Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Body Mass Index and Lung Function in Hospitalized Severe AECOPD Patients: Investigating Nonlinear Associations and the Role of Hemoglobin
Authors Zhang C ![]() , Ling W, Pan H, Bai R, He L
, Ling W, Pan H, Bai R, He L
Received 6 February 2025
Accepted for publication 18 April 2025
Published 1 May 2025 Volume 2025:20 Pages 1309—1320
DOI https://doi.org/10.2147/COPD.S521112
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Fanny Wai San Ko
Cong Zhang,1 Wenhao Ling,1 He Pan,2 Rui Bai,3 Li He1
1Department of Respiratory and Critical Care Medicine, Jingzhou Hospital Affiliated to Yangtze University, Jingzhou, Hubei, People’s Republic of China; 2Department of Laboratory Medicine, Jingzhou Hospital Affiliated to Yangtze University, Jingzhou, Hubei, People’s Republic of China; 3Department of Pulmonary Oncology, Zhongnan Hospital of Wuhan University, Wuhan, Hubei, People’s Republic of China
Correspondence: Li He, Department of Respiratory and Critical Care Medicine, Jingzhou Hospital Affiliated to Yangtze University, Jingzhou, People’s Republic of China, Email [email protected] Rui Bai, Department of Pulmonary Oncology, Zhongnan Hospital of Wuhan University, Wuhan, People’s Republic of China, Email [email protected]
Background: Chronic obstructive pulmonary disease (COPD) is a leading cause of global morbidity and mortality. Patients hospitalized with severe acute exacerbations of COPD (AECOPD) represent a high-risk group with poor outcomes and accelerated lung function decline. Body mass index (BMI) shows inconsistent associations with lung function across populations, and its role in AECOPD remains unclear. Understanding this relationship may improve clinical management. Hemoglobin (Hb), essential for oxygen transport, may further influence this association through physiological mechanisms. This study aimed to explore the relationship between BMI and lung function in hospitalized patients with severe AECOPD and to assess whether BMI influences length of hospital stay (LOHS), while evaluating the potential modifying role of Hb.
Methods: A retrospective, single-center cross-sectional study was conducted among 579 patients hospitalized for severe AECOPD from 2021 to 2023. Data on BMI, lung function, Hb levels, and LOHS were collected. Nonlinear and threshold effect analyses were used to explore associations between BMI and lung function or LOHS. Subgroup analyses assessed the modifying effect of Hb.
Results: BMI exhibited a nonlinear positive association with FEV1, FVC, FEV1% predicted, and FVC% predicted. Thresholds were identified at 25.39 kg/m² for FEV1, 26.23 kg/m² for FEV1% predicted, 21.67 kg/m² for FVC, and 22.19 kg/m² for FVC% predicted. The association was more pronounced in patients with higher Hb levels. No significant association was found between BMI and LOHS, suggesting that other factors such as infection severity, comorbidities, or treatment strategies may may exert greater influence.
Conclusion: A nonlinear, inverse L-shaped association was observed between BMI and lung function, further modified by Hb levels. These findings highlight the importance of individualized treatment and stratification strategies in severe AECOPD. Future longitudinal studies are needed to validate these observations.
Keywords: BMI, lung function, AECOPD, hemoglobin, LOHS
Introduction
Chronic obstructive pulmonary disease (COPD) is a heterogeneous respiratory condition and remains one of the three leading causes of death globally.1,2 Acute exacerbations of COPD (AECOPD) significantly impair patients’ health status and long-term prognosis,3–5 contributing to the progressive decline in lung function—particularly in those experiencing severe episodes that require hospitalization.6,7 Patients hospitalized with severe AECOPD represent a high-risk phenotype that warrants urgent clinical attention and individualized management. Obesity has become a global health burden and is known to affect pulmonary function in both healthy individuals and patients with COPD.8,9 It is also associated with increased healthcare costs among patients with COPD.10 Body mass index (BMI), the most widely used clinical indicator of obesity, has demonstrated complex and inconsistent associations with lung function in both general populations and individuals at risk for COPD. Some studies have reported an inverted U-shaped relationship between BMI and lung function,11,12 while others have shown negative,13,14 null,15 or even positive associations.16,17 In patients with stable COPD, higher BMI has been positively correlated with forced expiratory volume in 1 second as a percentage of the predicted (FEV1% predicted).18 In BMI-stratified analyses, underweight patients exhibited significantly lower FEV1, forced vital capacity (FVC), and FEV1/FVC ratio, whereas overweight or obese individuals tended to have higher values for these parameters.19 Furthermore, a higher BMI may confer protection against accelerated lung function decline in patients with COPD.20 Although observational studies have shown varying associations between BMI and lung function, the underlying physiological mechanisms remain incompletely understood. During acute exacerbations of COPD, patients experience increased respiratory demand, systemic inflammation, and metabolic stress. BMI may affect lung function through multiple pathophysiological pathways, including altered respiratory mechanics, systemic inflammation, muscle wasting, impaired gas exchange, and metabolic dysregulation.21–24 These mechanisms may be amplified in severe AECOPD, potentially contributing to variations in clinical presentation and outcomes. Yet, the relationship between BMI and lung function in the context of severe AECOPD remains underexplored. Collectively, these mechanisms may underlie the so-called “obesity paradox” in COPD, wherein a higher BMI has been paradoxically associated with better lung function and improved survival, while lower BMI correlates with an increased risk of mortality.25–27
Hemoglobin (Hb) plays a critical role in oxygen transport and has increasing clinical relevance in the context of COPD. Anemia is common among patients with COPD and has been associated with reduced exercise capacity, poorer quality of life,28 and increased in-hospital mortality.29,30 Conversely, elevated Hb levels may reflect a compensatory response to chronic hypoxemia and have been linked to lower dyspnea scores, fewer exacerbations, and improved survival outcomes.31,32 However, excessive erythrocytosis may contribute to adverse consequences such as pulmonary hypertension and cor pulmonale, both of which are indicators of poor prognosis.33 Given that both BMI and Hb are closely related to metabolic demand, and respiratory function, their interaction may jointly influence the severity and clinical outcomes of COPD. The bidirectional effects of Hb—beneficial or harmful depending on its level—may modify the association between BMI and clinical outcomes, including lung function. Despite these potential interactions, few studies have investigated the combined effects of BMI and Hb in patients hospitalized for severe AECOPD. In this population, prolonged length of stay has been associated with increased healthcare utilization and poorer clinical outcomes.34,35 However, the relationship between BMI and LOHS remains poorly understood.
Therefore, this study aimed to investigate the association between BMI and lung function parameters in patients hospitalized for severe AECOPD, and to assess whether BMI is associated with LOHS. In addition, the potential modifying effect of Hb on these associations was explored. Understanding these relationships may help clarify the interplay between metabolic and hematologic factors in severe AECOPD and offer insights for improving nutritional assessment, individualized treatment strategies, and patient stratification. Potential confounding factors, including smoking status, medication use, inflammatory and biochemical markers, and comorbidities, were also considered in the analysis to ensure the robustness of the findings.
Methods
Study Population
This single-center cross-sectional study retrospectively collected data on 855 inpatients with severe AECOPD from Jingzhou Central Hospital between January 2021 and December 2023. Inclusion criteria were as follows:
- a prior diagnosis of COPD, defined as a post-bronchodilator FEV1/FVC ratio <0.7 during the stable phase, and (ii) severe AECOPD was the primary discharge diagnosis for the current hospitalization. Exclusion criteria included common respiratory diseases such as bronchial asthma, bronchiectasis, interstitial pneumonia, and bronchopulmonary malignancies. Patients with missing BMI or pulmonary function parameters were also excluded. Finally, 579 patients were included in the final analysis (Figure 1).
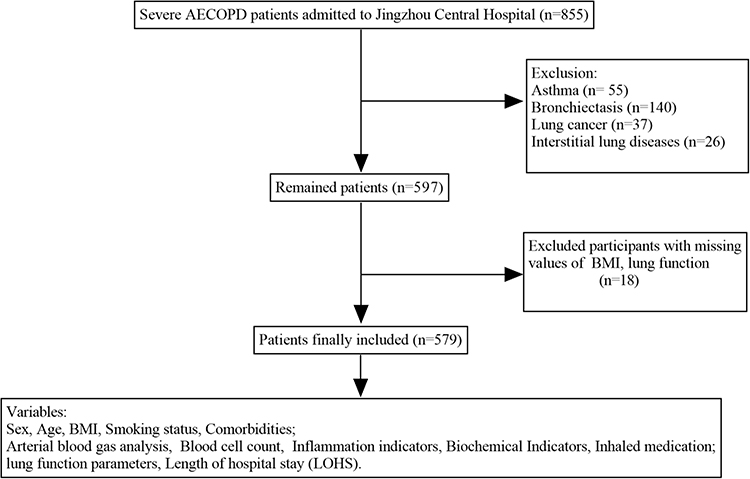 |
Figure 1 Flowchart depicting the selection of study participants. |
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Jingzhou Central Hospital (Approval No: 2022-058-01). The requirement for individual informed consent was waived due to the retrospective nature of the study. All patient data were anonymized before analysis, and strict confidentiality was maintained throughout, in compliance with institutional and national data protection regulations.
Data Collection
For all patients included in the analysis, the following variables were collected through the electronic medical record system: Demographic characteristics, including age, sex, and smoking status (Never-smoker/Ex-smoker/Current-smoker).36 Comorbidities, such as hypertension, diabetes, coronary artery disease, and chronic kidney disease. Blood test results at admission, including arterial blood gas parameters (PH, PaCO2, and oxygenation index [OI]), complete blood counts, Hb levels, fibrinogen, D-Dimer, C-reactive protein (CRP), and biochemical markers (albumin, blood urea nitrogen, and creatinine), Pro B-type Natriuretic Peptide (ProBNP), Inhalation therapy regimens at admission (LAMA/ICS+LABA/LABA+LAMA/ICS+LABA+LAMA), and LOHS. BMI was calculated using height (cm) and weight (kg) recorded at the time of admission. Pulmonary function parameters—including FEV1 (L/min), FEV1% predicted, FVC (L/min), FVC % predicted, and FEV1/FVC ratio—were measured during a clinically stable period, defined as either during hospitalization once the acute episode had resolved, or within approximately one month after admission.
Statistical Analysis
Continuous variables were presented as mean ± standard deviation (SD) or median with interquartile range (IQR), as appropriate, while categorical variables were expressed as counts and percentages. The Kruskal–Wallis test and chi-square test were used to compare patient characteristics across BMI quartiles. To assess the linear association between BMI and lung function parameters or LOHS, multiple linear regression models were applied. Three models were constructed: Model 1 was unadjusted; Model 2 was adjusted for sex, age, and smoking status; and Model 3 was adjusted for all covariates. Covariates known or suspected to be associated with BMI, lung function, or LOHS were selected based on clinical relevance and prior literature. These included demographic variables (age, sex, smoking status), comorbidities (hypertension, diabetes), inflammatory and biochemical markers (lymphocyte count, eosinophil count, CRP, D-dimer, fibrinogen, and albumin), and inhalation therapy at admission. Covariates were further refined using a stepwise selection approach. βcoefficients and 95% confidence intervals (CIs) were reported to quantify effect sizes for each model. Interaction tests were performed to assess whether the associations between BMI and clinical outcomes varied across subgroups defined by Hb levels. A generalized additive model (GAM) was employed to explore potential nonlinear relationships. To assess threshold effects of BMI on lung function and LOHS, a two-piecewise linear regression model was applied. The inflection point was determined using a recursive algorithm by comparing models with different candidate thresholds. Model fit was evaluated based on log-likelihood values, and the optimal threshold was selected according to the maximum likelihood estimate. A likelihood ratio test was conducted to compare the segmented model with a single-line linear model. To assess the robustness of the results, sensitivity analyses were performed. Missing values were handled using multiple imputation by chained equations (MICE), implemented via the “mice” package in R. Five imputed datasets were generated. Variables with missing data included smoking status (0.5%), PaCO2 (20.6%), lymphocyte count (2.4%), eosinophil count (3.3%), CRP (8.9%), fibrinogen (8.3%), D-dimer (5.4%), albumin (3.5%), and inhalation therapy regimen (3.1%). All variables included in the primary regression models were used as predictors in the imputation model. All statistical analyses were conducted using R software (version 4.2.0) and EmpowerStats (version 4.1). A two-sided p-value of <0.05 was considered statistically significant.
Results
Clinical Characteristics of Patients During Severe AECOPD
This retrospective study included 579 patients diagnosed with AECOPD who met the predefined inclusion and exclusion criteria. Baseline characteristics are summarized in Supplementary Table 1. The mean age was 69.48 ± 8.64 years, and the mean BMI was 22.15 ± 3.64 kg/m². Of the included patients, 487 (84.1%) were male and 92 (15.9%) were female. A history of smoking was reported in 463 patients (80.0%), and hypertension was the most common comorbidity, present in 219 patients (37.8%). Inhaled triple therapy was used by 315 patients (56.2%). The median LOHS was 8 days. Median lung function parameters were as follows: FEV1, 1.01 L/min; FEV1% predicted, 44.00%; FVC, 2.29 L/min; FVC % predicted, 74.00%; and FEV1/FVC ratio, 47.79%.
Differences in baseline characteristics across BMI quartiles were also examined (Table 1). Smoking status and inhaled medication regimens varied significantly among BMI groups. Patients in higher BMI quartiles showed a greater proportion of comorbidities, as well as significantly higher lymphocyte counts, Hb levels, red blood cell (RBC) counts, albumin, uric acid, and creatinine levels. Higher BMI was also associated with better lung function parameters and lower PaCO2 levels.
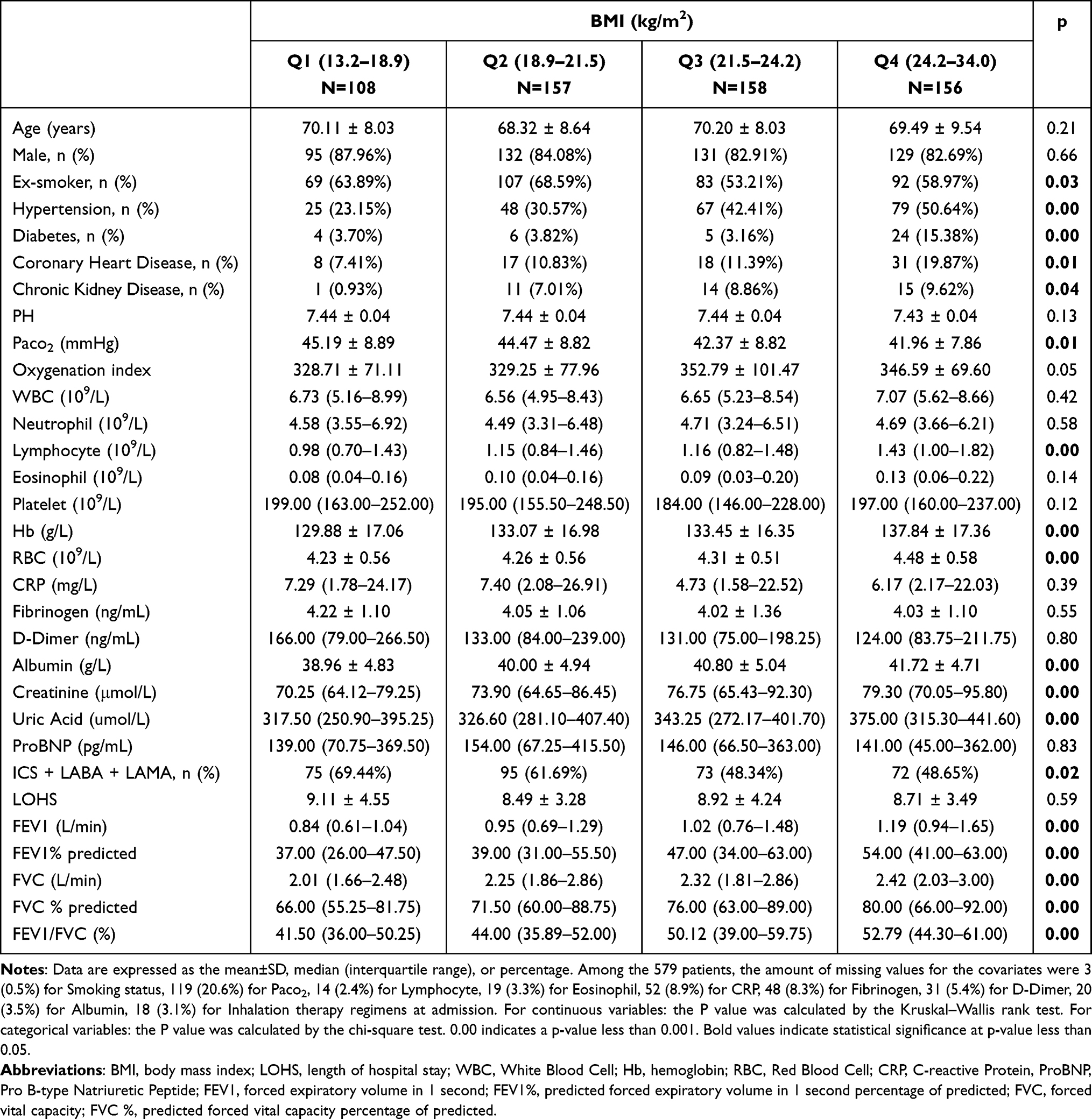 |
Table 1 Baseline Characteristics According to the Quartiles of the BMI |
Association Between BMI and Impaired Lung Function
In this study, the unadjusted linear association (Model 1) revealed a positive correlation between BMI and lung function parameters, with β coefficients of 0.04 (95% CI: 0.03, 0.05) for FEV1, 1.46 (95% CI: 1.01, 1.90) for FEV1% predicted, 0.03 (95% CI: 0.02, 0.05) for FVC, 1.07 (95% CI: 0.60, 1.55) for FVC% predicted, and 0.94 (95% CI: 0.69, 1.20) for FEV1/FVC. This positive association remained consistent in both Model 2 and Model 3. In Model 3, which adjusted for age, sex, smoking status, hypertension, diabetes, Paco2, lymphocyte count, eosinophil count, fibrinogen, D-dimer, albumin, CRP, and inhaled medication use, the association persisted with β coefficients of 0.02 (95% CI: 0.01, 0.04) for FEV1, 0.78 (95% CI: 0.29, 1.26) for FEV1% predicted, 0.02 (95% CI: 0.00, 0.04) for FVC, 0.70 (95% CI: 0.10, 1.29) for FVC% predicted, and 0.55 (95% CI: 0.24, 0.85) for FEV1/FVC. Detailed results are shown in Table 2. However, piecewise regression and smoothing curves revealed a nonlinear positive association between BMI and lung function parameters, except for FEV1/FVC (Figure 2). Threshold effect analysis identified turning points as follows: 25.39 kg/m² for FEV1, 26.23 kg/m² for FEV1% predicted, 21.67 kg/m² for FVC, and 22.19 kg/m² for FVC% predicted. Below these thresholds, a positive correlation was observed, with β coefficients of 0.04 (95% CI: 0.02, 0.05) for FEV1, 1.21 (95% CI: 0.60, 1.82) for FEV1% predicted, 0.09 (95% CI: 0.04, 0.13) for FVC, and 2.28 (95% CI: 1.08, 3.47) for FVC% predicted. No significant associations were observed above these thresholds. Results are summarized in Table 3.
 |
Table 2 Association of BMI with Lung Function Parameters and Subgroup Analysis by Hemoglobin Levels |
 |
Table 3 Threshold Effect Analysis of BMI on Lung Function Parameters and Its Clinical Relevance |
 |
Figure 2 Associations between BMI and pulmonary function parameters in all patients with AECOPD. (Left panel) A threshold, nonlinear association between BMI and FEV1, FEV1% predicted, FVC, and FVC% predicted was identified using a generalized additive model (GAM). The solid red line represents the smooth curve fit between variables, while the black dashed lines indicate the 95% confidence interval. (Right panel) Association between BMI and lung function, stratified by hemoglobin levels. The red line represents the Hblow-middle subgroup (combined first two terciles of hemoglobin levels), and the blue line represents the Hbhigh subgroup (third tercile of hemoglobin levels). All models were adjusted for age, sex, smoking status, hypertension, diabetes, PaCO2, lymphocyte count, eosinophil count, CRP, fibrinogen, D-Dimer, albumin, and inhalation therapy regimens at admission. |
Hb was stratified into tertiles—Hblow (range: 42.0–123.0 g/L), Hbmiddle (124.0–138.0 g/L), and Hbhigh (139.0–174.0 g/L)—to assess the association between BMI and pulmonary function within each group, and interaction tests were performed. In the fully adjusted model (Model 3), no significant associations were observed in the Hblow and Hbmiddle groups. However, in the Hbhigh group, BMI was significantly positively associated with all pulmonary function parameters (Supplementary Table 2). Subsequently, the Hblow and Hbmiddle tertiles were combined and compared with the Hbhigh group in a secondary stratified analysis. In Model 3, BMI remained unassociated with lung function in the Hblow–middle subgroup (mean ± SD: 123.70 ± 13.24), whereas in the Hbhigh subgroup (mean ± SD: 149.59 ± 8.19), BMI was positively associated with lung function, with β coefficients of 0.05 (95% CI: 0.03–0.06) for FEV1; 1.40 (95% CI: 0.70–2.11) for FEV1% predicted; 0.05 (95% CI: 0.02–0.07) for FVC; 0.97 (95% CI: 0.12–1.82) for FVC% predicted; and 1.03 (95% CI: 0.57–1.49) for FEV1/FVC (Table 2). Smoothing curves stratified by Hb level further supported these findings and are presented in Figure 2.
Association Between BMI and Length of Hospital Stay
The association between BMI and LOHS was assessed using both a multiple linear regression model (Model 1) and a piecewise linear regression model (Model 2). After adjusting for all confounding variables, neither model demonstrated a significant association between BMI and LOHS (Table 4).
 |
Table 4 Association of the BMI with LOHS |
Taken together, across all regression analyses—including those evaluating pulmonary function parameters and LOHS—the results remained consistent after multiple imputation of missing covariates (Supplementary Tables 3 and 4), further supporting the robustness of our findings. Imputed variables included PaCO2, CRP, fibrinogen, D-dimer, albumin, lymphocyte and eosinophil counts, smoking status, and inhalation therapy regimen.
Discussion
In the present study, we identified a potential inverse L-shaped association between BMI and lung function parameters, including FEV1, FEV1% predicted, FVC, and FVC% predicted, in patients hospitalized for severe AECOPD. In contrast, BMI was positively and linearly associated with the FEV1/FVC ratio. No significant association was observed between BMI and LOHS. Notably, the association between BMI and lung function appeared more evident among individuals with higher Hb levels.
The relationship between BMI and COPD is complex. Low BMI is a known risk factor for COPD development and is negatively associated with lung function.37 However, studies on the association between high BMI, lung function, and COPD have yielded inconsistent results due to variations in populations, ethnicities, and the number of confounding factors controlled in observational studies.11–17 With respect to COPD prognosis, existing evidence suggests that patients with higher BMI tend to have more favorable outcomes, including improved survival.26,38,39 Several prior studies have also reported a positive association between BMI and lung function in patients with COPD,18,19 which is consistent with the findings of our study. However, using nonlinear models, we further observed that BMI exhibited a nonlinear association with several lung function parameters, characterized by an inverse L-shaped pattern. In contrast, prior studies in healthy individuals and populations at high risk for COPD have reported an inverted U-shaped relationship between BMI and lung function.11,12 Several factors may explain the inverse L-shaped relationship observed in our study. First, lung function gradually declines as COPD progresses, and in patients hospitalized for acute exacerbations, lung function is often already severely impaired. This may result in a plateau effect, where further increases in BMI do not yield substantial changes in pulmonary function.40 Previous studies have shown that higher BMI is associated with a slower rate of lung function decline in COPD patients;20 thus, once BMI reaches a certain level, further increases may no longer lead to significant improvements or deterioration in lung function. Second, BMI is not a reliable indicator of nutritional status in COPD. Rather, it reflects a complex interplay of systemic inflammation, muscle wasting, and metabolic dysregulation,21,22 which may obscure or modify its association with lung function. Additionally, BMI does not distinguish between fat and lean mass, nor does it capture central obesity, which has a stronger correlation with adverse cardiopulmonary outcomes.41 Furthermore, patients with higher BMI have been reported to exhibit better respiratory endurance and a lower frequency of severe exacerbations.42,43 Since each exacerbation accelerates lung function decline, reduced exacerbation frequency may help mitigate the potential detrimental effects of higher BMI on lung function. Our study also found no significant association between BMI and LOHS, which is consistent with previous findings.44 LOHS may reflect both disease severity and a range of acute clinical factors—including pathogen virulence, degree of airway inflammation, comorbidity burden, and in-hospital management strategies—rather than chronic factors such as BMI. In addition, non-clinical influences, such as discharge policies, healthcare resource availability, and patient or family preferences, may further confound the relationship between BMI and LOHS.45,46
Our study revealed that Hb levels may modify the association between BMI and lung function. Moderate elevations in Hb may enhance oxygen transport efficiency, thereby improving systemic oxygen delivery even when pulmonary function is compromised. This compensatory mechanism may alleviate tissue hypoxia and reduce the ventilatory burden. Additionally, elevated Hb levels may improve oxygen diffusion gradients and maintain arterial oxygen content, which can support respiratory muscle function and delay fatigue, thereby contributing to better pulmonary performance.28,47 Prior studies have demonstrated that COPD patients with anemia tend to have reduced lung function,28 whereas those with higher Hb levels show better FEV1% predicted values.32 Several pathophysiological mechanisms may explain the observed interaction between BMI and Hb in patients with severe AECOPD. First, individuals with higher BMI may have better nutritional and metabolic reserves, which could augment the compensatory effects of elevated Hb, thereby amplifying its beneficial influence on lung function. Second, although elevated BMI may confer both beneficial effects—such as improved respiratory muscle strength and greater energy reserves—and adverse effects, including increased low-grade systemic inflammation,48 higher Hb levels may help shift this balance toward a net physiological benefit. Specifically, Hb has been shown to exert anti-inflammatory and antioxidant effects,49 which may attenuate the inflammation associated with higher BMI and enhance its positive effect on lung function. Third, patients with higher BMI are more prone to hypoventilation and CO2 retention, which can impair respiratory function and acid–base homeostasis. Elevated Hb levels may enhance the body’s buffering capacity for CO2 and help maintain acid–base balance,50 thus mitigating the respiratory burden associated with excess weight. This compensatory mechanism may help preserve lung function and strengthen the positive impact of BMI in individuals with higher Hb levels. In contrast, among those with lower Hb levels, the absence of such compensatory mechanisms may allow the detrimental effects of obesity to predominate, attenuating the overall benefit of increased BMI.
The identification of an inverse L-shaped relationship between BMI and lung function has important clinical implications. Our findings suggest that while increases in BMI may improve lung function in underweight or normal-weight patients with severe AECOPD, this benefit plateaus beyond a certain threshold. This underscores the need for individualized nutritional management, particularly in patients with low BMI, who may derive the greatest benefit from targeted interventions such as nutritional supplementation, pulmonary rehabilitation, or anabolic therapy. In contrast, excessive weight gain in already overweight patients may confer limited pulmonary benefit and may increase the risk of cardiovascular or metabolic complications. These findings highlight the importance of optimizing—not merely increasing—BMI as part of a comprehensive COPD management strategy. Moreover, our study is among the first to demonstrate that Hb levels may modify the positive association between BMI and lung function in patients with severe AECOPD. This interaction suggests that the beneficial effects of higher BMI on lung function are more pronounced in individuals with elevated Hb levels, as previously discussed. These results provide new insight into the obesity paradox in COPD and emphasize the potential value of incorporating hematologic markers into clinical risk assessment and management. Further studies are warranted to validate this interaction and to explore whether coordinated modulation of BMI and Hb could improve clinical outcomes.
This study has several limitations. First, its retrospective, cross-sectional, single-center design limits both causal inference and the generalizability of the findings. Second, missing data on certain covariates may have affected the results, although multiple imputation was used to reduce potential bias. Third, although the interaction between BMI and Hb levels reached statistical significance, the direction of association between BMI and lung function was consistent across Hb subgroups. Additionally, no formal correction for multiple comparisons (eg, Bonferroni adjustment) was applied, and the observed interaction effect may attenuate with a larger sample size. Finally, residual confounding from unmeasured variables cannot be ruled out. Although we adjusted for key demographic, clinical, and laboratory factors, other relevant variables—such as specific pharmacologic treatments, participation in pulmonary rehabilitation—were not fully accounted for and may have influenced the observed associations. Future prospective, multicenter studies are warranted to validate these findings and to evaluate the clinical utility of BMI and Hb as stratification markers in severe AECOPD. Longitudinal and interventional studies are also needed to clarify the causal relationships between metabolic and hematologic factors and pulmonary outcomes in this population.
Conclusion
In summary, this study identified an inverse L-shaped association between BMI and lung function in patients with severe AECOPD, with pulmonary benefits diminishing beyond a certain threshold. These findings underscore the need for individualized management strategies, particularly in underweight patients. Hemoglobin levels may further modify this association, highlighting the potential clinical relevance of combined metabolic and hematologic profiling. Prospective studies are warranted to validate these findings and to inform stratified treatment approaches in this high-risk population.
Abbreviations
BMI, body mass index; AECOPD, acute exacerbations of chronic obstructive pulmonary disease; LOHS, length of hospital stay; FEV1, forced expiratory volume in 1 second; FEV1% predicted, forced expiratory volume in 1 second percentage of predicted; FVC, forced vital capacity; FVC% predicted, forced vital capacity in 1 second percentage of predicted; OI, oxygenation index; Hb, hemoglobin; CRP, C-reactive protein; ProBNP, Pro B-type Natriuretic Peptide; SD, standard deviation; IQR, interquartile range; GAM, generalized additive model; RBC, red blood cell; mMRC, modified British medical research council; LAMA, long-acting muscarinic antagonist; ICS, inhaled corticosteroid; LABA, long-acting β2-agonist.
Data Sharing Statement
The clinical data used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Jingzhou Central Hospital (Approval No: 2022-058-01). All patient data were anonymized before analysis, and strict confidentiality was maintained throughout, in compliance with institutional and national data protection regulations.
Acknowledgments
We sincerely appreciate all the COPD patients who participated in this study.
Author Contributions
All authors made significant contributions to the work reported, including conception, study design, execution, data acquisition, analysis, and interpretation, or contributions in multiple areas. They participated in drafting, revising, or critically reviewing the manuscript, approved the final version for publication, agreed on the selected journal for submission, and accepted responsibility for all aspects of the work.
Funding
This work was supported by the Public Health Young Top-notch Talent Cultivation Program of Hubei Province (Hubei Weitong [2021] No. 74), the Hubei Provincial Health and Family Planning Commission Surface Project (WJ2017M241), and the Scientific Research Program of Hubei Provincial Department of Education (B2023238).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Celli B, Fabbri L, Criner G, et al. Definition and Nomenclature of Chronic Obstructive Pulmonary Disease: time for Its Revision. Am J Respir Crit Care Med. 2022;206(11):1317–1325.
2. Zeng B, Williams EM, Owen C, et al. Exploring the acoustic and prosodic features of a lung‑function‑sensitive repeated‑word speech articulation test. Front Psychol. 2023;14:1167902. doi:10.3389/fpsyg.2023.1167902
3. Jones PW, Lamarca R, Chuecos F, et al. Characterisation and impact of reported and unreported exacerbations: results from ATTAIN. Eur Respir J. 2014;44(5):1156–1165. doi:10.1183/09031936.00038814
4. Spencer S, Jones PW, GLOBE Study Group. Time course of recovery of health status following an infective exacerbation of chronic bronchitis. Thorax. 2003;58(7):589–593. doi:10.1136/thorax.58.7.589IF
5. Suissa S, Dell’Aniello S, Ernst P. Long-term natural history of chronic obstructive pulmonary disease: severe exacerbations and mortality. Thorax. 2012;67(11):957–963. doi:10.1136/thoraxjnl-2011-201518
6. Celli BR, Thomas NE, Anderson JA, et al. Effect of pharmacotherapy on rate of decline of lung function in chronic obstructive pulmonary disease: results from the TORCH study. Am J Respir Crit Care Med. 2008;178(4):332–338. doi:10.1164/rccm.200712-1869OC
7. Rodriguez-Roisin R. Toward a consensus definition for COPD exacerbations. Chest. 2000;117(5 Suppl 2):398S–401S. doi:10.1378/chest.117.5_suppl_2.398s
8. Sutherland TJ, Goulding A, Grant AM, et al. The effect of adiposity measured by dual-energy X-ray absorptiometry on lung function. Eur Respir J. 2008;32(1):85–91. doi:10.1183/09031936.00112407
9. Santana H, Zoico E, Turcato E, et al. Relation between body composition, fat distribution, and lung function in elderly men. Am J Clin Nutr. 2001;73(4):827–831. doi:10.1093/ajcn/73.4.827
10. Kirsch F, Schramm A, Kurz C, et al. Effect of BMI on health care expenditures stratified by COPD GOLD severity grades: results from the LQ-DMP study. Respir Med. 2020;175:106194. doi:10.1016/j.rmed.2020.106194
11. Leone N, Courbon D, Thomas F, et al. Lung function impairment and metabolic syndrome: the critical role of abdominal obesity. Am J Respir Crit Care Med. 2009;179(6):509–516. doi:10.1164/rccm.200807-1195OC
12. Tang X, Lei J, Li W, et al. The Relationship Between BMI and Lung Function in Populations with Different Characteristics: a Cross-Sectional Study Based on the Enjoying Breathing Program in China. Int J Chron Obstruct Pulmon Dis. 2022;17:2677–2692. doi:10.2147/COPD.S378247
13. Canoy D, Luben R, Welch A, et al. Abdominal obesity and respiratory function in men and women in the EPIC-Norfolk Study, United Kingdom. Am J Epidemiol. 2004;159(12):1140–1149. doi:10.1093/aje/kwh155
14. Wannamethee SG, Shaper AG, Whincup PH. Body fat distribution, body composition, and respiratory function in elderly men. Am J Clin Nutr. 2005;82(5):996–1003. doi:10.1093/ajcn/82.5.996
15. Park H, Jung SY, Lee K, et al. Prevalence of chronic obstructive lung disease in Korea using data from the fifth Korea national health and nutrition examination survey. Korean J Fam Med. 2015;36(3):
16. Çolak Y, Marott JL, Vestbo J, Lange P. Overweight and obesity may lead to under-diagnosis of airflow limitation: findings from the Copenhagen City Heart Study. COPD. 2015;12(1):5–13. doi:10.3109/15412555.2014.933955
17. Lee CM, Huxley RR, Wildman RP, Woodward M. Indices of abdominal obesity are better discriminators of cardiovascular risk factors than BMI: a meta-analysis. J Clin Epidemiol. 2008;61(7):646–653. doi:10.1016/j.jclinepi.2007.08.012
18. Jin X, Yang Y, Chen G, et al. Correlation between body composition and disease severity in patients with chronic obstructive pulmonary disease. Front Med Lausanne. 2024;11:1304384. doi:10.3389/fmed.2024.1304384
19. Wang X, Gan H, Wang Y, et al. Body mass index affects spirometry indices in patients with chronic obstructive pulmonary disease and asthma. Front Physiol. 2023;14:1132078. doi:10.3389/fphys.2023.1132078
20. Sun Y, Milne S, Jaw JE, et al. BMI is associated with FEV1 decline in chronic obstructive pulmonary disease: a meta-analysis of clinical trials. Respir Res. 2019;20(1):236. doi:10.1186/s12931-019-1209-5
21. Garcia-Rio F, Miravitlles M, Soriano JB, et al. Systemic inflammation in chronic obstructive pulmonary disease: a population-based study. Respir Res. 2010;11(1):63. doi:10.1186/1465-9921-11-63
22. Cerri S, Clini E. Do Not Forget to Assess the Muscle Integrity in Patients With COPD. Chest. 2019;155(6):1090–1091. doi:10.1016/j.chest.2019.01.025
23. Gea J, Sancho-Muñoz A, Chalela R. Nutritional status and muscle dysfunction in chronic respiratory diseases: stable phase versus acute exacerbations. J Thorac Dis. 2018;10(Suppl 12):S1332–S1354. doi:10.21037/jtd.2018.02.66
24. Chan SMH, Selemidis S, Bozinovski S, Vlahos R. Pathobiological mechanisms underlying metabolic syndrome (MetS) in chronic obstructive pulmonary disease (COPD): clinical significance and therapeutic strategies. Pharmacol Ther. 2019;198:160–188. doi:10.1016/j.pharmthera.2019.02.013
25. Cao C, Wang R, Wang J, Bunjhoo H, Xu Y, Xiong W. Body mass index and mortality in chronic obstructive pulmonary disease: a meta‑analysis. PLoS One. 2012;7(8):e43892. doi:10.1371/journal.pone.0043892
26. Spelta F, Fratta Pasini AM, Cazzoletti L, Ferrari M. Body weight and mortality in COPD: focus on the obesity paradox. Eat Weight Disord. 2018;23(1):
27. Prudente R, Franco EAT, Mesquita CB, Ferrari R, de Godoy I, Tanni SE. Predictors of mortality in patients with COPD after 9 years. Int J Chron Obstruct Pulmon Dis. 2018;13:
28. Ferrari M, Manea L, Anton K, et al. Anemia and hemoglobin serum levels are associated with exercise capacity and quality of life in chronic obstructive pulmonary disease. BMC Pulm Med. 2015;15(1):58. doi:10.1186/s12890-015-0050-y
29. Toft-Petersen AP, Torp-Pedersen C, Weinreich UM, Rasmussen BS. Association between hemoglobin and prognosis in patients admitted to hospital for COPD. Int J Chron Obstruct Pulmon Dis. 2016;11:2813–2820. doi:10.2147/COPD.S116269
30. Park SC, Kim YS, Kang YA, et al. Hemoglobin and mortality in patients with COPD: a nationwide population-based cohort study. Int J Chron Obstruct Pulmon Dis. 2018;13:1599–1605. doi:10.2147/COPD.S159249
31. Balasubramanian A, Henderson RJ, Putcha N, et al. Haemoglobin as a biomarker for clinical outcomes in chronic obstructive pulmonary disease. ERJ Open Res. 2021;7(3):00068–2021. doi:10.1183/23120541.00068-2021
32. Kollert F, Tippelt A, Müller C, et al. Hemoglobin levels above anemia thresholds are maximally predictive for long-term survival in COPD with chronic respiratory failure. Respir Care. 2013;58(7):1204–1212. doi:10.4187/respcare.01961
33. Criner GJ. Effects of long-term oxygen therapy on mortality and morbidity. Respir Care. 2000;45:105–118.
34. Celli BR, Fabbri LM, Aaron SD, Agusti A, Brook R, Criner GJ. An Updated Definition and Severity Classification of Chronic Obstructive Pulmonary Disease Exacerbations: the Rome Proposal. Am J Respir Crit Care Med. 2021;204(11):1251–1258. doi:10.1164/rccm.202108-1819PP
35. Hurst JR, Skolnik N, Hansen GJ, et al. Understanding the impact of chronic obstructive pulmonary disease exacerbations on patient health and quality of life. Eur J Intern Med. 2020;73:1–6. doi:10.1016/j.ejim.2019.12.014
36. World Health Organisation. Guidelines for Controlling and Monitoring the Tobacco Epidemic. Geneva: Tobacco or Health Programme, WHO; 1997.
37. Park HJ, Cho JH, Kim HJ, Park JY, Lee HS, Byun MK. The effect of low body mass index on the development of chronic obstructive pulmonary disease and mortality. J Intern Med. 2019;286(5):573–582. doi:10.1111/joim.12949
38. Wu TD, Ejike CO, Wise RA, McCormack MC, Brigham EP. Investigation of the Obesity Paradox in Chronic Obstructive Pulmonary Disease, According to Smoking Status, in the United States. Am J Epidemiol. 2019;188(11):1977–1983. doi:10.1093/aje/kwz185
39. Prescott E, Almdal T, Mikkelsen KL, Tofteng CL, Vestbo J, Lange P. Prognostic value of weight change in chronic obstructive pulmonary disease: results from the Copenhagen City Heart Study. Eur Respir J. 2002;20(3):539–544. doi:10.1183/09031936.02.00532002
40. Tantucci C, Modina D. Lung function decline in COPD. Int J Chron Obstruct Pulmon Dis. 2012;7:95–99. doi:10.2147/COPD.S27480
41. Bray GA. Beyond BMI. Nutrients. 2023;15(10):2254. doi:10.3390/nu15102254
42. Collins PF, Stratton RJ, Kurukulaaratchy R, Elia M. S163 The ‘Obesity Paradox’ in chronic obstructive pulmonary disease. Thorax. 2010;65(Suppl 4):A73–A74. doi:10.1136/thx.2010.150953.14
43. Wei YF, Tsai YH, Wang CC, Kuo PH. Impact of overweight and obesity on acute exacerbations of COPD - subgroup analysis of the Taiwan Obstructive Lung Disease cohort. Int J Chron Obstruct Pulmon Dis. 2017;12:2723–2729. doi:10.2147/COPD.S138571
44. Lainscak M, von Haehling S, Doehner W, et al. Body mass index and prognosis in patients hospitalized with acute exacerbation of chronic obstructive pulmonary disease. J Cachexia Sarcopenia Muscle. 2011;2(2):81–86. doi:10.1007/s13539-011-0023-9
45. Crisafulli E, Ielpo A, Barbeta E, et al. Clinical variables predicting the risk of a hospital stay for longer than 7 days in patients with severe acute exacerbations of chronic obstructive pulmonary disease: a prospective study. Respir Res. 2018;19(1):261. doi:10.1186/s12931-018-0951-4
46. Li M, Cheng K, Ku K, Li J, Hu H, Ung COL. Factors Influencing the Length of Hospital Stay Among Patients with Chronic Obstructive Pulmonary Disease (COPD) in Macao Population: a Retrospective Study of Inpatient Health Record. Int J Chron Obstruct Pulmon Dis. 2021;16:1677–1685. doi:10.2147/COPD.S307164
47. Webb KL, Gorman EK, Morkeberg OH, et al. The relationship between hemoglobin and V˙O2 max: a systematic review and meta-analysis. PLoS One. 2023;18(10):e0292835. doi:10.1371/journal.pone.0292835
48. Ellulu MS, Patimah I, H K, Rahmat A, Abed Y. Obesity and inflammation: the linking mechanism and the complications. Arch Med Sci. 2017;13(4):851–863. doi:10.5114/aoms.2016.58928
49. Vitturi DA, Sun CW, Harper VM, et al. Antioxidant functions for the hemoglobin β93 cysteine residue in erythrocytes and in the vascular compartment in vivo. Free Radic Biol Med. 2013;55:119–129. doi:10.1016/j.freeradbiomed.2012.11.003
50. Levitzky MG. Pulmonary Physiology.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Relationship Between BMI and Lung Function in Populations with Different Characteristics: A Cross-Sectional Study Based on the Enjoying Breathing Program in China
Tang X, Lei J, Li W, Peng Y, Wang C, Huang K, Yang T
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2677-2692
Published Date: 18 October 2022
Sex Differences in the Impact of BMI on Length of Hospital Stay in Hypertensive Patients Admitted to a Cardiology Department: A Retrospective Cohort Study
Łokieć K, Uchmanowicz B, Kwaśny A, Kubielas G, Smereka J, Surma S, Dissen A, Czapla M
Vascular Health and Risk Management 2024, 20:579-591
Published Date: 24 December 2024