Back to Journals » Veterinary Medicine: Research and Reports » Volume 13
Bovine Brucellosis: Epidemiology, Public Health Implications, and Status of Brucellosis in Ethiopia
Authors Tulu D ![]()
Received 2 November 2021
Accepted for publication 24 December 2021
Published 7 January 2022 Volume 2022:13 Pages 21—30
DOI https://doi.org/10.2147/VMRR.S347337
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Young Lyoo
Dereje Tulu
Ethiopia Institute of Agricultural Research, Tepi Agricultural Research Center, Tepi, Ethiopia
Correspondence: Dereje Tulu
Ethiopia Institute of Agricultural Research, Tepi Agricultural Research Center, PO Box 34, Tepi, Ethiopia
Email [email protected]
Abstract: Brucellosis is a globally distributed zoonotic disease that causes serious problems in developing countries such as Ethiopia. Brucella abortus is the primary cause of brucellosis in cattle, and Brucella melitensis and Brucella suis also occasionally cause Brucella infection in cattle. Abortion and the retained fetal membrane are typical signs in females, whereas orchitis and bursitis are the known signs in male cattle. Brucellosis is typically transmitted to healthy cattle by direct or indirect contact with diseased cattle or their discharges. Humans can acquire brucellosis through the consumption of unpasteurized milk or milk products, and through contact with diseased cattle or their discharges. The occurrence of bovine brucellosis is affected by different factors related to the management system, host, and environmental factors. In Ethiopia, the occurrence of brucellosis is high in pastoral and mixed cattle management systems, wherever humans live closely with cattle and so have a higher probability of picking up the Brucella organism. The most suitable technique in the management of Brucella infection is the vaccination of young female cattle. Brucella abortus can also be eradicated by the isolation of diseased cattle, administration of immunizing agents, and test-and-slaughter methods. Therefore, it is important to implement applicable management techniques and to increase public awareness about the transmission of brucellosis, and further research should be conducted on brucellosis in high-risk groups.
Keywords: brucellosis, cattle, epidemiology, public health, Ethiopia
Introduction
Ethiopia has the largest cattle population in Africa. However, the country has not used this resource effectively owing to various limitations.1 Animal disease, management problems, poor genetics, and nutritional deficiency are among the foremost impediments to cattle production in the country.2 Among the infectious diseases, Brucella infection is widely prevalent and causes extensive economic losses, and brucellosis is one of the most serious zoonotic diseases in Ethiopia.3,4 The introduction of higher-yielding cattle breeds is one of the major strategies to increase milk production in the country. However, brucellosis is the main challenge to the development of dairy farming in different parts of Ethiopia, since the disease causes reproductive inefficiency and pregnancy loss in cattle.5,6
Brucella infection causes huge financial losses and community health concerns in countries around the world, including Ethiopia.7–9 Brucella abortus, B. melitensis, and B. suis are the major causes of bovine brucellosis. The disease is known to cause abortion in the last stage of pregnancy, followed by retention of the fetal membrane and infertility in succeeding pregnancies in cattle.10 The Brucella organism spreads through interaction with aborting cattle and aborted materials or with contaminated fomites.11 Herd size, age and sex of the cattle, management system, contact with wild animals, environmental factors, and herding different species in a herd are among the reported risk factors. Vaccination of calves or heifers is the most effective means of managing Brucella in an endemic area. Moreover, brucellosis can be controlled by quarantining infected cattle, and by test-and-slaughter methods.12–15
In Ethiopia, a number of reports have shown that Brucella infection is a widespread cause of disease in cattle. These investigations indicated that the highest seroprevalence of the disease occurs in areas where people live in very close proximity to cattle.16,17 Seroprevalence rates of brucellosis ranging from 0.1% to 14.1% have been reported in Ethiopia.18,19 Research from various parts of the country, published in 2016,9,20,21 also showed that brucellosis was still a highly prevalent disease in Ethiopia, leading to high economic losses in cattle production. Nevertheless, there is limited evidence on the epidemiology and zoonotic implications of Brucella infection in cattle. Therefore, this article aims to review the epidemiology, zoonotic implications, and status of bovine brucellosis in Ethiopia.
Bovine Brucellosis
Etiology and Clinical Signs
Brucella abortus causes disease mainly in cattle, and at least nine biotypes (1–9) are recognized, as well as several variants.22 However, sheep, goats, and other domestic animals can also be infected. Cattle are also infected with B. suis and B. melitensis when they graze together with infected pigs, goats, or sheep.23,24 Brucella abortus is a small, Gram-negative, and facultative intracellular bacterium.25,26 The principal symptoms of Brucella infection are abortion in the last stage of pregnancy in female cattle, and orchitis and bursitis in male cattle.27,28 Brucella infection is assumed in herds when abortion and retention of placental occur in the last gestational stage, in the absence of other disease.7,22 Brucella infection results in abortion, stillbirths, retention of the placenta, and weak calves. Retention of the fetal membrane and endometritis are the outcomes of abortion. Female cattle generally abort just one, probably because of resistance. Hygromas on the leg joints of Brucella-infected cattle are a typical sign of the disease that results from chronic infection with Brucella.22,29
Epidemiology of Brucella Infection in Cattle
Transmission
Brucellosis is typically transmitted to other cattle by direct or indirect interaction with diseased cattle or their discharges.7 The spread of brucellosis in cattle occurs through the ingestion of contaminated feed and drinking water contaminated by the bacteria that are present in massive amounts in birth products and uterine discharge.11 Moreover, cattle typically lick their fetuses and newborn calves, which can have very high levels of bacteria and are the major source of infection.8 Brucella infection can also be transmitted by feeding pooled colostrum to newborn calves. Brucella infection is rarely spread through sexual contact in cattle. However, artificial insemination has been shown to spread the infection from infected cattle to healthy cattle.30 Humans typically acquire Brucella infection via the ingestion of unpasteurized milk or milk products. Interaction of the mucosa/abrasions with the fluid or tissues of aborted fetuses of diseased cattle can also be a source of disease in humans.26,31 Work-related contact with cattle or their products is the major risk for human brucellosis. Abattoir, farm, and laboratory workers, as well as veterinarians, are known risk groups for Brucella infection.32
Risk Factors for Bovine Brucellosis
The occurrence of Brucella infection is affected by a variety of factors associated with the management system, host, and environment. These include the age, sex, and breed of cattle, herd size and type, and agroecology.22,33,34 Age has been stated as the intrinsic factor related to Brucella infection. A higher seroprevalence of Brucella organisms has been determined in adult cattle than in young cattle.35,36 Sexually mature and pregnant cattle are more prone to being infected with Brucella than sexually immature cattle.13 This is because the Brucella organism confers a response in the reproductive tract owing to the concentration of erythritol sugar, generated within the fetal tissues of cattle, which stimulates the growth of Brucella organisms.22 However, the higher prevalence of Brucella in adults has also been related to longer interaction with diseased cattle. This could also be vital in the herd, while not culling the positive cattle.37
The effect of sex on the occurrence of Brucella infection in cattle has been stated previously.38 Female cattle are more likely than males to have Brucella infection.39 Although this is not easy to elucidate, it may be related to the biology of the Brucella organism and tropism to the fetal tissues.22 Because Brucella infection in males confers symptoms such as epididymitis and orchitis, the incidence in males may be lower than in females; as a result, they may be culled more quickly.40 However, the absence of symptoms such as abortion or metritis in non-pregnant diseased females may also mean that there is a higher prevalence in females. Moreover, brucellosis becomes chronic in non-pregnant cattle. This has important epidemiological consequences as, after the initial immune response in cattle that are symptomless carriers, the antibodies disappear from the circulation, and it can be challenging to identify them with standard serological methods.7
There is disagreement among investigators over whether particular breeds are more prone to Brucella infection. Thus, a higher seroprevalence of Brucella infection has been found in cross-breed than in local-breed (indigenous) cattle,12 while other reports indicated no association among breeds20 or a higher seroprevalence of Brucella infection in indigenous than in cross-breed cattle.41,42
Herd size is another risk factor for Brucella infection, with the risk being highest in large herds.2,12 This may be explained by the higher odds of identifying a minimum of one seropositive cattle, the rise of the spread of brucellosis by interaction among members of the herd, the use of common grazing lands, or inadequate cleaning and disinfection techniques on big farms.44 The low incidence of Brucella infection in small herds may be related to herd and/or arm management.40 Thus, small herds often graze nearby pastures, allowing interactions with other herds to be controlled, or using communal methods.45 A small herd can be simply managed during delivery, and cattle are frequently removed from the herd throughout parturition. This is extremely important in the case of abortion, to prevent contamination of the pasture. In small herds, substitutions are typically made by relocating animals and economic trade is uncommon. Hence, the lower rate of cattle movement reduces the chances of disease transmission. In contrast, cattle movement in large herds is common, both for replacement and for trade, thus increasing the risk of Brucella infection.46
Herding several species within a herd has been characterized as a risk factor for brucellosis,24,37 although there is no indication of the higher susceptibility of particular species to Brucella infection. As a result, the reason for the increased prevalence of brucellosis when various species mix is unclear, but it may be related to a higher probability of being infected with brucellosis owing to various sources of the disease. Brucella infection is seldom spread from small ruminants to cattle.47 Nevertheless, the threat to cattle on farms that also keep small ruminants suggests that some cases of bovine brucellosis may have originated from small ruminants, because B. melitensis biovar 3 has been isolated from cattle milk.48
Dairy cattle have a far greater probability of not only acquiring Brucella infection but also spreading it more rapidly than beef cattle. Cattle housed in small areas come into close contact with each other during feeding and milking.49 Dairy cattle are exposed to additional stress on farms, causing conditions that are more conducive to Brucella infection.50
Cattle purchase is considered as a risk for brucellosis and will increase the chance of introducing diseased cattle into the herd.13 Most infectious disease in previously brucellosis-free herds starts with the purchase of diseased cattle from unidentified sources.51 The effect of agroecology is also recognized as a Brucella infection risk factor, with a higher prevalence in dry areas.52 Because of a shortage of pasture in dry areas, cattle are put out to pasture over large areas, indicating uncontrolled cattle-to-cattle interaction with the potential risk of transmission. In addition, transmission through aerosol inhalation of contaminated dust from fetal discharges or abortions is likely.46
Large herd sizes are likely to be related to intensive management systems, which are generally tougher to manage and permit closer interactions between cattle and their surroundings, which can increase the probability of exposure to Brucella organisms.53 In addition, the stressful conditions of an intensive production system may make cattle more prone to infections. However, an extensive production system may also increase the risk of Brucella infection. This may be related to the management of abortions, identification of diseased cattle, and interactions among cattle.40 Since an extensive system implies rearing many cattle over a large area and sharing common pastures, the contamination of pastures with discharges from the reproductive tract may lead to brucellosis in the herds. Risk factors relating to farming and ecological conditions that affect the spread of brucellosis include giving birth, breeding in semi-dark settings, confined areas, and high cattle populations.53 The intensive system is another risk factor for brucellosis. This may be related to airborne transmission of disease-causing bacteria indoors.46 Similarly, the seasons have an influence on animal husbandry and nutrition, principally in pastoral areas.44 Rain influences the growth and nutritive status of animal feeds.
Diagnosis of Brucellosis
The isolation and identification of the Brucella organism offer a definitive diagnosis of brucellosis. This is important for epidemiology and to monitor the progress of vaccination programs in cattle.54 The diagnosis can be made using direct or indirect techniques.
Direct Diagnosis
Brucella infection can be confirmed by demonstration of the bacteria in smears with microscopic staining. The smears can be prepared from vaginal discharges, placenta, colostrum, fetal stomach fluid, the aborting cattle lochia, or the abomasum of the aborted fetus, with modified Ziehl-Neelsen (MZN) stain. Impression smears may be taken from freshly cut and blotted tissue surfaces, eg cotyledons, by firmly pressing the slide surface against the tissue. They are then allowed to air dry before heat fixation. Smears can also be prepared from fetal stomach fluid, cotyledons, or lochia, and stained with the improved Ziehl–Neelsen stain or stamp stain. In MZN-stained smears, the Brucella organism appears as red intracellular coccobacilli or rod shapes, whereas other bacteria stain blue.54
All Brucella strains are relatively slow growing, and as the isolated specimens are often heavily contaminated, the use of a selective medium, eg Farrell’s medium, is advocated. Incubation usually continues for 72 hours, but a negative diagnosis can only be made after a week-long incubation. Samples that can be used for B. abortus isolation include fetal stomach fluid, spleen, liver, placenta, lochia, milk (especially colostrum or milk within a week of calving), semen, and lymph nodes (supramammary lymph nodes are favored for chronic and latent infections, and retropharyngeal for early infections, but iliac, prescapular, and parotid lymph nodes may also be used). If serological reactions are thought to be caused by the S19 vaccine strain, then prescapular lymph nodes must also be gathered. All B. abortus isolates should be sent to laboratories with biotyping facilities. Farrell’s medium and Brucella albimi medium are selective enriched media for the isolation of Brucella species.7,54
Indirect Diagnosis
In the absence of culture facilities, the diagnosis of Brucella infection is usually based on serological tests, with various agglutination tests such as the Rose Bengal plate test (RBPT), serum agglutination test, and antiglobulins.55 Detection of antibodies (and to a lesser degree the measurement of cell-mediated immunity) against relevant Brucella epitopes is a more sensitive method.56 Serology can be used for an apparent diagnosis of Brucella infection or to screen a herd. Indirect and competitive enzyme-linked immunosorbent assays (i-ELISA and c-ELISA) are also used.7,45
The RBPT is a very sensitive test used for screening serum samples. It does not distinguish between field and S19 vaccine strain reactions, but it is quick, inexpensive, and easy to implement.57 False-negative reactions are rare but may sometimes be due to excessive heating in storage or in transit. The RBPT has a sensitivity of 96.10% and specificity of 99.30%.58
The diagnosis of brucellosis in cattle may be adversely affected by the presence of cross-reactions that give false-positive serological test results due to S19 vaccine or other Gram-negative bacteria that share similar epitopes, such as B. abortus O-chain polysaccharides.59,60 Thus, Yersinia enterocolitica 0:9, Escherichia coli 0157:H7, Salmonella group N (0:30), Francisella tularemia, Stenotrophomonas maltophilia, Pasteurella species, and Vibrio cholera can react in serological tests for Brucella infections in cattle.60–62 Therefore, the positive reaction should be investigated using appropriate confirmatory tests and/or epidemiological investigations. The RBPT appears to be adequate as a screening test for identifying diseased herds or to guarantee the absence of infection in Brucella infection-free herds.7
The complement fixation test (CFT) is the most generally used test for serological confirmation of Brucella infection in cattle, and is recommended by the World Organisation for Animal Health (OIE).7 The CFT is based on the detection of particular antibodies of type IgM and IgG1 that fix complement.60 The sensitivity and specificity of the CFT are acceptable in the hands of experienced users, and it can be used as a confirmatory blood test. Usually, the CFT is used on RBPT-positive sera, but similarly to the RBPT it is also influenced to a large extent by the misuse of S19 vaccine, mainly when recent or repetitive vaccinations have been carried out in sexually mature heifers and cows. It is almost impossible to suggest a strict cut-off reading that shows brucellosis significantly once the S19 vaccine reaction is involved, because of its misuse. The CFT is a comparatively complex test. The reagents include B. abortus CFT antigen, complement, amboceptor (hemolysin), ovine erythrocytes, and test serum, with veronal buffer as the diluent.54
The c-ELISA is usually conducted by choosing monoclonal antibodies (mAbs) with slightly higher affinity for the antigen than the vaccine or cross-reacting antibody, but with lower affinity than the antibody arising from the infection.63 The specificity of c-ELISA is very high and it is capable of identifying all antibody isotopes (IgM, IgG1, IgG2, and IgA).60 The c-ELISA has high diagnostic specificity (100%) and a sensitivity of 98.8%, and it was observed to be the most specific test.64 The high specificity of c-ELISA is a result of its using particular monoclonal antibodies as a conjugate, which have the ability to connect with other non-specific antibodies and fix to certain specific epitopes on the smooth lipopolysaccharides antigen.64,65 The indirect ELISA (i-ELISA) has been also used for serological diagnosis of serum or milk from cattle.66 The i-ELISA has been used for smooth lipopolysaccharide Brucella species, and it is sensitive and specific for B. abortus or B. melitensis, but it is not capable of differentiating antibodies induced by the vaccine strains S19 or Rev1.67 The sensitivity of the i-ELISA varies from 96% to 100% and its specificity from 93.8% to 100%.68
The confirmatory test has to demonstrate a high level of diagnostic specificity and maintain effective sensitivity to reduce the number of false-positive reactions to a minimum.69 The c-ELISA, in addition, is capable of reducing most reactions because of a residual antibody formed in reaction to vaccination with S19. The three OIE ELISA standard sera should be used by national reference laboratories worldwide to see or adjust the technique in question. The assay should be standardized, eg the optical density (OD) of the strongly positive OIE ELISA standard serum ought to be close to the highest level of inhibition.7 The only limitation of the c-ELISA is that it is more complex and cost to conduct than the screening tests.70 Weakly positive OIE ELISA common sera should provide a reaction that is moderate. The negative serum and the buffer or mAb control should give responses that are always less than the test population.7
Occurrence of Brucellosis
Brucellosis has a worldwide distribution and is mainly a problem in developing countries such as Ethiopia.8 This disease is economically important in cattle production in developing countries. Brucellosis has a significant influence on cattle and public health, as well as extensive socio-economic effects, particularly in countries with economies based on livestock production and dairy products (Table 1).
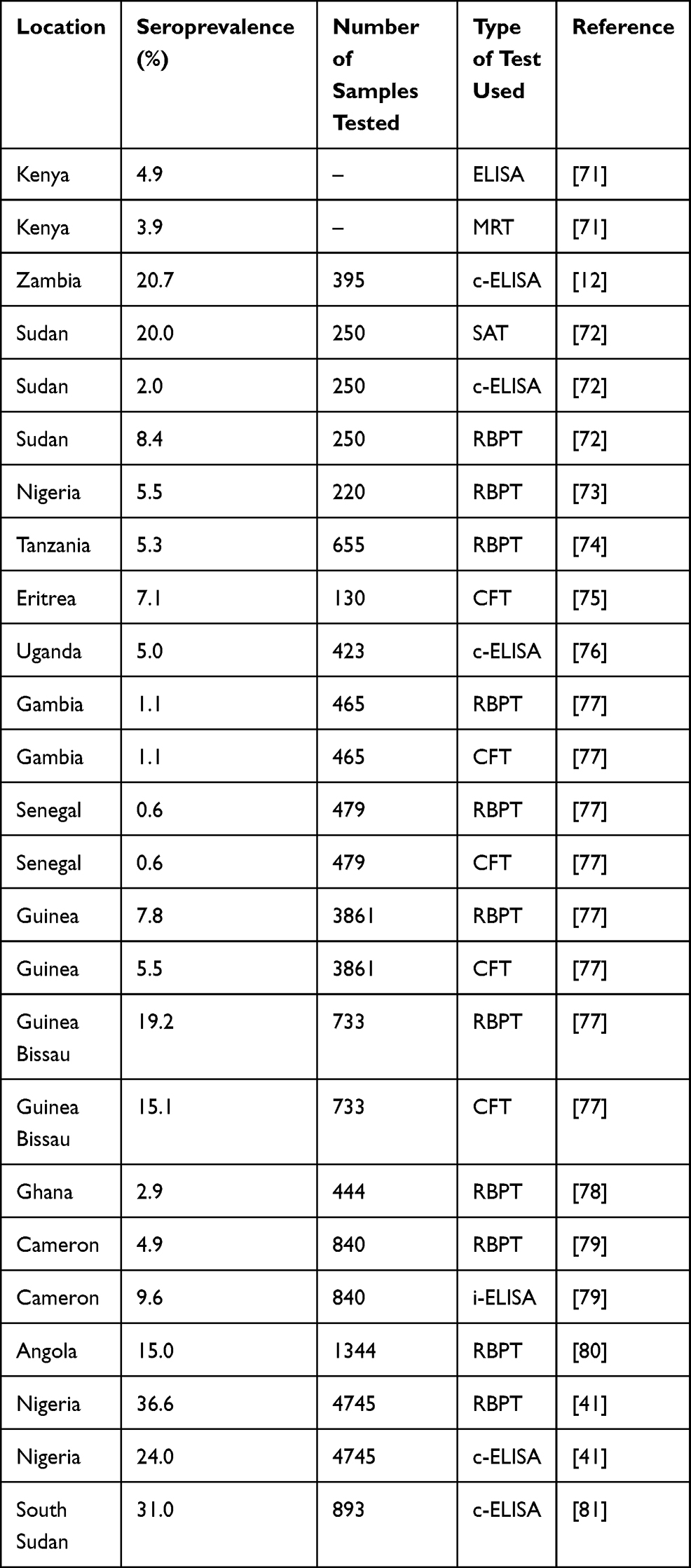 |
Table 1 Distribution of Brucellosis in Different African Countries |
Control and Eradication of Brucella Infection
Brucellosis treatment in animals is typically ineffective because of the intracellular nature of the organisms, which means that bacteria persist and multiply in the cells.22 Brucella infection typically enters the herd via diseased cattle, as well as the disease being acquired from the semen of infected bulls or fomites.30 Immunization of calves or heifers is the most effective means of managing Brucella in an endemic area. Newly introduced cattle should be free from Brucella and also come from disease-free areas. New animals must be quarantined and tested for Brucella infection before being introduced into the group.81,82 Brucellosis can be eradicated by quarantining infected cattle, vaccination, and test-and-slaughter methods. Moreover, several forms of investigation and tracebacks are important in eradication programs.33 Brucella organisms are killed by most typically available disinfectants.83 Two B. abortus vaccines, strain 19 and RB51, are used to manage brucellosis in common areas and as part of the eradication approach.45,82
Public Health Significance of Brucellosis
Brucella abortus causes serious zoonotic disease and is an invasive Brucella species in humans. Occupational contact is seen in people who have interacted with infected cattle or their tissues. Brucella infection is among the principal easily acquired laboratory infections. Humans can also contract the disease by consuming unpasteurized milk or milk products.84 The strain 19 B. abortus vaccine can also affect humans unless it is handled carefully. Adverse events have been reported with the RB51 vaccine, although it seems to be safer than strain 19.45
The prevalence of Brucella infection in humans is associated with the prevalence in nearby cattle.85 Brucellosis is a comparatively common disease among animals and humans in developing countries, and several cases of brucellosis occur each year.54 Symptoms of brucellosis in humans include fever, sweat, anorexia, malaise, weight loss, depression, headache, and joint pain. This disease may be confused with other diseases such as malaria and influenza.83,86,87 The highest seroprevalence of human brucellosis was reported in the Afar region (12%), whereas low seroprevalence was reported in the Fafan zone (0.4%) in Ethiopia using the CFT (Table 2).
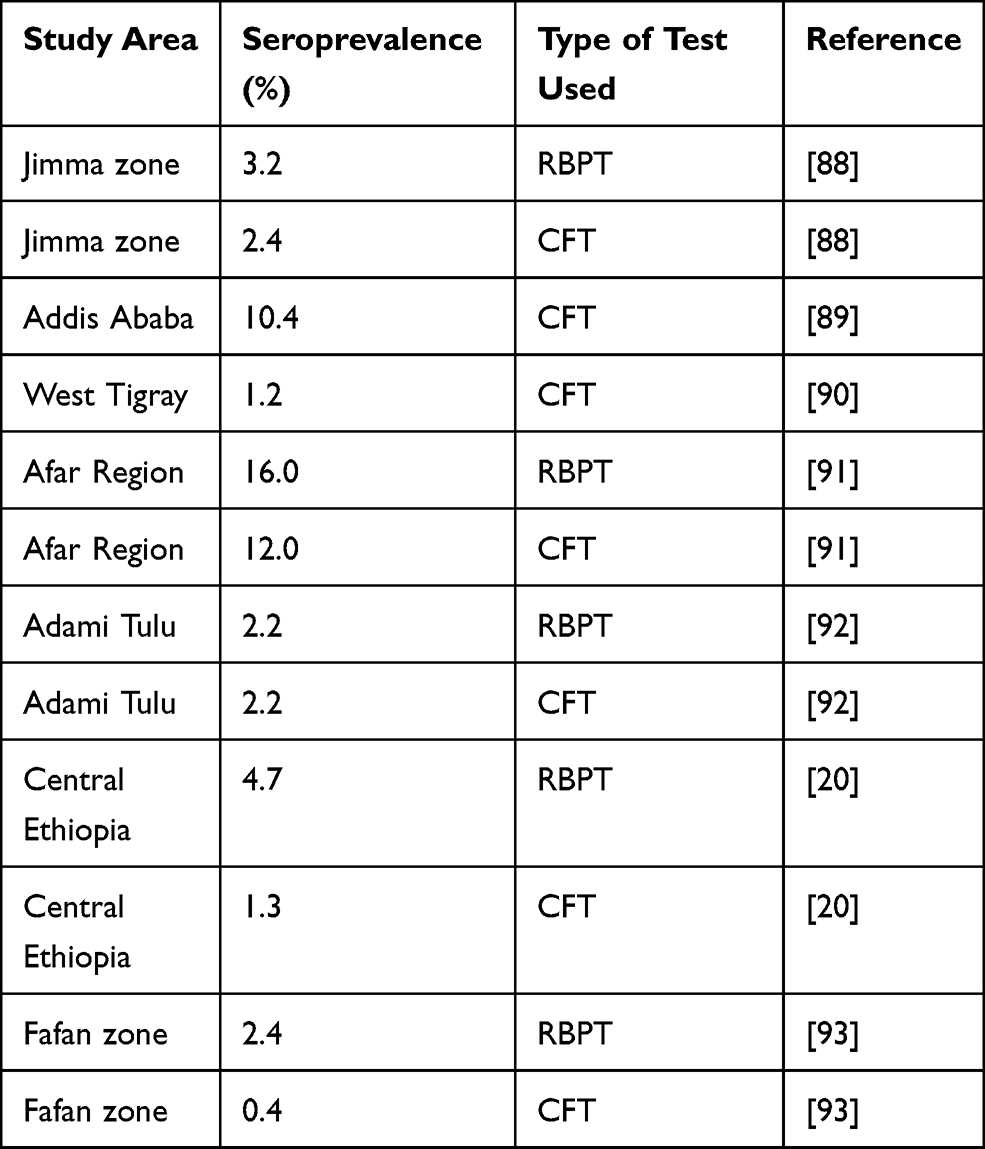 |
Table 2 Occurrence of Human Brucella Infection in Ethiopia |
Status of Brucella Infection in Ethiopia
Various investigations have shown that Brucella infection in cattle is common in Ethiopia, particularly in pastoral areas.16 Brucellosis has been assessed serologically in various locations around the country.5,94,95 A higher seroprevalence of Brucella infection was reported in intensive than in extensive production systems. The highest (50%) seroprevalence of Brucella was recorded in the Borena zone.96 In addition, a seroprevalence of 0.77% was reported in the Jimma zone94 and a prevalence of 1.7% was reported in an extensive production system.5,90 Another investigation, carried out in south and east Ethiopia, indicated that 3.5% of cattle were positive for Brucella antibodies.37 Several reports have shown that Brucella infection is prevalent in Ethiopia,9,20,21 as presented in Table 3.
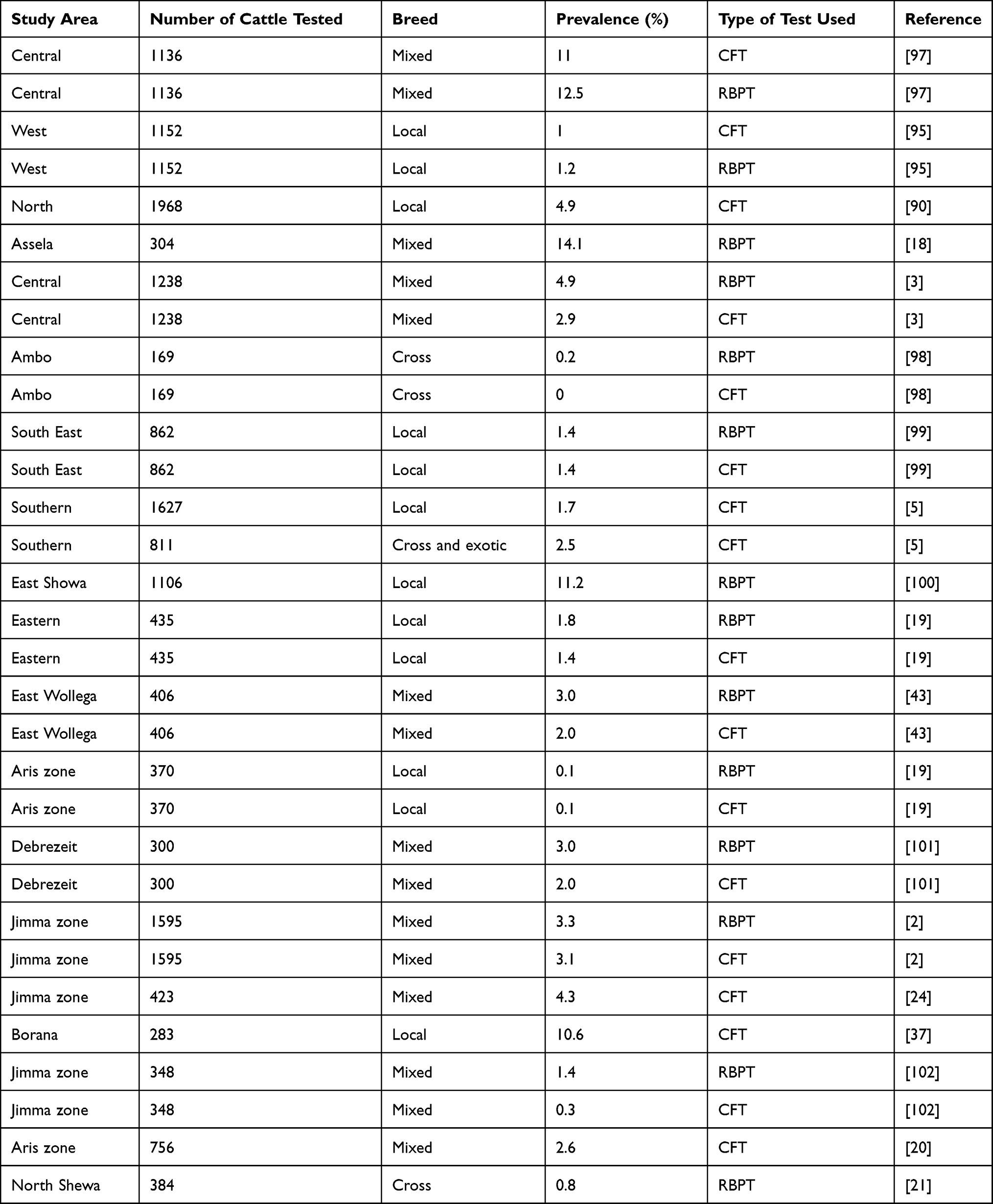 |
Table 3 Occurrence of Brucella Infection in Ethiopia |
Conclusion
Brucella infection is the major cause of production constraints in cattle and brucellosis is a serious zoonotic disease in Ethiopia. The occurrence of brucellosis in cattle is influenced by age, herd size, production system, and the agroecology of the area. Consumption of unpasteurized milk or its products and contact with infected cattle are the major methods of transmission of Brucella infection to humans. Brucellosis is a herd disease. The most suitable technique for managing Brucella infection is the vaccination of young female cattle. Therefore, it is important to implement applicable management methods and to increase public awareness about the transmission of brucellosis, and further research should be conducted on brucellosis in high-risk groups.
Disclosure
The author declared no conflicts of interest for this work.
References
1. Central Statistical Authority. Livestock and livestock characteristics, agricultural sample survey. Addis Ababa, Ethiopia. Stat Bull. 2017;2(583):9–13.
2. Ibrahim N, Belihu K, Lobago F, Bekana M. Sero-prevalence of bovine brucellosis and its risk factors in Jimma zone of Oromia Region, South-western Ethiopia. Trop Anim Health Prod. 2010;42:35–40. doi:10.1007/s11250-009-9382-z
3. Jergefa T, Kelay B, Bekana M, Teshale S, Gustafson H, Kindahl H. Epidemiological study of bovine brucellosis in three agro-ecological areas of central Oromia, Ethiopia. Rev Sci Tech. 2009;28(3):933–943. doi:10.20506/rst.28.3.1939
4. Asgedom H, Damena D, Duguma R. Seroprevalence of bovine brucellosis and associated risk factors in and around Alage district, Ethiopia. Springer Plus. 2016;5(851):1–8. doi:10.1186/s40064-016-2547-0
5. Asmare K, Asfaw Y, Gelaye E, Ayelet G. Brucellosis in extensive management system of Zebu cattle in Sidama Zone, Southern Ethiopia. Afr J Agric Res. 2010;5(3):257–263.
6. Tulu D, Deresa B, Begna F, Gojam A. Review of common causes of abortion in dairy cattle in Ethiopia. J Vet Med Anim Health. 2018;10(1):1–13. doi:10.5897/JVMAH2017.0639
7. OIE. Manual of diagnostic tests and vaccines for terrestrial animals. World Organisation for Animal Health. 2009;2(14):5–35.
8. FAO. Brucella melitensis in Eurasia and the Middle East. Rome: FAO Animal Production and Health Proceedings. No. 10; 2010.
9. Asfaw M, Ameni G, Kassa T, Tuli G, Arenas A, Mamo G. Seropositivity and risk factors for Brucella in dairy cows in Asella and Bishoftu towns, Oromia Regional State, Ethiopia. Afr J Microbiol Res. 2016;10(7):203–213. doi:10.5897/AJMR2015.7707
10. Robi DT. Epidemiology, economic and public health importance of small ruminant Brucella infection in Ethiopia. World J Vet Sci. 2020;2(1):1007.
11. Acha NP, Szyfres B. Brucellosis in zoonosis and communicable diseases common to humans and animals. 3rd edition. Washington, DC, USA: Pan American Health Organization; 2001:40–62.
12. Muma JB, Samui KL, Oloya J, Munyeme M, Skjerve E. Risk factors for brucellosis in indigenous cattle reared in livestock–wildlife interface areas of Zambia. Prev Vet Med. 2007;80:306–317. doi:10.1016/j.prevetmed.2007.03.003
13. Matope G, Bhebhe E, Muma JB, et al. Seroprevalence of brucellosis and its associated risk factors in cattle from smallholder dairy farms in Zimbabwe. Trop Anim Health Prod. 2011;43(5):975–982. doi:10.1007/s11250-011-9794-4
14. Mekonen H, Kalayou S, Kyule M. Serological survey of bovine brucellosis in Barka and Orado breeds (Bos indicus) of western Tigray, Ethiopia. Prev Vet Med. 2010;94:28–35. doi:10.1016/j.prevetmed.2009.12.001
15. Tolosa T, Bezabih D, Regassa F. Study on seroprevalence of bovine brucellosis, and abortion and associated risk factor. Bull Anim Health Prod Afr. 2010;58:236–247.
16. Berhe G, Belihu K, Asfaw Y. Seroepidemiological investigation of bovine brucellosis in the extensive cattle production system of Tigray Region of Ethiopia. Int J Appl Res Vet Med. 2007;5(2):65–71.
17. Tulu D, Deresa B, Begna F. Case-control study on risk factors associated with brucellosis in aborted cattle of Jimma zone, Ethiopia. Iran J Vet Sci Technol. 2020;11(2):27–36.
18. Deselegn TB, Gangwar SK. Seroprevalence study of bovine brucellosis in Assela government dairy farm of Oromia Regional State, Ethiopia. Int J Sci Nature. 2011;2(3):692–697.
19. Degefa T, Duressa A, Duguma R. Brucellosis and some reproductive problems of indigenous Arsi cattle in selected Arsi zones of Oromia Regional State, Ethiopia. Global Veterinary. 2011;7:45–53.
20. Tsegaye Y, Kyule M, Fikre lobago F. Seroprevalence and risk factors of bovine brucellosis in Arsi Zone, Oromia Regional State, Ethiopia. Am Sci Res J Eng Technol Sci. 2016;24(1):16–25.
21. Pal M, Lemu D, Worku S, Desta G. Sero-prevalence study of bovine brucellosis and reproductive problems in small-scale dairy farms of North Shewa, Ethiopia. Int J Livestock Res. 2016;6(9):1–10. doi:10.5455/ijlr.20160922081855
22. Radostits OM, Gay CC, Hinchcliff KW, Constable PD. Veterinary Medicine. A Text Book of Diseases of Cattle, Sheep, Pigs, Goats and Horses.
23. Godfroid J, Scholz HC, Barbier T, et al. Brucellosis at the animal/ecosystem/human interface at the beginning of the 21st century. Prev Vet Med. 2011;102:118–131. doi:10.1016/j.prevetmed.2011.04.007
24. Robi DT, Gelalcha BD. Epidemiological investigation of brucellosis in breeding female cattle under the traditional production system of Jimma zone in Ethiopia. Vet Animal Sci. 2020;9:100117. doi:10.1016/j.vas.2020.100117
25. OIE. Bovine brucellosis. In: OIE Manual of Diagnostic Tests and Vaccines for Terrestrial Animals. Pairs: Office International des Epizooties; 2012:616.
26. Quinn P, Markey B, Carter M, Donnely W, Lonard F, Maquire D. Brucella Species in Veterinary Microbiology and Microbial Disease. London: Blackwell Science; 2002:999–1000.
27. Bishop GC, Bosman PP, Herr S. Bovine brucellosis. In: Coetzer JAW, Thomson GR, Tustin RC, editors. Infectious Diseases of Livestock. Vol. 2. Cape Town, RSA: Oxford University Press; 1994:1053–1066.
28. Folitse RD, Boi-Kikimoto BB, Emikpe BO, Atawalna J. The prevalence of Bovine tuberculosis and Brucellosis in cattle from selected herds in Dormaa and Kintampo Districts, Brong Ahafo region, Ghana. Clin Microbiol. 2014;5(2):1–5.
29. Walker RL. Brucella. In: Hirsh DC, Zee YC, editors. Veterinary Microbiology. USA: Blackwell Science Inc; 1999:196–203.
30. Robinson A. Guidelines for coordinated human and animal brucellosis surveillance. FAO animal production and health paper; 2003:156.
31. Fugier E, Pappas G, Gorvel JP. Virulence factors in brucellosis implications for aetiopathogenesis and treatment. Expert Rev Mol Med. 2007;9:1–10. doi:10.1017/S1462399407000543
32. Memish A, Mah W. Brucellosis in laboratory workers at a Saudi Arabian hospital. Am J Infect Control. 2001;29:48–52. doi:10.1067/mic.2001.111374
33. Mcdermott JJ, Arimi SM. Brucellosis in sub-Saharan Africa: epidemiology, control and impact. Vet Microbiol. 2002;90:111–134. doi:10.1016/S0378-1135(02)00249-3
34. Gul ST, Khan A. Epidemiology and epizootology of brucellosis: a review. Pak Vet J. 2007;27:145–151.
35. Ashagrie T, Deneke Y, Tolosa T. Seroprevalence of caprine brucellosis and associated risk factors in South Omo Zone of Southern Ethiopia. Afr J Microbiol Res. 2011;5:1682–1685.
36. Borba MR, Stevenson MA, Goncalves VS, et al. Prevalence and risk-mapping of bovine brucellosis in Maranhao State, Brazil. Prev Vet Med. 2013;110:169–176. doi:10.1016/j.prevetmed.2012.11.013
37. Megersa B, Biffa D, Abunna F, Regassa A, Godfroid J, Skjerve E. Seroprevalence of brucellosis and its contribution to abortion in cattle, camel, and goat kept under pastoral management in Borana, Ethiopia. Trop Anim Health Prod. 2011;43:651–656. doi:10.1007/s11250-010-9748-2
38. Munoz PM, Boadella M, Arnal M, et al. Spatial distribution and risk factors of Brucellosis in Iberian wild ungulates. BMC Infect Dis. 2010;10:46. doi:10.1186/1471-2334-10-46
39. Talukder BC, Samad MA, Rahman AK. Comparative evaluation of commercial serodiagnostic tests for the seroprevalence study of brucellosis in stray dogs in Bangladesh. Bangladesh J Vet Med. 2012;9:79–83. doi:10.3329/bjvm.v9i1.11217
40. Coelho AM, Díez JG, Coelho AC. Brucelosis en pequeños rumiantes: efecto de la aplicación deun programa especial de vacunación en masa con REV-1. REDVET. Rev Electron de Vet. 2013;14:1–16.
41. Mai HM, Irons PC, Kabir J, Thompson PN. A large seroprevalence survey of brucellosis in cattle herds under diverse production systems in northern Nigeria. BMC Vet Res. 2012;8(144):1–14. doi:10.1186/1746-6148-8-144
42. Nahar A, Ahmed MU. Sero-prevalence study of brucellosis in cattle and contact human in Mymensingh district. Bangladesh J Vet Med. 2009;7:269–274. doi:10.3329/bjvm.v7i1.5071
43. Yohannes M, Mersha T, Degefu H, Tolosa T, Woyesa M. Bovine brucellosis: serological survey in Guto-Gida District, East Wollega Zone, Ethiopia. Global Veterinary. 2012;8:139–143.
44. Reviriego FJ, Moreno MA, Dominguez L. Risk factors for brucellosis seroprevalence of sheep and goat flocks in Spain. Prev Vet Med. 2000;44:167–173. doi:10.1016/S0167-5877(00)00108-2
45. Center for Food Security & Public Health. Bovine Brucellosis: Brucella Abortus. Ames, Iowa: College of Veterinary Medicine, Iowa State University; 2009.
46. Claudia AC, Diez JG, Coelho AM. Risk factors for Brucella spp. in domestic and wild animals. INTECH, World’s largest Science, Technology and Medicine Open Access book publisher; 2015:1–18.
47. Jackson R, Pite L, Kennard R, et al. Survey of the seroprevalence of brucellosis in ruminants in Kosovo. Vet Rec. 2004;154:747–751. doi:10.1136/vr.154.24.747
48. Smits HL. Brucellosis in pastoral and confined livestock: prevention and vaccination. Rev Sci Tech. 2013;32(1):219–228. doi:10.20506/rst.32.1.2200
49. Sammartino LE, Gil A, Elzer P. Capacity building for surveillance and control of bovine and caprine brucellosis. FAO Animal Production and Health Proceedings - AO/WHO/OIE Expert and Technical Consultation. Rome; 2006:55.
50. Kataria AK, Gahlot AK. Evaluation of oxidative stress in Brucella infected cows. J Stress PhysiolBiochem. 2010;6:2.
51. Islam MA, Khatun MM, Were SR, Sriranganathan N, Boyle SM. A review of Brucella seroprevalence among humans and animals in Bangladesh with special emphasis on epidemiology, risk factors and control opportunities. Vet Microbiol. 2013;166:317–326. doi:10.1016/j.vetmic.2013.06.014
52. Silva I, Dangolla A, Kulachelvy K. Seroepidemiology of Brucella abortus infection in bovids in Sri Lanka. Prev Vet Med. 2000;46:51–59. doi:10.1016/S0167-5877(00)00136-7
53. Talafhah AH, Lafi SQ, Al-Tarazi Y. Epidemiology of ovine brucellosis in Awassi sheep in Northern Jordan. Prev Vet Med. 2003;60:297–306. doi:10.1016/S0167-5877(03)00127-2
54. World Health Organization. Brucellosis in Humans and Animals. Geneva: World Health Organization; 2006:27–66.
55. Ruiz-Mesa D, Sanchez-Gonzalez J, Reguera M, Martin L, Lopez-Palmero S. Rose Bengal test: diagnostic yield and use for the rapid diagnosis of human brucellosis in emergency departments in endemic areas. Clin Microbiol Infect. 2005;11:221–225. doi:10.1111/j.1469-0691.2004.01063.x
56. Macmillan AP. Conventional serological tests. In: Animal Brucellosis. CRC Press Boca Raton; 1990:153–190.
57. Nielsen K, Ewalt DR. Bovine brucellosis. In: Manual of diagnostic tests and vaccines for terrestrial animals 2010. Paris: Office International Des Epizooties; 2010.
58. Etman RH, Barsoum SA, Ibrahim IG, El-Ashmawy WR, Abou-Gazia KA. Evaluation of efficacy of some serological tests used for diagnosis of brucellosis in cattle in Egypt using latent class analysis. Sokoto J Vet Sci. 2014;12(2):1–7. doi:10.4314/sokjvs.v12i2.1
59. Al Dahouk S, Nockler K, Scholz HC. Immunoproteomic characterization of Brucella abortus 1119-3 preparations used for the serodiagnosis of Brucella infections. J Immunol Methods. 2006;309:34–47. doi:10.1016/j.jim.2005.11.003
60. Nielsen K, Smith P, Yu W, et al. Serological discrimination by indirect enzyme immunoassay between the antibody response to Brucella spp. and Yersinia enterocolitica O: 9 in cattle and pigs. Vet Immunol Immunopathol. 2006;109:69–78. doi:10.1016/j.vetimm.2005.07.025
61. See W, Edward WH, Dauwalter S, et al. Yersinia enterocolitica: an unlikely cause of positive brucellosis test in Greater Yellowstone ecosystem Bison (Bison bison). J Wildl Dis. 2012;48(3):537–541. doi:10.7589/0090-3558-48.3.537
62. Adone R, Pasquali P. Epidemiological surveillance of brucellosis. Rev Sci Tech. 2013;32(1):199–205. doi:10.20506/rst.32.1.2202
63. Munoz PM, Marin CM, Monreal D, et al. Efficacy of several serological tests and antigens for diagnosis of bovine brucellosis in the presence of false-positive serological results due to Yersinia enterocolitica O:9. Clin Diagn Lab Immunol. 2005;12(1):141–151. doi:10.1128/CDLI.12.1.141-151.2005
64. Godfroid J, Nielsen K, Saegerman C. Diagnosis of brucellosis in livestock and wildlife. Croat Med J. 2010;51(4):296–305. doi:10.3325/cmj.2010.51.296
65. Nielsen K, Yu WL. Serological diagnosis of brucellosis. Section of biological medical sciences. Macedonia Acad Sci Arts. 2010;31(1):65–89.
66. Di Febo T, Luciani M, Portanti O, Bonfini B, Lelli R, Tittarelli M. Development and evaluation of diagnostic tests for the serological diagnosis of brucellosis in swine. Vet Ital. 2012;48:145–156.
67. Lim J, Kim H, Lee J, et al. Evaluation of recombinant 28 kDa outer membrane protein of B. abortus for the clinical diagnosis of bovine brucellosis in Korea. J Vet Med Sci. 2012;74:687–691. doi:10.1292/jvms.11-0512
68. Gall D, Nielsen K. Serological diagnosis of bovine brucellosis: a review of test performance and cost comparison. Rev Sci Tech. 2004;23:989–1002.
69. Poiester FP, Nielsen K, Samartino LE, Yu WL. Diagnosis of Brucellosis. Open Vet Sci J. 2010;4:46. doi:10.2174/1874318801004010046
70. Diaz R, Casanova A, Ariza J, Moriyon I. The rose Bengal test in human Brucellosis: a neglected test for the diagnosis of a neglected disease. PLoS Negl Trop Dis. 2011;5(4):950. doi:10.1371/journal.pntd.0000950
71. Kangethe EK, Arimi SM, Omore AO, et al.. The prevalence of antibodies to Brucella abortus in marketed milk in Kenya and its public health implications.
72. Senein A, Abdelgadir AE. Serological survey of cattle brucellosis in Eldein, eastern Darfur, Sudan. Afr J Microbiol Res. 2012;6(31):6086–6090.
73. Bwala DG, McCrindle C, Fasina OF, Ljagbone L. Abattoir characteristics and sero-prevalence of bovine brucellosis in cattle slaughtered at Bodija Municipal Abattoir, Ibadan, Nigeria. J Vet Med Anim Health. 2015;7(5):164–168. doi:10.5897/JVMAH2015.0370
74. Swai ES, Schoonman L. The use of rose Bengal plate test to assess cattle exposure to Brucella infection in traditional and smallholder dairy production systems of Tanga Region of Tanzania. Vet Med Int. 2010;2010:8. doi:10.4061/2010/837950
75. Omer KM, Assefaw T, Skjerve E, Tekleghiorghis T, Woldehiwet Z. Prevalence of antibodies to Brucella species risk factor related to high risk occupational groups in Eritrea. Epidemiol Infect. 2002;129:85–91. doi:10.1017/S0950268802007215
76. Makita K, Eric FM, Waiswa C, Kaboyo W, Mark EC, Susan WC. Spatial epidemiology of hospital-diagnosed brucellosis in Kampala, Uganda. Int J Health Geogr. 2011;10:52. doi:10.1186/1476-072X-10-52
77. Unger F, Münstermann S, Goumou A, Apia CN, Konte M, Hempen M. Risk associated with bovine brucellosis in selected study herds and market places in four countries of West Africa, animal health working paper 2. International Trypanotolerance Centre, Banjul, the Gambia; 2003.
78. Shey-Njila O, Nya E, Zoli PA, Walravens K, Godfroid J, Geerts S. Serological survey of bovine brucellosis in Cameroon. Rev Elev Med Vet Pays Trop. 2005;58(3):139–143.
79. Mufinda FC, Fernando SB, Carla SN. Prevalence and factors associated with cattle brucellosis in animal Herds of the Namibe Province in Angola. Alex J Vet Sci. 2015;47:7–17. doi:10.5455/ajvs.188809
80. Madut NA, Muwonge A, Nasinyama GW, et al. The sero-prevalence of brucellosis in cattle and their herders in Bahr el Ghazal region, South Sudan. PLoS Negl Trop Dis. 2018;12(6):e0006456. doi:10.1371/journal.pntd.0006456
81. Mantur BG, Amarnath SK, Shinde R. Review of clinical and laboratory features of human brucellosis. Indian J Med Microbiol. 2007;25:188–202. doi:10.1016/S0255-0857(21)02105-8
82. Poester FP, Samartino LE, Santos RL. Pathogenesis and pathobiology of brucellosis in livestock. Sci Tech Rev OIE. 2013;32(1):105–115. doi:10.20506/rst.32.1.2193
83. Yohannes M, Degefu H, Tolosa T, Belihu K, Cutler R, Cutler S. Distribution of brucellosis in different regions in Ethiopia. Afr J Microbiol Res. 2013;7:1150–1157. doi:10.5897/AJMR12.738
84. Habtamu T, Richard B, Dana H, Kassaw AT. Camel brucellosis: its public health and economic impact in pastoralists, Mehoni District, Southeastern Tigray, Ethiopia. J Microbiol Res. 2015;5(5):149–156.
85. Weidmann H. Survey of means now available for combating brucellosis in cattle in tropics. Tubmgen, Georg Hauser, Metzingen, Germany: Institute for Scientific Cooperation; 1991;98–111.
86. Corbel MJ. Brucellosis in Humans and Animals. Geneva, Switzerland: World Health Organization; 2006.
87. Dean AS, Crump L, Greter H, Hattendorf J, Schelling E, Zinsstag J. Clinical manifestations of human brucellosis: a systematic review and meta-analysis. PLoS Negl Trop Dis. 2012;6:e1929. doi:10.1371/journal.pntd.0001929
88. Tolosa T. Prevalence study of bovine brucellosis and its public health significance in selected sites of Jimma Zone, Western Ethiopia. A Thesis submitted to the Faculty of Veterinary Medicine, Addis Ababa University in partial fulfillment of the requirements for the Degree of Master of Science in Tropical Veterinary Medicine. 2004:4–29.
89. Kassahun J, Yimer E, Geyid A, et al. Seroprevalence of brucellosis in occupationally exposed people in Addis Ababa, Ethiopia. Ethiop Med J. 2006;44:245–252.
90. Haileselassie M, Kalayou S, Kyule M, Asfaha M, Belihu K. Effect of Brucella infection on reproduction conditions of female breeding cattle and its public health significance in Western Tigray, Northern Ethiopia. Vet Med Int. 2011;201:7.
91. Sisay WZ, Mekonnen H. Seroprevalence of Brucella infection in camel and its public health significance in selected districts of afar region. J Environment Occupat Health. 2012;1(2):91–98.
92. Tibesso G, Ibrahim N, Tolosa T. Sero prevalence of bovine and human brucellosis in Adami Tulu, Central Ethiopia. World Appl Sci J. 2014;31:776–780.
93. Lakew A, Hiko A, Abraha A, Mengistu HS. Sero-prevalence and community awareness on the risks associated with Livestock and Human brucellosis in selected districts of Fafan Zone of Ethiopian-Somali National Regional State. Vet Animal Sci. 2019;7:100047. doi:10.1016/j.vas.2019.100047
94. Tolosa T, Regassa F, Belihu K. Seroprevalence study of Bovine Brucellosis in Extensive Management System in Selected Sites of Jimma Zone, Western Ethiopia. Bull Anim Health Prod Afr. 2008;56:25–37. doi:10.4314/bahpa.v56i1.32823
95. Adugna KE, Agga GE, Zewde G. Seroepidemiological survey of bovine brucellosis in cattle under a traditional production system in western Ethiopia. Rev Sci Tech. 2013;32(3):1–20.
96. Alem W, Solomon G (2002). A retrospective sero-epidemiology study of bovine brucellosis in different production systems in Ethiopia.
97. Kebede T, Ejeta G, Ameni G. Seroprevalence of bovine brucellosis in smallholder farms in central Ethiopia (Wuchale-Jida district). Rev Med Vet. 2008;159(1):3–9.
98. Bashitu L, Afera B, Tuli G, Aklilu F. Sero-prevalence study of bovine brucellosis and its associated risk factors in Debrebirhan and Ambo towns. J Adv Dairy Res. 2015;3:131. doi:10.4172/2329-888X.1000131
99. Gumi B, Firdessa R, Yamuah L, et al. Seroprevalence of Brucellosis and Q-fever in Southeast Ethiopian pastoral livestock. J Vet Sci Med Diagnosis. 2013;2:1. doi:10.4172/2325-9590.1000109
100. Dinka H, Chala R. Seroprevalence study of bovine brucellosis in pastoral and agro-pastoral areas of East Showa Zone, Oromia Regional State, Ethiopia. Am Eurasian J Agric Environ Sci. 2009;6(5):508–512.
101. Alemu F, Admasu P, Feyera T, Niguse A. Seroprevalence of bovine brucellosis in Eastern Showa, Ethiopia. Acad J Animal Dis. 2014;3(3):27–32.
102. Bashahun GD, George WN, Benti DG. Seroprevalence and risk factors for brucellosis in cattle in selected districts of Jimma zone, Ethiopia. Trop Anim Health Prod. 2015;47(7):1–7. doi:10.1007/s11250-014-0709-z
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.