Back to Journals » International Journal of General Medicine » Volume 15
Body Dysmorphic Disorder Symptoms: Prevalence and Risk Factors in an Arab Middle Eastern Population
Authors Alghamdi WA, Subki AH ![]() , Khatib HA, Butt NS
, Khatib HA, Butt NS ![]() , Alghamdi RA
, Alghamdi RA ![]() , Alsallum MS
, Alsallum MS ![]() , Alharbi AA, Almatrafi MN, Alobisi AA, Al-Zaben F, Koenig HG
, Alharbi AA, Almatrafi MN, Alobisi AA, Al-Zaben F, Koenig HG
Received 17 July 2021
Accepted for publication 29 December 2021
Published 11 March 2022 Volume 2022:15 Pages 2905—2912
DOI https://doi.org/10.2147/IJGM.S329942
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Waleed Ahmed Alghamdi,1 Ahmed Hussein Subki,2 Hazim Abdulkarim Khatib,3 Nadeem Shafique Butt,4 Rahaf Ali Alghamdi,1 Mohammed Saad Alsallum,5 Ahmed A Alharbi,1 Mohammad Nasser Almatrafi,1 Abdullah Ahmed Alobisi,1 Faten Al-Zaben,1 Harold G Koenig1,6,7
1Department of Psychiatry, King Abdulaziz University, Jeddah, Saudi Arabia; 2Department of Internal Medicine, King Faisal Specialist Hospital & Research center, Jeddah, Saudi Arabia; 3Department of Internal Medicine, King Abdulaziz Hospital, Jeddah, Saudi Arabia; 4Department of Community Medicine, King Abdulaziz University, Jeddah, Saudi Arabia; 5Department of Neurology, King Abdulaziz Medical City, Jeddah, Saudi Arabia; 6School of Public Health, Ningxia Medical University, Yinchuan, People’s Republic of China; 7Duke University Medical Center, Durham, NC, USA
Correspondence: Waleed Ahmed Alghamdi; Harold G Koenig, Email [email protected]; [email protected]
Background: The present study examined the prevalence of and risk factors for symptoms of body dysmorphic disorder (BDD) in the general population of Jeddah, a large port city in Saudi Arabia.
Methods: This cross-sectional study surveyed a convenience sample of 520 adults. We used a validated self-screening measure to assess BDD, the body dysmorphic disorder questionnaire (BDDQ).
Results: The prevalence of significant BDD symptoms among the general Saudi population was 8.8% (ie, those scoring above the cut off for BDD on the BDDQ). Over half (52%) of all respondents reported concerns about the attractiveness of their body parts, and of those expressing such concerns, 66% were preoccupied with these thoughts. Only 3% of all respondents opted for cosmetic surgery because of these concerns, and most of those individuals (69%) had only one surgery. Nearly 9% of all respondents reported that these concerns affected their relationships with family and friends. Almost 15% of all participants spent an hour or more each day thinking about these concerns. Patients who reported a history of depression were 3.8 times more likely to have BDD. Other variables included in the model predicting high BDD scores (eg, age, job status, and marital status) did not achieve statistical significance.
Conclusion: Significant symptoms of BDD (based on the BDDQ) are not uncommon among the general population of Jeddah, Saudi Arabia. Risk factors for this condition were female gender, younger age, being unmarried, and in bivariate and multivariate analyses, history of depression and female gender. These findings underscore the need for increased awareness by clinicians of this disorder, particularly when treating patients with depressive disorder, particularly among women.
Keywords: body dysmorphic disorder, body image, prevalence, Saudi Arabia
Introduction
Body dysmorphic disorder (BDD) is an under-recognized body image disorder that has been associated with a high rate of delusional symptoms and suicide attempts. It is characterized by preoccupation with non-existent or slight defects in physical appearance. As a result, patients suffering from BDD believe that they look abnormal, unattractive, or deformed, when in reality their physical appearance is normal.1 These preoccupations can involve any body part, although, in the majority of the cases, it involves the nose, the ears, the face, hair, or features related to sexuality (eg, breasts in women; muscular build or penis size in men).2,3
Individuals with BDD are likely to present to mental health professionals and other clinicians such as dermatologists, plastic surgeons, primary care physicians, pediatricians, and dentists.4 Most BDD patients seek non-psychiatric treatment (most commonly dermatologic and surgical) for their perceived physical defects. However, this treatment appears ineffective for most patients and can be risky for clinicians.5 In contrast, the most effective treatment is pharmacotherapy (eg, selective serotonin reuptake inhibitors or clomipramine) and cognitive-behavioral therapy explicitly tailored to BDD.3 The prevalence of BDD in the general population ranges between 0.7% and 2.4% when diagnosed using the DSM-III-R or DSM-IV criteria.6
BDD is more common than most clinicians believe. Up to 1.9% of nonclinical samples, 6–12% of psychiatric outpatients, and 3–40% of patients in other clinical settings may have the disorder.7 However, the actual prevalence is uncertain given that there are relatively few epidemiological studies on BDD prevalence.6 In addition, the mean age of onset of BDD is approximately 14–19 years, and it usually develops gradually rather than abruptly, reducing insight into the disorder.6 BDD risk factors include having blood relatives with BDD or obsessive-compulsive disorder, negative life experiences (childhood teasing and trauma), certain personality traits (perfectionism, societal pressure or expectations of beauty), and psychiatric disorders (anxiety or depression).2,8–10
The actual prevalence of those suffering from BDD is underestimated because of feelings of shame and shyness that prevent individuals from seeking medical attention.8 At times, the delusional nature of such concerns and the lack of insight associated with the disorder may both be contributive factors. Thus, many people seek non-psychiatric treatment or no treatment at all (or present only late in the course of the disease) and therefore go undetected. Understanding the prevalence in Saudi Arabia is important because of cultural and religious factors that may influence the importance placed on physical appearance, which may increase such bodily concerns. Furthermore, identifying risk factors for BDD is crucial because it allows clinicians to screen those at particularly high risk for this condition. However, to the best of the authors’ knowledge, no studies have been reported from Saudi Arabia on the prevalence or risk factors for BDD in the general population. The present study seeks to fill that gap.
Materials and Methods
Study Design and Participants
A cross-sectional study was conducted to assess the prevalence and risk factors for BDD. A convenience sample of 520 adults in Jeddah, Saudi Arabia, completed a questionnaire. The response rate approached 90% (520 out of approximately 580 who were asked to complete the questionnaire).
Ethical Consideration
Written consent was obtained from each participant before asking them to complete the questionnaire. The purpose of the study was explained, and confidentiality was assured. Approval from the institutional review board (IRB) of King Abdulaziz University was obtained before beginning the study. The IRB approval number is 374–17. This study was conducted in accordance with the Declaration of Helsinki.
Data Collection and Measures
The first part of the questionnaire asked about age, gender, education level, nationality, occupation, income, and marital status. Participants were also asked if they had a history of depression or obsessive-compulsive disorder (yes or no, for each question). The second part of the survey focused on BDD-related questions using the self-rated Body Dysmorphic Disorder Questionnaire (BDDQ), a measure that has shown good concurrent validity when compared to the Structured Clinical Interview for DSM-IV (SCID), having a sensitivity of 94% in detecting BDD, a specificity of 90%, and a likelihood ratio of 9.4.11 One question was added in addition to the BDDQ: “Have you ever done any cosmetic surgery due to concerns about your appearance?” The original English version of the BDDQ was translated into Arabic by two independent native Arabic physicians fluent in English, and then the Arabic version was translated back to English by two independent native English physicians fluent in Arabic.
Statistical Analysis
Analyses were performed using the Statistical Package for Social Science (SPSS), version 22 (IBM, Armonk, NY, USA). The difference between respondents scoring positively on the BDDQ screening questionnaire and those scoring below the cutoff was determined by the independent samples t-test chi-square statistic and Fisher’s Exact test (for categorical variables). Odds ratio and 95% confidence intervals were derived from a logistic regression model. All variables were categorical in nature in bivariate and multivariate analyses, with the exception of age, which was treated as continuous in the multivariate analyses to increase the precision of the estimate. Statistical significance was set at 0.05.
Results
Table 1 describes the distribution of sociodemographic characteristics of the sample by significant BDD symptoms. Younger age was associated with significant BBD symptoms (p = 0.043). BDD-positive cases were more prevalent in those less than 40 years of age. Gender also distinguished the two groups (p = 0.019), with BDD cases more prevalent among females. BDD was more common in unmarried participants (p = 0.014). A self-reported past diagnosis of depression was also related to BDD (p = 0.020). No significant associations were found with nationality, education, living status, job status, income, or self-reported history of obsessive compulsive disorder.
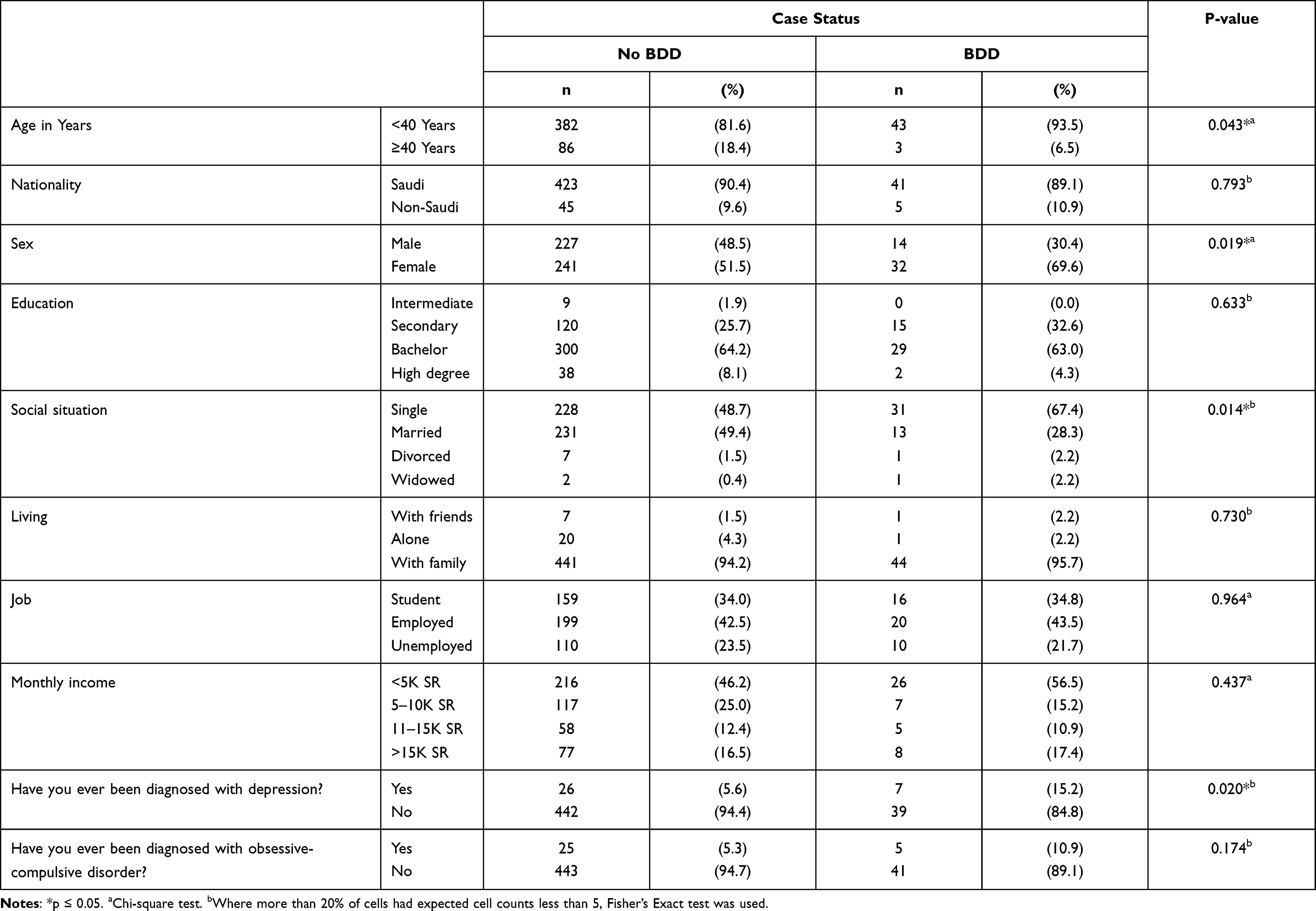 |
Table 1 Sociodemographic and Mental Health Characteristics of Participants by Cut-off Score on the BDDQ Indicating Significant BDD Symptoms |
Table 2 describes the distribution of responses to BDDQ. More than half (52%) of all respondents reported concerns about the attractiveness of their body parts, and of those, 66% were preoccupied with these concerns. Most of the respondents reported concern about their hair (33.5%), breast (17.9%), and skin (9.6%), while 13.1% of respondents reported multiple sites. Only 3.1% of all respondents opted for cosmetic surgery, and most of these individuals had only one surgery (68.8%). Emotional and social distress due to perceived appearance were reported by 25.8% and 15.2% of all respondents, respectively. Ten percent indicated they had difficulty performing tasks at school and in the workplace because of BDD concerns. Nearly one in five respondents said their concerns limited their participation in outdoor activities. In addition, 9% of all participants reported that their relationships with family and friends were affected by these concerns. Almost 15% of all respondents spent more an hour per day or more thinking about these concerns.
 |
Table 2 Distribution of Participant Responses to Body Dysmorphic Disorder Questionnaire |
Table 3 presents the results of logistic regression modeling. The overall model was significant, χ2(7) = 25.9, p < 0.001, suggesting that age, sex, job status, marital status, and history of depression had a significant effect on the likelihood of scoring above the cutoff on the BDDQ (case status). The regression coefficient for gender (B = 0.74, OR = 2.09, 95% CI = 1.04–4.21) indicated that women were more than twice as likely as men to score above the cutoff on the BDDQ. Similarly, a history of depression was also found to be a significant predictor (B = 1.34, OR = 3.83, 95% CI = 1.45–10.13). Participants with a history of depression were nearly four times more likely to have BDD. Age, job status, and marital status were unrelated to case status in the logistic regression model.
 |
Table 3 Results of Logistic Regression Analysis |
Discussion
The present study examined the prevalence and risk factors for significant BDD symptoms in the general population of Jeddah, Saudi Arabia. Nearly one in ten (8.8%) scored above the cutoff on the BDDQ. This prevalence rate was significantly higher than in the United States and Germany, with 2.4% and 1.7% rates, respectively.12,13 The international weighted prevalence of BDD has been reported to be 1.9%.7 Several studies have been conducted to assess the prevalence of BDD in Saudi Arabia in specific clinical populations, but none until the present study has done so in the general community. One study assessed BDD among patients visiting dermatology clinics, finding a prevalence of 18.6%.14 Another study that examined Arab dermatology patients reported a prevalence of 14.1%.15 Other studies of patients seeking facial plastic surgery and female medical students have reported a prevalence of 14.2% and 4.4%, respectively.16,17 The differences between our study and the studies in the US and Germany could be explained by methodological factors. The US study used experienced interviewers administering structured diagnostic interviews, and the German study used the face-to-face method of conducting its self-rating scales. The present study identified cases using a self-reported questionnaire, the BDDQ; thus, an accurate comparison could not be made. Another explanation for the high rate reported here may have been due to social or cultural factors. For instance, women in Saudi society may feel that their physical appearance affects their options with regard to marriage, which may lead to increased BDD concerns.18 In contrast to the present findings, several studies have found no difference in rates of BDD between males and females.7,12,13 The cultural norms in Saudi Arabia, which include the segregation between genders at school and college, may affect how Saudi women view their bodies, leading to anxiety, shame, and more severe judgment about physical appearance.8
Age, marital status, and employment status were not significant risk factors for BDD in the present study. This varies from reports in Germany, which found that those with BDD were more likely to be unemployed and not married.13 Although we found that being unmarried was associated with BDD in bivariate analyses, other factors appeared to explain this finding in multivariate analyses. The difference between the German study and the present study could be attributed to the social differences between the two societies and how BDD effects could depend on cultural factors. Multiple studies in Saudi Arabia, Beirut and Qatar showed female and male perception of ideal weight as being overweight.19–22 While an international study showed that in Western countries, including United States and Germany, the perception of ideal body is thin and even underweight.23 The differences in body perception between the Arabian and Western societies could be explained in part by differences in terms of privacy and conservativeness, since the Saudi society is closed one where privacy is among the most important values. Furthermore, religious beliefs in Islam require conservative clothing for women, which may affect the ideal standards for body image in this country.
A history of depression was a risk factor for BDD in the present study, which is consistent with most of the literature indicating a close relationship between depressive disorder and BDD.8,24 A temporal relationship, however, could not be established here in terms of causality. BDD was found to have an increased risk of suicide based on the presence of other psychiatric comorbidities, including major depressive disorder and personality disorders.25 Depression could develop due to having BDD, a result of prolonged anxiety and shame associated with BDD and the resulting social dysfunction.18 Alternately, BDD may be more likely to develop in those with pre-existing depression due to greater sensitivity over physical appearance caused by depression.
Study Limitations
Several limitations of the present study may affect the generalizability and interpretation of the results reported here. The first is the possible overestimation of BDD prevalence due to the self-reported nature of the BDDQ screening measure, rather than using a structured diagnostic interview administered by a clinician. Secondly and finally, the convenience nature of the sample acquired from a large port city in Saudi Arabia, which likely prevents generalizing these results to the entire country.
However, several strengths also deserve mention. First, to our knowledge, this is the first study examining the prevalence of BDD symptoms among a general community population in Saudi Arabia. Second, the BDDQ is a psychometrically valid measure of BDD symptoms that has been used in many countries throughout the world, allowing for comparison. Third, logistic regression analyses were used to control for potential confounders and variables, helping to identify independent risk factors for BDD.
Conclusions
The present study found a relatively high prevalence rate (8.8%) of significant BDD symptoms (based on scoring above the cutoff on the BDDQ) in a general community sample in Jeddah, Saudi Arabia. Risk factors associated with significant BDD symptoms were female gender and a history of depression. Given the relatively high prevalence of this condition in Saudi Arabia, clinicians need to become more aware of BDD and consider screening for BDD among patients presenting with depression, particularly female patients. Likewise, screening for depressive disorder among those with BDD should also be considered, as BDD is a debilitating disorder that often runs a chronic course without treatment and screening may facilitate earlier detection and intervention. Future studies, particularly longitudinal studies, are needed to determine the causal nature of risk factors for BDD identified in this study.
Abbreviations
BDD, body dysmorphic disorder; BDDQ, body dysmorphic disorder questionnaire.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics Approval and Consent to Participate
Ethical approval was obtained from the institutional review board (IRB) of King Abdulaziz University with reference number 374-17. Ethical principles were maintained throughout the research process. All participants signed informed consent, and confidentiality and anonymity were assured as no personal identifiers were used. All data were stored on workplace computers with access to study personal only.
Consent for Publication
Written informed consent for publication was obtained.
Acknowledgments
We want to thank profusely all the men and women who participated in this study.
Author Contributions
The first and corresponding author (WA) is the owner of the intellectual idea, contributed to the analysis, writing of the manuscript, and final review. AS contributed to the conceptualization of the project, proposal, methodology, and writing of the manuscript. HK contributed to data collection, and data entry, and writing of the manuscript and final review. NB contributed to data analysis and writing of the results. RA contributed to data collection, and data entry, and writing of the manuscript. MA contributed to data collection, and data entry, and writing of the manuscript. AA Alharbi contributed to data collection, and data entry, and writing of the manuscript. MA contributed to data collection, and data entry, and writing of the manuscript. AA Alobisi contributed to data collection, and data entry, and writing of the manuscript. FA was a supervising author in the paper and final review. HK was a supervising author in the paper, provided guidance, expertise, reviews, and valuable recommendations, and contributed to the writing of the paper as well. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research is self-funded.
Disclosure
The authors declare that they have no competing interests.
References
1. Veale D, Miles S, Valiallah N, et al. The effect of self-focused attention and mood on appearance dissatisfaction after mirror-gazing: an experimental study. J Behav Ther Exp Psychiatry. 2016;52:38–44. doi:10.1016/j.jbtep.2016.03.002
2. Rosen JC, Reiter J, Orosan P. Cognitive-behavioral body image therapy for body dysmorphic disorder. J Consult Clin Psychol. 1995;63(2):263. doi:10.1037/0022-006X.63.2.263
3. Husain Z, Janniger E, Krysicka J, Micali G, Schwartz R. Body dysmorphic disorder: beyond skin deep. G Ital Dermatol Venereol. 2014;149(4):447–452.
4. Ramos TD, Brito M, Piccolo MS, Rosella M, Sabino Neto M, Ferreira LM. Body dysmorphic symptoms scale for patients seeking esthetic surgery: cross-cultural validation study. Sao Paulo Med J. 2016;134(6):480–490. doi:10.1590/1516-3180.2016.0068160416
5. Nakamura M, Koo J. Personality disorders and the “difficult” dermatology patient: maximizing patient satisfaction. Clin Dermatol. 2017;35(3):312–318. doi:10.1016/j.clindermatol.2017.01.009
6. Möllmann A, Dietel FA, Hunger A, Buhlmann U. Prevalence of body dysmorphic disorder and associated features in German adolescents: a self-report survey. Psychiatry Res. 2017;254:263–267. doi:10.1016/j.psychres.2017.04.063
7. Veale D, Gledhill LJ, Christodoulou P, Hodsoll J. Body dysmorphic disorder in different settings: a systematic review and estimated weighted prevalence. Body Image. 2016;18:168–186. doi:10.1016/j.bodyim.2016.07.003
8. Weingarden H, Renshaw KD, Wilhelm S, Tangney JP, DiMauro J. Anxiety and shame as risk factors for depression, suicidality, and functional impairment in body dysmorphic disorder and obsessive compulsive disorder. J Nerv Ment Dis. 2016;204(11):832.
9. Angelakis I, Gooding PA, Panagioti M. Suicidality in body dysmorphic disorder (BDD): a systematic review with meta-analysis. Clin Psychol Rev. 2016;49:55–66. doi:10.1016/j.cpr.2016.08.002
10. Blashill AJ, Tomassilli J, Biello K, O’Cleirigh C, Safren SA, Mayer KH. Body dissatisfaction among sexual minority men: psychological and sexual health outcomes. Arch Sex Behav. 2016;45(5):1241–1247. doi:10.1007/s10508-015-0683-1
11. Brohede S, Wingren G, Wijma B, Wijma K. Validation of the body dysmorphic disorder questionnaire in a community sample of Swedish women. Psychiatry Res. 2013;210(2):647–652. doi:10.1016/j.psychres.2013.07.019
12. Koran LM, Abujaoude E, Large MD, Serpe RT. The prevalence of body dysmorphic disorder in the United States adult population. CNS Spectr. 2008;13(4):316–322. doi:10.1017/S1092852900016436
13. Rief W, Buhlmann U, Wilhelm S, Borkenhagen ADA, BrÄHler E. The prevalence of body dysmorphic disorder: a population-based survey. Psychol Med. 2006;36(6):877–885. doi:10.1017/S0033291706007264
14. PI HGA, Alharbi M, Alyousif LAM, et al. Prevalence of body dysmorphic disorder in patients attending dermatology clinic in Saudi Arabia/Qassim Region; 2019.
15. AlShahwan MA. Prevalence and characteristics of body dysmorphic disorder in Arab dermatology patients. Saudi Med J. 2020;41(1):73–78. doi:10.15537/smj.2020.1.24784
16. Al Shuhayb Z. Prevalence of body dysmorphic disorder among Saudis seeking facial plastic surgery. Saudi Surg J. 2019;7(3):83–86. doi:10.4103/ssj.ssj_11_19
17. Shaffi Ahamed S, Enani J, Alfaraidi L, et al. Prevalence of body dysmorphic disorder and its association with body features in female medical students. Iran J Psychiatry Behav Sci. 2016;10(2):e3868–e3868. doi:10.17795/ijpbs-3868
18. Phillips KA, Diaz SF. Gender differences in body dysmorphic disorder. J Nerv Ment Dis. 1997;185(9):570–577. doi:10.1097/00005053-199709000-00006
19. Musaiger AO, Shahbeek NE, Al-Mannai M. The role of social factors and weight status in ideal body-shape preferences as perceived by Arab women. J Biosoc Sci. 2004;36(6):699–707. doi:10.1017/S0021932003006412
20. Khawaja M, Afifi-Soweid R. Images of body weight among young men and women: evidence from Beirut, Lebanon. J Epidemiol Community Health. 2004;58(4):352–353. doi:10.1136/jech.2003.010785
21. Khalaf A, Westergren A, Berggren V, Ekblom Ö, Al-Hazzaa HM. Perceived and ideal body image in young women in South Western Saudi Arabia. J Obes. 2015;2015:697163. doi:10.1155/2015/697163
22. Al Qauhiz NM. Obesity among Saudi female university students: dietary habits and health behaviors. J Egypt Public Health Assoc. 2010;85(1–2):45–59.
23. Swami V, Frederick DA, Aavik T, et al. The attractive female body weight and female body dissatisfaction in 26 countries across 10 world regions: results of the International Body Project I. Pers Soc Psychol Bull. 2010;36(3):309–325. doi:10.1177/0146167209359702
24. Frare F, Perugi G, Ruffolo G, Toni C. Obsessive–compulsive disorder and body dysmorphic disorder: a comparison of clinical features. Eur Psychiatry. 2004;19(5):292–298. doi:10.1016/j.eurpsy.2004.04.014
25. Eskander N, Limbana T, Khan F. Psychiatric comorbidities and the risk of suicide in obsessive-compulsive and body dysmorphic disorder. Cureus. 2020;12(8):e9805–e9805. doi:10.7759/cureus.9805
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.