doi:10.1001/jama.2014.5559
27. Olivo SA, Macedo LG, Gadotti IC, et al. Scales to assess the quality of randomized controlled trials: a systematic review. Phys Ther. 2008;88(2):156–175. doi:10.2522/ptj.20070147
28. Lunny C, Brennan SE, McDonald S, et al. Evidence map of studies evaluating methods for conducting, interpreting and reporting overviews of systematic reviews of interventions: rationale and design. Syst Rev. 2016;5:4. doi:10.1186/s13643-015-0178-0
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.