Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Body Harmonization: The Definition of a New Concept
Authors Barbosa ADP ![]() , Espasandin I, Pinheiro de Lima L, de Souza Ribeiro C, Raquel Silva L
, Espasandin I, Pinheiro de Lima L, de Souza Ribeiro C, Raquel Silva L ![]() , Faria Quintal T, Nascimento Lima E, Catarina Duarte Vieira L, Soares TR, Autran Colaço AR
, Faria Quintal T, Nascimento Lima E, Catarina Duarte Vieira L, Soares TR, Autran Colaço AR
Received 20 July 2023
Accepted for publication 5 October 2023
Published 29 December 2023 Volume 2023:16 Pages 3753—3766
DOI https://doi.org/10.2147/CCID.S426813
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Antony de Paula Barbosa, Isabela Espasandin, Lucas Pinheiro de Lima, Caroline de Souza Ribeiro, Lara Raquel Silva, Thalita Faria Quintal, Evenny Nascimento Lima, Láila Catarina Duarte Vieira, Thaina Ribeiro Soares, Anna Raphaella Autran Colaço
Department of Research & Development, Health & Aesthetics, Antony Barbosa Institute, Belo Horizonte, MG, 30575-210 Brazil
Correspondence: Antony de Paula Barbosa, Department of Research & Development, Health & Aesthetics, Antony Barbosa Institute, Marco Aurélio de Miranda Street, 406/1104, Buritis, Belo Horizonte, Minas Gerais, 30575-210, Brazil, Email [email protected]
Abstract: Body Harmonization (BHA) is an innovative concept in aesthetics area based on a set of advanced injectable techniques that have shown promising results for body shaping. This is based on procedure combinations indicated to treat body aesthetic dysfunctions, such as localized fat, stretch marks, blemishes, flaccidity, buttocks remodeling, lean mass gain and muscle definition. This study aims to define the clinical concept of BHA, its applications and the main protocols used based on injectable pharmacotherapy. For this purpose, we performed a retrospective review of proven efficient injectable procedures with advanced results for the treatment of body aesthetic disorders, in addition to relying on data obtained from previous clinical experiences. Based on these data, we describe how different compounds can act for treatment of the main body aesthetic dysfunctions, such as lipolytic compounds and collagen biostimulators. In addition, the main application techniques and treatment protocols for each of these dysfunctions were defined. Minimally invasive injectable procedures offer an effective therapeutic option for patients who do not intend to undergo surgical interventions.
Keywords: body harmonization, BHA, aesthetic dermatology, injectable pharmacotherapy, aesthetic dysfunctions, mesotherapy, bioestimulating fillers, thread
Introduction
Aging gradually causes signs on the face and body, from skin changes to body shape. These are result of a combination of intrinsic factors, mainly related to genetics, metabolic reactions and hormonal status, and extrinsic factors, related to the environment, such as UV radiation exposure, diet and other lifestyle habits.1
Today’s society has increasingly imposed an almost unattainable standard of the perfect body, which is reinforced with the rise of social networks around the world. Following this trend of strive for perfection, the beauty industry is constantly growing and innovating, which encompasses the aesthetic market development. Technological innovations are emerging quickly and providing surprising results, with the aim of slowing down aging and enabling men and women to become their best version regardless of age.2
The most widespread concept of beauty today resulted from several theories developed since ancient Greece based on complex associations about art and philosophy associated with beauty and aesthetics. Therefore, the definition of a harmonic face or body is also strongly based on this concept. The visagism was developed by Fernand Aubry in 1937 and is a technique based on symmetry and harmony, as well as morphopsychology and neurobiology. This has been used more frequently in facial evaluation and aims to expose the individual’s internal qualities in a harmonious way, considering his style and personality. Therefore, this concept allows us to customize the pre-established and fixed standards of beauty.3,4
In addition, visagism is an interdisciplinary tool, based on sociological, psychological, anthropological and neurobiological values, enabling visual expression of emotions and personality traits. In this context, beauty and symmetry are two determinants that go together to achieve the idealized beauty, described by Plato as any object with harmony or unity in its composition, and by Socrates as everything with order and symmetry.3,5 The human mind associates perfection with symmetry and considers unbalanced proportions as something exotic, and therefore the measures adopted need to be proportional to each other, in a personalized and balanced way, without using ready-made formulas.6
Anatomovisagism emerged from visagism and establishes a set of techniques that provide harmony, symmetry and functionality of female and male morphological characteristics through proportions and anthropometric measurements of an individual’s face and body. This technique is related to a deeper knowledge of human anatomy, which allows the image customization of each person according to their main clinical complaints, desires and personality.3 This proposal disagrees with the way most aesthetic professionals work and the concept of body harmonization (BHA) emerged aiming to revolutionize the aesthetic market following the “every person is unique” principle. Thus, this work aims to define the clinical concept of BHA, its applications and the main protocols used based on injectable pharmacotherapy, being extremely important in order to achieve the best results and avoid intercurrences.
Materials and Methods
Study Design
The literature review was performed by consulting search engines for scientific articles, such as PubMed, Web of Science, Embase, Scielo, Science Direct and ClinicalTrials.gov aiming to identify eligible articles. All scientific materials addressing injectable procedures, pharmacology, aesthetic disorders, treatment techniques and clinical planning related to BHA were included.
The following BHA-related procedures were included in the searches: (i) plastic surgery, (ii) mesotherapy or intradermotherapy, (iii) dermal fillers, collagen biostimulators, PDO threads, plasma gel and platelet-rich plasma (PRP), (iiii) electrotherapy and (iiiii) aesthetic prescription. Articles were excluded based on title, abstract or both, if there was no clear indication that they were investigating procedures associated with these concepts.
Data Extraction
Each eligible article was critically reviewed, and the following information was extracted: aesthetic clinical manifestations, morphofunctional characteristics, compounds, therapeutic dose, treatment duration, therapeutic associations, techniques and clinical procedures. Then, the information extracted from the selected publications were crossed with data obtained from the clinical experiences of the researchers involved in this study to define concepts and standardize treatment techniques.
Review and Description of the Proposed Methodology
Definition of the Body Harmonization (BHA) Concept
Body Harmonization (BHA) consists of the combination of invasive, minimally invasive and non-invasive aesthetic procedures associated with the prescription of topical compounds and nutraceuticals aimed at the integral treatment of the body in a personalized way. In this context, it is possible to treat several aesthetic dysfunctions together, allowing the body to be organically stimulated to eliminate fat without acquiring irregular contours, flaccidity, stretch marks, cellulite, blemishes, skin dryness and acne lesions, respecting the anatomical and body biotypes of each one (based on anatomovisagism concept). BHA seeks to resolve patients’ clinical complaints through individualized therapeutic planning, avoiding frustrations with aesthetic standards and social comparison in body image.
The main techniques and procedures used in BHA include plastic surgery, mesotherapy and advanced intradermotherapy, high performance (HP), dermal fillers and collagen biostimulators, PDO threads, Plasma Gel and PRP, electrotherapy (ultrasound, radiofrequency, carboxytherapy, hydrolipoclasia or hydrochemolipoclasia) and aesthetic prescription (nutraceuticals/phytotherapics, cosmeceuticals and nutricosmetics). All BHA procedures are scoped by non-medical and medical professionals, except plastic surgery which can only be performed by medical plastic surgeons.
Basic and advanced mesotherapy and intradermotherapy techniques are fundamental parts of BHA. Mesotherapy is a minimally invasive procedure that consists of administering diluted injectable compounds (pharmacological actives) in local areas with minimal therapeutic doses, in which the compounds used have peripheral active sites and little systemic action.7,8 The tissues of mesotherapy application used in BHA are the upper dermis (intradermal), the deep dermis (intradermal), the hypodermis (subcutaneous) and muscle tissue (intramuscular).
Mesotherapeutic procedures are used to treat hair, facial and body aesthetic dysfunctions such as tissue and muscle flaccidity, fibroedema geloid (cellulite), localized lipodystrophy (localized fat), submental lipodystrophy (“double chin”) and generalized fat. In contrast, intradermotherapy consists of the administration of injectable compounds exclusively into the dermal tissue. Intradermal procedures are used to treat skin dysfunctions such as tissue sagging, stretch marks, scars, acne, skin devitalization, aging, facial and body hyperchromia (melasma and other types), periorbicular hyperpigmentation (“dark circles”) and capillary dysfunctions. Depending on the compounds chosen and the form of application carried out, it is common for some side effects to be presented. The most common are erythema, ecchymosis, local pain, formation of small temporary nodules and post-inflammatory hyperpigmentation. In addition to these, some less common effects that may occur are nausea, vomiting, diarrhea, hypersensitivity and necrosis. Because of this, it is extremely important that the professional who will perform mesotherapy procedures has the necessary expertise.7–11
Furthermore, in BHA context, subcision is a minimally invasive and very efficient technique, mainly used to treat depressive atrophic scars and cellulite. Its mechanism is based on the disruption of fibrotic strands and septa underlying the scars and cellulite, which also stimulates a local connective tissue reorganization. With regard to cellulite, the release of the reticular dermis from the underlying fibrous septal bands of the hypodermis results in the relocation and redistribution of the fat lobules present in the areolar layer of the hypodermis. Consequently, this procedure results in the local skin topography smoothing. The possible side effects resulting from this technique occur mainly due to the rupture of blood vessels in the region where it was performed, which can cause moderate local pain, edema, erythema and ecchymosis. These effects are relatively common and even expected, and disappear within a few days.12,13
Application Techniques
Intradermal with Needle (ID-N)
Punctual administration of the chosen blend of compounds in a maximum volume of 10 mL in the dermal tissue per session, with a minimum break of 2 two days between each session. In this technique, approximately 0.1mL must be applied per point or until a papule forms, using a 30G needle at an angle of 15° and a distance of 1 to 2 cm depending on the region. This application technique is used for treatment of stretch marks, skin flaccidity, scars, skin devitalization and hyperchromias. The chosen blend can also be applied by retroinjection, especially in the case of stretch marks (Figure 1).
 |
Figure 1 The intradermal with needle and with cannula application techniques. |
Intradermal with Cannula (ID-C)
Administration of substances of considerable density and collagen biostimulators by retroinjection or fan technique. Before application, the orifice must be carried out directly with the 18G or 21G needle, depending on the cannula chosen. Graduated cannulas with sizes of 22G for the abdominal region and 18G for the gluteal region and inner thighs must be used for the application. The injection should be performed at an angle of most 15° (Figure 1). Collagen biostimulators and eutrophic compounds of considerable density should be deposited at a depth between 4 and 6 mm. On the other hand, when the use of collagen biostimulator in the role of filler is desired, the product must be deposited at a depth of approximately 8 mm or more, in subcutaneous or periosteal tissue (Figure 2).
 |
Figure 2 The application technique for collagen biostimulators or fillers and the skin after it. |
Subcutaneous (SC)
Punctual administration of lipolytic or surfactant compounds in a maximum volume of 10mL per session on subcutaneous tissue, with a minimum break of 2 two days between each session. In this technique, approximately 0.2–0.4mL per point must be applied with 26G or 30G needles at a distance of 1–2cm from the region. The injection must be performed at an angle of 90° for fat folds over 2.5 cm and 45° for fat folds up to 2.5 cm. This route of administration is used for localized fat, cellulite and deepening of abdominal creases (Figure 3).
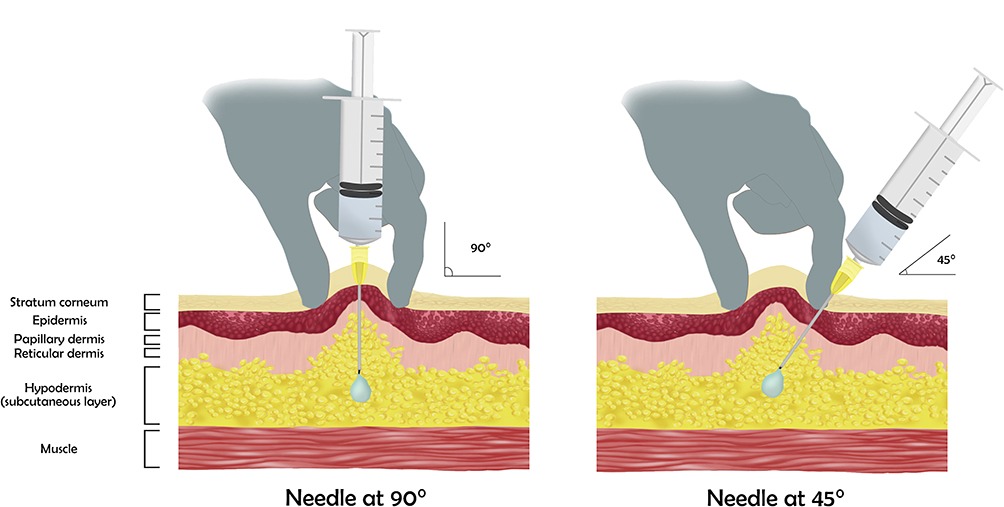 |
Figure 3 The subcutaneous application technique at an angle of 90° and 45°. |
Deep Intramuscular (D-IM)
Administration of compounds in a maximum volume of 10mL per session, corresponding to 5 mL for the upper outer quadrants of each gluteus, with a minimum break of 2 two days between each session. The application must be performed using 21G or 22G needles at an angle of 90°. The professional should always perform aspiration before application to make sure to make sure that no blood vessels are caught. This application technique is used for treatments aiming weight loss, metabolism acceleration, generalized mass gain and appetite suppression (Figure 4).
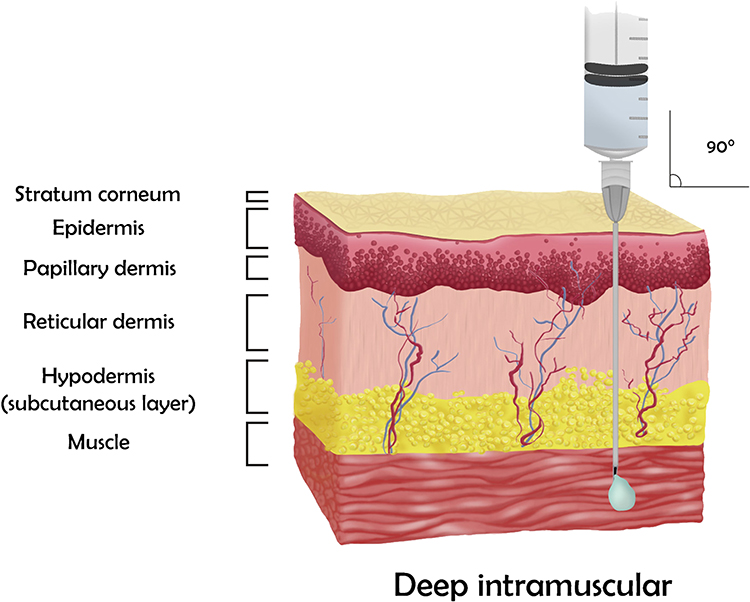 |
Figure 4 The deep intramuscular application technique. |
Z-Track Intramuscular (Zigzag)
It consists of an application technique that creates a zigzag movement through the tissues, consequently sealing the needle path, preventing the return of the injected blend. This differs from the conventional intramuscular application by displacing the tissues approximately 2.5 to 3.5cm downwards or laterally until complete delivery of the compound(s) in the muscle (Figure 5).
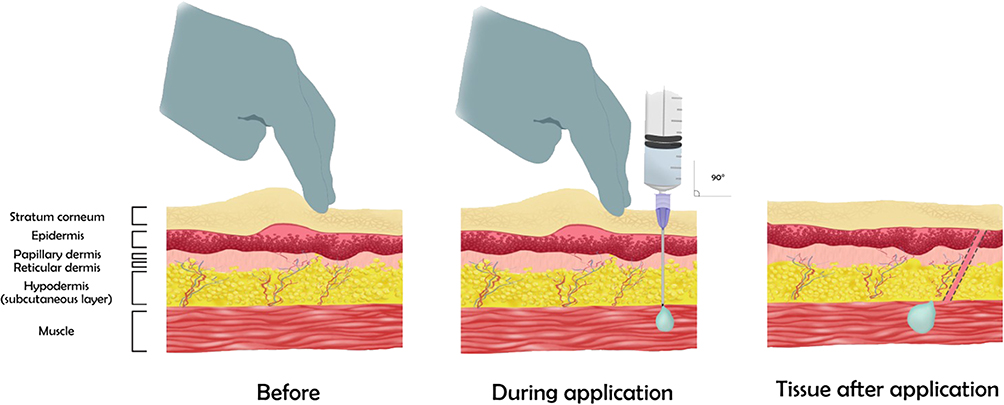 |
Figure 5 The Z-Track intramuscular (Zigzag) application technique. The skin before, during and after application. |
Subcision
This technique is usually performed by inserting a “duck beak” cannula 18G of 10–20mm into the subcutaneous layer, parallel to the skin surface, with the cutting blade pointed against the fibrotic septum. Repetitive cutting movements are then performed, thus creating a dissection plane. It is recommended that compression be applied at the site for 5–10 minutes to prevent bruising.12,13 The injection of effective compounds for cellulite treatment can be performed in association with subcision (Figure 6).
 |
Figure 6 The subcision technique with a “duck beak” cannula. |
Injectable Pharmacotherapy
In BHA, we must consider the drugs that will be administered to achieve the best results on our patients and achieve our goal with chosen treatment. In this context, a compound can be considered a pharmacological active or drug, which can be defined as a known chemical structure that produces a biological effect when it binds to a receptor. Receptors are found on the cell surface and do the communication from one cell to another, and the interaction between the cell and the extracellular field in which it is inserted. Receptors are the key to the chemical transduction system used by cellular organisms to coordinate their activities.14 The cellular effects manifested from these receptors can be divided by their operation, since some are very fast, acting in milliseconds, while others can take hours. One example is thyroid hormone receptors, which can take hours, while catecholamine receptors are effective in seconds.14
Based on bonds molecular structure and nature, we can distinguish the receptors into four types or superfamilies. Ionic channels controlled by ligands, or ionotropic receptors, have a fast response, controlling the fastest events of the nervous system. Neurotransmitters act on the postsynaptic nerve membrane or muscle cells temporarily increasing their permeability to Na+, K+ and Ca+. The ion input causes cell depolarization, generating action potential in a few milliseconds (Figure S1).14
The metabotropic receptors have a slow response and compose the largest receptors family. These channels are formed by seven transmembrane helices, subdivided into three groups that are different by details of their structure, such as the terminal helix length. The third loop of this structure houses the binding site of G proteins, which recognizes GPCRs (G protein coupled receptors) and transmits an action signal to the sector system, being responsible for activating a second messenger in the cell. These G proteins are subdivided into the subunits α, β and γ, which are linked to each other. The interaction of a GTP molecule with the α subunit enables the β and γ subunits to send a signal to the effector, resulting in an enzyme activation/inactivation or in a channel opening depending on GTP half-life. When the GTP undergoes hydrolysis, the α subunit will reconnect to β and γ subunits, interrupting the cascade of action and producing GDP, thus stopping the started cycle. The main targets of G protein are ionic channels (sodium and potassium channels), phospholipase C (formation of Inositol and diacylglycerol), adenylyl cyclase (formation of cAMP), Rho kinase (cell proliferation) and protein kinase activated by mitogens (cell division) (Figure S2).14
Furthermore, we have the receptors tyrosine kinases (RTKs), which are membrane receptors with an extracellular domain containing a terminal nitrogen and an intracellular kinase domain (followed by a terminal C tail) connected by a single transmembrane segment. They have an enzymatic activity, acting from the transfer of phosphate groups to protein substrates, which in this case is the amino acid tyrosine. In the activated complex, the intracellular domains form a dimer in which one kinase activates another in an allosteric way. When activated, it promotes the auto phosphorylation of the terminal C tails of the receptors, what allows the anchorage of numerous intracellular proteins. These last can act in several intracellular signaling pathways, which evidences the important role of RTKs as cellular processes regulators (Figure S3). An example of RTK is the insulin receptor (IR).15
Nuclear receptors bind directly to deoxyribonucleic acid (DNA) and act in gene expression regulation, therefore being commonly called transcription factors. These receptor ligands bind to lipophilic molecules, once to interact with the receptor they need to cross the plasmatic or nuclear membrane, such as endogenous hormones and vitamin S (Figure S4).16
It is possible to observe the multiple ways that a substance can act on the human body, depending on the interaction with different types of receptors, which can regulate cellular processes directly or indirectly when activated by this event. Therefore, any substance with affinity for a receptor (such as a drug) can be called a ligand, being able to activate or inactivate it. A ligand can interact with more than one receptor subtype according to the chemical structure. The binding site of a drug is not necessarily the same as that of an endogenous agonist and the receptor action depends on binding type that can be classified as agonist or antagonist. This classification arises from its observed effects that are generated on the receiver interaction with a particular ligand (Figure S5).17
The binding of an agonist, which can be endogenous drugs or ligands, to its receptor leads to its stabilization in a certain conformation, which is usually its active shape.18 A molecule capable of activating a receptor at its maximum level can be called a total agonist. Likewise, when a partial agonist interacts with its receptor, this one is not able to reach its full activation. An example is the buprenorphine, approved by the Food and Drug Administration (FDA) in the treatment of patients with opioid use disorder.19
An antagonist inhibits the action of an agonist, but has no effect on its absence. One of its mechanisms of action is to bind itself to its receptor active site and directly prevent the agonist binding. Another mechanism is the binding of the antagonist into the allosteric site, resulting in a conformation change required for receptor activation by agonist binding to be prevented. Antagonists can either be the competitive type, which binds themselves reversibly to the binding site causing receptor inactivation; or the non-competitive type, when this binding is effectively irreversible, regardless of whether it is at the active site or in an allosteric site.18
These concepts knowledge is important because compounds used in BHA interact with several body receptors present in different tissues to exert their effects. Therefore, the desired response is closely related with the drug receptors interaction in the human body, and the understanding of these events results in an optimized and targeted treatment.17 To perform these related procedures, the compounds can be managed by injectable, topical and even oral way. Commonly, lipolitical and metabolic accelerators, eutrophic and collagen biostimulators, vasoactive, anesthetics, ergogenic and hypertrophic accelerators are commonly used. Compounds with lipolytic activity or that act by inhibiting lipogenesis are some of the most used in different mesotherapy protocols used in BHA. Hence, to reach the best results, we need to understand these processes and their regulatory pathways.
Lipogenesis is the synthesis of fatty acids and triglycerides, which is mainly regulated by food, hormonal and genetic factors.20 Liver fatty acids metabolism begins with the triacylglycerol (TAG) hydrolysis – from the food – by pancreatic lipase, being then emulsified by bile acids. So, these molecules are resynthesized into TAG, which are finally packaged in chylomicrons, which can be captured by muscle and adipose tissue or delivered to the liver, where the remaining triacylglycerol will be endocytosed. The fatty acids release occurs during lysosomal processing of these particles. When, for many reasons, carbohydrates are present in large quantities, the liver converts glucose into fatty acids, a process called new lipogenesis, which has a direct link with body fat accumulation and hepatic steatosis. The new lipogenesis happens from the glucose molecules breakdown, and one of the glycolysis products is pyruvate, which is converted to citrate within mitochondria. Then, citrate turns into acetyl-CoA and, after some reactions, the palmitate is obtained, which can be modified to generate several other fatty acids. The main hormone acting in this process is the insulin, since it is responsible for transporting the glucose into the cell’s interior.21
The adipocyte works as a TAG store in lipid droplets. When the body demands for energy, these molecules are transformed into glycerol and fatty acids by lipolysis. Basal lipolytic activity in humans is regulated by several factors such as the location of fat deposits, age, sex, and others. Lipolysis is catalyzed by several enzymes, three main ones being: adipose triglyceride lipase (ATGL), monoacylglycerol lipase (MGL) and hormone-sensitive lipase (HSL).21
TAG degradation has a neuroendocrine control mainly established by catecholaminergic stimulation, through activation of the enzyme adenylate cyclase, whose action increases cAMP levels, favoring phosphorylation and consequent activation of HSL, which has an important performance in lipolysis process.22 Catecholamines exert their effect due to the establishment of several connections with adrenergic receptors present in adipocytes. It is known that, in the human body, β3 adrenergic receptors are closely related to lipolytic activity (excitatory activity), while α2 adrenergic receptors act in the opposite way (inhibitory activity). Certain situations such as negative energy balance and some substances, like the hormones T3, T4, TSH, catecholamines, GH, among others, can act on this process regulation. An important hormone that also affects this process is the insulin, which is the one responsible for glucose transport and when connected to its receptor, promotes the phosphatidyldyinositol 3-kinase (PI3K) complex and phosphodiesterase 3B (PDE3B) activation. This last catalyzes the cAMP conversion into 5’AMP, preventing HSL activation and consequently the basal lipolysis.22
Most of the compounds used in treatments to reduce fat accumulation target metabotropic receptors, present in adipocytes, which act by activating adenylate cyclase or inhibiting PDE3B. Therefore, these produce effects that result in an increase in cAMP levels, favoring lipolytic activity. In general, lipolytic compounds that interact with excitatory adrenergic receptors (β3) act as agonists, while those that interact with inhibitory adrenergic receptors (α2) act as antagonists. A well-known example is the lipolytic effect established by caffeine and other methylxanthines, which interact with excitatory receptors and act by inhibiting PDE3B, blocking the conversion of cAMP into 5’AMP, favoring HSL activation.22
It is notorious that these processes, commonly called fat breakdown, can be stimulated by different pathways and by different substances. Therefore, these are often used to compose blends of choice in aesthetic procedures included in BHA, due to their effect on key metabolic pathways aimed at optimizing these procedures.
Collagen Biostimulators
Biostimulators are increasingly being used as a non-surgical option to rejuvenate with a natural appearance both face and body, improving skin texture, sagging, cellulite, and fill areas. These are composed of biodegradable and bioresorbable substances which are phagocytosed and lasts 18 months to 4 years. It stimulates an inflammatory response that induces fibroblasts to produce collagen and other matrix proteins, causing this three-dimensional natural-like rejuvenation. Due to this controlled, desired and expected inflammatory response, some side effects may be presented, which is also expected for most biostimulators. The most common effects presented in the first few days after the application of biostimulators are edema, erythema, heat and controlled local pain. Furthermore, small blood vessels may occasionally rupture during application, which may lead to possible bruising. All of these effects normally disappear within the first few days after the procedure.23,24 The duration, purpose and end result of the treatment should be considered when choosing which product to use. While polycaprolactone (PCL) and Poly-L lactic acid (PLLA) lasts the longest, the calcium hydroxyapatite (CaHA) degrades faster but has a different mechanism than the one previously described.25,26
CaHA stimulates fibroblasts to promote collagen synthesis and has a filling effect, adding volume to the treated area. The histology of patients treated with CaHA showed more compact collagen and elastin fibers and more horizontal fibers after treatment. Excellent results were obtained when used for neck rejuvenation, increasing skin thickness and improving wrinkles as well as body, with the best results shown on the abdomen. This biostimulator has a viscoelastic texture with CaHA microspheres (30%) diluted in a gel (70%) composed primarily of water, glycerol and carboxymethyl cellulose (CMC).24,27,28 Most CaHA formulations currently marketed allow dilutions at different concentrations according to the treatment purpose and the application area. For body applications, a dilution resulting in a final concentration of 10% CaHA is recommended, and can be performed on the same day of application. In general, dilutions are carried out according to the formula: Ci*Vi = Cf*Vf (Ci=initial concentration; Vi= initial volume; Cf = final concentration and; Vf = final volume). One of the main formulations is Radiesse Duo® (Mers Aesthetics®, Frankfurt, Germany), which is presented as a suspension containing 30% CaHA and 70% CMC in a solution of 1.5 mL. Taking this as an example, to reach a concentration of 10% CaHA, we recommend adding 1.0 mL of 0.9% saline or injection water and 2.0 mL of 2% lidocaine, totalizing a final volume of 4.5 mL. The suspension formed must then be homogenized with the aid of a three-way connector coupled to two 10 mL syringes.26
PLLA is a biocompatible, biodegradable and semi-permanent filler that gradually stimulates fibroblasts, resulting in neocollagenesis by causing a local inflammatory response. During metabolism, capsules are formed around individual product microspheres, leading to increased deposition of collagen fibers by fibroblasts and subsequent skin thickness. Due to PLLA’s action in the skin, if the product is not resuspended correctly or if it is applied too superficially or in areas with thinner skin, nodules may be observed. To prevent these from forming, it is recommended that vigorous massages be carried out in the area of application for the first few months after the procedure.23 In addition to its long-standing classical use in facial indications, this polymer is now used for volumizing non-facial areas such as the neck and chest, contouring the body, sagging skin, cellulite and scars. It is also used as a treatment for buttocks, abdomen, arms, thighs, knees and reaching body.29 PLLA is generally marketed as a sterile lyophilized powder, which must be reconstituted prior to application. The main formulation is Sculptra® (Galderma®, Zug, Switzerland), for which the manufacturer recommends reconstitution in 10 mL of sterile injectable water (2 mL of this volume can be replaced by 2% lidocaine) per vial for facial applications and in 16 mL of sterile injectable water (2 mL of this volume can be replaced by 2% lidocaine) for body applications. Subsequently, the suspension must be gently homogenized, rolling the vial between the palms of the hands, until it becomes uniform and translucent. In order to achieve optimal hydration before application, the product must be kept at rest for at least one hour at a temperature of 5 to 30°C.26,29–31
PCL is a biostimulator composed of microspheres suspended in a CMC gel carrier that immediately brings volume upon application. In histological studies, an increase in type I collagen compared to his type III collagen was mainly observed in long-term treated animals. These characteristics make this biostimulator have a long-lasting effect for patients.32,33 These gels are composed of PCL microspheres, from 25 to 50 μm in size, which are identified by phagocytic cells, thus inducing the formation of new collagen fibers around them, the volume being preserved even after they are phagocytized. These spheres are suspended in a carrier gel which is hydrolyzed by the body, forming CO2 and water as a final product and is naturally and completely excreted. Collagen formation also provides improved skin support with an effect of 18–24 months. The main indications are volumization, contour improvement, rejuvenation, wrinkle and skin texture improvement.32,33
In addition to the biostimulators mentioned above, which are used in a liquid suspension form, there are also biostimulators in solid state, such as the absorbable threads. Of these, the most used are polydioxanone (PDO) threads, but there are also threads made from other materials, such as PLLA and polycaprolactone. The main types of threads are smooth, spiral or screw, barbed and multiple-monofilament threads. All of these can stimulate the production of different types of collagens, mainly I and III, by the fibroblasts in their surroundings. In addition, when threads are inserted, granulation tissue is formed, which stimulates generation of fibroblasts and myofibroblasts, thus influencing skin texture, tone, pore size, firmness and elasticity. These effects can start to be noticed within a few weeks and can last up to 2 years. The barbed threads also act in the traction of the skin, providing tissue repositioning. Therefore, these contribute to a lifting effect, providing an improvement in ptosis and greater definition and contour in the places where they are applied.34–36 The different types of PDO threads can be contained in a needle or cannula, so simply removing one or the other will leave the thread in place. Types of threads applied with the sole purpose of stimulating collagen, such as smooth threads, are usually inserted into a more superficial subcutaneous plane, forming a mesh. On the other hand, barbed threads are usually inserted into a deeper plane, forming vectors with strategic attachment points in order to provide support.34–36 Absorbable threads, mainly made from PDO, are widely used to improve the face skin quality and also for face lifting.35–37 More recently, these have also been used in BHA, in regions such as abdomen, thighs, arms, buttocks and breasts, improving skin quality, sagging, cellulite and even ptosis in some cases, producing a lifting effect.38–40
Clinical Guideline: The Main Aesthetic Dysfunctions Treated Within BHA
Localized Lipodystrophy
Localized fat is an aesthetic dysfunction related to the accumulation of adipocytes in the hypodermis. This disorder can affect different regions of the body, primarily in the abdomen, hips, arms and legs. The metabolic changes involved with localized lipodystrophy increase the risk of diabetes and cardiovascular disease.41 Adipose cells have receptors, in which the amount and type depend on the body region, so that the β3 adrenergic receptors further lipolysis and are located in the abdominal region, while the α2 adrenergic receptor inhibits lipolysis and are located in greater amounts in the region buttocks and thighs.41
Therefore, for the treatment of this aesthetic dysfunction, we usually use blends containing compounds belonging to classes of lipolytics, as methylxanthines and metabolism accelerators, being the main ones: Citrus Sinensis, Caffeine, Sodium Seoxycholate, Sunflower liposome, L-Carnitine, Tripeptide-41 plus and Yohimbine for cases of fat accumulation in the lower limbs, among others (Table S1).
The compounds choice must respect the density and location of the fat, as well as the physiological characteristics of each individual. These can be applied with a 30G needle, administering 0.2mL per point in the subcutaneous tissue (SC) in weekly sessions, with a minimum of 10 sessions.
Generalized Fat
Inadequate diet, lack of physical activity, tobacco and alcohol consumption, genetic predispositions, physical inactivity and hormonal disorders are among the main causes of generalized fat accumulation.42
For the treatment of this dysfunction, priority should be given to the choice of metabolism-accelerating compounds, which, in addition to the thermogenic function, promote a decrease in cholesterol, increase in lean mass, promote satiety and inhibit appetite. The main compounds of this class are: Lipoless®, Inositol, Taurine, Choline, L-Carnitine, L-Phenylalanine, Beta-hydroxy-beta-methylbutyric acid (HMB), Magnesium Sulfate and Chromium Picolinate (Table S1).
The association with other blends in weekly alternation is valid to achieve different mechanisms of metabolism acceleration. This treatment is based on twice a week or weekly sessions depending on the planning of each patient and the applications will be deep intramuscular (IM-D). Aerobic exercises are recommended 2 hours after application.
Fibroedema Geloid (FEG), Gynoid Hydrolipodystrophy (GHLD) or Cellulite
Gynoid hydrolipodystrophy (GHLD) or fibroedema geloid (FEG) is popularly known as cellulite and is a multifactorial aesthetic dysfunction characterized by a padded appearance or “orange peel” on the skin. This occurs due to an alteration in the subcutaneous tissue, resulting in local edema, alteration of the dermal connective tissue and of the veno-lymphatic function and sometimes in local inflammation. The hypodermis can be divided into three layers: areolar, fibrous lamina and lamellar. The areolar layer is the most superficial, composed of voluminous globular adipocytes oriented vertically, forming units separated by fibrous septa, which act as anchorage points for the skin to the muscle band. The increase of adipocytes in size and number in this layer, together with the vertical orientation of the fibrous septum (characteristic of women), tensioning the tissue downwards in a punctual way, results in cellulite. The predisposing factors for this dysfunction are genetic-constitutional in which multiple complex and interconnected etiological factors are related, namely hereditary factors (gender, ethnicity, body type and fat distribution), circulatory and hormonal problems (estrogens or adiponectin), poor diet, sedentary lifestyle or stress. Therefore, the main classes of pharmacological assets used in the treatment of this dysfunction include lipolytic, venotropic and eutrophic compounds (extracellular matrix remodelers).42
The lipolytic compounds of choice for the treatment of this dysfunction do not include the surfactants. Therefore, we can choose, for example: Chrysin, Inositol, Caffeine. The eutrophic compounds of choice can be: Asiaticoside, Baicalin and DMAE. Associated with these compounds and according to the degree of cellulite, we can include venotropic compounds to promote peripheral vasodilation, such as Blufomedil, DMSO, Pentoxifylline or Rutin + Benzopyrone, in addition to Yohimbine, which can be used as an adjuvant in the treatment, as well as Hyaluronidase, due to its mechanism of action (Table S1).
The chosen treatment blend must be administered from 0.2 mL applications in each identified cellulite point, using a 30G needle, inserting 2/3 of the needle at a 45-degree angle, aiming to reach the lamellar layer of the subcutaneous tissue (SC). Weekly applications are recommended, with a minimum of 10 sessions.
Before applying the blend, the subcision technique can be performed by forming asterisks or fans. This can be used to treat cellulite grades 3 and 4, with the aim of breaking up the fibrosis formed in the region. Sessions will be held every 15 or 30 days, depending on the degree of dysfunction of each patient and the response to treatment. This technique can be associated with the aforementioned mesotherapy technique in the subcutaneous tissue, with an interval of 15 days between applications.
Hypertrophic exercises should not be performed after the procedure and aerobic exercises are recommended 2 hours later. The patient should avoid the use of anti-inflammatory drugs after the procedure and, in case of pain, should prefer the use of analgesics without anti-inflammatory action.
Flaccidity
The loss of elasticity and muscle tone leads to sagging, which can be of the muscular or tissue type. The two forms can appear alone or associated. Muscle tone consists of a state of baseline muscle tension at rest, and skin elasticity is characterized by a healthy, hydrated, firm appearance, without wrinkles or creases.1
Muscle Flaccidity
Muscle flaccidity is related to loss of muscle tone, often caused by lack of stimuli, experiencing less activity of muscle fibers, which in turn become hypoatrophied. Certain factors tend to accelerate the dysfunction, such as: poor diet, obesity, hormonal disorders, pregnancy and sedentary lifestyle.1
Tissue Flaccidity or Cutaneous Flaccidity
Tissue sagging (or skin sagging) refers to the quality or state of sagging skin tissue, which can be observed when collagen fibers start to become thinner, disorganized, or lose collagen and elastin in the tissue, due to malnutrition, dehydration or aging. Other factors can also influence, such as solar radiation, poor diet and lack of daily care, which is always amplified by the action of gravitational force.1
For the treatment of both types of flaccidity, priority should be given to increasing the production of collagen, elastin and other extracellular matrix proteins. This can be stimulated from the administration of eutrophic compounds (DMAE, Chondroitin, Collagen, Silicon, among others as described in Table 1) and collagen biostimulators, such as CaHA, PLLA and PCL, in addition to smooth and spiculated PDO threads. The treatment protocol adopted will depend on the patient’s clinical history and the degree of flaccidity, being possible to associate different types of biostimulators and compounds, in addition to associating different techniques for greater collagen stimulation.
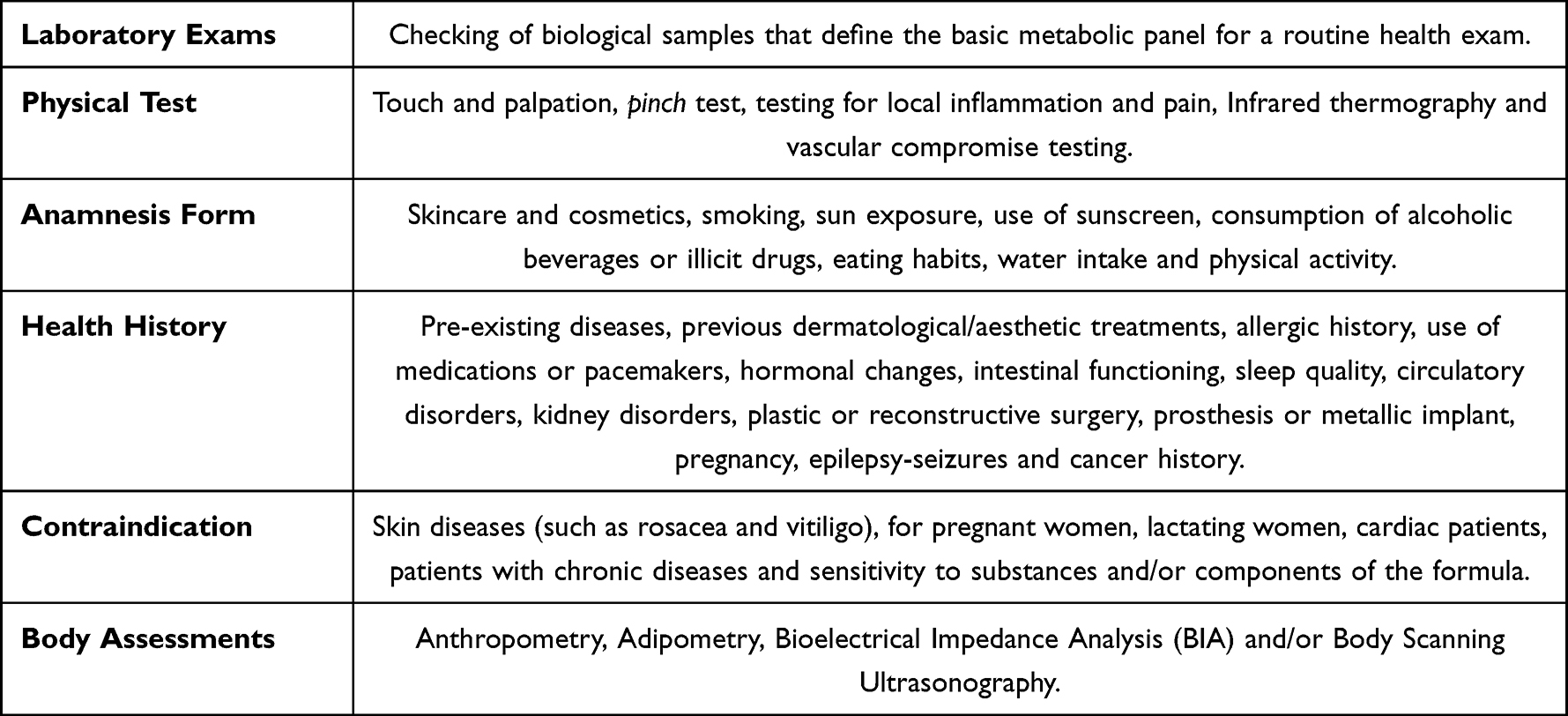 |
Table 1 The Main Methodologies Used in Clinical Evaluation for BHA |
The frequency of sessions for applying the treatment depends on the type of method chosen by the professional and may vary from weekly applications in the case of intradermotherapy, to applications every 30 to 45 days for collagen biostimulators. It is interesting to associate electrotherapy to intercalate with these applications.
Stretch Marks
The stretch mark is a tegumentary atrophy, caused by the rupture of elastic and collagen fibers due to the mechanical stretching of the skin, thus forming scars. The initial appearance of stretch marks are linear lesions of reddish color, depressed or slightly elevated in relation to the skin level. In the late phase, stretch marks acquire a white color and have variable thickness and width. This is a multifactorial aesthetic dysfunction, being related to genetic, endocrinological, familial and mechanical factors, always promoting, through different switches, the imbalance of the structures that make up the connective tissue. Its appearance occurs mainly in the breasts, thighs, buttocks, abdomen and back of the trunk.43
Therefore, the treatment of this aesthetic dysfunction aims to increase the stimulus for the formation of new collagen and elastin fibers, oxygenation and tissue nutrition with the administration of eutrophic compounds and collagen biostimulators, and when associated with microneedling or electro therapies the result is more satisfactory. Among the eutrophic, we have Chondroitin, Nano Growth Factors, Silicon, Vitamin C and Hyaluronic Acid (Table S1).
The compounds blend can be administered from intradermal applications with 30G needles in retroinjections, covering the entire extension of the striae or from drug delivery performed by microneedling along the entire extension of the striae. It is recommended that sessions be held every 28 days, with a minimum of 3 sessions. The two techniques described above can be alternated in different sessions for a tighter result. It is important to warn that the patient cannot expose the region to the sun in the first days after the procedure.
Clinical Evaluation
Clinical examination and body assessments are the initial steps in developing a treatment plan that meets the patient’s needs. The clinical examination is responsible for identifying the aesthetic dysfunctions, main clinical complaints, clinical history and primary photographic documentation. The anamnesis form should collect the information necessary to evidence diagnostic hypotheses and determine the therapeutic goals and the appropriate treatment. Table 1 briefly describes the main evaluation methodologies used.
Bioelectrical Impedance Analysis
Bioelectrical impedance is a method of assessing a patient’s body composition. Bioimpedance analysis is performed by passing a low-amplitude, high-frequency electrical current (imperceptible) through the patient, based on the principle that body tissues have a natural resistance to the passage of electrical current, which is known as bioresistance. It is known that the electric current is well conducted by the ions contained in the body fluids; therefore, the tissues that contain more water and ions in their composition, such as muscle and blood, will offer less resistance to the passage of the electric current, while the tissues such as fat, skin and bones, will not conduct electricity well.44,45
Bioimpedance analysis is able to estimate clinical parameters of body compartments (limbs and trunk) such as body weight, percentage of total body fat and visceral fat, muscle mass (in kilograms), bone mineral mass (in kilograms), basal metabolic rate (BMR), metabolic age, daily caloric intake and total body water (TBW). In order to obtain an accurate report, some recommendations are important, including fasting from food and beverages (4 hours before the exam time), not consuming alcoholic and caffeine-rich beverages (dark teas, coffee, energy drinks and chocolate) and not performing physical activity, intense physical activity and sauna the day before the exam.44,45
Body Scanning Ultrasonography
It is a high-precision diagnostic system for body scanning that is used by healthcare professionals. It consists of a portable device that, through its application by ultrasound technology, allows the visualization on the computer screen of images and values of subcutaneous fat and muscle thickness. Therefore, it is a detailed exam that allows you to accurately estimate the percentage of total body fat, basal metabolic rate (BMR), and muscle composition, following in real time the patient’s weight loss and hypertrophy process with complete reports and visualization of images of the superficial and deep layers of fat on the screen of electronic devices. Unlike bioimpedance, it does not need any preparation for its performance, it is not affected by the level of hydration, physical activity, consumption of caffeine, alcohol, hours of sleep and menstrual periods.46,47
Conclusion
This is the first study to present the Body Harmonization (BHA) concept and their clinical approaches. In addition, we demonstrate the arsenal available in the injectables pharmacotherapy in the management of aesthetic dysfunctions, as well as the different application techniques. Data also demonstrate an important therapeutic role for minimally invasive injectable procedures as an alternative to surgical interventions. Finally, the correct definition of BHA, as well as the appropriate techniques and compounds to be used, is extremely important for the guidance of professionals in the aesthetic area, enabling the achievement of the best results, avoiding intercurrences.
Acknowledgments
We would like to express our sincere gratitude to the Pineda Injectable Laboratory - Grupo Hervas for the valuable scientific partnership, and to the Institute of Science, Technology, and Quality (ICTQ) for providing the funding. Both institutions played a pivotal role in ensuring the successful publication of this work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zhang S, Duan E. Fighting against skin aging. Cell Transplant. 2018;27(5):729–738. doi:10.1177/0963689717725755
2. Kim YJ, Lee JH, Lee SG, Lee HH. Developing sustainable competitive strategies in the beauty service industry: a SWOT-AHP approach. Sustainability. 2021;13(19):10852. doi:10.3390/su131910852
3. Heli de Campos J. Visagismo, dimorfismo sexual, proporção áurea e simetria como bases sólidas para alterações imagéticas. Aesthet Orofac Sci. 2021;2(2). doi:10.51670/aos.v2i2.52
4. Arcadier J Individualização do plano de tratamento em harmonização orofacial: a importância da morfopsicologia e visagismo – revisão narrativa. Repositório Institucional da Universidade Fernando Pessoa; 2021. Available from: http://hdl.handle.net/10284/10838.
5. de Duarte CEO. Percepção de vaidade e beleza em adultos, idosos e longevos. Universidade de Passo Fundo; 2020. Available from: http://tede.upf.br:8080/jspui/handle/tede/1972.
6. Hallawell PC. Visagismo: Harmonia e Estética.
7. Mammucari M, Maggiori E, Russo D, et al. Mesotherapy: from historical notes to scientific evidence and future prospects. Sci World J. 2020;2020:1–9. doi:10.1155/2020/3542848
8. Stachowski J, Botts K, Rine L, Kato D, Pollock J. Mesotherapy: cosmetic applications. Int J Pharm Compd. 2006;10(5):331–334.
9. Jayasinghe S, Guillot T, Bissoon L, Greenway F. Mesotherapy for local fat reduction. Obes Rev. 2013;14(10):780–791. doi:10.1111/obr.12049
10. Khalili M, Amiri R, Iranmanesh B, Zartab H, Aflatoonian M. Safety and efficacy of mesotherapy in the treatment of melasma: a review article. J Cosmet Dermatol. 2022;21(1):118–129. doi:10.1111/jocd.14644
11. Matarasso A, Pfeifer TM. Mesotherapy for body contouring. Plast Reconst Surg. 2005;115(5):1420–1424. doi:10.1097/01.PRS.0000162227.94032.ED
12. Dadkhahfar S, Robati RM, Gheisari M, Moravvej H. Subcision: indications, adverse reactions, and pearls. J Cosmet Dermatol. 2020;19(5):1029–1038. doi:10.1111/jocd.13308
13. Friedmann D, Vick G, Mishra V. Cellulite: a review with a focus on subcision. Clin Cosmet Investig Dermatol. 2017;10:17–23. doi:10.2147/CCID.S95830
14. Rang H, Ritter J, Flower R, Henderson G, Dale M. Rang and Dale’s Pharmacology.
15. Trenker R, Jura N. Receptor tyrosine kinase activation: from the ligand perspective. Curr Opin Cell Biol. 2020;63:174–185. doi:10.1016/j.ceb.2020.01.016
16. Zuo H, Wan Y. Nuclear receptors in skeletal homeostasis. Curr Top Dev Biol. 2017;125:71–107. doi:10.1016/bs.ctdb.2017.01.002
17. Soudjin W, van Wijngaarden I, IJzerman AP. Stereoselectivity of drug-receptor interactions. IDrugs. 2003;6(1):43–56.
18. Golan DE, Armstrong EJ, Armstrong AW. Principles of Pharmacology: The Pathophysiologic Basis of Drug Therapy.
19. Shulman M, Wai JM, Nunes EV. Buprenorphine treatment for opioid use disorder: an overview. CNS Drugs. 2019;33(6):567–580. doi:10.1007/s40263-019-00637-z
20. Alves‐Bezerra M, Cohen DE. Triglyceride metabolism in the liver. Comprehensive Physiolo. 2017:1–22. doi:10.1002/cphy.c170012
21. Yang A, Mottillo EP. Adipocyte lipolysis: from molecular mechanisms of regulation to disease and therapeutics. Biochem J. 2020;477(5):985–1008. doi:10.1042/BCJ20190468
22. Frühbeck G, Méndez-Giménez L, Fernández-Formoso JA, Fernández S, Rodríguez A. Regulation of adipocyte lipolysis. Nutr Res Rev. 2014;27(1):63–93. doi:10.1017/S095442241400002X
23. de Freitas G. BIOESTIMULADORES DE COLÁGENO INJETÁVEIS: Ácido Poli-I-lático, Hidroxiapatita de Cálcio e Policaprolactona. Faculdade Sete Lagoas. 2021. Available from: https://faculdadefacsete.edu.br/monografia/items/show/3846.
24. Rebellato PRO, de Torre DS, Rastelli GJC, Schmitt JV, Medaglia CR. Calcium hydroxylapatite for collagen biostimulation in the neck. Int J Dermatol Venereology Leprosy Sci. 2020;3(1):27–31. doi:10.33545/26649411.2020.v3.i1a.35
25. Christen MO. Collagen stimulators in body applications: a review focused on Poly-L-Lactic Acid (PLLA). Clin Cosmet Investig Dermatol. 2022;15:997–1019. doi:10.2147/CCID.S359813
26. de Lima LP, de Almeida F, de Barbosa AP. BIOESTIMULADORES DE COLÁGENO: BENEFÍCIOS, INDICAÇÕES, CONTRAINDICAÇÕES, DILUIÇÃO E MÉTODOS DE APLICAÇÃO. J Appl Pharm Sci. 2022;7:140–162.
27. Van Loghem J, Yutskovskaya YA, Werschler WMP. Calcium hydroxylapatite: over a decade of clinical experience. J Clin Aesthet Dermatol. 2015;8(1):38.
28. de Almeida AT, Figueredo V, da Cunha ALG, et al. Consensus recommendations for the use of hyperdiluted calcium hydroxyapatite (radiesse) as a face and body biostimulatory agent. Plast Reconstr Surg Glob Open. 2019;7(3):e2160. doi:10.1097/GOX.0000000000002160
29. Haddad A, Kadunc BV, Guarnieri C, Noviello JS, da Cunha MG, Parada MB. Current concepts in the use of poly-L-lactic acid for facial rejuvenation: literature review and practical aspects. Surg Cosmet Dermatol. 2017;9(1). doi:10.5935/scd1984-8773.201791952
30. de Lima NB, Soares MDL. Utilização dos bioestimuladores de colágeno na harmonização orofacial. Clin Lab Res Dent. 2020. doi:10.11606/issn.2357-8041.clrd.2020.165832
31. Shridharani SM, Tisch GM, Ebersole TG, Moak TN, Edwartz C. Clinical experience of poly‐L‐lactic acid injections for body contouring treatment. J Cosmet Dermatol. 2021;20(6):1655–1662. doi:10.1111/jocd.14141
32. de Melo F, Nicolau P, Piovano L, et al. Recommendations for volume augmentation and rejuvenation of the face and hands with the new generation polycaprolactone-based collagen stimulator (Ellanse®). Clin Cosmet Investig Dermatol. 2017;10:431–440. doi:10.2147/CCID.S145195
33. Christen MO, Vercesi F. Polycaprolactone: how a well-known and futuristic polymer has become an innovative collagen-stimulator in esthetics. Clin Cosmet Investig Dermatol. 2020;13:31–48. doi:10.2147/CCID.S229054
34. Wong V. Hanging by a thread: choosing the right thread for the right patient. J Dermatol Cosmetol. 2017;1(4). doi:10.15406/jdc.2017.01.00021
35. Cobo R. Use of polydioxanone threads as an alternative in nonsurgical procedures in facial rejuvenation. Facial Plast Surg. 2020;36(4):447–452. doi:10.1055/s-0040-1714266
36. Suh DH, Jang HW, Lee SJ, Lee WS, Ryu HJ. Outcomes of polydioxanone knotless thread lifting for facial rejuvenation. Dermatol Surg. 2015;41(6):720–725. doi:10.1097/DSS.0000000000000368
37. Karimi K, Reivitis A. Lifting the lower face with an absorbable polydioxanone (PDO) Thread. J Drugs Dermatol. 2017;16(9):932–934.
38. Arora G, Arora S. Thread lift in breast ptosis. J Cutan Aesthet Surg. 2017;10(4):228–230. doi:10.4103/JCAS.JCAS_91_17
39. Yu AY. Restoration liposuction of the abdomen: high-definition liposuction with umbilicus and lower abdomen improvement using polydioxanone threads. Aesthet Surg J. 2023;43(6):NP413–NP423. doi:10.1093/asj/sjac232
40. Lee W, Jung YC, Yang EJ. Gluteal soft-tissue repositioning using polydioxane threads. Dermatol Surg. 2021;47(7):e195–e199. doi:10.1097/DSS.0000000000002975
41. Krupek T, Mareze-da-Costa CE. Mecanismo de Ação de Compostos Utilizados na Cosmética para o Tratamento da Gordura Localizada e da Celulite. Revista Saúde e Pesquisa. 2012;5(3):555–566.
42. Oliveira LPM, Assis AMO, Silva MDCMD, et al. Fatores associados a excesso de peso e concentração de gordura abdominal em adultos na cidade de Salvador, Bahia, Brasil. Cad Saude Publica. 2009;25(3):570–582. doi:10.1590/S0102-311X2009000300012
43. Oakley AM, Patel BC Stretch Marks.; 2022. [Internet]. Treasure Island (FL): StatPearls Publishing; 2023. PMID: 28613776.
44. Ward LC, Müller MJ. Bioelectrical impedance analysis. Eur J Clin Nutr. 2013;67(S1):S1–S1. doi:10.1038/ejcn.2012.148
45. Kushner RF. Bioelectrical impedance analysis: a review of principles and applications. J Am Coll Nutr. 1992;11(2):199–209. doi:10.1080/07315724.1992.12098245
46. Ponti F, de Cinque A, Fazio N, Napoli A, Guglielmi G, Bazzocchi A. Ultrasound imaging, a stethoscope for body composition assessment. Quant Imaging Med Surg. 2020;10(8):1699–1722. doi:10.21037/qims-19-1048
47. Wagner DR. Ultrasound as a tool to assess body fat. J Obes. 2013;2013:1–9. doi:10.1155/2013/280713
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.